Embed Size (px)
Citation preview

1180
Public Health
RELATION BETWEEN VACCINATION ANDNOTIFICATION RATES FOR WHOOPINGCOUGH IN ENGLAND AND WALES
RICHARD POLLARD
Epidemiological Research Laboratory, Central Public HealthLaboratory, Colindale Avenue, London NW9 5HT
Summary The number of notified cases of whoop-ing cough in the 1977-79 outbreak in
England and Wales was the largest for over 20 years.The percentage of children receiving pertussis vaccinehas declined sharply since 1974. Area Health Authoritieswith low vaccination acceptance had notification-rates60% above those with higher acceptance. There was apartial correlation coefficient of -0.57 (p<0.001) bet-ween vaccination and notification rates after eliminationof the effects of social class and overcrowding. The 1-4year age-group, which contained the children most affec-ted by the decline in vaccination-rates, showed a muchbigger increase in notifications than other age-groups.The evidence suggests a direct relation between thedecline in vaccination-rate and the increase innotifications.
INTRODUCTION
In recent years the percentage of children vaccinated
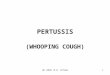
against whooping cough in England and Wales has fallensharply. From 1958 to 1974 approximately 73% ofchildren were fully immunised by the age of 2 years; by1978 the figure had declined to 30%. Whooping-coughnotifications began to increase in the late summer of1977, and the number of notifications in England andWales during the next 2 years was the largest since 1956-57 (fig. 1).The main features of the 1977-79 outbreak and the
relation between the falling vaccination-rate and theincrease in notifications are discussed below.
METHODS
. Weekly uncorrected notifications of whooping cough wereobtained from the Office of Population Censuses and Surveys(OPCS) Monitor weekly reports. Quarterly corrected notifica-
Fig. 1-Quarterly whooping-cough notifications for England andWales. 1950-79.
tions were used for the age-analysis and for calculatingnotification-rates for the 98 Area Health Authorities (AHAs) inEngland and Wales (OPCS Monitor MB2). These rates wereobtained by dividing the number of notifications by the mid-1977 population estimates of children under 15 in each AHA.’For more detailed age-analysis, mid-1977 and mid-1978 pop-ulation estimates for England and Wales were obtained fromOPCS Monitor PP1 78/2 and PP1 79/3. Because some of thedata were only available quarterly, the outbreak was defined asstarting at the beginning of the third quarter of 1977 and con-tinuing until the end of the second quarter of 1979, a period ofexactly 2 years. These were the quarters in which notificationsfirst began to increase and in which they finally declined to con-sistently lower levels (fig. 2).
Because of the boundary reorganisations of 1974, vaccina-tion figures for each AHA were only available for 2 years - i.e.,for children born in 1974 completing a primary course of vac-cination by the end of 1976, and for those born in 1975 com-pleting vaccination by the end of 1977. These figures wereobtained from the Department of Health and Social Security(DHSS) and the Welsh Office and were combined to give asingle vaccination-rate for the 2 years for each AHA.
RESULTS
1977-79 Outbreak
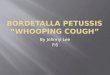
Weekly notifications for England and Wales fromJuly, 1977, to June, 1979, are shown in fig. 2. A consis-tent increase was first observed in Tyne and Wear in thethird quarter of 1977. At some time during the next 2years all AHAs had increased rates, though there was noclear pattern of spread throughout the country.The two major peaks during the outbreak were due to
whooping cough being notified mainly from one part ofthe country during the winter of 1977-78, decliningduring the summer, and increasing again throughout theremainder of the country in the autumn and winter of1978-79. A few AHAs also showed two peaks, usuallydue to different districts within the AHA having highnotification levels at different times.
VaccinationPertussis vaccine was introduced by some local health
authorities in 1942, and its use increased up to 1957,when vaccination became national policy. From 1958 to1974 about 75% of children were fully vaccinated.2There was then a fall in vaccination acceptance, so that
only 60% of children born in England and Wales in 1973were vaccinated by the end of 1975. This drop continuedwith figures of 38% recorded for 1976, 40% for 1977,and 30% for 1978.
Fig. 2-Weekly whooping-cough notifications for England andWales, July 1977-June, 79.

1181
TABLE I-WHOOPING COUGH NOTIFICATION-RATES FOR
ENGLAND AND WALES BY AGE
*Average of 1977 and 1978 mid-year population estimates.tAverage of 1974 and 1975 mid-year population estimates.
AgeThe whooping-cough notification-rate was highest for
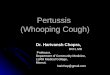
children aged 6 months to 4 years (table i). Overall the1977-79 notification rate was about 4 times that of 1974-75, but this increase varied considerably with age (fig. 3).Children in the 1 to 4 year age-range showed a sixfoldincrease, about twice that for the babies and olderchildren, while the adult rate increased fourfold.
Notification and VaccinationTo consider the effect of vaccination on notifications
in the 1977-79 outbreak, the AHAs were classified intothree groups according to their vaccination acceptancerates for children born in 1974 and 1975 (table 11). AHAswith vaccination-rates below 30% had a notification-rateof 1064 per 100 000 children under 15, compared with afigure of 670 for AHAs with a vaccination-rate of over50%. Whooping-cough notification-rates were thereforeabout 60% higher in the AHAs with low vaccinationacceptance. Furthermore, the two AHAs with by far thehighest notification-rates (Isle of Wight and West
Glamorgan, each with 2500 notified cases per 100 000children under 15), had vaccination-rates of 14% and
Fig. 3-Differences between July, 1977-June, 79 and 1974-1975whooping-cough notification-rates by age.
TABLE n——WHOOPING-COUGH VACCINATION-RATES IN 1976 AND
1977, AND NOTIFICATION-RATES, JULY, 1977-JUNE, 1979, FORALL AREA HEALTH AUTHORITIES IN ENGLAND AND WALES
18%, respectively, well below the national average. Con-versely, Leicestershire and Northumberland AHAs,which had the lowest notification rates (around 400 per100 000 children under 15), had the high vaccinationacceptance rates of 61% and 53%, respectively.The more densely populated. urban areas (i.e., the
metropolitan counties and Greater London) might beexpected to have higher whooping-cough notification-rates than the less urban non-metropolitan counties.
However, at each vaccination acceptance level, there waslittle difference between the notification-rates of thesetwo groups of AHAs (table in). Thus, in the 1977-79 out-break there was no evidence that the metropolitan areashad higher notification-rates than the rest of the country.
In a previous report two socioeconomic indicatorswere shown to affect whooping-cough notification-ratesand their relation with vaccination-rates. 3 Theseindicators were for overcrowding (here defined as thepercentage of households with more than one person perroom), and for social class (based on the number ofunskilled workers as a percentage of those economicallyactive). Both were derived for each AHA from dataobtained from the 1971 census for England only.4However, in the 1977-79 outbreak the relation betweenvaccination and notification rates was unaffected by con-sideration of these two indicators. For the 90 AHAs of
England the correlation coefficient between vaccinationand notification rates was -0.49 (p<0.001), while the
partial coefficient eliminating the influences of over-crowding and social class on the vaccination andnotification rates was -0.57 (p<0.001). Thus theassociation between vaccination and notification rates is
TABLE III-WHOOPING-COUGH VACCINATION RATES IN 1976 AND 1977 AND
NOTIFICATION-RATES, JULY, 1977-JUNE, 1979 FOR DIFFERENT TYPES OF
AREA HEALTH AUTHORITIES IN ENGLAND AND WALES

1182
highly significant even when the effects of social classand overcrowding are taken into account.
DISCUSSION
This report relies on OPCS notifications as a measureof the extent of whooping-cough throughout Englandand Wales in 1977-79. Notifications are not a completelyreliable indication of the true prevalence of the diseasesince they may be affected by other influences. Vaccina-tion returns may also be subject to error such as thatcaused by the migration of children from one AHA toanother. Nevertheless, the analysis of the available dataclearly shows a direct relation between the decline in vac-cination and the increase in notifications, consistent
throughout England and Wales.Firstly, a steep fall in vaccination-rate was rapidly
followed by the sudden reversal of a 25-year trend ofdeclining notifications. Secondly, between 1970 and1974 the number of children vaccinated against whoop-ing cough outnumbered notified cases by over 50 to 1.Thus, even allowing for incomplete efficacy of the vac-cine and under-notification of cases, vaccination was thechief factor in decreasing the number of susceptibles.Because of the fall in vaccination-rate, about 1 200 000children born between 1974 and 1976 were unvaccinatedand susceptible to whooping cough in 1977. Compared
with the 1974-75 outbreak, the notification-rate in the 1-4 year age-group, which contained most of these unvac-cinated children, showed a bigger increase than that inthe 5-14 age-group, in which more than 75% were vac-cinated. The increased notification-rate in the over-15
age-group was due mainly to a large rise in the 25-34age-group. These adults were probably too old to havebeen vaccinated and were potentially at high risk as theparents of young unvaccinated children. Finally, allAHAs in England and Wales showed a clear inverse rela-tion between vaccination and notification rates, evenafter allowing for differences in overcrowding and socialclass.
There is therefore clear evidence that the decline in
whooping-cough vaccination rates has been the principalcause of increased notifications.
I thank Dr C. L. Miller for help and advice.
REFERENCES
1. Office of Population Censuses and Surveys. Population estimates 1977.Series PP1 No 3. London: H.M. Stationery Office, 1979.
2. Department of Health and Social Security. Whooping-cough vaccination.Review of the evidence on whooping-cough vaccination by the Joint Com-mittee on Vaccination and Immunisation by the Joint Committee on Vac-cination and Immunisation. London H.M. Stationery Office, 1977.
3. Bassili WR, Stewart GT. Epidemiological evaluation of immunisation andother factors in the control of whooping-cough. Lancet 1976; i: 471-74.
4. Imber V. A Classification of the English personal social services authorities.D.H.S.S. Statistical and Research Report Series No. 16. London: H.M.Stationery Office, 1977.
Treatment of Tuberculosis
SHORT-COURSE CHEMOTHERAPY INPULMONARY TUBERCULOSIS
A controlled trial by the British Thoracic Association(third report)*
In 1972 a trial of short-course chemotherapy in
pulmonary tuberculosis was undertaken by the BritishThoracic Association (B.T.A.) with the support and
cooperation of most chest physicians in Britain. 802
patients with sputum-positive disease with drug-sensitiveorganisms were studied. The duration of chemotherapydepended upon the extent of cavitation on the pretreat-ment chest radiographs: 1) patients with no cavitation orwith no single cavity larger than 2cm in diameter wereallocated at random to either 6 or 12 months of rifam-
picin and isoniazid plus an initial supplement of etham-butol or streptomycin for 2 months, 2) patients with anycavity larger than 2cm in diameter were allocated atrandom to either 9 or 18 months of rifampicin andisoniazid plus an initial supplement of ethambutol orstreptomycin for 2 months.
*This is the third report of a trial organised by a subcommitteeof the research committee of the British Thoracic Associationwhose members were: Dr K. M. Citron (chairman); Dr J. H.Angel, Dr I. A. Campbell, Dr A. Dyson, Dr A. R. Somner(coordinators); and Dr P. A. Jenkins, Dr S. Lal, Dr J. B. Sel-kon, and Dr I. Sutherland. The report was prepared by Dr A.R. Somner with the help of Mrs C. P. Davison.
The dosages were as follows :-
Rifampicin-600 mg daily, orally (or 450 mg if the patient weighedless than 500 kg).Isoniazid-300 mg daily orallyEthambutol-25 mg per kg daily, orallyStreptomycin-0 75 g intramuscularly, 6 days a week.
The results of treatment of the patients who completedthe allocated period of chemotherapy and the earlyrelapse rates were reported in 1975.1The relapse rates among the 665 available patients up
to 33 months after the start of chemotherapy were repor-ted in 1976.2 Relapse after chemotherapy was defined astwo or more positive cultures in any period of 4 monthsin specimens taken at least 2 weeks apart. We report herethe final results 54 months from the start of
chemotherapy.
RESULTS
Among the 160 patients who had received 6 months’chemotherapy and were available for analysis of relapse33 months after the start of chemotherapy there were 8relapses (5%).2 Of the 155 patients who had received 12months’ chemotherapy and were available for analysis 2had relapsed (1%). None of the patients in the 9 and 18month regimens had relapsed.
33 - 54 months after the start of chemotherapy therewas only one further relapse. This was a patient on the 6month regimen, 35 months after treatment began, bring-ing the number of relapses for this group to 9 (7%) of130 patients still available for analysis. The patients inthe 6 month regimen had by then been observed for 4years since stopping chemotherapy.
None of the 52 patients who died between the end oftreatment and the end of the follow-up period died with