Embed Size (px)
Citation preview

Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care
The Chinese University of Hong Kong
Regional Anaesthesia for
Caesarean Section "The Best Recipe"

What I will not do…. • Magic recipes
• One shoe to fit all

What I will do…. • Discuss selected
controversial issues
• Practical recommendations

• Preassessment
• Premedication
• Consent
• Monitoring
• Vascular access
• 1-2-3
• Postop analgesia
BASICS

OUTLINE • Techniques
• Drug Choice
• Fluids
• Vasopressors
• Oxygen
• Drug Dose

Epidural Spinal CSE
Time
Simplicity
Drug Dose
Block Quality
Hypotension
Duration
Recovery
O P T I O N S

OUTLINE • Techniques
• Drug Choice

Local
Anaesthetic
Bupivacaine

Sia et al. (Cochrane Review)
Onset Speed (time to T5 block)

Conversion to General Anaesthesia
Sia et al. (Cochrane Review)


Coefficient of variation: 17.7% 21.9%
Block Height
Khaw et. Anesth Analg 2002;94:680-5.
• Opioids
• Adrenaline
• Clonidine
• Neostigmine
• Ketamine
Additives

Possible advantages:
1. Decrease side effects 2. Increase efficacy
Adding adjunct agents

Possible Disadvantages:
Adding adjunct agents
1. Drug error
2. Breach of sterility 3. Incompatibility
4. Cost
5. Safety (often “off-label”)


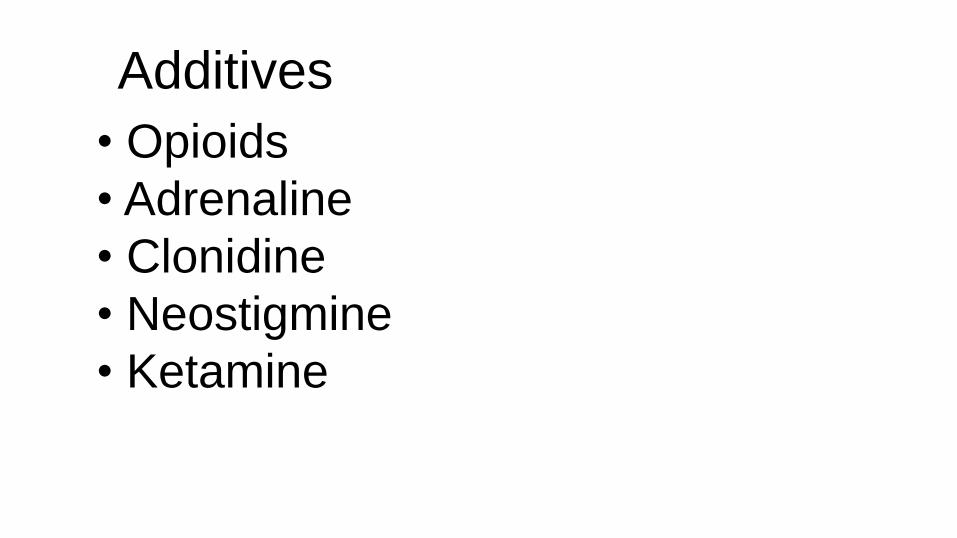
Elective Spinal Caesarean (n=56)
Height-adjusted IT Bupivacaine
• Quality of Block
• Intraoperative Analgesic Requirement
Added Fentanyl 0-50 µg
Hunt et al. Anesthesiology 1989;71:535-40.
0
20
40
60
80
100
1 2 3 4 5 6 7 80 2.5 5 6.25 12.5 25 37 50
Fentanyl Dose (µg)
Intraop
Opioid
(%)
67%
50%
25%
0% 0% 0% 0% 0%
Intraoperative Opioid Supplementation
Hunt et al. Anesthesiology 1989;71:535-40.


Elective Spinal Caesarean (n=30)
Hyperbaric Bupivacaine 12 mg
• FENTANYL: Less intraoperative pain
• FENTANYL: Less intraoperative nausea
Manullang et al. Anesth Analg 2000;90:1162-6.
IV Ondansetron
4 mg
IT Fentanyl
15 µg

OUTLINE • Techniques
• Drug Choice
• Drug Dose

Dose required for adequate spinal block
Single shot spinal


Low Dose
(≤ 8 mg bupivacaine)
Conventional Dose
(> 8 mg bupivacaine) VS

Arzola and Wieczorek. Br J Anaesth 2011;107:308-18
HYPOTENSION: Low Dose vs Conventional Dose

Arzola and Wieczorek. Br J Anaesth 2011;107:308-18
NAUSEA/VOMITING: Low Dose vs Conventional Dose

Arzola and Wieczorek. Br J Anaesth 2011;107:308-18
SUPPLEMENTATION: Low Dose vs Conventional Dose

“Low dose bupivacaine….compromises anaesthetic
efficacy…despite the benefit of lower maternal side
effects”
“Lower anaesthetic doses cannot be recommended
unless an epidural catheter is in place (CSE)…”

Recommendation: • Use smallest dose of LA for circumstances
• Add opioid (fentanyl/sufentanil)
• CSE: useful for high-risk or long surgery

OUTLINE • Techniques
• Drug Choice
• Fluids
• Drug Dose

Intravenous fluids
• Why?
• What?
• When?
• How much?
• How fast?
Uncertainties:

Crystalloid
Prehydration Cohydration
Colloid
- + + +
IV Fluid: Type and Timing
( )

CLINICAL INVESTIGATIONS
Anesthesiology
1999;91 1571-6
© 1999 American Society of Anesthesiologists, Inc.
Lippincott Williams & Wilkins, Inc
Effects of Crystalloid and Colloid Preload on Blood
Volume in the Parturient Undergoing Spinal
Anesthesia for Elective Cesarean section Hiroshi Ueyama, M.D.,* Yan-Ling He, Ph.D.,† Hironobu Tanigami, M.D.,* Takashi Mashimo, M.D.,‡ Ikuto
Yoshiya, M.D.

Elective Caesareans (n=36)
Lactated
Ringers
1.5 L
HES
0.5 L
HES
1.0 L
Ueyama et al. Anesthesiology 1999;91:1571-6.
• Hypotension
• Blood volume & cardiac output

Hyp
ote
nsio
n in
cid
en
ce (%
)
0
0.25
0.5
0.75
1.0
1.25
1.5
LR 1.5L HES 0.5L HES 1.0L
Blood volume increase
0
10
20
30
40
50
60
70
80
90
100 Hypotension incidence B
loo
d V
olu
me in
cre
ase (
L)
Adapted from Ueyama H et al. Anesthesiology 1999; 91:1561-6

• Cost.
• Effects on coagulation.
• Fluid overload.
• Hemodilution.
• Allergic reactions.
Colloid Prehydration:
D I S A D V A N T A G E S

Recommendation:
• Crystalloid: cohydration
• Colloid: prehydration or cohydration
• Don't rely on IV fluids
• Don't delay for IV fluids

OUTLINE • Techniques
• Drug Choice
• Fluids
• Vasopressors
• Drug Dose

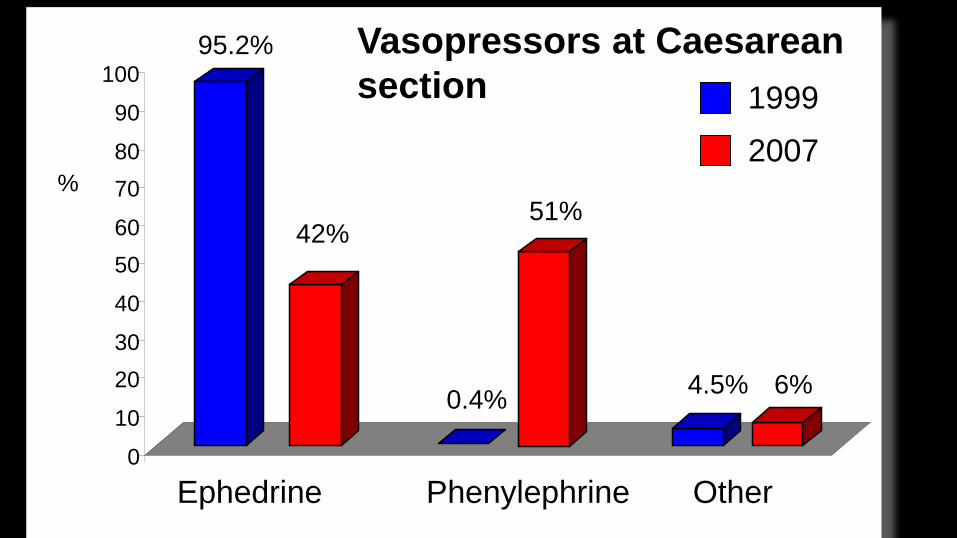
Phenylephrine

0
10
20
30
40
50
60
70
80
90
100
Ephedrine Phenylephrine Other
%
95.2%
0.4% 4.5%
42% 51%
6%
1999
2007
Vasopressors at Caesarean
section

• Phenylephrine is more effective
Why use phenylephrine?
• Ephedrine causes fetal acidosis

Lee A, Ngan Kee WD, Gin T. Anesth Analg 2002;94 920-6.
Figure 1. Meta-analysis of trials - effect on umbilical arterial pH
Weighted mean difference (umbilical cord arterial blood pH)
-0.10 -0.05 0.00 0.05 0.10
Alahuhta
Hall
LaPorta
Moran
Pierce
Thomas
Overall effect
Favours ephedrine Favours phenylephrine
Ephedrine depresses fetal pH and BE


0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
Ephedrine Phenylephrine
1.13
0.17
Placental Transfer of Ephedrine and Phenylephrine
*
* P < 0.0001
Umbilical Venous : Maternal Arterial (Median values)
Ngan Kee WD Anesthesiology 2009; 111:506-12

0
1
2
3
4
5
Ephedrine Phenylephrine
UA Lactate
50
55
60
65
Ephedrine Phenylephrine
UA Glucose
0
200
400
600
800
Ephedrine Phenylephrine
UA Adrenaline
0
1000
2000
3000
4000
5000
6000
Ephedrine Phenylephrine
UA Noradrenaline
pg/m
l
pg/m
l m
mo
l/l
mg/d
l
(all P < 0.05)
Ngan Kee WD Anesthesiology 2009; 111:506-12

Keeping blood pressure near baseline gives better
maternal outcome
Optimal Target Blood Pressure?
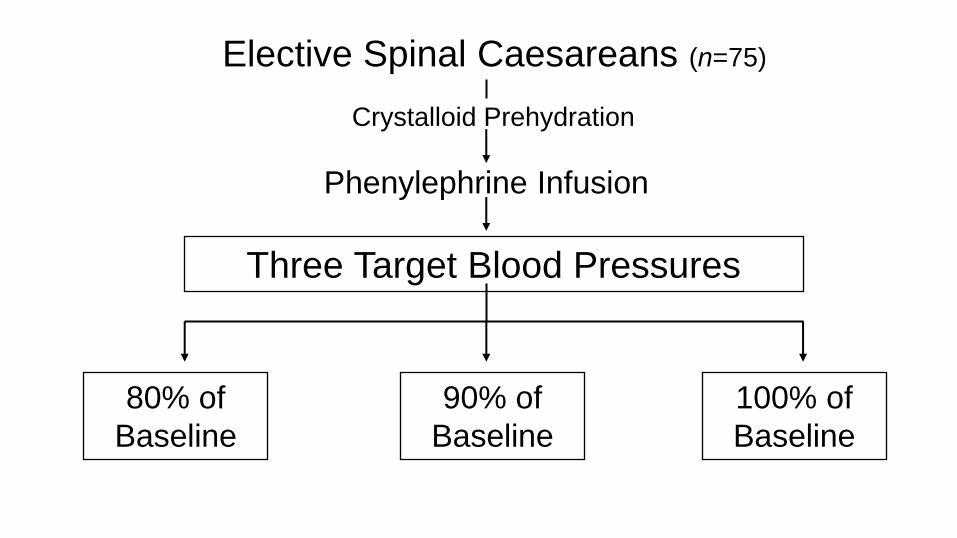
Elective Spinal Caesareans (n=75)
Crystalloid Prehydration
Phenylephrine Infusion
Three Target Blood Pressures
80% of
Baseline
90% of
Baseline
100% of
Baseline

0
20
40
60
80
100
Gp80 Gp90 Gp100
Incidence of Nausea/Vomiting
Ngan Kee et al. Br J Anaesth 2004;92:469-74
40%
16% 4%

How best to use phenylephrine?
• Timing of administration
• Method of administration
• Preparation

Dilute carefully…..

Prevention versus Treatment
Timing....
Most effective management:
• Start administration immediately after
intrathecal injection

Method….
• Both effective
• Intermittent bolus simple
• Infusion convenient
• Infusion less work
Infusion versus Boluses

INFUSION:
• Less hypotension
• More hypertension
• Less nausea/vomiting
• Fewer physician interventions


Recommendation: Infusion technique: • Syringe pump • Start 50 µg/min immediately after induction • Measure BP Q1min • Increase rate if BP falls • Decrease/stop if BP increases

Recommendation:
• Bolus dose: 50-100 µg • Begin immediately after IT injection • Measure BP Q1min • Further boluses when BP start to decrease
Bolus technique:

Recommendation: What about bradycardia? • Associated with cardiac output • Tolerate to 50-60 bpm
• BP low: IVF, ephedrine, atropine/glycopyrrolate*
• BP high/normal: stop and wait!
* Beware hypertension with anticholinergics!

• Preeclampsia • Fetal compromise
• Few studies • Less vasopressor needed • Use less aggressive dosing
Recommendation: What about high risk cases?

OUTLINE • Techniques
• Drug Choice
• Fluids
• Vasopressors
• Oxygen
• Drug Dose

• Can it do any harm?
• Should I (not) give oxygen?
O X Y G E N
• Does it do any good?

• Increase fetal oxygenation
• Reduce effects of hypoventilation
• Protection during prolonged U-D time
• Reduce effects of hypotension
• Safety in conversion to GA • Decrease nausea & vomiting
• Decrease wound infection
POTENTIAL B E N E F I T S



Elective C-sections (n=204)
Khaw, Ngan Kee et al. Br J Anaesth 2004; 92: 518-22
60% O2
40% O2
Air
• Cord gases & O2 content.
• Subanalysis for U-D time >180 s
High flow venturi facemask

21% 40%
UV PO2
(mmHg) 28 29
0 20 40 60 80
100
21% 40%
UV Hb
Saturation
(%) 63 67
0
5
10
15
20
21% 40%
UV O2
Content
(mL/dL) 12.9 13.4
Khaw KS, Ngan Kee WD et al. Br J Anaesth 2004; 92: 518-22.
0
10
20
30
40
60%
32 * P = 0.003
*
60%
70 ** P = 0.015
**
60%
14.4 *** P = 0.015
***

• Can it do any harm?
• Should I (not) give oxygen?
O X Y G E N
• Does it do any good?

Oxygen free radical generation

“In healthy parturients undergoing elective Caesarean section, it
would appear that additional oxygen is unnecessary.”
“It seems reasonable, based on current knowledge, to continue to
give supplementary oxygen to mothers undergoing
emergency/unplanned Caesarean section…”

Summary • Use spinal or CSE
• Heavy bupivacaine + opioid
• Dose: empirical
(low dose fentanyl 10-15µg)

Summary
• Crystalloid: cohydration
• Colloid: pre- or cohydration
• Don't rely on fluids
• Don't delay for fluids

Summary • Phenylephrine or metaraminol
• Start early
• Keep BP near baseline
• Care with anticholinergics

Summary • Routine O2 unnecessary
• Be guided by pulse oximeter
Warwick D. Ngan Kee Dept of Anaesthesia & Intensive Care
The Chinese University of Hong Kong
Regional Anaesthesia for
Caesarean Section "The Best Recipe"