Embed Size (px)
Citation preview

LAGOS STATE MINISTRY OF HEALTH
An Investment CaseMarch 2012
Reducing Health Disparities in Lagos State
Lagos is on the move, No one should be left behind
unite for children

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
1
health care through which the bulk of the
burden of diseases could be addressed; and
critical shortage of health care personnel
with an imbalance not in favour of peripheral
care.
The good news, however, is that these
cha l l enges and bo t t l enecks a re
surmountable. The document contains key
policy recommendations which address both
the supply and demand sides of the
equation. Some of these include the
acceleration of the existing momentum to
revitalize the State Primary Health Care
system; increased engagement of the
private health service providers especially in
recognition of their important role in the
supply of basic health services to the poor
and in slum areas; establishment of a State
Health Insurance Scheme to provide social
health protection for all categories of the
population including the poor and
vulnerable; pragmatic approach in the
reduction of fertility rate and promotion of
birth spacing of children; coordination of
action across the health and other
social/development sectors in order to
ensure that weaknesses in one sector do not
undercut the achievements of the other;
deepening of on-going community
participation and ownership of health
programs and projects. Evidence has also
been provided that additional incremental
investment of between 8 USD to 19 USD per
capita per year from 2012 to 2020 can
substantially improve the health indices of
the state and address the prevailing health
disparities.
It is instructive to note that the development
of this document followed due process with
wide consultations and meetings involving
various stakeholders including community
leaders, and was supported by technical
assistance from consultants procured for the
I am delighted to write the Foreword to this
document on Reducing Health Disparities
in Lagos State An Investment Case. The
journey started in December 2010 out of the
realization for the need to build an
Investment Case for Health that could be
used as an evidence-based advocacy tool for
leveraging increased resources for health
from the government, development partners
and the private sector including more
efficient use of such resources. To jumpstart
the process, a presentation on “Sensitization
/Orientation on Investment Case” was made
by UNICEF at the December 2010 first all-
embracing Joint Review Meeting for
partners operating in the Lagos State health
sector. The Investment Case Team, with
membership drawn from government
officials and development partners, was
inaugurated in February 2011 to drive the
process.
As articulated in its Strategic Health
Development Plan (2010-2015), Lagos State
is fully committed to its goal of ensuring that
every Lagosian enjoys unfettered access to
qualitative healthcare without significant
geographical, financial, cultural or political
barriers. However, in the course of the
development of this document, various
challenges and bottlenecks were identified
as militating against the realization of this
noble goal. These include, among others,
rapid population growth compounded by
inadequate investment in physical
infrastructure and associated sprouting of
urban slums; inequities in both geographical
and financial access to and quality of health
care between the urban, rural and slum areas
of the state; sub-optimal evidence-based
planning and budgeting due to inaccurate
and incomplete relevant data; inadequate
health spending which is disproportionately
in favour of tertiary and secondary health
care services at the expense of primary
Foreword

2
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
I hereby enjoin all who will be involved in the
implementation of the recommendations
contained in this document to be fully
committed to realizing identified accruable
benefits. There is indeed a role for everyone;
in fact no one should be left behind. On its
part, the Ministry would put in place the
necessary mechanism to ensure its effective
implementation.
process. I will like to especially acknowledge
the active partnership and support of
UNICEF and the commitment of the
Investment Case Team in this enterprise.
The contributions of DFID-supported
projects such as PATHS 2, SAVI, etc.; JICA
and other development partners are also
acknowledged.
Dr. Jide Idris
Honourable Commissioner for Health
March 2012

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
3
Table of Contents
Investment Case Team...............................................................................................5
1.1 Background.................................................................................................7
1.1.1 The challenge of population expansion in Lagos State.......................................7
1.1.2 Unplanned population and territorial expansion of Lagos' metropolitan areas........8
1.1.3 Topography of Lagos State............................................................................9
1.1.4 Twenty million people? Planning in the dark.....................................................9
1.1.5 Inequality and vulnerability...........................................................................10
1.1.6 Inadequate basic infrastructure.....................................................................10
1.1.7 Living conditions in Lagos' slums..................................................................10
1.2 Inequitable urban health..............................................................................13
1.2.1 Why do so many newborns and children die in Lagos State?............................13
1.2.2 Alarmingly high maternal mortality rates........................................................13
1.2.3 The unknown epidemiology of slums.............................................................13
1.2.4 An incomplete continuum of care.................................................................15
1.2.5 Large inequities in accessing health care.......................................................15
1.3 Methodology.............................................................................................18
1.3.1 Policy process............................................................................................18
1.3.2 Data collection...........................................................................................18
1.3.3 Bottleneck analysis.....................................................................................18
1.3.4 Modelling cost and impact...........................................................................19
2.1 Community care.........................................................................................20
2.2 Preventive services.....................................................................................22
2.3 Clinical care...............................................................................................25
2.3.1 Underutilization of existing facilities..............................................................25
2.3.2 Misdistribution of human resources...............................................................26
2.3.3 Financial accessibility and affordability of health care and drugs.......................27
2.3.4 Perceived quality of care.............................................................................29
2.3.5 Role of the private sector............................................................................29
1. INTRODUCTION & CONTEXT.................................................................................6
2. CHALLENGES IN ACCESS: Results of the Bottleneck Analysis.........................20

4
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
3. STRATEGIES TO IMPROVE ACCESS: Building on a Strong Foundation...............30
4. THE INVESTMENT CASE: Results of the Cost and Impact Modelling..................38
5. CONCLUSION: Achieving equitable health care in Lagos State..........................46
APPENDICES..........................................................................................................51
3.1 Bring health services closer to communities...................................................30
3.1.1 Increase the human workforce available to the most under-served populations....30
3.1.2 Rehabilitate and revitalize primary healthcare (PHC) centres..............................31
3.1.3 Implement pro-active outreach......................................................................31
3.1.4 Expand efforts to lower financial barriers and the cost of care..........................33
3.2 Bring communities closer to health...............................................................33
3.2.1 Affirm the right to health for all of the people of Lagos State...........................33
3.2.2 Encourage active community participation.....................................................34
3.2.3 Empower community volunteers by giving them status....................................34
3.3 Guarantee the quality of essential health services...........................................36
3.3.1 Align Lagos health services with international standards..................................36
3.3.2 Pilot performance-based financing................................................................36
3.3.3 Develop a decentralized monitoring system based on the
identified health bottlenecks........................................................................36
4.1 Strategies modelled....................................................................................38
4.2 More money for health, More health for the money..........................................38
4.3 The estimated investment required................................................................41
4.4 Dynamics in health financing.......................................................................45
5.1 Challenges and bottlenecks.........................................................................46
5.2 Key policy recommendations........................................................................47
5.2.1 Bring health services closer to communities...................................................47
5.2.2 Bring communities closer to health...............................................................48
5.2.3 Ensure the quality of essential health services................................................48
5.3 Windows of opportunity..............................................................................49
5.3.1 Continue to invest in infrastructure improvements...........................................49
5.3.2 Expand innovation with public-private partnerships.........................................49
5.3.3 Build on the dynamism in local communities..................................................49
5.4 The Investment Case..................................................................................49

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
5
Investment Case Team
Lagos State Ministry of Health
UNICEF
Partners
1. Dr. Monsurat Adeleke, Directorate of Family Health and Nutrition
2. Dr. Victoria Omoera, Directorate of Disease Control
3. Dr. Olusola Sokoya, Directorate of Healthcare Planning,
Research and Statistics
4. Mrs. Hamdalat Oladipo-Ojo, Directorate of Family Health and Nutrition
1. Ms. Sara Beysolow Nyanti, Chief of UNICEF Lagos Field Office
2. Dr. Isaac Aladeloye, Child Survival and Development Specialist,
UNICEF Lagos
3. Jerome Pfaffmann, Health Specialist, UNICEF West and Central Africa
Regional Office (WCARO)
4. Thi Minh Phuong Ngo, Social Policy Specialist, UNICEF WCARO
1. Dr. Bisi Tugbobo, PATHS2-DFID
2. Felix Obanubi, State Accountability and Voice Initiative
The Investment Case Team would like to acknowledge the leadership of the Honourable
Commissioner for Health, the Special Adviser to the Governor on Public Health, and the Office
of the Permanent Secretary, Lagos State Minister of Health.
The team also acknowledges the contributions of the Lagos State Health Partners'
Development Forum, other Ministries, Departments and Agencies of the Lagos State
government, and the participating communities of Lagos state.

6
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
organizations. (See page 5 for a list of Investment Case Team members.)
The Investment Case not only highlights the challenges facing healthcare provision in an urban environment, but recognizes the dynamic work that is already taking place under the leadership of the Government of Lagos State. Indeed, this Investment Case would not be possible without the considerable gains that have been made, despite difficult circumstances.
The background section of this report outl ines those circumstances and challenges, which include rapid population growth, compounded by inadequate i n ve s tmen t i n Lagos ' s phys i c a l infrastructure. This means that millions of people are living in very poor and-unhealthy-living conditions in slums that lack most basic services, from roads and electricity to clean water and sanitation. What's more, a
Ayear in the making, this report brings together new research and ground-breaking analysis to present a
compelling case for investing in achieving equitable health care in Lagos State. A partnership between the Lagos State Ministry of Health and UNICEF, it seeks to show that health care for all residents of Lagos State is not just a worthy vision, but a goal that is within reach. It lays out strategies and provides the opportunity for creative leadership by a range of actors, from health care professionals to community members
The idea for the Investment Case was born at the Lagos State Health Partners Forum in December 2010. In February 2011, The Honourable Commissioner, State Ministry of Health inaugurated the Investment Case Team, whose members represent the State Ministry of Health and UNICEF as well as nongovernmental and community-based
1. Introduction & Context

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
7
As this is an Investment Case, the fourth section forecasts the cost and impact of the strategies. (The modelling approaches used in constructing this case are described in the Methodology section below.) The news here is good: implementing the proposed measures will require an additional 15 USD per capita (averaged over nine years) until 2020. What's more, the results forecast by the model indicate that impressive outcomes can be accomplished with this investment, including a 50% reduction in under-five mortality as well as a 30% reduction in maternal mortality.
The final section summarizes the Investment Case, concluding that it is indeed a feasible - and worthwhile undertaking for a city that seeks to be a shining example of a Megacity for the African continent.
1.1.1 The challenge ofpopulation expansion in LagosState
Created in the 1967 restructuring of 1Nigeria's Federation, Lagos State is the
smallest of the 12 states, occupying an area of 3,577 square kilometres. Lagos was the capital of the Federal Republic of Nigeria until 1991, when the capital was moved to Abuja. However, Lagos State, which aims to be a “Centre of Excellence,” remains the commercial capital of Nigeria. From its historical origins as a wetland village, it has become one of the world's largest metropolises. Its position as Nigeria's commercial and industrial powerhouse is due to its favourable location on the Atlantic west coast of Africa and its border with Benin. It is an important port city and a major industrial, manufacturing and commercial hub in West Africa.
Although the smallest in size, Lagos State is the most populous state in Nigeria. Its 20.5
1.1 Background
paucity of accurate data, including population estimates, has made it difficult to carry out effective health planning. What is clear, however, is that health outcomes vary widely according to income, with the most poor, especially slum dwellers, receiving the least in terms of quality care.
The second section of the Investment Case focuses in on the specific “bottlenecks” to achieving equitable care in Lagos State. Using a participatory approach that included health experts as well as community members, the team identified a number of key issues, including a shortage of health care personnel, from doctors to nurses to community health workers, especially in the primary health-care system. On the demand side, the team found that many people from the poorer communities are not seeking care as often as they need it due to hidden user fees, a perception of poor-quality care (notably in public health facilities), and socio-cultural beliefs.
A third section describes strategies to address the bottlenecks and revitalize the primary health care system. They take to heart the Lagos Ministry of Health's commitment to “Bring care and healing closer to our citizens,” and build on several government initiatives underway. The strategies that address the supply side of the system, notably at the primary care level, include expanding the number and efficacy of community health workers and private health care providers as well as the government's promising Primary Health Care Flagship centres. Pro-active outreach strategies conducted by enabled community health extension workers would help fill the gaps in the continuum of care and bring essential preventive and follow-up care right up to the doorstep. Strategies addressing the demand side include removing financial barriers to access and forming closer partnerships within communities, including the Ward Health Development Committees. An important focus is to empower communities to be more pro-active in seeking quality care, and in advocating for their right to health.
1State (Creation and Transitional Provisions) Decree No.14 of 1967 restructured Nigeria's Federation into 12 States.

2million people make up 12.5% of the national population. It is also the most densely populated state in Nigeria, with 5,744 population per sq. km. Lagos has expanded at a very fast pace over the past decades from a population of 259,000 in 1950, 7.7 million in 1990, to over 20 million
3 in 2011. Administratively, the State of Lagos comprises 20 local government areas (LGAs), 37 local council development areas
4(LCDAs), and 2,000 communities. The 16 LGAs in metropolitan Lagos account for 91.5% of the state population (est. 18.8
5million inhabitants). The remaining four LGAs, which lie east (Epe, Ibeju-Lekki, Ikorodu) and west (Badagry) of the metropolitan area, are considered part of rural Lagos and account for 8.5% of the total population (est. 1.74 million inhabitants).
8
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
Thus, Lagos State constitutes the highest concentration of human beings in the smallest landmass in Africa.
In 2007, Lagos State had the largest gross domestic product (GDP) in Nigeria at USD 33.7billion (PPP), equal to 12% of Nigeria's
6 GDP. The services and manufacturing sectors account for 75% and 23% of State GDP respectively, with agriculture and fishing activities contributing to less than 2%. It is also estimated that the informal sector “which represents 45 percent of the state economy in terms of output constitutes the main source of income for
7the majority of city's households.” Lagos has a fairly educated population as can be expected from a largely urbanized population, with substantial disparities in
2Lagos Bureau of Statistics, 2011.3LMDGP Project Appraisal Document 2006, World Bank 2011, Lagos States Population Census 2006.4Olokesusi, Femi, 2011. Lagos: The challenges and opportunities of an emergent African Megacity. Paper presented at the NISER Seminar Series, 5 July 2011.5These 16 LGAs comprise Agege, Ajeromi-Ifelodun, Alimosho, Amuwo-Odofin,
Apapa, Eti-Osa, Ifako-Ijaiye, Ikeja, Kosofe, Lagos Island, Lagos Mainland, Mushin, Ojo, Oshodi-Isolo, Somolu, Surulere.6Lagos State Government http://www.lagosstate.gov.ng/index.php? page=speechdetail&spid=405&mnu=governor, accessed 2 January 2012.7World Bank, 2011. International Development Association Program Document, Report 54333-NG, p. 9.
Lagos State border
Ojota
Airport
Railway line
Ikeja
Oshodi
Mushin
Lagos Lagoon
Lagos IslandIddo
Ajegunle Ikoyi
Lekki peninsula
Maroko
Gulf of GuineaVictoria Island
Lagos in 1900
1901-1962
1963-1978
1978-present
Source: Gandy 2006
Figure 1. Map of Lagos Metropolitan Areas (1900-present)

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
9
rates than others. Today, the population in the whole of Lagos State is estimated to
11grow at 3.2% annually.
The population growth rate is even higher in 12urban areas at 4.8% p.a., which is
equivalent to the urban population doubling in 17-18 years. By comparison, other megacities such as Mumbai and Jakarta have seen their population grow at 2.3 %
13and 3.1% p.a. over a similar period.
Rapid expansion after independence as well
as during the oil boom of the 1970s drew
people from neighbouring states and
countries. Today, although 91% of the
population was born in Lagos State, 40% 14originate from other states or countries.
The population continued to increase even
during times of economic decline, including
the severe decline in Lagos's industrial
sector in the mid-1970s and the economic
crises and the structural adjustment periods 15of the 1980s and 1990s. As shown in
Figure 1, rapid population growth was
accompanied by a territorial expansion from
education levels nevertheless. On average, 85% of the population of Lagos is literate, while 80% of the population has completed either primary (30%) or secondary education (50% up to A-levels). On the other hand, 11% of the population is reported to
8neither read nor write.
1.1.2 Unplanned population and territorial expansion of Lagos' metropolitan areas
The city of Lagos, the fifth largest city in the 9world and the largest city in Africa, was
predicted to attain the status of megacity by 102015. However, with a population of 20.5
million and a projection of 24.4 million by 2015, Lagos would rank as the third-largest city in the world (behind Tokyo and Mumbai) and constitute the aggregate population of more than 32 African countries.
Lagos is also one of the ten fastest growing large cities in the world, with some districts experiencing more rapid population growth
<10000 10-20000 21-30000 31-40000 41-50000 51-80000 81-100000 >100000
Average monthly income (Nairas)
Source: Lagos State Government, Household Survey 2010 Edition, Lagos Bureau of Statistics,Ministry of Economic Planning and Budget
10
20
30
40
50
60
70
80
90
100
Figure 2:Cumulative Income Distribution in Lagos - Selected LGAs
8Lagos State Government, Household Survey 2010 Edition, Lagos Bureau of Statistics, Ministry of Economic Planning and Budget, p. 200.9UN Department of Economic and Social Affairs. World Urbanization Prospects 2009, File 11a, accessed 15 December 2011,http://esa.un.org/unpd/wup/index.htm.10UN Population Division. The World's Mega-cities, 2007 and 2025. World Urbanization Prospects: the 2007 revision.11World Bank, 2006. Project Appraisal Document for the Lagos Metropolitan
Development and Governance Project, Report no. 36433-NG12 World Bank, 2006, p. 1.13 World Bank, 2006, fn. 2 p. 1.
14Lagos Bureau of Statistics, Ministry of Economic Planning and Budget. Lagos State Household Survey, 2010, p. 199. 15Gandy, Matthew. Planning, Anti-planning and the Infrastructure Crisis Facing Metropolitan Lagos, Urban Studies, Vol. 43, No. 2, February 2006, p. 373.

1.1.4 Twenty million people?Planning in the dark
Population estimates of Lagos State are
strongly contested. Whereas 2006 Lagos
State Government estimates put it at about 1817.5 million, the 2006 National Population
Commission census put it at approximately 199 million. As of today, it is not possible to
know for certain how many people live in
Lagos. Estimates of annual population
growth rates for the city of Lagos also vary 20widely: 4.8% according to the World Bank,
213.74% according to UN-Habitat or 3.2%
according to the Lagos State Bureau of
Statistics. Programmatic evidence in the
health sector gives credence to the evidence
that the population of Lagos is in excess of
20 million over the last two years.
Immunization coverage of children below the
age of 5 years (20% of total population),
during Local Immunization Days (LIDs),
National Immunization Days (NIPDs) and
Maternal Newborn and Child Health Week
(MNCHW) activities have consistently been 22in the range of 4.3 million.
Evidence-based planning and budgeting is a major challenge when data is inaccurate andevidence is limited. In developing this Investment Case, the Lagos State Ministry of Health made the best possible use of available data to provide analysis and strategic directions. When data were not
its original setting in Lagos Island in 1900 to
a larger expanse encompassing Mushin,
Ikeja, Maroko and Ajegunle, which today
constitutes metropolitan Lagos.
The State's most recent population
estimates show an average population
density of about5,744 persons per square
km in Metropolitan Lagos. It ranges from
120,872 in Ajeromi-Ifelodun to 71,134 in 16Agege and 3,849 in Eti-Osa. The most
populous LGA in metropolitan Lagos is
Alimosho, with 12.7% of the population in
2006, followed by Ajeromi-Ifelodun and
Mushin, with 8.9% and 8.2% respectively.
Apapa and Amuwo-Odofin are the least-
populated LGAs, at 3.3%.
1.1.3 Topography of Lagos State
Lagos sits on 180km of low-lying coastland
stretching along the Atlantic Ocean. Its
fragmented topography is interspersed with
creeks, lagoons, mangroves and wetlands.
The reclamation of swamps and floodplains
allowed Metropolitan Lagos to expand
from its original lagoon. Since 1960, built
areas increased from 200 sq. km to an
estimated 1,140 sq. km. As a result of its
singular topographic situation, Lagos is
particularly prone to flooding, land loss, sea 17level rise.
Public services Current supply Estimated need
Power Supply Less than 1000 Mw 10,000 Mw
Water Supply 170 million gallons per day (mgd) 540 mgd
Waste Generation
Source: Lagos State Ministry of Physical Planning and Urban Development, 2010, cited in Olokesusi 2011 p.9
Table 1:Public services in Lagos
10,000 metric tons per day
10
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
16Office of Surveyor General.17Adelekan, I.O, 2009. Vulnerability of Poor Urban Coastal Communities to Climate Change in Lagos, Nigeria, Fifth Urban Research Symposium 2009.18Lagos State Strategic Health Plan 2010, p.18.
19National Population Commission (NPC) report, 2006.20World Bank, 2006, p. 1.21UN-Habitat, 2008, p. 177.22Lagos State Ministry of Health Immunization Report, 2010/2011.

triggering a long-lasting and on-going crisis affecting Lagos' existing physical infrastructure (roads, drinking water pipes, sanitation, and electricity), which is under severe strain (see Table 1). Today, Lagos suffers from inadequate basic amenities and
23public infrastructure. According to Gandy : “the limited investment in water and sanitation infrastructure had left a situation in which only 10 per cent of dwellings in the Lagos metropolitan area were directly connected to the municipal water system whilst the rest of the city relied on shared taps, stand-pipes, wells and polluted creeks […] As for the city's sewer system, the situation was even worse with the complete
absence of any functionalsystem at all.”
1.1.7 Living conditions inLagos' slums
A lack of affordable housing in the city helped fuel rapid growth in unplanned informal settlements, or slums. Millions live without adequate water and sanitation and public services such as garbage collection. The quality of housing is poorwooden shacks, concrete-block bungalows, or
24simply hutsmade of zinc sheets.
It is difficult to know with any precision the number of slums or slum households in Lagos. A study by UNDP in 1984, which was updated in 1995 and formed the basis for the World Bank-supported Lagos Slum Upgrading Programme, counted 42 slums in which an estimated 70% of the population
25lived. According to Gandy, there were an estimated 200 slums as of 2006.
Slums in Lagos vary in size and shape. They encompass entire districts such as Ajegunle and Mushin, where households have settled since the mid-1970s, or groups of shacks nested in the remaining interstices of the city, beneath highways or bridges or on
26reclaimed marshy areas, near the Lagoon. The vast proportion of lands reclaimed by slums lies below sea level and is prone to flooding.
readily available, triangulation of different estimates was made. For the purpose of the Investment Case, the 20.5 million figure of from the Lagos Bureau of Statistics will be used.
1.1.5 Inequality and Vulnerability
The household survey conducted in 2010 by the State Bureau of Statistics, State Ministry on Planning and Budget, revealed that 91% of the sampled respondents spent an average of $0.21 (N33) per day on consumption of food items. There are also large disparities in income and wealth, with the poorest households located in Lagos's rural areas (Epe, Badagry): In Epe, 70% of the population earns less than N20,000 per month. In Lagos Mainland, income is spread more widely, with the bottomfourth of the population earning less than N20,000 monthly, a majority (55%) earning between N20,000-40,000, and the top 1% earning more than N100,000.
1.1.6 Inadequate basicinfrastructure
Uncertainties concerning census data and the exact growth rate of the population by LGA mean that Lagos' fast population growth, fuelled by migration from rural areas as well as from neighbouring countries, is largely unplanned. Such unplanned population expansion has generated serious concerns about the state of welfare and living conditions (i.e. poor housing and infrastructure, lack of access to basic essential services) in informal settlements, or slums, forming in the interstices and outskirts of Lagos. Indeed, the growth of informal settlements makes it even more difficult to estimate the population because of systematic under-reporting.
Over the years, the rapid population and territorial expansion of Lagos has not been matched with adequate capital investments,
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
11
23Gandy, 2006, p. 378.24Emordi, E.C., and O.M. Osiki,“Lagos: the 'villagized' city,” Information, Society and Justice, Vol. 2.1, December 2008, pp. 95-109.25World Bank, 2006, p. 20, 84.
26Gandy, 2006, p. 372.27These slums are Agege, Ajegunle, Amukoko, Badia, Iwaya, Makoko, Ilaje, Bariga, Ijeshatedo and Itire (World Bank 2006, fn. 11, p. 5).

12
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
Figure :3Infrastructure: The Metropolitan Development and Governance Project

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
13
makes slum households particularly vulnerable to the spread of diarrhoeal diseases (cholera) and increased risk of vector-borne diseases such as malaria or dengue fever.
High levels of heavy metals such as lead, cadmium, zinc, or iron were found in the street food sampled in low-income LGAs (e.g. Kosofe) whilst water was found to be contaminated by both pathogens such as E.coli, Staphylococcus aureus and Salmonella as well as toxic levels of lead as a result of unsanitary modes of waste disposal (e.g. defecation in streams, dumping of
31refuse in pits, rivers or drainage channels).
According to the latest household survey for Lagos State, 38% of household flooding in their street. Flooding seems to be particularly prominent in ten LGAs: Badagry, Ojo, Alimosho, Lagos Island, in Kosofe, Lagos Mainland, Ifako/Ijaiye, Ajeromi-Ifelodun, Amuwo-Odofin and Apapa, where 70 - 40% of residents call flooding a major problem. Most recently, in July 2011, flash floods caused serious flooding in Lagos
State, in part due to drainage or river channels blocked by refuse or buildings built along the city's drainage system, affecting about 5,400 households 31 districts, mostly
32in Alimosho, Agege and Ebute-Meta.Cholera is therefore endemic in Lagos, with
27Nine of the largest slums , totalling an estimated 1 million people, were selected to be part of the on-going Lagos Metropolitan Development and Governance Project to upgrade living conditions. These slums are characterised by extremely high population growth (8% annually); an average household size of six persons living in poor and crowded housing; frequent flooding; and lack of basic infrastructure such as access to asphalted roads, drinking water pipes, waste disposal
28services and drainage facilities.
Across metropolitan Lagos, access to basic amenities and public infrastructure is fragmented. Whether rich or poor, communities and individual households often have to provide for their own water supply, electricity, garbage collection and
29 street clearing. Wealthier inhabitants of residential areas are more likely to benefit from adequate privatized services. In slums, the lack of piped water supplies forces people to depend on wells, boreholes and water tanks or illegal connections for drinking water. Without sewerage facilities, households resort to public toilets or open
defecation, while garbage collection needs are addressed by hiring private services. Unhealthy sanitary living conditions combined with the fact that slums tend to be located in low-lying swampy areas prone to
30flooding (notably during the rainy seasons)
28World Bank, 2006, p. 34, 83.29Gandy, 2006, p. 383.30Adelekan, 2009.
31Opeolu, Adebayo et al., “Physicochemical and Microbial Assessment of Roadside Food and Water Samples in Lagos and Environs.” J. Appl. Sci. Environ. Manage. March 2010 Vol. 14(1) 29–34,Full-text available online at www.bioline.org.br/ja.32International Federation Red Cross and Red Crescent Societies, 2011, Nigeria / West Africa: Floods, DREF Operation Update, 15 December 2011.http://www.ifrc.org/docs/appeals/11/MDRNG01001.pdf.
Definition of Slum adopted by the Lagos State Urban Renewal Board in 2002,which led to the identification of 42 slums hosting about 70% of the population (World Bank, 2006, p.85)
Definition of Slum and Slum Households according to UN-Habitat (2008)
Settlements or communities within the city which lack (i) basic essential municipal services so that the communities live in risky and environmentally degraded conditions, and (ii) communities with population density of not less than 200 people per hectare.
Slum: a contiguous settlement where the inhabitants are characterized as having inadequate housing and basic services; a slum is often not recognized and addressed by public authorities as an integral part of the city.
Slum households: a household that lacks one or more of the five elements, i.e. access to improved water; access to improved sanitation; security of tenure; durability of housing; and sufficient living area.

14
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
that of neighbouring countries such as Benin 35and Niger. There are steep inequalities in
maternal mortality across LGAs, with the starkest inequality between Alimosho, which has an MMR of 826 per 100,000 live births, and Lagos Island, which has an MMR of 310 (Figure 5). Mothers in Alimosho are 2.7 times more likely to die in childbirth than mothers in Lagos Island.
1.2.3 The unknownepidemiology of slums
To identify the spectrum and burden of diseases prevailing in the rapidly growing slums of Lagos, we draw upon a survey of nine slums selected by the Lagos State Government for slum upgrading. According to the study, owing to unhealthy conditions in the slums, “diarrhoea, hepatitis, typhoid, cholera and malaria are the most common diseases, and 66 percent of the diseases affecting children under the age of five are related to poor water quality and lack of
36 access to sanitation”. Non-communicable diseases affecting the general population are also on the rise, with hypertension and diabetes already accounting for 18-20% and 2-4% of the screened population respectively, according to the Lagos State Hypertension and Diabetes Screening Program. Evidence from slum areas in other countries indicates that such chronic non-communicable diseases as well as communicable diseases are likely to be major concerns due to the poor, unhygienic and hazardous living conditions in which slum
37households tend to live.
1.2.4 An incompletecontinuum of care
In recent years, the State of Lagos has made substantial investments to improve
38secondary and tertiary facility-based care. Such investments appear to have paid off, as exemplified by the high levels of coverage for health services provided at facilities such as skilled birth attendance (83%) and antenatal care (88% for at least one visit).
outbreaks likely to flare up in case of flooding. Given the highly contagious nature of cholera, a major epidemic is likely to occur without accelerated improvements in basic infrastructure such as piped water, safe sanitation and waste disposal together with continued public awareness campaigns on hygiene.
1.2.1 Why do so manynewborns and children die in lagos state?
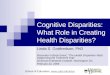
One in every 10 children born in Lagos does not live to celebrate his or her fifth birthday, and 37 of every 1,000 newborns die within the first month of life. A large proportion of child deaths (42%) occur during the neonatalperiod (i.e. during the first 28 days of life). Majorcauses of neo-natal deaths include complications of pre-term deaths, asphyxia, and severe infections. Preventable infectious diseases, i.e. malaria, diarrhoea, pneumonia, remain major child killers in Lagos, altogether accounting for 41% of all under-five child deaths (see Figure 4). Malaria alone is responsible for 22% of under-five child deaths, followed by pneumonia (10%) and diarrhoeal diseases (9%).
Malnutrition, which is estimated to be the underlying cause of one-third of under-five
33child deaths, remains a major health concern with 20.3% of the children being stunted, 9.4% wasted, and 15.6%
34underweight.
1.2.2 Alarmingly high maternal mortality rates
Maternal mortality rates (MMR) in Lagos are among the highest in the world. At 555 per 100,000 live births, it is higher or at par with
1.2 Inequitable urban health
33Nigeria Federal Ministry of Health, Newborn Health, 2011.34MICS3 Lagos, 2007.35Hogan, Margaret C. et al., “Maternal mortality for 181 countries, 1980–2008,” The L ancet, Vol. 375, No. 9726, 8 May 2010.
36 World Bank 2006, p. 9637Riley, Ko, Unger and Reis, “Slum health: diseases of neglected populations.” BMC Int Health Hum Rights. 7 March 2007, 7:2.38IDA World Bank First Lagos State Development Operation Policy, 2011, p. 17.

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
15
Diarrhoea, 9%
Other, 13%
Injuries, 1%
AIDS, 3%
Pneumonia, 10%
Malaria, 22%
Neonatal, 42%
Asphyxia, 23%
Preterm, 39%
Infection, 21%
Congenital, 9%
Other, 4%
Causes of neonatal mortality
Diarrhoea: 2%
Tetanus: 1%
Figure :4Causes of Neonatal and Under - Five Mortality
Source : Newborn Health, Federal Ministry of Health, revised second edition 2011, p. 103.
Figure :5Maternal Mortality Rate per LGA in Lagos State (2010)
826803
758 754736 725
690667 667 667
600
555 555
511
443 443421 421
354322 310
0
100
200
300
400
500
600
700
800
900
Average MMR for Lagos State
Source: Lagos State Ministry of Health (2010)

16
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
Figure :6Coverage along the continuum of care of Lagos
Pre-pregnancy
Pregnancy
Birth
Neonatalperiod
Infancy
Contraceptive prevalence rate
Antenatal visit (one or more)
Skilled attendant at birth
Postnatal care within 2 days
Exclusive breastfeeding <6 months (2007)
Measles immunization
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
28%
88%
83%
5%
20%
69%
Source : Newborn Health, Federal Ministry of Health, revised second edition 2011, p. 103.
for immunization is irregular, with large gaps at key junctures in the life journey of both child and mother. Undernourished children (stunted, wasted), those not optimally breastfed and those suffering from micro-nutrient deficiencies have substantially lower chances of survival. They are much more likely to suffer from a serious infection and to die from common childhood illnesses, yet coverage rates for nutritional health interventions lag (see Table 2).
1.2.5 Large inequities inaccessing health care
The social and geographical fragmentation of Lagos presented in Figure 8 translates itself in strikingly large inequities in access to and utilization of preventive and curative health care, both across LGAs and across wealth quintiles.
Figure 9 shows the coverage gap between the least and most deprived LGA for a given intervention. The gap is widest for full
Family practices and community health have not benefited from similar investments, resulting in low coverage of health interventions typically delivered through community-based care or outreach. As a result, the contraceptive prevalence rate remains at a low 28%; only 20% of infants less 6 months of age are exclusively breastfed; and full immunization for all children has not been achieved, with 24% children still unreached. The drop in coverage of BCG, the tuberculosis vaccine, to 92% and the drop in measles immunization to 76% shows that an increasing number of children are missed during routine vaccination or campaigns. Nevertheless, the 92% coverage rate of BCG shows that there is major adhesion of the communities to the vaccination programme overall. With better follow-up and efforts to remind mothers of the next vaccination visit, it is likely that most of the children could be covered.
Nonetheless, as shown in Figures 6 and 7, coverage along the continuum of care and

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
17
deprived LGAs shown in Figure 7 do not capture the extent of disparities within the LGAs, which are likely to be substantial. This is because impoverished informal settlements are scattered across Lagos and exist between wealthier enclaves.
Disparities between the poorest and richest wealth quintiles are largest for water and
sanitation as well as for services delivered at health facilities (e.g. antenatal care, skilled delivery at birth), whilst they are more muted for interventions linked to family or community health. Households in the poorest wealth quintiles have very low
immunization, with a 50 percentage point gap between the most deprived LGA (Apapa) and the least deprived one (Ikeja).
In Apapa, only 43% of children complete their full immunization schedule against 98% of children living in Ikeja. The gap for access to improved sanitation and improved water sources is also wide (about 30
percentage points): only 58% and 65% of households in Ibeju-Lekki enjoy access to improved sanitation and water sources, while coverage in the least-deprived LGA exceeds 90%. It is important to note that disparities between the most- and least-
Continuum of care (coverage rate) in Lagos Nutrition
Contraceptive
Prevalence
Rate
Antenatal
care
(ANC) 1+
Skilled
birth
attendants
Post-natal
care
(PNC)
within 2
days
Exclusive
breast-
feeding
<6m
Measles Stunting
(% of
children
under-
five
Wasting Low
birth
weight
28
88
83
5
20
69 21 10 14
Source: Newborn Health, Federal Ministry of Health, revised second edition 2011
Table 2:Coverage of essential high-impact health interventions in Lagos State
76%
71%68%
75%
67%
80%
77%
84%
92%
90%
100%
80%
70%
60%
50%
40%
30%
20%
10%
0%
BCG DPT1 DPT2 DPT3 Polio O Polio 1 Polio 2 Polio 3 MEASLES
Figure :7Immunization coverage in Lagos State (2010)
Source: NDHS 2008, MICS 3.

18
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
of the spectrum, the wealthiest households enjoy coverage levels across the continuum of care above 70% (for detailed data by LGA, see Appendix B).
coverage across all health interventions, from 10% for access to improved water sources to 30% for appropr iate management of pneumonia. At the other end
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Improved water source
Improved sanitation
BCG
Polio
Full immunization
Source: Lagos Ministry of Health (2010) (see Annex A for data by LGA)
Lowest coverage rate across
Highest coverage rate across
Figure 8:Inequities in Health Coverage across LGAs (lowest vs highest coverage rate in LGA)
Safe stool disposal
ante Natal Care (1 or more)
skilled delivery
initial Breast-Feedomg
measles vaccination coverage
Fully immunised
Appropraite mgt of Acute Respiratory Infections
Exclusive Breast feeding
poorest quintile
wealthiest quintile
% coverage rate
0 10 20 30 40 50 60 70 80 90 100
Figure 9:Inequities in continuum of care coverage (between poorest and wealthiest quintile) in Lagos State

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
19
neighbors told me my second child ate hair in my womb that's why he died” she lamented.
Typical of slums and poor communities, Ijora Badia is populated with artisans, petty traders and unemployed with no health infrastructures except for the clinic managed by an NGO. The extremely poor sanitary situation in Ijora Badia renders the inhabitants prone to ailments related to diarrhea, fever, vomiting and malaria.““I could not believe my eyes as my two children died not too long after each delivery” Endurance lamented.
Her four-yearbaby girl suffers from frequent childhood illnesses; and Endurance is fighting to keep her alive. Consequently, she doubled her efforts with a petty trading business to provide food with better nutritional value, as well as keep small savings for hospital bills whenever the need arises. She has realized that she has to help her husband or else there will not be sufficient funds for healthcare. Lagos is a place where any small trade can earn income. Her family still struggles to make ends meet but the pain of losing two children in a row “taught me a practical lesson on the need to make some more money, and to make sure to keep some for health care services from the right source. I know better now” she says.
Twenty-five year old Endurance Olurungbemi lives with herfamily of three in Ijora Badia, a back water slum by upscale Apapa area of Lagos: She is a petty trader whose parents are from Benue State while her haulage driver husband comes from Ondo state. Her family forms part of the migrant populations that regularly stream into rapidly growing Lagos for better economic opportunities.
Endurance at the moment is a mother of a baby girl. However, she had had two other children, but they all died. The only surviving child was delivered 4 years ago in a health facility in Benue state while she was still living with her parents. After Endurance moved with her husband, things were very difficult in Benue State where they lived. The husband opted for better opportunities in Lagos State.
When Endurance joined her husband, they were fortunate to have two more pregnancies, but that joy was soon turned to doom when both babies died after birth. Due to hardships, they were both delivered in her shop in Ijora Badia assisted by neighbors and surrounded by filthy black waters from the Lagoon.
The first one died exactly seven months after delivery from prolonged vomiting and stooling; while the second one could not make it into the second week. “My
Improved Health Seeking Behavior;My Only Surviving Child Will Not Die
Endurance Olurungbemi standing beside her shop

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
public health field. A final consensus was reached on the data gaps and the selection of “tracer interventions” for the bottleneck analysis.
1.3.3 Bottleneck analysis
Following the consensus reached on the health system database, a stakeholder meeting comprising health experts analyzed the major health system constraints using the “bottleneck analysis” based on the work of Tanahashi and Knippenberg et al. The approach examines six related determinants of the effective coverage of health, sanitation, nutrition and HIV-related interventions, including both supply and demand in the health system. The supply-side determinants include: the adequacy of essential commodities, sufficiency of human resources, and accessibility of service provision sites for the target population. The demand-side determinants include: the basic demand for or acceptability of a service, the continuous utilization of the service, and service quality.
At every level, health systems have constraints that can be termed as supply and demand side bottlenecks. In order to assess the constraints affecting the health system in Lagos, an analysis was performed that grouped health services into three service-delivery modes:
Individually oriented clinical services include curatives and obstetrical interventions delivered at fixed sites which require that patients seek regular care at a health facility;
Population-oriented, schedulable services cover preventive interventions delivered either in a health facility or outreached in communities on a schedulable basis;
Family and community-based care includes preventive and curative interventions and behaviours that families and community-based agents can undertake themselves.
1.3 Methodology
1.3.1 Policy process
At the Lagos State Health Partners Forum held in December 2010, a consensus was reached concerning the need for donor coordination and for the development of an Investment Case. In February 2011, the Honourable State Commissioner for Health inaugurated the Investment Case team, which was placed under the Office of the Permanent Secretary. A proposed road map was also approved.
1.3.2 Data collection
In May 2011, a weeklong training on a costing and impact estimates tool called Marginal Budgeting for Bottlenecks (MBB) was held at UNICEF's West and Central Africa Regional Office (WCARO) in Dakar, with the participation of two Lagos State technical officials and four staff from UNICEF Nigeria. A consultant from UNICEF WCARO then worked with officials from the Lagos Government for two weeks to collect data on the State's health system that was needed in order to model the Investment Case. Finding adequate and accurate data was challenging in most cases, neither household survey nor national information system statistics could be reliably disaggregated to the level required. Where data was missing, expert opinion from government counterparts and programming managers were gathered and discussed in order to reach a consensus through the
39Delphi method.
In May 2011 a consultative meeting was held to provide expert estimates for missing values in the database. Participants included representatives of development agencies (UNICEF, WHO, UNFPA, JICA, PATHS 2, ENR), Ministries Departments and Agencies, NGOs, research institutes and universities.In June 2011 a two-day meeting was held with a large group of participants from the
39Hsu, Chia-Chien and Brian A. Sandford, 2007, “The Delphi Technique: Making Sense of Consensus.” Practical Assessment Research & Evaluation, Vol. 12, No. 10. Available from:http://pareonline.net/getvn.asp?v=12&n=10.
40Tanahashi T., “Health service coverage and its evaluation.” Bulletin of the World Health Organization, 1978, 56(2): 295-303. Knippenberg R, Levy-Bruhl D, Osseni R, Drame K, Soucat A, Debeugny C. Initiative de Bamako: soins de santé primaires. Enfant Milieu Trop, 1990, 184-185: 5-94.
20
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
21
1.3.4 Modelling cost andimpact
Data processing and preliminary analysis took place between June and October 2011. The modelling of the costing and impact estimates was based on the recommended data collected during different workshops, and made use of a tool developed by The World Bank, UNICEF and the African Development Bank called Marginal Budgeting for Bottlenecks (MBB). Different scenarios were modelled using the version 5.6.1 of the tool during a five-day technical meeting held 28 November to 2 December 2011 in Lagos.
Parallel to the modelling, and in order to inform the strategic choices modelled, qualitative information was sought through field visits to a primary health care (PHC)
Within each mode of service delivery, three to four “tracer” interventions were closely examined to identify bottlenecks affecting the performance of the health system.
A community consultative forum held on July 5,2011 was attended by ten community members each invited from the local government areas of Ikorodu, Badagry and Eti-Osa, thus representing the urban, peri-urban and rural LGAs. They included traditional rulers, religious leaders (Muslim and Christians), chairmen of Community Development Committees, opinion leaders, representatives of market women, caregivers, women and youth leaders. Also present were the LGA Medical Officers of Health, LGA Health Educators, antenatal care (ANC) midwives and officials from the State Ministry of Health, including the Primary Health Care Board and the UNICEF Lagos Investment Case team.
41More information is available at http://www.devinfolive.info/mbb/mbbsupport/index.php.

incidence, access to vaccination and water and sanitation, by LGA (2010) are presented in Appendices A and B.
The second section of this Investment Case presents challenges and bottlenecks that hinder efforts to improve levels of health care coverage in Lagos State. It is followed by a third section that describes strategies to improve existing coverage levels for essential health interventions. The fourth section presents the results of the modelling, which includes estimates of the additional investment required to implement these strategies (taking into account the specific context of Lagos) as well as estimates of their impact on health outcomes. The fifth and concluding section observes that necessary investment is feasible over coming years and reviews the opportunities for taking concerted action toward achieving a shared vision of quality health care for all in Lagos State.
centre, a slum community, a private hospital, and a maternal and child clinic, all located in the Ajeromi/Ifelodun local government area
42using the Transect walk approach.For quality assurance, the model was shared with UNICEF MBB experts in New York and with Devinfo MBB support team in India.
Preliminary results and recommendations were presented to the Hon. Commissioner for Health along with the Special Adviser to the Governor on Public Health, the Chairman of the State Legislative Committee on Health, the Chairman of the State PHC Board, Permanent Secretaries of Ministry of Health and Health Services Commission, WHO, UNICEF and representatives of other bilateral agencies.
A summary table of key indicators for Lagos extracted from Nigeria Demographic Health Survey 2008 at the state level, as well as data on maternal mortality rates, diarrhoea
42Ahmed, et al., “Using formative research to develop MNCH programme in urban slums in Bangladesh: experiences from MANOSHI, BRAC,” BMC Public Health 2010, 10:663. Available from http://www.biomedcentral.com/1471-2458/10/663
22
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

level in that the system is reliant on a much broader sphere of actors and influencers. At the individual or household level, a health worker might not be as influential as other family members, community leaders or even peers and friends. Family in this context then extends beyond the immediate parents and children to a much wider circle of relatives, as is commonly the case in sub-Saharan Africa. Lagos is no different. Although Lagos is a melting pot for Nigeria, as in much of West Africa and Africa as a whole, the essence of community is not lost. Albeit change has led to some confusion around how a community must now be defined.
This complicated context directly impacts
the demand for services. Although services
are delivered at the community level, there is
an equally important dimension to health
system strengthening, which is that of
demand creation. This is also linked to the
he goal of every health system is to ensure a healthy population. The Tmission and vision of Lagos State is to
ensure that healthcare is affordable and equitable and provided with quality for all citizens.
In pursuit of this mission, the Investment Case team and a panel of health experts conducted a “Bottleneck Analysis” (described in the Methodology section above) that examined the effective coverage of health, sanitation, nutrition and HIV-related interventions. Please see Appendix D for a summary of the findings, which are discussed in more depth in this section.
The challenges of the health system are unique at the community and household
2.1 Community care
2. CHALLENGES IN ACCESS: Results of the Bottleneck Analysis
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
23

interventions and behaviours adopted or delivered at community level.
Central to the delivery of these interventions are community health extension workers (CHEWs) whose primary responsibilities are to provide the community with information about services and the relevant referral facilities treat minor ailments, identify health issues in the community, dispense drugs and undertake home visits amongst several others. To carry out these services, CHEWs are distributed according to population size and are intended to be 1 CHEW to 1,000 people, as per the Ward Minimum Healthcare Package established by the National Primary Health Care Development Agency (NPHCDA). This strategy is to ensure that the health system is strengthened to boost both supply and demand as a means to reverse the trend of generally low performance of interventions at the community level.
issue of access to information geared
towards ensuring that every individual
hasknowledge and skills to demand his or
her rights to health, education, identity and
others. Most strategies targeting behaviour
change reach individuals at their homes or at
the least, in their communities. This
information then competes with socio-
cultural, traditional and religious beliefs, not
only of the individual who has to make the
health decision, but of the broader family as
well.
To clearly identify the bottlenecks in the health system at the community level, key interventions such as the use of long-lasting insecticide-treated nets (LLINs), exclusive breastfeeding, infant and child care feeding practices and community illness management with a focus on oral rehydration therapy (ORT) were analyzed as tracers for the constraints for all the
0
50
100
150
200
250
300Expected CHEW in public PHC (as per Minimum Essential Package of Care)
Actual CHEWS post in public PHC
Source: Service in collaboration with PATHS 2
Availability Mapping (SAM) 2010, Lagos State Ministry of Health
Figure 10:
CHEWs in public PHC in Lagos State
24
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

development activities, referrals (community diagnosis), record keeping and data collection. These groups of critical workers form the link between the primary healthcare (PHC) centres and the community.
CHEWs are expected to spend between 60-80% of their working hours within the community and be supervised by community health officers (CHOs), nurses, midwives and doctors. However, this is not the current practice, which accounts for low coverage in community-oriented programmes. Figure 11 shows that in most communities, health volunteers in communities are not perceived as being effective at all.
On the demand side, there are challenges with utilization and effective coverage of essential, life-saving interventions at
On the supply side across almost all health interventions, human resources were a clear bottleneck. CHEWs are found to be virtually non-existent in the communities, in contradiction to the health policies of Lagos State. They are mostly placed in primary health care centres of both the public and private sectors. Figure 10 shows that in all LGAs except Surulere, the number of CHEWs per primary health facility where they are supposed to be posted is significantly lower than the recommended number as per the Ward Minimum Healthcare Package.
According to the National Primary Health Care Policy Guidelines, CHEWs are expected to perform a wide range of functions which include home visits, health education, nutrition and disease surveillance, maternal and child health and family planning activities. Also included are community
0
10
20
30
40
50
60
70
80
90
100
noteffective at all
fairly effective
veryeffective
Figure 11:
Perceptions of the Efficacy of CHEWs (2010)
Source: Bureau of Statistics, Ministry of Economic Planning and Budget, p.425
Lagos State Government, Household Survey 2010 Edition, Lagos
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
25

attitudes and behaviours towards patients, which leave a lot to be desired.
Preventives services, delivered mainly by primary healthcare (PHC) facilities, ranges from family planning for adults and adolescents to immunization for children, to pregnancy care, such as antenatal care or elimination of mother-to-child transmission (EMTCT) of HIV/AIDS. Preventive care, especially relevant in the slum areas, also includes efforts to provide water, sanitation and hygiene, collectively known as WASH interventions.
2.2 Preventiveservices
community level. For example, only 25% of all households in Lagos have at least one LLIN. Effective coverage is even less encouraging as only 6.5% of all under-five children had slept under an LLIN the previous night as per the NDHS 2008. In relation to exclusive breastfeeding, the overall performance for Lagos is low regardless of wealth quintile. According to public health experts and community leaders consulted during workshops, these performance gaps at the community level are largely linked to a lack of knowledge, low risk perception on the part of many mothers, the negative influence of family members (e.g. mothers-in-law and husbands) and also socio-cultural and traditional beliefs and practices. Communit ies' representatives also underscored the issues around the lack of trained health workers as well as their
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
General Hospital PHC
Frequency of HIV Counselling
None
On demand
Weekly
Daily
Source: Ministry Health Facility Assessment Baseline Data, Report compiled by the Department of Community Health, College of Medicine, University of Lagos, April 2010
of Health, Department of Reproductive Health (2010) UNFPA supported -
Figure 12:
Frequency of HIV Counselling in General Hospitals and PHC in Lagos
26
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Child Health Weeks in 2009 after the launch of the Integrated Maternal, Newborn and Child Health Strategy in 2007).
There are over 56 HIV Counselling and Testing (HCT) sites within the state and several mobile HCT initiatives providing free HIV counselling and testing services. App rox ima te l y 350 ,000 pe rsons (cumulative) have received counselling and testing for HIV to date. Despite the State's significant efforts to provide HCT services, survey data show that large proportions have not been reached with services. Also, it appears that the youth, while targeted, have not been prioritized overall by the state response actors.
The analysis of coverage for the different preventive services shows different levels of performance. Coverage levels for services such as antenatal care (80% coverage) or immunization (80% coverage of Penta 3) is relatively high compared to other services such as family planning (27.5%, NDHS
452008 ).
Reasons for the increased coverage for some interventions compared to others can be partly explained by the commitment of the health sector and of health workers to focused campaigns such as National Immunizat ion P lus Days, Annua l Breastfeeding Week, and Child Health Weeks (changed to Maternal Neonatal and
Source: Ministry of Health, Department of Reproductive Health (2010) UNFPA - supported Health Facility Assessment Baseline Data , Report compiled by the Department of Community Health, College of Medicine, University of Lagos, April 2010
-
Figure 13:
Availability of HIV Counselling in General Hospitals and PHC in Lagos State
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
General Hospital PHC
HIV counselling
Non available
Available
43NDHS, 2008.44Lagos, 2010.45Proportion of married women with demand for family planning currently using a modern contraceptive method (NDHS 2008).
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
27

worrying,given that Lagos has an estimated 220,000 people living with HIV (PLHIV), about 40% of whom would require ART. There are 286 health facilities offering antenatal care (ANC) in Lagos state, but only 28 (10%) offer PMTCT services. These sites tend to be located in urban local government areas, and only a few can be accessed by those who live in rural areas.
Major challenges in expanding access to preventive services are very muchlinked to creating the demand for and sustaining the
Approximately 65,000 pregnant women have been counselled, tested and have received their results. Unfortunately only 50% of them received antiretroviral prophylaxis.
There are 16 sites that provide free adult and paediatric antiretroviral therapy (ART) in the state, most located in general hospitals. To date over 10,000 persons have been reached with ART. This includes first and second line medications, with children accounting for about 10% of these clients. This coverage is
Elimination of Mother to Child Transmission
Currently Nigeria accounts for 32% of the global unmet needs for Elimination of Mother to aChild Transmission (EMTCT) of HIV in 2010. This situation has made the international
community focus on Nigeria in relation to EMTCT. This has resulted in Nigeria joining the global drive for EMTCT by 2015, through reducing new infections among women by 50%, reducing unmet need for family planning by 100%, providing ARVs to 90% of women and children in need, including during breastfeeding, and limiting breastfeeding among HIV positive women to 12 months.
The prevalence of HIV/AIDS in Lagos State is now 5.1%, which is one percentage point higher bthan the national average at 4.1%. HIV prevalence in both metropolitan and rural areas have
been on the increase over the years and are notably high in Lagos Island where they stood at c9% in 2008. The quality of services provided to people living with AIDS in Lagos needs
dimprovements with HIV-affected patients being subject to stigma from health providers. Traditional birth attendants, which attend to a large proportion of birth deliveries in Lagos still
elack knowledge and practice of prevention of mother-to-child transmission of HIV.
This existing network allows coverage of less than 25% of the estimated targeted population. It is therefore urgent to increase the availability of testing and treatment for pregnant women as well as to develop strong social communication mechanisms to increase awareness among the population if Lagos wants to able to fight effectively the specificity of HIV.
Lagos State is well placed to demonstrate movement against these ambitious targets. Currently the HIV comprehensive knowledge among men and women, knowledge that ARVs can reduce MTCT, and coverage of MNCH services is significantly higher than the national average. A commitment to provide PMTCT services as part of IMNCH services at all sites currently providing antenatal care (ANC), would dramatically increase PMTCT coverage in Lagos in a one year.
a Towards Universal Access, Scaling up priority interventions in the Health Sector response, 2010, WHO, UNAIDS and UNICEF.b 2010 HIV estimates.c Lagos State HIV/AIDS Response Review (2006–2010) and Lagos State HIV/AIDS Strategic Plan (2010–2015), p.29.d Adebajo, S.B., Bamgbala, A.O., Oyediran, M.A. “Attitudes of health care providers to persons living with HIV / AIDS in Lagos State, Nigeria”, African Journal of Reproductive Health, 2003, 7(1):103-112.e Balogun M, Odeyemi K. Knowledge and practice of prevention of mother-to-child transmission of HIV among traditional birth attendants in Lagos State, Nigeria, Pan African Med J., 29 April 2010, 5:7.
46Lagos State ERPS, 2009.
28
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

maternal and neonatal care, such as skilled birth deliveries, or child and adult care in the treatment of respiratory infections, to more complex management of diseases of public health importance such as tuberculosis, as well as more advanced service provision of procedures like C-sections.
Over the years, health investments have been concentrated in strengthening secondary and tertiary care facilities where specialized care is provided. The analysis of key bottlenecks affecting the effective delivery of facility-based interventions emphasizes the need to rebalance the entire pyramid of care by reducing the burden on high-level hospitals and reinstating the primary healthcare (PHC) centre as the foundation and entry point of the health system.
2.3.1 Underutilization ofexisting facilities
Efforts undertaken by the State Government to strengthen secondary facilities are showcased in Table 3. However, high-level facilities remain seriously underutilized with l ess than 50% bed occupancy.Reports have highlighted the crucial choices made by women on the uptake of services and health outcomes regardless of availability and access to services. It seems that a high proportion of women living in urban areas, which are well served by hospitals, still opt for non-facility based care.
supply of these services. Regarding family planning services for example, 73% of married women are currently using any contraceptive method. However, only 27.5% of them use modern methods. The total fertility rate (TFR) of Lagos state is 5.7%, which is high. This is likely linked to the socio-cultural, traditional and religious issues as identified in the bottleneck analysis. In addition, gender-based approaches are key, especially ensuring the involvement of husbands. Reduction in the number of children per householdand the proper spacing of the children would allow families theopportunity to adequately care for their children.
The situation of water, sanitation and hygiene in Lagos is also of concern. Urban water supply is making some improvements, but needs concerted strengthening. Lagos State has an installed water supply capacity of 160 million gallons per day (712.9 million litres per day). However, the Lagos Water Corporation facilities have an operational capacity of 57.2% and supplies water to only about 6.68 million people, about 40% of the state's population. Agboyi-Ketu andIbeju-Lekki LGAs do not have access to piped water. Only 5% of the Lagos State rural population is being served.
Curative services are services provided at health facilities ranging from primary level
2.3 Clinical care
Table 3:
Lagos State Health Service Commission Annual report
Year Total New Cases Out-Patient Attendances
Admissions (In-Patients) Bed Occupancy Rate (%)
2005 1,756,247 38,805 38.50
2006 2,202,993 45,059 30.65
2007
3,150,718 57,388 47.07 2008
Utilization of Public Secondary Health Facilities Services in Lagos State (2005-2008)
2,521,921 49,404 32.57
47NDHS, 2008.48Lagos State Water Supply and Sanitation Policy, November 2010; Lagos Water Corporation: Organizational History 2010 (www.lagoswater.org).49Lagos State Water Supply and Sanitation Policy, November 2010.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
29

Although AIDS contributes to only 3% of under-five mortality, HIV prevalence among those receiving antenatal care (ANC) is 5.1% in Lagos State. Knowing that HIV contributes to about 10.6% of deaths in women of reproductive age in most HIV-affected countries, HIV is likely to be a substantial underlying cause of maternal deaths in Lagos.
2.3.2 Misdistribution ofhuman resources
There are 6,747 medical doctors in private and public facilities in the state, with about 2,413 (35.76%) in public-owned facilities and 4,334 (64.24%) in private facilities. Ikeja LGA has the highest number of medical doctors in both private and public health facilities (999) while Ibeju-lekki has the lowest number of medical doctors in both private and public health facilities (36). There are 717 pharmacists in private and public facilities in the state, with about 418 in public, government-owned facilities and 218 in private facilities, while a total of 13,653 certified or registered nurses/midwives are available in both private and public facilities, with about 6,331 in public owned facilities and 7,322 in private facilities across the 20 LGAs in the state.
Their decisions to give birth with or without skilled attendants are still poorly understood. Nonetheless, several factors need mentioning.
Physical access to maternal facilities remains a concern. Indeed, LGAs with the highest maternal mortality rates such as Alimosho tend to have high population density relative to the availability of public health facilities providing specialised emergency care.
Socio-economic factors (low income, lower education levels), cultural values (perception among Yoruba communities that caesarean section or non-vaginal delivery is not acceptable) and religious beliefs are major determinants of maternal health care seeking in Lagos. In Isale Eko, one of Lagos' oldest slums, the majority of motherswho delivered outside of hospitals were assisted by traditional birth attendants (TBAs), despite numerous primary, secondary, and tertiary health facilities in the area. Hence, dealing with non-clinical factors (e.g. by training TBAs or providing maternal education) may matter as much as making maternity services with skilled birth attendants more
51accessible.
Figure 14:
Distribution of Nurses in all private and public health facilities (per 100,000 LGA population)
50Olusanya B.O., Alakija O.P., Inem V.A., “Non-Uptake of Facility-Based Maternity Services in an Inner-City Community in Lagos, Nigeria: an Observational Study,” J. Biosoc. Sci., 2010, 42, pp. 341–358.51Ibid.
52Factors contributing to Maternal Mortality in North-Central Nigeria, a 17-year review by LAO Kujah, 2005.
30
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Career elevation, which favours tertiary and secondary rather than primary health care facilities.
Different bodies regulate each cadre of personnel, i.e. Local Government Comm i s s i o n , Hea l t h Se r v i c e Commission, Primary Health Care Board, State Government, and Federal Government.
2.3.3 Financial accessibilityand affordability of health care and drugs
Financial barriers to health are major constraints to equitable health care in Lagos. Out-of-pocket expenditures represented 70% of all health expenditures in 2005, a large part of which financed medical fees and drugs bought in the private sector (Figure 16).
The average density of doctors in the state per 100,000 inhabitants is 33, which is slightly lower than the national figure of 37 doctors per 100,000 as of 2007. It is also estimated that approximately 60% of newly graduated doctors start their careers in the public sector.
There are considerable imbalances in the distribution of the health workforce. Across the tiers of service provision, it is estimated that 19% of doctors, 31% of nurse/ midwives, 38% of pharmacists and 42% of laboratory scientists provide services at the primary level of care. The majority of the other cadres of staff provide services at the secondary and tertiary levels. In addition, the availability of each medical staff varies substantially across LGAs (Figures 14 and15).The misdistribution of the health workforce can be attributed to the following institutional factors:
Figure 15:
Certified / Registered Nurse & Midwives in all private and public facilities (per 100,000 population)
0
20
40
60
80
100
120
140
160
180
200
Num
ber
per
100,0
00 p
opula
tion
53National HRH Strategic Plan, 2008-2010.54LSSHDP, 2010–2015.55Ibid.56Lagos State Ministry of Health, Service Availability Mapping (SAM) 2010.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
31

-
Federal Government
14.0% State Government5.6%
Local 0.4%
Governments
Households70.0%
Firms9.1%
Development partners
0.9%
Source: Table 4.97 in Soyibo A., Olaniyan O, Lawanson A.O. (2009) National Health Accounts of Nigeria 2003-2005 Incorporating Sub-National Health Accounts of States, Vol. I Main Report, submitted to the Federal Ministry of Health, Abuja., December 2009,
Figure 16:
Health Financing Sources in Lagos State (2005)
Source: Table 4.98 in Soyibo A., Olaniyan O, Lawanson A.O. (2009) National Health Accounts of Nigeria 2003-2005 Incorporating Sub-National Health Accounts of States, Vol. I Main Report, submitted to the Federal Ministry of Health, Abuja., December 2009,
Figure 17:
Allocation of Out of Pocket Expenditures for Health by Type of Service Provider in Lagos State (2005)
Federal Health Fac
10%
State Health fac
12%LGA health fac
5%NGOs2%
Private facilities63%
Chemist traditional
care8%
32
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

affecting effective implementation of the free care initiative for maternal and child health.
2.3.4 Perceived quality of care
Quality of care and perceived quality of services have been identified as particularly important concerns during consultations with representatives from communities. Public health experts suggest that under staffing in primary health care facilities is mainly responsible for the unfriendly atmosphere for patients. This inhospitable environment would also explain why people in Lagos State are more likely to seek care directly at secondary-level clinics rather than at PHC centres.
2.3.5 Role of the private sector
Difficulties in the public health sector may also explain why a significant proportion of
Another pressing issue is that of fee-paying (privately owned) pharmacies versus government-owned pharmacies, where drugs and insecticide-treated nets (ITNs) are provided for free. Since government pharmacies are often out of stock, drugs available for free are sold at private pharmacies in the same facility.
Such high levels of out-of-pocket expenditures bring to light the case of the poorest households, for whom such expenses are likely to represent catastrophic expenditures. In Lagos, out-of-pocket expenses account for 19% of total per capita expenditures on average. Among the poorest households, they represent 11% of their total
57expenditures.
The difficulties faced by the procurement and supply system of essential medicines should be further investigated through an operational research, as it has been identified as one of the main bottlenecks
Figure 18:
Out-patients seen in public vs private facilities (by LGA)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%Out - patients seen in Public Facility Out - patients seen in Private Facility
Source: Lagos Health Service Availablity Mapping (2010)
57Gustafsson-Wright, E., and J. van der Gaag,An Analysis of Nigeria's Health Sector by State, Amsterdam Institute for International Development, August 2008.58Ibid.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
33

health care delivery need to be more thoroughly understood in order to be able to design policies and a regulatory environment that are able to tackle existing quality and affordability issues related to private or
59traditional practices.
The types and quality of services provided by the private sector can be inequitably distributed depending on wealth. Indeed, the private sector used by the households in the richest quintile are not likely to be the same as those used by the poorest households, whether in terms of costs or provided quality. Avenues to build partnerships with the private sector will need to account for these differences to ensure that access to health is indeed equitable.
the population prefers to seek care in the private sector despite the cost. In fact, the private sector predominates in health care delivery,with 79% of PHC facilities privately owned. Insome LGAs, almost 90% of consultations are performed in the private sector (Table 4). In total, 63% of out-of-pocket expenditures are spent in private facilities while 8% go to chemists or traditional birth attendants. Major private actors also include traditional practitioners, who play a social as well as a medical function in the community.
In this context, partnering with the private sector will be critical to strengthen delivery of clinical services to all who live in Lagos State. Benefits and shortcomings in private
Table 4:
Ownership
Government 21
Private for Profit 73
Non-profit 6
Primary Health Care Facilities in Lagos by ownership and type of facility
Facility Type
Basic Health Centre 73
Comprehensive Health Centre 20
Hospitals 7
SourceEvidence from Four States”,p.13.
: World Bank, 2010, “Improving Primary Health Care Delivery in Nigeria:
59Olusanya, B.O., Roberts, A.A., Olufunlayo, T.F., Inem, V.A. “Preference for private hospital-based maternity services in inner-city Lagos, Nigeria: An observational study.”Health Policy.August 2010, 96(3):210-6.
34
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

build on this momentum and accelerate efforts underway—efforts to leverage improvements for the health of all people in Lagos State.
One of the major constraints in ensuring effective coverage of health interventions in Lagos is the insufficient supply of health services, especially for the poorest and most disadvantaged communities.
3.1.1 Increase the human workforce available to the most under-served populations
The number of community health extension workers (CHEWs) in Lagos falls well short of
3.1 Bring healthservices closer tocommunities
Residents of Lagos have a wide array of health service providers from which to choose. These range from
teaching hospitals, general hospitals to secondary-level and primary health care
centres, and from private clinics and chemists to traditional health providers. This vibrant context provides a range of opportunities for the Government of Lagos, together with its partners and communities, to pro-actively plan to ensure universal access to health—finding innovative ways to effectively cover communities and families through the entire health system.
The Government of Lagos has already initiated a number of health policies aimed at removing many bottlenecks described in the previous section (and summarized in Appendix D). Indeed, policymakers have created considerable political momentum to improve the health system in Lagos. Therefore, rather than presenting a new set of policy recommendations, this section highlights a series of actions that could
3. STRATEGIES TO IMPROVE ACCESS: Building on a Strong Foundation
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
35

high, it is likely that political decisions will need to be taken at both State and LGA levels with regard to developing capacity for training, supervision and remuneration of CHEWs.
b. Institute rotating posts for doctors and nurses, along with performance-based financing.
A key measure to redress the misdistribution of doctors and nurses across the three tiers of the health system is the provision of incentives for staff to take up rotational postings in PHCs as part of their career elevation. This should be combined with performance-based financing, a form of contracting that uses incentives to motivate individuals and institutions to improve their performance. These contracts are structured around outputs, as opposed to inputs or working processes. This type of contracting is a key way to make service providers more accountable by linking pay to measurable results.
c. Use performance-based contracts with private health providers. Performance-based contracts are seen as a key instrument to expand the use of public
finances to pay private health providers to deliver basic health services to the poor, especially in slums. For example, contracts could specify that services be delivered to a certain number of people from vulnerable groups. While this type of contracting is not new, it has been getting more attention in the past few years in recognition that the private sector can, in some cases, deliver
the recommended number of 1 CHEW per 1,000 of the populat ion as per recommended national standards set in the NPHCDA Minimum Essential Package of Care (see Figure 10). Primary healthcare (PHC) centres are also short of qualified doctors and nurses, who are more likely to be found in secondary and tertiary-level facilities. There are also steep inequities in the distribution of available human resources across local government areas (LGAs). Three measures are advised to redress the imbalance in health resources across the three levels of the pyramid of care, and across LGAs:
a. Recruit, train and supervise more community health extension workers.
CHEWs must be employed up to the recommended national minimum standards in each PHC facility (Table 5) in order to bring essential health services closer to communities. Indeed, their role is critical to the provision of information about essential health services, including which services can to be found at relevant facilities. To perform their roles, CHEWs will need to be given clear tasks, responsibilities and areas of responsibility.
They will also need to be supported with renewed motivation, supervision and training. One promising path is to expand existing initiatives conducted by the PHC Board to reorder CHEW's roles and responsibil ities towards conducting outreach activities and acting as links between health facilities and communities. Since the numbers of required CHEWs is
Recommended human resources required for a primary healthcare centre to provide the Minimum Health Care Package (NPHCDA)
Health Post:
Primary Health Clinic: 2 community health extension workers (CHEW); 4 JCHEWs
Primary Health Care Centre (Ward Health Centre):1 community health officer (CHO); 1 public health nurse; 3 CHEWs; 6 JCHEWs; 3 nurse/midwives; 1 medical assistant (optional)
1 junior community health extension worker (JCHEW)
Source: NPHCDA 2007. Ward Minimum Health Care Package
36
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
37
Conducting regular outreach interventions
that go beyond campaigns (e.g. Health
Weeks) in order to increase coverage is
crucial to achieving the health related MDGs.
This can be carried out using the support of
the CHEWs to deliver services on family
planning, immunisation, HIV counselling and
testing and antenatal care. In addition, the
educational aspect of the outreach would
need to be strengthened to ensure
information geared towards removing the
bottleneck of tradition, cultural and religious
beliefs and myths.
3.1.4 Expand efforts to lower
financial barriers and the cost of
care
The issue of financial resources is one of the
problems the government faces in providing
quality health services for all. In the past,
Lagos State has relied heavily on the federal
allocation for health. However, the trend has
changed since 2003 with the drive to
increase internally generated revenue.
Out-of-pocket expenditures contributed by
individual households represented 70% of
total health expenditures in 2005. This is
comparable to other sub-Saharan African
countries, which average 79.5% as against
about 20% in high-income countries. All
high-income countries have more equitable
health care services except the USA.
The issue of cost for care and out-of-pocket
expenditure is not a Lagos specific problem.
This is a common issue in most developing
nations and major metropolis such as Lagos.
In addition to this, even if costs are
acceptably low, utilization will still rely
heavily on public attitude and perception
about the service provision. People are
willing to pay for services if they feel that the
services are good. However, many still
question government's capacity to provide
good public services.
essential health services to poor people as or more efficiently than the public sector.
3.1.2 Rehabilitate and revitalize primary healthcare(PHC) centres
A number of initiatives are underway here that can be built upon. The ongoing revitalization of 57 Flagship PHCs by the Public Health Care Board goes some way towards improving the supply of services at the primary care level. Selected PHCs will be provided with water, electricity, a clean environment, proper disposal of waste products, a generator for each facility, and concomitant recruitment of required human resources. The supply chain management of essential commodities required for immunisation, family planning, and the treatment of diarrhoeal diseases through the Drug Revolving Fund (DRF) and Free Drug Initiatives will also be strengthened.
Other current and essential initiatives to strengthen existing health care systems in Lagos State include scaling up the presence of skilled attendants at delivery and expanding facility-based services for women. They should be complemented by community-oriented initiatives that will effectively address the socio-cultural dynamics that underpin maternal health-seeking behaviour, particularly in the slum areas. Such interventions should be targeted at both providers of services and their clients, particularly at antenatal clinics.
3.1.3 Implement pro-activeoutreach
Interventions and strategies for improving reproductive, maternal, newborn and child health and survival are closely related and must be provided through a continuum-of-care approach. When linked together and included as integrated programmes, these interventions can lower costs, promote greater efficiencies and reduce duplication
60of resources.
60A Global Review of the Key Interventions related to Reproductive, Maternal, Newborn and Child Health (RMN CH), The Partnership for Maternal, Newborn and Child Health, 2011.
61Soyibo A., Olaniyan O, Lawanson A.O. (2009) National Health Accounts of Nigeria 2003-2005 Incorporating Sub-National Health Accounts of States, Vol. I Main Report, submitted to the Federal Ministry of Health, Abuja, December 2009.62World Bank, 2005; IMF, 2005; WHO, 2005.

because I found out that the common complaints we hear from these people are all traceable to poor environmental hygiene. Cases of diarrhea, vomiting, fever and malaria are rampant”.
However, for Bimbo, home visits have become less frequent. She now consults mainly at the Primary health Care Centers and does follow-up via the telephone. ”The
increasing GSM coverage throughout Lagos metropolis makes it possible and easier that way especially when I do not readily have the materials and drugs to dispense to them when I visit” she explains.
Beyond the assigned duties, Bimbo has had to fund the purchase of drugs she prescribed for her patients when they come for treatment and the drugs are out of stock while the patients have no money to buy them from the drug store. “Sometimes we even have to provide food out of pocket for some patients that need injections but did not eat before coming to the center and have no money to buy food right away“. However, “Knowing that through this work I can help alleviate the pains of others - especially in the poor communities - makes me very happy”.
Bimbo Asalu, 38, was born and raised in Mushin, a suburb of Lagos state. Like most Lagosians, Bimbo's parents migrated from neighboring Ogun state in search of economic prosperity. A commercial and industrial hub, Lagos is a hotbed for such migrations and is fast becoming one of the world's largest cities, home to myriad Nigerian ethnicities as well as foreign nationalities.
Bimbo had always wanted to go into medical practice due to the care she received at a teaching hospital where her parents took her for a dental treatment. “When I saw how some young doctors were attending to people so smartly and nicely I started dreaming to be like them. And after what they gave me took care of my prolonged toothache, I made up my mind to go into the medical profession if only to help alleviate other people's pains, too” she says.
As a Community Health Extension Worker (CHEW), Bimbo's job involves home visits, health education, nutrition, disease surveillance, maternal & child health and family planning activities. All these services help bring essential preventive and follow up care right to the doorsteps of people in the communities. “I do more of health education
Going the extra mile - a community health extension worker in Eti-Osa Local Council
Bimbo Asalu examines a child strapped to his mother's back at the Eti Osa Primary Health Care Center
38
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
39
Proposals to Strengthen Existing Campaigns
Annual Breastfeeding Week
This campaign is in line with the 2008 Lancet Nutrition Series [4] that reinforced the
significance of optimal IYCF on child survival. Optimal IYCF, especially exclusive
breastfeeding, was estimated to prevent potentially 1.4 million deaths every year among
children under five (out of the approximately 10 million annual deaths). The observance of this
week is done annually in Lagos State, but its effect is unknown as there is no available
anecdotal or empirical data. The rate of exclusive breastfeeding is still low at 13% (NDHS
2008). Because of weaknesses in complementary feeding amongst others, 21% of children are
stunted, while 10.1% of children are wasted. The rate for underweight children is slightly
better at 9.8%.
The current campaign primarily places emphasis on social mobilization and media campaigns;
and it is led by the wife of the Governor of the State and simultaneously decentralized with
campaigns led by the wives of the Local Government Chairmen. This has yielded some good
results, especially for radio call in programmes and other media events which result in good
participation of women. However, this is insufficient given the Lagos context in which working
mothers have long drives to and from work (the infamous Lagos traffic) and the opportunity
costs for women such as traders and other daily waged women who need to generate daily
income to feed themselves and the other non-breastfeeding children. The campaigns need to
be strengthened to take into consideration the challenges of the diverse groups of women in
Lagos State and address each subgroup appropriately.
IMCI (MNCH Weeks), National Immunization Days, Supplemental Immunization Plus Days, etc.
The implementation of child survival interventions in Lagos State was largely vertical, focusing
on immunization, malaria control and breastfeeding promotion. However, the state has
adopted the national strategy of conducting Maternal New-born Child Health weeks twice a
year. This provides a valuable platform to improve the health-seeking behaviours of the whole
family, especially mothers and caregivers of children under five years of age. It allows for the
promotion of services such as routine immunization for children aged between 0 and 59
months; de-worming for kids aged 1 and older, malnutrition assessments, and the use of long-
lasting insecticide treated nets (LLITN).
The MNCHW has been successful for the most part, but has not been without challenges. Over
the past years, social mobilization in Lagos State has been one of the weakest points.
Availability of commodities such as de-worming tablets has also been an issue. The biggest
challenge in Lagos however still remains the lack of effective coverage of the riverine areas of
the state. However, noting these challenges, concerted efforts have been made by
policymakers, traditional, religious and community leaders, service providers and care givers at
all levels to ensure improved social mobilization. This has improved the coverage over the last
events with a notable improvement in November 2011.
In addition to the MNCHW, National Immunization Days (NIDs) are implemented in the state.
These are aimed at polio eradication and Vitamin A supplementations. A main challenge is
social mobilization. Lagos State has been wild polio virus (WPV) free for over three years. The
State government has indicated its commitment to ensure that it remains WPV free. The state
is very strategic to the country as it is the commercial and industrial nerve centre of the nation.
WPV in Lagos could translate into a catastrophe for Nigeria and even West Africa, given the
sub-regional trade in Lagos. Indeed, given the centrality and complexity of Lagos, there is a
need to ensure sustained social mobilization for NIDs and SIPDs.

40
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
3.2 Bring communitiescloser to health
3.2.1 Affirm the right to health for all of the people of Lagos State
The Convention on the Rights of the Child was ratified by Nigeria in 1991, and subsequently, a Child Rights Act was enacted in 2003 at the federal level. Lagos State built upon both instruments and successfully passed the Lagos State Child Rights Law in 2007. The right to health is a fundamental part of the law, and it clearly articulates the responsibility of duty bearers to fulfil those rights. Duty bearers such as the state government, inclusive of its health sector organs, must ensure provision of quality services without discrimination to any child.
This remains a challenge in the Lagos context, especially given the mobile populations and difficulties in identifying and serving hard-to-reach and marginalized populations. The absence of data on rights holders does not negate the binding responsibilities of the duty bearers to ensure fulfilment of their rights.
In Lagos, birth registration, a critical element to ensuring the fulfilment of other rights, remains low, at 62%. Although some children are not registered and go uncounted, the knowledge of their existence begs the fulfilment of their rights.
However, there are also responsibilities that accompany any set of rights. Rights holders should insist on the fulfilment of their rights and have a crucial role to play in holding duty bearers accountable.
3.2.2 Encourage activecommunity participation
Active community participation in health care means that people should be knowledgeable about their own health problems. They should identify the needs for their solution or reduction, and draw out
Nonetheless, Lagos State has initiated a
range of efforts to remove financial barriers,
such as the Free Health care initiative and
the Community-Based Health Insurance
Scheme. The state is also keying into the
National Health Insurance Scheme to ensure
that free premiums are given to the poorest.
However, this initiative is only being piloted
in one LGA at this stage, and should be
evaluated and scaled up. There might be a
need to consider a customized scheme for
the poorest of the poor, with costs fully
borne by the state.
Unfortunately, due to the complex
demographic challenges of Lagos State, the
Free Health care initiative is inadequately
budgeted to cater for all dependent groups
(under 12 and over 60 year-old). The scheme
is also too limited in scope to have a
significant impact on removing financial
barriers. The bottleneck analysis clearly
revealed numerous hidden costs in the
health sector for services, which are
supposed to be free. The insurance scheme
might not necessarily address this
phenomenon. It will have to be addressed
through a system that ensures that all health
workers who charge additional fees to
clients are disciplined. This would curtail the
practice significantly. Establishing a State
Health Insurance Scheme to provide social
health protection for all categories of the
population — including the formal sector
(public and private), informal sector, rural
dwellers, retirees/pensioners, the poor and
vulnerable — would go a long way towards
alleviating the high financial burden of health
care borne by residents of Lagos State. Other
options to explore include conditional cash
transfers. Cash transfer programmes are
emerging as indispensable components of
poverty reduction strategies with its short-
term objectives of alleviating poverty and the
long-term human capital development goals.
Although Lagos State does not have any
documented on-going conditional cash
transfer (CCTs), there are some lessons
which could be learned from the education
sector's pilot of CCTs in two other states.
Lagos State could take a cue from the
pilot projects, study the lessons, and
design an appropriate model for the health
sector.

Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
41
activitieswithin their wards. This includes identifying the ward's health and social needs, plan solutions, mobilize human and material resources, as well as supervise, monitor and evaluate health activities in the ward. Further responsibilities may soon include mobilization of community participation in health, liaison with government, NGO and other partners in implementing of health programmes, supervision and support to traditional birth attendants, volunteer health workers and community health workers and support for the establishment of health facilities and overseeing their functions at ward level. WHDCs can be further developed to play a greater role in community health issues such as health promotion for the management of diarrhoea, hand washing, and the distribution of LLINs. They are currently being trained to serve as a critical link between the community and primary health facilities.
To further boost their status, the WHDCs should appoint community volunteers with the primary responsibility of conducting the activities of the WHDC. These volunteers would also liaise with the health facilities and possiblybe involved in the PHC management committee. However, depending on the size of ward, the committee should decide how many community volunteers are required. A typical ward in Nigeria ranges from 15–20,000, but in Lagos, this averages about 54,500 persons per ward.
Lagos has developed and is now implementing a plan to ensure its status as a megacity by the year 2020. Lagos has also articulated its desire to be Africa's best, as in its adopted slogan: the Centre of Excellence, and as stated in the Lagos State Health
3.3 Guarantee the quality of essentialhealth services
plans of action according to the priority and the resources available. They should also organize and implement these programmes, and monitor and control their progress, periodically evaluate, seek feedback, and revise their programmes. However, under poor social and economic conditions as in the Lagos slums, it may be hard to expect spontaneous participation from the people. People have to be mobilized and encouraged to take responsibility for the maintenance of their own health. Initially, the involvement may be passive, and this has to be gradually and progressively made more active.
63The Lagos State Government has already cited the work of its various health missions, stating that bringing “care and healing closer to our citizens will continue as will our preventiveand advocacy strategy on blindness prevention, diabetes and hypertension, cancer screening, [making] Lagos Polio free [and] eradicating and curbing the contagion of malaria.” This demonstrates the state's recognition of and commitment to bringing health closer to its citizens. Accomplishing this goal will require duty bearers and rights holders to work together to strengthen the health system overall.
3.2.3 Empower communityvolunteers by giving themstatus
Existing structures in the local government are positioned to support the empowerment of communities in getting closer to the health system. The Lagos State Primary Healthcare Board has oversight functions for establishing and supporting the local government health authorities. They also have oversight for strengthening Ward Health Development Committees (WHDC). The WHDC is a multi-disciplinary body at the ward level and is made up of community members.
The WHDCs in Lagos' 376 wards are tasked with coordinating primary health care
63 2011 Lagos State Budget Report, p.11.

“is a problem” says Olabisi, “most of our
women whose labour pains come at night
often resort to patronizing quacks or the
traditional birth attendants and in most
cases have lost their babies or had serious
complications in the process”.
Determined to get the authorities to increase
access by providing health care services
round the clock, Olabisi initiated a local
campaign calling for a 24- hour shifts in their
health center. She currently encourages
other women through an existing pressure
group of women and artisans to speak up for
this course. The group has their own home-
grown sustainable idea of how government
can increase the staff strength of the health
center as well as run 24 hour shifts. “We are
encouraging them to train some of our
children who are out of secondary schools as
health care providers because they
understand our problems and are
permanently here to care for us at any time
of the day or night” Olabisi concluded.
Thirty five year old Olabisi Sousu runs a small tailoring business from her home in Sagbokoji, a small island off the Apapa side of the Lagos Lagoon in Amuwo-Odofin local council. At Sagbokoji, access tobasic social amenitiesis a luxury. Before the Primary Health Care Centre in the community was commissioned, Bisi, a mother of three and other members of the community have to regularly brave the rough sea by boat to cross into Apapa, followed by a two hours trek to the nearest government hospital. “I almost gave birth to my first child on the road because it was at night that the labour started. After we managed to cross the sea into Apapa, we did not see any okada (motor bike) to take me to the hospital” she said.
The new health center provides basic
services such as immunization, ante-natal
and post natal care. However, the center
does not run a 24-hour shift. The hospital
staff resides outside the community where
social amenities are better. This arrangement
Community Action in a Riverine Area - Change Starts with an Individual
Bim
bo
Asa
lu e
xam
ines
a c
hild
str
apped to h
is m
oth
er's
ba
ck a
t th
e E
ti O
sa P
rim
ary
Health
Care
Cente
r
Olabisi with her 7 month old baby outside her home
42
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Reaching the hidden population of the slums: A transect walk through a slum in Lagos
It is well known globally that addressing the needs of slum dwellers is a major challenge that depends on the nature of the slums and the existing socio-political structures. More structured slums provide a means through which targeting key health interventions can be successful. Because this analysis does not have the requisite data to support general statements on the makeup of slums in Lagos, a field visited was conducted in two slums located in the Ajeromi local government area.
The two slums that were visited are parallel to each other, divided by a canal. The slums fall into two wards, Akere and Owoyemi. They share several similarities, but there are also many differences between them. With the desperate fight for living space, migrants have reclaimed land on both edges of the canal with trash and debris – hence widening both Akere and Owoyemi wards and reducing the width of the canal between the two. A key difference between the two slums pertains to their informal governance structures. The slum of Owoyemi (Aganyi) had an organized system for community mobilization, information dissemination and communal works such as construction of pedestrian bridges and some minimal attempts at managing sanitation. By contrast, Akere slum on the other side of the canal was unorganized in this regard. As a result, Akere was more environmentally unsafe than Owoyemi. Both slums had ready access to nearby public health facilities (MCC, general hospital) as well as several private health service providers and chemists located within the slums or nearby. Traditional birth attendants were also mentioned as major providers of antenatal care and maternal care for pregnant women. Slum residents met during the transect walk mentioned their reluctance to attend public health facilities because of long waiting time, the unfriendliness of the environment and the lower perceived quality of care compared to the private sector. It was also mentioned that drugs are rarely provided for free at public facilities because of drug stock-outs.
Based on observational information and qualitative discussions with community members, the following action points could be considered to facilitate access to health for slums residents:
Targeted outreach service: Ensure that key integrated services such as those for high-impact cost-effective interventions such as immunization, Vitamin A and others are taken to the slums in order to provide access to primary healthcare. This would be done through special outreach programmes by the LSMOH, which would specifically target the riverine areas and slums due to the fact that they are sometimes missed or underserved during regular campaigns. It could also be taken as a part of the already existing outreach services, but ensure that there are dedicated teams which are trained, given all necessary logistics and monitored to ensure that hard to reach areas are adequately covered.
Conditional Cash Transfer: Design and implement a programme to ensure that slum dwellers are given an incentive towards achieving certain health outcomes with an emphasis on preventive care. For example, the government could consider a provision of N500 to every pregnant woman (who meets agreed criteria) living in a slum for each completed ANC visit. This will require an operational research to really appreciate the effect and impact.
Free premium for health insurance: The government could consider underwriting the cost of premium for all slum dwellers as per the new definition that would be derived from the research proposed above.
Community mobilization and participation on health governance at ward level: Government should strengthen the informal leadership structure to engender active participation, a sense of ownership and sustainability of systems put in place with a view to inclusion of said representatives on health committees and boards.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
43

adhere to health policies and standing orders. Three elements have the potential to support the Lagos Health Ministry's vision.
3.3.1 Align Lagos healthservices with internationalstandards
Protocols must be aligned with international best practices as articulated by the Child Health Evaluation and Research Group (CHERG). Health worker training will have to undergo a strategic shift to be in line with the above protocols. This includes the revision of training workshops, on-the-job training and on-the-job supervision.
3.3.2 Pilot performance-basedfinancing
Regular performance assessments of health staff must be conducted. Funding should be disbursed to local government health authorities on the basis of two sets of results: the number of patients enrolled and performance on output and outcome-oriented tracers (health indicators) in the target group. Independent service providers
Ministry's vision statement,“to attain excellence in health service delivery by applying best practices at all levels of care.”
In order to achieve excellence, it is imperative that all policies, strategies, guidelines and tools are aligned with globally accepted best practices and evidence-based approaches. Today, closer attention needs to be paid to the implementation and monitoring of evidence-based strategies using innovative and participatory approaches. In this regard, trainings that take place in workshops held away from health workers' duty posts would need to be re-evaluated.
In addition, developing standards can prove futile if their implementation is not appropriately monitored to ensure timely feedback into subsequent reviews and planning. The health system must have coherent and in-built mechanisms to ensure that regulations are adhered to and that progress is captured and reported for lessons learned, best practices, and replication. A key part of this drive for implementation and monitoring is the need to strengthen performance management with strong reward and sanction mechanisms, which would signal to health workers the need to
An immunization team in the riverine areas.
44
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

programme monitoring for health in urban
settings with a view to tracking progress,
identifying shortfalls as well as corrective
actions. It is crucial to apply the monitoring
framework to a representative sample of all
57 LGAs/LCDAs. Institutionalize this
monitoring as part of the State Joint Annual
Review (JAR) processes. The newly
established Health Sector Partners' Forum is
expected to drive the annual JAR, and as
such should take the leadership on this
process.
should be reimbursed for eligible treatment provided to patients enrolled in the program. Beneficiaries would be free to choose their service provider and providers would compete for patients on the basis of quality.
3.3.3 Develop a decentralized monitoring system based on the identified health bottlenecks
Implement the WHO Urban HEART
monitoring framework that addresses
Urban Health Equity Matrix
The Urban Health Equity Matrix is a set of indicators in a simplified visual format to inform
policymakers and key stakeholders on local-level performance to guide the prioritization of local
and national policies and strategic interventions in terms of:
Where to focus national assistance on given specific weaknesses at the local level.
Comparing performance between different parts of a city and between cities.
The Urban HEART Matrix can be applied to the following areas:
Comparative performance of cities or neighbourhoods within cities. The Matrix summarizes
the performance of cities or urban areas in the different policy domains, and presents in a
simple visual form a relative comparison of city accomplishments.
Comparative effectiveness of policies and programmes. The Matrix provides a broad picture of
the effectiveness of policies and programme interventions as denoted by their indicators.
Figure 19 gives an example of the Matrix where the performance of neighbourhoods within a
city is plotted against their respective indicators of health determinants. A similar approach can
be applied to health outcome indicators. The colour codes in each square indicate the level of
accomplishment, with green denoting good performance and red denoting poor performance
(in relation to defined location-specific, national or international goals or averages), while
yellow denotes performance below the intended goal but better than the lower benchmark.
Columns represent the performance of neighbourhoods or cities based on the different
determinants. For example, a city or local urban area with many green squares is performing
better than a counterpart scoring many red squares.
Rows provide a broad picture of the effectiveness of a particular policy or programme
intervention.Extract from URBAN HEART, Urban Health Equity Assessment and Response Tool,
WHO:www.who.or.jp/urbanheart/UrbanHEART_GUIDE.pdf
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
45

INDICATORSLGA/LCDA
Ward 1
Ward 2
Ward 3
Ward4
Ward 5
Availability of essential commodities
Availability of human resources compared to Lagos Standards
Proportion of the population covered by 24-hour primary health care centre (PHC)
Proportion of targeted communities covered as planned with outreach session
Availability of EMTCT services at PHCs
Functional Free Drugs Initiative
Coverage of the National Health Insurance Scheme
Skilled birth attendance
Fully immunized children
Children sleeping under LLIN
Functional Ward Development committees
Number of active supervision compared to need
POLICYDOMAIN
AVAILABILITY OF SERVICES
UTILIZATION OF SERVICES
QUALITY OFCARE
Figure 19:
Health Equity Monitoring Matrix
Note: This matrix was adapted from the Urban HEART template for the Lagos Investment Case. Colours indicate the wards' level of performance. However, the colours here have been randomly chosen for illustration purposes.
46
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

access to primary care, priority interventions include rehabilitating existing PHC centres and ensuring adequate staffing through the redistribution of the health workforce. Bottlenecks affecting the demand for health are addressed by eliminating user fees for all quintiles and through cash transfers.
Modelling results show that an equity-focused strategy that prioritises access to evidence-based essential health services to the most under-served and deprived populations of Lagos is highly cost-effective: with an average of 15 USD additional per yearper capita, Lagos could expect to reduce under-five mortality by 50% and achieve a 30% reduction in maternal mortality by 2020.
The model's estimated reduction in maternal mortality by 2020 is substantial,with almost a third of maternal deaths are averted compared to today, but further efforts to accelerate maternal survival are still necessary.The estimated reduction is limited by inadequate knowledge of the magnitude of the different causes of maternal mortality. Improving knowledge will be critical to be able to better tailor maternal health preventive and curative interventions to the population in order to make sure that pregnancy in Lagos is a moment of happiness and not a life-threatening condition. Deaths of newborns in the first month of life are expected to be nearly halved during this period, according to the model.
The investment proposed here can also significantly reduce the impact of HIV/AIDS, tuberculosis and malaria. Indeed, such improvements of the Lagos health system can potentially reverse the HIV/AIDS epidemic by decreasing the number of new
4.2 More money for health, more health for the money
I
4.1 Strategiesmodelled
n order to get a sense of their cost and of their impact, the strategies to remove major health system bottlenecks
discussed in the previous chapter were modelled using the Marginal Budgeting for Bottleneck (MBB) tool as described in the Methodology section. The estimates of the investment required as well as the potential impact on health outcomes were calculated for a nine-year period from 2012 to 2020 in order to be aligned with Lagos State's Vision for 2020. Cost estimates present additional funds required to strengthen service delivery for reproductive, maternal, newborn and child health in order to focus on Lagos State's commitments to achieve the health MDGs.
Uncertainty concerning the total population of Lagos has been a major constraint for the costing of health system strengthening strategies. Indeed, investments needed for a population of 20 million are not the same as forone of 9 million. Costs presented in this section were calculated using population estimates of approximately 20 million inhabitants as per official estimates from Lagos State.To facilitate understanding of the results presented below, estimates are presented per capita, per year.
Key strategies for the revitalization of the primary health care system were modelled as presented in Table 6. A major focus is on improving community and family care through such policies as: task-shifting to community-based Integrated Maternal, Newborn, and Childhood Management of Illnesses; and human resources strategies to improve the performance, retention and deployment of community health workers in the most deprived areas. Another strong focus is to universalize access to preventive services through campaigns, outreach activities, and by strengthening the existing routine system. In terms of strengthening
4. THE INVESTMENT CASE: Results of the Cost and Impact Modelling
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
47

Service delivery modes
Community and family care
Preventive services (in facility or outreach)
Strong focus: Universal access through campaigns, outreach activities, and by strengthening the existing routine system.
Curative careModerate focus:
Limited infrastructure investment, mostly rehabilitation and upgrading.
Primary health care
Strong focus: Aims for universal access to skilled birth attendants. Full maternity services at primary levels including waiting houses.
Secondary and tertiary ospital
Moderate focus: Status quo plus upgrading of one district hospital for complicated emergency obstetric care.
Financial access
Direct cost Strong focus:
Elimination of user fees for all quintiles.
Contracting out of services to non-government providers.
Indirect cost Strong focus: Means-tested conditional cash transfers.
Community participation
Information, education, communication and participation in governance
Strong focus: Emphasizes community empowerment and demand promotion and continuity in partnership with community based enablers and promoters.
Additional cost
Supply side
Pre-service training and remuneration for existing and additional community health workers.
Performance incentives and hardship allowances for all other health workers.
Additional in-workers.
service training and supervision of all
Supply management at the district level.
Rehabilitation and equipment of primary care facilities as maternities and one hospital per district to perform C-sections and provide laboratory services.
Demand side
Conditional cash transfers for all the wealth deprived.
Drugs and supplies for interventions introduced or scaled up (including additional drugs and supplies triggered by blanket abolition of user fees).
Education, communication and social mobilization.
Quality Health information systems and monitoring.
Table 6:Strategies for revitalizing the primary health care system in Lagos
48
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

health system. It is very important, as recommended in the Africa Investment Case developed by the HHA partnership, that innovative financing options be devised based on the contextual opportunities and possibilities.
The levels of financing required to implement the strategies outlined in this Investment Case are shown in Table 8. Costs were calculated using Lagos State official population estimates of approximately 20 million inhabitants. Estimates are also presented on a per capita basis from 2012 to 2020.
By progressively increasing per capita health spending from 8 USD in 2012 to 19 USD in 2020, Lagos could upgrade its health system
4.3 The estimatedinvestment required
cases (incidence) by 22%, and lowering the total number of persons living with HIV (prevalence) by 23%.
Our cost estimates are comparable to those found in Lagos State's Strategic Health
Development Plan where an additional 10 USD per year is estimated to be required until 2015. These estimates are also below those calculated by the partnership Harmonization for Health in Africa (HHA), which estimated the additional investment required in Africa to be between 21 to 36 USD per capita.
These levels of investments are in line with recommendations made by the High Level Taskforce Platform (HLTF) on Innovative International Financing for Health Systems, which estimated the levels of investment
64required to reach the health-related goals.
Nevertheless, additional funding cannot be the only financing policy for improving the
-50%
-45%
-40%
-35%
-30%
-25%
-20%
-15%
-10%
-5%
0%
2012 -2014 2015 -2017 2018 -2020
Perc
enta
ge r
eduction
U5MR reduction IMR reduction NNMR reduction
Figure 20:
Reduction in Child and Infant Mortality (2012-2020)
64High Level Task Force on International Partnership and Health. International Health Partnership, April 2009.
65Harmonization for Health in Africa, “Investing in health for Africa: The case for st rengthening systems for better hea l th outcomes,” 2011, http://www.who.int/pmnch/topics/economics/20110414_investinginhealth_africa/en/index.html.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
49

private partnerships, as well as existing donor contribution levels.
The two types of new investments detailed in Table 8 include capital investments, such as rehabilitating existing health facilities or building new ones, and recurrent costs related to human resources or to policies that remove financial barriers to access.
to a level that would match the city's vision of excellence for 2020 and guarantee that no one in Lagos State has been left behind. The additional investment would amount to an average increase of 15 USD per capita for the period 2012-2020. It is believed that the necessary fiscal space can be made available, particularly given the Lagos State Government's emphasis on creating internally generated revenue and public-
Figure 21:
Reduction in Maternal Mortality
1 in 0
1 in 20
1 in 40
1 in 60
1 in 80
1 in 100
1 in 120
-40%
-35%
-30%
-25%
-20%
-15%
-10%
-5%
0%
2012 -2014 2015 -2017 2018 -2020
Lifetim
e r
isk o
f dyin
g
Perc
enta
ge r
eduction
Lifetime risk of dying of maternal causes (right-hand side axis)MMR reduction
Reduction in Malaria, HIV/AIDS and TB2012-
2014
2015-
2017
2018-
2020
% Reduction of Malaria Mortality
14.9%
17.4% 29.2%
% Reduction in AIDS mortality
% Reduction in TB Mortality
0.0% 0.0% 6.5%
21.3% 30.4% 37.3%
% Reduction of HIV/AIDS prevalence 10.3% 12.1% 21.6%
% Reduction of malaria incidence in under fives 25.4% 30.0% 45.0%
% Reduction of HIV/AIDS Incidence 11.0% 13.0% 23.1%
Table 7
50
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

the number of Lagos State residents who
utilize the health system. Responses might
include phasing interventions, such as
targeting mid-level human resource
personnel cadres to work with the slum
population.
Since Lagos benefits from a relatively good
network of infrastructure, capital
investments are substantial in the first year
but decrease significantly over time. In
contrast, recurrent costs become more
important due to a rising need for human
resources owing to the expected increase in
Additio
nal budget
by s
erv
ice d
eliv
ery
mode
U
SD
)(in
2012 -
2014
2015 -
2017
2018 -
2020
2012
2013
2014
2015
2016
2017
2018
2019
2020
1.
Fam
ily-o
riente
d c
om
munity-
base
d s
erv
ices
Capital in
vest
ment
9,3
74,6
24
9,3
36,5
76
9,3
11,2
11
15,5
73,1
01
15,5
35,5
20
15,5
10,4
66
25,6
03,0
73
25,5
03,7
37
25,4
37,5
13
Recurr
ent
34,8
03,1
57
69,6
06,3
13
104,4
09,4
70
122,3
65,6
99
140,3
21,9
28
158,2
78,1
57
172,3
63,1
90
186,4
48,2
22
200,5
33,2
55
2.
Popula
tion
oriente
d s
chedula
ble
serv
ices
Capital in
vest
ment
12,2
49,7
25
6,9
68,0
09
3,4
46,8
64
13,5
66,9
52
7,3
16,1
51
3,1
48,9
51
17,4
38,0
42
9,6
84,5
69
4,5
15,5
87
Recurr
ent
19,7
37,9
80
39,2
74,2
20
58,6
75,9
66
64,0
81,8
34
69,2
81,9
86
74,3
44,9
94
76,6
55,5
74
78,8
02,6
88
80,8
40,8
24
3.
Indiv
idual-oriente
d c
linic
al se
rvic
es
81,8
47,7
59
78,2
72,1
77
83,3
49,5
45
87,0
50,0
48
85,7
43,9
81
85,9
79,4
14
97,2
09,9
50
93,1
27,7
41
90,4
78,5
54
Capital in
vest
ment
58,1
48,5
74
31,3
12,4
44
13,4
21,6
91
12,2
61,9
71
6,6
09,6
102,8
41,3
69
12,6
05,4
117,4
73,2
56
4,0
51,8
20
Recurr
ent
23,6
99,1
85
46,9
59,7
32
69,9
27,8
54
74,7
88,0
77
79,1
34,3
71
83,1
38,0
45
84,6
04,5
38
85,6
54,4
85
86,4
26,7
34
4.
Dis
tric
t, p
rovin
cia
l and n
ational gove
rnance a
nd
managem
ent
Capital in
vest
ment
1,3
49,0
44
684,2
39
241,0
36
1,0
16,0
48
514,0
50
179,3
84
2,8
70,9
78
1,4
50,8
97
504,1
76
Recurr
ent
14,0
21,7
53
27,9
61,5
18
41,8
46,6
26
47,1
70,2
72
52,4
65,2
15
57,7
41,0
24
65,0
52,3
52
72,3
23,9
37
79,5
69,0
27
Tota
l
Capital in
vest
ment
81,1
21,9
68
48,3
01,2
68
26,4
20,8
02
42,4
18,0
72
29,9
75,3
30
21,6
80,1
69
58,5
17,5
04
44,1
12,4
59
34,5
09,0
95
Recurr
ent
92,2
62,0
75
183,8
01,7
84
274,8
59,9
16
308,4
05,8
82
341,2
03,5
01
373,5
02,2
22
398,6
75,6
54
423,2
29,3
32
447,3
69,8
40
Additio
nal in
vest
ment
per
capita
1.
Fam
ily -
oriente
d c
om
munity -
base
d s
erv
ices
2.0
33.5
55.0
25.9
66.6
17.2
48.0
88.5
28.9
5
2.
Popula
tion -
oriente
d s
chedula
ble
serv
ices
1.4
72.0
82.7
43.3
53.2
53.2
33.8
43.5
63.3
8
3. I
ndiv
idual-o
riente
d c
linic
al se
rvic
es
3.7
6
3.5
2
3.6
8
3.7
6
3.6
4
3.5
8
3.9
73.7
53.5
8
4.
Dis
tric
t, p
rovin
cia
l and n
ational gove
rnance a
nd
managem
ent
0.7
1
1.2
9
1.8
6
2.0
8
2.2
5
2.4
1
2.7
72.9
73.1
7
Tota
l per
capita (
USD
)7.9
510
.44
13.2
915.1
515.7
516.4
718.6
718.8
019.0
9
173,3
84,0
42
232,1
03,0
52
301,2
80,7
18
350,8
23,9
54
371,1
78,8
31
395,1
82,3
91
457,1
93,1
58
467,3
41,7
91
481,8
78,9
35
15,3
70,7
97
28,6
45,7
57
42,0
87,6
61
48,1
86,3
20
52,9
79,2
65
57,9
20,4
08
67,9
23,3
31
73,7
74,8
34
80,0
73,2
03
31,9
87,7
06
46,2
42,2
29
62,1
22,8
30
77,6
48,7
86
76,5
98,1
37
77,4
93,9
45
94,0
93,6
16
88,4
87,2
56
85,3
56,4
11
44,1
77,7
80
78,9
42,8
89
113,7
20,6
81
137,9
38,8
00
155,8
57,4
48
173,7
88,6
23
197,9
66,2
63
211
,951,9
59
225,9
70,7
67
Table
8:
Additio
nal Budget
Required t
o Im
ple
ment
the S
trate
gie
s
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
51

9.1%
5.8%5.5% 5.6%
6.9%
6.0%
5.5%5.3%
5.1% 5.1% 5.2%
6.0%
8.2%
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0
50,000,000,000
100,000,000,000
150,000,000,000
200,000,000,000
250,000,000,000
300,000,000,000
350,000,000,000
400,000,000,000
450,000,000,000
500,000,000,000
550,000,000,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Perc
enta
ge
Naira
Total Health Budget (Naira) Total State Budget (Naira)
Share of State Budget (in %-right-hand size axis)
Figure 22:
Lagos State Health Budget (1999 - 2012)
Figure 23:
Additional Budget Per Capita (2012 - 2020, MBB simulations)
0
2
4
6
8
10
12
14
16
18
20
2012-2014 2015-2017 2018-2020
US$ p
er
capita
1. Family oriented community based services
2. Population oriented schedulable services
3. Individual oriented clinical services
4. District, provincial and national governance and management
52
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Figure 24:
Additional Budget (as a percentage of total additional budget, 2012-2020,MBB simulations)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2012-2014 2015-2017 2018-2020
As a
% o
f to
tal additio
nal budget
1. Family oriented community based services
2. Population oriented schedulable services
3. Individual oriented clinical services
4. District, provincial and national governance and management
Figure 25:
Additional Budget per service delivery mode
2012 2013 2014 2015 2016 2017 2018 2019 20200
100,000,000
200,000,000
300,000,000
400,000,000
500,000,000
600,000,000
US$
1. Family oriented community based services
2. Population oriented schedulable services
3. Individual oriented clinical services
4. District, provincial and national governance and management
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
53

needs of the health system, which have increased considerably due to a rise in the population, the persistent burden of old and new diseases, and increasing poverty levels documented earlier.
There is a need for the government to increase total expenditures in the health sector and to maintain the new spending level. Transparency and efficiency in the utilization of funds could also be used as a source for advocacy for increasing allocations to the health sector in line with the recommended level of 15% of total budgetary allocation (Figure 22).
Additionally, Lagos State's current budget amounts to approximately 6% of Lagos gross domestic production. This proportion of GDP is similar to that prevailing in very low-income countries such as Niger or Burkina Faso. However, if emerging countries such as Mexico, Brazil or South Africa are used as benchmarks, Lagos could afford to increase the total government budget to 10 to 12% of GDP.
These two parameters, the possibility of increasing the health budget to 15% of the total government budget instead of 6% as of 2011, and the possibility of increasing the government budget to 10-12% of Lagos GDP compared to 6% today, would provide the Lagos government with the fiscal space to make substantial progress in achieving equitable health care for its people.
4.4 Dynamics inhealth financing
Since 2008, the government of Lagos has shown its dedication to improving the health of people living in Lagos State by increasing the share of health in its total budget from an average of 5% during the majority of the 2000s to 6% in 2010 and 7% in 2011. For 2012, the share is expected to increase to
668.2% (or naira 40 billion).
This commendable increase in spending reverses the declining trend observed between 2004 and 2008. During that period, the total State budget increased by a factor of 5, from naira 77.4 billion to 403.4 billion. On the other hand, the health budget grew by factor of only 3, lowering the relative share of health expenditures in the total State budget from 6.0% to 5.1%.
By international standards, Lagos' current share of the health budget in total government expenditures are below the average for the African region (9.6%) as well as for low-income countries (8.7%) (WHO). The prospective budget allocation for 2012 at 8.2% would come closer but would still be far below the 15% Abuja declaration commitments.
Government health expenditure levels remain too low to adequately respond to the
A Mother and Child Centre (MCC).
66Governor’s speech, 24 November 2011.
54
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

those who live in the slums. This serious imbalance means that far too many children and mothersfrom the most deprived neighbourhoods are not getting the kind of care they need at critical junctures in their lives.
There is a critical shortage of health care personnel—from doctors and nurses to community health extension workers (CHEWs). Moreover, a disproportionate number of them serve at secondary and tertiary health facilities. This disparity can also be seen within local government areas (LGAs).
Many factors limit access to and use of health care services among Lagos's poorest populations, including geographical and financial barriers, socio-cultural and traditional beliefs and myths, as well as a widespread perception of poor quality of care in public facilities, often attributed to the attitudes of health personnel.
The Lagos State government is committed to reversing inequities through the removal of bottlenecks, and has mounted a number of initiatives and campaigns to ensure that a full range of public and private health services are accessible to all people in Lagos State. The Governor of Lagos State has stated his belief that Lagos can achieve the Millennium Development Goals by 2015. This is the vision upon which a hypothesis was conceptualized for testing: Is Lagos State positioned to achieve the health-related MDG targets with equity in light of the current level of investments and strategies? This question gave birth to a process geared towards building on the current momentum and political will in the state to ensure that the health-related MDGs don not lag behind the state gears up for full implementation of the Lagos State Vision for 2020.
The process began in February 2011, when the Lagos State Commissioner of Health inaugurated a team to produce Reducing Health Disparities in Lagos State: An Investment Case. A partnership between the
“The goal is that every Lagosian enjoys unfettered access to qualitative healthcare without significant geographical, financial, cultural or political barriers.”
—The Lagos State Strategic Health Development Plan 2010-2015
Each year, nearly 1 in 10 children in Lagos State dies of preventable and treatable diseases before they are five years old. Of these children, 40% die during the first 28 days of their lives. Preventable infectious diseases such as malaria, diarrhoea and pneumonia remain major child killers. Maternal mortality rates are also alarming: an estimated 555 maternal deaths per 100,000 live births. Perhaps not surprisingly, one's health depends on the neighbourhood he or she lives in. Mothers in crowded and flood-prone Alimosho, for example, are 2.7 times more likely to die in childbirth than mothers in Lagos Island.
These inequities are largely linked to bottlenecks within and around the health system. Some key bottlenecks revealed during the research are:
The rapid growth of the population from internal and external migration, and the territorial expansion of the city, have not been matched by adequate capital investment. This has led to an on-going crisis affecting Lagos' physical infrastructure. As a result, millions live in slum areas that lack basic services such as roads, drinking water, sanitation and electricity as well as a d e q u a t e h o u s i n g — s e r i o u s l y compromising their health.
Evidence-based planning and budgeting for health care services in Lagos is a major challenge because of inaccurate and incomplete population data.
Health spending has tended to favour secondary and tertiary health care services over the primary and private health care systems that cater to more than 70% of the population, especially
5. CONCLUSION: Achieving equitablehealth care in Lagos State
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
55

Morocco. The achievements would benchmark Lagos wi th emerg ing countries—and commensurate with the Lagos Vision for 2020.
The investments articulated above are crucial for scale up and expansion of existing and ongoing life-saving and cost-effective interventions. In addition, investments would be directed at where they are needed most--to families and communities, for strengthening preventive care and enhancing access to primary care. This would be done through innovative and strategic shifts in policy geared towards increasing access for the poor and enhancing quality care for all.
The policy recommendations outlined below seek to accelerate the revitalization of Lagos' primary health care system that is already underway thanks to several government initiatives. They take to heart the motto of the Lagos Ministry of Health, to “Bring care and healing closer to our citizens.”
Bring health services closer to communities
Children in Lagos die from preventable infectious diseases such as malaria, diarrhoea and pneumonia, which together account for 41% of all under-five child deaths. The majority of these deaths can be prevented through high-impact preventive and curative interventions delivered at the primary health care level. Hence, we recommend to:
Accelerate the existing momentum to revitalise Lagos' primary health care system by scaling up the government's Primary Health Care Flagship Centres project in order to improve the supply and quality of services. This process should go along with efforts to further rationalise the referral level hospitals by providing organisational and financial advantage to referred patients and discourages persons to directly use the
5.2 Key policyrecommendations
Lagos State Ministry of Health and UNICEF, it seeks to show that health care for all people of Lagos State is not just a worthy vision, but a goal that is within reach.
The Investment Case team used new research and tested methodologies to identify bottlenecks to care as well as strategies to remove those bottlenecks. The team then modelled the costs of implementing the strategies and projected their impact.
The findings were remarkable: the modelling showed that these equity-focused strategies were particularly cost-effective—they achieved more health for the money.
The Investment Case modelled the cost of implementing the recommended strategies and found that they would require an additional investment equal to an average of 15 USD per capita per year. The additional initial investment would rise progressively, from 8 USD in 2012 to 19 USD in 2020. By 2020, the proposed investment could potentially achieve the following health impacts:
Decrease under-five mortality rates by 50%.
Reduce maternal mortality by 33%.
Significantly decrease the impact of HIV/AIDS, tuberculosis and malaria.
Reverse the HIV/AIDS epidemic by decreasing the number of new cases by 22%, and lowering the total number of persons living with HIV (prevalence) by 23%.
Reduce health disparities in Lagos state by bringing the health system closer to the poorest of the poor.
These are big results. The reduction of under-five mortality would place Lagos at the level of countries such as India or South Africa, and close to a country such as
5.1 The InvestmentCase
56
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

use of public funds.
Keep the momentum and strengthen existing campaigns for Maternal New-born Child Health Weeks, National Immunization Days, Supplemental Immunization Plus Days and Local Immunization Plus Days.
Establish a State Health Insurance Scheme to provide social health protection for all categories of the population (including the formal sector, both public and private, the informal sector, rural dwellers, retirees and pensioners, the poor and vulnerable).
Reduce financial barriers to health care access (direct and indirect costs) through the elimination of user fees, and use of mechanisms such as subventions and third-party payments.
Explore the use of cash transfer programmes, which are emerging as an indispensable component of poverty reduction strategies.
Identify champions at the highest level in Lagos State to campaign for the reduction of the fertility rate and for birth spacing of children. A successful campaign in Lagos could trigger a national campaign.
Bring communities closer tohealth
The success of revitalising the primary health care system will depend on the capacity of all those living in Lagos State, including the most underserved, to take ownership of the health system and ensure that it works for them. To do this, they must be given the knowledge and skills to identify their problems (from health to water and sanitation issues), as well as the means to address them. This vital partnership between the people of Lagos and the health system can be achieved through the following endeavours.
St rengthen par tnersh ips wi th community-based enablers and promoters to ensure that the
hospital for first aid. This would reduce the number of cases that are unnecessarily referred to secondary and tertiary levels, and enhance quality and cost of care through better doctor/nurse -to-patient ratios at all facilities.
Increase the number of community health extension workers (CHEWs), who are in insufficient supply and unequally distributed across LGAs, up to the recommended level, particularly in the most under-served areas. With their unique insights into the health problems of the community, CHEWs play a vital role in revitalising Lagos' primary health-care system. In order to fulfil this role, their work conditions, responsibilities and tasks, well defined number of families covered per CHEW, along with their remuneration, supervision and training, will need to be revised.
Tackle current gaps in the continuum of care through a re-energised and pro-active outreach programme in the most under-served areas. This will require enabling CHEWs to bring family planning, antenatal care, immunization, HIV counselling and testing to households, thus raising the awareness and demand for high-impact preventive interventions at the community level.
Redress the uneven distribution of the skilled health workforce across the three tiers of the health system as well as across LGAs. Ensure that primary care facilities are adequately staffed with skilled personnel through incentives such as performance-based financing and rotational posting for doctors and nurses. Also use these strategies to enhance the performance, re tent ion and dep loyment of community health personnel.
Pilot performance-based contracts (especially for preventive interventions) with private health service providers, which play an important role in Lagos' health system. This would help increase the supply and quality of basic health services to the poor, especially in the slums, and ensure the cost-effective R
educin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
57

weaknesses of one sector do not undercut the achievements of the other. This is important regarding nutrition, water improvement, sanitation, and hygiene, and regarding child health, which requires protection from abuse, neglect and exploitation alongside health and nutrition interventions. Also, strengthen information, education and communication to ensure that key household practices are learned and utilized.
Lagos can exploit three important opportunities to accelerate its health reforms.
Continue to invest ininfrastructureimprovements
The Lagos Mega City Regional Plan offers a wide range of incentives for bridging the urban divide as it concentrates on programmes and projects of strategic significance for the redevelopment of the entire city. On-going megacity and slum upgrade projects show that the Lagos State government is taking urban planning seriously in the face of fast-growing population. It is important to build on and to sustain the momentum behind planning for health infrastructure, particularly investment in water and sanitation and dealing with unsafe housing issues. The current initiative to upgrade seven slums in Lagos (LMDG programme) should be scaled up to cover the more than 100 slums across Lagos.
Expand and continue toinnovate in the use of public-private partnerships
Lagos State Government is the only state that has a dedicated office for public-private partnerships (PPP). A large proportion of health care in the state is provided by the private sector, and this partnership could be
5.3 Windows ofopportunity
community takes health matters seriously and is empowered to demand their rights to health.
Revitalize the role of Ward Health Development Committees as a core part of the Ward Development Council's mandate.
Ensure the wards appoint community volunteers to support their role and ensure representation on public health-care centre management committees, the active promotion of health, and feedback and consultations with their ward members.
Ensure the quality ofessential health services
Despite the challenges, Lagos arguably has the best health system in Nigeria and must not just maintain, but build on this reputation by ensuring that the standards of care continue to increase. As the pacesetters of Nigeria, the quality of health-care services must be improved across the state—thus leading a new wave of high-quality health services in the nation. To do this, the state should:
Align Lagos health services with international standards (health protocols and health workforce training).
Implement e-Health, a decentralized monitoring system focused on the identified bottlenecks in order to help build the State's health management information system (HMIS), monitor progress in coverage at the LGA level and evaluate the effectiveness of interventions and strategies to improve the health of the population.
Imp lement the Urban HEART assessment tool as a way to inform policymakers and key stakeholders on local-level performance to guide the prioritization of local and national policies and strategic intervention.
Coordinate action across the health and development sectors to ensure that the
58
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Besides building on the windows of opportunity, it is paramount that all actors take the document as a live tool to be used to enhance their ownership of and participation in processes which are intended to yield results for better health outcomes in Lagos. Decisive steps should be taken at all levels. In particular, the following key steps are recommended:
1. LGA/LCDA and Community levels –
Ward Council persons and LGA Chairpersons should now look decisively at how they can start to implement the recommendations herein.
Feedback and dissemination to communities; especially those that participated in the formulation of this document.
Operational plans at the LGA/LCDA level would be essential. Further decentralization to the ward level is encouraged where Ward Operational Plans could be developed.
Formulation of agreements/compacts b e t we e n c o m m u n i t i e s a n d Government to ensure that all levels of accountability are articulated.
2. State level
Ensure adoption and implementation of all policy recommendations
Ensure a systematic review of implementation to include:
Joint annual reviews of the health system with all partners ensuring that the monitoring tool forms a critical part of the review
Joint LGA monitoring by government and partners
Review of the investment case every 3 years using the current data as the baseline. Results thereof should formulate the basis for elaboration of the next SSHDP or its extension
strengthened through possible private sector subcontracts to implement other functions of care. The aim should be to cover the most vulnerable, improving community demand and increasing utilization of existing health services. Additional efforts could leverage corporate social responsibility (CSR) funds to increase the state's internally generated revenue (IGR) and enhance information exchange and management to generate health sector evidence and improve planning.
Build on the dynamism in local communities
Several local initiatives in slum areas observed by the Investment Case team could be considered for evaluation and replication. Most notable are community-driven advocacy activities that led to provision of electricity and structured garbage collection. Slum communities should be encouraged to promote other interventions such as toilet provision for the reduction of open defecation. Given the water, sanitation and hygiene challenges in the slums, basic information, education and communication regarding key household practices should be implemented, including cost-effective interventions such as hand washing with soap. It will also be important to create a new local definition of slums in the Lagos context, and based on the identified indicators, conduct a rapid assessment to better understand the sociology and the needs for each slum area.
While the measures proposed here will benefit all those living in Lagos State, the strategy focuses on equity—providing better access to quality essential health services for those who live in Lagos's most deprived neighbourhoods. They are the ones who bear the largest burden of disease and mortality. In short, the strategy will accelerate progress toward meeting the health Millennium Development Goals through a laser-like focus on reducing health disparities.
5.4 What Next?
a.
b.
c.
d.
a.
b.
i
ii
iii
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
59

scope for raising health allocation in order to meet the Abuja target of 15% of government spending allocated to health.
The Convention on the Rights of the Child, signed by the Lagos State Government, recognizes the right to child survival and development and the right to health. We now stand before an enormous opportunity. By investing in health in a way in which everyone can benefit from the improvements, Lagos can be a frontrunner in an equitable approach to social development—and an example for Nigeria and the world. Challenges will of course be difficult. But if the appropriate means are given, and with the commitment of politicians, private sector, health providers and communities, it can be achieved. It is hoped that this Investment Case will inspire focused action across the state and serve as a key step forward in pursuit of that vision. This is Lagos!! There is a role for everyone.
In Lagos, nothing is impossible.
3. Donor partners
Ensure that the LSHDP and the Investment case are utilized as together towards realization of the goals of Lagos State. The Lagos state Health Partners Forum should equally coordinate reviews and hold all donors accountable to work within the framework of the two documents.
Suppor t be t te r coord ina t ion and commit to a move towards implementat ion of the Par is Declaration and a sector wide approach to health in Lagos
An important momentum for the health sector has been increased fund allocation to health. With the rise in state revenue generation which has grown from N7 to 30 billion per month, the state government has ensured prioritization of health. The increase in the percentage of the budget allocated to health—from 5.1 to 8.2 since 2007—is a clear demonstration of this prioritization by the Government of Lagos. Although this allocation is still below the 9.6% average for the Africa region, there appears to be ample
a.
b.
In Lagos, no one will be left behind.
60
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

(a dream on the verge of reality)
In Lagos, ANYTHING is possible!Eko Oni Baje o!
The new Eko Atlantic City
of Lagos State

1. In all actions concerning children,whether
undertaken by public or private social
welfare institutions, courts of law,
administrative authorities or legislative
bodies, the best interests of the child shall be
a primary consideration.
2. States Parties undertake to ensure the
child such protection and care as is
necessary for his or her well-being, taking
into account the rights and duties of his or
her parents, legal guardians, or other
individuals legally responsible for him or her,
and, to this end, shall take all appropriate
legislative and administrative measures.
3. States Parties shall ensure that the
institutions, services and facilities
responsible for the care or protection of
children shall conform with the standards
established by competent authorities,
particularly in the areas of safety, health, in
the number and suitability of their staff, as
well as competent supervision.
Article 23
1. States Parties recognize that a mentally or
physically disabled child should enjoy a full
and decent life, in conditions which ensure
dignity, promote self-reliance and facilitate
the child's active participation in the
community.
2. States Parties recognize the right of the
disabled child to special care and shall
Appendices
encourage and ensure the extension, subject
to available resources, to the eligible child
and those responsible for his or her care, of
assistance for which application is made and
which is appropriate to the child's condition
and to the circumstances of the parents or
others caring for the child.
3. Recognizing the special needs of a
disabled child, assistance extended in
accordance with paragraph 2 of the present
article shall be provided free of charge,
whenever possible, taking into account the
financial resources of the parents or others
caring for the child, and shall be designed to
ensure that the disabled child has effective
access to and receives education, training,
health care services, rehabilitation services,
preparation for employment and recreation
opportunities in a manner conducive to the
child's achieving the fullest possible social
integration and individual development,
including his or her cultural and spiritual
development
4. States Parties shall promote, in the spirit
of international cooperation, the exchange of
appropriate information in the field of
preventive health care and of medical,
psychological and functional treatment of
disabled children, including dissemination of
and access to information concerning
methods of rehabilitation, education and
vocational services, with the aim of enabling
States Parties to improve their capabilities
and skills and to widen their experience in
these areas. In this regard, particular
account shall be taken of the needs of
developing countries.
Appendix A. Convention of the Rights of
the Child (1989)
Article 3
62
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Appendix
B. M
ate
rnal m
ort
alit
y r
ate
s, d
iarr
hoea incid
ence,
access
to v
accin
ation a
nd w
ate
r and s
anitation,
by local govern
ment
are
a (LG
A), 2
010
Sourc
e: La
gos
Min
istr
y o
f H
ealth 2
010 R
eport
MM
RD
iarr
hoea
BC
GPolio
Full
imm
unization
cove
rage
House
hold
s w
ith
impro
ved s
ourc
e o
f drinkin
g w
ate
r
House
hold
s w
ith
impro
ved
sa
nitary
fa
cili
ties
(not
share
d)
A
limosh
o
826
Ib
eju
-Lekki
29%
Ibeju
-Lekki
10
0%
A
gege
78%
A
papa
43%
Ib
eju
-Lekki
65%
Ib
eju
-Lekki
58%
Epe
803
Badagry
24%
Badagry
92%
A
jero
mi-
Ifelo
dun
75%
La
gos
Main
land
47%
La
gos
Isla
nd
74%
Badagry
61%
Ib
eju
-Lekki
758
A
gege
23%
Ikeja
86%
A
limosh
o
78%
M
ush
in
51%
A
muw
o-O
dofin
75%
A
papa
64%
Ik
oro
du
754
Koso
fe
20%
Koso
fe
85%
A
muw
o-O
dofin
75%
Ib
eju
-Lekki
55%
Suru
lere
77%
Epe
67%
A
jero
mi-
Ifelo
dun
736
Ik
eja
18%
Epe
85%
A
papa
77%
Epe
56%
Koso
fe
78%
O
jo
68%
Eti-O
sa
725
M
ush
in
16%
Suru
lere
84%
Badagry
92%
A
jero
mi-I
felo
dun
59%
Ifako
-Ija
iye
80%
Lagos
Main
land
69%
Ifako
-Ija
iye
690
Suru
lere
16%
Ikoro
du
84%
Epe
88%
La
gos
Isla
nd
59%
O
jo
81%
Ifako
-Ija
iye
71%
A
gege
667
Epe
15%
Mush
in
81%
Eti-O
sa
67%
Koso
fe
60%
Som
olu
82%
Ik
oro
du
71%
O
jo
667
Som
olu
14%
Som
olu
81%
Ibeju
-Lekki
83%
Eti-O
sa
63%
Aje
rom
i-Ifelo
dun
83%
Agege
76%
Som
olu
667
Lagos
Main
land
13%
Lagos
Main
land
80%
Ifako
-Ija
iye
64%
Som
olu
70%
Eti-O
sa
83%
Alim
osh
o
76%
Badagry
600
Aje
rom
i-Ifelo
dun
12%
Agege
78%
Ikeja
84%
Am
uw
o-O
dofin
71%
Lagos
Main
land
84%
Osh
odi-Iso
lo
77%
A
muw
o-O
dofin
555
Ifako
-Ija
iye
12%
Alim
osh
o
78%
Ikoro
du
80%
Ojo
72%
Agege
87%
Ikeja
78%
M
ush
in
511
Ikoro
du
11%
Ojo
77%
Koso
fe
90%
Ikoro
du
74%
Osh
odi-Iso
lo
87%
Koso
fe
81%
La
gos
Main
land
443
Ojo
11%
Aje
rom
i-Ifelo
dun
76%
Lagos
Isla
nd
72%
Ifako
-Ija
iye
76%
Alim
osh
o
89%
Mush
in
82%
O
shodi-Iso
lo
443
Alim
osh
o
10%
Lagos
Isla
nd
76%
Lagos
Main
land
81%
Alim
osh
o
76%
Mush
in
90%
Som
olu
85%
A
papa
421
Am
uw
o-O
dofin
9%
Osh
odi-Iso
lo
75%
Mush
in
83%
Osh
odi-Iso
lo
76%
Badagry
91%
Aje
rom
i-Ifelo
dun
85%
Koso
fe
421
Apapa
8%
Eti-O
sa
71%
Ojo
80%
Badagry
77%
Apapa
91%
Eti-O
sa
88%
Ik
eja
354
Eti-O
sa
7%
Apapa
70%
Osh
odi-Iso
lo
75%
Suru
lere
77%
Ikeja
92%
Lagos
Isla
nd
89%
Suru
lere
322
Osh
odi-Iso
lo
7%
Ifako
-Ija
iye
64%
Som
olu
79%
Agege
79%
Ikoro
du
92%
Am
uw
o-O
dofin
89%
La
gos
Isla
nd
310
Lagos
Isla
nd
7%
Am
uw
o-O
dofin
62%
Suru
lere
87%
Ikeja
98%
Epe
95%
Suru
lere
92%
Ave
rage
555
Ave
rage
13%
Ave
rage
78%
Ave
rage
79%
Ave
rage
78%
Ave
rage
84%
Ave
rage
78%
Sm
alle
st
310
Sm
alle
st
7%
Sm
alle
st
62%
Sm
alle
st
64%
Sm
alle
st
43%
Sm
alle
st
65%
Sm
alle
st
58%
Larg
est
826
Larg
est
29%
Larg
est
10
0%
Larg
est
92%
Larg
est
98%
Larg
est
95%
Larg
est
92%
Media
n634
Media
n13%
Media
n79%
Media
n80%
Media
n71%
Media
n84%
Media
n77%
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
63

Basic public services
Water Improved sources of drinking water (pop) 67.7
Sanitation Improved sanitation, not shared facility (pop) 25.3
Electricity Access toElectricity
Appendix C: Summary of key indicators for Lagos. Nigeria Demographic and Health Survey (2008)
91.4
Birth registration
52.8
Exposure to mass media (women)
Reads a newspaper at least once a week 28.7
Watches television at least once a week 86.1
Listens to radio at least once a week 77.6
All three media at least once a week 26.2
Sexual & Reproductive Health
Fertility
5.7
Median age at firth birth
24.3
Teenage pregnancy (15-19)
5.3
Knowledge of modern contraceptive method
Women
97.9
Men
99
Current use of contraceptive
27.5
Antenatal care
Skilled
87.6
TBA
8
Place of delivery
Public
20.5
private
56.4
home
9.1
Type of birth delivery
Skilled birth delivery
82.8
Delivered by C section
5.2
BMI women
normal 55
overweight 26.3
obese 12.4
Timing of first postnatal check-up
Less than 4 hours
66
4-23 hours
8.5
2 days
5.1
3-41 days
7.9
No check up
9.5
Child Health
Vaccination
BCG
84.6
DPT1
86.1
DPT2
83.2
DPT3
73.6
Polio0
75.1
Polio1
83.1
Polio2
77.2
Polio3
60.9
Measles
69.2
All basic vaccination
52.8
Prevalence of Fever
U5 with fever past 2 weeks
7.4
Treatment for fever
Percentage for whom advice or treatment was sought from a health facility or provider
57.7
Percentage who took anti-malarial drugs 57.8
Percentage who took antibiotic drugs 30.8
U5 with fever who took anti-malarial drug 57.8
U5 with fever who took anti -malarial drug same of next day 19.3
Diarrhea
Prevalence of U5 in past 2 weeks with diarrhea 6.1
Percentage of women who know about ORS packets or ORS pre-packaged liquids
83.2
Safe disposal of children's stools
70.9
Nutrition
Percentage given vitamin A supplements in past 6 months 51.2
Percentage given iron supplements in past 7 days 55.9
Percentage given deworming medication in past 6 months 62.1
Stunting 2SD
21
Wasting 9.8
Underweight 10.1
Initial BF ownership 9.3
ITN children sleeping under ITN 6.5
Health Care Seeking
Problems accessing health care
Getting permission to go for treatment 2.1
Getting money for treatment 39.7
Distance to health facility 23.7
Having to take transport 19.7
Not wanting to go alone 9.1
Concerned no female provider available 13.5
Concerned no provider available 18.9
Concerned no drugs available 24.3
At least one problem accessing health care 43.1
HIV-AIDS % women with comprehensive knowledge HIV 26.9
% women with comprehensive knowledge of MTCT 45.2
64
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Appendix D. Bottleneck Analysis, summary of findings by the Public Health Expert Group
Bottlenecks
A Family -Oriented Community -Based Services
1 Community health extension workers (CHEWs) not available in the community.
2Perceived opportunity cost: mother had other things to do, lack of awareness about expressing milk means
hinders exclusive breast feeding (EBF).
3 Political influence around long -lasting insecticide -treated nets (LLINs).
4 Socio-cultural, religious, taboos and beliefs; resistance to EBF and to complementary feeding.
5
Social mobilization is not disseminating enough information or creating enough demand. There are gaps
between State and local government areas (LGAs), and between LGAs and wards regarding transparency
and tracking of funds.
B Population -Oriented (Outreach) Immunization, Family Planning, Antenatal Care (Preventive)
1Gender and social imbalance in health decisionmaking (women may need permission or help making
health a priority).
2Inadequate number of facilities and care providers (i.e. inadequate trained staff). Access to ARV during
delivery to PMTCT. Inadequate geographical a ccess to PMTCT.
3Poor demand creation and community empowerment through social mobilization and community
awareness.
4
Lack of outreach services means preventive services are facility based. No outreach linking services to slum
areas (comprehensive pack ages taken to grassroots as outreach, e.g. FP, immunization).
C Facility -Based Clinical Care
1Inappropriate distribution of human resources (i.e. career elevation favours secondary and tertiary rather
than primary health care).
2 Informal user fees collected by facilities render care inaccessible to the poor.
3 Financial accessibility: clients not able to afford to pay for private and public services.
4Perceived quality of care (attitude of community health workers, preference for patronizing secondary
facilities).
5 Weak policy mechanisms to standardise and enforce health policy in private sector.
6 Perception of an unfriendly environment (physical access to services).
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
65

Appendix E. Community Participation in
Bottleneck Analysis in Health Care Service
Delivery in Lagos State
In order to benefit from direct community
input in the Bottleneck Analysis, the
Investment Case team held a one-day
meeting at the Airport Hotel, Ikeja on
Tuesday, 5 July 2011. It was attended by 30
community members from the Lagos State
local government areas (LGAs) of Ikorodu,
Badagry and Eti-Osa.
The three teams of ten included traditional
rulers, religious leaders (Muslim and
Christians), Chairmen of Community
Development Committees, opinion leaders,
representatives of market women,
caregivers, women and youth leaders. Also
present were the LGA medical officers of
health, LGA health educators, antenatal care
(ANC) midwives and officials from the State
Ministry of Health, including the Primary
Healthcare Centre Board. The UNICEF team
included the team leader, the consultant to
the Investment Case, three specialists on
water and sanitation (WASH), health and
C4D and programmes assistant.
The meet ing commenced with a
presentation by an M&E officer from Lagos
State Ministry of Health on the coverage
levels of three interventions: ITN use, routine
i m m u n i z a t i o n a n d V i t a m i n A
supp lementa t i on . She made the
presentation in Yoruba language. This was
followed by a presentation by UNICEF on
community participation in the Bottleneck
Analysis.
The presentation, which was delivered both
in English and Yoruba languages, included
explanations of the Bottleneck Analysis
methodology, the three service delivery
modes and health financing options. Special
emphasis was on community health
insurance scheme and analysis of user fees,
which generated much interest from
participants.
Next the Investment Case team shared the
template for group work, and the
participants from each of the three LGAs
constituted teams according to the three
health service delivery modes: (i) family-
oriented community-based services, (ii)
population-oriented schedulable services,
and (iii) individual-oriented clinical services.
The following table summarizes the findings
of these three groups.
66
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

1
Use o
f In
secticid
e t
reate
d
“Bed-
nets
”
? ?
S/N
INTERV
EN
TIO
NS
BO
TTLEN
EC
KS
PO
SSIB
LE C
AU
SES
PRO
PO
SED
OPERATIO
NA
L S
TRATEG
IES /
SO
LUTIO
NS
Inadequate
supply
of
ITN
Non rele
ase/d
istr
ibution
?
Refu
sal to
use
?
Govern
ments
not
com
mitte
d
?
Belie
fs:
o
Heat
o
Makes room
s look u
ntidy
o
Psy
cholo
gic
al re
ason (ly
ing in-sta
te f
or
dead b
odie
s)
?
Many c
laim
they react
to t
he c
hem
ical
?
Aggre
ssiv
e aw
are
ness c
am
paig
ns
?
Health E
ducation
?
Advocacy t
o g
overn
ments
2H
and-
washin
g w
ith s
oap
and w
ate
r
?
Unavaila
bili
ty o
f w
ate
r
?
Cost
of
com
moditie
s
?
Ignora
nce a
bout
the im
port
ance o
f w
ashin
g h
ands
?
Povert
y
?
Behavio
ura
l A
ttitude
?
Ineff
icie
nt
Sta
te W
ate
r C
orp
ora
tion
?
Com
munity a
ware
ness,
tra
inin
g a
nd
physic
al dem
onstr
ation
?
Behavio
ura
l C
hange m
ate
rials
?
Inclu
sio
n o
f hand-w
ashin
g in s
chool
child
ren c
urr
iculu
m
?
Pro
vis
ion o
f port
able
wate
r by t
he
govern
ments
3O
ral Rehydra
tion T
hera
py
?
Lack o
f know
ledge
?
Unple
asant
taste
of t
he
wate
r
?
Cost
of
sugar
and s
alt
?
Ignora
nce
?
Lazi
ness o
n t
he p
art
of
care
giv
ers
?
Povert
y
?
Lack o
f port
able
wate
r
?
Continuous h
ealth e
ducation
pro
gra
mm
es
?
Inte
nsiv
e a
ware
ness c
reation o
n O
RS
?
ORS c
orn
ers
in H
Fs
4Exclu
siv
e B
reast
Feedin
g
?
Ignora
nce
?
Poor la
cta
tion m
anagem
ent
?
Lack o
f aw
are
ness
?
Harm
ful Tr
aditio
nal belie
f
?
Ineff
ective A
NC
?
If m
oth
er
is ill
or
dead
?
Mul
tiple
birth
s
?
Cosm
etic reasons
?
Civ
il serv
ant
/ corp
ora
te m
oth
ers
(i)
Deliv
ery
Mode: Fam
ily-O
riente
d C
om
munity B
ased S
erv
ices
?
Moth
ers
death
? ? ? ?
Inte
nsifie
d h
ealth e
ducation
Altern
ative m
edic
ine
Good a
nte
nata
l care
/ n
utr
itio
n
Surr
ogate
moth
er
Appendix
E. C
ON
TIN
UED
Com
munity P
art
icip
ation in B
ott
leneck A
naly
sis
in H
ealth C
are
Serv
ice D
eliv
ery
in L
agos
Sta
te
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
67

Appendix
E.
CO
NTIN
UED
Com
munity P
art
icip
ation in B
ott
leneck A
naly
sis
in H
ealth C
are
Serv
ice D
eliv
ery
in L
agos
Sta
te
(ii) D
eliv
ery
Mode:
Popula
tion
-Oriente
d S
chedula
ble
Serv
ices
S/N
IN
TERV
EN
TIO
N
BO
TTLEN
EC
KS
PO
SSIB
LE C
AU
SES
PRO
PO
SED
OPERATIO
NA
L S
TRATEG
IES /
SO
LUTIO
NS
1
Imm
uniz
ation
?
Poor
access
to h
ealth
facili
ties.
?
Hum
an reso
urc
e s
hort
age
?
Short
age o
f C
om
moditie
s
?
Unatt
ractive
infr
ast
ructu
res
?
Poor
roads
netw
ork
?
Lack o
f lo
gis
tics
?
Inadequate
qualif
ied s
taff
?
Lack o
f lo
gis
tic s
upport
fro
m t
he L
GA
, e.
g g
enera
tor
the
keep v
accin
es
pote
nt
?
Lack o
f in
centive
s to
com
munity m
obili
zers
? Eff
ective
monitoring
? A
dequate
serv
ices
? Separa
tion o
f child
welfare
fro
m
tuberc
ulo
sis
clin
ic
?
Gove
rnm
ent
to e
mplo
y m
ore
qualif
ied
staff
s.
2
Fam
ily P
lannin
g
?
Belie
f of
the p
eople
?
Taboos
?
Public
enlig
hte
nm
ent
? Pro
vis
ion o
f enough m
ate
rial
3
Ante
nata
l C
are
(A
NC
)
?
Short
age o
f m
idw
ives
?
Poor
access
to H
Fs
?
In
adequate
skill
ed s
taff
(m
idw
ives)
?
Pove
rty le
vel of
the p
eople
?
Dem
otiva
ted s
taff
s
?
Lack o
f com
munity s
upport
?
Insu
ffic
ient
train
ing a
nd retr
ain
ing o
f th
e s
taff
? G
ovt
to e
nsu
re c
onduciv
e w
ork
ing
environm
ent
? C
onsi
dera
tion o
f pro
xim
ity t
o H
Fs
when
post
ing s
taff
s.
? Em
plo
ym
ent
of
more
docto
rs
? In
tensi
fy Public
Enlig
hte
nm
ent
? C
om
munity s
upport
? C
om
munity a
ccepta
nce
? Fo
rmation o
f w
ard
lev
el com
mitte
e
4
HIV
Pre
vention a
nd C
are
(PM
TCT)
?
Pove
rty L
evel
?
Socia
l att
achm
ent
?
D
iscoura
gem
ent
due t
o lack o
f dru
gs
and o
ther
fam
ily
pla
nnin
g c
om
moditie
s
?
Stigm
atiza
tion
?
Lack of
support
fro
m rela
tions
?
Lack o
f heart
to h
eart
centr
e (priva
cy)
68
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Appendix
E.
CO
NTIN
UED
Com
munity P
art
icip
ation in B
ott
leneck A
naly
sis
in H
ealth C
are
Serv
ice D
eliv
ery
in L
agos
Sta
te
(iii)
Deliv
ery
Mode:
Indiv
idual O
riente
d C
linic
al Serv
ices
S/N
IN
TERV
EN
TIO
N
BO
TTLESN
EC
KS
PO
SSIB
LE C
AU
SES
PRO
PO
SED
OPERATIO
NA
L
STRATEG
IES/S
OLU
TIO
NS
1
Illness
Tre
atm
ent
? La
ck o
f qualit
y h
ealth
serv
ices
? Non p
atr
onage
? ? ? ? ? ? ? ?
Inadequate
medic
al equip
ment
Nonchala
nt
att
itude o
f th
e h
ealth w
ork
ers
, N
urs
es
&
Docto
rs
Nom
inatio
n o
f non t
echnic
al pers
on a
s a h
ealth c
hairm
an
to m
onitor
the a
ffairs
of
health w
ork
ers
In a
dequate
man p
ow
er
La
ck o
f in
centive
s at
the h
ealth c
entr
es
Short
age o
f dru
gs
Dela
ys
Inappro
priate
em
plo
ym
ent
of
health s
taff
by p
olit
icia
ns
Pro
vis
ion o
f m
edic
al equi
pm
ent
Orienta
tion a
nd d
iscip
line o
f st
aff
s
Em
pow
erm
ent
of
local and w
ard
s health a
uth
ority
Superv
isio
n f
or
health s
hould
be w
ith
technic
al know
ledge
Em
plo
ym
ent
of
more
appro
priate
sta
ff
Const
ant
and regula
r m
onitoring
Regula
r pro
vis
ion o
f dru
gs
Gove
rnm
ent
sh
ould
em
bra
ced D
RF
Orienta
tion a
nd h
ealth e
ducation o
n
dru
g u
sage f
or
the c
om
munity m
em
bers
Regula
r m
onitoring o
f TBA
s by t
he
TBA
s board
, TBA
s sh
ould
work
in
conju
nction w
ith h
ealth w
ork
ers
.
2
Skill
ed A
ttendants
at
birth
? La
ck o
f needed s
taff
s
? Short
age o
f sk
illed h
ealth p
rovid
ers
?
Dela
yed r
efe
rral at
all
circle
?
Dis
tance o
f th
e c
om
munity t
o t
he h
ealth c
entr
es
?
Com
munity d
ialo
gue
Em
plo
ym
ent
of
skill
ed h
ealth p
rovid
ers
Pro
vis
ion o
f m
edic
al equip
ment
and
supply
of
dru
gs
to h
ealth c
entr
es
Advo
cacy
to t
he c
om
muni
ty,
com
munity h
eads
and relig
ious
leaders
Sta
ff t
o b
e a
t th
eir d
uty
post
at
the
appro
priate
tim
e.
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
?
? ? ? ?? ? ? ? ? ?
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
69

Appendix
F. Exis
ting Initia
tives
Addre
ssin
g Identified B
ott
lenecks
SN
Bott
lenecks
Exis
ting Initia
tives
Refe
rences
AFa
mily
Oriente
d C
om
munity –
Base
d S
erv
ices
1C
HEW
S n
ot
availa
ble
in t
he
com
munity
PH
C B
oard
eff
ort
to r
eord
er
CH
EW
’s role
s and resp
onsi
bili
ties
to c
onduct
outr
each
activitie
s and a
ct
as
link b
etw
een t
he
facili
ties
and t
he c
om
munitie
s.
2O
pport
unity c
ost
–
moth
er
had o
ther
thin
gs
to d
o,
they a
re n
ot
aware
of
expre
ssin
g m
ilk s
o t
hey d
on’t
do
Exclu
sive B
reast
Feedin
g (
EBF)
?
Cele
bra
tion o
f annual bre
ast
feedin
g w
eek
by t
he s
tate
to c
reate
aw
are
ness
of
EBF
since 1
990
?
Govern
ment
pro
nouncem
ent
on c
reation
of
baby -fr
iendly
centr
es
at
the w
ork
pla
ce
to e
ncoura
ge m
oth
ers
pra
cticin
g E
BF
3Polit
ical in
fluence a
bout
LLIN
s lin
k
the L
LIN
dis
trib
ution t
o p
olit
ical
cam
paig
ns
events
Impro
ved logis
tics
pla
n e
nfo
rcin
g
dis
trib
ution t
hro
ugh r
outine n
etw
ork
channels
to c
urb
excess
es
of
polit
icia
ns
abuse
of
LLIN
s dis
trib
ution in t
heir L
GA
s and
com
munitie
s
4Socio-c
ultura
l, relig
ious,
taboos
and
belie
fs;
they r
esi
st t
hin
g lik
e E
BF (
we
to intr
oduce c
om
ple
menta
ry f
eedin
g)
moth
er–
in-law
s vie
ws
bein
g s
trong
and a
rchaic
.
?
Health P
rom
otion C
am
paig
ns
in
com
munitie
s ta
rgeting s
ele
cte
d
com
munity m
em
bers
(t
raditio
nal/re
ligio
us
leaders
; m
oth
ers-
in-law
; husb
ands,
etc
) –
Str
ength
enin
g
Health P
rom
otion/E
ducation U
nit a
t all
levels
?
Reactivation o
f School H
ealth C
lubs
to
dis
sem
inate
info
rmation t
o f
am
ilies
on
health rela
ted iss
ues
esp
ecia
lly o
n m
yth
s and t
aboos.
5
Socia
l m
obili
zation n
ot
dis
sem
inating
enough info
rmation a
nd n
ot
enough
dem
and c
reation.
There
are
gaps
betw
een S
tate
and L
GA
s, L
GA
s and
Ward
s re
gard
ing t
ransp
are
ncy a
nd
trackin
g o
f fu
nds.
Incre
ase
d m
edia
covera
ge c
om
bin
ed w
ith
eff
ort
s of
com
munity s
ocia
l m
obili
zation
agents
.
Fro
m C
HEW
s st
andin
g
ord
er/
Job D
esc
ription a
s conta
ined in t
he S
erv
ice
Schem
e
?
Innocenti D
ecla
ration o
f 1990 o
rigin
ate
d b
y W
orld
Alli
ance f
or
Bre
ast
Fe
edin
g A
ction
?
Baby F
riendly
Hosp
ital
initia
tive g
uid
elin
e
Roll
back M
ala
rial in
Lagos
Sta
te SSH
DP
Launched in J
une 2
011
MoH
str
ate
gy d
ocum
ent
in
pro
gre
ss
? ? ? ? ? ? ? ? ? ? ? ? ? ?
70
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

SN
Bott
lenecks
Exis
ting Initia
tives
Refe
rences
B
Popula
tion O
riente
d
(Outr
each)
Imm
uniz
ation,
FP,
AN
C (
Pre
ventive)
1
Gender
and s
ocia
l im
bala
nce in h
ealth
decis
ion
-
makin
g (
i.e.
wom
en h
avin
g
perm
issi
on,
how
to p
rioritize
health
activitie
s over
oth
er
activitie
s
Pass
age &
sig
nin
g into
law
Lagos
Specia
l
People
Law
2011
All
em
plo
yers
of
labour
hav
ing s
taff
str
ength
of
100 p
ers
ons
shall
hav
e a
t
least
10 p
er
cent
of
such
staff
consi
stin
g o
f
qualif
ied a
nd c
om
pete
nt
pers
ons
with d
isabili
ty
(section 2
9(5
)).
2 In
adequate
num
ber
of
facili
ties
and
care
pro
vid
ers
(i.e.
inadequate
train
ed s
taff
) A
ccess
to A
RV
during
deliv
ery
to P
MTCT.
Inadequate
geogra
phic
al access
to P
MTCT
Serv
ice A
vaila
bili
ty M
appin
g t
o identify
deficie
ncie
s fo
r bett
er
pro
gra
mm
ing
SA
M R
eport
; M
aps
and
Directo
ry
3 Poor
dem
and c
reation &
com
munity
em
pow
erm
ent
thr
ough s
ocia
l
mobili
zation a
nd c
om
munity
aware
ness
Health P
rom
otion C
am
paig
ns
in
com
munitie
s ta
rgeting s
ele
cte
d c
om
munity
mem
bers
(tr
aditio
nal/re
ligio
us
leaders
;
moth
ers
-in
-law
; husb
ands
etc
) –
Str
ength
enin
g H
ealth P
rom
otion/E
ducation
Unit a
t all
levels
SSH
DP
4 La
ck o
f outr
each s
erv
ices
hence
pre
ventive s
erv
ices
are
facili
ty b
ase
d,
no o
utr
each lin
kin
g s
erv
ices
to s
lum
are
as
(com
pre
hensi
ve p
acka
ges
take
n
to g
rass
roots
as
outr
eaches
e.g.
FP,
Imm
uniz
ation e
tc).
PH
C B
oard
eff
ort
to r
eord
er
CH
EW
’s role
s
and resp
onsi
bili
ties
to c
onduct
outr
each
activitie
s and a
ct
as
link b
etw
een t
he
facili
ties
and t
he c
om
munitie
s.
Reorienta
tion o
f C
HEW
s on t
heir role
s
and r
esp
onsi
bili
ties
usi
ng t
he C
HEW
s
Sta
ndin
g O
rder
Fro
m C
HEW
s st
andin
g
ord
er/
job d
esc
ription
?
?
?
?
?
?
?
?
?
?
?
?
?
?
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
71

SN
Bott
lenec
ks
Exis
ting Initia
tive
s
Ref
eren
ces
C
Faci
lity-B
ased
Clin
ical
car
e
1
Inap
pro
priat
e dis
trib
ution o
f H
um
an res
ourc
es (
i.e.
car
eer
elev
atio
n f
avouring s
econdar
y
and T
ertiar
y rat
her
than
prim
ary
hea
lth c
are
Dev
elopm
ent
of
HRH
Polic
y t
o
addre
ss r
edis
trib
ution a
nd ince
ntive
s
Hea
lth S
ecto
r W
ork
load
Anal
ysis
for
redep
loym
ent
of
Hea
lth w
ork
forc
e
Dra
ft H
RH
Polic
y D
ocu
men
t O
ctober
2011
Dra
ft W
ork
load
Anal
ysis
Rep
ort
– N
ov 2
011
2
Ava
ilabili
ty o
f co
mm
oditie
s but
not
acce
ssib
le t
o t
he
peo
ple
(info
rmal
use
r fe
es c
olle
cted
by
faci
litie
s, t
he
poore
st b
een
affe
cted
)
Pass
age
& s
ignin
g into
law
Lag
os
Spec
ial Pe
ople
Law
2011
Cap
acity b
uild
ing o
n D
RF w
ith p
lan
to s
upply
of
See
d s
tock
to 6
LG
As
in
Feb 2
012
Str
ength
enin
g C
LMS t
hro
ugh t
he
new
ly inau
gura
ted S
DSS c
om
mitte
e in
August
2011
.
Pers
on w
ith d
isab
ility
sh
all be
entitled
to f
ree
med
ical
and h
ealth c
are
in
all La
gos
Sta
te h
ealth
inst
itutions
(sec
tion
27(2
)).
Quan
tifica
tion c
om
ple
ted
for
all public
fac
ilities
6
LGA
s an
d d
rug
pro
cure
men
t on g
oin
g
3
Fin
anci
al a
cces
sibili
ty t
o s
ervic
es
clie
nts
not
able
to a
fford
to p
ay
for
priva
te a
nd p
ublic
ser
vic
es
Ikosi
Com
munity B
ased
Hea
lth
Insu
rance
sch
eme
pilo
ted in 2
008
and s
cale
d u
p t
o t
wo
com
munitie
s (Iber
ekodo a
nd A
woya
ya)
in 2
011
Pro
-Poor
Priva
te H
ealth Insu
rance
–Pa
rtner
ship
Initia
tive
bet
wee
n H
MO
s an
d M
FIs
com
men
ced in M
ay 2
011
st
arting w
ith D
eman
d A
sses
smen
t an
d W
illin
gnes
s to
pay
surv
ey w
ith
MFIs
and A
ctuar
ial Stu
die
s w
ith
HM
Os
Act
uar
ial Stu
die
s co
nduct
ed M
arch
2010
an
d R
evie
w o
f Ik
osi
-Ish
eri
CBH
IS in J
une
2011
Str
ateg
ic D
ocu
men
t of
the
PPH
I In
itia
tive
- W
ork
in
pro
gre
ss
72
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

Bott
lenecks
Exis
ting Initia
tives
Refe
rences
Facili
ty B
ase
d C
linic
al care
(continued)
Perc
eiv
ed q
ualit
y o
f care
(att
itude o
f health w
ork
ers
, pre
fere
nce f
or
patr
oniz
ing s
econdary
facili
ties)
Inst
itutionaliz
ation o
f In
tegra
ted
Support
ive S
uperv
isio
n (
ISS)
at
all
levels
in
itia
ted in O
cto
ber
2011
Rev
italiz
ation o
f PH
C s
erv
ices
–
upgra
din
g o
f PH
Cs
to p
rovid
e M
inim
um
Serv
ice P
acka
ge in lin
e w
ith t
he H
ealth
Secto
r Refo
rm L
aw o
f 2006 t
hat
led t
o:
Inaugura
tion o
f PH
C B
oard
in F
eb
2009
Const
itution a
nd Inaugura
tion o
f Lo
cal G
overn
ment
Health A
uth
orities
in 5
7 L
GA
/LC
DA
s in
A
ugust
2010
o o o
Inaugura
tion o
f W
ard
Health
Com
mitte
es
for
managem
ent
of
PH
Cs
at
facili
ty lev
el com
menced in J
an
2011
and is
ongoin
g
Incre
ase
d c
om
munity p
art
icip
ation in
Health a
t com
munity/f
acili
ty lev
el th
rough
WH
Cs
and o
ther
com
munity s
take
hold
er
gro
ups
Report
of
meetings
Dev
elo
pm
ent
of
ISS t
ools
Health S
ecto
r Refo
rm L
aw
Dra
ft C
om
munity
part
icip
ation in H
ealth
Str
ate
gy D
ocum
ent
in N
ov
2010
Weak p
olic
y f
ram
ework
/ m
echanis
m
to s
tandard
ized a
nd e
nfo
rce h
ealth
polic
y t
o p
rivate
secto
r
Est
ablis
hm
ent
of
Health F
acili
ty M
onitoring
and A
ccre
ditation A
gency (
HEFA
MA
A)
with
mandate
to r
egula
te t
he s
erv
ices
of
both
public
and p
rivate
serv
ice p
rovid
ers
in t
he
Sta
te
Perc
eption o
n f
riendly
environm
ent
(Physi
cal access
to s
erv
ices)
Pass
age &
sig
nin
g into
law
Lagos
Specia
l People
Law
2011
Renovation/F
ace lifting o
f health f
acili
ties
A
port
ion o
f ev
ery
park
ing
lot
shall
be m
ark
ed
and
rese
rved f
or
pers
ons
with
dis
abili
ties
(section 2
0(1
)).
A
s fr
om
2016,
all
public
build
ings
in L
agos
shall
be
access
ible
to p
ers
ons
with
dis
abili
ty (
section 2
5 (
5))
.
? ?
–
SN
C
4
5
6
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
73

Appendix G. Summary of the field visit to
two slums (Aganyi and Canal Boundary)
using the Transect Walk approach (Nov 30,
2011).
Geography:Awodi Ora comprises 52
settlements with a population of 38,669,
which makes it the largest ward in the local
government area (LGA). The slums Aganyi
estate and Canal Boundary are bordered in
the north by Amuwo Odofin, Achapo to the
south, Akere to the west and Owoyemi to
the east. Aganyi Estate is under the
responsibility of Ajeromi LGA while Canal
Boundary is under Ifelodun LCDA.
The slums are located on opposite sides of
the canal and are constructed on swampy
land which was originally used by the
government for refuse disposal. About 20
years ago, the purported landowner sold
plots of land to individuals who gathered
garbage to fill the land and erected
wooden/plank houses. They now rent the
houses at a monthly rate of about N1200.
The communities have access to one of the
24 primary schools in Ifelodun LCDA but the
secondary school is located too far away (a
more than 30-minute walk). The
environment and housing conditions are
deplorable and contribute to illnesses and
diseases in the communities.
Urban planning: There is no baseline or
census information on how many
inhabitants reside in the slums, which
renders urban planning extremely difficult.
The unplanned nature of the settlements
means that the population does not have
access to bas ic phys ica l pub l ic
infrastructure: no drainage facilities, no
public waste disposal or public garbage
collection services, no public water pipes, no
access to asphalted road, and no public
toilets. Streets are therefore filled with
garbage and lined with extremely poor and
crowded housing. The housing conditions
are extremely poor: dirty, unsafe and
unstable buildings. Potable water needs to
be bought from private vendors at a cost of
N20 per bucket.People are literally seen to
be fighting for space just to exist! Some are
cohabiting with pigs and other animals and
reptiles.
Epidemiology:The community members we
met described the health situation as very
poor. The main illnesses in the slums are
fever (malaria) and diarrhoeal diseases
(including cholera) as well as recent
incidences of measles. During the rainy
season, the slums are affected by severe
floods, which worsen diarrhoeal illnesses.
Health facilities within the slum areas: No
primary health care centre (therefore, it is
difficult to obtain referral to go to secondary
health facilities), one or more private clinics,
five TBAs, four chemists. The general
hospital and the MCC are nearby, adjacent to
Canal Boundary slum. More private clinics
are available outside the slums.
Therapeutic itinerary (self-medication, TBA,
private sector vs public facilities): The
people we met reported problems with
attending public health facilities due to
delays and long waiting times, non-
availability of doctors. At the MCC, the
requirement of donating blood as a pre-
condition to receiving treatment constitutes
a constraint to their patronage. As a result,
people prefer to turn to private and faith-
based clinics as well as traditional birth
attendants (TBA). For instance, the mother
of four we met delivered twice in a faith-
based clinic and twice with a TBA.
Cost of private care: When they go to the
private clinic, they pay an initial registration
fee (e.g. N3000). After that, they can have
74
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

antenatal care with no payment, until
delivery, when they have to pay between
N10,000 - 25,000.
Other observations and findings: So-called
free public health care is not free for the
users.
They know that birth registration,
immunization, antenatal, drugs (MCHC in
general) should be provided at not costs at
public facilities. However, we heard several
complaints about the fact that one needed to
pay N200 to obtain a birth certificate.
Expensive drugs also have to be paid
because of drug stock-outs in public health
facilities.
They seem to prefer to use private health
services despite the high costs of private
care because of better quality of care
(particularly less waiting time) and more
respectful and good inter-personal
relationships with health staff. TBAs are also
seen to provide more appropriate care they
provide the spiritual environment, which is
an important aspect of people's beliefs and
culture and is particularly important at
delivery times for fathers and mothers. We
also heard that husbands insist that their
wives use TBAs. Antenatal care is offered at
public or private health centres but delivery
often takes place with TBAs.
LLIN were distributed in the communities in
late September. However, at the time of our
visit, the mosquito nets were not being used.
Despite the information provided by health
workers, people believed that if one does not
spread the bed nets under the shade for 24
hours, they may cause poisoning. Therefore,
they used the bednets as window / blinds.
Community organization and leadership:The
Aganyi estate has a strong sense of
community (people come from Badagry and
Togo) and strong leadership. They
successfully mobilized the community to
clean the environment (as much as they
could!), organize private garbage collection,
ensure that houses are built away from the
canal itself, erect electricity poles and a
pedestrian bridge linking the estate to the
main road into Ajeromi. By contrast,
Boundary Canal estate located on the other
side of the canal does not seem to have
benef i t ed f rom such commun i ty
mobilization. Their environment is worse in
terms of having garbage-filled and unclean
street as well as extremely poor-quality and
unhealthy housing.
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case
75

Appendix H. Summary table of strategies modelled (Marginal Budgeting for Bottlenecks
method)
Strategies for revitalizing primary health care system in Lagos
Service delivery modes
Community and family care
Strong focus:Aims for 80% access in most and medium deprived areas. Task shifting to community based Integrated Maternal, Newborn and Childhood Management of Childhood Illnesses. Human resources strategy to improve performance, retention and deployment of community health workers.
Preventive services delivered in a facility or outreached
Strong focus:Universal access through campaigns.
Curative care
Moderate focus:Limited infrastructure investment, mostly rehabilitation and upgrading.
Primary health care
Strong focus: Aims for universal access to skilled birth attendant. Full maternity services at primary levels including waiting houses
Secondary and tertiary hospital
Moderate focus:Status quo plus upgrading of 1 district hospital for complicated emergency obstetric care.
Financial access
Direct costStrong focus:Elimination of user fees for all quintiles. Contracting out of services to Non-government providers
Indirect cost
Community participation
Information, education, communication and participation to the governance
Strong focus:
Emphasizes community empowerment and demand promotion and continuity in partnership with community based enablers and promoters.
Additional cost
Supply side
Pre-service training and remuneration for existing and additional community health workers.
Performance incentives and hardship allowances for all other health workers.
Additional in-service training and supervision of all workers.
Supply management at the district level.
Rehabilitation and equipment of primary care facilities as maternities and one hospital per district to perform C-sections and provide laboratory services.
Demand side
Conditional cash transfers for all the wealth deprived
Drugs and supplies for interventions introduced or scaled up (including additional drugs and supplies triggered by the blanket abolition of user fees)
Education, communication and social mobilization
Quality Health information systems and monitoring
Strong focus:Means-tested conditional cash transfers
76
Reducin
g H
ealth D
isparities
in L
agos
Sta
te: A
n Invest
ment
Case

To institutionalize an evidence-based health system that promotes
the delivery of quality, effective, affordable, accessible, acceptable,
cost-efficient and equitable health services to the people of Lagos
State, applying appropriate technology and driven by a highly
motivated staff, thereby contributing to the sustainable economic
development of the State.
Mission statement of Lagos Ministry of Health
LAGOS STATE MINISTRY OF HEALTH unite for children