Embed Size (px)
Citation preview
Ovarian Cancer CMG – January 2010 Final Version
REGIONAL GYNAECOLOGY GROUP
Document Title
Guidelines for the Screening, Investigation and Management of Ovarian Cancers
Document Date
January 2010 – Version 4 - Final
Document Purpose
This guidance has been produced to support the diagnosis, treatment and management of ovarian cancer Treatment decisions for individual patients require the weighing of a multiplicity of factors, which cannot all be accounted for in a CMG. The CMG provides a description of the range of treatment options available for a clinical scenario. To maximise the benefit of multiprofessional working management strategies for the individual are best discussed with a multidisciplinary meeting (MDM)
Authors
Dr Ian Harley, Consultant Gynaecologist Prof Glen McCluggage, Consultation Pathologist Dr Sarah McKenna, Consultant Oncologist Dr Joanne Millar, Consultant Oncologist Dr Geoff McCracken, Consultant Gynaecologist Ms Wendy Cunnigham, Clinical Trials Ms Maureen Clarke, Patient Representative Ms Elish McColgan, Clinical Nurse Specialist Ms Pippa McCabe, Physiotherapist
Version Changes
Changes made to version 3 by Dr Ian Harley, Dec 09 Appendix 2 score for Menopause changed from
4 to 3 Ms Pippa McCabe changed lymphodema paragraph – Dec 09
Ovarian Cancer CMG – January 2010 Final Version
INTRODUCTION Ovarian cancer is the primary cause of mortality among gynaecological
malignancies. The lifetime risk of ovarian cancer by age 75 years, in women
from developed countries, is approximately 1 in 70 (Risch H.A, 2001). The
median age at diagnosis is 60 years. In Northern Ireland ovarian cancer
accounts for 4% of all cancers registered and is the commonest
gynaecological malignancy. There are approximately 168 cases diagnosed
annually in Northern Ireland. The mean overall survival is 32 months. (Cancer
registry Northern Ireland)
Primary ovarian tumours are histologically classified into those that are
epithelial (implying an origin from the surface / coelomic epithelium), those
that are of sex cord -stromal type, and originating from sex cord mesenchymal
elements), and those that are of germ cell type (originating from germ cells).
The majority of primary tumours (85-90%) are epithelial in origin (Im D.D,
2001). Less commonly ovarian tumours may be metastatic from other primary
sites, including non-gynaecological tumours.
Epithelial tumours are further classified into distinct histological/morphological
sub-groups (mainly serous, endometrioid, cleat cell and mucinous) based on
microscopic appearances. A simplified version of the WHO classification for
ovarian tumours is illustrated in Appendix 1.
The majority of ovarian tumours are sporadic. However, 12% are familial
cancers, due to an underlying genetic defect. Mutations in the BRCA1 and
BRCA2 genes account for the majority (75-90%) of familial epithelial ovarian
cancers, followed by mutations in Mismatch Repair genes (5-12%). Women
with a BRCA1 or BRCA2 gene mutation have a 40-60% and 20-40% lifetime
risk of developing epithelial ovarian cancer by age 75 years respectively. Risk
of borderline and non-epithelial tumours do not appear to be greater in BRCA
1/2 carriers than the background risk within the population.
Ovarian Cancer CMG – January 2010 Final Version
Patients with ovarian cancer commonly present with vague symptoms and
signs. Consequently, most patients (85%) present with advanced disease.
Thus a minority will present with early stage disease. In women with
macroscopic disease confined to the ovary 25% will have a normal Ca125.
30% will have microscopic spread to the lymph nodes and 22% will be
upstaged by a comprehensive surgical staging procedure.
Surgery is the primary treatment of choice. The aim of surgery is to remove as
much tumour as is possible, provide surgical staging and histological
diagnosis. Residual disease after initial surgery remains one of the most
important variables in the prognosis for women with epithelial ovarian
carcinoma (EOC). Although there are no randomized studies, nor are there
likely to be, the best evidence available has resulted in cytoreductive surgery
being the primary treatment in EOC. The aim is to debulk the tumour to less
than 1cm of residual disease remaining in any site of the abdomino-pelvic
cavity. If achieved, this is termed “optimal cytoreduction (debulking)”.
A meta-analysis by Bristow et all (2002) of 81 cohorts of patients (totalling
6,885 cases) of stage III or IV EOC identified a significant improvement in
survival in women who had maximal cytoreductive surgery. Maximal
cytoreductive surgery was defined according to the largest diameter of
residual disease. 95% of studies used 1cm or 2cm as discriminating criteria.
Cohorts with <25% maximal cytoreduction had a mean weighted median
survival of 22.7 months. This is in contrast to cohorts with >75% maximal
cytoreduction who had a mean weighted median survival of 33.9 months
(p<0.001). This correlation remained after controlling for other prognostic
variables.
Following surgery adjuvant chemotherapy is usually recommended in
advanced tumours and selected early stage disease.
Ovarian Cancer CMG – January 2010 Final Version
SCREENING FOR OVARIAN CANCER As stated above, in the general population the lifetime risk of developing
ovarian cancer by the age of 75 years is 1.4% (1 in 70). In the absence of a
mutation in BRCA 1/2 the relative risk for women with one affected first
degree relative is 3.1 (95% CI 0.3-1.6), ie: the lifetime risk is increased to
4.3%. When more than one relative is affected (first or second degree) the
relative risk is increased to 11.7 (95% CI 5.3 – 25.9), ie: the lifetime risk is
increased to 16.38%.(Stratton J F).
Patients with a strong family history of malignancy (including ovary, breast,
bowel, pancreatic and prostate) should be referred to medical genetics for a
risk assessment.
Only those patients testing positive for BRCA1/2, HNPCC or on recommendation of medical genetics should be referred to the familial ovarian cancer screening clinic for ovarian screening or prophylactic surgery. The UKTOCS trial of ovarian cancer screening in the general population does
not currently provide enough evidence to support the screening of
asymptomatic women in the general population (Menon U et al Lancet 2009).
Screening asymptomatic low risk women may lead to a larger number of
unnecessary surgical interventions. However, the mature data should be
available in 2014, including the outcome for unscreened women.
The evidence does support screening high risk women for Ovarian Cancer.
Screening methods currently used include a combination of history,
examination, ultrasound scan of pelvis and Ca125.
Women considered at high risk of ovarian cancer should be counselled for prophylactic surgery. The minimal surgical intervention should be a laparoscopic (or open if unsuitable for minimum access surgery) bilateral salpingo-oophorectomy. There is currently no data to support hysterectomy in addition to a BSO for prophylaxis of malignancy in patients with BRCA1/2 mutation.
Ovarian Cancer CMG – January 2010 Final Version
HRT therapy after Prophylactic Surgery in BRCA 1/2 mutation carriers Approximately 3% of invasive breast cancers are attributed to BRCA1 and 2
(Newman B 1998). Women who carry a mutation in the BRCA 1 gene have a
60-80% lifetime risk of developing breast cancer. This risk can be reduced by
50% with prophylactic oophorectomy before menopause (Eisen A 2005,
Rebbeck T 2009). Because the reduction of risk is believed to be due to the
withdrawal of ovarian hormones, there is concern about the administration of
exogenous hormones in women with the BRCA 1 or BRCA 2 mutation, to
alleviate climacteric symptoms.
In case control studies, BRCA1 and BRCA 2 carriers, who have had
prophylactic BSO and are prescribed HRT, do not appear to loose the risk
reduction for breast cancer (Rebbeck T 2005, Eisen A 2008). In these studies
there appeared to be no difference in HRT preparation (Oestrogen alone or
combined oestrogen and progesterone).
BRCA 1 and BRCA 2 carriers who undergo prophylactic BSO should be
carefully counseled of the effects of surgical menopause before surgery is performed. Post operative use of HRT should be discussed, including
alternative treatments to relieve menopausal symptoms and prevent
osteoporosis. Patients may be offered referral to the HRT clinic.
Ovarian Cancer CMG – January 2010 Final Version
DIAGNOSIS Suspicion for ovarian cancer should be made by the GP, Medical / Surgical
clinician or Gynaecologist on taking a good clinical history and full
examination. Appropriate initial investigations should be carried out on all
women with a suspected ovarian malignancy before referral to the Lead
Clinician of the Gynae. Cancer Unit.
Investigations should include:
Ultrasound scanning,
relevant tumour markers (Epithelial: Ca125, Ca19-9 and CEA Germ
Cell: AFP, hCG and LDH Sex Cord Stromal: Inhibin ) [Germ cell
tumour markers should always be considered in younger women. It
may be useful in young people to perform a serum calcium since
ovarian small cell carcinoma of hypercalcaemic type, a rare but
aggressive form of ovarian malignancy in young women, is associated
in most cases with a raised serum level]
+/- CT / MRI scan.
These initial investigations may be supplemented by cytology or histology
where appropriate.
To avoid treatment delay diagnostic work up should be completed in a timely fashion with advice from the Unit Lead Clinician if required.
All General Gynaecologists and Gynaecological Cancer Unit Lead Clinicians
should calculate the Risk of Malignancy Index (RMI) score in an attempt to
discriminate between benign and malignant ovarian pathology. Calculation of
the RMI is detailed in appendix 2. RMI scores > 250 should be discussed at the Specialist Gynae. Oncology MDT.
25% of women with an early stage epithelial malignancy confined to the ovary
may have a normal Ca125. Therefore in some women the RMI may fall below
250. However, if radiological imaging shows complex features and
malignancy is suspected, the case must be reviewed, with all relevant
investigations, at the Regional Gynae. Oncology MDT. Women with ovarian
lesions associated with normal Ca125, “benign” radiological features and RMI
Ovarian Cancer CMG – January 2010 Final Version
<250 should not be referred to the Regional MDT unless abnormal pathology
is reported.
All suspected or diagnosed cases of ovarian cancer must be presented to the
Regional Gynaecological MDT for discussion and a management plan
constructed. All relevant investigations should be made available to the
Regional MDT in a timely fashion, prior to the patients case discussion. This
should include:
clinical history,
radiological/haematological/cytological/histological investigations; and
calculation of the RMI.
All histopathology should have a central review by a Consultant pathologist
within the MDT. All relevant radiological imaging should be reviewed by
Consultant radiologists within the MDT.
TREATMENT A treatment plan for each case must be discussed and documented at the
Regional Gynaecological MDT. All those involved in the patient care should
have access to the MDT documentation and treatment plan. Treatment should
be discussed with the patient as early as possible. Patients should not be
given an appointment for treatment until diagnosis has been discussed with
the patient by the referring clinician.
If a patient is not fit for surgery, or optimal debulking is felt to be unachievable,
a tissue diagnosis must be obtained before commencing alternative
treatment. Cytology alone is not sufficient for a patient be started on
chemotherapy.
1. Surgery Outside the setting of clinical trials, patients should be offered primary
surgery, if appropriate.
Ovarian Cancer CMG – January 2010 Final Version
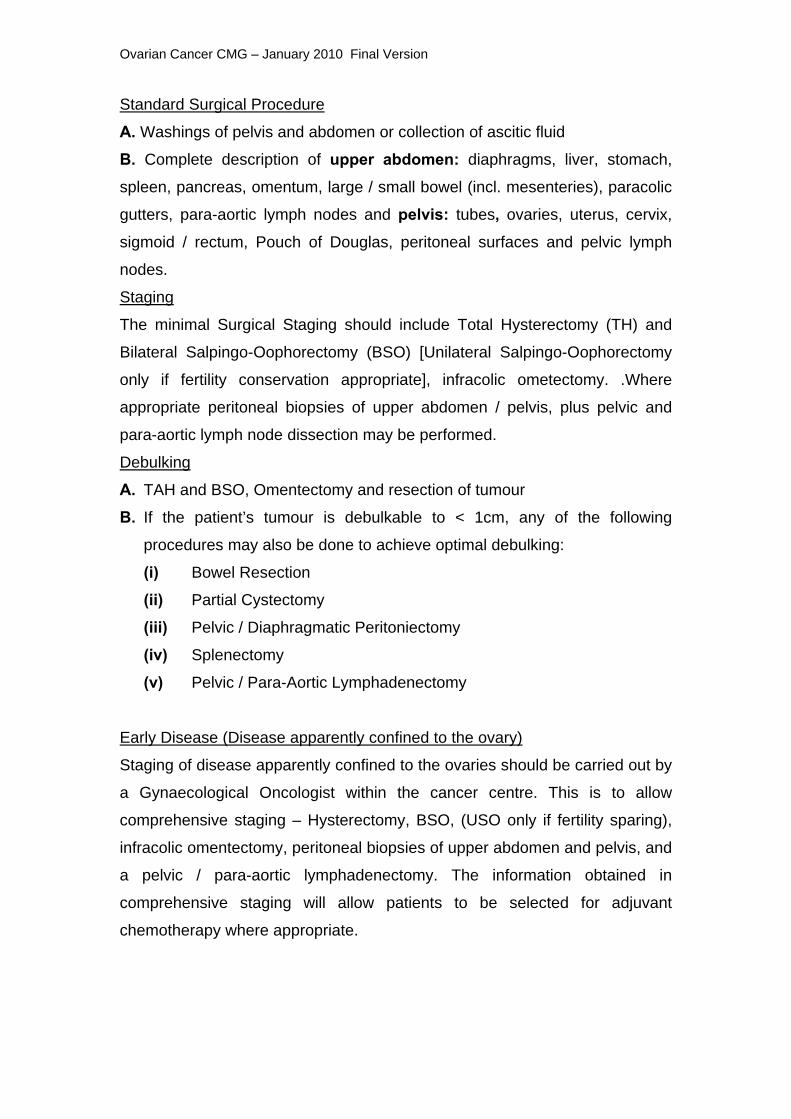
Standard Surgical Procedure
A. Washings of pelvis and abdomen or collection of ascitic fluid
B. Complete description of upper abdomen: diaphragms, liver, stomach,
spleen, pancreas, omentum, large / small bowel (incl. mesenteries), paracolic
gutters, para-aortic lymph nodes and pelvis: tubes, ovaries, uterus, cervix,
sigmoid / rectum, Pouch of Douglas, peritoneal surfaces and pelvic lymph
nodes.
Staging
The minimal Surgical Staging should include Total Hysterectomy (TH) and
Bilateral Salpingo-Oophorectomy (BSO) [Unilateral Salpingo-Oophorectomy
only if fertility conservation appropriate], infracolic ometectomy. .Where
appropriate peritoneal biopsies of upper abdomen / pelvis, plus pelvic and
para-aortic lymph node dissection may be performed.
Debulking
A. TAH and BSO, Omentectomy and resection of tumour
B. If the patient’s tumour is debulkable to < 1cm, any of the following
procedures may also be done to achieve optimal debulking: (i) Bowel Resection
(ii) Partial Cystectomy
(iii) Pelvic / Diaphragmatic Peritoniectomy
(iv) Splenectomy
(v) Pelvic / Para-Aortic Lymphadenectomy
Early Disease (Disease apparently confined to the ovary)
Staging of disease apparently confined to the ovaries should be carried out by
a Gynaecological Oncologist within the cancer centre. This is to allow
comprehensive staging – Hysterectomy, BSO, (USO only if fertility sparing),
infracolic omentectomy, peritoneal biopsies of upper abdomen and pelvis, and
a pelvic / para-aortic lymphadenectomy. The information obtained in
comprehensive staging will allow patients to be selected for adjuvant
chemotherapy where appropriate.

Ovarian Cancer CMG – January 2010 Final Version
Staging of Borderline Tumours
Borderline tumours account for 10-15% of all ovarian tumours. Most are of a
serous or mucinous subtype. 7-18% of serous borderline tumours have lymph
node spread. All borderline tumours should be discussed at the Regional MDT.
The minimal staging for borderline tumours should include a Hysterectomy
and BSO (USO / cystectomy alone if fertility sparing), plus infracolic
omentectomy. Pelvic and para-aortic lymphadenectomy should be considered
in serous borderline tumours.
Frequently the histological diagnosis of a borderline cystadenoma comes after
surgery for a tumour thought to be benign. Therefore a staging procedure may
not have been conducted. Restaging should be discussed at the MDT and
based on additional information (histological subtype, radiological evidence of
incompletely excised disease and patient’s fitness for surgery).
Restaging
Patients who have had a diagnosis of ovarian cancer following a previous
surgical procedure, but have not been comprehensively surgically staged
should be offered further staging surgery if:
(i) restaging (laparotomy / laparoscopy) will provide additional
information that will impact on treatment or prognosis
(ii) restaging will spare an individual from chemotherapy (i.e.
apparent stage 1, grade 1/2 with no staging including
omentectomy and lymphadenectomy).
Surgery following relapse after primary surgery
Patients who have a clinically isolated (confirmed radiological) recurrence
should be considered for surgery where there is a disease free interval > 12
months.
Ovarian Cancer CMG – January 2010 Final Version
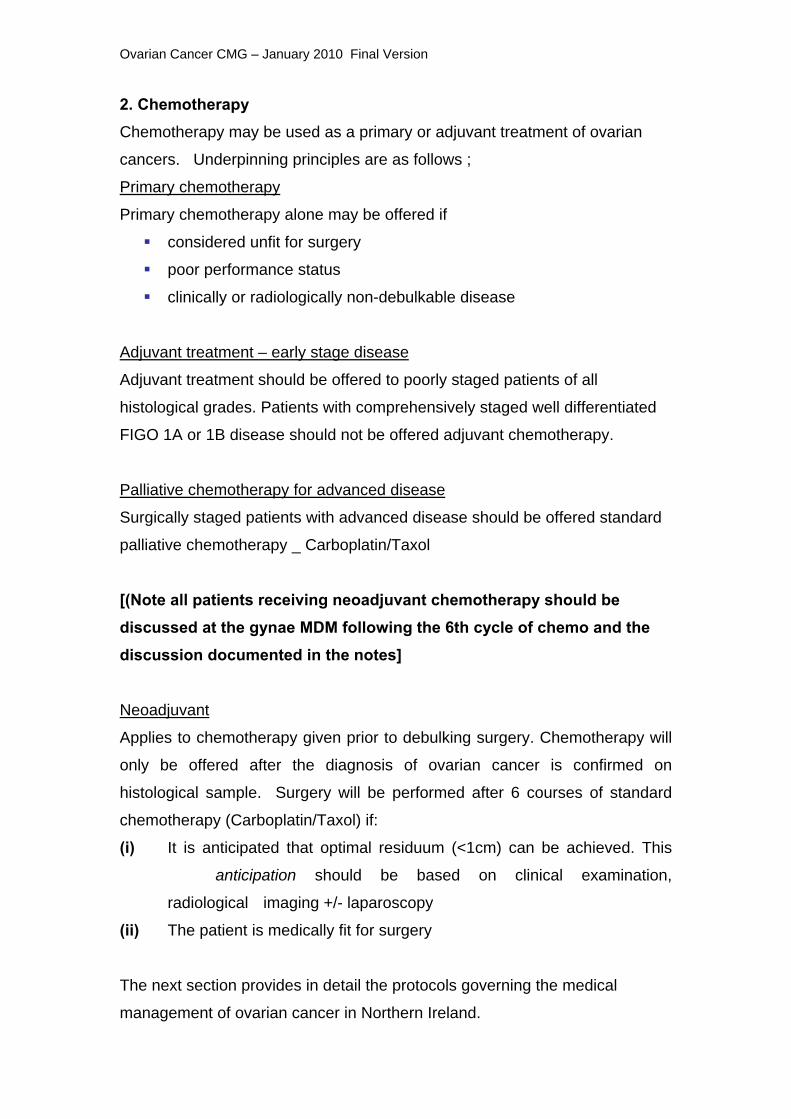
2. Chemotherapy Chemotherapy may be used as a primary or adjuvant treatment of ovarian
cancers. Underpinning principles are as follows ;
Primary chemotherapy
Primary chemotherapy alone may be offered if
considered unfit for surgery
poor performance status
clinically or radiologically non-debulkable disease
Adjuvant treatment – early stage disease
Adjuvant treatment should be offered to poorly staged patients of all
histological grades. Patients with comprehensively staged well differentiated
FIGO 1A or 1B disease should not be offered adjuvant chemotherapy.
Palliative chemotherapy for advanced disease
Surgically staged patients with advanced disease should be offered standard
palliative chemotherapy _ Carboplatin/Taxol
[(Note all patients receiving neoadjuvant chemotherapy should be discussed at the gynae MDM following the 6th cycle of chemo and the discussion documented in the notes] Neoadjuvant
Applies to chemotherapy given prior to debulking surgery. Chemotherapy will
only be offered after the diagnosis of ovarian cancer is confirmed on
histological sample. Surgery will be performed after 6 courses of standard
chemotherapy (Carboplatin/Taxol) if:
(i) It is anticipated that optimal residuum (<1cm) can be achieved. This
anticipation should be based on clinical examination,
radiological imaging +/- laparoscopy
(ii) The patient is medically fit for surgery
The next section provides in detail the protocols governing the medical
management of ovarian cancer in Northern Ireland.
Ovarian Cancer CMG – January 2010 Final Version
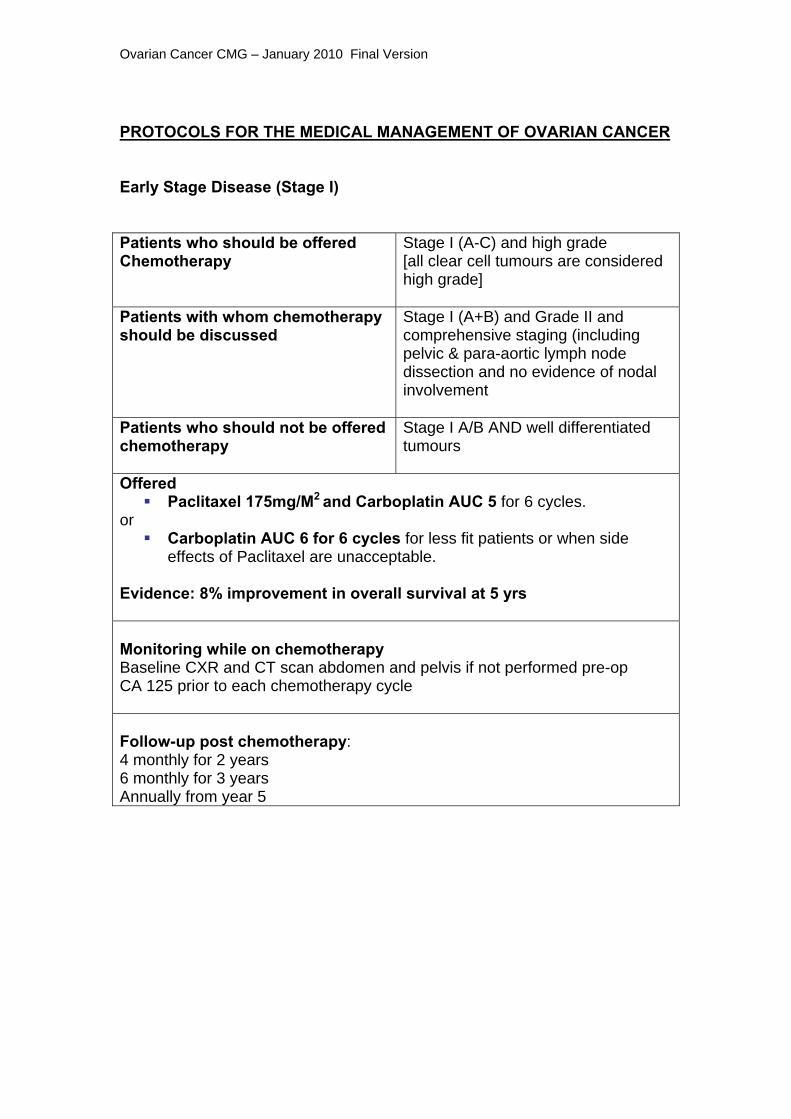
PROTOCOLS FOR THE MEDICAL MANAGEMENT OF OVARIAN CANCER Early Stage Disease (Stage I)
Patients who should be offered Chemotherapy
Stage I (A-C) and high grade [all clear cell tumours are considered high grade]
Patients with whom chemotherapy should be discussed
Stage I (A+B) and Grade II and comprehensive staging (including pelvic & para-aortic lymph node dissection and no evidence of nodal involvement
Patients who should not be offered chemotherapy
Stage I A/B AND well differentiated tumours
Offered Paclitaxel 175mg/M2 and Carboplatin AUC 5 for 6 cycles.
or Carboplatin AUC 6 for 6 cycles for less fit patients or when side
effects of Paclitaxel are unacceptable. Evidence: 8% improvement in overall survival at 5 yrs Monitoring while on chemotherapy Baseline CXR and CT scan abdomen and pelvis if not performed pre-op CA 125 prior to each chemotherapy cycle Follow-up post chemotherapy: 4 monthly for 2 years 6 monthly for 3 years Annually from year 5

Ovarian Cancer CMG – January 2010 Final Version
Advanced Ovarian Cancer (Stage 2-4)
Post Surgical Debulking OR Neoadjuvant Treatment for Patients unfit for chemotherapy or whose disease is not optimally debulkable.
Offered
Paclitaxel 175mg/M2 and Carboplatin AUC5 for 6 cycles or
Single agent Carboplatin AUC6 for 6 cycles could be considered for: Patients less medically fit Older patients Evidence: 70-80% response to Paclitaxel/Carboplatin. 60-70% response to Carboplatin Average progression free interval - 1-2yrs Average overall survival 2-3 years BUT small number of long term survivors Monitoring while on chemotherapy Baseline CXR and CT scan abdomen and pelvis No need to repeat if normal If abnormal repeat on completion of 6 cycles of chemotherapy unless there is clinical evidence of disease progression CA 125 prior to each chemotherapy cycle Follow-up post chemotherapy: 4 monthly for 2 years 6 monthly for 3 years Annually from year 5
Ovarian Cancer CMG – January 2010 Final Version
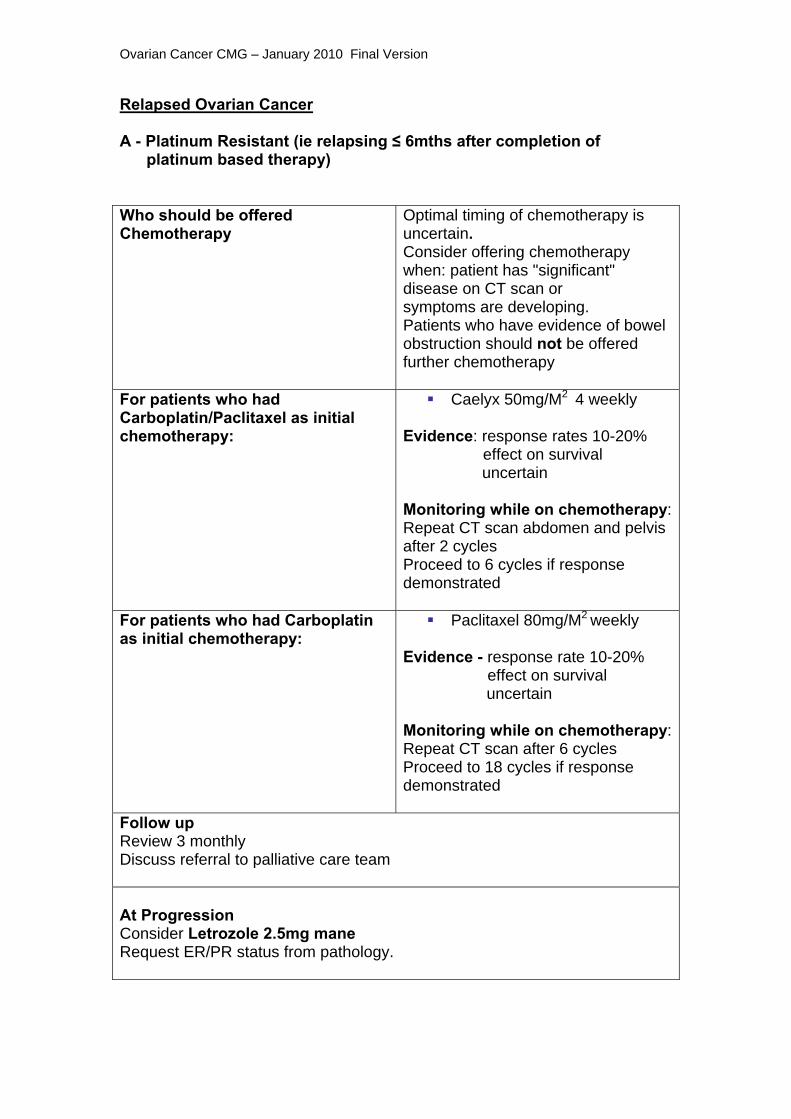
Relapsed Ovarian Cancer A - Platinum Resistant (ie relapsing ≤ 6mths after completion of platinum based therapy) Who should be offered Chemotherapy
Optimal timing of chemotherapy is uncertain. Consider offering chemotherapy when: patient has "significant" disease on CT scan or symptoms are developing. Patients who have evidence of bowel obstruction should not be offered further chemotherapy
For patients who had Carboplatin/Paclitaxel as initial chemotherapy:
Caelyx 50mg/M2 4 weekly Evidence: response rates 10-20% effect on survival uncertain Monitoring while on chemotherapy: Repeat CT scan abdomen and pelvis after 2 cycles Proceed to 6 cycles if response demonstrated
For patients who had Carboplatin as initial chemotherapy:
Paclitaxel 80mg/M2 weekly Evidence - response rate 10-20% effect on survival uncertain Monitoring while on chemotherapy:Repeat CT scan after 6 cycles Proceed to 18 cycles if response demonstrated
Follow up Review 3 monthly Discuss referral to palliative care team At Progression Consider Letrozole 2.5mg mane Request ER/PR status from pathology.

Ovarian Cancer CMG – January 2010 Final Version
B – Partially Platinum Sensitive (ie relapsing 6-12mths following platinum based chemotherapy) Relapsing 6-12mths following platinum based chemotherapy as demonstrated by "significant" disease progression on CT scan or as evidenced by symptoms and rising CA 125. For patients who had Carboplatin/Paclitaxel as initial chemotherapy:
Caelyx 50mg/M2 4 weekly Evidence: response rates 10-30% effect on survival uncertain Monitoring while on chemotherapy: Repeat CT after 2 cycles Proceed to 6 cycles if response demonstrated
For patients who had Carboplatin as initial chemotherapy:
Paclitaxel 80mg/M2 weekly Evidence - response rate 10-20% effect on survival uncertain Monitoring while on chemotherapy:Repeat CT scan after 6 cycles Proceed to 18 cycles if response demonstrated
Follow up Review 3 monthly Discuss referral to palliative care team At Progression At progression: consider Paclitaxel 175mg/M2 Carboplatin AUC 5 or Carboplatin AUC 6 (poor PS or residual neurotoxicity from Paclitaxel) Evidence - response rate 30% probable small improvement in survival Follow up after chemotherapy: review 3 monthly discuss referral to palliative care team At progression: consider Letrozole 2.5mg (request ER/PR status from pathology)
Ovarian Cancer CMG – January 2010 Final Version
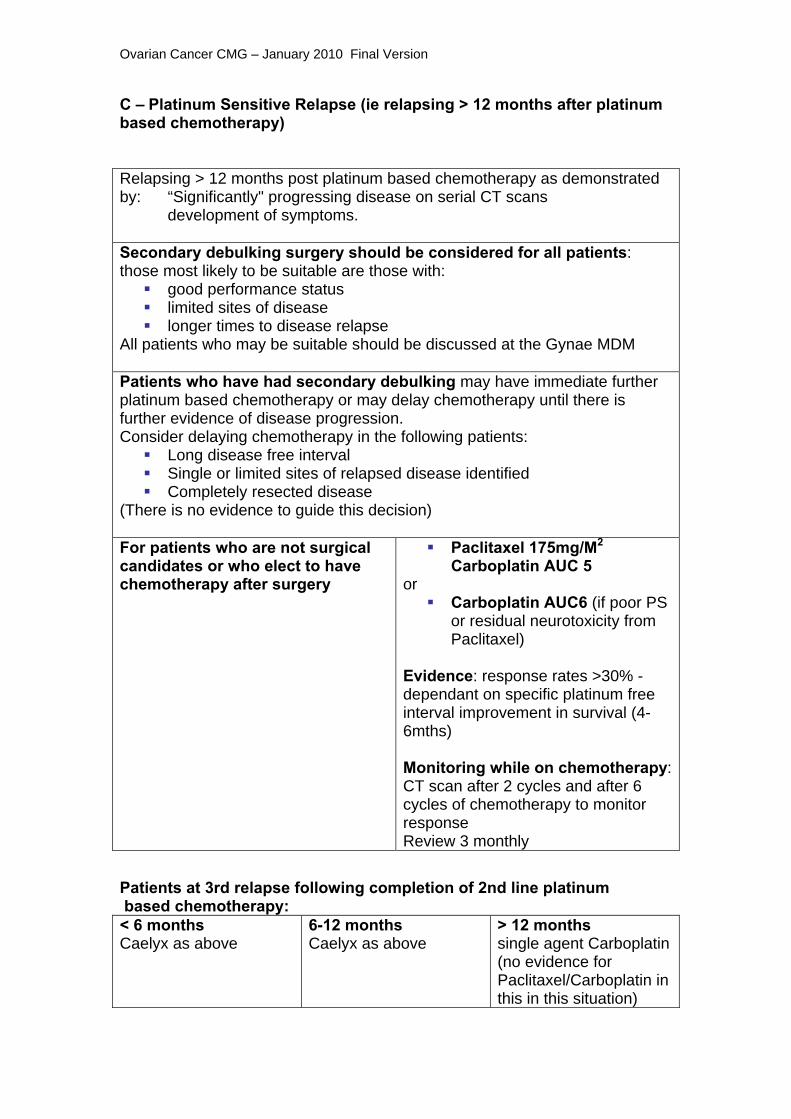
C – Platinum Sensitive Relapse (ie relapsing > 12 months after platinum based chemotherapy) Relapsing > 12 months post platinum based chemotherapy as demonstrated by: “Significantly" progressing disease on serial CT scans development of symptoms. Secondary debulking surgery should be considered for all patients: those most likely to be suitable are those with:
good performance status limited sites of disease longer times to disease relapse
All patients who may be suitable should be discussed at the Gynae MDM Patients who have had secondary debulking may have immediate further platinum based chemotherapy or may delay chemotherapy until there is further evidence of disease progression. Consider delaying chemotherapy in the following patients:
Long disease free interval Single or limited sites of relapsed disease identified Completely resected disease
(There is no evidence to guide this decision) For patients who are not surgical candidates or who elect to have chemotherapy after surgery
Paclitaxel 175mg/M2
Carboplatin AUC 5 or
Carboplatin AUC6 (if poor PS or residual neurotoxicity from Paclitaxel)
Evidence: response rates >30% - dependant on specific platinum free interval improvement in survival (4-6mths) Monitoring while on chemotherapy:CT scan after 2 cycles and after 6 cycles of chemotherapy to monitor response Review 3 monthly
Patients at 3rd relapse following completion of 2nd line platinum based chemotherapy: < 6 months Caelyx as above
6-12 months Caelyx as above
> 12 months single agent Carboplatin (no evidence for Paclitaxel/Carboplatin in this in this situation)

Ovarian Cancer CMG – January 2010 Final Version
SPECIAL CONSIDERATIONS
1. HRT and ovarian cancer: Women premenopausal at time of diagnosis: No evidence of adverse effect
Consider HRT for patients for:
1) Management of acute menopausal symptoms
2) For patients with early stage disease to prevent long term complications of
early menopause (these patients should be referred to the HRT clinic in the
RVH)
Women post menopausal at diagnosis: Little evidence to guide decision
Probably safe for short term use in patients with troublesome acute
symptoms.
References: Estrogen replacement therapy for ovarian cancer survivors-a randomised controlled trial. Guidozzi et al. Cancer 1999 Sept 15;86(6) :1013-8
2. Carboplatin allergies: Carboplatin allergies are well described typically in patients receiving 2nd and
subsequent lines of Carboplatin chemotherapy.
While desensitistation protocols have been described their efficacy is
uncertain.
Our management of Carboplatin allergy is as follows:
Patient should NOT receive further Carboplatin
Patient may be offered Cisplatin 100mg/M2 but should be counselled that
there is some cross reactivity between the 2 drugs and a proportion of
patients may also develop a reaction to Cisplatin References: The dilemna of Carboplatin-associated hypersensitivity reactions in ovarian cancer management. Markman M. Gynecol Oncol. 2007 Nov;107(2):163-5 Use of Cisplatin without desensitisation after Carboplatin hypersensitivity reaction in epithelial ovarian and primary peritoneal cancer. Callahan MB et al. Am J Obstet Gynecol. 2007 Aug;197(2):199
Ovarian Cancer CMG – January 2010 Final Version
Quality of Life Issues Women with ovarian cancer can experience many challenges to their quality
of life, including psychosocial and survivorship issues. From diagnosis, all
women with ovarian cancer should have a named Key Worker, ideally a
Clinical Nurse Specialist, who can co-ordinate the various aspects of their
care, as well as giving information and support. The key worker may change
throughout the patient’s cancer journey, to, for example, Community Hospice
Nurse.
Patients should receive written information on support services available
locally and nationally. Patients having surgery or chemotherapy should
receive written information on their treatment, which includes possible side
effects and risks associated with treatment. Patients having chemotherapy
will be given information on the 24 hour helpline.
From initial presentation onwards, patients may need dietary advice and
symptom management. Referral to a dietician and Palliative Care Team,
either in hospital or the community is beneficial for many patients.
Patients may need assessed regarding ascites if it is affecting their activities
of daily living. It may be appropriate to tap for relief of symptoms, either in the
cancer centre or their referring hospital.
Surgery for ovarian cancer may, in a small number of cases, result in bowel
surgery. For this reason, all patients with suspect ovarian cancer should be
seen by a stoma nurse pre operatively, and have a site marked. This does
increase patient anxiety, but is of huge benefit to the small number of patients
who have stoma formation.
Written information should be given to all patients on how treatment may
affect their sexual functioning, relationships and fertility. Referral to a
counsellor or psychologist is often helpful for patients, and services are
available at the cancer centre or locally.
Ovarian Cancer CMG – January 2010 Final Version
Patients rendered menopausal by their treatment will be advised regarding
risks and benefits of HRT. Post treatment assessment may indicate the need
to refer patients to their local menopause/HRT clinic for ongoing monitoring
and advice.
Lymphodema Lymphoedema is a chronic, life long condition that may occur as a result of
gynaecological surgery and/or radiotherapy involving the lymph nodes. In the
later stages of disease, lymphoedema may also occur when the lymph nodes
are involved in the disease process or when there is increased pressure
within the pelvis.
Written information should be given to all women at risk of developing
lymphoedema pre treatment. Patients who have lymph node dissection or
radiotherapy to lymph nodes are at risk of lymphoedema, and should be
referred to their local lymphoedema team at the first signs, in order to prevent
complex, long term problems. Those lymphoedema patients having
chemotherapy or radiotherapy will be seen in the cancer centre if
lymphoedema is an issue at that time.
Ovarian Cancer CMG – January 2010 Final Version
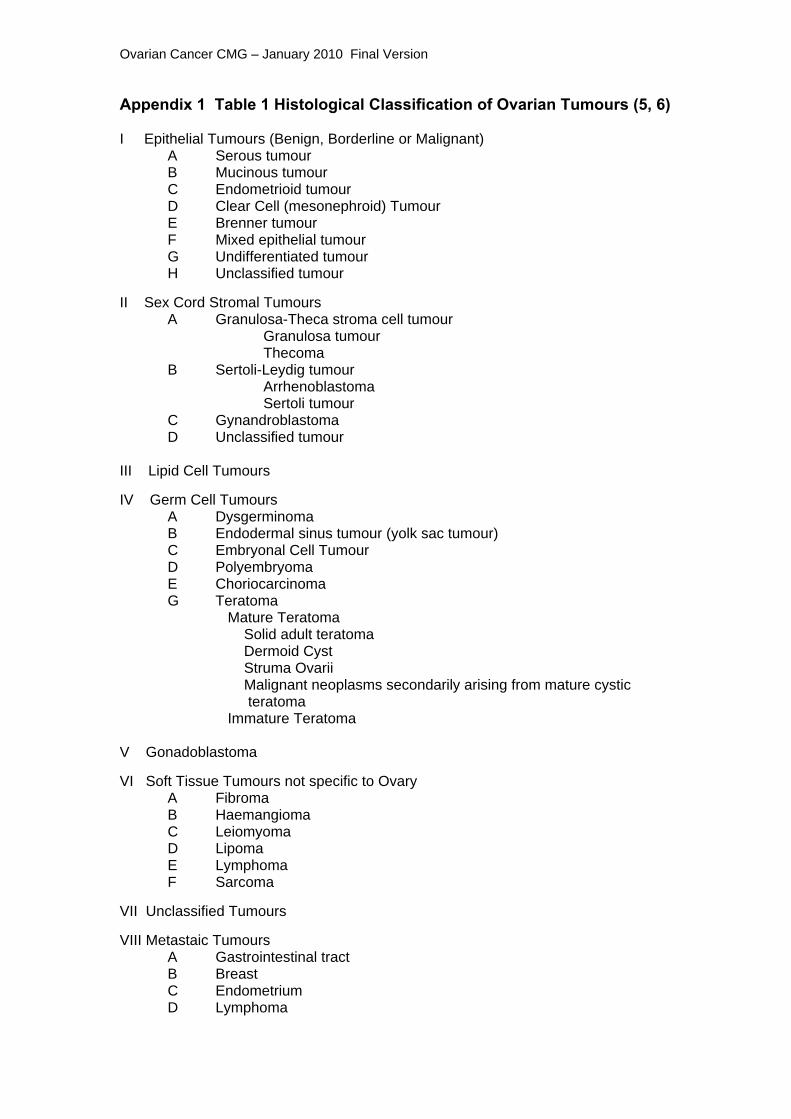
Appendix 1 Table 1 Histological Classification of Ovarian Tumours (5, 6) I Epithelial Tumours (Benign, Borderline or Malignant) A Serous tumour B Mucinous tumour C Endometrioid tumour D Clear Cell (mesonephroid) Tumour E Brenner tumour F Mixed epithelial tumour G Undifferentiated tumour H Unclassified tumour
II Sex Cord Stromal Tumours A Granulosa-Theca stroma cell tumour Granulosa tumour Thecoma B Sertoli-Leydig tumour Arrhenoblastoma Sertoli tumour C Gynandroblastoma D Unclassified tumour III Lipid Cell Tumours
IV Germ Cell Tumours A Dysgerminoma B Endodermal sinus tumour (yolk sac tumour) C Embryonal Cell Tumour D Polyembryoma E Choriocarcinoma G Teratoma Mature Teratoma Solid adult teratoma Dermoid Cyst
Struma Ovarii Malignant neoplasms secondarily arising from mature cystic teratoma
Immature Teratoma
V Gonadoblastoma VI Soft Tissue Tumours not specific to Ovary A Fibroma B Haemangioma C Leiomyoma D Lipoma E Lymphoma F Sarcoma VII Unclassified Tumours VIII Metastaic Tumours A Gastrointestinal tract B Breast C Endometrium D Lymphoma

Ovarian Cancer CMG – January 2010 Final Version
Appendix 2 RISK OF MALIGNANCY INDEX (RMI)
Aim: To define patients with probable Ovarian carcinoma Measurement: RMI index if > 250 then 90% positive predictive
value for ovarian carcinoma RMI index = Menopausal score (M) x Ultrasound score (U) x CA 125 serum level Menopause score Pre-menopause = 1 Post-menopause = 3 Ultrasound score sum of: Multilocular cyst = 1 Solid areas in cyst = 1 Bilateral cysts = 1 Ascites = 1 Abdominal metastases e.g. omentum = 1 Then if total score 0-1 then U = 1 > 2 then U = 4 CA 125 - absolute serum level in U/ml Examples: 1 A 59-year old woman presents with a pelvic mass, USS shows a solid
ovarian cyst, ascites and an omental cake. CA 125 is 450 U/ml
RMI = M (3) x U (1+1+1 = 3 - score is 4) x C (450) = 4x4x450 = 6,600 REFER TO THE CANCER CENTRE
2 A 39 year old woman presents with a large mobile pelvic mass, USS
shows multilocular cyst with no ascites. CA 125 is 67 U/ml
RMI = M (1) x U (1 - score is 1) x C (67) = 67 NO NEED TO REFER TO CANCER CENTRE
Ovarian Cancer CMG – January 2010 Final Version
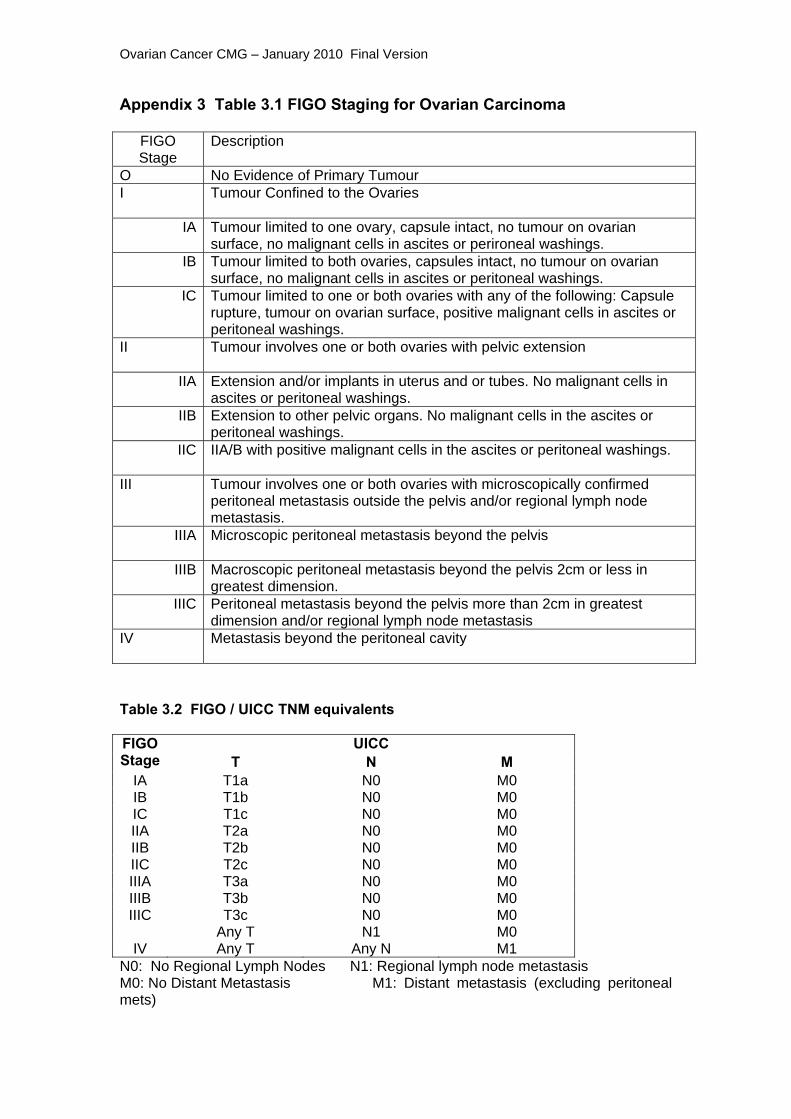
Appendix 3 Table 3.1 FIGO Staging for Ovarian Carcinoma
FIGO Stage
Description
O No Evidence of Primary Tumour I Tumour Confined to the Ovaries
IA Tumour limited to one ovary, capsule intact, no tumour on ovarian surface, no malignant cells in ascites or perironeal washings.
IB Tumour limited to both ovaries, capsules intact, no tumour on ovarian surface, no malignant cells in ascites or peritoneal washings.
IC Tumour limited to one or both ovaries with any of the following: Capsule rupture, tumour on ovarian surface, positive malignant cells in ascites or peritoneal washings.
II Tumour involves one or both ovaries with pelvic extension
IIA Extension and/or implants in uterus and or tubes. No malignant cells in ascites or peritoneal washings.
IIB Extension to other pelvic organs. No malignant cells in the ascites or peritoneal washings.
IIC IIA/B with positive malignant cells in the ascites or peritoneal washings.
III Tumour involves one or both ovaries with microscopically confirmed peritoneal metastasis outside the pelvis and/or regional lymph node metastasis.
IIIA Microscopic peritoneal metastasis beyond the pelvis
IIIB Macroscopic peritoneal metastasis beyond the pelvis 2cm or less in greatest dimension.
IIIC Peritoneal metastasis beyond the pelvis more than 2cm in greatest dimension and/or regional lymph node metastasis
IV Metastasis beyond the peritoneal cavity
Table 3.2 FIGO / UICC TNM equivalents
UICC FIGO Stage T N M
IA T1a N0 M0 IB T1b N0 M0 IC T1c N0 M0 IIA T2a N0 M0 IIB T2b N0 M0 IIC T2c N0 M0 IIIA T3a N0 M0 IIIB T3b N0 M0 IIIC T3c N0 M0
Any T N1 M0 IV Any T Any N M1
N0: No Regional Lymph Nodes N1: Regional lymph node metastasis M0: No Distant Metastasis M1: Distant metastasis (excluding peritoneal mets)
Ovarian Cancer CMG – January 2010 Final Version
REFERENCES Risch, H. A., McLaughlin, J. R., Cole, D. E., Rosen, B., Bradley, L., Kwan, E., Jack, E., Vesprini, D. J., Kuperstein, G., Abrahamson, J. L., Fan, I., Wong, B., and Narod, S. A. Prevalence and penetrance of germline BRCA1 and BRCA2 mutations in a population series of 649 women with ovarian cancer. Am J Hum Genet, 68: 700-710, 2001 Im, D. D., McGuire, W. P., and Rosenshein, N. B. Contemporary management of ovarian cancer. Obstet Gynecol Clin North Am, 28: 759-773, 2001. Bristow, R. E., Tomacruz, R. S., Armstrong, D. K., Trimble, E. L., and Montz, F. J. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol, 20: 1248-1259, 2002. International Collaborative Ovarian Neoplasm trial 1: a randomised trial of adjuvant chemotherapy in women with early-stage ovarian cancer. Colombo et al. J Natl Cancer Inst. 2003 Jan 15;95(2)125-32 Impact of adjuvant chemotherapy and surgical staging in early-stage ovarian cancer: European Organisation for Research and Treatment of Cancer-Adjuvant Chemotherapy in Ovarian Neoplasm. Trimbos et al. J Natl Cancer Inst. 2003 Jan 15;(95(2):113-25 International Collaborative Ovarian Neoplasm trial 1 and Adjuvant Chemotherapy in Ovarian Neoplasm Trial: two parallel randomized phase III trials of adjuvant chemotherapy in patients with early-stage ovarian cancer. Trimbos et al. J Natl Cancer Inst. 2003 Jan 15;95(2):105-12 NCCN Practice Guidelines in Oncology. V1 2009. SIGN Guidelines. 2003 Cyclophosphamide and Cisplatin compared with Paclitaxel and Cisplatin in patients with Stage III and Stage IV ovarian cancer. Mc Guire et al. N Engl J Med. 1996 Jan 4;334(1)1-6 Randomised intergroup trial of Cisplatin-Paclitaxel versus Cisplatin-Cyclphosphamide in women with advanced epithelial ovarian cancer: three-year results. J Natl Cancer Inst. 2000 May 3;92(9):699-708 A randomized clinical trial of Cisplatin/Paclitaxel versus Carboplatin/Paclitaxel as first-line treatment of ovarian cancer. du Bois et al. J Natl Cancer Inst. 2003 Sep 3;95(17);1320-9 Phase III trial of Carboplatin and Paclitaxel compared with Cisplatin and Paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncology Group study. Ozols et al. J Clin Oncol. 2003 Sep 1;21(17):3194-200 NCCN Practice Guidelines in Oncology. V1 2009.
Ovarian Cancer CMG – January 2010 Final Version
SIGN Guidelines. 2003 Recurrent epithelial ovarian carcinoma:a randomised phase III study of pegylated liposomal doxorubicin versus topotecan. Gordon AN et al. J Clin Oncol. 2001 Jul 15;19(14):3312-22. Phase II trial of weekly single-agent Paclitaxel in platinum/paclitaxel refractory ovarian cancer. Markman et al. J Clin Oncol. 2002 May 1;20(9):2365-9. Phase II trial of weekly paclitaxel (80mg/M2) in platinum and paclitaxel-resistant ovarian cancer and primary peritoneal cancers: a Gynecologic Oncology Group Study. Markman et al Gynecol Oncol. 2006 Jun;101(3)436-40. Antioestrogen therapy is active in selected ovarian cancer cases: the use of Letrozole in ER positive patients. Smyth JF et al. Clin Cancer Res. 2007 Jun 15;13(12):3617-22 Efficacy of Letrozole in the treatment of recurrent platinum and taxane resistant high grade cancer of the ovary or peritoneum. Ramirez et al. Gynecol Oncol 2008 Jul;110(1):56-9. NICE 2002: 2002/040 Guidance on the use of PLDH (Caelyx) for ovarian cancer. Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer:the ICON4/AGO-OVAR-2.2 trial. Parman MK et al. Lancet.2003 Jun 21;361(9375) 2099-106. The role of secondary cytoreduction in the management of the first relapse in epithelial ovarian cancer. Oksefjell H et al. 2009 Feb;20(2):286-93. Cytoreductive surgery for patients with recurrent epithelial ovarian cancer. Tebes SJ et al. Gynecol Oncol. 2007 Sep;106:482-7.