Embed Size (px)
Citation preview

Department of Medicine
Renal Disease in Asians
Division of Nephrology
6th Asian Health SymposiumOctober 7, 2017
San Francisco, CA
Chi-yuan Hsu, MD, MScProfessor and Chief
UCSF Division of Nephrology

DisclosuresNo relevant disclosures
– author and peer reviewer: UpToDate– Medical advisory board member: Satellite
Healthcare– Consultant: Merck, AstraZeneca/Ice Miller– donation of device for research: Microlife,
Teco/Scanostics, Nova Biomedical

OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach

The kidneys maintain stable internal milieu for the body


Glomerular filtration rate (GFR)• Considered single best index of kidney
function • Usually estimated in clinical practice from
serum Cr e.g. MDRD equation GFR (ml/min/1.73m2)
= 175*(Cr)-1.154*(age)-0.203[*0.742 if female] [*1.212 if black]• Correlates with complications with kidney
disease e.g. metabolic derangement, retention of salt, need for dialysis

• Chronic kidney disease (CKD)
• End-stage renal disease (ESRD) = kidney failure severe enough to be treated with dialysis or kidney transplant

• Chronic kidney disease (CKD)
The critical importance of proteinuria, or albuminuria as a sign of kidney damage

Peterson Ann Intern Med 1995

Beyond Cr: proteinuria quantification
• Beyond dipstick urinalysis spot urine protein (or albumin) to Cr ratio
• A random urine protein (or albumin)/Cr ratio approximates gm of protein (or albumin) excreted per 24-hours (e.g. 300 mg/dl / 100 mg/dl ≈ 3 grams per day)
• This is because many people make (and excrete in the urine) ~ 1 gm of Cr per day
• So per 1 gm of Cr is per 24-hr (easier than 24-hour urine collections)

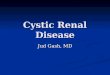
Why does proteinuria predict progression?
A. Reflects intra-glomerular hypertension which is deleterious

Glomerular filtration, intra-glomerular pressure and
proteinuria
Afferent arteriole Efferent arteriole
SNGFR = LPS (∆P - ∆Π)

Why does proteinuria predict progression?
A. Reflects intra-glomerular hypertension which is deleterious
B. Filtered protein itself is nephrotoxic (contains complement cascade proteins, transferrin etc.)

Zandi-Nejad KI 2004

OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach

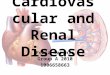
Asians > white ESRD incidence
US Renal Data System 2016 Annual Data Report

International comparison

US Renal Data System 2016 Annual Data Report


Baseline characteristics White Asian Black(n=221,686) (n=17,793) (n=59,689)
Age (yr) 39 ±14 36 ±12* 35 ±12*
Female 53% 54%* 58%*
BP (mmHg) 129/ 76 123/75* 131/78*
DM 1.9% 1.9% 2.7%*
BMI (kg/m2) 24±4 22±3* 26±5*
Cr (mg/dl) 0.95±0.24 0.89±0.23* 0.97±0.25*
* p< 0.05

White Asian BlackProteinuria Negative 96.2% 96.8% 94.8%Trace 2.1% 1.5% 2.9%1-2 + 1.6% 1.4% 2.0%3-4+ 0.2% 0.2% 0.3%
Education High school or less 34% 26% 41%
Some college 23% 23% 24%College graduate 21% 24% 9%
* p< 0.05 for Asians vs. white and for black vs. white

Multivariable hazard ratios (95% CI)Asian Black (v. white)
Unadjusted 1.7 (1.3-2.2) 5.3 (4.8-5.9)
+adjusting for age, sex, education 1.6 (1.3-2.1) 5.1 (4.6-5.8)
+DM, MI, Cr, 1.7 (1.3-2.2) 3.7 (3.3-4.2)BP, proteinuria, hematuria
+Smoking, chol, BMI 2.1 (1.6-2.7) 3.3 (2.9-3.7)

• Several other studies have also shown that Asians have more rapid rates of renal function loss/kidney failure (compared with whites)
Hall CJASN 2010 Among the urban poor in San FranciscoBarbour NDT 2010 Canadian patients referred to nephrologyDerosa AJKD 2013 Kaiser S. California enrolleesBarbour KI 2013 Canadian IgA nephropathy patients
• No study has shown less rapid rates of loss Peralta JASN 2011 NIH cohort study (MESA) participants Conley AJKD 2012 Citizens of Alberta, Canada
• Generally lower rates of mortality

What could be some reasons for higher risks of kidney failure?
• Higher incidence of glomerulonephritis?• Use of herbal medications?

OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach

“In the early 1970s, mandatory kidney disease screening was started with urinalysis in the Japanese health examination program for all workers and school-age children. In 1983, nationwide urinalysis screening in adults aged >40 yr was mandated in the community-based health examination program. Because glomerulonephritis was an endemic disease and the leading cause of end-stage renal disease in Japan until 1997, the urinalysis in the annual health examination program aimed for early detection of glomerulonephritis and early referral of patients to physicians.”


OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach








OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach


http://baike.baidu.com/view/14324.htm (accessed August 12, 2014)
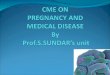
Fatigue Dizziness
Ringing in the ears
Forgetfulness
Sore in back and knees
Nocturnal emission (wet dream)
Erectile dysfunction
Male Femalemanifestation of weak kidneys
Kidneys Weakness

http://zh.m.wikipedia.org/wiki/五臟 (accessed August 12, 2014)

Hippocrates, Galen and humorism
http://en.wikipedia.org/wiki/Humorism (accessed August 12, 2014)
“The Human body contains blood, phlegm, yellow bile and black bile. These are the things that make up its constitution and cause its pains and health. Health is primarily that state in which these constituent substances are in the correct proportion to each other, both in strength and quantity, and are well mixed.”
--On the nature of man (Hippocrates)

The kidneys maintain stable internal milieu for the body

OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach


OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies)
4. Resources and approach

Bottomline
• At a fundamental level, approach to chronic kidney disease in Asians in no different from approaching chronic kidney disease in non-Asians
• Raise awareness, appropriate work-up and management (culturally sensitive)

http://nkdep.nih.gov/resources/NKDEP_Explaining_kidney_test_results_Vietnamese_508.pdf

http://nkdep.nih.gov/resources/NKDEP_Explaining_kidney_test_results_Chinese_508.pdf

Approach to (Asian) patients with CKD
• Treatment targeted to underlying etiology (e.g. glomerulonephritis)
• General treatment to retard CKD progression (e.g. blood pressure and proteinuria reduction)
• Manage CVD risk factors (e.g. lipid)• Treat complications of CKD (e.g. anemia,
acidosis)• Prepare for renal replacement therapy
(transplant evaluation, peritoneal dialysis, pre-emptive fistula)

OutlineBasic concepts in chronic kidney disease (CKD)Unique aspects of CKD in Asians1. Epidemiology2. Risk factors (e.g. glomerulonephritis,
herbal medications)3. Lessons from clinical practice (e.g.
Eastern vs. Western view of “the kidney”; use of traditional remedies
4. Resources and approach