Embed Size (px)
Citation preview

Reparative Therapy for Acute
Ischemic Stroke with AllogeneicMesenchymal Stem Cells from Adipose Tissue:A Safety AssessmentA Phase II Randomized, Double-blind, Placebo-controlled,
Single-center, Pilot Clinical Trial
Exuperio D�ıez-Tejedor, MD, PhD, FAHA, FESO, Mar�ıa Guti�errez-Fern�andez, BS, PhD,
Patricia Mart�ınez-S�anchez, MD, PhD, Berta Rodr�ıguez-Frutos, BS, PhD,
Gerardo Ruiz-Ares, MD, PhD, Manuel Lara Lara, MD,
and Blanca Fuentes Gimeno, MD, PhD
From the Stroke Ce
University Hospital, IdiP
Aut�onoma de Madrid, M
Received February 5, 20
June 15, 2014.
This study was suppo
Policy and Equality (EC1
2694
Background: Few studies have evaluated the possible beneficial effect of the admin-
istration of stem cells in the early stages of stroke. Intravenous administration of allo-
geneic mesenchymal stem cells (MSCs) from adipose tissue in patients with acute
stroke could be a safe therapy for promoting neurovascular unit repair, consequently
supporting better functional recovery. We aim to assess the safety and efficacy of
MSC administration and evaluate its potential as a treatment for cerebral protection
and repair. Materials: A Phase IIa, prospective, randomized, double-blind, placebo-
controlled, single-center, pilot clinical trial. Twenty patients presenting acute ischemic
strokewill be randomized in a 1:1 proportion to treatment with allogeneicMSCs from
adipose tissue or to placebo (or vehicle) administered as a single intravenous dose
within the first 2 weeks after the onset of stroke symptoms. The patients will be fol-
lowed up for 2 years. Primary outcomes for safety analysis: adverse events (AEs)
and serious AEs; neurologic and systemic complications, and tumor development.
Secondary outcomes for efficacy analysis: modified Rankin Scale; NIHSS; infarct
size; and biochemical markers of brain repair (vascular endothelial growth factor,
brain-derived neurotrophic factor, and matrix metalloproteinases 9). Results and
Conclusions: To our knowledge, this is the first, phase II, pilot clinical trial to investi-
gate the safety and efficacy of intravenous administration of allogeneic MSCs from
adipose tissue within the first 2 weeks of stroke. In addition, its results will help us
define the best criteria for a future phase III study. Key Words: Acute ischemic
stroke—stem cells—reparative therapy—clinical trial—safety.
� 2014 by National Stroke Association
Introduction
Cerebrovascular disease is a serious public health prob-
lem. In Spain, it is the leading cause of mortality in
nter, Department of Neurology, La Paz
AZ Health Research Institute, Universidad
adrid, Spain.
14; revision receivedMay 12, 2014; accepted
rted by Spanish Ministry of Health, Social
0-171).
Journal of Stroke and Cerebrovascular Diseases
women and the third in men and the estimated annual
incidence of stroke is 187 cases per 100,000 individuals.1
It also represents the greatest cause of disability.
Address correspondence to Exuperio D�ıez-Tejedor, MD, PhD,
FAHA, FESO, Department of Neurology and Stroke Center, La Paz
University Hospital, IdiPAZ Health Research Institute, Paseo de la
Castellana 261, Madrid 28046, Spain. E-mail: exuperio.diez@salud.
madrid.org.
1052-3057/$ - see front matter
� 2014 by National Stroke Association
http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2014.06.011
, Vol. 23, No. 10 (November-December), 2014: pp 2694-2700

REPARATIVE THERAPY FOR ACUTE ISCHEMIC STROKE 2695
Therefore, strategies for prevention and treatment of
stroke need to be improved to reduce its incidence and
avoid potential sequelae.
Brain repair is a natural process that is activated after
injury and that involves neurogenesis, gliogenesis, oligo-
dendrogenesis, synaptogenesis, and angiogenesis. These
inter-related processes could provide new therapeutic
tools to mitigate the damage caused by stroke.2 The pro-
motion of brain plasticity can be achieved by stimulating
endogenous mechanisms through the use of rehabilitation
and trophic factors or by exogenousmechanisms using cell
therapy to promote tissue repair and functional recovery.
Stem cells are immature cells with the capacity to differ-
entiate into multiple cell types. Various stem cell lines
have been tested in neurologic diseases, and preclinical
data regarding mesenchymal stem cells (MSCs) suggest
that strategies based on these cells may become effective
and safe therapies for a large number of diseases associ-
ated with inflammation and/or tissue damage.3 Progress
in this field has opened a new and promising avenue in
the search for new therapeutic strategies for stroke: the
enhancement of brain plasticity, a therapy that would
complement the current treatment of acute cerebral
infarction.
At present, designing new clinical trials that demon-
strate efficacy is complicated by a number of ethical, tech-
nical, and medical issues,4-6 some of which are related to
discovering a more suitable cell type, route, and time of
administration. In terms of cell type, the safer cells for
use would be autologous because the risk of rejection is
eliminated. However, this therapy’s primary limitation
is that it can only be applied several weeks after the
stroke because it takes time to cultivate the cells. The
administration of allogeneic stem cells could be a good
option because these cells demonstrate a lack of
HLA-class II antigens,7 thus avoiding the risk of rejection.
An important point regarding translational research is
that the optimal route of administration remains unclear.
For the transition to clinical practice, less invasive
methods such as intravenous administration would be
preferable. Several studies have shown that MSCs do
not need to migrate and nest at the injury site to achieve
good functional recovery, which could be related to the
stimulation or secretion of trophic factors.8,9
Another issue for investigation is the proper time win-
dow. Most of the studies using animal models have been
conducted in the later stages after stroke.10 However, in
our opinion, stem cells should be administered during
the acute phase to help inhibit the first steps of the
ischemic cascade and to enhance the mechanisms of pro-
tection and brain repair.
MSC transplantation has been tested on animal models
for the treatment of various neurologic diseases, including
cerebral infarction,11,12 and has produced good results in
terms of structural and functional recovery.10,11,13 The use
of MSCs from adipose tissue has recently gained more
interest because these cells are easier to obtain than
MSCs from bone marrow and are also effective in stroke
models.14,15 With respect to the intravenous
administration of allogeneic MSCs from adipose tissue,
our group has conducted a study on cerebral infarction
in rats in which these allogeneic MSCs were compared
with other bone marrow-derived MSCs. The results
showed that both cell types have similar efficacy in func-
tional recovery with reduced brain damage (cell death)
and increases in cellular proliferation, neurogenesis, oligo-
dendrogenesis, synaptogenesis, and angiogenesis markers
at 14 days after stroke.15
From a clinical standpoint, these cells have been suc-
cessfully transplanted into the brains of stroke patients,
with excellent tolerability and without complications. A
clinical trial that evaluated the safety of the procedure
and the tolerance of the stereotactic implantation of autol-
ogous bone marrow-derived MSCs in 5 patients with
cerebral infarction showed no significant adverse effects
during the 1-year follow-up. Improvements were noted
in the patients’ neurologic condition, but conclusive re-
sults could not be obtained given the small sample
size.16 Regarding other noninvasive routes of administra-
tion, a clinical trial of intravenous administration of autol-
ogous MSCs in 5 patients with severe stroke showed this
treatment to be feasible and safe, with improved neuro-
logic recovery.17 Another study evaluated the long-term
safety and efficacy of intravenous transplantation of
MSCs in 85 patients with cerebral infarction. In this
case, the therapy was found to be safe and recovery
improved, which was correlated with serum levels of
stromal cell-derived factor 1 (SDF-1 alpha).18
There are currently 31 registered worldwide clinical
trials on stem cell therapy for cerebral infarct, using a
variety of cell types, with most of the studies focusing
on the later stages of stroke recovery (between 1 month
and 5 years).19
Thus, few studies to date have evaluated the possible
beneficial effect of MSC administration in the early stages
of stroke, and it would be useful to evaluate its efficacy in
stimulating brain plasticity in this phase. As mentioned
previously, our research group has developed preclinical
studies with positive results, both in terms of safety and
efficacy, in an animal model of cerebral ischemia using
MSCs from bone marrow and adipose tissue.15 For the
transition to clinical practice, we propose the use of
allogeneic MSCs from adipose tissue in acute cerebral
infarction, given that this type of MSC could have a signif-
icant scientific and health impact because they are easier
to obtain than from other sources such as bone marrow.
Regarding safety, prior studies have shown that the intra-
venous infusion of autologous MSCs is feasible and safe,
and results have suggested an improvement in neurologic
recovery in patients with severe stroke. The use of alloge-
neic stem cells could be an alternative because of the
demonstrated lack of HLA-class II expression in

E. D�ıEZ-TEJEDOR ET AL.2696
mesenchymal cells, which means no allergic reactions
neither than immunologic response nor rejection would
be expected. This therapy has not been associated with
cancer development; however, to our knowledge, no
studies are available on the safety of the intravenous
administration of allogeneic MSCs from adipose tissue
in patients within the first days after a stroke.
Hypothesis
The intravenous administration of allogeneic MSCs
from adipose tissue in patients with acute stroke is a
safe therapy that will result in the stimulation of neuro-
genesis, gliogenesis, oligodendrogenesis, synaptogenesis,
and angiogenesis in the injured area, promoting the repair
of the neurovascular unit and repairing cortical and
subcortical brain damage.
Therefore, the administration of MSCs in the acute
phase of stroke, along with the conventional treatment
of cerebral infarction, will significantly improve patient
recovery in the early stages of stroke by repairing
ischemic brain tissue.
Methods
Design
A Phase IIa, pilot, single-center, prospective, random-
ized, double-blind, placebo-controlled clinical trial.
Patients will be included sequentially, and a safety analysis
will be conducted after the inclusion of every 3 patients.
Patient Population: Inclusion and Exclusion Criteria
Patients presenting an acute ischemic stroke within
24 hours of onset.
Inclusion Criteria
(1) Male and female acute ischemic patients,
60-80 years of age, with symptoms of acute cere-
bral infarction less than 12 hours from stroke
onset. If the time of symptom onset is unknown,
this shall refer to the last time the patient was
observed as asymptomatic.
(2) Patients should have been treated within 2 weeks
from the onset of stroke symptoms.
(3) Patients with a measurable focal neurologic deficit
that persists to the time of treatment without
clinically meaningful improvement.
(4) A computed tomography (CT) and/or magnetic
resonance imaging (MRI) scan compatible with
the clinical diagnosis of acute ischemic stroke in
the region of the middle cerebral artery.
(5) A score on the National Institute of Health Stroke
Scale (NIHSS) of 8-20, with at least two of these
points in sections 5 and 6 (motor deficit) at the
time of inclusion.
(6) A prestroke score on the Modified Rankin Scale
(mRS) #1 (no symptoms at all or no significant
disability despite symptoms and able to perform
everyday tasks and activities).
(7) A negative pregnancy test for women of child-
bearing age.
(8) Signed informed consent (after a detailed explana-
tion of the nature and purpose of this study, the
patient or their guardian or legal representative
must give their consent to participate by signing
the informed consent document); or consent from
a relative or caregiver if the patient is unable to pro-
vide meaningful consent (eg, in cases of dysphasia,
confusion, or reduced level of consciousness).
Exclusion Criteria
(1) Comatose patients; patients with a score of 2 or
more on item 1a of the NIHSS related to the degree
of awareness.
(2) Evidence on neuroimaging (CT or MRI) of a brain
tumor, cerebral edema with midline shift and a
clinically significant compression of ventricles, cere-
bellar or brainstem infarction, and intraventricular,
intracerebral, or subarachnoid hemorrhage.
(3) Current drug or alcohol use or dependence that, in
the opinion of the site investigator, would interfere
with adherence to the study requirements.
(4) Active infectious disease, including human immu-
nodeficiency virus, hepatitis B, and hepatitis C.
(5) Pre-existing dementia.
(6) A health status, any clinical condition (eg, short
life expectancy, and coexisting disease) or other
characteristic that precludes appropriate diag-
nosis, treatment, or follow-up in the trial.
(7) Patients who are participating in another clinical
trial.
(8) Inability or unwillingness of the individual or
their legal guardian/representative to provide
written informed consent.
Randomization
Each patient will be sequentially assigned a number as
they enter the study. The patients will be assigned the
study drug according to a randomization schedule based
on the randomization plan. Randomization will be simple
rather than stratified. The study drug will be labeled with
the study number and a unique identification number.
The 2 treatments (allogeneic MSCs and placebo) will be
indistinguishable.
This studywill be double-blind and placebo-controlled.
To maintain the blinding during the course of the study,
the following procedures will be established: the placebo
and the study treatment (allogeneic MSCs) will be sup-
plied in identical vials, and the protocols will be designed
to ensure that the physician evaluating patient safety and

REPARATIVE THERAPY FOR ACUTE ISCHEMIC STROKE 2697
efficacy outcomes (clinical stroke scales: NIHSS, mRS, and
infarct volume), as well as the laboratory analysis, will not
have access to the randomization codes.
Treatment or Intervention
The experimental drug is a solution of MSCs from adi-
pose tissue. The manufacturing process is detailed in the
investigator’s brochure, which is available at the study
center and has been approved by the Spanish Agency of
Medicines and Health Products. In brief, it consists of
the release of the active ingredient composed of MSCs
obtained from the adipose tissue of the same donor
from whom the adipose tissue was previously obtained
for this study. Cells are maintained using the technology
of the cellular in vitro culture until the number of MSCs
is obtained that cover the administration of the product
to the patient, while meeting the required quality control
procedures according to good manufacturing practice
guidelines. The MSC solution is prepared for its final con-
ditioning and is transported to the study center for
administration to the patient.
Thus, once a patient is randomized, there are 3 steps
before the administration of the MSCs to the patient,
which takes approximately 7-10 days:
(1) Phase 1: unfrozen and in vitro maintenance of the
MSCs.
(2) Phase 2: preparation and conditioning of the final
product.
(3) Phase 3: transport of the drug under investigation
from the manufacturer’s laboratory to the study
center.
The patients assigned to the placebo armwill be given a
vehicle solution with the same appearance as the drug
under investigation. The drug will be administered in a
single intravenous dose within the first 2 weeks from
the onset of stroke symptoms. All patients will receive
conventional treatment for ischemic stroke according to
current clinical practice guidelines and pathways.
All study medications will be manufactured, tested, and
released according to current goodmanufacturing practice
guidelines. The study medications will be prepared in
identical vials containing either allogeneic MSCs or pla-
cebo solutions. Regarding the treatment dose, its adminis-
tration, and dispensing, included patients will receive an
intravenous infusion of the study medication (allogeneic
MSCs or placebo) within the first 2 weeks from stroke
onset. The dose will be 1 million units per kilo of weight,
administered at an infusion rate of 4-6 mL/minute. The
study medication must be discontinued if any of the
following conditions occur: a suspected anaphylactic reac-
tion, a severe adverse event, or withdrawal of consent by
either the patient or their representative.
All included patients will be managed according to cur-
rent guidelines20-22 for acute stroke management and the
stroke clinical pathway of the Stroke Center at La Paz
University Hospital.23 They will be admitted to the stroke
unit, and continuous noninvasive monitoring will be pro-
vided during the first days following the stroke until the
physician in charge evaluates the patient’s clinical stabil-
ity and approves a transfer to the neurology ward. This
approval will be independent from the inclusion of the
patient in the study.
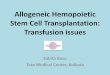
Study Schedule
The study will have a total duration of 24 months per
patient and will consist of 9 scheduled visits (Table 1,
Figure 1).
Primary Outcomes
The safety of MSCs from adipose tissue will be assessed
using the following parameters:
(1) Adverse events (AEs), reported spontaneously or
in response to prespecified questions at each study
visit. Serious AEs will be recorded at each visit
during the study period.
(2) Neurologic and systemic complications: deterio-
rating stroke, stroke recurrences, brain edema, sei-
zures, hemorrhagic transformation, respiratory
infections, urinary tract infections, deep venous
thrombosis, pulmonary embolism, and gastroin-
testinal hemorrhage will be recorded at each visit
during the study period.
(3) Tumor developments.
Secondary Outcomes
The efficacy of MSCs from adipose tissue will be
assessed using the following parameters:
(1) mRS, which will be measured on day 7 and at
3 months.
(2) NIHSS, which will be measured during all the
scheduled visits.
(3) Infarct size, which indicates the total volume of the
infarction, measured in neuroimaging (MRI) on
day 7 and at 3 months.
(4) Biochemical markers of brain repair (vascular
endothelial growth factor, brain-derived neurotro-
phic factor, and matrix metalloproteinases 9),
which will be measured at baseline, on day 7 and
at 3 months.
Data Management and Monitoring Committee
(1) Monitoring will be performed by a Clinical
Research Organization. Safety will be carefully
monitored during the trial. An independent data
monitoring committee will monitor the accumu-
lated safety data through periodic reviews of the
unblinded data to identify any safety issues.

Table 1. Flowchart
Flowchart Screening
V1 V2 V3 V4 V5 V6 V7 V8 V9
0 h 2 h 24 h Day 7 Month 3 Month 6 Month 12 Month 18 Month 24
Informed consent signature x
Inclusion and exclusion
criteria review
x
Past medical/surgical history x
Physical examination x x x x x x x x
Pregnancy test in women of
childbearing age
x
NIHSS x x x x x x x x x x
Modified Rankin Scale (prestroke) x x x x x x
Charlson Index x x x
Blood pressure x x x x
Heart rate x x x x
Body temperature x x x x
Oxygen saturation x x x x
Capillary blood glucose x x x x
Transcranial Doppler x
Neuroimaging (brain CT) x
Neuroimaging (brain MRI) x x x
Laboratory assessments
Hematology, coagulation
test, and biochemistry
x x x
Brain repair markers x x x
Recording of adverse events x x x x x x x x x
Concomitant drugs x x x x x x x x x
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
E. D�ıEZ-TEJEDOR ET AL.2698
(2) Collection and processing of safety data and re-
view by independent data monitoring commit-
tee: safety will be carefully monitored during
the trial. An independent data monitoring com-
mittee will monitor the accumulated safety data
through periodic reviews of the unblinded data
to identify any safety issues. The independent
data monitoring committee will provide recom-
mendations as to whether to continue the trial
based on the results of the safety analysis. The
independent committee will follow the re-
commendations listed in the ‘‘Guideline on
Data Monitoring Committees’’ of the European
Medicines Agency (EMEA) (Ref. Doc EMEA/
CHMP/EWP/5872/03).
Sample Size
This pilot trial will include 20 patients, distributed to
each treatment group in a proportion of 1:1. A formal pre-
determination of sample size cannot be calculated because
of the exploratory nature of this pilot study. This sample
size should allow us to obtain sufficient information for
the development of further studies (Phase III).
The estimated recruitment period is 2 years, as it is
feasible to include approximately 10 patients per year,
Figure 1. Schematic diagram(s) of the trial
design.

REPARATIVE THERAPY FOR ACUTE ISCHEMIC STROKE 2699
taking into account the inclusion and exclusion criteria
and the number of acute ischemic stroke admissions to
the stroke unit of the Neurology Department of La Paz
University Hospital (approximately 350 per year).
Statistical Analyses
The demographic and baseline characteristics will be
summarized for each treatment group to assess the
comparability of both groups. For this purpose, the
following variables will be considered: age, gender, race,
smoking and drinking habits, vascular risk factors (eg, hy-
pertension, dyslipidemia, diabetes mellitus, metabolic
syndrome, and heart disease), previous strokes, comorbid-
ity (Charlson Index), prior functional status (mRS), time
from stroke onset, and start of study treatment.
(1) Primary analysis: safety. The safety analysis will
be based on the reports of AEs, clinical and labora-
tory data, and vital signs. The incidence of serious
AEswill be provided, regardless of their classifica-
tion as AEs due to treatment, to their relationship
with the study drug, or to the deaths related to
them.
(2) Secondary analysis: efficacy. For continuous vari-
ables, the following information will be provided:
number of subjects, mean, standard deviation,
median, minimums, maximums, 25% and 75%
quartiles, and changes from baseline to end visit
values. For categorical variables, the frequency
distribution (absolute and relative) and 95% confi-
dence interval, if applicable, will be provided. An
exploratory analysis will be conducted by
comparing both treatment groups using Student
t test or the Mann–Whitney test, according to the
data distribution.
The ‘‘intention to treat’’ population will consist of the
patients for whom basal variables and at least 1 value of
a principal or secondary outcome variable will be avail-
able. If the patient does not attend the final visit, the
data will be replaced by the last available value (Last
Observation Carried Forward). The ‘‘per-protocol’’ popu-
lation will consist of the patients who have begun treat-
ment with the study drug and for whom major
violations of the protocol do not exist.
Study Organization and Funding
The study is investigator initiated, is promoted by the
Fundaci�on de Investigaci�on del Hospital Universitario La
Paz, and is funded by the Spanish Ministry of Health, So-
cial Policy and Equality. It has been approved by the La Paz
University Hospital Ethics Committee and by the Spanish
Agency of Medicines and Health Products. EudraCT:
2011-003551-18. The study is registered at http://www.
clinicaltrials.gov and identified by NCT01678534.
Recruitment is aimed to begin in May 2014.
Study Procedures:
(1) Screening and informed consent
Once the diagnosis of cerebral infarction has been
confirmed and it has been determined that the patient
fulfills the inclusion criteria and meets none of the exclu-
sion criteria, written informed consent will be obtained
from the patient or the patient’s representative before the
performance of any trial-specific procedure. A copy of the
signed informed consent will be given to the participants.
The original signed form will be retained at the study site.
(2) Data management
All data management will follow the principles of the
Spanish law Ley Org�anica de Protecci�on de Datos (LOPD
15/1999), ensuring the confidentiality of all personal data.
In compliance with European regulations/International
Conference of Harmonization Good Clinical Practice
(ICHGCP) Guidelines,24 the investigator and institution
are required to permit authorized representatives of the
company, of the regulatory agency(s), and the IEC/IRB
direct access to review the subject’s original medical re-
cords for verification of study-related procedures and data.
(3) Study schedule
The study will have a total duration of 24 months per
patient and will consist of 9 scheduled visits. The baseline
visit will take place during the first 24 hours of the stroke
and before the first administration of the study drug. The
second visit will take place 2 hours after the inclusion of
the patient in the study and will coincide with the
completion of intravenous treatment. Other visits will
be conducted at 24 hours, 7 days (or hospital discharge
if it occurs before day 7), 3 months, 6 months, 12 months,
18 months, and 24 months, according to the schedule
illustrated in the Table 1 and Figure 1. The efficacy end-
points will be evaluated by an investigator blinded to
the treatment received by the patient.
Discussion
Autologous MSCs have been successfully transplanted
into the brains of stroke patients with excellent tolerance
and no complications. The intravenous infusion of autol-
ogous MSCs has been shown to be feasible and safe and
has improved neurologic recovery in patients with se-
vere stroke. The safety of this therapy at 5 years post-
treatment has been reported. The use of allogeneic
MSCs could be an alternative therapy because it has
been demonstrated that they lack HLA-class II antigens,
and no allergic reactions other than an immunologic
response or rejection would be expected. In addition,
this therapy has not been associated with the develop-
ment of tumors.
To our knowledge, this is the first pilot, phase II, clinical
trial to investigate the safety and efficacy of intravenous

E. D�ıEZ-TEJEDOR ET AL.2700
administration of allogeneic MSCs from adipose tissue
within the first 2 weeks of stroke. In addition, its results
will help us to define the best criteria for a future phase
III study.
References
1. D�ıaz-Guzman J, Egido JA, Gabriel-S�anchez R, et al.Stroke and transient ischemic attack incidence rate inSpain: the IBERICTUS study. Cerebrovasc Dis 2012;34:272-281.
2. Guti�errez M, Merino JJ, de Leci~nana MA, et al. Cerebralprotection, brain repair, plasticity and cell therapy inischemic stroke. Cerebrovasc Dis 2009;27(Suppl1):177-186.
3. Locatelli F, Bersano A, Ballabio E, et al. Stem cell therapyin stroke. Cell Mol Life Sci 2009;66:757-772.
4. Stem Cell Therapies as an Emerging Paradigm in Stroke(STEPS): bridging basic and clinical science for cellularand neurogenic factor therapy in treating stroke. Stroke2009;40:510-515.
5. Savitz SI, Chopp M, Deans R, et al. Stem Cell Therapy asan Emerging Paradigm for Stroke (STEPS) II. Stroke 2011;42:825-829.
6. Kalladka D, Muir KW. Stem cell therapy in stroke:designing clinical trials. Neurochem Int 2011;59:367-370.
7. Ryan JM, Barry FP, Murphy JM, et al. Mesenchymal stemcells avoid allogeneic rejection. J Inflamm (Lond) 2005;2:8.
8. Guti�errez-Fern�andez M, Rodr�ıguez-Frutos B, Alvarez-Grech J, et al. Functional recovery after hematic adminis-tration of allogenic mesenchymal stem cells in acuteischemic stroke in rats. Neuroscience 2011;175:394-405.
9. Li Y, Chen J, Chen XG, et al. Human marrow stromal celltherapy for stroke in rat: neurotrophins and functionalrecovery. Neurology 2002;59:514-523.
10. van Velthoven CT, Kavelaars A, van Bel F, et al. Regener-ation of the ischemic brain by engineered stem cells: fuel-ling endogenous repair processes. Brain Res Rev 2009;61:1-13.
11. Leu S, Lin YC, Yuen CM, et al. Adipose-derived mesen-chymal stem cells markedly attenuate brain infarct sizeand improve neurological function in rats. J Transl Med2010;8:63.
12. Chen J, Li Y, Wang L, et al. Therapeutic benefit of in-travenous administration of bone marrow stromal
cells after cerebral ischemia in rats. Stroke 2001;32:1005-1011.
13. Li Y, Chopp M, Chen J, et al. Intrastriatal transplantationof bone marrow nonhematopoietic cells improves func-tional recovery after stroke in adult mice. J Cereb BloodFlow Metab 2000;20:1311-1319.
14. Li D, Fang Y, Wang P, et al. Autologous transplantation ofadipose-derived mesenchymal stem cells attenuatescerebral ischemia and reperfusion injury through sup-pressing apoptosis and inducible nitric oxide synthase.Int J Mol Med 2012;29:848-854.
15. Guti�errez-Fern�andez M, Rodr�ıguez-Frutos B, Ramos-Cejudo J, et al. Effects of intravenous administration ofallogenic bone marrow- and adipose tissue-derivedmesenchymal stem cells on functional recovery and brainrepair markers in experimental ischemic stroke. StemCell Res Ther 2013;4:11.
16. Su�arez-Monteagudo C, Hern�andez-Ram�ırez P, Alvarez-Gonz�alez L, et al. Autologous bone marrow stem cellneurotransplantation in stroke patients. An open study.Restor Neurol Neurosci 2009;27:151-161.
17. Bang OY, Lee JS, Lee PH, et al. Autologous mesenchymalstem cell transplantation in stroke patients. Ann Neurol2005;57:874-882.
18. Lee JS, Hong JM, Choi JY, et al. A long-term follow-upstudy of intravenous autologous mesenchymal stem celltransplantation in patients with ischemic stroke. StemCells 2010;28:1099-1106.
19. http://clinicaltrials.gov/.20. Adams HP, del Zoppo G, Alberts MJ, et al. Guidelines for
the early management of adults with ischemic stroke.Stroke 2007;38:1655-1711.
21. Egido JA, Alonso de Lecinana M, Martinez-Vila E,et al. Gu�ıa para el tratamiento del infarto cerebralagudo. In: D�ıez-Tejedor E, ed. Gu�ıa para el trata-miento y prevenci�on del ictus. Madrid: Prous Science2006:97-132.
22. European Stroke Organisation (ESO) Executive Commit-tee. ESOWriting Committee. Guidelines for managementof ischaemic stroke and transient ischaemic attack 2008.Cerebrovasc.Dis 2008;25:457-507.
23. Martinez-Sanchez P, Fuentes B, Medina-Baez J, et al.Development of an acute stroke care pathway in ahospital with stroke unit. Neurologia 2010;25:17-26.
24. ICH Tripartite Harmonised Guideline: Good ClinicalPractice: Consolidated Guideline (E6). 2010.