Embed Size (px)
Citation preview

Renal_2012 Due August 17, 2012
RENAL DISEASE PACKET Name: Birgit Humpert
PLEASE ANSWER ALL QUESTIONS IN YOUR OWN WORDS. LIST THE APPLICABLE REFERENCES AT THE END OF EACH SECTION.
A.) MEDICAL TERMINOLOGY
1. Fill in the blanks in the following table:
BODY PART RELATED ROOT WORD
PRIMARY FUNTION OF BODY PART
Example: Renal Pelvis pyel Collects urine produced by the kidney
Kidney nephr, ren Filtration of blood, removal of waste through urine, and several regulatory functions (fluid, blood pressure, pH, electrolytes).
Urine (urinary tract) -uria, urin Fluid produced by the kidneys. (Urinary tract is the system that produces, stores and excretes urine).
Ureter ureter Transports urine from renal pelvis to bladder.
bladder cyst, vesic Reservoir for urine.
Urethra ureth Transports urine to the outside of the body.
2. Break the following words up into their prefix, root and suffix and then provide the meaning of the word. Not all words will have all three parts.
Medical Term Prefix & Meaning
Root & Meaning Suffix & Meaning Meaning of Medical Term
Ex: Nephrotic - nephro - kidney tic – pertaining to Pertaining to the Kidney
Uremia ur/o - urine emia - blood condition
nitrogen-containing waste in the blood
Nephrologist nephr/o - kidney logist - specialist kidney specialist
Anuria an - not/without ur/o - urine inability to produce urine
- 1 -

Renal_2012 Due August 17, 2012
Nephrosis nephr/o - kidney osis - condition degenerative changes in the kidney
Glomerulo-nephritis
glomerul/o - glomerulus/glomeruli
nephr/o - kidney itis - inflammation
glomeruli in the kidney are inflammed
Nephrolithiasis nephr/o - kidney lith/o - stone iasis - condition presence of kidney stones
Cystorrhagia cyst/o - bladder rrhagia excessive bleeding of the bladder
Hemodialysis hem/o - blood dia - through lysis - freeing blood is filtered through membrane to remove waste
Cystectomy cyst/o - bladder ectomy - removeal
removal of the bladder
Polyuria poly - many ur/o large quantity of urine
- 2 -

Renal_2012 Due August 17, 2012
B.) NORMAL RENAL ANATOMY AND FUNCTION
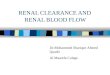
1. Label the parts of the kidney.
List your answers here
a. renal pyramid e. proximal/distal convoluted tubule
b. ureter f. collecting duct
c. renal pelvis g. loop of Henle
d. Bowman capsule with glomerulus
2. In your own words, discuss the mechanism of action for the following functions of the kidneys:
a. Blood filtration, excretion and regulation of body wastes.
Blood enters the kidney via the renal artery and the afferent arteriole brings it to the
glomerulus. 20 % of the plasma is filtered, 80 % leave the glomerulus unfiltered. The
blood enters the glomerulus under high pressure and is pressed through small openings
into the Bowman's capsule. Large proteins and blood cells stay behind. The ultrafiltrate
that is produced here then goes through the tubules. In the proximal convoluted tubule
water, glucose, and other substances are reabsorbed. In the loop of Henle sodium,
- 3 -
a.
b.
c.
e.
f.
d.
g.

Renal_2012 Due August 17, 2012
potassium, and chloride are reabsorbed. In the distal convoluted tubule more sodium is
reabsorbed in exchange for potassium. Acid also enter the filtrate which then goes to
the collecting tube. In the collecting tube more water can be reabsorbed before the urine
goes to the renal pelvis and then to the bladder where it is collected. Waste products
that are excreted into the urine either come from metabolic processes, like urea, uric
acid, and creatinine, or from ingestion like drugs and toxins.
b. Regulation of blood volume, blood pressure and electrolyte balance.
To be able to regulate blood volume the kidneys reabsorb water, but not much sodium
when the ultrafiltrate moves down the descending loop, and reabsorb sodium in the
ascending loop. This leads to a high concentration of sodium in the low part of the loop
which lays in the medulla. When the filtrate then goes down the collecting duct it
passes through the medulla again and via osmosis water can be reabsorbed here.
The ability of water to pass through the cell walls in the collecting duct is regulated by
vasopressin/antidiuretic hormone. When the pituitary gland produces more vasopressin
more water can be reabsorbed in the kidneys and the urine gets more concentrated.
When more water is reabsorbed in the kidney blood volume and blood pressure
increase. Vasopressin is released when pressure drops or when osmolality of the
extracellular fluid is increased.
Fluid and electrolyte balance are regulated by the renin-angiotensin/aldosterone system.
When hydrostatic pressure decreases the kidneys release renin. Renin converts
angiotensinogen from the liver to angiotensin I which is then converted to angiotensin
II under the influence of angiotensin-converting enzyme. Angiotensin II increases
aldosterone excretion from the adrenal cortex . Aldosterone influences the kidneys to
reabsorb sodium. If more sodium is reabsorbed water follows along and blood volume
and blood pressure rise.
Potassium levels are regulated by aldosterone. If aldosterone secretion is increased
more potassium is excreted.
Calcium and phosphorus levels also depend on regulation by the kidneys. When levels
of calcium in the blood are low the parathyroid gland releases parathyroid hormone.
- 4 -

Renal_2012 Due August 17, 2012
This triggers calcium reabsorption, phosphorus excretion, and vitamin D activation in
the kidney. Vitamin D increases calcium absoption in the intestines. Together with
release of calcium from the bones all this mechanisms raise blood calcium levels which
then lead to a negative feedback to the parathyroid gland.
c. Acid-base regulation of body fluids
Together with the lungs the kidneys are responsible for maintaining a constant pH.
Unlike the lungs the kidneys deal with fixed acids. They regulate bicarbonate
concentration, which is an important buffer in the blood. To do so hydrogen ions are
secreted and bicarbonate is also filtered in the glomeruli. They combine and form
carbonic acid which splits up into water and carbon dioxid. Carbon dioxid and water
react and produce bicarbonate and hydrogen which are reabsorbed. When acidosis
occurs the amount of secreted hydrogen is greater than the amount of filtered
bicarbonate and hydrogen is lost in the urine until pH of the blood is back to normal. If
alkalosis occurs less hydrogen is secreted than bicarbonate filtered out, and as a
consequence less bicarbonate can be reabsorbed.
d. Gluconeogenesis (occurs under specific condition)
Gluconeogenesis produces glucose from lactate, glycerol, and amino acids. The
necessary enzyme, glucose-6-phospatase, is only found in the liver and the kidneys. It
is thought that gluconeogenesis happens mostly in the liver and that the kidneys
produce glucose mostly under acidotic conditions and after long fasting. But there is
also evidence that the kidneys play a more significant role in glucose homeostasis, and
may release up to 20 - 40 % of the glucose produced in gluconeogenesis under normal
circumstances.
e. Note: Hormone production is another important function but is discussed in later sections.
Reference for this section:
Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy & Pathophysiology (2nd ed.). Belmont, CA: Wadsworth
- 5 -

Renal_2012 Due August 17, 2012
Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins
Freudenrich, C. How Your Kidneys Work. How Stuff works. Available from
http://science.howstuffworks.com/environmental/life/human-biology/kidney2.htm
Gerich, J.E., Meyer, C., Woerle, H.J., Stumvoll, M. (2001). Renal Gluconeogenesis. It's Important in Human Glucose Homeostasis. Diabetes Care. American Diabetes Association.doi: 10.2337/diacare.24.2.382 Diabetes Care February 2001 vol. 24 no. 2 382-391
- 6 -

Renal_2012 Due August 17, 2012
C.) RENAL DISEASES AND CONDITIONS
1. Define the following as they relate to renal function or disease.a. Azotemia
Azotemia is a condition where nitrogenous waste products, like urea and creatinine
build up in the blood. The cause of azotemia is insufficient filtration by the kidneys.
b. Oliguria
Urine excretion is reduced to less than 400 ml; below 400 ml the body can not
eliminate metabolic waste sufficiently.
c. Hyperparathyroid
Hyperparathyroidism occurs as a result of chronic kidney disease. Normally the
parathyroid gland excretes parathyroid hormone (PTH) into the blood if levels of
calcium are low. This triggers calcium reabsorption, phosphorus excretion, and vitamin
D activation in the kidney. Together with release of calcium from the bones all this
mechanisms raise blood calcium levels which lead to a negative feedback to the
parathyroid gland. In CKD this feedback loop does not work because the kidney does
not reabsorb calcium, can not active vitamin D, and can not excrete phosphorus as
normal. This triggers a constant release of parathyroid hormone which leads to
hyperplasia of the parathyroid gland.
c. Glomerular filtration rate (GFR), what does it measure and how is it used?
GFR estimates how well the glomeruli can filter the blood. The GFR is based on a
formula that consists of the creatinine level in the blood and factors like age, gender,
and weight. Different formulas are used, and some are not only based on creatinine
levels but take also serum albumin and blood urea nitrogen (BUN) into consideration.
A normal GFR ranges from 90 - 120 mL/min/1.73 m2.
Reference: Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth eGFR (2012). Lab Tests Online. Available from http://labtestsonline.org/understanding/analytes/gfr/tab/test
For each of the following kidney diseases and conditions:
7

Renal_2012 Due August 17, 2012
a. I am giving you the definition of the disease or condition
b. I am giving you the causes (etiologies)
c. You describe the physical changes specific to the disease process and progression (pathogenesis).
d. You explain how the disease impacts the patient’s nutritional status (in some cases there will be no impact.)
e. You tell me - is a modified diet recommended for this condition? If so what is the diet prescription?
2. Glomerulonephritisa. Definition: Condition resulting from inflammation of the capillaries of the glomeruli.
b. Etiology: Acute GN is most commonly triggered by an infectious process, often
streptococcal, but may also result from drug/toxin exposure, immunological
abnormalities, vascular or other systemic disease. Starts as an acute syndrome but if
underlying cause isn’t treated, may persist in the form of rapidly progressing
glomerulonephritis (RPGN). Chronic GN is often an autoimmune disease.
c. Pathogenesis: Inside the glomeruli antigen-antibody complex reactions become
trapped. This leads to the development of scarring, edema, and inflammation.
Edema due to fluid retention is often the first sign of acute glomerulonephritis. Oliguria
and anuria with blood in the urine may occur and temporary dialysis may become
necessary if acute kidney failure develops. Other symptoms are blood pressure increase
and swelling of the brain with headaches, blurred vision, seizure, and coma. Some
patients will only experience a general feeling of illness with nausea, some patients
with acute glomerulonephritis won't have symptoms at all.
With rapidly progressing glomerulonephritis the patient might experience fatigue,
weakness, fever, nausea, vomiting, abdominal and joint pain. Edema and oliguria are
common, high blood pressure is uncommon. Protein and blood are found in the urine
and in rapidly progressing glomerulonephritis urine samples also contain clumps of red
or white blood cells.
In chronic glomerulonephritis glomeruli are destroyed and as a result of renal tissue
loss, the kidney can't concentrate the urine. More urine is excreted and blood and
8

Renal_2012 Due August 17, 2012
protein is lost in the urine. Chronic glomerulonephritis often causes very few, mild
sypmptoms. Edema and high blood pressure may occur.
d. Nutritional Status: The general feeling of illness combined with nausea and vomiting
can lead to anorexia and inadequate intake. Inadequate intake combined with a higher
energy need due to inflammatory processes can lead to protein energy malnutrition.
Loss of protein in the urine can also contribute to this.
e. MNT: Protein restriction to 0.6 - 0.8 g/kg are usually prescribed unless the patient is
already malnourished, has cancer, an acute infection, or needs protein for growth. Half
of the protein should be of high biological value. It is important to provide enough
energy to prevent muscle catabolism that can lead to increased production of urea. 30 -
40 kcal/kg with 60 % carbohydrates and 30 % fat are usually prescribed. Protein should
be spared as much as possible so that it can be used for kidney regeneration.
With edema, high blood pressure, and oliguria fluid is restricted (500 - 700 ml) as well
as sodium (2 - 3g/d). Phosphorus and potassium are monitored and restricted as needed.
Reference: Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins Glomerulonephritis (2007) The Merck Manual Home Health Handbookfor Patients and Caregivers. Available at http://www.merckmanuals.com/home/kidney_and_urinary_tract_disorders/kidney_filtering_disorders/glomerulonephritis_nephritic_syndrome.html?qt=glomerulonephritis&alt=sh
3. Acute Renal Failurea. Definition: An abrupt decline in renal function with elevation of BUN and plasma
creatinine levels. Oliguria or anuria is common in the first phase, although urine
output may be normal or increased.
b. Etiology: Chronic risk factors include diabetes, heart failure, HTN, other renal disease
or damage, chronic liver disease, advancing age.
Causes may be:
prerenal (associated with alterations in the blood supply to the kidneys –
9

Renal_2012 Due August 17, 2012
hypovolemia, decreased cardiac output, obstruction of renal blood flow);
intrarenal or intrinsic (damage to the kidney nephrons – inflammatory, lack of blood flow within the renal tubules, toxic effect of medications or other substances); or
postrenal (obstruction to the urinary tract beyond the kidney – stones, UTI, strictures, tumor.
c. Pathogenesis: Reduced blood supply in prerenal causes of ARF reduces filtration
pressure. Prerenal conditions are reversible and don't cause permanent damage unless
the loss in blood supply leads to ischemia. Reabsorption of water and sodium is
increased, urine output is low.
Renal causes of acute renal failure can damage different structures in the kidney. If
glomeruli are involved then GFR is reduced and proteinuria occurs. Tubules can be
obstructed or damaged and this leads to a reduction in sodium reabsorption and high
sodium in the urine. Urine output varies. In the prodromal phase urine output is normal,
in the oliguric phase urine output is reduced to 50 - 400 ml, and in the postoliguric
phase urine output returns to normal.
Obstruction in the urinary tract in postrenal causes of ARF causes increased pressure in
the glomeruli and a reduction in GFR. Blood flow also decreases. Depending on
location of the obstruction urine output can be low or stop altogether.
Acute renal failure progresses quickly and nitrogenous waste products build up in the
blood. The patient experiences anorexia, nausea, and vomiting. ARF can cause
seizures, pulmonary edema, and coma with worsening azotemia and when fluid and
electrolyte imbalances, like hyperkalemia develop. Hyperphosphatemia, hypocalcemia,
and acidosis are also results of the impaired filtration function of the kidneys.
d. Nutritional Status: A catabolic state is very common in ARF and nitrogen losses, loss
of lean body mass, as well as anorexia, nausea, vomiting, and dialysis all can lead to a
quick worsening of the nutritional status of the patient. Underlying diseases also
contribute to the catabolic processes and protein-energy malnutriton.
e. MNT: Nutritional therapy depends on the underlying cause of ARF, the nutritonal
10

Renal_2012 Due August 17, 2012
status of the patient, and therapy (for example dialysis).
If the patient is not on dialysis protein is reduced to 0.6 g/kg, if dialysis is done protein
recommendation can go up to 1.4 g/kg. Both essential and nonessential amino acids
should be consumed. 30 -35 kcal/kg should be provided to maintain or improve
nutritional status. Depending on underlying cause energy recommendation can go up to
50 kcal/kg.
Fluid intake depends on renal function. It is usually calculated as 24 h-urine output plus
500 ml. Fluid status and electrolyte levels should be monitored. Sodium
recommendation is based on blood pressure and edema, and sodium can be reduced to
1 -2 g/d.
Due to reduced renal clearance trace mineral toxicity can develop. In general vitamins
and minerals according to the DRI are used. If the patient is on parenteral nutrition
standard guidelines for vitamins/minerals are followed.
If the patient can not take in food orally enteral or parenteral support is given, standard
formulas or formulas with lower electrolytes can be used if needed.
If the patient has to go on dialysis recommendations for dialysis apply (see below).
Reference: Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins Acute Renal Failure (2007). The Merck Manual for Health Care Professionals. Available from http://www.merckmanuals.com/professional/genitourinary_disorders/renal_failure/acute_renal_failure_arf.html?qt=acute%20renal%20failure&alt=sh
4. Chronic Renal Failure a. Definition: Progressive and irreversible loss of renal function. May take months to
years to develop.
b. Etiology: Diabetes is the leading cause, uncontrolled HTN is another common cause.
CRF often results from other renal conditions, or from unresolved ARF.
11

Renal_2012 Due August 17, 2012
c. Pathogenesis of AFR and glomerulonephritis should be described above. Either can
progress to CRF if not effectively treated. Continue with the pathogenesis from other
causes here:
Diabetes causes kidney disease by damaging the glomeruli. Thickening and sclerosis of
the glomeruli leads to an increase in permeability. The filtration function declines and
albumin is excreted into the urine. Over time more and more nephrons are damaged,
and the kidney can not clear enough solutes and the concentration of body fluids
increases.
Hypertension can lead to chronic kidney disease by damaging large or small blood
vessels in the kidneys. This damage can cause decrease in filtration function.
In CKD exocrine, endocrine, and metabolic function of the kidney decline in a slow,
irreversible process. Only when more than half of the kidney function is lost renal
failure becomes apparent. Kidney function is measured with GFR and when GFR is
below 60 mL/min/1.73 m2 for three month and/or more than 30 mg of albumin per
gram urinary creatinine is excreted it is defined as CKD according to the National
Kidney Disease Education Program.
There are several stages of CKD. In stage 1 kidney damage occurs but GFR is still
normal and the patient has no symptoms. In stage 2 kidney damage is accompanied by
mild decrease in GFR. In stage 3 GFR falls below 60 mL/min/1.73m2. Albumin is lost
in the urine. In this stage high blood pressure, uremia, anemia, and early bone disease
can occur. In stage 4 GFR falls below 30 mL/min/1.73m2. More protein is lost in the
urine, nitrogenous waste in the blood and blood pressure increase. In stage 5 GFR is
below 15 mL/min/1.73 m2 and kidney replacement therapy is necessary.
Decreased filtration capacity and damage of the kidney leads to various sypmptoms:
- Azotemia occurs, this is the buildup of nitrogenous waste products like blood urea
nitrogen, urea, and creatinine in the blood.
- Uremia describes the range of symptoms that occur as a result of the biochemical
changes, the symptoms range from anorexia, pruritus, lethargy, and fatigue to
12

Renal_2012 Due August 17, 2012
decreased mental alertness and even coma.
- Metabolic acidosis occurs because hydrogen ions can not be excreted.
- Another result of decreased kidney function is hyperkalemia. Potassium can not be
excreted and blood levels rise.
- Secondary hyperparathyroidism is another consequence of CKD. Because of high
phosporus levels parathyroid hormone secretion is constantly stimulated which results
in hyperplasia of the thyroid and secondary hyperparathyroidism.
- Because of the altered vitamin D, calcium, and phosphorus metabolism it comes to
renal bone disease.
- Hypertension occurs when GFR declines. It comes to sodium retention, edema, and
hypertension.
- The kidney does not produce erythropoietin which normally stimulates red blood cell
production. It comes to microcytic anemia and iron deficiency.
d. Nutritional Status: In the early stages of CKD the nutritional status is determined by the
underlying disease. Any recommendations for protein restriction must take catabolic
processes and underlying protein-energy malnutrition into consideration.
In patients with advanced chronic kidney disease and those on dialysis malnutrition is
common. Anorexia, nausea, vomiting, medications, changes in taste, dietary
restrictions, and other factors can lead to decreased intake. Increased catabolism with
protein loss, inflammatory processes, losses through dialysis and other factors lead to
increased needs.
e. MNT: MNT depends on the stage of the disease and the treatment.
In stage 1 and 2 nutrition therapy focuses on the underlying disease. Good blood
glucose control in diabetics and reduction of blood pressure can slow down the
progression of the disease. Control of blood lipids is also important to control
cardiovascular disease processes. Vitamin D, calcium, and phosphorus need to be
monitored because changes in mineral metabolism, secondary hyperparathyroidism,
and renal bone disease can start as early as stage 2.
13

Renal_2012 Due August 17, 2012
In stage 3 and stage 4 it is important to provide enough energy to avoid malnutrition.
Control of blood glucose, blood pressure, and blood lipids is still important. With
decreasing GFR (25 mL/min/1.73 m2) patients are usually put on a low-protein diet
with 0.6 - 0.75 g/kg protein. Low protein diets can control uremia and slow down the
progression of the disease but maintaining low protein intake while at the same time
providing enough energy and protein to avoid malnutrition is a difficult balancing act.
At least half the protein should come from protein sources with high biological value.
For patients younger than 60 years 35 kcal/kg is recommended. For patients older than
60 years the recommendation is 30 - 35 kcal/kg. Sodium restrictions vary from 1 - 3
g/d to no added salt depending on blood pressure and edema. Fluid is usually not
restricted. If potassium levels are high potassium is restricted. Phosphorus is limited to
800 - 1000 mg/d or 10 -12 mg/g protein to maintain phosphorus and parathyroid
hormone levels in the normal range. Calcium and other vitamins and minerals are
usually recommended according to the DRI before dialysis. Vitamin D can be given to
control parathyroid hormone. Iron and zinc are given according to individual needs.
Reference: Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins
5. End-stage Renal Disease (will discuss diet prescriptions in Nutrition Prescription section, can leave it out here.)a. Definition: Final stage of chronic, irreversible kidney failure. Less than 10% of renal
function remains. Treatment with dialysis or transplantation is required.
b. Etiology: May be last stage of chronic disease or resulting from infection or acute
disease. Previous sections should discuss etiology.
c. Pathogenesis: End-stage renal disease is stage 5 of chronic kidney disease wich GFR
below 15 mL/min/1.73 m2. Severe symptoms of uremia occur with azotemia, renal
bone disease, electrolyte imbalances, hypertension, edema, and oliguria/anuria.
14

Renal_2012 Due August 17, 2012
At this point replacement therapy becomes necessary and patients will either go on
dialysis or receive a kidney transplant.
d. Nutritional Status: The patient might experience nausea, vomiting, anorexia, and
fatigue which will all make adequate food intake difficult.
Patients on dialysis have additional factors that can contribute to protein-energy
malnutrition than discussed above for chronic kidney disease. They lose protein,
glucose, and vitamins through their dialysis treatment and they have increase needs due
to inflammatory processes.
Reference: Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins
6. Polycystic Kidney Diseasea. Definition: Loss of kidney function due to the formation of multiple fluid-filled cysts in
the kidneys.
b. Etiology: This is most commonly a genetic disease. Autosomal recessive PCK (rare)
occurs in fetuses and infants, half of whom die within a few days of birth, 25% live to
their 10th year. Autosomal dominant PCK (90% of cases) is also genetic but generally
doesn’t manifest until adulthood; symptoms usually start between ages 30 and 50.
A third type is acquired cystic kidney disease (ACKD) most typically occurs in patients
with kidney failure from other causes who have been on long term dialysis.
c. Pathogenesis: The gen mutations in autosomal dominant PCK causes tubules to dilate
and fill with filtrate. With progressing disease the tubules are transformed to cysts.
Bleeding into the cysts can occur and lead to hematuria. Kidney stones can sometimes
develop and patients have an increased risk for pyelonephritis.
Most patients with autosomal dominant PCK have no symptoms while the disease
develops and some remain without symptoms and are never diagnosed.
Symptoms are caused by the enlargement of the kidneys from the cysts and from
15

Renal_2012 Due August 17, 2012
inflammatory processes. They include pain in the side, lower back, and abdomen.
Stones and hemorrhaging can cause acute pain. Hematuria and hypertension occur in
half of the patients, proteinuria is less common. Erythropoietin production is usually
intact and anemia is rare. 35 - 45 % of patients eventually develop renal failure.
Vasopressin/ADH is constantly working and stimulating the production of cyclic
adenosine monophosphate which also contributes to the disease progression.
Most patients also have cysts in the liver, which usually don't interfere with liver
function and only cause symptoms if they become enlarged or infected.. Some have
cysts in the pancreas and the intestines, as well as diverticula and hernias. Some
patients also have valvular heart disorders, and aneurisms in the aorta, the coronary
arteries, or the brain.
Autosomal recessive PKD effects the kidneys, liver, spleen and pancreas; children born
with this disease have high blood pressure, polyuria, urinary tract infections, unusual
facial features, low blood cell count, varicose veins, and hemorrhoids.
d. Nutritional Status: As long as patients with ADPKD remain asymptomatic their
nutritional status is not effected. When they develop symptoms of kidney disease they
can experience anorexia, nausea, and vomiting and this can lead to protein-energy
malnutrition.
Children with ARPKD have failure to thrive and remain small for their age.
e. MNT: Nutritional therapy can support the treatment of high blood pressure with a low
sodium diet, for example the DASH diet.
The diet is modified according to the symptoms of renal disease. Protein is restricted if
there is extensive proteinuria. If renal replacement therapy is needed recommendations
for either dialysis or kidney transplantation should be followed. Food high in
antioxidants and foods with anti-inflammatory effects are beneficial.
For children with PKD adequate nutrition with enough energy and protein for growth is
important.
16

Renal_2012 Due August 17, 2012
Reference: Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins Autosomal Dominant Polycystic Kidney Disease (2009). The Merck Manual for Health Care Professionals. Available from http://www.merckmanuals.com/professional/genitourinary_disorders/cystic_kidney_disease/autosomal_dominant_polycystic_kidney_disease_adpkd.html?qt=polycystic%20kidney%20disease&alt=sh
7. Renal tubular acidosisa. Definition: Metabolic acidosis develops because kidneys don’t excrete excess acid into
the urine and/or are unable to retain adequate bicarbonate to buffer the blood.
b. Etiology: May be caused by drug or heavy metal toxicity, by autoimmune disorders,
diabetes, or obstruction. Types 1 and 2 may also be hereditary.
c. Pathogenesis: In type 1 hydrogen ion secretion is decreased which leads to systemic
acidosis and a low urine pH. Potassium levels in the blood are low and calcium
secretion is increased while citrate excretion is decreased. This type is rare.
In type 2 bicarbonate resorption is decreased. This leads to alkalosis and high urine pH.
This type is very rare and is often accompanied by excretion of glucose, uric acid,
phosphate, protein, potassium, calcium, and other substances in the urine due to a
general dysfunction of the tubules.
Type 4 is most common. There is either not enough aldosterone or tubules are
unresponsive to aldosterone. The result is reduced potassium excretion, hyperkalemia,
reduced acid secretion, and metabolic acidosis.
Renal tubular acidosis can be asymptomatic. Type 1 and 2 can impact the bones and
lead to bone pain, osteomalacia and rickets.
Electrolyte imbalance, especially hypokalemia can be severe, and cause muscle
weakness, paralysis, and arrhythmias.
d. Nutritional Status: Except for the electrolyte balances there are no changes in
nutritional status.
e. MNT: Nutrition therapy can support the correction of pH and electrolyte imbalances,
17

Renal_2012 Due August 17, 2012
although administration of electrolytes is usually a medical not a dietary treatment.
Patients may be treated depending on imbalances with alkaline agents, potassium if
needed, vitamin D, and calcium supplements.
In type 4 dietary potassium is restricted to help lower potassium levels in the blood.
Reference: Renal Tubular Acidosis (2009). The Merck Manual for Health Care Professionals. Available fromhttp://www.merckmanuals.com/professional/genitourinary_disorders/renal_transport_abnormalities/renal_tubular_acidosis_rta.html?qt=renal%20tubular%20acidosis&alt=sh
18

Renal_2012 Due August 17, 2012
D.) NUTRITION RELATED TOPICS
1. Describe the process of hemodialysis and how it works. How does CAPD differ from hemodialysis?In hemodialysis a patients blood is pumped through a dialyzer with a selective
semipermeable membrane that allows osmosis, ultrafiltration, and diffusion into the
dialysate that is pumped in the opposite direction on the other side of the membrane. The
filtered blood is then returned into the patients blood vessels. There is a concentration
gradient between blood and the dialysate which leads to the removal of urea nitrogen,
creatinine, and other substances. The electrolyte concentration is similar to normal blood
which leads to normalization of fluid and electrolyte balance. To access the patients body
there is either a arteriovenous fistula or an arteriovenous graft created. For emergency
and/or temporary dialysis a catheter into a central vein is used. Hemodialysis is usually
done three times per week for three to five hours in a dialysis center. It is also possible to
do it at home if trained support is available.
CAPD is continuous ambulatory peritoneal dialysis. In this form of renal replacement
therapy the patients peritoneum is used as the semipermeable membrane. Through a
catheter into the peritoneum dialysate (two to three liter) flows into the peritoneal cavity. It
stays there for four to six hours during the day, and eight to twelve hours at night, is then
drained again, and replaced with new dialysate. The blood vessels in the peritoneum deliver
the blood that is filtered. Because less blood then in hemodialysis is filtered in a given time
the process takes longer, but is also less stressful for the body. The amount of fluid and
solutes that are removed depends on the dwell time of the dialysate in the body, the number
of exchanges per day, and the dextrose concentration of the dialysate. CAPD is more
flexible and comfortable for the patient because it can be done at home but it also requires
more involvement from the patient.
2. What is “dry” weight?Dry weight is the weight the patient has without accumulated fluids. When patients go on
dialysis they produce little or no urine. That means that in between dialysis treatment fluids
accumulate in their body. Ultrafiltration volume and rate are set so that the patient has
19

Renal_2012 Due August 17, 2012
achieved his dry weight at the end of the dialysis. It is the lowest weight that can be
achieved without experiencing hypotension and other symptoms. There is no standard
measure to determine dry weight and it is usually determined clinically by 'trial and error'.
It is important to achieve the lowest weight possible to avoid fluid overload and high blood
pressure in between dialysis treatments. Dry weight can change when the patients lean
body weight changes due to changes of nutritional status over time, and he gains or loses
weight. This can lead to overestimation or underestimation of dry weight. Several methods
to measure dry weight with biochemical markers or bioimpedance analysis are proposed
but non has proven to be a the gold standard to determine dry weight.
3. Why would a dialysis patient be prescribed a daily water-soluble vitamin supplement instead of a regular multivitamin? A multivitamin contains vitamins that renal patients don't need or can not metabolize.
Vitamin A can build up in the body because there is more carrier protein, it is not
catabolized in the kidney, and not removed by dialysis. Vitamin E can also built up and
become toxic. Inactive vitamin D in a multivitamin can not be converted by the kidneys
into calcitriol, the active form, and is useless for the body. Vitamin K is generally not
needed unless production in the intestines is not functioning. Supplementation with vitamin
K might be contraindicated because patients on dialysis get anticoagulants to avoid blood
clotting during dialysis. Multivitamin preparations might also contain minerals and
electrolytes that are contraindicated. Special renal vitamin formulas are available that
contain B vitamins, folic acid, and vitamin C. Iron, zinc, and active vitamin D are given on
an individual basis.
4. Discuss the causes of anemia in chronic renal failure. Are iron supplements an effective treatment? Why or why not?Many patients with kidney disease have anemia because the kidneys don’t produce
sufficient amounts of erythropoietin, the hormone that stimulates the production of red
blood cells. Another cause for anemia are blood losses in hemodialysis treatment due to
blood testing, losses in tubing/dialyzer, gastrointestinal bleeding, and leaking if there is a
vascular access. Patients are treated with rHuEPO ( recombinant human epoetin alfa). EPO
works in the same way erythropoietin does, but it can only be effective if adequate iron is
20

Renal_2012 Due August 17, 2012
available. Therefor most dialysis patients are supplemented with iron. Oral iron
supplementation is often not sufficient to maintain iron levels in hemodialysis, and most
often IV iron is used. In peritoneal dialysis there is less blood loss from the procedure and
oral iron is often sufficient.
Oral iron supplementation can lead to stomach upset, nausea, and vomiting. This is
especially problematic in already anorexic renal patients.
5. How would a low serum albumin impact your interpretation of calcium labs and why?A low albumin level could lead to underestimation of the calcium status because about half
of the calcium in the blood is bound to albumin. If albumin levels are low this would
impact calcium levels. Instead of measuring total calcium it is better to test for ionized
calcium (not bound to a carrier).
6. Describe the influence of dietary oxalates on urinary oxalates. Give examples of foods with high bioavailability of oxalate that may increase urinary oxalate excretion. Dietary oxalate has only a limited influence on urinary oxalate and dietary oxalate is not a
major risk factor for the formation of calcium oxalate kidney stones. Some foods are high
in oxalate but bioavailability is low. Food with high oxalate should be limited or avoided
by patients who tend to develop calcium oxalate kidney stones. Examples for foods high in
oxalate are beets, chocolate, cola/coffee/tea, rhubarb, nuts, soy/soy products, wheat bran,
and spinach.
Reference for this section:
Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth
Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins
Jaeger, J.Q., Mehta, R.L., (1999). Assessment of Dry Weight in Hemodialysis. Journal of the American Society of Nephrology. JASN February 1, 1999 vol. 10 no. 2 392-403. Available from http://jasn.asnjournals.org/content/10/2/392.full
Calcium (2012). Lab Tests Online.
21

Renal_2012 Due August 17, 2012
Available from http://labtestsonline.org/understanding/analytes/calcium/tab/test
Hemodialysis (2007). The Merck Manual for Health Care Professionals. Available from http://www.merckmanuals.com/professional/genitourinary_disorders/renal_replacement_therapy/hemodialysis.html
Peritoneal Dialysis (2007). The Merck Manual for Health Care Professionals. Available from http://www.merckmanuals.com/professional/genitourinary_disorders/renal_replacement_therapy/peritoneal_dialysis.html
Vitamins and Supplements for ESRD Patients (2005). American Association of Kidney Patients. Available from http://www.aakp.org/aakp-library/Vitamins-&Supplements/
22

Renal_2012 Due August 17, 2012
E.) NUTRITION PRESCRIPTIONS
1. For each of the following treatments, list the nutrient recommendations in the chart. Then answer the related questions below in your own words.
Calories Protein Fluid Sodium Potas-sium
Phos-phorous
Calcium
Impaired renal function(non-dialyzed)
30 -35 kcal/kg for > 60 yrs35 kcal/kg for < 60 yrs
0.6 - 0.75 g/kg
normally not limited
1 -3 g/d to no added salt
only restricted if serum levels are high
800 - 1000 mg/d, 10 -12 mg/g protein
DRI, serum levels should be maintained in normal range
Hemo-dialysis
30 -35
kcal/kg
for > 60
yrs
35 kcal/kg for < 60 yrs
1.2 g/kg or more
output + 1 l
2 g/d 2000 - 3000 mg, adjusted to serum levels
800 - 1000 mg/d, 10 -12 mg/g protein
< 2 g, including binder
(CAPD) 30 -35
kcal/kg
for > 60
yrs
35 kcal/kg for < 60 yrsincluding kcal from dialysate
1.2 -1.3 g/kg or more
adjusted to maintain balance
2 g/d adjusted to maintain fluid balance
3000 - 4000 mg, adjusted to serum levels
800 - 1000 mg/d, 10 -12 mg/g protein
< 2 g, including binder
Transplant 30 -35 kcal/kg or more depending on complica
1.3 - 1.5 g/kg in the acute phase post surgery,
no restrictions if graft works
2 - 4 g/d 2 -4 g if hyperkalemia post surgery, no restrictio
1200 - 1500 mg, supplements needed
1200 - 1500 mg
23

Renal_2012 Due August 17, 2012
tions, in the chronic phase energy is adjusted to maintain desirable weight
later 1 g/kg
ns later if no hyperkalemia
2. Give the rational for the protein restriction in impaired renal function. What are the hazards vs. benefits of this practice? What would you monitor to determine the adequacy of protein intake in these patients?When the kidney function is impaired the urea that is produced when protein is metabolized
can not be removed, builds up in the body and leads to uremia and azotemia. Protein
restriction in CKD can help with the symptoms of uremia, slow down the progression of the
disease, and delay the need for renal replacement therapy. But following a protein
restriction while at the same time meeting the additional needs and providing adequate
nutrition for often anorexic patients is difficult.
There are different possibilities to monitore adequate protein intake. Serum album is useful
to determine visceral protein status. But acute illness, metabolic stress, inflammation, and
hydration status influence serum albumin levels and with a half-life of 17 -21 days it does
not show short-term changes. Prealbumin has a shorter half-life but it is also effected by
infection and inflammation.
3. Why is it recommended for these patients to have at least 50% of their protein from sources that have high biological value (HBV)?50 % of protein from sources with high biological value is recommended to make sure that
all essential amino acids are provided. If all essential amino acids are provided and enough
other amino acids to built non-essential amino acids the nitrogen balance can be kept
neutral and protein stores can be maintained or even improved.
4. Why are CAPD patients allowed more sodium, potassium and fluid than HD patients?CAPD diet allows more fluid, sodium, and potassium because it is removed daily and not
only three times per week as in hemodialysis. Fluid and sodium recommendations are
24

Renal_2012 Due August 17, 2012
usually individualized based on the ultrafiltrate that is used. If the ultrafiltrate contains more
glucose it can remove more fluids, but also cause more complications.
5. When might CAPD patients need more protein than HD patients? Explain why.CAPD patients need more protein than HD patients when they have peritonits
(inflammation of the peritoneum). Even if peritonitis is mild protein losses can increase by
50 - 100% and remain high for some time.
6. Why is fluid restricted in most hemodialysis patients? Make 4 suggestions to help patients control their fluid intake.Fluid is restricted to keep fluid retention in between dialysis treatments to a minimum.
Patients should not gain more than 5 % between treatments. If fluid gains are high this can
lead to shortness of breath, hypertension, edema, congestive heart failure as well as sudden
blood volume changes and hypotension during dialysis.
Fluid intake can be controlled by limiting salt intake. Patients should avoid processed
meats, soups, and other sodium-rich foods. Beverages should be in small glasses. Chewing
gum, sucking on sour candy, brushing teeth often, and using lip balm can help. Sucking on
ice chips or eating frozen fruits will help to keep the mouth moist for a longer periode (ice
must be counted as fluid).
7. Why is potassium a critical restriction in kidney failure? If patients are oliguric or anuric they are at greater risk for hyperkalemia. Hyperkalemia
can lead to arrhythmias that can be fatal.
8. List 6 commonly consumed foods or beverages that are high in potassium and suggest alternatives that would be acceptable and economical substitutions in menu planning.
HIGH POTASSIUM FOOD LOWER POTASSIUM ALTERNATIVE
banana blueberries
orange apple
black beans corn
brokkoli kale
milk soy milk
potatoes rice
25

Renal_2012 Due August 17, 2012
9. List 3 potential problems resulting from an excessive sodium intake in a patient with kidney failure. Make 4 suggestions to help patients control their sodium and salt intake.
Excessive sodium intake can lead to increased fluid retention, edema, and high blood
pressure.
Instead of table salt patients can use other flavorings like pepper, garlic, curry, herbs, lemon
juice, or salt-free seasoning blends.
Patients should avoid store-bought soups, sauces, and dressings and make their own with
other spices.
Patients should avoid salty snack foods like crackers and pretzels and find unsalted
alternatives.
Instead of processed meat products like ham, bacon, and deli meat patients can eat fresh
meat with salt-free seasonings.
10.
The balance between serum levels of calcium and phosphorus is difficult to maintain in patients with kidney failure, sometimes resulting in a condition called renal osteodystrophy.
Discuss the following related to this balance: a. Give at least 3 reasons that serum calcium levels drop with progressive kidney disease.
Calcium levels are low because the kidney is unable to reabsorb calcium even though
PTH levels are high due to high phosphate levels. The kidney can not produce the
active form of vitamin D, calcitriol, so that absorption in the intestines is decreased.
Dietary restrictions that effect calcium rich foods like dairy (high in phosphorus,
potassium, protein), almonds (high in potassium and phosphorus), beans (high in
phosphorus and potassium) can also contribute to low calcium levels.
b. How does kidney failure impact the regulation of calcium-phosphate product (also known as calcium-phosphate ratio)? How might these changes lead to osteomalcia? How might they lead to tissue calcification and why is this a critical issue?Due to normal or low calcium levels and high phosphorus levels the calcium-
phosphate ratio increases. This in an independent risk factor for complications of renal
diesease. If the calcium-phosphate ratio is higher than 72 mg2/dL2 patients have an 34
26

Renal_2012 Due August 17, 2012
% increased risk of death.
Different factors lead to inadequate mineralization of bone tissue in renal disease. High
levels of hyperthyroid hormone stimulate bone resorption which leads to osteomalacia.
The kidneys' inability to convert vitamin D, decrease in absorption, and decreased
intake all contribute to osteomalacia. Free calcium in the body binds with excessive
phophate, accumulates in soft tissue, and leads to soft tissue calcification. This is
critical because it raises the cardiovascular risk for renal patient which is already very
high.
c. List 5 foods that have the highest levels of phosphorus. Why are phosphate binders used? What are their nutrition related side effects?Dried beans, chocolate, beer, dark colas, and dairy products are some foods high in
phosphorus.
Phosphate binders are used to reduce absorption of phosphorus in the intestines when
dietary restriction alone is not enough. Phosphate binders are often calcium based and
hypercalcemia can be a side effect. Phosphate binders need to be considered when
assessing calcium intake and overall calcium intake from food, supplements, and
phosphate binders should not be more than 2 g in dialysis patients.
d. What are the diet modifications suggested for renal osteodystrophy?To prevent or treat renal osteodystrophy the diet needs to be modified to normalize
phosphorus and calcium levels. This can be achieved by restricting phosphorus intake
and/or using phosphate binders. An increase in calcium levels can be achieved by
adequate dietary calcium intake and by supplementing active vitamin D, to make sure
calcium can be absorbed.
e. Would you suggest increasing milk intake to treat low serum calcium levels in a renal patient? Why or why not?Milk and dairy products in high amounts are not recommended to increase calcium
levels because they contain high levels of phosphorus and also potassium.
f. What is calcitriol and why is it often supplemented in kidney failure. Why must the response to calcitriol be carefully monitored?
27

Renal_2012 Due August 17, 2012
Calcitriol is the active form of vitamin D. It is supplemented because the kidneys can
not longer convert inactive vitamin D in the active form. Active vitamin D is needed to
increase calcium absorption, and maintain healthy calcium levels. It also increases
bone resorption, increases reabsorption of calcium in the kidney, and decreases PTH
production. Calcitriol can have side effects like anorexia, nausea, weight loss,
abdominal cramping, headache, and fatigue. These could contribute to malnutrition in
renal patients. It can also lead to increased phosphate deposits in arteries, lungs, and
other soft tissue.
11
.
Your patient is starting hemodialysis and has a nutrition prescription of: 35 kcal/kg, 1.2 g protein/kg, 2 g K, 1 g phosphorus, 2 g Na, 1,000 mL fluid + urine output per day; decrease saturated fat and cholesterol intake. She has approximately 200 ml urine output per day. Use a weight of 75 kg for the calculations.
Consider her typical intake, plan a sample menu to meet her nutrition prescription. Do a nutrition analysis to show that your menu meets the recommendations.
28

Renal_2012 Due August 17, 2012
Nutrient Analysis: Calories: 2450 kcal, Protein: 83 g, Potassium: 2025 mg, Sodium: 1812 mg , Phosphorus: 1047 mg, Fluid: 1200 ml, Saturated fat: 15 g (= 6.4% total kcal), Cholesterol: 129 g.
References for this section:
Nelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &Pathophysiology (2nd ed.). Belmont, CA: Wadsworth
Escott-Stump, S. (2011). Nutrition and Diagnostic Related Care (7th ed.). Lippincott Williams & Wilkins
29
Typical Intake Sample Menu RecommendationBreakfast: Cold cereal (¾ c unsweetened), 2% milk (½c)
1/2 cup cottage cheese1/2 cup blueberries
Bread (2 slices) or fried potatoes (1 med potato)
2 slices bread, low sodium
1 fried egg (occasionally) 1 tbsp butter
Lunch: Bologna sandwich (2 slices white bread, 2 slices bologna, mustard)
Salad with 1 cup lettuce, 2 oz. chicken breast, 2 tbsp. olive oil, vinegar,1/8 teasp. salt, 1/2 cup grated carrots and 1/2 cup bell pepper, 1 roll
Potato chips (1 oz) 1 oz corn chips
1 can Coke
Dinner: Chopped meat (3 oz beef) 1 cup rice, 2 oz salmon, 1 cup green beans, 2
tbsp. canola oil, 1/8 teasp. saltFried potatoes (1½ medium)
HS Snack: Crackers (6 saltines) and peanut butter (2 tbsp)
several snacks throughout the day- 1 cup appelsauce with 2 graham crackers- 1 cup canned pears (without liquid) with 2 rice cakes- 8 oz Nepro Berry Shake - 32 oz of water fluid throughout the day (including 1 cup coffee if patient wants that)

Renal_2012 Due August 17, 2012
McCarron, D.A. (2005) Protecting Calcium and Phosphate Balance in Chronic Renal Disease. Journal of the American Society of Nephrology. doi: 10.1681/ASN.2005060661 JASN November 1, 2005 vol. 16 no. 11 suppl 2 S93-S94
MyPlate Food Tracker. Available from
https://www.choosemyplate.gov/SuperTracker/default.aspx
30