Embed Size (px)
Citation preview
Removal time of fiber posts versus titanium posts
ABSTRACT: Purpose: To evaluate the time needed to remove a glass reinforced fiber post versus a titanium post.Methods: 40 extracted anterior teeth were mounted in acrylic blocks then treated endodontically. They were randomlyassigned to three groups. The teeth were sectioned horizontally, with the coronal portion removed. The fiber posts werecemented with resin cement and the titanium posts were cemented with glass ionomer or resin cement. The fiber postswere removed by coring them out internally. The titanium posts were removed by creating a trough around the post thenvibrating with ultrasonic energy. The teeth were examined visually and radiographically to ensure complete removal ofthe post and cement. Removal time included the time to make radiographs necessary to ensure complete removal.Results: Post-cement combination significantly affected the median rank of the removal time (Kruskal-Wallis test; H=12.709; P= 0.002). The mean rank removal time of titanium posts cemented with resin cement were significantly higherthan the mean rank of the other two post-cement combinations (Dunn's multiple comparison test; P< 0.05). There wasno significanrdifference between the other two combinations. (Am J Dent 2008 ;21: 175-178).
CLINICAL SIGNIFICANCE: When removing a fiber post, there is no need to create a trough around the fiber post or touse ultrasonic vibration than may weaken the tooth. The canal space can be cleaned and a new post placed or the canalcan b~ enlarged and additional retentive features added.
~: Dr. Robert Q. Frazer, Department of Prosthodontics, University of Kentucky College of Dentistry, Room D-640,Chandler Medical Center, Lexington, KY 40539-0297, USA. E-~: [email protected]
Introduction
Though advancements in endodontic techniques, sealers,fillers, posts and cores continue, as many as 36% of root canalswill eventually require re-treatment, and at least a quarter ofthese will involve removal of a post. I
Cast posts had been advocated for-ov~I\ a century, butprefabricated posts have become the predominant. modalityover the last 50 years. In the last two decades, the" trend hasbeen away from stainless steel towards titanium alloy, fromactive (threaded) posts towards passive, and from wedge-shaped posts towards parallel?
The dental literature is anything but unanimous about theideal technique for the removal of posts. A number of casestudies describe the use of mechanical removal devices that canbe used without root fracture, but there is very little supportingtheir efficacy.3.6 Most of these devices involve creation of acircumferential gutter around the coronal extremity of the postin order to adequately grasp and extract the post. Such guttersincrease the amount of tooth sacrificed during post removal.
A 1993 survey7 of U.S. endodontists disclosed that for postremoval, most would rather ,employ a hemostat (97%) and/ordrill them out with burs (62%). Some respondents report~d theythought post removal-devices were too dangerous, could not beused universally, or that they did not work. A 2002 survey4 ofAustralian and New Zealand endodontists revealed thatultrasonic vibration was u.sed by 95% of respondents.
Ultrasonic energy applied to the exposed metal post for 16minutes would break down the zinc phosphate cement, andcould reduce the amount of force necessary in vitro to extractmetal prefabricated posts.8 Two studies9
.10 demonstrated that
some ultrasonic sources and tips were more effective thanothers. Also, application of ultrasonic energy to posts createdmicrocracks in the remaining dentin, and that it took longer toremove posts after ultrasonic energy application than it tookwith a Gonan remover.3 Contradicting the conclusions ofJohnson et al,4 Hauman et alii found that neither alloy type,
cement type or 16 minutes of ultrasonic vibration decreased theforce required to remove titanium posts After comparing the 4mm deep gutter technique to a lO-minute ultrasonic procedure,Chandler et al12 concluded that neither approach was parti-cularly successful.
In most cases, the practitioner is resigned to approach theremoval of these posts on a case-by-case basis armed only withan insurance code and little formal training for the procedure.Regardless of the preferred removal technique, the properties ofa metallic post and the typical length of their penetration dictatethat the post be removed intact. Clinically, the ease or difficultyof removal may depend on numerous factors, including: thecondition of the tooth, leakage, corrosion activity, length ofpost insertion, and presence of a restoration and/or prosthesis.Titanium posts cemented with adhesive resin cements weremore difficult to remove after ultrasonic vibration than thosecemented with zinc phosphate or glass-ionomer cements. 13
The consensus of the dental literature fails to support anyparticular method for post removal. Current textbooks andconversations with experienced clinicians suggest that removalprocedures should include: (1) a circumferential trough createdwith a bur, (2) ultrasonic energy to dissolve cement, and (3)some tugging to remove the post. 14
In 1990, Duret et ailS patented an endodontic post made ofcarbon fiber reinforced composite. Introduced as theComposiposta these became immediately popular in Europe,and were introduced to the US marketplace in 1995 as the C-Post.b Exhibiting good strength and an elastic modulus(rigidity) close to that of dentin and a fraction that of metal,these posts have been shown to reduce, if not eliminate theincidence of root fracture in vitrol6
.17and in ViVO.
18•19 Even when
bonded in place with bonding agent and resin cement, thecarbon fiber posts could be easily removed by hollowing themout from their center.20 Because of the inherent clinical advan-tages of fiber posts, this basic technology has been widelyimitated and improved upon. Recently marketed fiber posts are
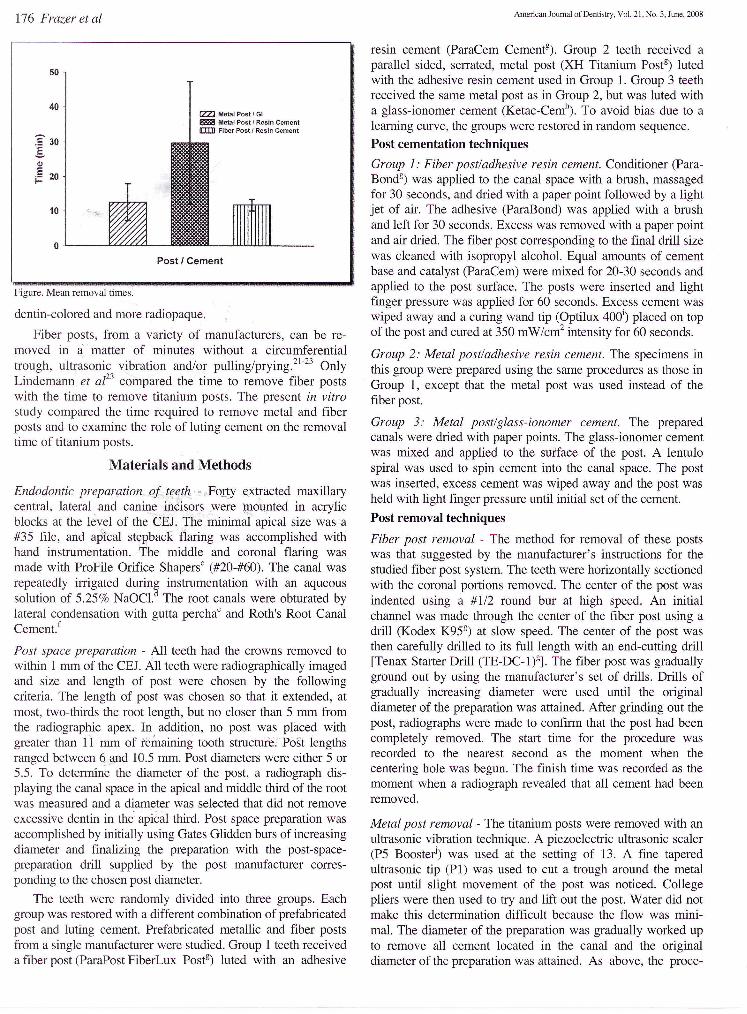
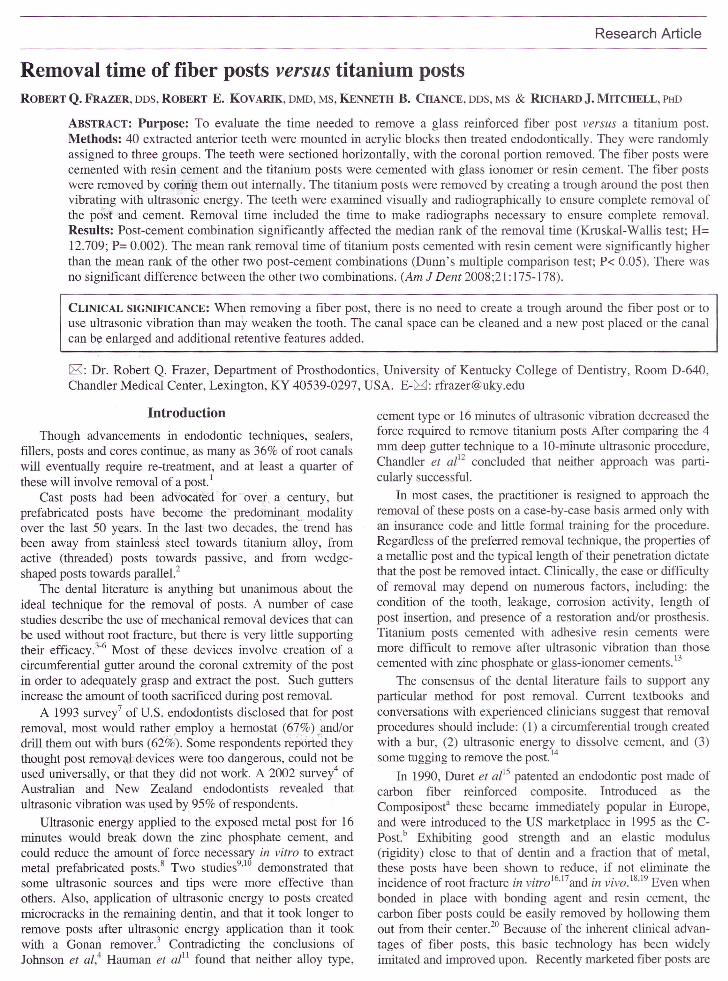
:? 30.§.Ql
Ei= 20
CZZI Metal Post f GlZ888 Metal Post {Resin Cementn:IID Fiber Post I Resin Cement
dentin-colored and more radiopaque.
Fiber posts, from a variety of manufacturers, can be re-moved in a' matter of minutes without a circumferentialtrough, ultr~sonic vibration and/or pulling/prying?1-23 OnlyLindemann et az23 compared the time to remove fiber postswith the time to remove titanium posts. The present in vitrostudy compared the time required to remove metal and fiberposts and to examine the role of luting cement on the removaltime of titanium posts.
Materials and Methods
Endodontic preparation of teeth - ."Forty extracted maxillarycentral, lateral. and canine in~is'Ors .were tpo:qnted in acrylicblocks at the level of the CEl The minimal apical size was a#35 file, and apical stepback flaring was accomplished withhand instrumentation. The middle and coronal flaring wasmade with ProFile Orifice Shapersc (#20-#60). The canal wasrepeatedly irrigated during instrumentation with an aqueoussolution of 5.25% NaOCLd The root canals were obturated bylateral condensation with gutta perchae and Roth's Root CanalCement.f
Post space preparation - All teeth had the crowns removed towithin I mm of the CEJ. All teeth were radiographically imagedand size and length of post were chosen by the followingcriteria. The length of post was chosen so that it extended, atmost, two-thirds the root length, but no closer than 5 mm fromthe radiographic apex. In addition, no post was placed withgreater than Ii mm of remaining tooth structure: Post lengthsranged between 6.qnd 10.5 mm. Post diameters were either 5 or5.5. To determine the diameter of the post, a radiograph dis-playing the canal space in the apical and middle third of the rootwas measured and a diameter was selected that did not removeexcessive dentin in th~ apic31 third. Post space preparation wasaccomplished by initially using Gates Glidden burs of increasingdiameter and finalizing the preparation with the post-space-preparation drill supplied by the post manufacturer corres-ponding to the chosen post diameter.
The teeth were randomly divided into three groups. Eachgroup was restored with a different combination of prefabricatedpost and luting cement. Prefabricated metallic and fiber postsfrom a single manufacturer were studied. Group I teeth receiveda fiber post (ParaPost FiberLux Postg) luted with an adhesive
resin cement (ParaCem Cementg). Group 2 teeth received aparallel sided, serrated, metal post (XH Titanium Postg) lutedwith the adhesive resin cement used in Group 1. Group 3 teethreceived the same metal post as in Group 2, but was luted witha glass-ionomer cement (Ketac-Cemh
). To avoid bias due to alearning curve, the groups were restored in random sequence.Post cementation techniques
Group 1: Fiber post/adhesive resin cement. Conditioner (Para-Bondg) was applied to the canal space with a brush, massagedfor 30 seconds, and dried with a paper point followed by a lightjet of air. The adhesive (ParaBond) was applied with a brushand left for 30 seconds. Excess was removed with a paper pointand air dried. The fiber post corresponding to the final drill sizewas cleaned with isopropyl alcohoL Equal amounts of cementbase and catalyst (ParaCem) were mixed for 20-30 seconds andapplied to the post surface. The posts were inserted and lightfinger pressure was applied for 60 seconds. Excess cement waswiped away and a curing wand tip (Optilux 400i) placed on topof the post and cured at 350 mW/cm2 intensity for 60 seconds.
Group 2: Metal post/adhesive resin cement. The specimens inthis group were prepared using the same procedures as those inGroup I, except that the metal post was used instead of thefiber post.
Group 3: Metal post/glass-ionomer cement. The preparedcanals were dried with paper points. The glass-ionomer cementwas mixed and applied to the surface of the post. A lentulospiral was used to spin cement into the canal space. The postwas inserted, excess cement was wiped away and the post washeld with light finger pressure until initial set of the cement.Post removal techniques
Fiber post removal - The method for removal of these postswas that suggested by the manufacturer's instructions for thestudied fiber post system. The teeth were horizontally sectionedwith the coronal portions removed. The center of the post wasindented using a #1/2 round bur at high speed. An initialchannel was made through the center of the fiber post using adrill (Kodex K95g) at slow speed. The center of the post wasthen carefully drilled to its full length with an end-cutting drill[Tenax Starter Drill (TE-DC-I)g]. The fiber post was graduallyground out by using the manufacturer's set of drills. Drills ofgradually increasing diameter were used until the originaldiameter of the preparation was attained. After grinding out thepost, radiographs were made to confirm that the post had beencompletely removed. The start time for the procedure wasrecorded to the nearest second as the moment when thecentering hole was begun. The finish time was recorded as themoment when a radiograph revealed that all cement had beenremoved.
Metal post removal - The titanium posts were removed with anultrasonic vibration technique. A piezoelectric ultrasonic scaler(P5 Boosteri) was used at the setting of 13. A fine taperedultrasonic tip (PI) was used to cut a trough around the metalpost until slight movement of the post was noticed. Collegepliers were then used to try and lift out the post. Water did notmake this determination difficult because the flow was mini-mal. The diameter of the preparation was gradually worked upto remove all cement located in the canal and the originaldiameter of the preparation was attained. As above, the proce-

dure was continued until cement removal was confIrmed;therefore, multiple radiographs may have been required. Thestart time for the procedure was recorded as the moment thatthe trough around the tooth was begun. The finish time wasrecorded as the as the moment when a radiograph revealed thatall cement had been removed.
Results
The Figure shows the mean removal times. The initial planwas to use an ANOV A to analyze this data. The underlyingassumption of ~ANOVA is that the sample populations to becompared each ~ have a normal distribution and that thevariances of the means are homogeneous.24 Tests fornormality25 showed that the sample population of each groupwas normal. However, the null hypothesis that the variances ofthe removal times are equal was rejected (Levene's Test forHomogeneity of Means,25 F= 7.16; P= 0.0028).
Since ANOV A could not be used, a one-way Kruskal-Wallis ANOV A of median ranks was used. This is a nonpara-metric test, which requires neither a normal distribution nor ho-mogeneous variances.24 The one-way Kruskal-Wallis ANOVAof median ranks is the nonparametric analogue of the para-metric ANOV A.24 The data was converted to ranks and theKruskal-Wallis test was run for the effect of group on the rankof the removal time. Test group was found to significantlyaffect the median rank of the removal time (H= 12.709; P=0.002)}6 Dunn's multiple comparison test (P< 0.05) showedthat the median rank of the removal time for titanium postscemented with resin cements was signifIcantly higher than themedian rank of either of the other -two groups. Groups 1 and 3were not signifIcantly different from one another}6
Kruskal-Walli§ one-way'ANOVA were also used to investi-gate whether post length or post diameter had a significanteffect on removal time. For each of the groups, post length wasfound to have no signifIcant effect on rank removal time(Group 1, H= 3.69, P= 0.72; Group 2, H= 6.82, P= 0.23; Group3, H= 4.81, P= 0.44). Similarly, post diameter also had nosignifIcant effect on removal time (Group 1, H= 0.75, P= 0.39;Group 2, H= 0.83, P= 0.36; Group 3, H= 0.32, P= 0.57)}6
Discussion
This study confIrms previous studies21-23showing that fIberposts can be removed in very little time. Retreatment of failedpost-containing restorations need not take excessive time. Themean removal time for fIber posts reported here was longerthan that found by either' of the previous studies 0.2-1.4minutes,21 0.3-D.'",7__minutes,22 and 2.5-7.0 minutes23). Thelonger removal trmes in this study were due to the time requiredto make radiographs of the canals to confIrm complete cementremoval. Gesi et az22 did not check for complete cementremoval but rather stopped canal preparation when gutta perchafIrst appeared. Following removal of the post, Lindemann etaP sectioned the roots vertically and used an optical micro-scope to score the removal effectiveness. Cormier et az2°.21 usedthe technique of Sakkal20where canal preparation was completewhen the post was removed to the cement layer.
The present study confIrms the result of Lindemann et aZ23
that fIber posts can be removed much more quickly thantitanium posts that have been luted with adhesive resin cement.This study also shows that removal time for titanium posts can
be reduced if the posts are luted with a glass-ionomer cement.Unfortunately, luting with glass-ionomer cement cannot berecommended. To achieve the highest retention values, titaniumposts are routinely cemented with adhesive resin cement ratherthan with glass ionomer or zinc phosphate cements.27,28
In this study the posts were cut off at the level of the CElIn previous studies3,8,10,29the posts were left projecting abovethe top of the root for use as a handle. Removal of the post atthe level of the root simulated the complete fracture and loss ofthe tooth crown. This makes removal of titanium posts muchmore difficult. If the tooth is trenched around the post to allowan instrument to grasp the post, the tooth may be furtherweakened. There should be sufficient tooth structure above theosseous crest to allow for the creation of a ferrule preparation.Long term survival of the tooth might be jeopardized if there isnot space for at least a 1.5-2 mm ferrule. 30
This study confirmed that fiber posts can be more rapidlyremoved than titanium posts. Moreover, removal can beaccomplished without resorting to ultrasonic vibration that mayfurther weaken the tooth.3 Fiber posts exhibited adequateclinical performance. 18,31That they can be quickly and safelyremoved is another reason to choose fIber posts for therestoration of endodontically treated teeth.
a. RTD, St. Egreve, France.b. Bisco Dental Products, Schaumburg, IL, USA.c. Dentsply, Tulsa, OK, USA. ..d. Clorox; Clorox Inc., Oakland CA, USA.' .e. Coltene Whaledent, Mahwah, NJ, USA.f. Roth International, Chicago, IL, USA.g. Coltene Whaledent, Cuyahoga FalJs, OH, USA.h. 3M ESPE, Minneapolis, MN, USA.i. Demetron, Danbury, CT, USA.j. Acteon Co., Mount Laurel, NJ, USA.
Dr. Frazer is Assistant Professor of Prosthodontics, Dr. Kovarik is AssociateProfessor of Restorative Dentistry, Dr. Chance is Professor of Endodontics, andDr. Mitchell is Associate Professor of Restorative Dentistry, University ofKentucky College of Dentistry, Chandler Medical Center, Lexington, Kentucky,USA.
1. Abbott PV. Analysis of a referral-based endodontic practice: Part 2.Treatment provided. J Endod 1994;20:253-257.
2. Fernandes AS, Shetty S, Coutinho I. Factors determining post selection: Aliterature review. J Prosthet Dent 2003;90:556-562.
3. Altshul JH, Marshall G, Morgan LA, Baumgartner Je. Comparison ofdentinal crack incidence and of post removal time resulting from postremoval by ultrasonic or mechanical force. J Endod 1997 ;23 :683-686.
4. Castrisos T, Abbott PV. A survey of methods used for post removal inspecialist endodontic practice. Int Endod J 2002;35: 172-180.
5. Abbott PV. Incidence of root fractures and methods used for post removal.Int Endod J 2002;35:63-67.
6. Ruddle CJ. Nonsurgical retreatment. J Endod 2004;30:827-845.7. Stamos DE, Gutmann JL. Survey of endodontic retreatment methods used
to remove intraradicular posts. J Endod 1993;19:366-369.8. Johnson WT, Leary JM, Boyer DB. Effect of ultrasonic vibration on post
removal in extracted human premolar teeth. J Endod 1996;22:487-488.9. Dixon EB, Kaczkowski PJ, Nicholls IT, Harrington GW. Comparison of
two ultrasonic instruments for post removal. J Endod 2002;28:111-115.10. Buoncristiani J, Seto BG, Caputo AA. Evaluation of ultrasonic and sonic
instruments for intraradicular post removal. J Endod 1994;20:486-489.11. Hauman CH, Chandler NP, Purlon DG. Factors influencing the removal of
posts. Int Endod J 2003;36:687-690.12. Chandler NP, Qualtrough AJ, Purlon DG. Comparison of two methods for
the removal of root canal posts. Quintessence Int 2003;34:534-536.13. Gomes AP, Kubo CH, Santos RA, Santos DR, Padilha RQ. The influence
of ultrasound on the retention of cast posts cemented with different agents.Int Endod J 2001 ;34:93-99.
14. Cohen S, Burns RC. Pathways of the Pulp. 7"' ed. St. Louis, Missouri:Mosby, 1998;799-801.
15. Duret B, Reynaud M, Duret F. A new concept of corono-radicularreconstruction, the Composipost (2). Chir Dent Fr 1990;60:69-77. (InFrench).
16. Dean JP, Jeansonne BG, Sarkar N. In vitro evaluation of a carbon fiberpost. J Endod 1998;24:807-810.
17. Isidor F, adman P, Brondum K. Intermittent loading of teeth restored usingprefabricated carbon fiber posts.Int J Prosthodont 1996;9:131-136.
18. Ferrari M, Vichi A, Garcia Godoy F. Clinical evaluation of fiber-reinforcedepoxy resin posts and cast post and cores. Am J Dent 2000;13:15B-18B.
19. Fredriksson M, Astback J, Pamenius M, Arvidson K. A retrospective studyof 236 patients with teeth restored by carbon fiber-reinforced epoxy resinposts. J Prosrhet Dent 1998;80:151-157.
20. Sakkal S. Carbon-fiber post removal technique. Compend Contin EducDent SuppI1996;20:S86.
21. Cormier CJ, Burns DR, Moon P. In vitro comparison of the fractureresistance and failure mode of fiber, ceramic, and conventional postsystems at various stages of restoration. J Prosthodont 2001; 10:26-36.
22. Gesi A, Magnolfi S, Goracci C, Ferrari M. Comparison of two techniquesfor removing fiber posts. J Endod 2003;29:580-582.
23. Lindemann M, Yaman P, Dennison JB, Herrero AA. Comparison of theefficiency and effectiveness of various techniques for removal of fiberposts. J Endod 2005;31:520-522.
24. Daly LE, Bourke GJ. Interpretation and uses of medical statistics. 5"' Ed.Oxford, UK: Blackwell Science; 2000.
25. SASJnstitute. Proc CLM. SAS 9.1. Cary, NC, USA: SAS Institute Inc.; 2002.26. Systat_Software. Kruskal-Wallis Analysis of Variance on Ranks.
SigmaStat 3.1 for Windows. Point Richmond, CA, USA: Systat Software,Inc.; 2004.
27. Cheung W. A review of the management of endodontically treated teeth.Post, core and the final restoration. JAm Dent Assoc 2005;136:611-619.
28. Schwartz RS, Robbins JW. Post placement and restoration ofendodontically treated teeth: A literature review. J Endod 2004;30:289-301.
29. Berbert A, Filho MT, Ueno AH, Bramante CM, Ishikiriama A. Theinfluence of ultrasound in removing intraradicular posts. Int Endod J1995;28:54-56.
30. Morgana SM. Restoration of pulpless teeth: Application of traditionalprinciples in present and future contexts. J Prosthet Dent 1996;75:375-380.
31. Mitsui PH, Marchi GM, Pimenta LA, Ferraresi PM. In vitro study offracture resistance of bovine roots using different intraradicular postsystems. Quintessence Int 2004;35:612-616.
~ Oral cancer: Current and future diagnostic techniques.C. Scully, J. V. Gaban, C. Hopper & JB. Epstein
~ Hardness and elasticity of caries-affected and sound primary tooth dentin bondedwith 4~META one~tep'self-etch adhesives.Y. Hosoya, F.R. ray, S. MiyakQ.shi & DB. Pashley
~ Comparison of detachment forces of two implant overdenture attachment types:Effect of detachment speed.SR. Jefferies, D.W. Boston, M.P. Damrow & C.T. Galbraith
~ Cytotoxic effects and pulpal response caused by a mineral trioxide aggregateformulation and calcium hydroxide.C.A.de Souza Costa, P.T. Duarte, P.P. Chaves Souza, EM. Aparecida Giro & J. Hebling
~ Histological evaluation of mineral trioxide aggregate and calcium hydroxide in directpulp capping of human immature permanent teeth.L. Sawicki, CB. Pameijer, K. Emerich & B. Adamowicz-Klepalska
~ The influence of dynamic fatigue loading on the separate components of the bracket-cement-enamel system.T.J. 'Atgera, C.J. Kleverlaan, KPrahl-Andersen & A.J. F eilzer
)? ;::-Translucencyof varied brand and shade of resin composites.B. Yu & Y-K. Lee
~ Eff~ct of different 1% chlorhexidine varnish regimens on mutans streptococci levels insaliva and dental biofilm.L.G. Maia Ribeiro, L.N. Hashizume & M. Malz





























