Embed Size (px)
Citation preview

Laryngotracheal stenosis in children should be treated effectively with minimal delay, and the tracheostomy should be closed within a reasonable period after surgery so that the child may develop normal speech and lan- guage. Successful reconstruction of the laryngotracheal complex was achieved by applying the superiorly based compound myocutaneous ster- nocleidomastoid muscle flap for wedge enhancement and resurfacing of the endolaryngeal and endotracheal lumen. A short stenting period, incor- porating a custom-carved soft silicone laryngeal stent in direct continuity with an oversized silicone T-tube, helped in stabilizing the airway and en- suring good take of the flap. Postoperative recovery was relatively short, with good ventilation and vocal results. This single-stage technique may be readily performed, and it interferes minimally with the child’s development.
HEAD & NECK SURGERY 4:16-21 1981
RECONSTRUCTION OF THE LARYNGOTRACHEAL COMPLEX IN CHILDREN USING THE STERNOCLEIDOMASTOID MYOCUTANEOUS FLAP
1. ELIACHAR, MD, and A. R. MOSCONA, MD
T h e frequent application of mechanical ventila- tory support through either endotracheal intuba- tion or tracheostomy has increased the survival rate of critically ill patients, with a concomitant increase in the incidence of laryngeal and tracheal stenosis. This is notwithstanding various steps taken to counteract these potential hazards.
The laryngotracheal airway of infants and children is particularly susceptible to obstructive changes. Relatively mild pathologic changes, congenital or acquired, can result in critical nar- rowing of the airway. Laryngotracheal obstruc- tion in children may often necessitate emergency intubation or tracheostomy because of the rapid development of respiratory insufliciency . Long periods of tracheal intubation or tracheal cannu- lation are undesirable, being associated with various complications such as life-threatening respiratory tract infections and stenosis. Ex- tubation or decannulation may be difficult in babies and small children once an adequate air- way is established and may increase the risk of serious complications.
Once the diagnosis of laryngeal or tracheal stenosis is established, every effort should be made to overcome the problem so that prolonged tracheostomy may be avoided. Dilatations and corticosteroids, whether locally or systemically applied, are generally ineffective, and require weeks or months of treatment.
It is our policy to consider early surgical re- construction of the larynx and trachea to provide
a stable, adequate airway following a short post- operative recovery period. The proximity and mo- bility of the sternocleiodmastoid (SCM) muscle and its high vascularity render it suitable for laryngotracheal reconstruction. The bulk of the muscle in the anterior portion of the neck is not a problem because after transfer of the flap the muscle atrophies and fibrosis sets in, with a re- sulting reduction in the bulk of the muscle.
In this paper we present 2 cases of combined laryngeal and tracheal stenosis in pediatric pa- tients in whom the laryngotracheal complex was successfully reconstructed using a superiorly based SCM myocutaneous island flap.
AN ATOMV
The blood supply to the skin consists of 2 systems:
1. Segmental arteries which lie deep to the mus- cle and send out musculocutaneous perforating
From the Departments of Otolaryngology (Dr Eliachar) and Plastic and Reconstructive Surgery (Dr Moscona) Rambam Medical Center Technion-Faculty of Medicine. Haifa, Israel
Address reprint requests to Dr Eliachar at the ENT Department, Rambam Medical Center Haifa. Bat-Galim, Israel
Accepted for publication January 5. 1981
0148-6403/0401/0016 $01 25/0 1981 John Wiley & Sons. Inc
16 SCM Myocutaneous Flap in Children HEAD & NECK SURGERY Sep/Oct 1981

Figure 1 . Preoperative planning of laryngotracheal reconstruction using the sternocleidomastoid myocutaneous flap. The apron and the sternocleidomastoid myocutaneous island flaps are marked.
branches to supply the muscle and the overly- ing skin. This system comprises the predomi- nant blood supply to the skin.
2. Direct cutaneous arteries which lie above the muscle and supply the overlying skin only.
In several anatomic sites, dependence of the skin on the underlying muscle allows areas of skin and muscle to be elevated as a compound (myocutane- ous) flap.
The SCM muscle is supplied by 3 different vessels: the occipital artery in the upper portion, the superior thyroid artery in the middle portion, and a branch from the thyrocervical trunk in the lower portion. A muscle flap can be elevated and rotated safely on any one of these vascular pedi- cles (superiorly or inferiorly based).2
The skin overlying the SCM muscle is supplied in an axial fashion by the posterior au- ricular artery superiorly and by the transverse cervical artery inferiorly. Therefore, skin in the SCM region may be raised either on superiorly or on inferiorly based flaps. The latter can extend safely over the entire length of the SCM muscle, while in a superiorly based skin flap, the viability of the lower portion of the SCM is ~nre l i ab le .~ However, as the occipital, superior thyroid, and transverse cervical arteries are myocutaneous vessels, islands of skin attached to different sec- tions of the underlying SCM muscle can also be transferred safely. Clinical report^^,^ confirm that the compound myocutaneous flap enhances skin s ~ r v i v a l . ~
Figure 2. The apron flap is reflected upwards. The larynx and the upper tracheal rings are exposed for excision of the stenosed segment.
OPERATIVE TECHNIQUE
The site, extent, and severity of the airway stenosis are determined preoperatively using radiologic and endoscopic techniques. Anesthesia is administered with the patient in the supine po- sition, through a properly placed endotracheal tube or tracheostomy cannula. Skin incisions are carefully planned and marked (Fig. 1). An apron flap is elevated, exposing the larynx and trachea. The anterior wall of the thyroid and cricoid car- tilages with the upper tracheal rings are split open to expose the stenosed segment (Fig. 2). The thyroid and cricoid cartilage do not spring back after removal of the stent because we usually overextend the free alae of the cartilage after cre- ation of the laryngofissure to the extent of crack- ing the posterior plate of the cricoid ring, so that the cartilage is free from behind and readily ad- justs to a new position and angle. The cicatrix or tumor is carefully excised submucosally, using soft cloth pledgets soaked in 1:100,000 adrenaline in saline and wet-field diathermy to control bleed- ing. Cartilage is not resected unless it is dis- placed, deformed, or contributes in any way to the narrowing of the airway. The tracheostomy can- nula or the endotracheal tube is replaced by a slightly oversized Montgomery silicone T-tube (E. Benson Hood Inc., Duxbury, MA) topped by a custom-carved soft silicone laryngeal stent (Fig. 3). From this point on, anesthesia is administered through the T-tube.
SCM Myocutaneous Flap in Children HEAD & NECK SURGERY Sep/Oct 1981 17
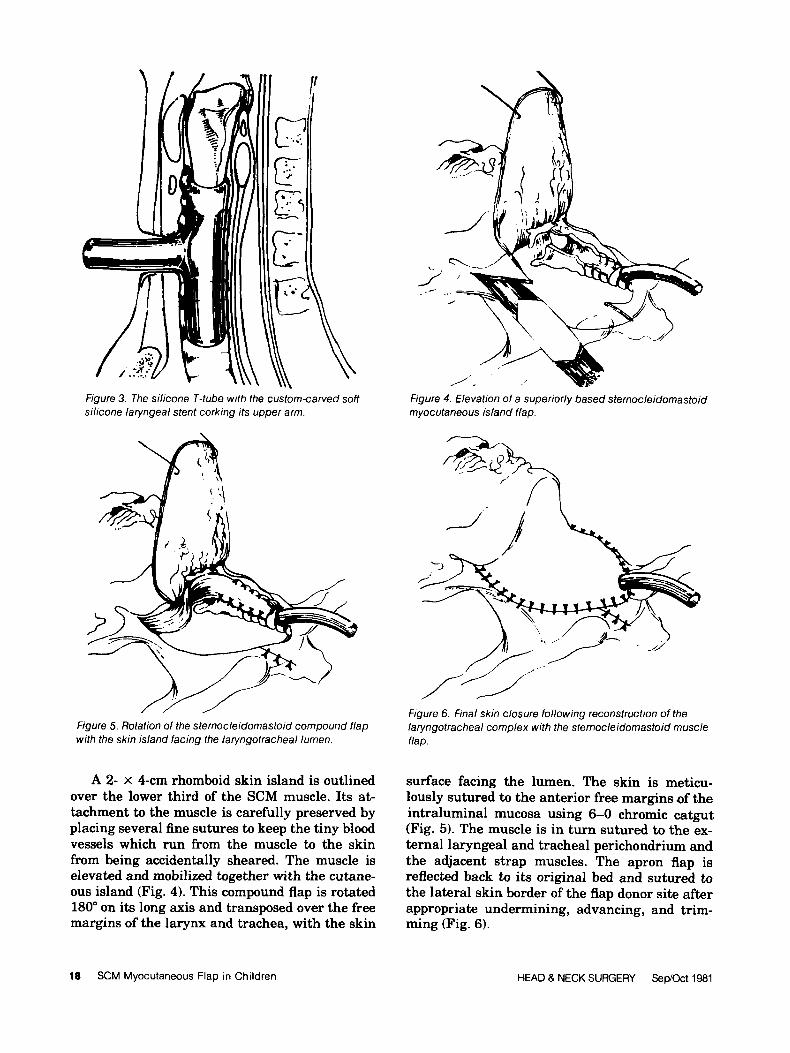
Figure 3. The silicone T-tube with the custom-carved soff silicone laryngeal stent corking its upper arm.
Figure 5. Rotation of the sternocleidomastoid compound flap with the skin island facing the laryngotracheal lumen.
A 2- x 4-cm rhomboid skin island is outlined over the lower third of the SCM muscle. Its at- tachment to the muscle is carefully preserved by placing several fine sutures to keep the tiny blood vessels which run from the muscle to the skin from being accidentally sheared. The muscle is elevated and mobilized together with the cutane- ous island (Fig. 4). This compound flap is rotated 180" on its long axis and transposed over the free margins of the larynx and trachea, with the skin
Figure 4. Elevation of a superiorly based sternocleidomastoid myocutaneous island flap.
Figure 6. Final skin closure following reconstruction of the laryngotracheal complex with the sternocleidomastoid muscle flap.
surface facing the lumen. The skin is meticu- lously sutured to the anterior free margins of the intraluminal mucosa using 6-0 chromic catgut (Fig. 5) . The muscle is in turn sutured to the ex- ternal laryngeal and tracheal perichondrium and the adjacent strap muscles. The apron flap is reflected back to its original bed and sutured to the lateral skin border of the flap donor site after appropriate undermining, advancing, and trim- ming (Fig. 6).
18 SCM Myocutaneous Flap in Children HEAD & NECK SURGERY SewOct 1981

Figure 7. Lateral x-ray of the neck in patient 1 demonstrating the tracheal T-tube, topped by the laryngeal stent.
POSTOPERATIVE CARE
Hemovacs are used for immediate postoperative drainage, and nasogastric tube feeding is pro- vided for 1 week following the procedure. The T-tube with its incorporated laryngeal stent re- mains in site for 4 to 6 weeks postoperatively. The laryngeal stent may then be pulled out endoscopi- cally and the T-tube may be removed shortly thereafter. The tracheostoma is allowed to heal spontaneously. Endoscopic and radiographic studies are performed as indicated by the recov- ery of the individual patient. Xeroradiography has been found most suitable for follow-up, be- cause of the fine resolution of cartilage and soft tissue obtained by this radiographic technique.
CASE REPORTS
patient I. A 7-year-old girl was admitted to the in- tensive care unit after sustaining a brain concus- sion in a road accident. She was unconscious for more than 10 days during which she received ven- tilation through a nasotracheal cuffed tube. After surgical evacuation of an infected subdural
hematoma, she gradually regained consciousness, and extubation was begun. Respiratory distress developed 3 days following withdrawal of the en- dotracheal tube. Direct laryngoscopy revealed web formation at the anterior commissure, ex- tending backwards upon the free margins of the true vocal cords. A 5-mm rigid bronchoscope was gently forced through the glottis, demonstrating severe segmental subglottic stenosis, extending down to the level of the second tracheal ring. A tracheostomy was performed over the broncho- scope. Reconstruction surgery was performed a week later. The granulation tissues and some of the extensive subglottic edematous tissues in the larynx and upper trachea were meticulously ex- cised, and the glottic web was separated. A silicone T-tube was inserted into the lower laryngeal and upper tracheal lumen with its hori- zontal arm extending out through the tracheos- toma. A soft silicone stent was adapted on the operating table to conform to the glottis and shaped into a cone to fit tightly into the upper wing of the silicone T-tube (Fig. 7). Ventilation and anesthesia were provided through the T-tube. A superiorly based SCM myocutaneous island flap was raised and rotated axially over the tracheal and laryngeal fissure to resurface the an- terior wall of the upper airway. The SCM muscle provided ample bulk and semirigid support. The laryngeal stent was endoscopically removed after 6 weeks. At that time the larynx was healed, stable, and completely resurfaced. The T-tube was removed and the tracheostoma was closed in the 10th postoperative week. The patient’s airway was adequate even during physical exertion (Fig. 8). Her voice was initially hoarse but within 6 months became clear. Endoscopy revealed func- tional mucosal folds acting as vocal cords extend- ing to the newly reconstructed cutaneous anterior commissure. The patient has been followed for more than 18 months.
Patknt 2. A 2-month-old baby girl was admitted to the intensive respiratory care unit with severe dyspnea. Nasotracheal intubations with assisted respiration were immediately provided. Difficulty in passing the endotracheal tube beyond the true vocal cords was noted. Attempts to extubate the child failed and bronchoscopy was performed, which revealed severe asymmetrical subglottic stenosis primarily on the anterior and right walls of the airway at the level of the cricoid ring. A low tracheostomy was performed over the broncho- scope. Ten days later, the stenosis was exposed by
SCM Myocutaneous Flap in Children HEAD & NECK SURGERY Sep/Oct 1981 19
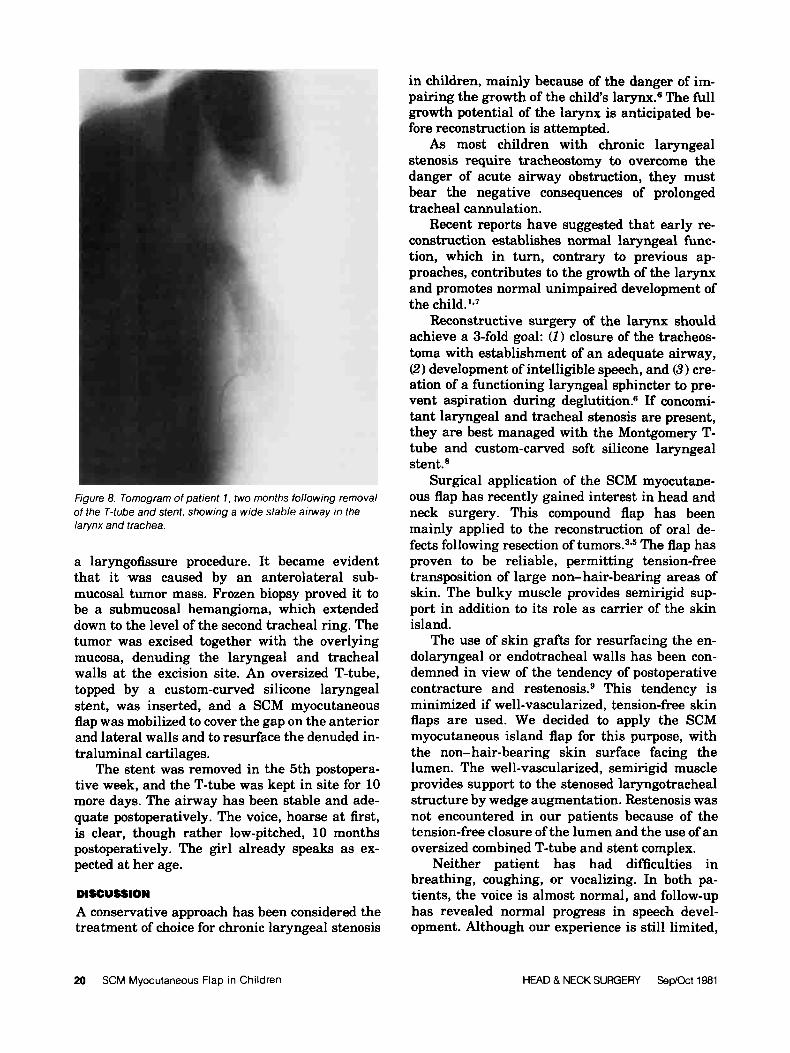
Figure 8. Tomogram of patient 1 , two months following removal of the T-tube and stent, showing a wide stable airway in the larynx and trachea.
a laryngofissure procedure. It became evident that it was caused by an anterolateral sub- mucosal tumor mass. Frozen biopsy proved it to be a submucosal hemangioma, which extended down to the level of the second tracheal ring. The tumor was excised together with the overlying mucosa, denuding the laryngeal and tracheal walls at the excision site. An oversized T-tube, topped by a custom-curved silicone laryngeal stent, was inserted, and a SCM myocutaneous flap was mobilized to cover the gap on the anterior and lateral walls and to resurface the denuded in- traluminal cartilages.
The stent was removed in the 5th postopera- tive week, and the T-tube was kept in site for 10 more days. The airway has been stable and ade- quate postoperatively. The voice, hoarse at first, is clear, though rather low-pitched, 10 months postoperatively. The girl already speaks as ex- pected at her age.
DISCUSSION A conservative approach has been considered the treatment of choice for chronic laryngeal stenosis
in children, mainly because of the danger of im- pairing the growth of the child's larynx.s The full growth potential of the larynx is anticipated be- fore reconstruction is attempted.
As most children with chronic laryngeal stenosis require tracheostomy to overcome the danger of acute airway obstruction, they must bear the negative consequences of prolonged tracheal cannulation.
Recent reports have suggested that early re- construction establishes normal laryngeal func- tion, which in turn, contrary to previous ap- proaches, contributes to the growth of the larynx and promotes normal unimpaired development of the child.'.'
Reconstructive surgery of the larynx should achieve a 3-fold goal: (I) closure of the tracheos- toma with establishment of an adequate airway, (2) development of intelligible speech, and (3) cre- ation of a functioning laryngeal sphincter to pre- vent aspiration during deglutition.6 If concomi- tant laryngeal and tracheal stenosis are present, they are best managed with the Montgomery T- tube and custom-carved soft silicone laryngeal stent.8
Surgical application of the SCM myocutane- ous flap has recently gained interest in head and neck surgery. This compound flap has been mainly applied to the reconstruction of oral de- fects following resection of t u r n ~ r s . ~ * ~ The flap has proven to be reliable, permitting tension-free transposition of large non- hair-bearing areas of skin. The bulky muscle provides semirigid sup- port in addition to its role as carrier of the skin island.
The use of skin grafts for resurfacing the en- dolaryngeal or endotracheal walls has been con- demned in view of the tendency of postoperative contracture and restenosi~.~ This tendency is minimized if well-vascularized, tension-free skin flaps are used. We decided to apply the SCM myocutaneous island flap for this purpose, with the non- hair-bearing skin surface facing the lumen. The well-vascularized, semirigid muscle provides support to the stenosed laryngotracheal structure by wedge augmentation. Restenosis was not encountered in our patients because of the tension-free closure of the lumen and the use of an oversized combined T-tube and stent complex.
Neither patient has had difficulties in breathing, coughing, or vocalizing. In both pa- tients, the voice is almost normal, and follow-up has revealed normal progress in speech devel- opment. Although our experience is still limited,
20 SCM Myocutaneous Flap in Children HEAD & NECK SURGERY Sep/Oct 1981

we found the technique easily adapted to pediat- ric laryngotracheal reconstruction.
Since the submission of this manuscript, 7 ad- ditional patients have undergone surgery in ac- cordance with the principles described. All pa- tients have recovered satisfactorily and now enjoy
a free airway. In addition, the technique has been used in 6 adults, in 4 of whom posterior stenotic lesions were excised as well as anterior ones. These lesions were resurfaced either with an ex- tension of the SCM skin graft or with a separate mucoperichondrial graft derived from the nose.
REFERENCES
1. Kushner DC, Clifton Harris G B Obstructing lesions of the larynx and trachea in infanta and children. Radio1 Clin North Am 16181-194,1978
2. Ariyan S One-stage reconstruction for defects of the mouth usine a sternomastoid mvocutaneous flaD. Plast Reconstr Sur;63:61&625,1979 "
3. Jabaley ME, Heckler ER, Wallace WH, Knott LH: Sterno- cleidomastoid regional flaps: a new look at an old concept. Br J P l a t Surg 32:106-113,1979
4. OBrien B: A muscle-skin pedical for total reconstruction of the lower lip. Plast Reconstr Surg 45395-398,1970
5. Sassaki C T The sternocleidomastoid myocutaneous flap. Arch Otolaryngol 106:74-76,1980
6. Skolnik EM, Tardy EM Jr: Laryngeal stenosis. Otolaryngol Clin North Am 3:56%580, 1970
7. Fearon B, Cotton R Surgical correction of subglottic stenosis of the larynx in infanta and children. Ann Otol Rhino1 Laryngol 83:428-430, 1974
8. Eliachar I, Goldsher M, Adler 0, Joachims HZ: Combined treatment of concurrent laryngeal & tracheal stenosis. J Laryngol Otol93:59-66,1979
9. Lore J Head and Neck Surgery, Vol. 2. WB Saunders, Philadelphia, PA, 1973. p 19
SCM Myocutaneous Flap in Children HEAD & NECK SURGERY Sep/Oct 1981 21