Embed Size (px)
Citation preview

Red Blood Cell Red Blood Cell DisordersDisorders
Erin SmithErin Smith
AOA Heme/Onc ReviewAOA Heme/Onc Review
November 22, 2009November 22, 2009

A 25 y/o woman has a 3 yr h/o A 25 y/o woman has a 3 yr h/o arthalgias. PE shows no joint arthalgias. PE shows no joint deformity, but she appears deformity, but she appears pale. Lab studies are shown. pale. Lab studies are shown. Peripheral blood smear shows Peripheral blood smear shows hypochromatic and microcytic hypochromatic and microcytic RBC’s. Total serum Fe and RBC’s. Total serum Fe and ferritin levels are within normal ferritin levels are within normal limits. Hb electrophoresis limits. Hb electrophoresis shows an elevated Hb A2 level shows an elevated Hb A2 level of 5.8%. Which of the following of 5.8%. Which of the following is the most likely diagnosis?is the most likely diagnosis?
A) Autoimmune A) Autoimmune hemolytic hemolytic
anemiaanemiaB) Beta thalassemia B) Beta thalassemia
minorminorC) Infection with C) Infection with
Plasmodium vivaxPlasmodium vivaxD) Anemia of chronic D) Anemia of chronic diseasediseaseE) Iron deficiency E) Iron deficiency
anemiaanemia
HbHb 12.512.5
HctHct 3737
Platelet Platelet countcount
217217
RBC RBC countcount
3.73.7

AnswerAnswer
A) Autoimmune hemolytic anemiaA) Autoimmune hemolytic anemia
B) Beta thalassemia minorB) Beta thalassemia minor
C) Infection with C) Infection with Plasmodium vivaxPlasmodium vivax
D) Anemia of chronic diseaseD) Anemia of chronic disease
E) Iron deficiency anemiaE) Iron deficiency anemia
Beta thalassemia and iron deficiency anemia both have hypochromic and microcytic RBC’s. Normal Beta thalassemia and iron deficiency anemia both have hypochromic and microcytic RBC’s. Normal serum ferritin excludes iron deficiency anemia and anemia of chronic disease. serum ferritin excludes iron deficiency anemia and anemia of chronic disease.

A 30 y/o woman has a constant A 30 y/o woman has a constant feeling of lethargy. On PE, she is feeling of lethargy. On PE, she is afebrile and has a pulse of 80/min, afebrile and has a pulse of 80/min, respirations 15/min, and BP 110/70. respirations 15/min, and BP 110/70. The spleen tip is palpable, but there The spleen tip is palpable, but there is no abdominal pain or tenderness. is no abdominal pain or tenderness. Lab studies show Hb of 11.7, platelet Lab studies show Hb of 11.7, platelet count of 159, and WBC count of 5390. count of 159, and WBC count of 5390. Peripheral blood smear shows Peripheral blood smear shows spherocytosis and the RBC’s have an spherocytosis and the RBC’s have an increased osmotic fragility. An increased osmotic fragility. An inherited abnormality in which of the inherited abnormality in which of the following RBC components best following RBC components best accounts for these findings?accounts for these findings?
A) Glucose-6-phosphate A) Glucose-6-phosphate dehydrogenasedehydrogenase
B) Membrane cytoskeletal defectB) Membrane cytoskeletal defect
C) Alpha globin chainC) Alpha globin chain
D) HemeD) Heme
E) Beta globin geneE) Beta globin gene
F) Carbonic anhydraseF) Carbonic anhydrase

AnswerAnswer
A) Glucose-6-phosphate dehydrogenaseA) Glucose-6-phosphate dehydrogenase
B) Membrane cytoskeletal defectB) Membrane cytoskeletal defect
C) Alpha globin chainC) Alpha globin chain
D) HemeD) Heme
E) Beta globin geneE) Beta globin gene
F) Carbonic anhydraseF) Carbonic anhydrase
Hereditary spherocytosis is caused by a mutation in ankyrin or spectrin that causes an increase in Hereditary spherocytosis is caused by a mutation in ankyrin or spectrin that causes an increase in osmotic fragility of the RBC membrane. These deformed cells are destroyed in the spleen. osmotic fragility of the RBC membrane. These deformed cells are destroyed in the spleen.

A 69 y/o female has been A 69 y/o female has been
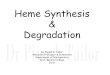
feeling increasingly tired and feeling increasingly tired and weak for 4 months. On PE she weak for 4 months. On PE she is afebrile. There is no is afebrile. There is no hepatosplenomegaly or hepatosplenomegaly or lymphadenopathy. Lab studies lymphadenopathy. Lab studies show Hb of 9.3, platelet count show Hb of 9.3, platelet count of 250, and WBC count of of 250, and WBC count of 6820. The peripheral smear is 6820. The peripheral smear is shown. Which of the following shown. Which of the following conditions should be conditions should be suspected as the most likely suspected as the most likely cause of these findings?cause of these findings?
A) Pernicious anemiaA) Pernicious anemiaB) Gastrointestinal blood lossB) Gastrointestinal blood lossC) Aplastic anemiaC) Aplastic anemiaD) Beta thalassemia majorD) Beta thalassemia majorE) Warm autoimmune E) Warm autoimmune hemolytic anemiahemolytic anemia

AnswerAnswer
A) Pernicious anemiaA) Pernicious anemia
B) Gastrointestinal blood lossB) Gastrointestinal blood loss
C) Aplastic anemiaC) Aplastic anemia
D) Beta thalassemia majorD) Beta thalassemia major
E) Warm autoimmune hemolytic anemiaE) Warm autoimmune hemolytic anemia
The RBC’s show microcytosis and hypochromia which is found in iron deficiency. The most common The RBC’s show microcytosis and hypochromia which is found in iron deficiency. The most common cause in the elderly is due to chronic blood loss from the GI tract. RBC’s are normal in patients with cause in the elderly is due to chronic blood loss from the GI tract. RBC’s are normal in patients with aplastic anemia. Microcytosis can accompany thalassemias but this would already be diagnosed at aplastic anemia. Microcytosis can accompany thalassemias but this would already be diagnosed at an earlier age. Autoimmune HA have a normocytic anemia.an earlier age. Autoimmune HA have a normocytic anemia.

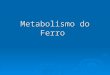
A 40 y/o man has had pain and A 40 y/o man has had pain and burning on urination for the burning on urination for the past week. On PE, he is febrile past week. On PE, he is febrile and has a pulse of 92/min, RR and has a pulse of 92/min, RR 18/min, and BP 80/45. Digital 18/min, and BP 80/45. Digital rectal exam indicates a rectal exam indicates a tender, enlarged prostate. tender, enlarged prostate. Scattered ecchymoses are Scattered ecchymoses are present over the trunk and present over the trunk and extremities. Blood cx is + for extremities. Blood cx is + for Klebsiella pneumoniaeKlebsiella pneumoniae. The . The blood smear is shown. These blood smear is shown. These findings are indicative of findings are indicative of which of the following?which of the following?
A) Hereditary spherocytosisA) Hereditary spherocytosisB) Autoimmune hemolytic B) Autoimmune hemolytic anemiaanemiaC) Microangiopathic hemolytic C) Microangiopathic hemolytic anemiaanemiaD) Iron deficiency anemiaD) Iron deficiency anemiaE) Megaloblastic anemiaE) Megaloblastic anemia

AnswerAnswer
A) Hereditary spherocytosisA) Hereditary spherocytosis
B) Autoimmune hemolytic anemiaB) Autoimmune hemolytic anemia
C)C) Microangiopathic hemolytic anemiaMicroangiopathic hemolytic anemia
D) Iron deficiency anemiaD) Iron deficiency anemia
E) Megaloblastic anemiaE) Megaloblastic anemia
The patient has Gram negative sepsis leading to DIC. The fragmented RBC’s known as shistocytes or The patient has Gram negative sepsis leading to DIC. The fragmented RBC’s known as shistocytes or helmet cells are typical of conditions that can produce a microangiopathic HA such as DIC, TTP, SLE, helmet cells are typical of conditions that can produce a microangiopathic HA such as DIC, TTP, SLE, HUS, and malignant HTN. Autoimmune HA there is extravascular hemolysis.HUS, and malignant HTN. Autoimmune HA there is extravascular hemolysis.

Three days after starting the prophylactic antimalarial drug Three days after starting the prophylactic antimalarial drug primaquine, a 23 y/o African American passes dark reddish-primaquine, a 23 y/o African American passes dark reddish-brown urine. He is surprised by this, since he has been brown urine. He is surprised by this, since he has been healthy up to now. CBC shows a mild normocytic anemia, healthy up to now. CBC shows a mild normocytic anemia, but the peripheral smear shows precipitates of denatured but the peripheral smear shows precipitates of denatured globin (Heinz bodies) with scattered bite cells. Which of the globin (Heinz bodies) with scattered bite cells. Which of the following is the most likely diagnosis?following is the most likely diagnosis?
A) Beta thalassemia minorA) Beta thalassemia minor
B) Glucose 6- Phosphate dehydrogenase deficiencyB) Glucose 6- Phosphate dehydrogenase deficiency
C) Autoimmune hemolytic anemiaC) Autoimmune hemolytic anemia
D) Pyruvate kinase deficiencyD) Pyruvate kinase deficiency
E) Microangiopathic hemolytic anemiaE) Microangiopathic hemolytic anemia
F) Alpha ThalassemiaF) Alpha Thalassemia

AnswerAnswer
A) Beta thalassemia minorA) Beta thalassemia minor
B) Glucose 6- Phosphate dehydrogenase B) Glucose 6- Phosphate dehydrogenase deficiencydeficiency
C) Autoimmune hemolytic anemiaC) Autoimmune hemolytic anemia
D) Pyruvate kinase deficiencyD) Pyruvate kinase deficiency
E) Microangiopathic hemolytic anemiaE) Microangiopathic hemolytic anemia
F) Alpha ThalassemiaF) Alpha Thalassemia
G6PD deficiency causes oxidative damage to RBC’s with exposure to primaquine, sulfonamides, G6PD deficiency causes oxidative damage to RBC’s with exposure to primaquine, sulfonamides, nitrofurantoin, phenacetin, and aspirin. Infection can also cause RBC oxidation and lysis. nitrofurantoin, phenacetin, and aspirin. Infection can also cause RBC oxidation and lysis.

A 60 y/o man has developed widespread ecchymoses over A 60 y/o man has developed widespread ecchymoses over the skin in the past month. His medical history includes a the skin in the past month. His medical history includes a diagnosis of mucinous adenocarcinoma of the rectum. On diagnosis of mucinous adenocarcinoma of the rectum. On PE, he appears cachectic and pale. An abdominal CT scan PE, he appears cachectic and pale. An abdominal CT scan shows multiple hepatic masses. Lab studies reveal PT of 30 shows multiple hepatic masses. Lab studies reveal PT of 30 sec, PTT of 55 sec, platelet count of 15200, fibrinogen level sec, PTT of 55 sec, platelet count of 15200, fibrinogen level of 75, and fibrin split product levels that are very elevated. of 75, and fibrin split product levels that are very elevated. Which of the following morphologic findings is most likely to Which of the following morphologic findings is most likely to present on the peripheral blood smear?present on the peripheral blood smear?
A) Howell- Jolly bodiesA) Howell- Jolly bodies
B) Teardrop cellsB) Teardrop cells
C) Macro- ovalocytesC) Macro- ovalocytes
D) SchistocytesD) Schistocytes
E) Target cellsE) Target cells

AnswerAnswer
A) Howell- Jolly bodiesA) Howell- Jolly bodies
B) Teardrop cellsB) Teardrop cells
C) Macro- ovalocytesC) Macro- ovalocytes
D) SchistocytesD) Schistocytes
E) Target cellsE) Target cells
This is an example of DIC with associated microangiopathic HA. Howell- Jolly bodies are caused by This is an example of DIC with associated microangiopathic HA. Howell- Jolly bodies are caused by asplenia. Micro-ovalocytes are due to megaloblastic anemias. Teardrop cells are due to asplenia. Micro-ovalocytes are due to megaloblastic anemias. Teardrop cells are due to myelofibrosis. Targets are due to HbC disease or severe liver disease.myelofibrosis. Targets are due to HbC disease or severe liver disease.

A 50 y/o man sees his physician A 50 y/o man sees his physician because he has experienced because he has experienced chronic fatigue and weight loss chronic fatigue and weight loss for the past 3 months. There for the past 3 months. There are no remarkable findings on are no remarkable findings on PE. Labs are shown. ANA test is PE. Labs are shown. ANA test is positive. Which of the following positive. Which of the following is the most likely diagnosis?is the most likely diagnosis?
A) Anemia of chronic A) Anemia of chronic diseasedisease
B) Aplastic anemiaB) Aplastic anemia
C) Microangiopathic C) Microangiopathic hemolytic hemolytic
anemiaanemia
D) Iron deficiency D) Iron deficiency anemiaanemia
E) Megaloblastic anemiaE) Megaloblastic anemia
F) Thalassemia minorF) Thalassemia minor
HbHb 11.211.2
HctHct 33.333.3
Platelet Platelet countcount
240240
RBC RBC countcount
2.692.69
MCVMCV 9191
WBC WBC countcount
75507550
Serum FeSerum Fe 8080
TIBCTIBC 145145
Serum Serum FerritinFerritin
565565

AnswerAnswer
A) Anemia of chronic diseaseA) Anemia of chronic disease
B) Aplastic anemiaB) Aplastic anemia
C) Microangiopathic hemolytic anemiaC) Microangiopathic hemolytic anemia
D) Iron deficiency anemiaD) Iron deficiency anemia
E) Megaloblastic anemiaE) Megaloblastic anemia
F) Thalassemia minorF) Thalassemia minor
The patient has a positive ANA test which is commonly seen in rheumatologic diseases like SLE. The patient has a positive ANA test which is commonly seen in rheumatologic diseases like SLE. Increased ferritin concentration and reduced TIBC are hallmarks of anemia of chronic disease, such Increased ferritin concentration and reduced TIBC are hallmarks of anemia of chronic disease, such as an autoimmune process. Increased cytokine levels cause sequestration of storage iron in as an autoimmune process. Increased cytokine levels cause sequestration of storage iron in macrophages.macrophages.

A 39 y/o woman complains of A 39 y/o woman complains of abdominal pain and intermittent low abdominal pain and intermittent low volume diarrhea for the past 3 volume diarrhea for the past 3 months. A stool sample is positive months. A stool sample is positive for occult blood. On colonoscopy, for occult blood. On colonoscopy, biopsy results reveal Crohn’s biopsy results reveal Crohn’s disease. She has surgery to remove disease. She has surgery to remove part of her colon and terminal part of her colon and terminal ileum. She is transfused with 2 units ileum. She is transfused with 2 units of RBC’s. 2 weeks later she c/o of RBC’s. 2 weeks later she c/o fatigue. Labs are shown. Which of fatigue. Labs are shown. Which of the following is the most likely to the following is the most likely to produce these findings?produce these findings?
A) Hemolytic anemiaA) Hemolytic anemia
B) Aplastic anemiaB) Aplastic anemia
C) Chronic blood lossC) Chronic blood loss
D) Anemia of chronic diseaseD) Anemia of chronic disease
E) Bone marrow metastasesE) Bone marrow metastases
F) Vitamin B12 deficiencyF) Vitamin B12 deficiency
HbHb 10.610.6
HctHct 31.631.6
PlatelPlatelet et countcount
378378
RBC RBC countcount
2.692.69
MCVMCV 118118
Retic Retic countcount
0.3%0.3%

AnswerAnswer
A) Hemolytic anemiaA) Hemolytic anemia
B) Aplastic anemiaB) Aplastic anemia
C) Chronic blood lossC) Chronic blood loss
D) Anemia of chronic diseaseD) Anemia of chronic disease
E) Bone marrow metastasesE) Bone marrow metastases
F) Vitamin B12 deficiencyF) Vitamin B12 deficiency
High MCV indicated macrocytosis. B12 is absorbed in the terminal ileum and removal causes B12 High MCV indicated macrocytosis. B12 is absorbed in the terminal ileum and removal causes B12 deficiency.deficiency.

A 22 year old woman has experienced malaise A 22 year old woman has experienced malaise and sore throat for 2 weeks. She has a temp of and sore throat for 2 weeks. She has a temp of 37.8C and her pharynx is erythematous. 37.8C and her pharynx is erythematous. Monospot test is positive. The direct and indirect Monospot test is positive. The direct and indirect Coombs test results are positive at 4C, but not at Coombs test results are positive at 4C, but not at 37C. Which of the following substances on the 37C. Which of the following substances on the surfaces of the RBC’s accounts for these findings?surfaces of the RBC’s accounts for these findings?
A) Ig EA) Ig EB) IgGB) IgGC) HistamineC) HistamineE) Complement C3b and IgME) Complement C3b and IgMF) Fibronectin F) Fibronectin

AnswerAnswer
A) Ig EA) Ig E
B) IgGB) IgG
C) HistamineC) Histamine
E) Complement C3bE) Complement C3b
F) FibronectinF) Fibronectin
The patient has cold agglutinin disease (cold antibody hemolytic anemia), with IgM antibodies that bind The patient has cold agglutinin disease (cold antibody hemolytic anemia), with IgM antibodies that bind to the RBC’s at low temperature and fix complement. With a rise in temp. the IgM leaves the cell, to the RBC’s at low temperature and fix complement. With a rise in temp. the IgM leaves the cell, and the C3b remains attached to the RBC membrane. This is an extravascular hemolysis.and the C3b remains attached to the RBC membrane. This is an extravascular hemolysis.

A 3 y/o boy of Italian ancestry is brought to the physician A 3 y/o boy of Italian ancestry is brought to the physician because he has a poor appetitie and is underweight for his because he has a poor appetitie and is underweight for his age and height. PE shows hepatosplenomegaly. Hb is 6, age and height. PE shows hepatosplenomegaly. Hb is 6, and peripheral blood smear shows hypochromic, microcytic and peripheral blood smear shows hypochromic, microcytic RBC’s. Total serum Fe is normal and retic count is 10%. A RBC’s. Total serum Fe is normal and retic count is 10%. A radiograph of ths skull shows maxillfacial deformities and radiograph of ths skull shows maxillfacial deformities and an expanded marrow space. Which of the following is the an expanded marrow space. Which of the following is the most likely principle cause of the child’s illness?most likely principle cause of the child’s illness?
A) Reduced synthesis of Hb FA) Reduced synthesis of Hb FB) Imbalance in production of alpha and beta globin chainsB) Imbalance in production of alpha and beta globin chainsC) Sequestration of iron in reticuloendothelial cellsC) Sequestration of iron in reticuloendothelial cellsD) Increased fragility of RBC membraneD) Increased fragility of RBC membraneE) Relative deficiency of vitamin B12E) Relative deficiency of vitamin B12

AnswerAnswer
A) Reduced synthesis of Hb FA) Reduced synthesis of Hb FB) Imbalance in production of alpha B) Imbalance in production of alpha and beta globin chainsand beta globin chainsC) Sequestration of iron in C) Sequestration of iron in reticuloendothelial cellsreticuloendothelial cellsD) Increased fragility of RBC membraneD) Increased fragility of RBC membraneE) Relative deficiency of vitamin B12E) Relative deficiency of vitamin B12
The patient has beta thal major. There is a severe reduction in synthesis of beta globin chains with The patient has beta thal major. There is a severe reduction in synthesis of beta globin chains with normal production of alpha chains. The alpha chains form aggregates that precipitate and cause cell normal production of alpha chains. The alpha chains form aggregates that precipitate and cause cell death. This results in inefective erythropoiesis and iron overload (hemochromatosis). Patients have death. This results in inefective erythropoiesis and iron overload (hemochromatosis). Patients have infiltrative cardiomyopathy, hepatic cirrhosis, and bronze diabetes. EPO stimulates the bone marrow infiltrative cardiomyopathy, hepatic cirrhosis, and bronze diabetes. EPO stimulates the bone marrow causing BM expansion. Hepatosplenomegaly occurs with extramedullary hematopoiesis. causing BM expansion. Hepatosplenomegaly occurs with extramedullary hematopoiesis.

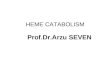
A 12 y/o boy has a h/o A 12 y/o boy has a h/o episodes of severe episodes of severe abdominal pain and back abdominal pain and back pain since early childhood. pain since early childhood. On PE, he is afebrile. Labs On PE, he is afebrile. Labs show Hb 11.2, platelets 194, show Hb 11.2, platelets 194, and WBC 9020. Peripheral and WBC 9020. Peripheral blood smear is shown. Hb blood smear is shown. Hb electrophoresis shows 1% electrophoresis shows 1% HbA2, 6%Hb F, and 93%Hb HbA2, 6%Hb F, and 93%Hb S. Hydroxyurea is started. S. Hydroxyurea is started. Which of the following is the Which of the following is the most likely mechanism of most likely mechanism of this drug?this drug?A) Increase in production of A) Increase in production of Hb AHb AB) Increase in oxygen B) Increase in oxygen affinity for Hbaffinity for HbC) Stimulation of RBC C) Stimulation of RBC productionproductionD) Increase in production of D) Increase in production of HbFHbFE) Decrease in overall globin E) Decrease in overall globin synthesissynthesis

AnswerAnswer
A) Increase in production of Hb AA) Increase in production of Hb A
B) Increase in oxygen affinity for HbB) Increase in oxygen affinity for Hb
C) Stimulation of RBC productionC) Stimulation of RBC production
D) Increase in production of HbFD) Increase in production of HbF
E) Decrease in overall globin synthesisE) Decrease in overall globin synthesis
The crescent shaped RBC’s are characteristic of Hb SS. Sickled cells can undergo hemolysis and cause The crescent shaped RBC’s are characteristic of Hb SS. Sickled cells can undergo hemolysis and cause microvascular occlusions causing pain crises (acute chest syndrome, splenic infarction). Howell jolly microvascular occlusions causing pain crises (acute chest syndrome, splenic infarction). Howell jolly bodies are result of autosplenectomy. Hydroxyurea can increase the HbF concentration, which bodies are result of autosplenectomy. Hydroxyurea can increase the HbF concentration, which interferes with the polymerization of Hb S. interferes with the polymerization of Hb S.

Resources to UseResources to Use
Robbins Review of Pathology Robbins Review of Pathology questionsquestions
http://library.med.utah.edu/http://library.med.utah.edu/WebPath/webpath.htmlWebPath/webpath.html