Embed Size (px)
Citation preview

Thorax 1995;50:869-874
Relation of bronchoalveolar lavageT lymphocyte subpopulations to rate ofregression of active pulmonary tuberculosis
C-T Yu, C-H Wang, T-J Huang, H-C Lin, H-P Kuo
Departnentof Thoracic Medicine,Chang Gung MemorialHospital, Taipei,TaiwanC-T YuC-H WangT-J HuangH-C LinH-P Kuo
Reprint requests to:Dr Han-Pin Kuo.Received 29 July 1994Returned to authors12 December 1994Revised version received14 February 1995Accepted for publication24 April 1995
AbstractBackground - Effective host defenceagainst mycobacterial infection chiefly de-pends on the interactions between macro-phages and T lymphocytes. This studyinvestigated the relation of cellular com-ponents and their activity of cells obtainedby bronchoalveolar lavage (BAL) from thelower respiratory tract to disease re-gression in patients with active pulmonarytuberculosis without HIV infection.Methods - Clinical indices including age,sex, the presence of diabetes, fever, thepresence of resistant strains of myco-bacteria, the bacterial load in sputum,and disease extent on chest radiographyat presentation were assessed before com-mencing four-drug antituberculous ther-apy. Twenty two patients with activepulmonary tuberculosis were divided intorapid, intermediate, and slow regressiongroups. Subpopulations ofalveolarmacro-phages separated using discontinuousPercoll density gradient centrifugationand T lymphocytes (with CD3, CD4, CD8,and CD25 monoclonal antibodies) werequantified.Results - There were no differences amongrapid, intermediate, and slow regressiongroups in terms of age, sex, the presenceof diabetes, the presence of resistantstrains of mycobacteria, or the bacterialload in sputum. No differences were foundbetween the groups in terms of sub-populations of alveolar macrophages ornumbers of CD3 and CD4 lymphocytes.By contrast, an increase in CD8 cells wasshown in the slow regression group com-pared with the rapid and intermediate re-gression groups. CD25 cell numbers wereincreased in the rapid regression groupcompared with the slow regression group.The CD4/CD8 ratio was decreased in theslow regression group compared with therapid and intermediate regression groupsand the relation between the proportion ofCD25 cells and the CD4/CD8 ratio in BALfluid was significant.Conclusions -A decreased CD4/CD8 ratiowith an increase in CD8 cells in the al-veolar spaces was associated with slow dis-ease regression in patients with activepulmonary tuberculosis without HIV in-fection, suggesting that the balance of Tlymphocyte subsets mayplay a central part
in the modulation of host defence againstmycobacterial infection.(Thorax 1995;50:869-874)
Keywords: pulmonary tuberculosis, bronchoalveolarlavage, alveolar macrophage, T lymphocyte sub-populations.
Tuberculosis remains the leading cause ofdeathin the world and accounts for 6 7% of alldeaths in the developing world.' Cell-mediatedimmunity plays a critical part in eliminatingmycobacteria. It is believed that mycobacteriainhaled into the airways are phagocytosedby alveolar macrophages and then processedfor antigen presentation to T lymphocytes;lymphokines released from activated lym-phocytes may prime macrophages to inhibitmycobacterial replication within macro-phages.2A Host defence against mycobacteriatherefore chiefly depends on the interactionsbetween macrophages and T lymphocytes foreffective control ofinfection. More than 95% ofindividuals affected by pulmonary tuberculosiscan be cured with various antituberculousdrugs introduced in recent years. However, thepattern ofresolution ofpulmonary tuberculosisdiffers between patients, suggesting that in-dividual variations in cellular immunity againstmycobacterial invasion may be an importantfactor in determining the rate of mycobacterialeradication. This is especially the case inpatients with pulmonary tuberculosis and HIVinfection.5
Short six month courses of antituberculouschemotherapy are now widely used throughoutthe world, and it is possible that certain in-dividuals might require more intensive treat-ment. However, there are no data to indicate forwhom this more protracted treatment should beconsidered. Since host defence against myco-bacterial invasion occurs within broncho-alveolar spaces, bronchoalveolar lavage (BAL)could provide a valuable insight into the mag-nitude of the individual cellular immune re-sponse which may be an important determinantof the prognosis and this may lead to a betterapproach to treatment of active pulmonarytuberculosis.
Recent reports have investigated peripheralblood and pleural fluid,"'0 but less is knownof BAL cells. We have therefore evaluated therelationship of BAL cells recovered from thelower respiratory tract and their activity statuswith clinical indices in patients with active
869
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from

Yu, Wang, Huang, Lin, Kuo
pulmonary tuberculosis without HIV infectionbefore or within one week of antituberculoustreatment.
MethodsSTUDY POPULATIONTwenty two patients with active pulmonarytuberculosis (15 men and seven women, in-cluding 13 diabetics) with a mean (SE) age of47-7 (3 6) years were enrolled in this study. Allwere negative for HIV infection. The nu-tritional status of each patient was assessed,including measurement of body mass, height,triceps skinfold thickness, mid arm circum-ference, and serum albumin level. Patients inpoor nutritional status (body mass <90th per-centile or mid arm circumference and tricepsskin fold thickness <25th percentile) wereexcluded. None of the patients was takingcorticosteroids or other immunosuppressantmedication.
CLINICAL INDICESClinical indices including age, sex, the presenceof diabetes, fever, the presence of resistantstrains of mycobacteria, the bacterial load inthe sputum, and disease extent on chest radio-graphy at presentation were assessed. Feverwas defined as an initial presentation with atemperature of >37 5°C, persisting for morethan five days, which subsided on starting anti-tuberculous therapy, together with the ex-clusion of common bacterial or viral infection.
SPUTUM ASSESSMENTThe patients were encouraged to cough deeplyto expectorate a specimen of lower respiratorytract secretions suitable for microscopic ex-amination and culture. If contaminated salivaor large oropharyngeal squamous cells werepredominant, the aliquot was discarded. Thebronchopulmonary origin of the specimen wasassured if it contained mucous strands in whichinflammatory polymorphonuclear cells, mono-cytes, macrophages, and bronchial epithelialcells were embedded. In all patients early morn-ing sputum collected freshly on three differentdays was centrifuged and the sediment wasstained for acid fast bacilli by the auraminefluorochrome procedure after an examinationto assure its bronchopulmonary origin. Bac-terial numbers were determined by counting30 fields under oil immersion and were gradedby an independent experienced technician intofour categories: (0) absence of bacilli; (1) 1-9bacilli; (2) 10-29 bacilli; and (3) >30 bacilli per30 oil-immersed fields. The bacterial gradingsfrom specimens collected on three days weretotalled and presented as an index of sputumbacterial load. In all patients at least one spu-tum specimen was positive for acid fast bacillion microscopic examination and grew Myco-bacterium tuberculosis. Sputum conversion wasassessed in the first 3-6 months and, oc-casionally, up to 9-12 months if a sputumsample was available. The presence of resistantstrains was recorded according to the final
culture results. Multidrug-resistant strains aredefined here as M tuberculosis resistant toisoniazid and rifampicin, with or withoutresistance to other drugs, as previouslydescribed."
GRADING OF DISEASE EXTENT ON CHESTRADIOGRAPHYPosteroanterior chest radiographs were takenof all patients at the time of hospital admissionand every three months thereafter for at leastnine months. A grading of the extent of diseaseproposed by the World Health Organisation(1960) was adopted to assess the severity ofdisease at presentation'2: 0=no involvement;1 = trivial; 2 = slight; 3 = limited; 4 = moderate;5= extensive; and 6= gross.
PATIENT GROUPINGThe study population was allocated to one ofthree groups according to the resolution ofpulmonary lesions: (1) rapid regression group(RR) showing more than 50% improvement inthe extent of disease on chest radiographywithin three months ofcommencing treatment,and either complete resolution within ninemonths of treatment or residual fibrotic lesionswhich were unchanged for at least three monthsafter cessation of treatment; (2) intermediateregression group (IR) showing 50% im-provement in the extent of disease on chestradiography after 3-6 months oftreatment, andeither complete resolution within nine monthsof treatment or residual fibrotic lesions whichwere unchanged for at least three months aftercessation of treatment; and (3) slow regressiongroup (SR) showing less than 50% im-provement in the extent of disease on chestradiography after six months of treatment, andeither persistent active pulmonary lesions orincomplete resolution within nine months oftreatment. To avoid observer bias the radio-graphs were initially assessed independentlyby two pulmonary physicians who were notaware of the laboratory results or clinical pre-sentations, and they arrived at the same gradingfor 19 of 22 patients. Two patients were as-sessed IR by one observer and RR by the other;one patient was assessed RR by one observerand IRby the other. After discussion, consensusagreement was reached for the groupings forthese three patients. Assessment throughoutthe study was also performed blind.
ANTITUBERCULOUS TREATMENTAll 22 patients received four-drug anti-tuberculous chemotherapy including isoniazid(5 mg/kg/day), rifampicin (10 mg/kg/day) andethambutol (20 mg/kg/day) for at least ninemonths, as well as pyrazinamide (25 mg/kg/day) for the initial two months of treatment.All patients took medication regularly withoutinterruption.
PREPARATION OF BAL CELLSBAL was performed before or within one weekof antituberculous treatment using five aliquots
870
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from
Regression ofpulmonary tuberculosis and T lymphocyte subpopulations
(50 ml each) of 0 9% saline solution as de-scribed previously.'3 Briefly, sterile prewarmed(37°C) saline solution was introduced into theinvolved segment(s). The lavage fluid was thenrecovered by gentle aspiration and pooled andfiltered through two layers of sterile gauze. Thetotal cell count was evaluated on an aliquotof the pooled fluid using a haemocytometer.Differential cell counts were determinedfrom cytocentrifuge preparations with modifiedWright-Giemsa staining. The remaining fluidwas centrifuged at 600 g for 20 minutes at 4°C.The cell pellet was then washed sequentiallyand resuspended in RPMI-1640 (Flow Labora-tories, Paisley, UK) at 106 cells/ml. Informedconsent for bronchoscopy was obtained fromall patients.
DENSITY FRACTIONATION OF ALVEOLARMACROPHAGESAlveolar macrophages were separated usingdiscontinuous Percoll (Pharmacia Fine Chem-icals, Uppsala, Sweden) density gradient cent-rifugation as previously described.'4 IsosmoticPercoll was prepared by mixing stock Percollwith 9% saline solution at ratios calculated toproduce working Percoll of specific gravities1 030, 1 040, 1 050, and 1 070 g/ml. Specificgravities were checked with a refractometerbefore centrifugation. The alveolar macro-phages (5 x 106 in 5 ml RPMI-1640) werelayered onto the top Percoll layer in a centrifugetube containing 5 ml aliquots ofthe four Percollsolutions (least dense to most dense, top tobottom) and then centrifuged for 20 minutesat 400 g at 20°C. The cells that localised ateach fractional interface were collected andnamed for the density upon which it floated.Total and differential cell counts were madefrom each layer. Proportional recovery of agiven interface was defined as the number ofcells recovered from the gradient expressed asa ratio of total cells recovered so that the sumof cells recovered totalled 1-0. All fractionscomprised >95% alveolar macrophages andviability was determined by trypan blue dyeexclusion. More than 90% ofthe cells recoveredfrom the column after centrifugation werefound in five fractions, with the remainderof the cells (lymphocytes, granulocytes, andeosinophils) being located in the pellet withspecific gravity greater than the densest Percoll
Table 1 Demographic data at presentation in three groups ofpatients with activepulmonary tuberculosis
Rapid Intermediate Slowregression regression regression(n = 8) (n = 9) (n = 5)
Mean (SE) age (years) 43-6 ( 6 5) 52-0 ( 5-6) 46-4 (7 4)Sex (M:F) 6:2 5:4 4:1Diabetics 5 5 3Presence of drug-resistant tuberculosis:no resistant strain 5 6 1resistant to ethambutol 0 0 2resistant to isoniazid 1 1 2resistant to isoniazid and streptomycin 2 1 0resistant to isoniazid and rifampicin 0 1 0
Fever (% of patients) 5 (62 5%) 4 (44 4%) 0* (0%)Sputum bacterial load 5-3 ( 1-1) 3-7 ( 0 9) 2-6 ( 0 8)Profusion score on chest radiograph 5-0 ( 0 3) 4 0 ( 0 4) 3-6 ( 0 3)**
* p<0 05, ** p<0 02 compared with rapid regression group.
fraction used. Hypodense subpopulations weredefined as cells with a specific gravity of<1 040 g/ml.
T LYMPHOCYTE SUBPOPULATIONST lymphocyte subpopulations were identifiedas CD3, CD4, CD8 or CD25 using mono-clonal antibodies anti-Leu-4/CD3 FITC, anti-Leu-3a/CD4 FITC, anti-Leu-2a/CD8PE oranti-IL-2R-anti-Tac, respectively (BecktonDickinson) and assayed by fluorescence-activated flow cytometry with a fluorescence-activated cell sorter (FACStar) (BecktonDickinson).
STATISTICAL ANALYSISResults are expressed as means (SE). Statisticalanalysis of results was performed by the twotailed Student's t test for unpaired data. Fordata not normally distributed the Mann-Whit-ney U test was used. One-way analysis of vari-ance followed by Bonferroni corrected t test orKruskal-Wallis statistical analysis was per-formed when multiple comparisons were made.The relation between clinical indices, suchas the disease extent on chest radiography orbacterial load in sputum, and T lymphocytesubpopulations in BAL fluid was sought bymultiple regression analysis, then Spearman'srank correlation test or linear regression ana-lysis was applied to examine the significance ofcorrelations between groups. X2 analysis wasused for nominal data comparisons betweentwo or three groups. A p value of <0 05 wasconsidered significant.
ResultsCLINICAL INDICESTable 1 shows the clinical features of patientsin the RR, IR, and SR groups. There were nosignificant differences among these groups interms of age, sex, the presence of diabetes, thepresence of resistant strains of M tuberculosis,or the bacterial load in the sputum. Patientsin the RR group (62 5%) had fever at initialpresentation compared with none of the five inSR group (p<005). Although more patients inthe IR group (n= 4) were febrile than in the SRgroup, this did not reach statistical significance.The disease extent on chest radiography atinitial presentation was significantly lower inthe SR group (mean (SE) 3-6 (0 3)) than inthe RR group (5 0 (0 3), p<0.02), but notsignificantly different from the IR group (4 0(0 4)).
ALVEOLAR MACROPHAGE AND T LYMPHOCYTESUBPOPULATIONSTable 2 shows total cell numbers and sub-populations recovered by BAL in the threestudy groups. Total cell numbers and per-centages ofmacrophages and lymphocytes werenot significantly different among the groups,and there were no differences in proportions ofalveolar macrophage subpopulations separated
871
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from
Yu, Wang, Huang, Lin, Kuo
Table 2 Mean (SE) total cell numbers and percentages of macrophage and Tlymphocyte subpopulations recovered from BAL fluid ofpatients with active pulmonarytuberculosis
Rapid Intertnediate Slowregression regression regression(n = 8) (n= 9) (n= 5)
Alveolar macrophagestotal cell number ( x I04 cells/ml) 3-6 (0-4) 3-5 (0-3) 3-1 (0 5)proportion of hypodense 35-0 (5-0)% 35-7 (6-4)% 30-2 (7-5)%subpopulations (<1-040 g/ml)
T lymphocytestotal cell number (x 10' cells/ml) 4-3 (0-5) 4-1 (0-3) 3-7 (0-4)absolute numbers (x 10' cells/ml) andproportion of subpopulationsCD3 cells 3-6 (0-6) 3-4 (0-4) 3-4 (0-4)
81-3 (7-5)% 82-0 (5-2)% 90-8 (2-4)%CD4 cells 2-7 (0-5) 2-2 (0-3) 2-0 (0-2)
60-5 (6-9)% 53-1 (5-2)% 52-4 (2-1)%CD8 cells 1-0 (0-1)* 1-0 (0-2)t 1-5 (0-3)
21-5 (3.2)%* 23-8 (3-1)%t 40-4 (5-4)%CD25 cells 0-5 (0 1)* 0-4 (0-1) 0-2 (0-1)
10-8 (0Q9)%* 8-9 (0-9)% 6-0 (0-9)%CD4/CD8 ratio 3-2 (0.4)** 2-5 (0-3)-f 1-4 (0-3)
* p<O-Ol, ** p<002 compared witi slow regression group.t p<002, tt p<O-05 compared with slow regression group.
by density gradient or total and percentage ofCD3 and CD4 T cells.The five patients in the SR group had sig-
nificantly higher percentages and total numbersofCD8 cells (40-4% (5-4%) and 1-5 (0-3) x 103cells/ml, respectively) than the eight patients inthe RR group (21-5% (3-2%) and 1-0(0-1) x 103 cells/ml, respectively; p<0-01) andthe nine patients in the IRgroup (23-8% (3-1 %)and 1-0 (0-2) x 103 cells/ml, respectively;p<0-02). Patients in the RR group had a sig-nificantly higher proportion and total cell num-ber of CD25 cells (10-8% (0-9%) and 0-5(0-1) X 103 cells/ml, respectively) than those inthe SR group (6-0% (0-9%) and 0-2 (0- 1) x 103cells/ml, respectively; p<0- 01), but not thosein IR group (8-9% (0-9%) and 0-4 (0 1) x 103cells/ml). There was no difference in CD25cell numbers between the IR and SR groups.The CD4/CD8 ratio was significantly lower inthe SR group (1-4 (0 3)) than(3-2 (0-4); p<0 02) and the IRp<005), but there was no dithe RR and IR groups.
5
4
0
0.
oo00In
04
3
2
1
0
r= 076,p<0-01
_ 0
* *00
0
I
0 5CD25 cells (% of ti
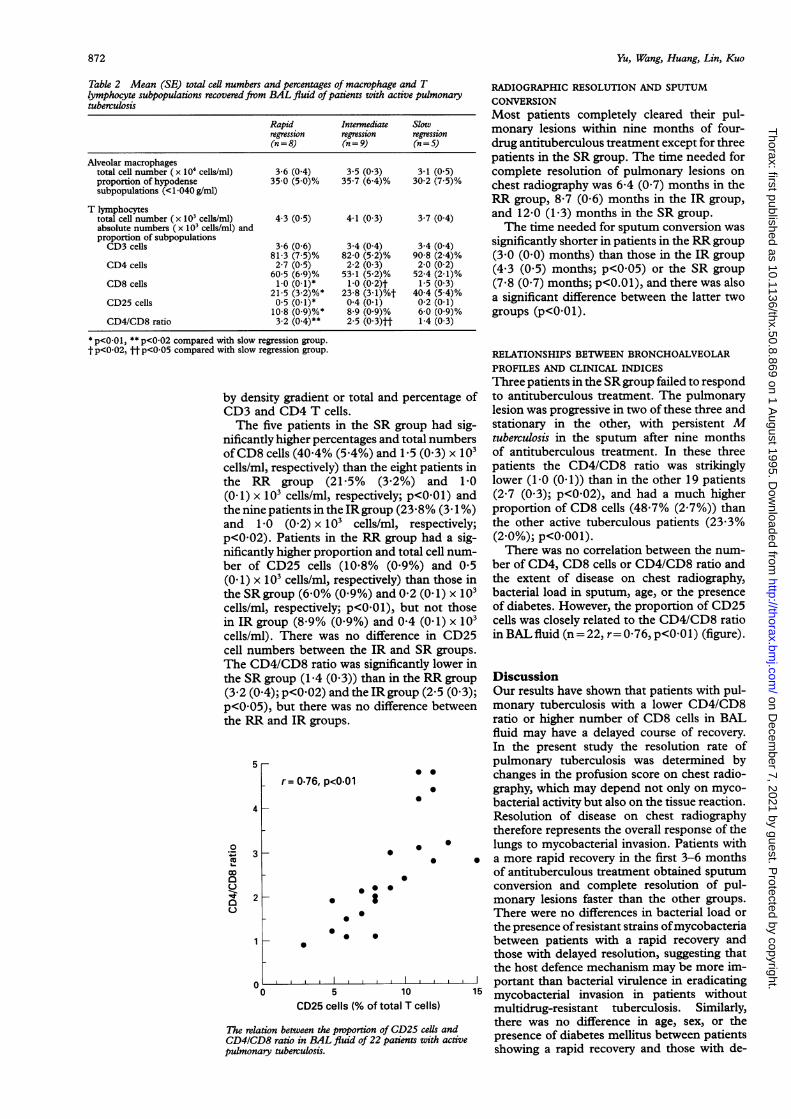
The relation between the proportion oCD4/CD8 ratio in BAL fluid of 22pulmonary tuberculosis.
RADIOGRAPHIC RESOLUTION AND SPUTUMCONVERSIONMost patients completely cleared their pul-monary lesions within nine months of four-drug antituberculous treatment except for threepatients in the SR group. The time needed forcomplete resolution of pulmonary lesions onchest radiography was 6-4 (0.7) months in theRR group, 8-7 (0-6) months in the IR group,and 12-0 (1-3) months in the SR group.The time needed for sputum conversion was
significantly shorter in patients in the RR group(3-0 (0-0) months) than those in the IR group(4-3 (0-5) months; p<0 05) or the SR group(7-8 (0-7) months; p<0.01), and there was alsoa significant difference between the latter twogroups (p<0-01).
RELATIONSHIPS BETWEEN BRONCHOALVEOLARPROFILES AND CLINICAL INDICESThree patients in the SR group failed to respondto antituberculous treatment. The pulmonarylesion was progressive in two of these three andstationary in the other, with persistent Mtuberculosis in the sputum after nine monthsof antituberculous treatment. In these threepatients the CD4/CD8 ratio was strikinglylower (1-0 (0-1)) than in the other 19 patients(2-7 (0-3); p<0-02), and had a much higherproportion of CD8 cells (48-7% (2-7%)) thanthe other active tuberculous patients (23-3%(2-0%); p<0-001).There was no correlation between the num-
ber of CD4, CD8 cells or CD4/CD8 ratio andthe extent of disease on chest radiography,bacterial load in sputum, age, or the presenceof diabetes. However, the proportion of CD25cells was closely related to the CD4/CD8 ratioin BAL fluid (n= 22, r= 0-76, p<001) (figure).
in the RR group Discussion.group (2-5 (0-3); Our results have shown that patients with pul-ifference between monary tuberculosis with a lower CD4/CD8
ratio or higher number of CD8 cells in BALfluid may have a delayed course of recovery.In the present study the resolution rate ofpulmonary tuberculosis was determined by
* 0 changes in the profusion score on chest radio-* graphy, which may depend not only on myco-
* bacterial activity but also on the tissue reaction.Resolution of disease on chest radiographytherefore represents the overall response of the
i * lungs to mycobacterial invasion. Patients with* i i a more rapid recovery in the first 3-6 months
of antituberculous treatment obtained sputum* conversion and complete resolution of pul-
monary lesions faster than the other groups.There were no differences in bacterial load orthe presence ofresistant strains ofmycobacteriabetween patients with a rapid recovery andthose with delayed resolution, suggesting thatthe host defence mechanism may be more im-
I portant than bacterial virulence in eradicating10 15 mycobacterial invasion in patients without
otal T cells) multidrug-resistant tuberculosis. Similarly,
)f CD25 cells and there was no difference in age, sex, or thepatients with active presence of diabetes mellitus between patients
showing a rapid recovery and those with de-
872
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from
Regression ofpulmonary tuberculosis and T lymphocyte subpopulations
layed resolution, indicating that these factorsdid not contribute to the recovery rate frompulmonary tuberculosis.Host defence against mycobacteria depends
chiefly on the interactions between macro-phages and T lymphocytes. The macrophageis the effector cell in eradicating mycobacteriaand is dependent on interactions with activatedT lymphocytes.The proportion of hypodense alveolar
macrophages, an index of macrophage ac-tivation,'4 is increased in patients with activepulmonary tuberculosis.'5 In the present studywe failed to identify any relation between totalcell number or the subpopulations of alveolarmacrophages defined by density and recoveryrate from active pulmonary tuberculosis. Theincrease in the proportions of hypodense al-veolar macrophages in our previous report'5and here may therefore represent a local re-sponse of macrophages to mycobacterial in-vasion without reflecting significant differencesin prognosis.T lymphocytes also play a central part in the
cell-mediated immune defence against Mtuberculosis. Cytokines such as IL-2 or gammainterferon released from CD4 cells may activatemacrophages to ingest and kill mycobacteriamore effectively6"16 ' and to prime macrophagesfor massive release of tumour necrosis factorafter ingestion ofmycobacteria. 1 Some ofthesecytokines secreted in tuberculosis are endo-genous pyrogens'9 that may induce fever. Inthe present study patients with a delayed orslow recovery were less febrile, which mightsuggest lower cytokine production that couldreflect impaired interaction between T lym-phocytes and macrophages. Suppressive lym-phocytes have been identified in humantuberculous infections.202' The CD8 cell popu-lation may also represent functionally sup-pressive lymphocytes which downregulate theproliferation of CD4 cells and suppress theantimycobacterial action of macrophages.22This could cause less tissue damage but at theexpense of delaying clearance of the or-ganisms.22 An inverse relation between the re-covery rate of miliary tuberculosis and CD8cells in BAL fluid has been reported pre-viously.22 Consistent with this, in our study theproportion as well as the total cell number ofCD8 cells was significantly inversely relatedto the recovery rate with a predominance ofCD8 cells seen in the SR group comparedwith the IR and RR groups. When CD8 cellscomprised >40% of the total T lymphocytenumbers the time required for 50% im-provement in disease extent was more than sixmonths and complete resolution exceeded ninemonths. It is possible that tuberculosis as-sociated with a higher proportion of CD8 cellsin BAL fluid results in a less efficient hostdefence response, possibly due to down-regulation of CD4 T cell and macrophage ac-tivity, leading to delayed resolution of disease.The mechanism responsible for the increase
in CD8 cells is unclear. An increase in CD8cells with a reduced CD4/CD8 ratio hasbeen reported in advanced or disseminatedtuberculosis.68102223 A large bacterial load was
reported to shift the T cell activation towardsa predominance of CD8 cells. However, in thepresent study the disease extent (in terms ofchest radiographic abnormality or bacterialload in sputum) was not related to numbers ofCD4 or CD8 cells in BAL fluid.
Activated T lymphocytes may express IL-2receptors on their cell membrane - that is,CD25 positive cells. A lower proportion ofCD25 positive cells in patients with a lowerCD4/CD8 ratio implies that T lymphocytes inthose patients are less activated than in patientswith a higher CD4/CD8 ratio. A significantincrease in CD25 cells was found in patientswith a rapid resolution of pulmonary tuber-culosis compared with those with delayedresolution. The rate of recovery of activepulmonary tuberculosis therefore depends notonly on the fine balance between CD4 andCD8 cells, but also the T lymphocyte activationstatus.
Recovery from tuberculosis, assessed by im-provement in disease extent on chest radio-graphy, therefore depends upon the hostresponse to mycobacterial invasion, and thisresponse may be more critical than bacterialvirulence or load in determining the efficiencyof mycobacterial eradication. A decrease inthe CD4/CD8 ratio with an increase in theproportion and total number of CD8 cells inthe alveolar spaces can be a predictor for diseaseresolution in patients with active pulmonarytuberculosis.
1 Murray CJL, Styblo K, Rouillon A. In: Jamison DT, MosleyWH, eds. Disease control priorities in developing countries.New York: Oxford University Press for the World Bank,1992:50.
2 Unanue ER, Allen PM. The basis for the immunoregulatoryrole of macrophages and other accessory cells. Science1987;236:551-2.
3 Takemura R, Weib Z. Secretory products of macrophagesand their physiological functions. Am J Physiol 1984;246:1_9.
4 Rook GAW, Champion BR, Steel J, Varey AM, Stanford JL.I-A restricted activation byT cell lines of anti-tuberculosisactivity in murine macrophages. Clin Exp Immunol 1985;59:414-20.
5 Jones BE, Young SMM, Antoniskis D, Davidson PT,Kramer F, Barnes PF. Relationship of the manifestationsof tuberculosis to CD4 cell counts in patients with humanimmunodeficiency virus infection. Am Rev RespirDis 1993;14:1291-7.
6 Shiratsuchi H, Tsuyaguchi I. Analysis of T cell subsets bymonoclonal antibodies in patients with tuberculosis afterin vitro stimulation with purified protein derivative oftuberculin. Clin Exp Immunol 1984;57:271-8.
7 Simon MR, Desai SG, Jennings J, Engel D. T cell differ-entiation antigens and antigenic lymphocyte reactivity inpleural effusion. Asian Pac J Allergy Immunol 1986;4:19-27.
8 Bhatnagar R, Malaviya A, Narayanan S, Raigopalan P,Kumar R, Bharadwaj OP. Spectrum of immune responseabnormalities in different clinical forms of tuberculosis.Am Rev Respir Dis 1977;115:207-12.
9 Ellner JJ. Pleural fluid and peripheral blood lymphocytefunction in tuberculosis. Ann Intern Med 1978;89:932-3.
10 Swanson Beck J, Potts RC, Kardjito T, Grange JM. T4lymphopenia in patients with active pulmonary tuber-culosis. Clin Exp Immunol 1985;60:49-54.
11 Iseman MD. Treatment of multidrug-resistant tuberculosis.N EnglJ Med 1993;329:784-91.
12 Simon G. Radiology in epidemiological studies and sometherapeutic trials. BMJ 1966;2:491-4.
13 Godard P, Chantreuil J, Damon M, Coupe M, Flandre 0,Crastes de Paulet A, et al. Functional assessment of al-veolar macrophages: comparison of cells from asthmaticsand normal subjects. J Allergy Clin Immunol 1982;70:88-93.
14 Chanez P, Bousquet J, Couret I, Cornillac L, Barneon G,Vic P, et al. Increased numbers of hypodense alveolarmacrophages in patients with bronchial asthma. Am RevRespirDis 1991;144:923-30.
15 Kuo H-P, Yu C-T. Alveolar macrophage subpopulations inpatients with active pulmonary tuberculosis. Chest 1993;104:1773-8.
873
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from

Yu, Wang, Huang, Lin, Kuo
16 Edwards D, Kirkpatrick CH. The immunology of myco-bacterial diseases. Am Rev Respir Dis 1986;134:1062-71.
17 Kaufmann SHE. In vitro analysis ofthe cellular mechanismsinvolved in immunity to tuberculosis. Rev Infect Dis 1989;11:S448-54.
18 Rook GAW, Taverne J, Leveton C, Steele J. The role ofgamma-interferon, vitamin D3 metabolites and tumornecrosis factor in the pathogenesis of tuberculosis. Im-munology 1987;62:229-34.
19 Dinarello CA, Wolff SM. Pathogenesis of fever. In: MandellGL, Douglas RG Jr., Bennett JE, eds. Principles andpracticeof infectious diseases. New York: Churchill Livingstone,1990:462-7.
20 Tsuyuguchi I, Shiratsuchi H, Teraoka 0, Hirano T. Increasein T cells bearing IgG Fc receptors in peripheral blood ofpatients with tuberculosis by in vitro stimulation with
purified protein derivative. Am Rev Respir Dis 1980;121:951-7.
21 Katz P, Goldstein RA, Fauci AS. Immunoregulation ininfection caused by Mycobacterium tuberculosis: the pres-ence of suppressor monocytes and alteration of sub-populations of T lymphocytes. Infect Dis 1979;140:12-21.
22 Ainslie GM, Solomon JA, Bateman ED. Lymphocyte andlymphocyte subset numbers in blood and in broncho-alveolar lavage and pleural fluid in various forms ofhumanpulmonary tuberculosis at presentation and during re-covery. Thorax 1992;47:513-8.
23 Singhal M, Banavalikar JN, Sharma S, Saha K. PeripheralbloodT lymphocyte subpopulations in patients with tuber-culosis and the effect of chemotherapy. Tubercle 1989;70:171-8.
874
on Decem
ber 7, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.8.869 on 1 August 1995. D
ownloaded from





























