Embed Size (px)
Citation preview
RECONSTRUCTIVE
Reconstruction of Complex Abdominal WallDefects with Free Flaps: Indications andClinical Outcome
Chin-Ho Wong, M.R.C.S.Chih-Hung Lin, M.D.
Brian Fu, M.R.C.S.Jen-Feng Fang, M.D.
Taipei, Taiwan; and Singapore
Background: Free flaps have a distinct role in a select group of patients withlarge abdominal wall defects. They offer a completely autologous reconstructivesolution in a single stage for difficult abdominal wounds for which pedicled flapswould be inadequate.Methods: From 1996 to 2005, five patients with complex abdominal wall defectsunderwent reconstruction using free flaps. All patients had multiple comor-bidities, making the use of alloplastic materials relatively contraindicated. Flapsused included a free radial forearm flap in one patient, a tensor fasciae lataemyocutaneous flap in two patients, a free anterolateral thigh myocutaneous flapin one patient, and free conjoined tensor fasciae latae and anterolateral thighmyocutaneous flaps in the last patient.Results: The mean defect size was 470 cm2 (range, 136 to 875 cm2). The femoralartery and long saphenous vein reliably provided recipient vessels in cases for whichsuitable vessels could not be located within the abdomen. A temporary arterio-venous shunt of the long saphenous vein to the femoral artery could be created. Thiswas later divided to provide a recipient artery and vein. Flap complications werewound edge necrosis, hematoma, infection, and venous thrombosis. All were suc-cessfully managed and there were no flap failures. The average length of hospi-talization was 64 days (range, 41 to 128 days). Lateral thigh flaps based on the lateralcircumflex femoral system are our preferred donor site. A large amount of softtissue, strong fascia, and innervated muscle are available, enabling single-stageautologous reconstruction of the entire anterior abdominal wall.Conclusions: Free flaps offer a reliable single-stage solution to complex ab-dominal wall defects. With these techniques, even the most challengingdefects can be reconstructed with completely autologous tissue. (Plast.Reconstr. Surg. 124: 500, 2009.)
Reconstruction of complex abdominal walldefects is clinically challenging and techni-cally demanding. Requirements for satisfac-
tory reconstruction are soft-tissue coverage andrestoration of the musculofascial support for ab-dominal contents.1 In patients with significant tis-sue loss, primary closure is not feasible. Tech-niques such as component separation and localflaps are generally the preferred reconstructive
options.1–3 Alloplastic materials such as Gore-Tex(W. L. Gore and Associates, Flagstaff, Ariz.) orMarlex mesh (Davol, Inc., Cranston, R.I.) havebeen widely used for restoration of the musculo-fascial integrity of the abdominal wall, with vari-able success.4–9 Such foreign materials are rela-tively contraindicated in immunocompromisedpatients, as they are associated with unacceptablyhigh complication rates.10 Free tissue transfer isoften regarded as the option of last resort in ab-dominal wall reconstruction. However, free-tissuetransfer offers some distinct advantages over localflaps and has a definite role in a selected group of
From the Division of Trauma, Department of Plastic andReconstructive Surgery, Chang Gung Memorial Hospital,Chang Gung University; the Department of General Surgery,Chang Gung Memorial Hospital; and the Department ofPlastic, Reconstructive, and Aesthetic Surgery, SingaporeGeneral Hospital.Received for publication December 3, 2008; acceptedFebruary 20, 2009.Copyright ©2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181addb11
Disclosure: The authors did not receive any fund-ing for this work and have no conflict of interest todisclose.
www.PRSJournal.com500

patients. This article described our experiencewith the use of free flaps in the reconstruction ofcomplex abdominal wall defects and details ourindications for the use of free flaps in abdominalwall reconstruction.
PATIENTS AND METHODSFrom 1996 to 2005, five patients with complex
abdominal wall defects underwent reconstructionwith free flaps. All patients were treated initially bygeneral surgeons at our institution and were sub-sequently referred to the senior author (C.-H.L.)for reconstruction. Four patients were men andone was a woman. Contaminated or infected ab-dominal wounds were debrided serially and cov-ered temporarily with occlusive dressings until thewounds were clean and the nutritional status ofthe patients was optimized.11 Reconstruction wasperformed with a free tensor fasciae latae myocu-taneous flap in two patients, a free radial forearmflap in one patient, a free anterolateral thigh myo-cutaneous flap in one patient, and a free con-joined tensor fasciae latae and anterolateral thighmyocutaneous flap in one patient. The selectionof flap was guided by defect requirement in termsof size and components needed. The lateral thighbased on the lateral circumflex femoral system isour preferred donor site. The entire anterior ab-dominal wall can be reconstructed by harvestingconjoined vascular territories such as that of thetensor fasciae latae and anterolateral thigh, safelyincorporating up to half the skin of the lateralthigh. In one of our patients, the radial forearmwas used, as the patient has severe peripheral vas-cular disease with bilateral above-knee amputa-tions.
The femoral artery (just below the inguinalligament) and the long saphenous vein offer areliable and robust source of “extraabdominal”recipient vessels in cases where intraabdominalvessels are unavailable or inadequate. It is partic-ularly useful in cases where severe trauma or mul-tiple previous incisions have compromised thecommonly used intraabdominal recipient vessels.In two patients, a temporary arteriovenous shuntwas created. The long saphenous vein was mobi-lized from the groin down to the thigh and leg forthe required length. An end-to-side anastomosis ofthe distal end of the greater saphenous vein to thefemoral artery was then performed in the groinjust below the inguinal ligament. This arterio-venous loop was then swung 180 degrees into theabdominal and subsequently divided at its mid-point to create an inflow and outflow for arterialand venous anastomosis to the donor vessels. In
one patient, when long segments vein grafts wereneeded, both the long and short saphenous veinswere harvested. In another patient, the long sa-phenous vein was used to provide a second venousanastomosis to improve venous outflow.
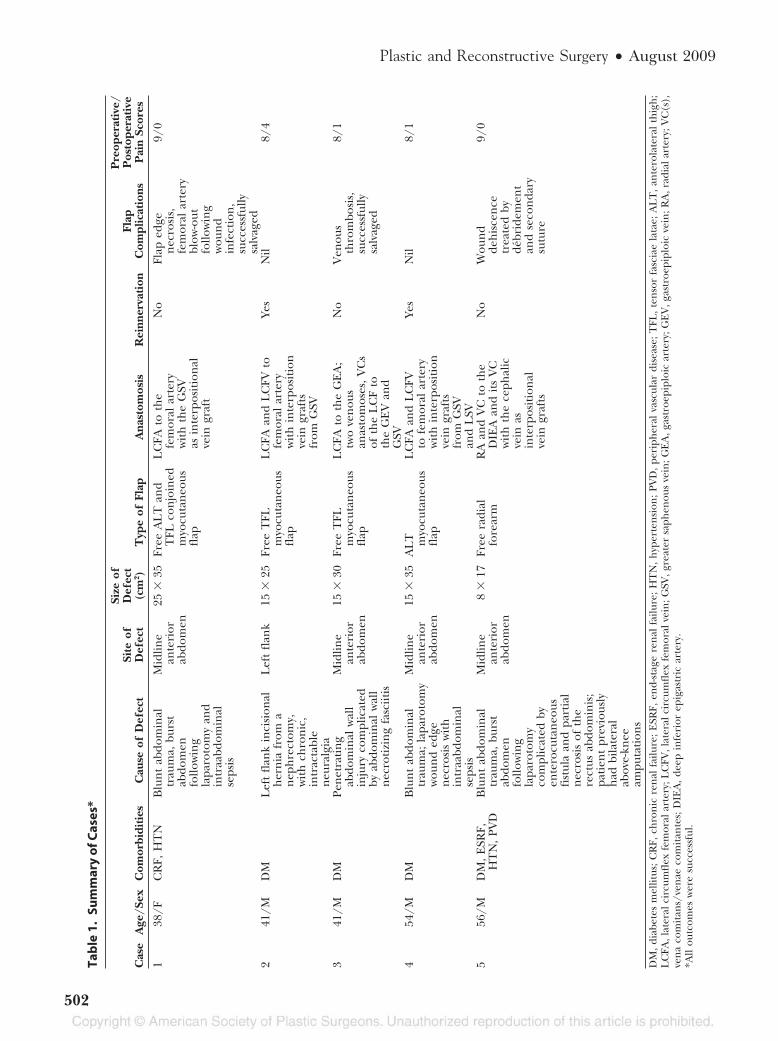
RESULTSTable 1 gives a summary of the patients and
reconstructive outcomes. The mean defect sizewas 470 cm2 (range, 136 to 875 cm2). The meanfollow-up was 23 months (range, 12 to 102months). Flap complications occurred in three ofour five patients, partly because of the multiplecomorbidities and poor nutritional status of ourpatients. These were successfully managed withdebridements and reanastomosis if necessary.There were no flap failures. The average time ofhospitalization was 64 days (range, 41 to 128 days).At follow-up, none of the patients developed anyabdominal wall herniation and the donor-sitemorbidity was well tolerated.
CASE REPORTSCase 1
A 38-year-old woman fell from a height of three floors. Thisresulted in blunt abdominal trauma and a right femoral shaftfracture. An emergent laparotomy found hemoperitoneumwith hepatic laceration, pancreatic contusion, and small bowelperforations. Postoperatively, she developed enterocutaneousfistula and wound edge necrosis of the midline laparotomywound. She was given total parenteral nutrition and the woundswere debrided serially. She presented to us 33 days after herinitial operation with a 25 � 35-cm2 defect (Fig. 1, left). Thewound was clean but the rectus abdominis was partially resectedand there was significant loss of domain of the abdominal wall.A conjoined anterolateral thigh and tensor fasciae latae myo-cutaneous flap was designed incorporating the deep fascia ofthe lateral thigh based on the lateral circumflex femoral arterysystem (Fig. 1, above and below, right). Inset was performed inlayers, with the deep fascia sutured to the musculofascial layerof the abdomen to restore abdominal wall support (Fig. 2, left).The long saphenous vein was harvested down to the knee anda temporary arteriovenous loop created as described. This wasthen turned cephalically into the abdominal wall and divided,creating a recipient artery and vein measuring 20 cm each. Thedonor site was closed with split-thickness skin grafts.
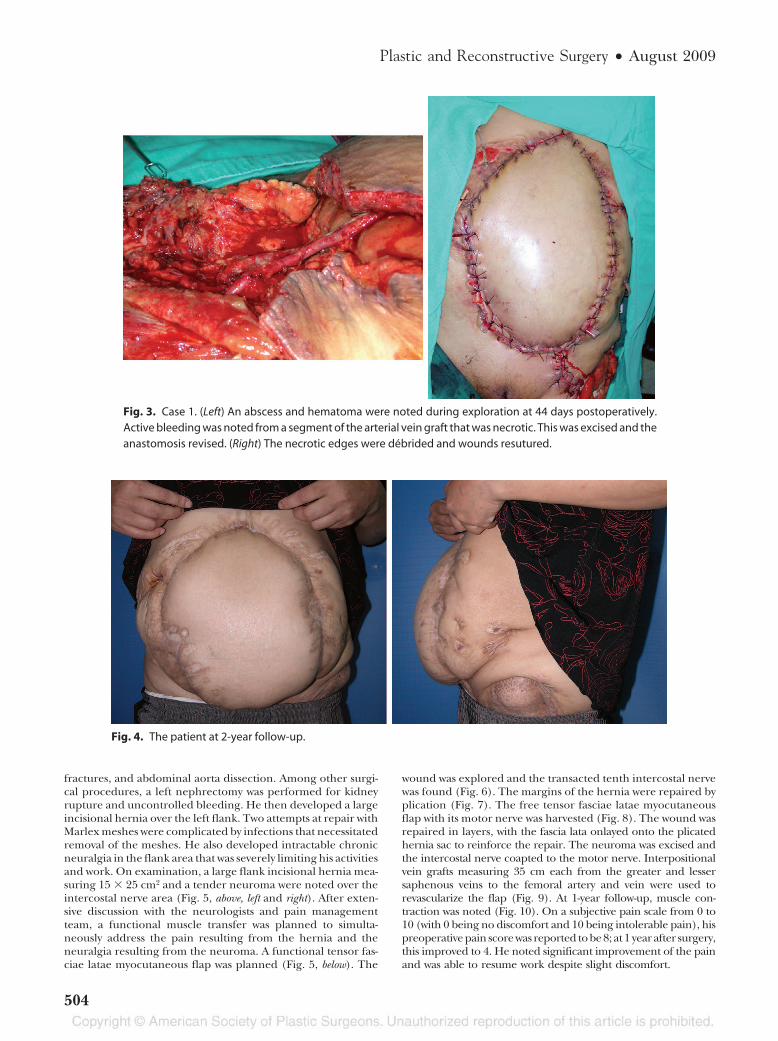
Forty-four days after the initial procedure, the edge of theflap was also noted to be dusky (Fig. 2, right). The patient wentinto hypovolemic shock and was resuscitated aggressively withfluid and blood transfusions. Emergent exploration noted anabscess around the pedicle, with an arterial blow-out at the siteof the end-to-side anastomosis (Fig. 3, left). Debridement wasperformed and the artery anastomosis was redone. The necroticwound edge was excised and the wound resutured (Fig. 3, right).Healing was subsequently achieved. At 2-year follow-up, goodabdominal support with no herniation was noted (Fig. 4).
Case 2A 41-year-old man with a history of diabetes mellitus sus-
tained blunt abdominal trauma in a road traffic accident. Hesustained thoracolumbar spine fracture (T12 to L1), lower limb
Volume 124, Number 2 • Complex Abdominal Wall Defects
501
Tab
le1
.Su
mm
ary
ofC
ases
*
Cas
eA
ge/S
exC
omor
bidi
ties
Cau
seof
Def
ect
Site
ofD
efec
t
Size
ofD
efec
t(c
m2 )
Typ
eof
Flap
Ana
stom
osis
Rei
nner
vati
onFl
apC
ompl
icat
ions
Pre
oper
ativ
e/P
osto
pera
tive
Pai
nSc
ores
138
/FC
RF,
HT
NB
lun
tab
dom
inal
trau
ma,
burs
tab
dom
enfo
llow
ing
lapa
roto
my
and
intr
aabd
omin
alse
psis
Mid
line
ante
rior
abdo
men
25�
35Fr
eeA
LT
and
TFL
con
join
edm
yocu
tan
eous
flap
LC
FAto
the
fem
oral
arte
ryw
ith
the
GSV
asin
terp
osit
ion
alve
ingr
aft
No
Flap
edge
nec
rosi
s,fe
mor
alar
tery
blow
-out
follo
win
gw
oun
din
fect
ion
,su
cces
sful
lysa
lvag
ed
9/0
241
/MD
ML
eft
flan
kin
cisi
onal
her
nia
from
an
eph
rect
omy,
wit
hch
ron
ic,
intr
acta
ble
neu
ralg
ia
Lef
tfl
ank
15�
25Fr
eeT
FLm
yocu
tan
eous
flap
LC
FAan
dL
CFV
tofe
mor
alar
tery
wit
hin
terp
osit
ion
vein
graf
tsfr
omG
SV
Yes
Nil
8/4
341
/MD
MPe
net
rati
ng
abdo
min
alw
all
inju
ryco
mpl
icat
edby
abdo
min
alw
all
nec
roti
zin
gfa
sciit
is
Mid
line
ante
rior
abdo
men
15�
30Fr
eeT
FLm
yocu
tan
eous
flap
LC
FAto
the
GE
A;
two
ven
ous
anas
tom
oses
,V
Cs
ofth
eL
CF
toth
eG
EV
and
GSV
No
Ven
ous
thro
mbo
sis,
succ
essf
ully
salv
aged
8/1
454
/MD
MB
lun
tab
dom
inal
trau
ma;
lapa
roto
my
wou
nd
edge
nec
rosi
sw
ith
intr
aabd
omin
alse
psis
Mid
line
ante
rior
abdo
men
15�
35A
LT myo
cuta
neo
usfl
ap
LC
FAan
dL
CFV
tofe
mor
alar
tery
wit
hin
terp
osit
ion
vein
graf
tsfr
omG
SVan
dL
SV
Yes
Nil
8/1
556
/MD
M,
ESR
F,H
TN
,PV
DB
lun
tab
dom
inal
trau
ma,
burs
tab
dom
enfo
llow
ing
lapa
roto
my
com
plic
ated
byen
tero
cuta
neo
usfi
stul
aan
dpa
rtia
ln
ecro
sis
ofth
ere
ctus
abdo
min
is;
pati
ent
prev
ious
lyh
adbi
late
ral
abov
e-kn
eeam
puta
tion
s
Mid
line
ante
rior
abdo
men
8�
17Fr
eera
dial
fore
arm
RA
and
VC
toth
eD
IEA
and
its
VC
wit
hth
ece
phal
icve
inas
inte
rpos
itio
nal
vein
graf
ts
No
Wou
nd
deh
isce
nce
trea
ted
byde
brid
emen
tan
dse
con
dary
sutu
re
9/0
DM
,dia
bete
sm
ellit
us;C
RF,
chro
nic
ren
alfa
ilure
;ESR
F,en
d-st
age
ren
alfa
ilure
;HT
N,h
yper
ten
sion
;PV
D,p
erip
her
alva
scul
ardi
seas
e;T
FL,t
enso
rfa
scia
ela
tae;
AL
T,a
nte
rola
tera
lth
igh
;L
CFA
,lat
eral
circ
umfl
exfe
mor
alar
tery
;LC
FV,l
ater
alci
rcum
flex
fem
oral
vein
;GSV
,gre
ater
saph
enou
sve
in;G
EA
,gas
troe
pipl
oic
arte
ry;G
EV
,gas
troe
pipl
oic
vein
;RA
,rad
iala
rter
y;V
C(s
),ve
na
com
itan
s/ve
nae
com
itan
tes;
DIE
A,
deep
infe
rior
epig
astr
icar
tery
.*A
llou
tcom
esw
ere
succ
essf
ul.
Plastic and Reconstructive Surgery • August 2009
502
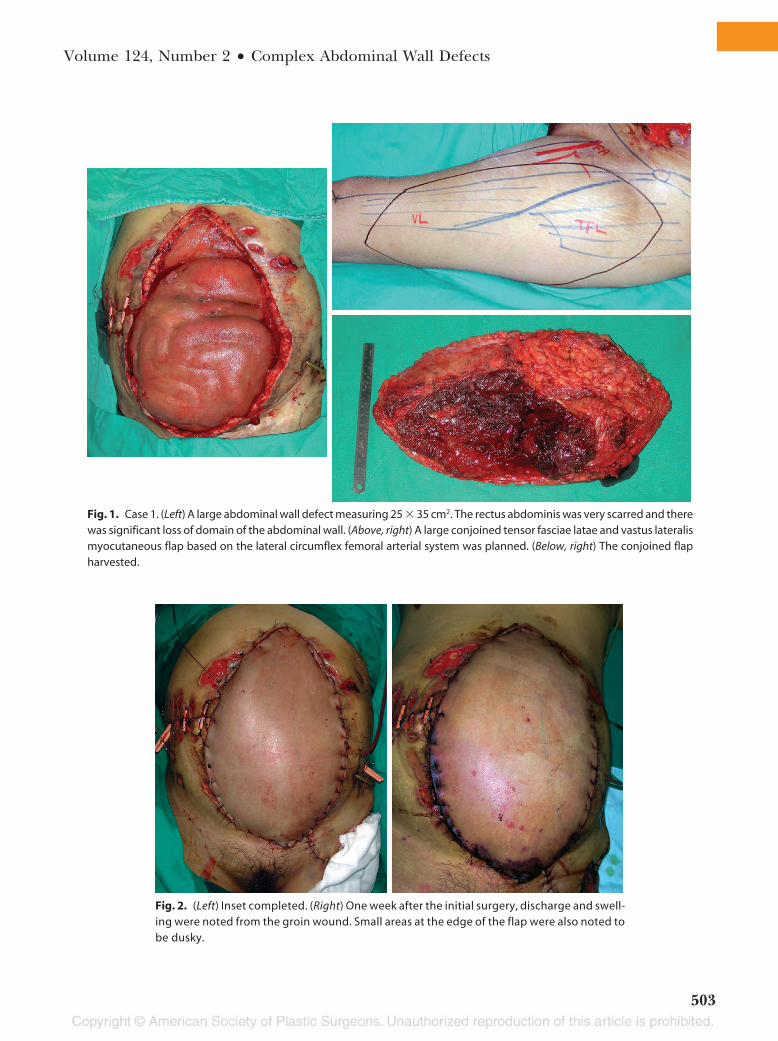
Fig. 1. Case 1. (Left) A large abdominal wall defect measuring 25 � 35 cm2. The rectus abdominis was very scarred and therewas significant loss of domain of the abdominal wall. (Above, right) A large conjoined tensor fasciae latae and vastus lateralismyocutaneous flap based on the lateral circumflex femoral arterial system was planned. (Below, right) The conjoined flapharvested.
Fig. 2. (Left) Inset completed. (Right) One week after the initial surgery, discharge and swell-ing were noted from the groin wound. Small areas at the edge of the flap were also noted tobe dusky.
Volume 124, Number 2 • Complex Abdominal Wall Defects
503
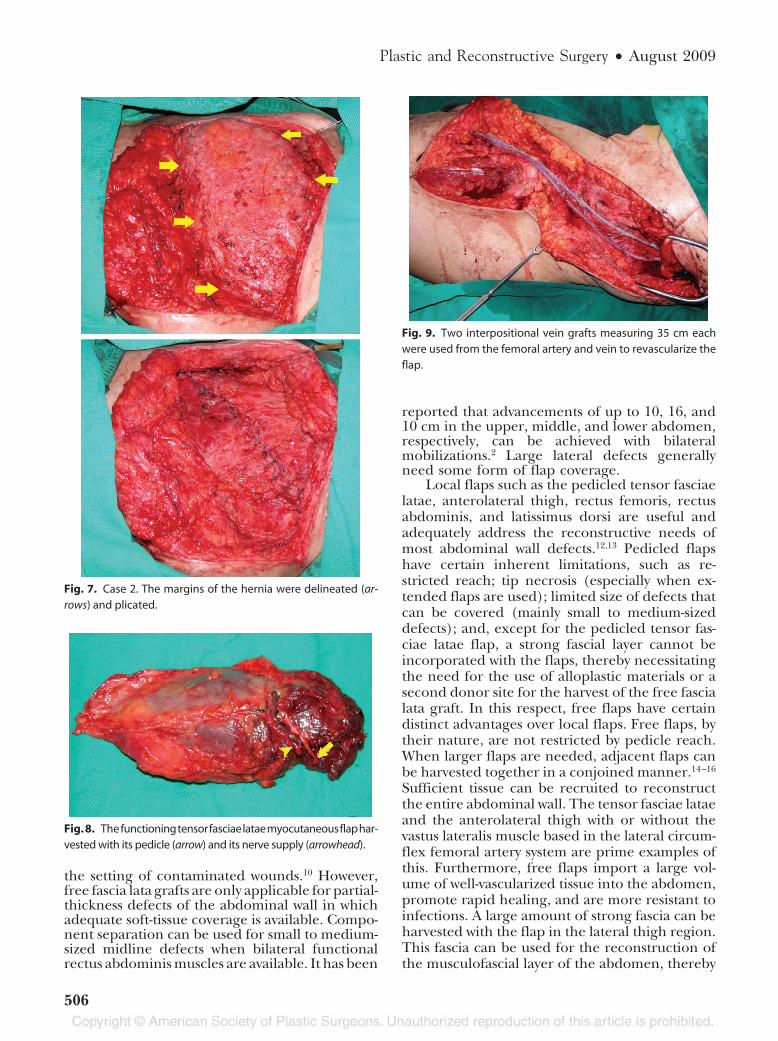
fractures, and abdominal aorta dissection. Among other surgi-cal procedures, a left nephrectomy was performed for kidneyrupture and uncontrolled bleeding. He then developed a largeincisional hernia over the left flank. Two attempts at repair withMarlex meshes were complicated by infections that necessitatedremoval of the meshes. He also developed intractable chronicneuralgia in the flank area that was severely limiting his activitiesand work. On examination, a large flank incisional hernia mea-suring 15 � 25 cm2 and a tender neuroma were noted over theintercostal nerve area (Fig. 5, above, left and right). After exten-sive discussion with the neurologists and pain managementteam, a functional muscle transfer was planned to simulta-neously address the pain resulting from the hernia and theneuralgia resulting from the neuroma. A functional tensor fas-ciae latae myocutaneous flap was planned (Fig. 5, below). The
wound was explored and the transacted tenth intercostal nervewas found (Fig. 6). The margins of the hernia were repaired byplication (Fig. 7). The free tensor fasciae latae myocutaneousflap with its motor nerve was harvested (Fig. 8). The wound wasrepaired in layers, with the fascia lata onlayed onto the plicatedhernia sac to reinforce the repair. The neuroma was excised andthe intercostal nerve coapted to the motor nerve. Interpositionalvein grafts measuring 35 cm each from the greater and lessersaphenous veins to the femoral artery and vein were used torevascularize the flap (Fig. 9). At 1-year follow-up, muscle con-traction was noted (Fig. 10). On a subjective pain scale from 0 to10 (with 0 being no discomfort and 10 being intolerable pain), hispreoperative pain score was reported to be 8; at 1 year after surgery,this improved to 4. He noted significant improvement of the painand was able to resume work despite slight discomfort.
Fig. 3. Case 1. (Left) An abscess and hematoma were noted during exploration at 44 days postoperatively.Active bleeding was noted from a segment of the arterial vein graft that was necrotic. This was excised and theanastomosis revised. (Right) The necrotic edges were debrided and wounds resutured.
Fig. 4. The patient at 2-year follow-up.
Plastic and Reconstructive Surgery • August 2009
504

DISCUSSIONIn the management of abdominal wall defects,
three main factors should be taken into consid-eration: (1) medical status of the patient (in par-ticular, the presence of any comorbidities); (2)wound depth (full-thickness versus partial-thick-ness defects); and (3) size and position of thedefect.1 In general, patients with significant co-morbidities such as diabetes mellitus have muchhigher infective complications associated with theuse of foreign materials, and autologous tissue ispreferred.10 In particular, a history of previousfailed attempts at reconstruction with alloplasticmaterials should be regarded as a relative contra-indication for the further use of such foreign ma-terials. Disa et al. have clearly demonstrated thesuperiority of autologous free fascia lata grafts in
Fig. 5. Case 2. (Above, left and right) Preoperative views showing a large flank incisional hernia measuring15 � 25 cm2. Marked tenderness and hyperesthesia over the left subcostal area was also elicited. (Below)Preoperative markings. The tenth intercostal nerve was planned to be used as the recipient motor nerve(arrowhead). The planned tensor fasciae latae functioning muscle was marked with the blue line (blue arrow)indicating the incision site and the black markings (black arrow) delineating the planned fascia lata to beharvested.
Fig. 6. The offending neuroma was located (arrow).
Volume 124, Number 2 • Complex Abdominal Wall Defects
505
the setting of contaminated wounds.10 However,free fascia lata grafts are only applicable for partial-thickness defects of the abdominal wall in whichadequate soft-tissue coverage is available. Compo-nent separation can be used for small to medium-sized midline defects when bilateral functionalrectus abdominis muscles are available. It has been
reported that advancements of up to 10, 16, and10 cm in the upper, middle, and lower abdomen,respectively, can be achieved with bilateralmobilizations.2 Large lateral defects generallyneed some form of flap coverage.
Local flaps such as the pedicled tensor fasciaelatae, anterolateral thigh, rectus femoris, rectusabdominis, and latissimus dorsi are useful andadequately address the reconstructive needs ofmost abdominal wall defects.12,13 Pedicled flapshave certain inherent limitations, such as re-stricted reach; tip necrosis (especially when ex-tended flaps are used); limited size of defects thatcan be covered (mainly small to medium-sizeddefects); and, except for the pedicled tensor fas-ciae latae flap, a strong fascial layer cannot beincorporated with the flaps, thereby necessitatingthe need for the use of alloplastic materials or asecond donor site for the harvest of the free fascialata graft. In this respect, free flaps have certaindistinct advantages over local flaps. Free flaps, bytheir nature, are not restricted by pedicle reach.When larger flaps are needed, adjacent flaps canbe harvested together in a conjoined manner.14–16
Sufficient tissue can be recruited to reconstructthe entire abdominal wall. The tensor fasciae lataeand the anterolateral thigh with or without thevastus lateralis muscle based in the lateral circum-flex femoral artery system are prime examples ofthis. Furthermore, free flaps import a large vol-ume of well-vascularized tissue into the abdomen,promote rapid healing, and are more resistant toinfections. A large amount of strong fascia can beharvested with the flap in the lateral thigh region.This fascia can be used for the reconstruction ofthe musculofascial layer of the abdomen, thereby
Fig. 7. Case 2. The margins of the hernia were delineated (ar-rows) and plicated.
Fig. 8. Thefunctioningtensorfasciaelataemyocutaneousflaphar-vested with its pedicle (arrow) and its nerve supply (arrowhead).
Fig. 9. Two interpositional vein grafts measuring 35 cm eachwere used from the femoral artery and vein to revascularize theflap.
Plastic and Reconstructive Surgery • August 2009
506
precluding the need to use alloplastic materials.Functional muscle transfer is also possible with theinclusion of the nerve supply to the muscle.17
Our indications for the use of free flaps inabdominal wall reconstruction include the follow-ing: (1) immunocompromised patients and pa-tients with previous failed reconstruction with al-loplastic materials resulting from infection orextrusion; (2) contaminated or infected woundsin which the use of totally autologous tissue ispreferred and the defects are more laterally lo-cated such that local flaps would be inadequate;and (3) patients with large midline defects pre-cluding the use of component separation or incases where the rectus abdominis and its fasciasheath are unavailable.
The lateral thigh is our “warehouse” donor sitefor a variety of reconstructive needs in abdominalwall reconstruction.18–20 The lateral circumflexfemoral system is versatile and allows the harvestof the tensor fasciae latae myocutaneous flap, an-terolateral thigh flap, or anteromedial thigh flapeither alone or in combination as conjoined flaps.An important advantage of the thigh is the pres-ence of the strong deep fascia in the lateral thigh,including the iliotibial tract and fascia lata that canbe used to reconstruct the musculofascial layer ofthe abdominal wall, thereby preventing postoper-ative hernia. This strong and tough deep fasciallayer is considered the ideal material for abdom-inal fascial restoration. In this respect, the tensorfasciae latae myocutaneous flap is preferred forsmaller defects, as this flap harnesses the strongest
part of the deep fascia, the iliotibial band. Moredistally and medially (i.e., in the territory of theanterolateral thigh flap), the deep fascia tends tobecome thinner and more attenuated.
Intraperitoneal or extraperitoneal recipientvessels can be used in abdominal free flaps. Theformer include the gastroepiploic vessels and thelatter include the superior epigastric vessels, infe-rior epigastric vessels, intercostal vessels, and su-perficial circumflex iliac vessels. When available,these vessels are reliable and can be safely used. Inour experience, the use of “extraabdominal” re-cipient vessels with the creation of a temporaryarteriovenous loop is often necessary for two rea-sons. First, the abdomen may be severely scarredand vessels damaged from placement of drainsand stomas so that they are unavailable for recon-struction. Second, the pedicle may be short. Thisis particularly so when conjoined flaps are raised.The inclusion of both the transverse and descend-ing branches of the lateral circumflex femoral ves-sels in the flap tethers the pedicle to the flap,resulting in a short “usable” pedicle. We thereforeprefer the use of a temporary arteriovenous looptechnique to reliably import extraabdominal re-cipient vessel into the abdominal wall. The greatersaphenous vein is conveniently located and highlyversatile for this purpose. It is easily accessible andcan be mobilized down to the level of the ankleand turned cephalad to achieve a venous pediclelength of up to 80 cm. We have found this to bea reliable and safe method of revascularizing theflaps. In addition, in cases where venous outflow
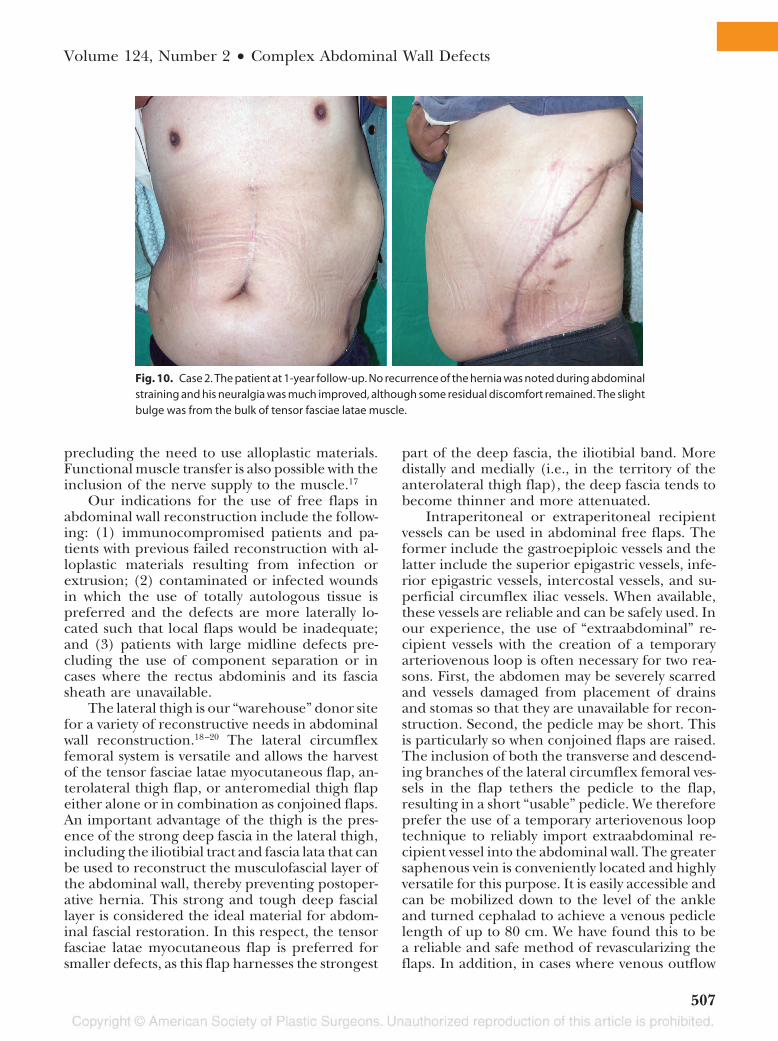
Fig. 10. Case 2. The patient at 1-year follow-up. No recurrence of the hernia was noted during abdominalstraining and his neuralgia was much improved, although some residual discomfort remained. The slightbulge was from the bulk of tensor fasciae latae muscle.
Volume 124, Number 2 • Complex Abdominal Wall Defects
507

is insufficient with a single venous anastomosis orthere is significant mismatch in vein sizes, thegreater saphenous vein can reliably be used toprovide additional venous outflow.
To prevent herniation, the fascia should besutured to healthy, innervated abdominal wall tis-sue. The fascia is inset using in an underlay tech-nique as described by McCarthy and Tweist, plac-ing the fascia in an intraperitoneal position.6 Careshould be taken to ensure even distribution oftension. The repair should be taut but not exces-sively tight. One rare but devastating and poten-tially fatal complication with closure of massiveabdominal defects with techniques that exert sig-nificant tension to recruit surrounding tissue suchas the component separation technique is abdom-inal compartment syndrome. An added advantageof flap repair in this regard is that, as additionaltissue is delivered to the abdominal wall, raisedintraabdominal pressures following repair istherefore much less likely. This is an importantconsideration for frail patients with poor respi-ratory reserves.
Abdominal wall transplantation is a subjectthat has been hotly debated recently. Currently, theonly place for this is probably in patients under-going intestinal autotransplantation with concom-itant abdominal wall defects that cannot be closedprimarily.20–22 There is currently no role for iso-lated abdominal wall transplantation, because ofthe side effects and risks of immunosuppression.Furthermore, as demonstrated by the cases pre-sented here, advancements in reconstructive tech-niques (in particular, the use of conjoined flaps)have enabled us to safely and reliably replace almostthe entire anterior abdominal wall when necessary.
CONCLUSIONSThe use of free flaps in abdominal wall recon-
struction provides an added dimension for recon-struction of complex abdominal wall defects. Theirversatility offers satisfactory solutions to problemswhere pedicle flaps are inadequate to completelyaddress the problem. With techniques availabletoday, the entire abdominal wall can be reliablyand safely reconstructed. The use of completelyautologous tissue in a single stage offers a definiteadvantage in immunocompromised patients, inwhom the incorporation of alloplastic materialsinto the reconstruction is associated with unac-ceptably high complication rates. The lateral thighregion based on the “dispensable” lateral circum-flex femoral system, has the potential to provide alarge amount of soft tissue and a large amount of
strong fascia. It is our first choice free flap donorsite for complex abdominal wall defects.
Chih-Hung Lin, M.D.Trauma Center
Department of Plastic Reconstructive SurgeryChang Gung Memorial Hospital
5, Fu-Hsing StreetKweishan, Taoyuan 33333, Taiwan
REFERENCES1. Rohrich RJ, Lowe JB, Hackney FL, Bowman JL, Hobar PC. An
algorithm for abdominal wall reconstruction. Plast ReconstrSurg. 2000;105:202–216.
2. Ramirez OM. Inception and evolution of the componentsseparation technique: Personal recollections. Clin Plast Surg.2006;33:241–246.
3. Rodriguez ED, Bluebond-Langner R, Silverman RP, et al.Abdominal wall reconstruction following severe loss of do-main: The R Adams Cowley Shock Trauma Center algorithm.Plast Reconstr Surg. 2007;120:669–680.
4. Mathes SJ, Steinwald PM, Foster RD, Hoffman WY, An-thony JP. Complex abdominal wall reconstruction: A com-parison of flap and mesh closure. Ann Surg. 2000;232:586–596.
5. Voyles CR, Richardson JD, Bland K, et al. Emergency ab-dominal wall reconstruction with polypropylene mesh: Shortterm benefits versus long term complications. Ann Surg.1981;194:219–223.
6. McCarthy JD, Tweist MW. Intraperitoneal polypropylenemesh support of incisional herniorrhaphy. Am J Surg. 1981;142:707–711.
7. Wong CH, Tan BK, Koong HN, Lim CH, Chia SJ, Song C. Useof the omentum flap as additional soft-tissue cover for ab-dominal wall defects reconstructed with Gore-Tex. Plast Re-constr Surg. 2005;116:1715–1720.
8. Brown GL, Richardson JD, Malangoni MA, et al. Comparisonof prosthetic materials for abdominal wall reconstruction inthe presence of contamination and infection. Ann Surg. 1985;201:705–711.
9. Lamb JP, Vitale T, Kaminski DL. Comparative evaluation ofsynthetic meshes used for abdominal wall replacement. Sur-gery 1983;93:643–648.
10. Disa JJ, Goldberg NH, Carlton JM, Robertson BC, Slezak S.Restoring abdominal wall integrity in contaminated tissue-deficient wounds using autologous fascia grafts. Plast ReconstrSurg. 1998;101:979–986.
11. Kirshtein B, Roy-Shapira A, Lantsberg L, Mizrahi S. Use ofthe “Bogota bag” for temporary abdominal closure in pa-tients with secondary peritonitis. Am Surg. 2007;73:249–252.
12. Williams JK, Carlson GW, Howell RL, Wagner JD, Nahai F,Coleman JJ. The tensor fasciae latae free flap in abdominal-wall reconstruction. J Reconstr Microsurg. 1997;13:83–90; dis-cussion 90–91.
13. Kimata Y, Uchiyama K, Sekido M, et al. Anterolateral thighflap for abdominal wall reconstruction. Plast Reconstr Surg.1999;103:1191–1197.
14. Kuo YR, Kuo MH, Lutz BS, et al. One-stage reconstruction oflarge midline abdominal wall defects using a composite freeanterolateral thigh flap with vascularized fascia lata. AnnSurg. 2004;239:352–358.
15. Sasaki K, Nozaki M, Nakazawa H, Kikuchi Y, Huang T. Recon-struction of a large abdominal wall defect using combined free
Plastic and Reconstructive Surgery • August 2009
508
tensor fasciae latae musculocutaneous flap and anterolateralthigh flap. Plast Reconstr Surg. 1998;102:2244–2252.
16. Dorai AA, Halim AS. Extended double pedicle free tensorfasciae latae myocutaneous flap for abdominal wall recon-struction. Singapore Med J. 2007;48:e141–e145.
17. Ninkovic M, Kronberger P, Harpf C, Rumer A, Anderl H.Free innervated latissimus dorsi muscle flap for reconstruc-tion of full-thickness abdominal wall defects. Plast ReconstrSurg. 1998;101:971–978.
18. Lin YT, Lin CH, Wei FC. More degrees of freedom by usingchimeric concept in the applications of anterolateral thighflap. J Plast Reconstr Aesthet Surg. 2006;59:622–627.
19. Lin CH, Wei FC, Lin YT, Yeh JT, Rodriguez Ede J, Chen CT.Lateral circumflex femoral artery system: Warehouse forfunctional composite free-tissue reconstruction of the lowerleg. J Trauma 2006;60:1032–1036.
20. Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH. Havewe found an ideal soft-tissue flap? An experience with 672 antero-lateral thigh flaps. Plast Reconstr Surg. 2002;109:2219–2226.
21. Levi D, Tzakis A, Kato T, et al. Transplantation of the ab-dominal wall. Lancet 2003;36:2173–2176.
22. Selvaggi G, Levi DM, Kato T, et al. Expanded use of transplan-tation techniques: Abdominal wall transplantation and intesti-nal autotransplantation. Transplant Proc. 2004;36:1561–1563.
Online CME CollectionsThis partial list of titles in the developing archive of CME article collections is available online atwww.PRSJournal.com. These articles are suitable to use as study guides for board certification, to help readers refamiliarizethemselves on a particular topic, or to serve as useful reference articles. Articles less than 3 years old can be taken for CMEcredit.
Reconstructive
Trunk
Donor-Site Morbidity Comparison between Endoscopically Assisted and Traditional Harvest of Free Latis-simus Dorsi Muscle Flap—Chih-Hung Lin et al.Reconstruction of a Severe Chest and Abdominal Wall Electrical Burn Injury in a Pediatric Patient—CraigMacKinnon et al.The Separation of Anatomic Components Technique for the Reconstruction of Massive Midline AbdominalWall Defects: Anatomy, Surgical Technique, Applications, and Limitations Revisited—Kenneth C. Shestaket al.Endoscopically Assisted “Components Separation” for Closure of Abdominal Wall Defects—James B. Loweet al.An Algorithm for Abdominal Wall Reconstruction—Rod J. Rohrich et al.The Surgical Treatment of Brachial Plexus Injuries in Adults—Julia K. Terzis and Vasileios K. KostopoulosPharmacologic Optimization of Microsurgery in the New Millennium—Matthew H. Conrad and William P.Adams, Jr.Risks Associated with “Components Separation” for Closure of Complex Abdominal Wall Defects—JamesB. Lowe, III, et al.The Surgical Treatment of Obstetric Brachial Plexus Palsy—Saleh M. Shenaq et al.Tissue Engineering: Progress and Challenges—Mark A. F. Knight and Gregory R. D. EvansFire in the Operating Room: Principles and Prevention—Stephen P. Daane and Bryant A. TothGender Identity Disorder: General Overview and Surgical Treatment for Vaginoplasty in Male-to-FemaleTranssexuals—Gennaro Selvaggi et al.Further Clarification of the Nomenclature for Compound Flaps—Geoffrey G. HallockBurn Injuries Inflicted on Children or the Elderly: A Framework for Clinical and Forensic Assessment—AdamR. Greenbaum et al.Management of Posterior Trunk Defects—David Mathes et al.Platelet-Rich Plasma: A Review of Biology and Applications in Plastic Surgery—Barry L. Eppley et al.Microvascular Surgery—Brandon C. D. Evans and Gregory R. D. EvansBasics of Immune Responses in Transplantation in Preparation for Application of Composite TissueAllografts in Plastic and Reconstructive Surgery: Part I—Maria Siemionow and Aleksandra KlimczakAcute Burns—Chia Chi Kao and Warren L. Garner
Volume 124, Number 2 • Complex Abdominal Wall Defects
509

![GSV Publications requiring copyright permission Publications requiring copyright permission: 4 GSV Library 929.2 CANE CAN 67. Canty, Wendy. All the shades of Gray. [Photocopy] GSV](https://img.dokumen.tips/doc/110x75/5aa7f75b7f8b9a54748cb5e9/gsv-publications-requiring-copyright-permission-publications-requiring-copyright.jpg)



























