Embed Size (px)
Citation preview

Relationships among biomarkers of one-carbon metabolism
Will D. King • Vikki Ho • Linda Dodds •
Sherry L. Perkins • R. Ian Casson •
Thomas E. Massey
Received: 7 July 2011 / Accepted: 16 April 2012 / Published online: 24 April 2012
� Springer Science+Business Media B.V. 2012
Abstract One-carbon metabolism is a network of meta-
bolic pathways, disruption of which has been associated with
cancer and other pathological conditions. Biomarkers of
these pathways include homocysteine (HCY), S-adenosyl-
methionine (SAM), and S-adenosylhomocysteine (SAH). A
better understanding of the relationships between these
biomarkers is needed for their utilization in research. This
study investigated the relationships between fasting con-
centrations of plasma HCY, SAM, SAH and the ratio of
SAM:SAH, and serum folate, vitamin B12 and creatinine in
a healthy adult population. A cross-sectional study recrui-
ted 678 volunteers; only subjects with complete data
(n = 581) were included in this analysis. Correlations were
used to examine bivariate relationships among the bio-
markers and multivariate linear regression determined
independent relationships with HCY, SAM and SAH
treated as dependent variables in separate models. Multi-
variate logistic regression examined determinants of a low
SAM:SAH ratio (defined as having a SAM:SAH ratio in
the bottom quartile and SAH value in the top quartile).
HCY correlated inversely with folate and vitamin B12 and
weakly correlated with SAH and creatinine. Both SAM and
SAH correlated with creatinine but were independent of
serum folate and vitamin B12. In multivariate analyses,
folate, vitamin B12, creatinine, sex and age were associated
with HCY; age and creatinine were determinants of SAM,
and sex and creatinine determinants of SAH. Finally, male
sex and increasing creatinine levels were associated with
having a low SAM:SAH ratio. Findings suggest that HCY,
SAM and SAH are relatively independent parameters and
reflect distinct aspects of one-carbon metabolism.
Keywords Homocysteine � S-Adenosylmethionine �S-Adenosylhomocysteine � Creatinine � One-carbon
metabolism
Introduction
There is considerable evidence that aberrant DNA methylation
patterns play a critical role in gene regulation; DNA methyl-
ation is an important feature of epigenetics that is increasingly
being implicated in disease states including cancer, cardio-
vascular disease, renal disease, neurodegenerative disease and
W. D. King (&) � V. Ho
Department of Community Health and Epidemiology, Queen’s
University, Carruthers Hall, Kingston, ON K7L 3N6, Canada
e-mail: [email protected]
V. Ho
e-mail: [email protected]
L. Dodds
Department of Obstetrics and Gynaecology, Perinatal
Epidemiology Research Unit, IWK Health Centre, Halifax,
NS B3K 6R8, Canada
e-mail: [email protected]
S. L. Perkins
Department of Pathology and Laboratory Medicine, The Ottawa
Hospital and University of Ottawa, Ottawa, ON K1H 8L6,
Canada
e-mail: [email protected]
R. I. Casson
Centre for Studies in Primary Care, Queen’s University,
Kingston, ON K7L 5E9, Canada
e-mail: [email protected]
T. E. Massey
Pharmacology and Toxicology Graduate Program, Department
of Biomedical and Molecular Sciences, Queen’s University,
Botterell Hall, Kingston, ON K7L 3N6, Canada
e-mail: [email protected]
123
Mol Biol Rep (2012) 39:7805–7812
DOI 10.1007/s11033-012-1623-y

birth defects [1]. DNA methylation patterns are supported by
one-carbon metabolism as methyltransferases utilizes S-
adenosylmethionine (SAM), a metabolite of one-carbon
metabolism, as a methyl group donor [1]. As interest in the role
epigenetics play on the pathogenesis of many disease states
grows, metabolites of one-carbon metabolism including
homocysteine (HCY), SAM and S-adenosylhomocysteine
(SAH) are increasingly being used as predictors, intermediate
effects and outcomes in epidemiologic studies [2–5].
The known effects of SAM and SAH on cellular
methylation suggest that concentrations of SAM and SAH
may be useful measures representing an individual’s DNA
methylation capacity. SAM is a methyl donor for numerous
cellular methyltransferase reactions and SAH is the
demethylated product of SAM with a potent ability to
inhibit DNA methyltransferase reactions; thus, the ratio of
SAM to SAH has been referred to as the ‘‘methylation
index’’ [1, 6]. However, interpretation of the ratio of
SAM:SAH is complex since a low SAM to SAH ratio
could be due either to decreased levels of SAM (limited
substrate availability), increased concentrations of SAH
irrespective of SAM concentrations or their combination
[6–8]. On the other hand, HCY as a biomarker has been
investigated as a risk factor for many pathological condi-
tions, most notably applied in cardiovascular, neurode-
generative and certain types of cancer research. The two
main hypotheses that have been postulated to explain the
role of elevated HCY levels in these conditions include the
generation of reactive oxygen species and aberrant DNA
methylation patterns through an influence of HCY on SAM
and SAH concentrations [8]. Specifically, Gellekink et al.
[6] have shown that DNA hypomethylation is associated
with moderate elevations of HCY and SAH concentrations,
and a decreased SAM to SAH ratio. Due to the close
interrelationships between these biomarkers, it is unclear
which is causally implicated when considering these bio-
markers in relation to the pathogenesis of disease.
Detailed diagrams and descriptions of the biochemical
processes associated with one-carbon metabolism are
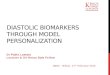
available in several sources [2, 9, 10]. Figure 1 depicts a
simplified schematic illustrating the pathways involved in
one-carbon metabolism. It is important to note that one-
carbon metabolism is complex and intersects with other
pathways necessary for the synthesis and utilization of
other significant metabolites such as folic acid, thymidyl-
ate, and cysteine and its derivatives [11, 12].
In one-carbon metabolism, methionine is activated by
adenosine triphosphate (ATP) to produce SAM. Transmeth-
ylation of SAM in which the methyl group of SAM is trans-
ferred to an acceptor results in the formation of SAH. These
reactions include the methylation of small molecules and
macromolecules such as creatine (the precursor of creatinine),
proteins, RNA and DNA [13]. Under physiologic conditions,
SAH is hydrolyzed by S-adenosylhomocysteine hydrolase
(SAHH) to HCY and adenosine in a reversible reaction that
strongly favours SAH synthesis rather than hydrolysis [4, 14].
Diet
TS
Cysteine & Taurine
Vitamin B12
ATP
FOLATE METABOLISM
ONE-CARBON METABOLISM Methylated
acceptor
Acceptor
SAHH
Dihydrofolate
Folic Acid
dUMP
dTMP
Tetrahydrofolate
5,10-Methylene Tetrahydrofolate
5-Methyl Tetrahydrofolatea
(Serum Folate)
Methionine
SAM
SAH
HCY
Vitamin B6
MS
Fig. 1 Simplified schematic of
one-carbon metabolism.
Biomarkers included in this
study appear in bold
(S-adenosylmethionine,
S-adenosylhomocysteine,
homocysteine, serum folate, and
vitamin B12). dUMPdeoxyuridine monophosphate,
TS thymidylate synthase, dTMPdeoxythymidine
monophosphate, MS methionine
synthase, ATP adenosine
triphosphate, SAMS-adenosylmethionine, SAHS-adenosylhomocysteine, SAHHS-adenosylhomocysteine
hydrolase, HCY homocysteine.a 5-methyl-THF may also be
derived from diet
7806 Mol Biol Rep (2012) 39:7805–7812
123

HCY is then metabolized by two biochemical pathways,
transsulfuration and remethylation. In the transsulfuration
pathway, HCY is catabolized to form the amino acids cysteine
and taurine in a series of irreversible reactions [10]. Alterna-
tively, to initiate a new cycle of one-carbon group transfer,
HCY is remethylated back to methionine by methionine
synthase (MS), a ubiquitous enzyme in most tissues, with
vitamin B12 acting as a co-factor and 5-methyltetrahydrofolate
(5-methyl-THF) a substrate. Thymidine synthesis competes
with the one-carbon metabolism cycle for the common sub-
strate 5,10-methylenetetrahydrofolate (5,10-methylene-THF),
a precursor of 5-methyl-THF produced during folate metab-
olism [9]. The reaction converts deoxyuridine monophosphate
(dUMP) to deoxythymidine monophosphate (dTMP) and is
catalyzed by thymidylate synthase (TS). The complexity of
the involved pathways clearly illustrates the importance and
the goal of metabolic regulation of one-carbon metabolism—
to balance and appropriately distribute metabolites among
these pathways while preventing the accumulation of the
involved intermediates (e.g., HCY, SAH and SAM) [11, 12].
As illustrated, HCY, SAM and SAH are essential
intermediates in one-carbon metabolism. However, a better
understanding of how these biomarkers are interrelated is
necessary for effective utilization in research and to
interpret findings. This study investigated the relationships
between HCY, SAM, SAH, the ratio of SAM to SAH,
folate, vitamin B12 and creatinine in a healthy middle-aged
Canadian population.
Methods
Study population
The data for this analysis were collected in a study focusing
on environmental exposures and markers of DNA meth-
ylation capacity. From 2006 to 2009, a cross-sectional
study recruited 678 healthy volunteer subjects, age 20–50,
from three study centers situated in Kingston, Ontario,
Ottawa, Ontario and Halifax, Nova Scotia, Canada. These
study centers were selected specifically to provide variation
in the environmental factors of interest; disinfection by-
products in public water supplies. Those with health con-
ditions that might be related to the biomarkers of interest
(e.g., history of coronary artery disease or other vascular
disease, or diabetes), or who had been pregnant within the
past year were not eligible. Eligible subjects consenting to
participate in this study provided 12 h fasting blood sam-
ples, completed a short questionnaire, and returned a take
home water sampling kit. Subjects with non-fasting blood
samples (n = 80) and incomplete questionnaire and bio-
chemical data (n = 17) were not included in the analysis,
resulting in a sample size of 581.
Laboratory analyses
Blood sampling, processing and aliquoting procedures were
standardized between the three study centers; a total of
15 mL of venous blood were drawn from each participant.
Specifically, concentrations of plasma SAM, SAH and HCY
were determined from 10 mL of blood drawn into tubes with
ethylenediaminetetraacetic acid (EDTA) and 5 mL of blood
was obtained in a serum separator tube (SST) for measure-
ments of serum folate, vitamin B12 and creatinine concen-
trations. After withdrawal, the EDTA tube was kept on ice
and centrifuged at 4 �C within 1 h of collection; 6 mL of
plasma was then extracted and stored in two separate aliquot
tubes for separate analysis of HCY, and SAM and SAH. For
the SST tube, 2 mL of serum was extracted after the speci-
men was allowed to clot and centrifuged at 4 �C within 1 h
of collection. Serum and plasma samples were kept frozen at
-80 �C prior to analysis; under these storage conditions,
levels of SAM, SAH and HCY have been reported to remain
stable for up to 4 years [14, 15]. Plasma HCY and serum
folate, vitamin B12 and creatinine were measured at the
Ottawa Hospital, Department of Pathology and Laboratory
Medicine, Division of Biochemistry, Ottawa, Canada.
Plasma SAM and SAH were measured at the Saskatchewan
Disease Control Laboratory, Saskatchewan, Canada. All
serum and plasma samples were shipped on dry ice.
Plasma HCY concentrations were quantified by the
Abbott AxSYM immunoassay based on fluorescence polar-
ization immunoassay technology (Abbott AxSYM, Abbott
Laboratories, Abbott Park, Illinois, USA). This assay has an
analytical range of 1–50 lmol/L and coefficients of variation
(CV) of 5.5 % at 7.4 lmol/L, 6.2 % at 13.5 lmol/L, and
5.4 % at 25.9 lmol/L. Plasma SAM and SAH were mea-
sured using a tandem mass spectrometry method developed
by Struys et al. [16] and Gellekink et al. [6]. Modification to
the published methods included the use of deuterium labelled
SAM (2H3-SAM) as an internal standard for both SAM and
SAH analyses; otherwise testing conditions of the assay were
conducted as described. Briefly, SAM and SAH were
obtained from Sigma (St. Louis, MO, USA) and 2H3-SAM
from CDN Isotopes (Pointe-Claire, Quebec, Canada). All
analyses were performed on an API 4000 triple quadrupole
tandem mass spectrometer and binary HPLC pump (Agilent
1200 series). This assay has CV of 7 and 15 % for SAM and
SAH, respectively. Recoveries for both SAM and SAH were
comparable to percentages published by Gellekink et al. [6]
(mean recoveries for SAM and SAH[90 %). Determination
of serum folate and vitamin B12 status was accomplished
using a two-step competitive immuno-enzymatic assay with
chemiluminescence detection on a Beckman Coulter DMXi
immunoassay analyzer (Beckman Coulter, Inc., Fullerton,
California, USA). This assay has analytical linearity of
1–45 nmol/L and a CV of 9.4 % at 3.4 nmol/L, 5.0 % at
Mol Biol Rep (2012) 39:7805–7812 7807
123

9.3 nmol/L, and 5.6 % at 22.0 nmol/L. Extreme values of
serum folate (n = 6) were truncated at three standard devi-
ations (SD) above the mean (mean serum folate ? 3
SD = 84.5 nmol/L). Finally, serum creatinine was deter-
mined colourimetrically by the Jaffe rate method on the
Beckman Coulter LX20PRO (Beckman Coulter, Inc., Ful-
lerton, California, USA) [17]. This assay has CV of 6 % at
60 lmol/L and 2.0 % or less at 180 and 610 lmol/L.
Statistical analyses
Distributions are presented according to quartiles, means
and SD. Pearson correlation coefficients were calculated to
evaluate bivariate relationships. Sensitivity analyses were
conducted to test the effect of non-normality on the Pear-
son correlation coefficient by comparing values obtained
through Pearson correlation to Spearman correlation.
Multivariate linear regression was used to determine
independent relationships with HCY, SAM and SAH
treated as dependent variables in separate models. In each
model the covariates included age, sex, serum folate, serum
vitamin B12 and serum creatinine.
In the multivariate linear regression analysis, all of the
variables were standardized (i.e., the difference between
each individual measurement and the overall mean was
divided by the SD). For serum creatinine, standardization
was conducted according to sex since serum creatinine
concentrations vary between males and females (e.g., the
difference between each individual female measurement of
serum creatinine and the overall female mean was divided
by the female SD). As a result all standardized biomarkers
have a mean of zero and SD of 1 and coefficients in the
regression model (e.g., slope [b] of the regression line) are
interpretable as the proportion of a SD change in the
dependent variable for a 1 SD change in the independent
variable. A variable representing the three study centers
was included as a random effects parameter to account for
the cluster sampling design.
The ratio of SAM to SAH has been proposed as a
methylation index; however, reports have indicated that a
decrease in the SAM:SAH ratio was only predictive of
reduced methylation capacity in the presence of high SAH
levels [4, 14]. For this study, a dichotomous variable rep-
resenting a low SAM:SAH ratio was defined as having a
SAM:SAH ratio in the bottom quartile of values and a SAH
value in the top quartile of values. Multivariate logistic
regression was used to examine relationships between the
dichotomous outcome of a low SAM:SAH ratio and stan-
dardized HCY, folate, vitamin B12 and creatinine; age and
sex were included in the regression model as covariates.
The cluster sampling design was accounted for by includ-
ing study center as a random effects parameter in the
logistic model.
Results
This analysis included 581 subjects with complete data on
all of the variables of interest. Subject recruitment was
designed to result in approximately balanced distribution
by sex and age. The final study had a greater proportion of
females (55 %) and a relatively balanced age distribution.
The distribution (quartiles), mean and SD of the bio-
markers under study are presented in Table 1.
Pearson correlation coefficients for the six biomarkers
are presented in Table 2. Plasma HCY did not correlate
with SAM, but had a positive correlation with SAH and
serum creatinine, and negative correlations with serum
folate and vitamin B12. SAM and SAH were found to only
correlate with serum creatinine. Folate and vitamin B12 had
a positive correlation. All of the markers have an approx-
imately normal distribution with a slight right skew and
Shapiro–Wilk tests for non-normal distribution were sta-
tistically significant (p value \ 0.05). However, violation
of the normality assumption tends to have little effect on
Pearson correlation coefficients given a sufficiently large
sample size [18]. In a sensitivity analysis (not presented)
Spearman correlation coefficients were found to be similar
to Pearson correlation coefficients presented.
The results of multivariate linear regression models with
standardized HCY, SAM and SAH treated as dependent
variables are presented in Table 3. Each coefficient is
interpretable as the proportion of a SD change of the
dependent variables for a one unit change in the indepen-
dent variable. Higher serum folate and vitamin B12 were
associated with decreased HCY levels and HCY increased
with serum creatinine, male sex and age. HCY was not
related to SAM or SAH. For the model using SAM as the
dependent variable, age and serum creatinine were the only
statistically significant predictors. With SAH as the
Table 1 Distribution of concentrations of HCY, SAM, SAH in
plasma, and folate, vitamin B12 and creatinine in serum (n = 581)
25th
percentile
Median 75th
percentile
Mean SD
HCY (lmol/L) 7.0 8.4 10.0 8.8 2.4
SAM (nmol/L) 54.7 62.2 73.2 64.0 13.6
SAH (nmol/L) 20.0 24.4 29.5 25.5 10.6
Folate (nmol/L) 21.8 28.2 35.5 29.4 11.1
Vitamin B12
(qmol/L)
161.0 213.0 284.0 234.9 110.0
Creatinine—
females
(lmol/L)
66.0 72.0 78.0 72.3 9.0
Creatinine—males
(lmol/L)
84.0 91.0 98.0 91.1 12.0
7808 Mol Biol Rep (2012) 39:7805–7812
123

dependent variable, SAH levels increased with serum
creatinine and were higher in males than in females.
A low SAM:SAH ratio was identified in 16.8 % of
subjects (e.g., a low SAM:SAH ratio in the presence of
high SAH). Table 4 presents odds ratios (OR) and 95 %
confidence intervals (95 % CI) for relationships with this
outcome. Higher serum creatinine and male sex were the
only factors associated with having a low SAM:SAH ratio.
Discussion
This study investigated the relationships between key
intermediates in one-carbon metabolism measured in fast-
ing blood samples obtained from 581 healthy adults. Our
mean SAM and SAH concentrations were found to be
similar to one of three studies conducted in fasting samples
of healthy subjects within a comparable age range [7].
Specifically, Loehrer et al. [7] reported mean SAM and
SAH levels that were similar to those observed in this
study. Tao et al. [19] and Valli et al. [20] both reported
higher mean SAM and SAH concentrations. Two addi-
tional studies that measured SAM and SAH levels in non-
fasting participants within a comparable age range both
reported higher mean SAM and lower SAH concentrations
[6, 21]. Reference values for plasma HCY measured in
healthy individuals are readily available in the literature;
our mean HCY was found to be consistent with those
reported in the literature [15].
The relationships between key intermediates in one-
carbon metabolism were investigated through bivariate and
multivariate analyses which address two different dimen-
sions of these relationships. Bivariate analysis gives
information on the extent to which each biomarker may
represent different aspects of one-carbon metabolism,
while multivariate analysis provides further insight into
underlying relationships among this set of biomarkers.
This discussion will focus on HCY, SAM and SAH.
With respect to bivariate analysis the main findings of note
were that: (1) HCY had only a weak positive association
with SAH and creatinine, was not associated with SAM,
and had strong negative correlations with folate and vita-
min B12 and; (2) SAM and SAH correlated with creatinine
but were independent of folate and vitamin B12. Few
studies have investigated the inter-relationships between
HCY, SAM and SAH in a healthy population sample; only
four studies have been identified [8, 22–24]. Becker et al.
[22] reported bivariate analysis of HCY, SAM and SAH
conducted among an older population (n = 97; aged
60–65); Yi et al. [23] investigated relationships with HCY,
SAM and SAH in a healthy female population (n = 58;
aged 19–53); Loehrer et al. [24] examined the correlation
between HCY, SAM and SAH as a sub-analysis conducted
among a healthy control group (n = 50; aged 41–87); and
Table 2 Pearson correlation coefficients between concentrations of
HCY, SAM, SAH in plasma, and folate and vitamin B12 in serum
HCY SAM SAH Folate Vitamin B12
SAM 0.00
SAH 0.09* 0.07
Folate -0.28* -0.03 -0.06
Vitamin B12 -0.18* -0.06 -0.01 0.20*
Creatinine 0.11* 0.10* 0.12* 0.00 -0.03
* p value \ 0.05
Table 3 Mulitvariate linear
regression analysis with
standardized HCY, SAM or
SAH as the dependent variable
Variable HCY SAM SAH
Coefficient p value Coefficient p value Coefficient p value
HCY (per 1 SD) -0.01 0.88 0.03 0.54
SAM (per 1 SD) -0.01 0.88 0.06 0.19
SAH (per 1 SD) 0.02 0.54 0.05 0.19
Folate (per 1 SD) -0.25 \0.01 0.02 0.71 -0.03 0.48
Vitamin B12 (per 1 SD) -0.16 \0.01 -0.03 0.53 0.00 0.98
Creatinine (per 1 SD) 0.13 \0.01 0.09 0.02 0.10 0.01
Sex (male vs female) 0.57 \0.01 -0.11 0.19 0.27 \0.01
Age (per 10 years) 0.11 \0.01 0.13 \ 0.01 0.04 0.43
Table 4 Multivariate OR and 95 % CI for a low SAM:SAH ratio
Variable OR (95 % CI)
HCY (per 1 SD) 1.20 (0.96–1.49)
Folate (per 1 SD) 1.01 (0.80–1.27)
B12 (per 1 SD) 1.05 (0.84–1.30)
Creatinine (per 1 SD) 1.26 (1.08–1.47)
Sex (male vs female) 2.10 (1.26–3.51)
Age (per 10 years) 0.92 (0.72–1.19)
A low SAM:SAH ratio was defined as the bottom 25th percentile of
SAM:SAH and top 25th percentile of SAH (16.8 % of subjects)
Mol Biol Rep (2012) 39:7805–7812 7809
123

Stabler and Allen [8] conducted bivariate analysis among a
healthy group of volunteers (n = 48; mean age 38.5). The
relationships between HCY, SAM and SAH reported in
these studies are inconsistent. Specifically, Becker et al.
[22] reported no correlations between HCY and SAH, and
HCY and SAM but a strong positive correlation between
SAM and SAH (r = 0.68; p \ 0.001). Yi et al. [23]
reported a stronger positive correlation between HCY and
SAH (r = 0.73; p \ 0.001) than the correlation observed
in our study but supported our finding of no association
between HCY and SAM; the bivariate relationship between
SAM and SAH was not reported. In bivariate analysis,
Loehrer et al. [24] reported no relationship between HCY,
SAM and SAH. Finally, Stabler and Allen [8] found a
moderate correlation between HCY and SAH (r = 0.29;
p = 0.047), no correlation between HCY and SAM and a
strong correlation between SAM and SAH (r = 0.50;
p \ 0.001).
Our finding of a positive correlation between HCY and
SAH was not unexpected since the hydrolysis of SAH to
HCY is a reversible reaction that favours the synthesis of
SAH; thus, any accumulation of HCY would be expected
to drive the reversal of the SAHH reaction and increase
SAH concentration [4]. However, evidence supports a
more facile transport of HCY across the plasma membrane
as compared to SAH. Therefore, concentration of plasma
HCY is almost threefold greater than SAH and correlation
between plasma levels of SAH and HCY is likely affected
by the dynamic balance between tissue and plasma con-
centrations [4]. The strong negative correlations between
HCY and folate, and HCY and vitamin B12 are consistent
with a large body of research, as both folate and vitamin
B12 play critical roles in the metabolism of HCY [24, 25].
Likewise, among a healthy population, the correlation
between creatinine and HCY has been consistently repor-
ted in the literature [26–33]. The lack of correlation found
between SAM and SAH in our study was unexpected, but
consistent with the finding reported by Loehrer et al. [24].
Finally, the correlations between creatinine, and SAM and
SAH in a healthy population have been investigated by
Stabler and Allen [8], serum creatinine was found to pos-
itively correlate with serum SAH but not SAM levels.
In multivariate analysis, the main findings of interest were
that: (1) there were no associations between HCY and SAM
and SAH levels; (2) lower serum folate and vitamin B12
levels, higher serum creatinine level, male sex and increasing
age were associated with higher HCY levels; (3) higher levels
of SAM were associated with increasing serum creatinine and
age and; (4) higher SAH levels were observed with increasing
serum creatinine levels and in males. Two studies that have
investigated similar determinants of HCY, SAM and SAH
were identified. In a study conducted by van Driel et al. [34]
among 336 healthy women (median age 32.7), only serum
folate and vitamin B12 were found as determinants of HCY
while serum creatinine and its associations with HCY, SAM
and SAH were not considered. Becker et al. [22] reported
similar findings where serum folate, serum creatinine and sex
were found to be determinants of HCY, and serum creatinine
and sex were determinants of SAH; no significant determi-
nants of SAM were found.
As SAM is the universal methyl donor for methylation
reactions and SAH is the product and inhibitor of meth-
yltransferase reactions, the ratio of SAM:SAH has been
suggested as a indicator of methylation capacity. However,
it has been reported that a decrease in SAM:SAH ratio was
predictive of methylation capacity only in the presence of a
high SAH value [4]. We defined a low SAM:SAH ratio as
those in the lowest quartile of SAM:SAH ratio and the
highest quartile of SAH. In this study, increasing serum
creatinine and male sex were found to be associated with a
low SAM:SAH ratio. Becker et al. [22] examined SAM:-
SAH as a continuous variable and also observed a rela-
tionship with serum creatinine and sex.
Limitations
The study population was aged 20–50, primarily Caucasian
and exposed to folic acid food fortification since 1998;
therefore generalizability to other age groups, ethnic pop-
ulations and unfortified populations may be limited. The
study was cross-sectional and included a one-time blood
draw for measurement of the relevant biomarkers. The
stability of these measures is therefore critical for mean-
ingful interpretation of the study results. HCY, SAM and
SAH concentrations in an individual are relatively constant
over at least 1 month [3, 35]. The CV for HCY, SAM, SAH,
folate, vitamin B12 and creatinine laboratory analyses
indicate a potential for random misclassification. Caution
was exercised to ensure that the samples were prepared in a
uniform manner between and within the three study centers.
In particular, prevention of any room temperature storage or
incubation at any time from phlebotomy to analysis was
strictly enforced as SAM is unstable and partially degrades
to SAH after relatively short intervals of room temperature
or 4 �C incubation [6, 16]. This degradation would have a
particular implication on the low SAM:SAH ratio variable.
Prior to analysis, all samples were stored at -80 �C and
shipped on dry ice to minimize degradation of SAM [14].
However, the potential for sample thawing in transit is a
possibility. Alternatively, stabilizing agents could have
been added for preservation; for example, plasma samples
are recommended to be acidified with acetic acid prior to
storage for SAM and SAH analysis and EDTA and ascorbic
acid are stabilizing agents for folate in blood [6, 36–38].
The use of a deuterium labelled SAH rather than SAM as an
internal standard for SAH analyses would have been ideal;
7810 Mol Biol Rep (2012) 39:7805–7812
123

however, at the time the samples were analyzed, deuterium
labelled SAH was not available. It is noteworthy that the
impact of the use of SAM as an internal standard for SAH
quantification may have biased the estimate of mean SAH
levels in our population, but is less likely to have biased
relative measures of SAH and therefore the analyses of the
interrelationships between SAM, SAH, HCY and relevant
dietary factors. Furthermore, our measure of folate status is
serum folate rather than red blood cell concentration. This
represents a potential limitation since serum folate tends to
represent short term folate and red blood cell concentrations
may be a better reflection of folate status over a longer
period of time [39]. It is also important to emphasize that
these biomarkers were measured in blood and that the
relationship between blood levels and critical target organs
has not been established and is likely complex; for instance,
the correlation between plasma concentrations of HCY and
SAH is likely influenced by tissue concentrations [4].
Finally, this study did not investigate whether HCY, SAM,
SAH or the ratio of SAM:SAH are valid markers of DNA
methylation and in the literature, it is not fully clarified
which of the moieties is most relevant to methylation.
Conclusion
This is the largest study to investigate the interrelationships
between markers of one-carbon metabolism among healthy
adults aged 20–50. The lack of strong correlations between
plasma HCY, SAM and SAH concentrations suggest that
HCY, SAM and SAH are relatively independent parame-
ters and therefore reflect different aspects of one-carbon
metabolism. However, it is noteworthy that serum creati-
nine levels correlated with those of plasma HCY, SAM and
HCY concentrations. These results do not support the use
of any single marker and illustrate the necessity to capture
each of these markers in risk factor research.
Acknowledgements The authors would like to thank the study
participants and study coordinator Gwyneth Fairfield. This research
was supported by an operating grant from the Canadian Institutes of
Health Research.
Conflict of interest No potential conflicts of interest to disclose.
References
1. Castro R, Rivera I, Struys EA, Jansen EE, Ravasco P, Camilo ME
et al (2003) Increased homocysteine and S-adenosylhomocysteine
concentrations and DNA hypomethylation in vascular disease.
Clin Chem 49(8):1292–1296
2. Mason JB (2003) Biomarkers of nutrient exposure and status in
one-carbon (methyl) metabolism. J Nutr 133(Suppl 3):941S–
947S
3. Poirier LA, Wise CK, Delongchamp RR, Sinha R (2001) Blood
determinations of S-adenosylmethionine, S-adenosylhomocys-
teine, and homocysteine: correlations with diet. Cancer Epi-
demiol Biomarkers Prev 10(6):649–655
4. James SJ, Melnyk S, Pogribna M, Pogribny IP, Caudill MA
(2002) Elevation in S-adenosylhomocysteine and DNA hy-
pomethylation: potential epigenetic mechanism for homocyste-
ine-related pathology. J Nutr 132(8 Suppl):2361S–2366S
5. Hobbs CA, Cleves MA, Melnyk S, Zhao W, James SJ (2005)
Congenital heart defects and abnormal maternal biomarkers of
methionine and homocysteine metabolism. Am J Clin Nutr
81(1):147–153
6. Gellekink H, van Oppenraaij-Emmerzaal D, van Rooij A, Struys
EA, den Heijer M, Blom HJ (2005) Stable-isotope dilution liquid
chromatography-electrospray injection tandem mass spectrome-
try method for fast, selective measurement of S-adenosylmethi-
onine and S-adenosylhomocysteine in plasma. Clin Chem
51(8):1487–1492. doi:10.1373/clinchem.2004.046995
7. Loehrer FM, Angst CP, Brunner FP, Haefeli WE, Fowler B
(1998) Evidence for disturbed S-adenosylmethionine : S-adeno-
sylhomocysteine ratio in patients with end-stage renal failure: a
cause for disturbed methylation reactions? Nephrol Dial Transpl
13(3):656–661
8. Stabler SP, Allen RH (2004) Quantification of serum and urinary
S-adenosylmethionine and S-adenosylhomocysteine by stable-
isotope-dilution liquid chromatography–mass spectrometry. Clin
Chem 50(2):365–372. doi:10.1373/clinchem.2003.026252
9. Jacobsen DW (2000) Biochemistry and metabolism. In: Robinson
K (ed) Homocysteine and vascular disease. Kluwer, Dordrecht,
pp 59–84
10. Selhub J (1999) Homocysteine metabolism. Annu Rev Nutr
19:217–246. doi:10.1146/annurev.nutr.19.1.217
11. Finkelstein JD (2001) Regulation of homocysteine metabolism.
In: Carmel R, Jacobsen DW (eds) Homocysteine in health and
disease. Cambridge University Press, Cambridge, pp 92–99
12. Alonso-Aperte E, Gonzalez MP, Poo-Prieto R, Varela-Moreiras
G (2008) Folate status and S-adenosylmethionine/S-adenosylho-
mocysteine ratio in colorectal adenocarcinoma in humans. Eur J
Clin Nutr 62(2):295–298. doi:10.1038/sj.ejcn.1602722
13. Kerins DM, Koury MJ, Capdevila A, Rana S, Wagner C (2001)
Plasma S-adenosylhomocysteine is a more sensitive indicator of
cardiovascular disease than plasma homocysteine. Am J Clin
Nutr 74(6):723–729
14. Wagner C, Koury MJ (2007) S-Adenosylhomocysteine: a better
indicator of vascular disease than homocysteine? Am J Clin Nutr
86(6):1581–1585
15. Blau N, Duran M, Gibson KM (2008) Laboratory guide to the
methods in biochemical genetics. Springer, Heidelberg,
pp 91–114
16. Struys EA, Jansen EE, de Meer K, Jakobs C (2000) Determina-
tion of S-adenosylmethionine and S-adenosylhomocysteine in
plasma and cerebrospinal fluid by stable-isotope dilution tandem
mass spectrometry. Clin Chem 46(10):1650–1656
17. Whelton A, Watson AJ, Rock RC (1994) Nitrogen metabolites
and renal function. In: Burtis CA, Ashwood ER (eds) Tietz
textbook of clinical chemistry, 2nd edn. WB Saunders, Phila-
delphia, pp 1513–1575
18. Zeller RA, Levin ZH (1974) The effects of violating the nor-
mality assumption underlying r. Sociol Method Res 2(511):
511–518. doi:10.1177/004912417400200406
19. Tao J, Yang M, Chen Z, Huang Y, Zhao Q, Xu J et al (2008)
Decreased DNA methyltransferase 3A and 3B mRNA expression
in peripheral blood mononuclear cells and increased plasma SAH
concentration in adult patients with idiopathic thrombocytopenic
purpura. J Clin Immunol 28(5):432–439. doi:10.1007/s10875-
008-9223-2
Mol Biol Rep (2012) 39:7805–7812 7811
123

20. Valli A, Carrero JJ, Qureshi AR, Garibotto G, Barany P, Axels-
son J et al (2008) Elevated serum levels of S-adenosylhomocys-
teine, but not homocysteine, are associated with cardiovascular
disease in stage 5 chronic kidney disease patients. Clin Chim
Acta 395(1–2):106–110. doi:10.1016/j.cca.2008.05.018
21. Kirsch SH, Knapp JP, Geisel J, Herrmann W, Obeid R (2009)
Simultaneous quantification of S-adenosyl methionine and
S-adenosyl homocysteine in human plasma by stable-isotope
dilution ultra performance liquid chromatography tandem mass
spectrometry. J Chromatogr B 877(30):3865–3870. doi:10.1016/
j.jchromb.2009.09.039
22. Becker A, Smulders YM, Teerlink T, Struys EA, de Meer K,
Kostense PJ et al (2003) S-Adenosylhomocysteine and the ratio
of S-adenosylmethionine to S-adenosylhomocysteine are not
related to folate, cobalamin and vitamin B6 concentrations. Eur J
Clin Invest 33(1):17–25
23. Yi P, Melnyk S, Pogribna M, Pogribny IP, Hine RJ, James SJ
(2000) Increase in plasma homocysteine associated with parallel
increases in plasma S-adenosylhomocysteine and lymphocyte
DNA hypomethylation. J Biol Chem 275(38):29318–29323. doi:
10.1074/jbc.M002725200
24. Loehrer FM, Tschopl M, Angst CP, Litynski P, Jager K, Fowler B
et al (2001) Disturbed ratio of erythrocyte and plasma S-adeno-
sylmethionine/S-adenosylhomocysteine in peripheral arterial
occlusive disease. Atherosclerosis 154(1):147–154
25. Refsum H, Nurk E, Smith AD, Ueland PM, Gjesdal CG, Bjelland
I et al (2006) The Hordaland homocysteine study: a community-
based study of homocysteine, its determinants, and associations
with disease. J Nutr 136(6 Suppl):1731S–1740S
26. Ueland PM, Refsum H, Schneede J (2000) Determinants of
plasma homocysteine. In: Robinson K (ed) Homocysteine and
vascular disease. Kluwer, Dordrecht, pp 59–84
27. Vrentzos GE, Papadakis JA, Malliaraki N, Bampalis DE, Repa A,
Lemonomichelaki V, Petinellis EG, Ganotakis ES (2006) Serum
homocysteine concentration as a marker of nutritional status of
healthy subjects in Crete, Greece. J Hum Nutr Dietet 19:117–123
28. Krivosıkova Z, Krajcovicova-Kudlackova M, Spustova V,
Stefıkova K, Valachovicova M, Blazıcek P, Nemcova T (2010)
The association between high plasma homocysteine levels and
lower bone mineral density in Slovak women: the impact of
vegetarian diet. Eur J Nutr 49:147–153. doi:10.1007/s00394-
009-0059-1
29. Rauh M, Verwied S, Knerr I, Dorr HG, Sonnichsen A, Koletzko
B (2001) Homocysteine concentrations in a German cohort of
500 individuals: reference ranges and determinants of plasma
levels in healthy children and their parents. Amino Acids 20:
409–418. doi:10.1007/s007260170037
30. Bjorkegren K, Svardsudd K (2001) Serum cobalamin, folate,
methylmalonic acid and total homocysteine as vitamin B12 and
folate tissue deficiency markers amongst elderly Swedes—a
population-based study. J Intern Med 249:423–432. doi:10.1046/
j.1365-2796.2001.00819.x
31. Herrmann W, Quast S, Ullrich M, Schultze H, Bodis M, Geisel J
(1999) Hyperhomocysteinemia in high-aged subjects: relation of
B-vitamins, folic acid, renal function and the methylenetetrahy-
drofolate reductase mutation. Atherosclerosis 144(1):91–101.
doi:10.1016/S0021-9150(99)00036-2
32. Marouf R, Mohammad Z, Olusegun MA, Mohammad Q, Nabila
AA, Hanan WA, Salah HA (2006) Determinants of plasma
homocysteine in relation to hematological and biochemical
variables in patients with acute myocardial infarction. South Med
J 99(8):811–816. doi:10.1097/01.smj.0000231245.44439.47
33. Jacques PF, Rosenberg IH, Rogers G, Selhub J, Bowman BA,
Gunter EW, Wright JD, Johnson CL (1999) Serum total homo-
cysteine concentrations in adolescent and adult Americans:
results from the third National Health and Nutrition Examination
Survey. Am J Clin Nutr 69(3):482–489
34. van Driel LM, Eijkemans MJ, de Jonge R, de Vries JH, van
Meurs JB, Steegers EA et al (2009) Body mass index is an
important determinant of methylation biomarkers in women of
reproductive ages. J Nutr 139(12):2315–2321. doi:10.3945/jn.
109.109710
35. Garg UC, Zheng ZJ, Folsom AR, Moyer YS, Tsai MY,
McGovern P et al (1997) Short-term and long-term variability of
plasma homocysteine measurement. Clin Chem 43(1):141–145
36. Elloitt P, Peakman TC (2008) The UK Biobank sample handling
and storage protocol for the collection, processing and archiving
of human blood and urine. Int J Epidemiol 37(2):234–244. doi:
10.1093/ije/dym276
37. Holland NT, Smith MT, Eskenazi B, Bastaki M (2003) Biological
sample collection and processing for molecular epidemiological
studies. Mutat Res 543(3):217–234. doi:10.1016/S1383-5742(02)
00090-X
38. Kerkay J, Coburn CM, McEvoy D (1977) Effect of sodium
ascorbate concentration on the stability of samples for determi-
nation of serum folate levels. Am J Clin Pathol 68:481–484
39. Herbet V (1998) Folic acid. In: Shils M, Olson JA, Shike M, Ross
AC (eds) Modern nutrition in health and disease, 9th edn. Lip-
pincott Williams & Wilkins, Baltimore, pp 443–446
7812 Mol Biol Rep (2012) 39:7805–7812
123