-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 581
[ CLINICAL COMMENTARY ]
The role of muscles in joint protection and stabilization has
beenof increasing interest to researchers and clinicians involved
inspinal pain and rehabilitation. Evidence for the importance
ofdeep posterior muscles of the spine in the management of
people
with low back pain (LBP) has been provided by
biomechanical7,60,80,82
and neurophysiological46,48 investigations. Imaging studies have
furtherallowed denition of both normal morphology and
impairments
in paraspinal muscles.22,27,32,33 Rehabili-tative ultrasound
imaging (RUSI) is apotentially useful tool in physical thera-py for
the assessment and treatment ofthese muscles. The advantages of
RUSIover other imaging techniques have beendiscussed in a recently
published related
cles can be incorporated into neuromus-culoskeletal
rehabilitation. The mainapplications of RUSI for measurementof
morphological characteristics (mor-phometry) and visualization of
musclecontraction for biofeedback are dis-cussed. The lumbar
multidus is themost widely studied paraspinal muscle,in both
healthy populations68 and peoplewith spinal pain and
injury.22,26,27 Stud-ies of different cervical muscles are
alsoemerging.37,39,61-63 In the thoracic region,the lower trapezius
is the rst muscle tobe measured with ultrasound imaging.53
Quantitative evaluation of the posteriorparaspinal musculature
using static anddynamic imaging has been used to studymuscle
morphology and behavior dur-ing contraction.34,39,64,74,76 In this
context,behavior relates to level of contraction(change in
thickness), changes in sizeover time and with respect to
othermuscles, as well as observation of con-traction as a
biofeedback tool for the pa-tient or therapist. In this
commentarywe review what is known about RUSI asapplied to the
paraspinal musculature,propose guidelines for standardizingthe
imaging and measurement tech-niques in clinical and research
applica-tions, and propose future directions forresearch.
T SYNOPSIS: Interest in rehabilitative ultra-sound imaging
(RUSI) of the posterior paraspinalmuscles is growing, along with
the body ofliterature to support integration of this techniqueinto
routine physical therapy practice. This clinicalcommentary reviews
how RUSI can be used asan evaluative and treatment tool and
proposesguidelines for its use for the posterior muscles ofthe
lumbar and cervical regions. Both quantita-tive and qualitative
applications are described,as well as measurement reliability and
validity.Measurement of morphological characteristics ofthe muscles
(morphometry) in healthy populationsand people with spinal
pathology are described.Preliminary normal reference data exist for
mea-surements of cross-sectional area (CSA), linear
dimensions (muscle depth/thickness and width),and shape ratios.
Compared to individuals withoutlow back pain, changes in muscles
size at rest andduring the contracted state have been observedusing
RUSI in people with spinal pathology. Visualobservation of the
image during contractionindicates that RUSI may be a valuable
biofeed-back tool. Further investigation of many of
theseobservations is required using controlled studiesto provide
conclusive evidence that RUSI enhancesclinical practice. J Orthop
Sports Phys Ther2007;37(10):581-595.
doi:10.2519/jospt.2007.2599
T KEY WORDS: cervical muscles, lumbarmuscles, lumbar spine,
neck, morphometry,sonography
1Professor of Neuromuscular Rehabilitation, Director of
Research, School of Health Professions and Rehabilitation Sciences,
University of Southampton, UK; Visiting Professor,Department of
Physiotherapy, Trinity College, Dublin, Ireland. 2Senior Lecturer,
Division of Physiotherapy, School of Health and Rehabilitation
Sciences, University of Queensland,Brisbane, Australia; Clinical
Director, UQ/Mater Back Stability Clinic, Mater Health Services,
Brisbane, Australia. 3Assistant Professor, Department of Physical
Therapy, RegisUniversity, Denver, CO; Doctoral Candidate, Division
of Physiotherapy, School of Health and Rehabilitation Sciences,
University of Queensland, Brisbane, Australia. 4AssistantProfessor,
Department of Physical Therapy, University of Evansville,
Evansville, IN; Assistant Professor, University of Kentucky,
Lexington, KY. 5Professor and NHMRC PrincipalResearch Fellow,
Director, Division of Physiotherapy, School of Health and
Rehabilitation Sciences, University of Queensland, Brisbane,
Australia. Address correspondence toDr Maria Stokes, Professor of
Neuromuscular Rehabilitation and Director of Research, School of
Health Professions and Rehabilitation Sciences, University of
Southampton,Higheld Campus, Southampton, Hants SO17, 1BJ, UK.
E-mail: [email protected]
manuscript.79
The primary purpose of this clinicalcommentary is to review the
currentscientic literature on RUSI related tothe posterior
paraspinal muscles andto increase the understanding of howRUSI of
the posterior paraspinal mus-
Rehabilitative Ultrasound Imagingof the Posterior Paraspinal
Muscles
MARIA STOKES, PhD, MCSP1 JULIE HIDES, PhD, MPhtySt, BPhty2
JAMES ELLIOTT, PT, MS3 KYLE KIESEL, PhD, MPT, ATC, CSCS4 PAUL
HODGES, PhD, MedDr, BPhty (Hons)5
-
582 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]ANATOMY OF THEPARASPINAL MUSCULATURE
Interpretation of RUSI is depend-ent on an understanding of the
ana-tomical features and function of the
musculoskeletal structures of the spine.This section presents an
overview of theanatomical and biomechanical propertiesof the
paraspinal musculature, focusingon the lumbar and cervical muscles
inrelation to RUSI. The reader is referredto the following
manuscripts for furthermore specic details of anatomy
andfunction.2-4,6,8,52,55,60
Posterior Lumbar Spine MusculatureThe lumbar paraspinal muscles,
lyingbehind the transverse processes, havebeen divided into 3
groups by Bogduk.3
The rst and deepest group includes thedeep intersegmental
muscles, interspi-nales, and intertransversarii mediales.These
muscles are short and too small toprovide sufficient clarity of
their bordersfor adequate visualization by ultrasoundimaging (USI).
The second group com-prises the polysegmental muscles, whichattach
directly to the lumbar vertebrae
and include the multidus and lumbarportions of the erector
spinae (ES), lon-gissimus, and iliocostalis muscles (TABLE1). The
third and most supercial groupof muscles consists of long,
polysegmen-tal muscles, which traverse the lumbarregion from the
thoracic levels. Thesemuscles attach to the ilium and sacrum,and
include the thoracic portions of the
ES muscles.Lumbar Multidus This is the most me-dial of the
lumbar muscles and Macin-tosh et al44 have described it as a
large,multifascicular muscle composed of 5overlapping layers, with
its size increas-ing in a caudal direction (FIGURE 1, TABLE1). The
morphometry of the lumbar mul-tidus muscle can be assessed with
RUSI
TABLE 1 Anatomy of Selected Lumbar and Cervical Posterior
Paraspinal Muscles
Muscle Origin Insertion
Lumbar multidus44 Laminae and spinous processes of each lumbar
vertebra Descend in a caudal direction to cross 3 to 5
vertebrae
Deep laminar bers: inferior edge of a lamina Mamillary bodies
and zygapophyseal joint capsule
of the vertebra 2 levels caudal
Supercial bers: along the spinous process Cross up to 5 levels:
attach to the mamillary
processes of the caudal vertebra, sacrum, and
posterior superior iliac spine
Erector spinae43
Longissimus Lumbar transverse and accessory processes Ventral
surface of posterior superior iliac spine
Iliocostalis Tips of lumbar transverse processes and adjacent
middle layer of Ventral edge of iliac crest
the thoracolumbar fascia
Cervical multidus2 Laminae and spinous processes of cervical
vertebrae Capsules of cervical facet joints81
Semispinalis cervicis2 Transverse processes of the upper 5 or 6
thoracic vertebrae Cervical spinous processes of C2 to C5
Splenius capitis2 Spinous processes of C7 and T3 or T4 Just deep
to sternocleidomastoid into the mastoid
process and occipital bone just below lateral third of
superior nuchal line
Semispinalis capitis2 Tips of transverse processes of T6 and T7,
and C1-C3 articular processes Mastoid process
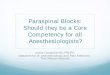
FIGURE 1. Cadaver dissection of lumbar multidus (M), rotatores
(R), and the semispinalis (SS) musculature,showing fascicles
passing down in a caudal direction over the lumbar spine.
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 583
using either a transverse or parasagittalimage. On the
transverse section, lumbarmultidus can be identied as a
singleregion of muscle and separate fasciclesare not often visible
(FIGURES 2 and 3).The advantage of imaging using a trans-verse
section is that the cross-sectionalarea (CSA) of the muscle can be
mea-sured.21,68 Conversely, in a parasagittal(longitudinal) image,
muscle fasciclescan be identied from the connectivetissue between
muscle bers (FIGURE 4).
Parasagittal views are easier to interpretthan transverse views,
both for measur-ing muscle thickness34 and for providingbiofeedback
of changes in the muscleduring contraction.24,74
Researchers using biomechanicalmodels based on anatomical data
havesuggested that the supercial bers oflumbar multidus create a
posteriorsagittal rotation (extension) of the lum-bar spine, in
addition to intervertebralcompression,43,4 while the deeper
bersprimarily generate compressive forces,with minimal associated
torque.4,47 It hasbeen proposed that the intersegmentalnature of
the deep lumbar multidusprovides an advantage to the neuromus-
cular system for controlling the stabilityof the motion
segment.55 For this rea-son, clinicians aim to include
voluntarycontraction of the deep bers in theirexercise (or
rehabilitative) programs.24
Electromyographic (EMG) studies ofarm movement suggest
differential ac-tivation of the deep (earlier onset) andsupercial
bers.51 This nding suggeststhat different exercises may be
neces-sary for selectively re-educating the deepversus the
supercial bers, but this re-quires investigation.
There is consistent evidence that thelumbar multidus muscle
controls spi-nal motion, contributing to interverte-bral
stiffness.31,55,80 Lumbar multidusRUSI studies have identied
reducedCSA in people with acute LBP,26,27 andEMG evidence suggests
that changes inmotor control may be more localized tothe deep
bers.42 However, it is impor-tant to consider that all lumbar
mus-cles contribute to stability of the
lumbarspine.7,8,12,18,47,48,80
Lumbar ES The lumbar ES lie lateralto multidus and consist of
longissimusthoracis pars lumborum and iliocostalislumborum pars
lumborum (TABLE 1).43
In the upper lumbar region, research-ers have demonstrated that
the longis-simus muscle overlaps the bers of themultidus muscle.43
Various studies haveshown that the ES muscles contribute tolateral
exion, extension, and rotationof the lumbar spine, as well as
stabil-ity.7,8,12,18,47,48,80 Regarding imaging, theES muscles are
too large to allow CSAmeasurements using RUSI. However,Watanabe et
al78 have measured thick-ness successfully in the sagittal plane
byplacing the transducer longitudinally.Their technique illustrates
the use of theechogenic (reective, white) transverseprocesses and
subcutaneous tissue-mus-cle border as landmarks to assess
thick-ness of the ES muscles.
Posterior Cervical Spine MusculatureThe posterior musculature of
the cervi-cal spine is commonly divided into 4 lay-ers (FIGURE 5).
The most supercial layer
FIGURE 2. Schematic diagram of a cross section at the level of
the fourth lumbar vertebra (L4). The lumbarmultidus muscle (M) lies
lateral to the spinous process, superior to the lamina (L), and
medial to erector spinae(ES). Abbreviations: AT, adipose tissue;
IL, iliocostal ligament; S, skin; SP, spinous process; TP,
transverse process;VB, vertebral body.
FIGURE 4. Parasagittal ultrasound image of thelumbar multidus
muscle, taken lateral to the spinousprocess using a 5-MHz
curvilinear transducer. Thefacet joints (F) can be used as
landmarks for thelower border of the muscle.
FIGURE 3. Bilateral transverse ultrasound image atL4, using a
5-MHz curvilinear transducer, showingthe spinous process (SP) in
the center of the imageand the echogenic laminae (L) appearing as
brightwhite horizontal landmarks, either side of the baseof the SP
and beneath the lumbar multidus (M)muscle. The lateral borders are
not clear enoughto enable measurement of area and require
thetransducer to be angled more appropriately for eachside
separately.
-
584 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
consists of the upper trapezius muscles,the second layer
consists of the spleniuscapitis muscle,62 the third layer
consistsof the semispinalis capitis63 and semispi-nalis cervicis
muscles,71 while the deepestlayer contains the multidus and
rotatoresmuscles. Some studies place semispinaliscervicis in this
deepest layer,61 while othersalso include the suboccipital muscles
ofrectus capitis posterior minor (RCPmin)and major (RCPmaj).71 We
have limitedthe description of anatomical features ofcervical
muscles to those described by re-searchers using
RUSI.37,39,61-63
Cervical Multidus and Semispinalis Cer-vicis Winkelstein et al81
have suggestedthat the ability of the multidus muscle tocontrol
cervical segmental motion couldbe compromised by its insertion
directlyinto the capsules of the facet joints (TABLE1), which have
been widely implicated inneck pain and injury.41,56,65,82
Degenerativechanges in the deep cervical paraspinalmusculature have
been found in studiesusing RUSI and magnetic resonance im-aging
(MRI) in patients with persistentneck pain following
trauma.15,19,37,73 Thesemispinalis cervicis muscle (along withthe
capitii musculature) is considered aprimary cervical spine
extensor.52
Splenius Capitis and Semispinalis Capi-tis These muscles have
been describedas broad and at, extending upward andlateral to their
attachment on the mastoidprocess (TABLE 1).62,63 The main
functionof these muscles is neck extension,46,71
and they are more active during large,fast movements of the
neck11 than duringsustained postural activity.
QUANTITATIVE EVALUATION
The procedures described arebased on developmental studies
byHides et al,21,26,27 Kiesel et al,34 and
a relatively large population study byStokes et al,68 and reect
the suggestionsof the team of authors of this commen-tary. Both
static and dynamic techniquesfor quantitative evaluation of muscles
aredescribed.
Imaging Procedure for Lumbar MultidusImages of lumbar multidus
have eitherbeen obtained from transverse (FIGURE3)21,22,26,27,68 or
parasagittal (FIGURE 4)34
orientations.Positioning As originally suggested byHides et
al,21 the subject is usually relaxedin a prone lying position. But
this is notalways possible, as Coldron et al10 realizedwhen
attempting to scan lumbar mul-tidus in women who had recently
givenbirth. Researchers have shown that theside-lying position can
be used to obtainimages without affecting muscle size atrest.10 But
this is not the case when im-aging with the subject in a standing
pos-ture.40 Lee et al40 found that in healthycontrol subjects,
lumbar multidus CSAincreased from prone lying to uprightstanding,
then gradually decreased dur-ing forward exion. In patients with
LBP,CSA also increased from prone to uprightstanding, but forward
exion produced afurther increase in CSA, suggesting al-tered
function of lumbar multidus.40
As suggested by Hides et al,21 we recom-mend that, in prone
lying, 1 to 2 pillows
be placed under the hips to minimize thelumbar lordosis, so that
the muscles lie ashorizontally as possible along the
spine.Inclinometers were used by Hides et al25
and Kiesel et al34 to ensure the lumbarspine was within 10 of
horizontal.
Positioning of the operator relative tothe subject is important
for standardiza-tion of the technique to achieve correctimage
interpretation. So, with the subjectprone, we recommend that the
scannerand operator be situated to the left of theprone subject
(the opposite to imaginganterior structures in the supine
subject),in keeping with standardized protocols
inradiology.9,79
The lumbar spinous processes are pal-pated and their position
located on theskin with an indelible marker, such asan eye liner
pencil, which is water insol-uble but easily removed with an
alcoholswab.54 In most individuals, the spinousprocess of L5 is a
deep, small, bluntedbony point lying at the center of the
lum-bosacral depression and can be found bypalpating cranially from
the sacrum.5 Onprogression in a cranial direction is
thecomparatively large spinous process ofL4. The remaining lumbar
spinous pro-cesses are then identied by continuingpalpation
cranially. These locations canbe veried with USI by including
thesacral base in the image and counting thespinous processes
cranially.Transducers Various transducers havebeen used for imaging
the lumbar mul-tidus muscle, but we suggest the use ofa curved
transducer with a frequency of5 MHz, which is used for transverse
im-aging in the majority of studies (TABLE 2).This is because more
of the sound wavesemitted by a curved transducer are likelyto be
perpendicular to the rounded bor-der of multidus than those from a
lineartransducer. For parasagittal imaging, weconsider transducer
shape less impor-tant, so curvilinear34 or linear25 arrays canbe
used. Regarding transducer frequency,the depth of lumbar multidus
is moresuited to 5 MHz21,68 for image clarity thanlower or higher
frequencies, such as 3MHz or 7 to 10 MHz, respectively.79 The
FIGURE 5. Magnetic resonance images: (A) sagittal cross section
of the C6 vertebral level; (B) the correspondingaxial scan at the
C6 level showing the cervical multidus (M), semispinalis cervicis
(SEC), semispinalis capitis(SCP), splenius capitis (SC), and
trapezius (T) muscles.
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 585
size of the transducer varies with differ-ent ultrasound
machines (TABLE 2), but wesuggest using as large a footprint
(lengthof array surface) as possible, with a mini-mum of 5 cm, to
ensure sufficient contactwith the skin to enable a wide eld of
viewon the scan. For further details on select-ing transducers, see
a related publica-tion by Whittaker et al,79 which discussesthe
relationships between muscle shape,depth, and transducer
specications.Imaging Technique We endorse thetechnique used by a
number of research-ers,21,25,27,68 in which the transducer wasrst
placed longitudinally and centrallyover the lower lumbar spine to
orientand conrm the marks on the skin. The
indicator mark on the side of the trans-ducer (either a line or
light) was directedcranially, producing a scan showing thespinous
processes, as seen in FIGURE 6. Forparasagittal imaging,
researchers havedescribed moving the transducer later-ally to image
lumbar multidus,34,74 usingthe facet joints inferiorly as a
landmark(FIGURE 4). For transverse imaging, thetransducer was
rotated from the central
longitudinal orientation through 90, tolie transversely in the
midline with its in-dicator mark towards the operator,21,68 sothat
the right side of the anatomy wouldappear on the right side of the
screen.This produced an image in which the spi-nous process and
laminae could be seen,with lumbar multidus muscles visibleon both
sides of the spine (FIGURE 3). Ifthe muscles were too large for
bilateralimaging, they were scanned individuallyby moving the
transducer laterally, to theleft and right (FIGURES 7 and 8). As in
thesepreviously cited studies, we recommendthat the echogenic
(bright) vertebrallaminae be used as landmarks to identifythe
muscles deep border, which is impor-tant when measuring CSA, as
there is alarge difference in CSA over the span of1 vertebral level
if a consistent landmarkis not used.
The lateral border of the lumbar mul-tidus muscle is often
difficult to dis-tinguish from the lumbar longissimusmuscle, and
strategies to produce musclecontraction can help to identify the
bor-der during real-time imaging (TABLE 3).However, if a test
movement is used, it isimportant that the subject relaxes
beforemeasurements are taken. Off-line mea-surements on stored
images do not havethe advantage of dynamic (real-time) im-aging for
locating muscle borders and itmay me more of a matter of
extrapolatingbetween identiable areas of a border.
TABLE 2Transducers for Ultrasound Imagingof the Posterior Lumbar
and Cervical
Paraspinal Muscles*
Muscles Transducer Researchers Footprint Size (cm)
Lumbar
Multidus
Transverse image 5.0 MHz curvilinear Van et al74 5.5
Stokes et al68 5.0
Parasagittal image 5.0 MHz curvilinear Kiesel et al34 7.0
7.5 MHz linear Hides et al25 7.5
Cervical (Transverse)
Semispinalis capitis 7.5 MHz linear Rankin et al61 8.0
Deep posterior group 5.0 MHz curvilinear Rankin et al61 5.0
Multidus 10.0 MHz linear Lee et al39 3.8
7.5 MHz linear Kristjansson37 7.0
* Transducers with a large footprint (>5 cm) are preferable
for sufficient contact with the skin to enablea wide eld of view.
Transducer size and frequency depend on availability with a
particular scanner.The preferable transducer for transverse imaging
of lumbar multidus is 5 MHz curvilinear. Not reported in paper
cited (detail gained from authors). The deep posterior cervical
group comprises the semispinalis cervicis, multidus, and
rotatores.
FIGURE 6. Ultrasound image showing a sagittal viewof the lumbar
spine. The 5-MHz linear transducer wasplaced centrally over the
spinous processes (SP).
FIGURE 8. Transverse ultrasound image of the rightlumbar
multidus muscle at L5, using a 5-MHzcurvilinear transducer. The
spinous process (SP) isshorter and the lateral edge less steep than
at L4(Figure 7). (Reproduced from Stokes et al,68
withpermission).
FIGURE 7. Transverse ultrasound image of a leftlumbar multidus
(M) muscle at L4, using a 5-MHzcurvilinear transducer. The oval
shape of the muscleis evident and is bordered inferiorly by the
lamina (L),medially by the spinous process (SP), and laterally
bylongissimus (Lo).
-
586 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
Static Measurement of Lumbar MultidusThe CSA (cm2) of multidus
is measuredby tracing around the muscle borderwith the on-screen
cursor or off-line us-ing an image-processing package such asImageJ
(http://rsb.info.nih.gov/ij/docs/index.html). For consistency, the
precisepart of the border needs to be traced eachtime and the inner
edge of the border isoften used.68 Two linear dimensions areoften
measured, dened as the great-est depth (anteroposterior [AP])
andthe greatest width (lateral dimension[Lat]), lying perpendicular
to the APdimension.21 Hides et al21 described theshape of the
lumbar multidus muscle asa ratio of the linear measurements,
withthe AP divided by the lateral dimension(AP/Lat). Stokes et al68
made anthropo-metric measurements on ultrasound im-ages to examine
their relationships withCSA, including the length (cm) of
thespinous process (SPL) and the horizontaldistance (cm) between
the lateral edgeof each lamina (bilateral lamina width).Researchers
have also used whole-bodymeasurements and characteristics to
as-sess their predictive value for estimat-ing lumbar multidus
size, includingheight, age, body mass, and body massindex
(BMI).21,27,68 Relationships alludedto here, particularly between
muscle di-mensions, will be discussed later in thecommentary.
Dynamic Measurement of LumbarMultidusReal-time RUSI can be used
to assessmuscle during active movements. Dy-namic measures are
described for theposterior cervical39 and the lumbar
mul-tidus,34,74,75 as well as muscular fatigue.64
The most common RUSI measurementof the paraspinal muscles to
representmuscle contraction is change in musclethickness. Watanabe
et al78 measuredthickness change of the lumbar ES mus-cles in the
sagittal plane. Signicantdifferences were found in measures
ob-tained in neutral, exed, and extendedstatic postures. Kiesel et
al34 used gradedresistance of contralateral upper extrem-ity lifts,
performed in prone, to produceincremental activation of lumbar
mul-tidus and demonstrated a positive re-lationship between
increases in musclethickness and ne-wire EMG signals (seevalidity
section below). Vasseljen et al75
used high-speed motion mode (M-mode)ultrasound, compared with
ne-wireEMG, to identify movement of the deepbers of the lumbar
multidus muscleduring rapid arm lifting. Lee et al39 foundsignicant
increases in thickness of cervi-cal multidus during contractions,
whichwere similar at 3 levels from C4 to C6.
It is clear that RUSI can be used tomeasure thickness of the
posterior trunkmusculature.34 Preliminary studies of as-
ymptomatic subjects comparing RUSI tothe gold standard of
intramuscular EMGare encouraging and suggest that RUSImay be used
to measure both magni-tude34,39 and timing75 of activation in
theparaspinal muscles.
Morphometry of the Lumbar MultidusThe lumbar multidus muscle, in
the ab-sence of pathology, has been described asgenerally round or
oval in shape, and itssize varies among the vertebral levels.25
Studies with similar methodology andsubject groups provide
consistent data,as summarized in TABLE 4.Cross-sectional Area At
the level of thefourth lumbar vertebra (L4), the meanCSA of
multidus has been reported tobe approximately 8 cm2 in males and
ap-proximately 6 cm2 in females (TABLE 4).The muscle becomes larger
at L5 (ap-proximately 9 cm2 in males and approxi-mately 7 cm2 in
females). The CSAs at L4and L5 are highly correlated (r = 0.82
formales, 0.80 for females), so one could bereasonably well
estimated from the otherusing predictive equations.68 A
multilevelanalysis of the entire lumbar spine indi-cated that
multidus CSA increases fromL2 to L5 and then decreases at S1.25
Meandata from a group of 10 young femaleswere approximately 2.0 cm2
at L2, 3.3cm2 at L3, 4.9 cm2 at L4, 7.1 cm2 at L5,and 6.4 cm2 at
S1.Linear Dimensions The thickness orAP dimension of lumbar
multidus isapproximately 2.6 cm and the lateraldimension is
approximately 2.8 cm inhealthy males (TABLE 4). In females, themean
values are approximately 2.2 cmfor the AP dimension and 3.0 cm for
thelateral dimension.Muscle Shape The linear dimensions in-dicate
that the muscle is almost round inmales but more oval in a
horizontal di-rection in females (ie, atter).21,68 A studyof 120
healthy subjects reported round,oval, and triangular lumbar
multidusmuscle shapes.68 Gender, age, vertebrallevel, and physical
activity accounted forthese different shapes.
The shape of the lumbar multidus
TABLE 3Strategies for Identifying the LateralBorder of Lumbar
Multifidus During
Transverse Imaging
Maneuver by the Subject
Raise (extend) the ipsilateral lower limb slightly24
Shorten ipsilateral limb gently
Raise the contralateral upper limb34
Imagine the muscles are sausages on either side of the spine and
try to shorten and fatten the sausages
Note: ensure that movements are minimal to maintain the test
position and avoid movement of the transducer
from the scanning site
Observe on Transverse Image
Movement of multidus and adjacent erector spinae muscle
(longissimus) in relation to each other. Fascicles
of multidus move in a swirling motion, sliding round against
each other, which differs from the movements
of longissimus
Although a lateral border may not be visible, the relative
motions of the muscles will indicate the boundary
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 587
muscle is not always regular, particularlyin subjects with
relatively large muscles,where it can appear more triangular68
(FIGURE 9). The medial and inferior (deep)borders of the
multidus are conned bythe spinous process and lamina, so
themultidus can only hypertrophy in a lat-eral or superior
(supercial) direction,which may explain the more triangularshape of
hypertrophied muscles.68 Insuch cases, the shape ratio is
mislead-ing as it would tend to suggest a roundshape. Stokes et
al68 suggested that it maybe more appropriate to describe a
trian-gular-shaped muscle using 3 measure-ments (the superior,
medial, and lateralborders), but this requires investigation.The
clinical relevance of lumbar multi-dus shape and whether or not it
reectsmuscle tone have yet to be explored.
Prediction of CSA From Linear Mea-surements Researchers have
shown that
linear measurements can reect CSA ac-curately.21,27,68 Linear
measurements canbe made more quickly and easily thantracing the
muscle border to measurearea (an option not available on all
ultra-sound apparatus). Linear measurementsare therefore more
applicable for clinicaluse than CSA, provided they predict
CSAaccurately. The combined linear measure-ments (AP Lat) were
highly correlatedwith CSA at L4 and L5 (range in males,r = 0.95 to
0.98; range in females, r =0.93 to 0.95) in 3 studies (TABLE
4).21,27,68
However, it is known that this correla-tion for resting muscle
weakens whenmuscle becomes atrophied (r = 0.75 and0.85 in males and
females, respectively27)and cannot be assumed in all
situations.Thus the clinical utility of the predictionof CSA from
resting linear measures may
TABLE 4Lumbar Multifidus Morphometry From Images
in Prone Lying in Healthy Populations
Abbreviations: AP, anteroposterior; CSA, cross-sectional area;
L, left; NR, not reported; R, right.* Mean 1 SD, range.
CSA VersusLinear
AP Dimension Lateral DimensionsPopulation Age (y)* Researchers
CSA (cm2)* Shape Ratio* Thickness (cm)* Dimension (cm)* Multiplied
(r)
Fourth Lumbar Vertebra
Males
n = 21 18-35 Hides et al21 6.15 0.93 (4.35-8.5) 0.91 0.12
(0.68-1.19) 2.55 0.3 (2.03-3.35) 2.82 0.23 (2.50-3.31) 0.98n = 52
40 13 (20-69) Stokes et al68 7.78 1.85 (4.24-11.5 [95%]) 1.02 0.15
(0.72-1.33) NR NR 0.96n = 19 41.7 (35-47) Lee et al40 R, 7.68 1.29;
L, 7.62 1.38 NR NR NR NR
Females
n = 27 18-35 Hides et al21 5.6 0.8 (4.18-7.23) 0.75 0.13
(0.42-0.98) 2.24 2.98 (1.63-2.75) 3.05 3.25 (2.35-3.96) 0.93n = 10
25.5 (21-31) Hides et al27 4.87 1.22 NR NR NR NRn = 68 34 13
(20-64) Stokes et al68 5.55 1.28 (3.03-8.06 [95%]) 1.05 0.21
(0.64-1.47) NR NR 0.95
Fifth Lumbar Vertebra
Males
n = 45 39 13 (20-69) Stokes et al68 8.91 1.68 (5.62-12.30 [95%])
1.03 0.17 (0.70-1.36) NR NR 0.95n = 19 41.7 (35-47) Lee et al40 R,
7.25 2.11; L, 7.14 1.55 NR NR NR NR
Females
n = 10 25.5 (21-31) Hides et al27 7.12 0.68 NR NR NR NRn = 46 32
12 (20-64) Stokes et al68 6.65 1.0 (4.69-8.60 [95%]) 0.95 0.17
(0.62-1.28) NR NR 0.94
L4/5
Males and 28 5.6 Kiesel et al34 NR NR 2.48 0.19 NR
NRfemales,
n = 5
FIGURE 9. Transverse ultrasound image of atriangular shaped left
lumbar multidus muscleat L4, taken using a 5-MHz curvilinear
transducer.(Reproduced from Stokes et al,68 with permission.)
-
588 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]be limited, as in most cases comparisonof
atrophied and nonatrophied musclesis the objective of the
assessment. Dur-ing contraction, however, Kiesel et al33
found that the AP linear measurementof lumbar multidus was
consistentlydecreased by induced pain, indicatingthat this simple,
time-efficient measuremay be clinically useful for assessment
ofcontraction capability. Correlations werefound to be poor between
muscle size andbody anthropometry.68
Muscle thickness (AP dimension) wasalso highly correlated with
CSA at L4(males, r = 0.8; females, r = 0.7). Howev-er, at L5,
although statistically signicant(P.001), the relationship was not
strongenough to be of clinical value (males, r =0.66; females, r =
0.54), assuming thatcorrelation coefficients above 0.70 arerequired
to be clinically signicant.36 Wesuggest that multiplication of the
lineardimensions, although not representativeof a round or oval
shape, is preferable toa single measurement when area cannotbe
measured, based on evidence of itshigh correlation with lumbar
multidusCSA.21,27,68
Symmetry Mean between-side differ-ence in lumbar multidus muscle
sizein healthy individuals without pain orpathology has been found
to be below10% (mean SD, 3 4%27; 9.6% 8% in males,68 8.1% 6% in
females68).Marked asymmetry can occur with acuteLBP27 and be a
useful clinical indicator ofabnormality.Effect of Age Researchers
have not founddifferences in lumbar multidus musclesize among
different age groups.68 How-ever, the quality of the muscle may
be-come altered, as changes in water andfat content that occur with
age producechanges in signal intensity on MRIscans.72 Inltration
with fatty or broustissue increases the echogenicity of mus-cle,
making it appear whiter than usual,as observed in some of the older
subjects(up to age 69 years) studied by Stokes etal.68 But a
reliable method for quantica-tion of these changes in ultrasound
im-ages has yet to be developed.
Imaging Procedure for the PosteriorCervical MusclesThere are
limited published data on RUSIof the cervical muscles. Those
studiedinclude splenius capitis,62 semispinaliscapitis,61,63
multidus,37,39 and the deepposterior cervical muscle group
compris-ing semispinalis cervicis, multidus, androtators.61
Positioning Imaging of the cervical mus-cles has been described
with the subjectsitting39,63 or prone lying,37,61,62,63 with
theneck in a neutral position. Rezasoltani etal63 used an
inclinometer to help ensurethat the thoracic and cervical
postureswere horizontal during the ultrasoundmeasurements. Locating
the vertebrallevels to be imaged has been achieved bypalpation of
the cervical spinous process-es between C2 (the rst bony
landmarkcaudal to the occiput) and C7 (the mostprominent spinous
process), as detailedby Lee et al.39
Transducers Examples of transducersused for the different
muscles are listedin TABLE 2. For example, a 7.5-MHz lin-ear
transducer was used for imagingsemispinalis capitis61,63 and
splenius ca-pitis,62 which are relatively supercialat muscles,
while a 5-MHz curvilineartransducer was used for the deep
musclegroup, which has a more oval shape.61
Conversely, for imaging cervical multi-dus, a deep oval muscle,
Lee et al39 used a10-MHz linear transducer and Kristjans-son37 used
a 7.5-MHz linear transducer,possibly determined by availability
oftransducers rather than suitability. Mostresearchers have held
the transducer inplace manually, but custom-made devicesto hold the
transducer have also been de-scribed.39 The devices can enable a
moreconsistent technique than manual appli-cation but need to allow
the transducer tobe tilted or angled to sharpen the imageif
necessary. Devices obviously have costimplications.Imaging
Technique Procedures havebeen described for splenius capitis
atC3,62 semispinalis capitis at C3,61,63 thedeep muscles as a group
at C3,61 and mul-tidus at C437 and C4 to C6.39 In all cases,
the transducer was placed transversely inthe midline over the
spinous process atthe level of interest and then moved lat-erally
to image the left or right muscles.Identication of the echogenic
(bright,reective) laminae is then useful, which-ever muscles are
imaged.
The splenius capitis lies deep to thetrapezius and is a broad,
at muscle. Thesemispinalis capitis is easily recognizedas a long,
strap-like muscle divided into2 sections by an aponeurotic
intersection(FIGURE 10). The deep neck muscle grouphas a
distinctive teardrop shape, but thefascia between the 3 constituent
muscles(semispinalis cervicis, multidus, androtatores) are not
always easy to distin-guish in symptomatic or asymptomaticsubjects
with RUSI (FIGURE 11). The cervi-cal multidus muscle lies ventral
to thesemispinalis cervicis and the fascia be-tween them is more
consistently denedusing 7.5- to 10.0-MHz linear transduc-ers than a
5.0-MHz curvilinear trans-ducer (FIGURE 11).
Morphometry of the Posterior CervicalMusclesResearchers have
reported data for CSA,linear dimensions, and shape ratios inhealthy
populations and some examplesare shown in TABLE 5. The muscles of
theneck are relatively small (mean CSA be-tween 1 and 3 cm2)
compared with thelumbar muscles. Atrophy of the cervicalmultidus
muscle was demonstrated inwomen with chronic whiplash-associ-ated
disorder (mean SD multidusCSA at C4: right, 0.96 0.19 cm2;
left,
FIGURE 10. Transverse ultrasound image of the leftsemispinalis
capitis muscle, a long strap-like muscle,using a 7.5-MHz linear
transducer. The cross-sectionalarea and aponeurosis (A) dividing
the muscle intomedial and lateral parts are indicated.
(Reproducedfrom Rankin et al,61 with permission).
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 589
1.06 0.19 cm2) compared with healthyfemales (right, 1.23 0.09
cm2; left, 1.25 0.10 cm2) (P.05).37 Studies of mul-tidus at C4
showed slight differencesin CSA between the groups studied
butmarked differences in shape ratio,37,39 as
evident in TABLE 5. These differences forcervical multidus could
have been dueto the different postures used for imag-ing, as in 1
study the subjects were ly-ing prone37 and in the other they
weresitting,39 which could have affected thetonic activity of the
resting muscle. Therewere no differences in measurements ofthe
semispinalis capitis muscle made inprone and sitting,63 and the 2
studies ofthe semispinalis capitis were in agree-ment.61,63 The
shape ratio value indicatesthe shape well, for example, the 2
atsupercial muscles, splenius capitis andsemispinalis capitis, were
approximately7 to 8 times wider than they were thick.The multiplied
linear dimensions werecorrelated with CSA in all muscles (r
=0.77-0.96).
Reliability of Measurement of ParaspinalMusclesVarious factors
inuence the robustness
of measurements and have been discussedelsewhere in a related
commentary.79 Con-sistently recognizable bony features canbe useful
internal landmarks, such as theechogenic vertebral laminae, when
imag-ing the paraspinal muscles.68 To our knowl-edge, 8 studies
have reported the reliabilityof using RUSI to measure paraspinal
mus-culature. Differences in study design, sta-tistical tests, and
reporting method makedirect comparisons somewhat difficult,but
those values considered key when in-terpreting reliability have
been included inTABLE 6. The majority of researchers mea-sured
muscle girth (CSA),59,61,63,68 whileothers measured thickness
utilizing theparasagittal view.34,74,76 Intraclass correla-tion
coefficient (ICC) values range from0.72 to 0.98.
In addition to the ICCs, the standarderror of measurement (SEM)
or 95% lim-its of agreement, both of which are con-sidered measures
of response stability,
FIGURE 11. Bilateral transverse ultrasound image ofthe deep
posterior cervical muscle group, using a 7.5-MHz linear transducer,
showing the teardrop shape,consisting of multidus, rotatores, and
semispinalis.The cross-sectional area of cervical multidus
isindicated on the right side of the image. (Reproducedfrom
Kristjansson37 with permission.)
TABLE 5 Cervical Paraspinal Muscle Morphometry in Healthy
Populations*
Abbreviations: AP, anteroposterior; CSA, cross-sectional area;
Lat, lateral; L, left; NR, not reported; R, right.* Subject
positioning is indicated for each study. Data are mean 1 SD, except
for age ranges, with 2 exceptions.
CSA VersusLat Linear
Shape AP Dimension Dimension DimensionsMuscle/Position Level
Population Age (y) CSA (cm2) Ratio Lat/AP (Thickness) (cm) (cm)
Multiplied (r)
Splenius capitis
Prone lying62 C3 Females, n = 10 19-29 R, 1.90 0.23 R, 8.83 1.05
NR NR 0.77L, 1.76 0.25 L, 8.54 1.08
Semispinalis capitis
Sitting63 C3 Males, n = 18 19-34 R, 1.99 0.37 R, 6.82 0.93 R,
0.58 0.08 R, 3.85 0.39 0.85L, 1.93 0.38 L, 6.58 1.04 L, 0.59 0.08
L, 3.76 0.36
Females, n = 28 19-34 R, 1.57 0.35 R, 7.00 1.07 R, 0.51 0.08 R,
3.55 0.42L, 1.56 0.34 L, 6.86 1.10 L, 0.52 0.07 L, 3.53 0.41
Prone lying61 C3 Males, n = 46 20-72 1.77 0.40 7.20 1.14 0.53
0.08 3.73 0.39 0.86Females, n = 53 18-70 1.34 0.42 7.10 1.34 0.48
0.11 3.27 0.48 0.84
Deep neck muscles
Prone lying61 C3 Males, n = 46 20-72 3.15 0.67 0.57 0.06 2.76
0.36 1.57 0.17 0.96Females, n = 53 18-70 2.60 0.05 0.57 0.10 2.49
0.28 1.40 0.19 0.84
Cervical multidus
Sitting39 C4-C6 Males and 26.8 3.8 C4, 0.92 0.16 C4, 2.40 0.47
C4, 0.72 0.10 C4, 1.70 0.20 NRfemales, n = 17 C5, 0.96 0.16 C5,
2.67 0.52 C5, 0.68 0.08 C5, 1.80 0.25 NR
C6, 1.20 0.29 C6, 2.54 0.63 C6, 0.77 0.09 C6, 1.90 0.38 NRProne
lying37 C4 Females n = 10 31.5 11.4 R, 1.23 0.09 R, 1.68 0.19 NR NR
NR
L, 1.25 0.10 L, 1.58 0.14 NR NR NR
-
590 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
may be reported (TABLE 6). The purposeof the measurement must
also be takeninto consideration. For example, it hasbeen shown that
by taking an average of3 measures of the transversus
abdominismuscle with RUSI, the SEM is reducedby approximately
50%.67 Reducing theSEM may be helpful in detecting groupdifference,
but may be more importantwhen the purpose of the measure is to
as-sess change postintervention. To be 95%condent that true change
(greater thanmeasurement error) has occurred frompreintervention to
postintervention, thechange score must exceed the minimaldetectable
change (MDC) for that mea-sure. The MDC95 is SEM 2 1.96,where 1.96
represents the value of the tdistribution for a 95% condence
inter-val (CI) and is in the units of the mea-sure. For example,
Van et al74 used RUSI
to measure lumbar multidus musclethickness during contraction.
The ICCwas reported to be 0.98 and the SEM was0.31 cm. If this
measurement were usedto assess change in muscle thickness
fol-lowing an intervention period, the MDC95could be calculated. To
be 95% condentthat true change occurred, the thicknessmeasured
would have had to change byat least the value of the MDC95, which
is0.86 cm, based on 0.31 2 1.96 =0.86. In general, the reliability
of usingRUSI to measure paraspinal musculaturecan be considered to
be fair to excellent(ICC = 0.72-0.98) and acceptable forclinical
use, as dened by Portney andWatkins.58
Validity of Measurements of ParaspinalMusclesHides et al25
conducted a study to deter-
mine the validity of RUSI measures oflumbar multidus compared
with MRI.Bilateral measurements of CSA weremade at vertebral levels
from L2 to S1in healthy females. No signicant differ-ences were
demonstrated between RUSIand MRI, despite the inherent differenc-es
in position for imaging (prone lying forRUSI and supine lying for
MRI), whenresearchers adhered to a strict measure-ment
protocol.25
To validate the use of RUSI for mea-suring muscle contraction,
changes inmuscle thickness have been compared toEMG activity of
various muscles, includ-ing the transversus abdominis49,29
andlumbar multidus muscles.34 The rela-tionship varies between
muscles and theexperimental protocol (eg, contractiontype), but, in
general, it is considered tobe curvilinear.
TABLE 6Reliability of Rehabilitative Ultrasound
Imaging of the Paraspinal Muscles
Abbreviations: CSA, cross-sectional area; ICC, intraclass
correlation coefficient; L, left; NR, not reported; R, right; SEM,
standard error of measurement.
Interrater Reliability
Researchers Population and Muscles ICC Response Stability ICC
Response Stability
Stokes et al68 10 healthy subjects (5 male). Within session and
95% limits of agreement NR NR
Lumbar multidus CSA at L4 between days, within session, 0.25
to
0.98-1.0 0.5 cm2; between days,
0.62 to 0.67 cm2
Pressler et al59 15 healthy females.
Multidus CSA at S1 Between-days ICC3,1: SEM: R, 0.32 cm2; NR
NR
R, 0.80; L, 0.72 L, 0.37 cm2
Kiesel et al34 8 healthy subjects. Lumbar ICC3,1 = 0.85 NR
Measurements made by NR
multidus thickness measured both raters on same
on parasagittal images scans. ICC3,1 = 0.95
Van et al74 25 healthy subjects. Lumbar Within-day ICC1,1, 0.98
SEM: rater 1, 0.31 cm; ICC2,3 = 0.98 SEM, 0.31 cm
multidus thickness at L4/5 and 0.97 rater 2, 0.32 cm
Wallwork et al77 Lumbar multidus thickness ICC1,3 = 0.92, NR
ICC3,2 = 0.97 NR
at L4/5 both raters
Rankin et al61 Semispinalis capitis CSA Within session and 95%
limits of agreement NR NR
between days, 0.99 within session, 0.09
to 0.16 cm2; between
days, 0.16 to 0.16 cm2
Rankin et al61 Deep cervical muscles CSA 0.98-0.99 95% limits of
agreement NR NR
within session, 0.27 to
0.28 cm2; between days
0.04 to 0.41 cm2
Rezasoltani et al63 Semispinalis capitis CSA 0.98 NR 0.98 NR
Intrarater Reliability
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 591
In the parasagittal view of the lum-bar multidus muscles, Kiesel
et al34
studied the relationship between thick-ness change (percent
change from rest)and ne-wire EMG activity (percent ofmaximum)
during a contralateral pronearm-lifting task with increasing
resis-tance, which automatically recruited theipsilateral multidus
muscle. This taskproduced contractions from 19% to 43%of maximum
effort, with a strong corre-lation (r = 0.79, P.001) between
thick-ness change and EMG activity. But, therewas no signicant
difference in multi-dus thickness change between the last 2levels
of activation, indicating that theEMG signal continued to increase
withload but thickness change was nearingits maximum. Muscles are
consideredto reach their maximum thickness atrelatively low EMG
values (approxi-mately 20% of maximal contraction).29
In isometric contractions this relates tothe point at which
tendon stiffness pre-cludes further tendon stretch and themuscle
continues to form cross-bridgesand increase electrical activity,
but withminimal further change in length and,therefore, thickness.
Many functionaldaily activities involve contractions atrelatively
low forces, which would fallwithin the linear part of the
relationship,where change in EMG reects change inmuscle thickness.
With respect to jointstabilization, mathematical models
havepredicted that only low-level contrac-tions of the lumbar
multidus muscleare required to stiffen the spine.6 Clini-cians have
therefore advocated low-levelvoluntary contractions to train the
mul-tidus muscle for this role, which can beaided by observing
changes in thicknesson RUSI images.24
Vasseljen et al75 used high-speed M-mode ultrasound to identify
deformationof the deep bers of the lumbar multid-us muscle with
concurrent EMG signal totest the validity of using the ultrasoundto
measure the timing of activation. Sub-jects performed rapid arm
lifting, whichis known to activate the deep and super-cial lumbar
multidus muscle,51 the onset
of which may be delayed in patients withLBP. Visual
determination of the muscleonset using ultrasound was comparableto
EMG, but with a small systematic de-lay. Although preliminary,
these resultssuggest that ultrasound may be used inthe future to
measure deep muscle onsetsclinically.
Validity of RUSI against MRI was ex-amined for the cervical
multidus musclein 10 healthy subjects at 3 cervical levelsfrom C4
to C6.39 Lee et al39 consideredthat validity was acceptable for
musclethickness measurements (R2 = 0.42-0.64), but not for CSA (R2
= 0.11-0.39)and width (R2 = 0.16-0.69). The smallCSA of the muscle
(approximately 1 cm2
compared with 7 cm2 for lumbar multi-dus) may amplify errors,
thus inuencethe variability of measurements.
CLINICAL STUDIES OF STATICPARAMETERS
The paraspinal muscles have beenstudied using RUSI to assess the
ef-fects of acute and chronic LBP, as
well as the effects of interventions, suchas exercise and spinal
surgery.
Acute LBPHides et al27 found marked side-to-sideasymmetry of the
lumbar multidus mus-cle CSA in 26 patients with rst-episodeacute
unilateral LBP. The smaller musclewas found at the symptomatic
segment(identied by manual palpation), was onthe side ipsilateral
to symptoms, and wasconned predominantly to 1 vertebrallevel. In
the 26 subjects with LBP, aver-age (SD) between-side difference
was31% 8%, compared with 3% 4% in51 asymptomatic subjects. It was
not pos-sible to determine whether the reductionin CSA was
pre-existing in these subjects.However, data from a study using a
por-cine model have conrmed that the CSAof the lumbar multidus
muscle reducesrapidly (as early as 3 days) after injury toan
intervertebral disc, is isolated to a sin-gle segment (the level
below the injureddisc), and is associated with histochemi-
cal changes in the muscle.28
Kiesel et al33 demonstrated the effect ofpain on lumbar multidus
muscle func-tion experimentally in humans. Increasesin multidus
thickness during arm-liftingtasks were signicantly reduced by
painin response to injection of saline into theerector spinae
muscles. This investigativeapplication of RUSI not only
contributedto knowledge about the effects of pain onmuscle
activation but added to the valid-ity of RUSI as a clinical
measurement ofmuscle dysfunction.
Chronic LBPSignicant atrophy of CSA was found byHides et al22 in
patients with chronic LBPcompared with healthy controls at
thelowest 2 lumbar vertebral levels. Greatestasymmetry was seen at
L5 in those withunilateral pain. These results were in agree-ment
with previous computed tomographystudies indicating that the
pattern of lum-bar multidus muscle atrophy in patientswith chronic
LBP was localized to the lowerregion of the spine rather than
generalized13
and that asymmetry occurred in those withunilateral pain.1 In an
MRI study of patientswith LBP, Barker et al1 also reported
thisselective, localized atrophy. Conversely, an-other study using
computed tomography tomeasure patients with chronic LBP
foundgeneralized atrophy in the lumbar spinebut also relatively
greater CSA of multi-dus on the symptomatic side.70 This ndingwas
consistent with histological evidence oftype I ber hypertrophy and
type II beratrophy in individuals with chronic LBP,17
possibly indicating an adaptive responseto muscle wasting. We
speculate that thispseudohypertrophy could also be related tofatty
inltration.35
Prelumbar Surgery and PostlumbarSurgeryImaging techniques have
proved use-ful for investigating the effects of spi-nal surgery on
the lumbar multidusmuscle.32,38,66 In cases of unilateral
LBP,researchers using computed tomographyfound that paraspinal
muscles were 10%to 30% smaller on the affected side com-
-
592 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]pared to the unaffected side and fatty
de-generation was also evident.38 Reducedmuscle CSA was seen using
RUSI inpatients prior to surgery with atrophybeing more severe in
those with greaterLBP.32 Postoperative images showed nofurther
decrease in CSA. However, it wasnot possible to conrm that muscle
at-rophy had not occurred, as size changescould have been masked by
intramus-cular inammation, seen as hypoechoicareas. Long-term
follow-up at 1 year in-dicated that multidus muscle atrophywas long
lasting.
QUALITATIVE ASSESSMENTAND FEEDBACK
Both static and dynamic param-eters can be assessed
qualitativelyusing RUSI. Static assessment gen-
erally involves evaluating the ultrasoundimage focusing on
tissue quality. The as-sessment of dynamic parameters includesusing
USI to evaluate the ability of themuscle to contract and teaching
muscleactivation using the image as a source ofbiofeedback.
Assessment of Static ParametersImpairments of the lumbar muscles
insubjects with LBP have been demon-strated in terms of both
decreased mus-cle size and density.27,50 Decreased muscledensity
can be caused by fatty inltration(increased fat-muscle ber ratio)
or ac-tual fatty replacement of bers.35,45 Whilechanges in density
have been predomi-nantly reported in computed tomographyand MRI
studies, changes in consistencyof the lumbar multidus muscles
havebeen observed using USI.27,32 The ultra-sound appearance of
healthy muscle isusually dark, due to its excellent perfu-sion and
resultant high uid content.The presence of fatty inltration,
brouschanges, or scar tissue (noncontractiletissue) leads to a
change in its sonograph-ic appearance, as noncontractile tissue
ishyperechoic, making muscle appear morewhite (FIGURE 12).27 On
computerized to-mographic scans, normal healthy muscle
appears grey and uniform. Consistencychanges will present as
dark areas. Incontrast, on specic MRI sequencing,fatty inltration
and brous changes ap-pear white. Consistency changes havemost
commonly been reported in sub-jects with chronic LBP.30
The fat content of the lumbar multi-dus and longissimus muscles
was mea-sured in 25 patients with chronic LBPand 25 matched
asymptomatic volun-teers using MR spectroscopy.50 There wasa
signicantly higher mean percentage offat content in subjects with
chronic LBP(23.6%; 95% CI: 17.5%, 29.7%) than inasymptomatic
subjects (14.5%; 95% CI:10.8%, 18.3%). Values for the longissi-mus
muscle did not differ between pa-tients and control subjects.
Further work
is required to validate the interpretationof muscle density on
RUSI and to de-termine reliability. This is likely to be acomplex
task because image brightnessis inuenced by the individualized
gainsettings used by the operator.
Lumbar multidus muscle atrophy ap-pears to be a common nding in
patientswith chronic LBP. In a recent MRI studyof 78 patients with
LBP (with and withoutlower extremity pain), changes in multif-idus
muscle consistency were graded asmild (fatty or brous tissue
replacementless than 10%), moderate (replacementless than 50%), and
severe (greater than50%).30 Degeneration of multidus waspresent in
80% of the subjects with LBP,and most commonly occurred at the
L4-L5 and L5-SI levels. Sixty-six of the 78patients with LBP (85%)
had degener-ated lumbar discs on MRI.
Assessment of Dynamic ParametersClinical assessment of
paraspinal muscleperformance involves palpation of thelumbar
multidus muscles at each ver-tebral level as the patient
preferentiallyactivates the muscle. Muscle thicknesschanges can be
seen using real-timeRUSI (FIGURE 13) as the patient performsthe
test maneuver and have been dem-onstrated reliably in the
lumbar24,26 andcervical muscles.39
FIGURE 13. Biofeedback of lumbar multidus: parasagittal view
using split-screen function and 5-MHz curvilineartransducer. The
facet joints (F) were used as landmarks for the lower borders of
the multidus (M) muscle. Duringcontraction (right panel), the
muscle becomes thicker and the angle of the bers becomes steeper,
providingfeedback. The left panel shows the muscle at rest.
FIGURE 12. Hyperechoic lumbar multidus muscleat L5 in a patient
with chronic low back pain, usinga 5-MHz curvilinear transducer.
The muscle tissueappears whiter compared with that in the scans
ofnormal subjects in Figures 3, 7, 8, and 9.
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 593
The ability of patients with chronicLBP to activate the lumbar
multidusmuscle has been found to be reduced, asevidenced by smaller
increases in thick-ness on RUSI images during contrac-tion than in
asymptomatic controls.77 Arandomized controlled trial of
healthysubjects by Van et al74 examined whethervisual biofeedback
using RUSI enhancedthe ability to activate the lumbar multi-dus
muscle. All subjects received clinicalinstruction on how to
activate the mul-tidus muscle isometrically and verbalfeedback on
performance (acquisitionphase). The intervention group
receivedvisual biofeedback with RUSI in parasag-ittal
section.24,26,34 Both subject groupsimproved voluntary contraction
(increas-es from resting thickness) in the acqui-sition phase, but
the RUSI biofeedbackgroup achieved greater improvements.On
reassessment a week later (retentionphase), the RUSI group
maintained theimprovements, whereas performance inthe control group
decreased.
A clinical randomized controlled tri-al of people with acute LBP
used RUSIsuccessfully for feedback of lumbar mul-tidus muscle
activation.26 Symmetry ofmultidus CSA was restored in the exer-cise
intervention group within 4 weeks.Despite pain relief and the
general muscleuse associated with return to normal ac-tivity
levels, patients in the control group(conventional treatment) still
displayedmultidus atrophy at a 10-week fol-low-up. Long-term
results revealed thatsubjects from the specic-exercise
groupexperienced fewer recurrences of LBPthan the control group.23
A limitation ofthis work is the lack of comparison withan exercise
group focusing on multidusrehabilitation without RUSI
feedback.Nevertheless, other investigators havesimilarly advocated
the benets of RUSIfor teaching muscle activation.14,20,24,74
The principles of motor learning16 mayexplain why visual
feedback is of benet forsubjects with LBP. In the initial stages
oflearning a new skill (cognitive stage), timeis spent
understanding the demands of thetask, what to do, and what to feel.
The clin-
ical observation that people with LBP ndit difficult to contract
the lumbar multi-dus muscle may be due to processes suchas reex
inhibition,69 which was thought toplay a role in multidus wasting
in individ-uals with acute LBP.27 Biofeedback may bebenecial as
subjects with LBP have beenshown to have decreased
proprioception,57
which affects their ability to provide andprocess internal
feedback.
Clinical ImplicationsPrescription of therapeutic exercise forthe
patient with LBP is based on knowl-edge of normal function of the
paraspinalmuscles, and the presence and nature ofimpairment in
terms of size or activation.Impairment of lumbar multidus is of-ten
specic to the side and vertebral levelof symptoms22,24,26,27 and
this has beenfound in subjects with acute and chronicLBP. Before
the introduction of RUSIinto clinical practice, physical
therapistscould only palpate for multidus muscleatrophy. This may
have previously ledto an underestimation of atrophy.
Viavisualization of the paraspinal musclesusing RUSI, impairments
can be betterassessed and documented. In addition toobjective
measurements of muscle size,changes in muscle consistency can
alsobe observed. RUSI can be used to pro-vide baseline measures of
impairments,and also to document improvements overtime and with
intervention. Therapeuticexercise may need to be as specic asthe
impairments that occur in order toaddress them. RUSI can provide
visualfeedback to enhance motor learning forcontracting a specic
muscle or part of amuscle. From a clinical perspective, theuse of
imaging techniques has alreadyprovided a wealth of information in
bothresearch and clinical practice.
Evidence that feedback with RUSI en-hances motor learning holds
promise forthe future but studies are needed on sub-jects with LBP,
and therapeutic exerciseinterventions need to be compared withand
without the use of RUSI for biofeed-back, to ultimately determine
the benetsof this rehabilitation tool.
DIRECTION OF FUTURERESEARCH
Almost all lines of research onparaspinal muscles produce
morequestions or uncover areas of un-
certainty. If RUSI is to become a routineaid to physical therapy
practice and a ro-bust research tool, standardized protocolsare
needed. Technical studies of the sizeof the transducer and whether
linear andcurvilinear arrays produce the same mea-surements are
needed to provide guid-ance on appropriate methodology.
Thepredictive value of linear measurementsto provide an estimate of
CSA needs to beestablished for different muscles in dif-ferent
states, such as resting, contracted,wasted, or hypertrophied. The
validityof using linear measurements to predictthe CSA of
irregularly shaped muscles re-quires attention.
Comprehensive studies of healthypopulations are needed to
generate refer-ence databases for assessing the effects ofpathology
and interventions. Factors toconsider include age, gender, body
type(physical characteristics including heightand body mass),
ethnicity, geographicdistribution (due to lifestyle
differences),and levels of habitual physical activityfrom sedentary
to elite sporting groups.Data for interrelationships between
dif-ferent spinal levels would be useful fordetecting abnormality
at a specic level.
Substantial work remains to validatethe dynamic techniques for
measuringboth magnitude and timing of changes inmuscle for clinical
use. Longitudinal epi-demiological studies are needed to deter-mine
those at risk of developing LBP orneck conditions, whether wasting
occursbefore the onset of injury and/or pain,and to help elucidate
the mechanisms ofwasting.
The contribution of noncontractiletissue to CSA, affecting the
density (orconsistency) of muscle, needs to be quan-tied to
determine true muscle size withpathology, particularly in subjects
withchronic pain, and aging. The sonographictechnique of
elastography is potentially
-
594 | october 2007 | volume 37 | number 10 | journal of
orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]
@ MORE INFORMATIONWWW.JOSPT.ORG
REFERENCES
1. Barker KL, Shamley DR, Jackson D. Changes inthe
cross-sectional area of multidus and psoasin patients with
unilateral back pain: the rela-tionship to pain and disability.
Spine. 2004;29:E515-519.
2. Bogduk N. The clinical anatomy of the cervicaldorsal rami.
Spine. 1982;7:319-330.
3. Bogduk N. Clinical Anatomy of the LumbarSpine and Sacrum.
Edinburgh, UK: ChurchillLivingston; 2006.
4. Bogduk N, Macintosh JE, Pearcy MJ. A universal
model of the lumbar back muscles in the up-right position.
Spine. 1992;17:897-913.
5. Burton A. Regional lumbar sagittal mobility:measurement by
exicurves. Clin Biomech.1986;1:20-26.
6. Cholewicki J, McGill SM. Mechanical stability ofthe in vivo
lumbar spine: implications for injuryand chronic low back pain.
Clin Biomech (Bris-tol, Avon). 1996;11:1-15.
7. Cholewicki J, Panjabi MM, Khachatryan A.Stabilizing function
of trunk exor-extensormuscles around a neutral spine posture.
Spine.1997;22:2207-2212.
8. Cholewicki J, VanVliet JJ. Relative contributionof trunk
muscles to the stability of the lumbarspine during isometric
exertions. Clin Biomech(Bristol, Avon). 2002;17:99-105.
9. Chudleigh T, Thilaganathan B. Obstetric Ultra-sound. London,
UK: Churchill Livingstone; 2004.
10. Coldron Y, Stokes M, Cook K. Lumbar multidusmuscle size does
not differ whether ultrasoundimaging is performed in prone or side
lying. ManTher. 2003;8:161-165.
11. Corneil BD, Olivier E, Richmond FJ, Loeb GE, Mu-noz DP. Neck
muscles in the rhesus monkey. II.Electromyographic patterns of
activation under-lying postures and movements. J
Neurophysiol.2001;86:1729-1749.
12. Crisco JJ, third, Panjabi MM. The intersegmentaland
multisegmental muscles of the lumbarspine. A biomechanical model
comparing lateralstabilizing potential. Spine. 1991;16:793-799.
13. Danneels LA, Vanderstraeten GG, CambierDC, Witvrouw EE, De
Cuyper HJ. CT imaging oftrunk muscles in chronic low back pain
patientsand healthy control subjects. Eur Spine
J.2000;9:266-272.
14. Dietz HP, Wilson PD, Clarke B. The use of peri-neal
ultrasound to quantify levator activity andteach pelvic oor muscle
exercises. Int Urogy-necol J Pelvic Floor Dysfunct.
2001;12:166-168;discussion 168-169.
15. Elliott J, Jull G, Noteboom JT, Darnell R, Gal-loway G,
Gibbon WW. Fatty inltration inthe cervical extensor muscles in
persistentwhiplash-associated disorders: a magneticresonance
imaging analysis. Spine. 2006;31:E847-855.
16. Fitts PM, Posner MI. Human Performance. Bel-mont, CA:
Brooks/Cole; 1967.
17. Fitzmaurice R, Cooper RG, Freemont AJ. A histo-morphometric
comparison of muscle biopsiesfrom normal subjects and patients with
ankylos-ing spondylitis and severe mechanical low backpain. J
Pathol. 1992;163:182A.
18. Granata KP, Marras WS. Cost-benet of musclecocontraction in
protecting against spinal insta-bility. Spine.
2000;25:1398-1404.
19. Hayashi N, Masumoto T, Abe O, Aoki S, OhtomoK, Tajiri Y.
Accuracy of abnormal paraspinalmuscle ndings on contrast-enhanced
MR im-ages as indirect signs of unilateral cervical root-avulsion
injury. Radiology. 2002;223:397-402.
20. Henry SM, Westervelt KC. The use of real-timeultrasound
feedback in teaching abdominal hol-
lowing exercises to healthy subjects. J OrthopSports Phys Ther.
2005;35:338-345.
21. Hides J, Cooper DH, Stokes MJ. Diagnostic ultra-sound
imaging for measurement of the lumbarmultidus muscle in normal
young adults. Phys-iother Theor Pract. 1992;8:19-26.
22. Hides J, Gilmore C, Stanton W, Bohlscheid E.Multidus size
and symmetry among chronicLBP and healthy asymptomatic subjects.
ManTher. 2006 Oct 26; [Epub ahead of print].
23. Hides JA, Jull GA, Richardson CA. Long-term ef-fects of
specic stabilizing exercises for rst-ep-isode low back pain. Spine.
2001;26:E243-248.
24. Hides JA, Richardson CA, Jull G. Use of real-time ultrasound
imaging for feedback in reha-bilitation. Man Ther.
1998;3:125-131.
25. Hides JA, Richardson CA, Jull GA. Magneticresonance imaging
and ultrasonography of thelumbar multidus muscle. Comparison of
twodifferent modalities. Spine. 1995;20:54-58.
26. Hides JA, Richardson CA, Jull GA. Multidusmuscle recovery is
not automatic after resolu-tion of acute, rst-episode low back
pain. Spine.1996;21:2763-2769.
27. Hides JA, Stokes MJ, Saide M, Jull GA, CooperDH. Evidence of
lumbar multidus musclewasting ipsilateral to symptoms in
patientswith acute/subacute low back pain.
Spine.1994;19:165-172.
28. Hodges P, Holm AK, Hansson T, Holm S. Rapidatrophy of the
lumbar multidus follows ex-perimental disc or nerve root injury.
Spine.2006;31:2926-2933.
29. Hodges PW, Pengel LH, Herbert RD, Gande-via SC. Measurement
of muscle contractionwith ultrasound imaging. Muscle
Nerve.2003;27:682-692.
30. Kader DF, Wardlaw D, Smith FW. Correla-tion between the MRI
changes in the lumbarmultidus muscles and leg pain. Clin
Radiol.2000;55:145-149.
31. Kaigle AM, Holm SH, Hansson TH. Experi-mental instability in
the lumbar spine. Spine.1995;20:421-430.
32. Kelley SM. The Effect of Two Exercise ProgramsFollowing Back
Surgery [thesis]. Queensland,Australia: University of Queensland;
2005.
33. Kiesel KB, Uhl T, Underwood FB, Nitz AJ. Re-habilitative
ultrasound measurement of selecttrunk muscle activation during
induced pain.Man Ther. 2006 Dec 30; [Epub ahead of print].
34. Kiesel KB, Uhl TL, Underwood FB, Rodd DW, NitzAJ.
Measurement of lumbar multidus musclecontraction with
rehabilitative ultrasound imag-ing. Man Ther. 2007;12:161-166.
35. Kjaer P, Bendix T, Sorensen JS, Korsholm L, Le-boeuf-Yde C.
Are MRI-dened fat inltrations inthe multidus muscles associated
with low backpain? BMC Med. 2007;5:2.
36. Kline P. A Handbook of Test Construction. Lon-don, UK:
Methuen; 1986.
37. Kristjansson E. Reliability of ultrasonographyfor the
cervical multidus muscle in asymp-tomatic and symptomatic subjects.
Man Ther.2004;9:83-88.
useful for distinguishing the biome-chanical behavior of these
tissues.53,79 Itwould be of interest to know if the ratio
ofnoncontractile tissue to contractile tissuecan be altered with
therapeutic exercise.Elastography may also help distinguishbetween
activity of the deep and super-cial parts of muscle to study their
differ-ing functions.
The effects of different pathologieson the paraspinal muscles
need to beestablished in musculoskeletal and neu-rological
disorders. Large randomizedcontrolled trials are needed to
demon-strate that RUSI is a reliable outcomemeasure for assessing
the effects of in-terventions. We recommend that futurestudies
present data consistently and usethe same statistical methods, as
outlinedby Whittaker et al79 to enable valid com-parison between
studies and to enhanceaccumulation of large reference databas-es as
a common resource for evaluationof abnormality.
ACKNOWLEDGEMENTS
We thank the following forproviding images for the gures:Dr
Cliff Barnes, Associate Pro-
fessor in charge of Neuroanatomy in theDepartment of Physical
Therapy at RegisUniversity, Denver, for help with produc-ing the
image of the cadaver dissectionin FIGURE 1; Nick Smith, Peter
Worsley,and Martin Warner, School of HealthProfessions and
Rehabilitation Sciences,University of Southampton, UK, for
theultrasound scan in FIGURE 4. T
-
journal of orthopaedic & sports physical therapy | volume 37
| number 10 | october 2007 | 595
38. Laasonen EM. Atrophy of sacrospinal musclegroups in patients
with chronic, diffuselyradiating lumbar back pain.
Neuroradiology.1984;26:9-13.
39. Lee JP, Tseng WY, Shau YW, Wang CL, Wang HK,Wang SF.
Measurement of segmental cervicalmultidus contraction by
ultrasonography in as-ymptomatic adults. Man Ther.
2007;12:286-294.
40. Lee SW, Chan CK, Lam TS, et al. Relation-ship between low
back pain and lumbarmultidus size at different postures.
Spine.2006;31:2258-2262.
41. Lord SM, Barnsley L, Wallis BJ, Bogduk N.Chronic cervical
zygapophysial joint pain afterwhiplash. A placebo-controlled
prevalencestudy. Spine. 1996;21:1737-1744; discussion1744-1745.
42. MacDonald D, Moseley GL, Hodges PW. Thefunction of the
lumbar multidus in unilaterallow back pain. Proceedings of World
Congress ofLow Back and Pelvic Pain. Melbourne,
Australia;2004:329.
43. Macintosh JE, Bogduk N. 1987 Volvo award inbasic science.
The morphology of the lumbarerector spinae. Spine.
1987;12:658-668.
44. Macintosh JE, Valencia F, Bogduk N, Munro RR.The morphology
of the human lumbar multi-dus. Clin Biomech. 1986;1:196-204.
45. Mayer TG, Vanharanta H, Gatchel RJ, et al.Comparison of CT
scan muscle measurementsand isokinetic trunk strength in
postoperativepatients. Spine. 1989;14:33-36.
46. Mayoux-Benhamou MA, Revel M, ValleeC. Selective
electromyography of dorsalneck muscles in humans. Exp Brain
Res.1997;113:353-360.
47. McGill SM. Kinetic potential of the lumbartrunk musculature
about three orthogonalorthopaedic axes in extreme postures.
Spine.1991;16:809-815.
48. McGill SM, Grenier S, Kavcic N, Cholewicki J.Coordination of
muscle activity to assure stabil-ity of the lumbar spine. J
Electromyogr Kinesiol.2003;13:353-359.
49. McMeeken JM, Beith ID, Newham DJ, Milligan P,Critchley DJ.
The relationship between EMG andchange in thickness of transversus
abdominis.Clin Biomech (Bristol, Avon). 2004;19:337-342.
50. Mengiardi B, Schmid MR, Boos N, et al. Fat con-tent of
lumbar paraspinal muscles in patientswith chronic low back pain and
in asymptomaticvolunteers: quantication with MR
spectroscopy.Radiology. 2006;240:786-792.
51. Moseley GL, Hodges PW, Gandevia SC. Deepand supercial bers
of the lumbar multidusmuscle are differentially active during
voluntaryarm movements. Spine. 2002;27:E29-36.
52. Nolan JP, Jr., Sherk HH. Biomechanical evalua-tion of the
extensor musculature of the cervicalspine. Spine. 1988;13:9-11.
53. Ophir J, Cespedes I, Ponnekanti H, Yazdi Y, Li
X.Elastography: a quantitative method for imag-ing the elasticity
of biological tissues. UltrasonImaging. 1991;13:111-134.
54. OSullivan C, Bentman S, Bennett K, Stokes
M. Rehabilitative ultrasound imaging of thelower trapezius
muscle: technical descriptionand reliability. J Orthop Sports Phys
Ther.2007;37(10):620-626.
55. Panjabi M, Abumi K, Duranceau J, Ox-land T. Spinal stability
and intersegmentalmuscle forces. A biomechanical model.
Spine.1989;14:194-200.
56. Panjabi MM, Cholewicki J, Nibu K, Grauer JN, Ba-bat LB,
Dvorak J. Mechanism of whiplash injury.Clin Biomech (Bristol,
Avon). 1998;13:239-249.
57. Parkhurst TM, Burnett CN. Injury and proprio-ception in the
lower back. J Orthop Sports PhysTher. 1994;19:282-295.
58. Portney LG, Watkins MP. Foundations of ClinicalResearch:
Applications to Practice. London, UK:Prentice-Hall Health;
2000.
59. Pressler JF, Heiss DG, Buford JA, Chidley JV.Between-day
repeatability and symmetry ofmultidus cross-sectional area measured
usingultrasound imaging. J Orthop Sports Phys
Ther.2006;36:10-18.
60. Quint U, Wilke HJ, Shirazi-Adl A, ParnianpourM, Loer F,
Claes LE. Importance of the inter-segmental trunk muscles for the
stability of thelumbar spine. A biomechanical study in vitro.Spine.
1998;23:1937-1945.
61. Rankin G, Stokes M, Newham DJ. Size andshape of the
posterior neck muscles measuredby ultrasound imaging: normal values
inmales and females of different ages. Man
Ther.2005;10:108-115.
62. RezaSoltani A, Kallinen M, Malkia E, Vihko V.Ultrasonography
of the neck splenius capitismuscle. Investigation in a group of
young healthywomen. Acta Radiol. 1996;37:647-650.
63. RezaSoltani A, Kallinen M, Malkia E, Vihko V.Neck
semispinalis capitis muscle size in sittingand prone positions
measured by real-timeultrasonography. Clin Rehabil.
1998;12:36-44.
64. Shi J, Zheng YP, Chen X, Huang QH. Assessmentof muscle
fatigue using sonomyography: musclethickness change detected from
ultrasound im-ages. Med Eng Phys. 2007;29:472-479.
65. Siegmund GP, Myers BS, Davis MB, BohnetHF, Winkelstein BA.
Mechanical evidence ofcervical facet capsule injury during
whiplash:a cadaveric study using combined shear,compression, and
extension loading. Spine.2001;26:2095-2101.
66. Sihvonen T, Herno A, Paljarvi L, Airaksinen O,Partanen J,
Tapaninaho A. Local denervationatrophy of paraspinal muscles in
postoperativefailed back syndrome. Spine. 1993;18:575-581.
67. Springer BA, Mielcarek BJ, Neseld TK, TeyhenDS.
Relationships among lateral abdominalmuscles, gender, body mass
index, and handdominance. J Orthop Sports Phys
Ther.2006;36:289-297.
68. Stokes M, Rankin G, Newham DJ. Ultrasoundimaging of lumbar
multidus muscle: normalreference ranges for measurements and
prac-tical guidance on the technique. Man Ther.2005;10:116-126.
69. Stokes M, Young A. The contribution of reex in-
hibition to arthrogenous muscle weakness. ClinSci (Lond).
1984;67:7-14.
70. Stokes MJ, Cooper RG, Jayson MIV. Selectivechanges in
multidus dimensions in patientswith chronic low back pain. Eur
Spine J.1992;1:38-42.
71. Takebe K, Vitti M, Basmajian JV. The functionsof
semispinalis capitis and splenius capitismuscles: an
electromyographic study. Anat Rec.1974;179:477-480.
72. Tsubahara A, Chino N, Akaboshi K, OkajimaY, Takahashi H.
Age-related changes of waterand fat content in muscles estimated by
mag-netic resonance (MR) imaging. Disabil
Rehabil.1995;17:298-304.
73. Uetani M, Hayashi K, Hashmi R, Nakahara N,Aso N, Ito N.
Traction injuries of the brachialplexus: signal intensity changes
of the posteriorcervical paraspinal muscles on MRI. J ComputAssist
Tomogr. 1997;21:790-795.
74. Van K, Hides JA, Richardson CA. The use ofreal-time
ultrasound imaging for biofeedbackof lumbar multidus muscle
contraction inhealthy subjects. J Orthop Sports Phys
Ther.2006;36:920-925.
75. Vasseljen O, Dahl HH, Mork PJ, Torp HG. Muscleactivity onset
in the lumbar multidus musclerecorded simultaneously by ultrasound
imagingand intramuscular electromyography. Clin Bio-mech (Bristol,
Avon). 2006;21:905-913.
76. Wallwork T, Hides J, Stanton W, Belavy D. Intra-rater and
interrater reliability of assessment oflumbar multidus muscle
thickness using real-time ultrasound imaging. J Orthop Sports
PhysTher. 2007;37(10):608-612.
77. Wallwork TL. The Effect of Chronic Low BackPain on the Size
and Activation of the LumbarMultidus Muscle [thesis]. Queensland,
Austra-lia: University of Queensland; 2006.
78. Watanabe K, Miyamoto K, Masuda T, Shimizu K.Use of
ultrasonography to evaluate thickness ofthe erector spinae muscle
in maximum exionand extension of the lumbar spine.
Spine.2004;29:1472-1477.
79. Whittaker JL, Teyhen DS, Elliott J, et al. Reha-bilitative
ultrasound imaging: understanding thetechnology and its
applications. J Orthop SportsPhys Ther. 2007;37:434-449.
80. Wilke HJ, Wolf S, Claes LE, Arand M, Wiesend A.Stability
increase of the lumbar spine with dif-ferent muscle groups. A
biomechanical in vitrostudy. Spine. 1995;20:192-198.
81. Winkelstein BA, McLendon RE, Barbir A, MyersBS. An
anatomical investigation of the humancervical facet capsule,
quantifying muscle inser-tion area. J Anat. 2001;198:455-461.
82. Winkelstein BA, Nightingale RW, Richardson WJ,Myers BS. The
cervical facet capsule and its rolein whiplash injury: a
biomechanical investiga-tion. Spine. 2000;25:1238-1246.
@ MORE INFORMATIONWWW.JOSPT.ORG
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/CropGrayImages false /GrayImageMinResolution 150
/GrayImageMinResolutionPolicy /OK /DownsampleGrayImages true
/GrayImageDownsampleType /Bicubic /GrayImageResolution 150
/GrayImageDepth -1 /GrayImageMinDownsampleDepth 2
/GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages true
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/CropMonoImages false /MonoImageMinResolution 300
/MonoImageMinResolutionPolicy /OK /DownsampleMonoImages true
/MonoImageDownsampleType /Bicubic /MonoImageResolution 300
/MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000
/EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode
/MonoImageDict > /AllowPSXObjects true /CheckCompliance [ /None
] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false
/PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000
0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true
/PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXOutputIntentProfile () /PDFXOutputConditionIdentifier ()
/PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped
/False
/Description > /Namespace [ (Adobe) (Common) (1.0) ]
/OtherNamespaces [ > /FormElements false /GenerateStructure true
/IncludeBookmarks false /IncludeHyperlinks false
/IncludeInteractive false /IncludeLayers false /IncludeProfiles
true /MarksOffset 6 /MarksWeight 0.250000 /MultimediaHandling
/UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ]
/PDFXOutputIntentProfileSelector /NA /PageMarksFile /RomanDefault
/PreserveEditing false /UntaggedCMYKHandling /UseDocumentProfile
/UntaggedRGBHandling /UseDocumentProfile /UseDocumentBleed false
>> > ]>> setdistillerparams> setpagedevice