-
8/2/2019 Renal Control of BP
1/12
Renal Control of BP
MCT
-
8/2/2019 Renal Control of BP
2/12
Hemorrhage
Venous return blood volume
MAP
SV and CO Atrial volume
LP Baroreceptors
HP BaroreceptorsCentral
Chemoreceptors
Peripheral
Chemoreceptors
Medullary
Cardiovascular
Control Center
SYMPATHETIC RESPONSE
Heart rate
Contractility
Vasoconstriction
(arteriole/venous)
Hormonal response
-Angiotensin/Renin
-ADH release
-ANP (decreased)
-
8/2/2019 Renal Control of BP
3/12
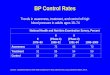
Long-term and short-term control of ABP
resistence &
compliance
Short-termBaroreflex
Long-term
hypertrophy Angiotensin II
Vasopressin
NO
ANP
Endothelin
Sympathetic nervous
system
heart Blood Volume
Drinking
Renal excretion
Na-intake
EPO
Ackermann
-
8/2/2019 Renal Control of BP
4/12
Blood pressure regulation
vasodilatation vasoconstriction
stimulation ofcGMP
stimulation ofcAMP
inhibition ofcAMP
Stimulation ofIP
3
In smooth muscle, cGMP and cAMPstimulates Ca2+ pump of
thesarcoplasmic reticulum
Decrease of Ca2+ concentration in
smooth muscle cell
Slower decreaseof Ca2+
IP3releases Ca2+from thesarcoplasmicreticulum
NO
ANP
adenosine A2histamine H2adrenaline b2
VIP
serotonin
adrenaline a2
angiotensin II
serotonin
adrenaline a1
vasopressin
-
8/2/2019 Renal Control of BP
5/12
Regulation of blood flow
myogenic stretch-activated cation channels
causevasoconstriction
metabolic metabolic products cause vasodilatation
sheardependent
vasodilatation by NO, which is produced invascular
endothelium
neural sympathetic constrictor nerves in mosttissues
parasympathetic dilator nerves in somesecretory and spongiform
tissues
humoral constriction by angiotensin II, epinephrine,vasopressin,
serotonin
dilatation by ANP, histamine, inflammatory
mediators
-
8/2/2019 Renal Control of BP
6/12
circulation local metabolic
control
sympathetic
control
mechanical
effects
coronary hypoxia
adenosine
least important compression
during systolacerebral CO2
H+
least important increasedintracranialpressuredecreases CBF
skeletalmuscle
during exercise
lactate
K+
adenosine
at rest
a vasoconstriction
b vasodilatation
muscularactivitycompressesblood vessels
skin - a vasoconstriction -
pulmonary hypoxiavasoconstricts
least important lung inflation
renal myogenic least important
-
8/2/2019 Renal Control of BP
7/12
Juxtaglomerular Apparatus
aglomerular
angial cells =
ation, structuralport, and
gocytosis
aglomerular /Lacis
angial cells = EPO
-
8/2/2019 Renal Control of BP
8/12
Renal circulation
25 % of cardiac output (1.3 L/min)
Renal blood flow is autoregulated
Constant blood flow even when renal perfusion pressurechanges
(80-200 mmHg)
Renal autoregulation is independent of sympatheticinnervation
(transplanted kidney)
Angiotensin II vasoconstrictor for both afferent and
efferent arterioles, but Efferent arteriole is more
sEnsitive
Prostaglandins (E2, I2 produced locally) vasodilatation ofboth
arterioles
-
8/2/2019 Renal Control of BP
9/12
The filtration relies on a net differential pressure
comprised of three components: Capillary hydrostatic pressure
(45 mmHg)
Bowmans hydrostatic pressure (10 mmHg)
Plasma protein oncotic pressure (25mHg)
Net pressure = PHyd + POnc = (45-10) 25 = 10 mmHg
The GFR is dependent on perfusion pressure to the
kidney, and therefore there are a group of smooth musclecells
that comprise thejuxtaglomerular apparatus andthey detect changes
in this pressure. NB These cells areregulating GFR, not BP.
Glomerular Filtration of Blood
-
8/2/2019 Renal Control of BP
10/12
Juxtaglomerular cells
Modified, granular smooth muscle cells on
afferent and efferent glomerular arterioles,
responsible for synthesizing and releasing renin
Release renin in response to:
Decreased afferent arteriolar pressure
(detected directly)
Increased sympathetic tone
Decreased [NaCl] as detected in the Macula
densa cells
Prostaglandin and NO release
Macula densa cells
Tubular cells that detect [NaCl] in the distal
tubule
When [NaCl] is low MD cells:
Release vasodilator in to afferent arterioles
Increase renin release in to afferent and
efferent arterioles by stimulating JG cells
Net effect of activation within this system is to
increase arteriolar pressure to restore GFR
Glomerular Filtration of Blood
-
8/2/2019 Renal Control of BP
11/12
Renin (an enzyme) released in to blood due to:
Decreased renal arteriolar pressure b1 receptor activation from
SNS
Decreased [NaCl] at MD cells
Renin cleaves angiotensin I from angiotensinogen Angiotensinogen
is made in the liver
Angiotensin I has no activity
Angiotensin II is cleaved from angiotensin I by ACE Angiotensin
II effects:
Systemic vasoconstriction (AT-I receptor)
Increased Na+ and H20 retention Direct action on renal cells
Aldosterone release from adrenal cortex
ADH release from pituitary
Thirst
Cardiac and vascular growth (AT-II receptor)
Renin Angiotensin Aldosterone System (RAAS)
-
8/2/2019 Renal Control of BP
12/12
One renal artery is occluded in a patient with two kidneys
Constricted kidney:
Decreased renal arteriolar pressure
Renin secretion
Angiotensin II effects Increased GFR
Increased Na and H2O absorption
Normal kidney: Also increases Na and H2O absorption due to
ischemic kidney renin production
Hypertension
Markers of renal insufficiency such as plasma creatinine are
often masked
due to the hyperfiltrationin the functional kidney.
2 Major causes of renal artery stenosis:
Atherosclerotic disease
Fibromuscular dysplasia = Autosomal dominant disorder resulting
in an
abnormal thickening of the intima, media or adventitia of the
renal artery
Unilateral Stenosis of Renal Artery (2-KidneyGoldblatt HTN)