Embed Size (px)
Citation preview

* Correspond7318762.
E-mail addr
1748-6815/$-seedoi:10.1016/j.bj
Journal of Plastic, Reconstructive & Aesthetic Surgery (2008) 61, 195e199
CASE REPORT
Reconstruction of knee joint soft tissue andpatellar tendon defects using a compositeanterolateral thigh flap with vascularizedfascia lata
Yur-Ren Kuo a,*, Po-Chung An a, Mei-Hui Kuo b, Nai-Siong Kueh a,Sheng-Fa Yao a, Seng-Feng Jeng a
a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital,Kaohsiung Medical Center, Chang Gung University, College of Medicine,Kaohsiung 83305, Taiwanb Department of Rehabilitation and Physical Medicine, Chang Gung Memorial Hospital,Kaohsiung Medical Center, Chang Gung University, College of Medicine,Kaohsiung 83305, Taiwan
Received 9 February 2006; accepted 20 June 2006
KEYWORDSAnterolateral thighflap;Vascularized fascialata;Patellar tendon
ing author. 123 Ta-Pei
esses: t1207816@ms22
frontmatterª2006Britisps.2006.06.012
Summary Reconstruction of a complex knee trauma with knee joint exposureand composite soft tissue and patellar tendon deficiency remains a challengingtask. Multiple-stage reconstruction is time-consuming and produces considerablesuffering for patients. Early mobilization following knee reconstruction hasachieved good outcomes. Herein, we reported one-stage reconstruction with anALT myocutaneous flap with vascularized fascia lata was utilized for one patientwith a large complex knee joint soft tissue defect, and segmental deficiency ofthe patellar tendon. The fascia lata sheet was rolled to mimic a patellar tendon.The exposed knee joint was obturated by the vastus lateralis muscle of the ALTmyocutaneous flap. The skin and soft tissue defect was reconstructed usingthe skin paddle of the ALT flap. The patient’s postoperative course was unevent-ful. An MRI examination demonstrated good continuity of the reconstructedpatellar tendon. The active ROM of the injured knee reached 100� (extensiondeficiency 20� and flexion 120�) at 5 years. Objective functional assessment of
Road, Niao-Sung Hsiang, Kaohsiung Hsien, Taiwan. Tel.: þ886 7 7317123x8002; fax: þ886 7
.hinet.net, [email protected] (Y.-R. Kuo).
hAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.Allrightsreserved.

196 Y.-R. Kuo et al.
the patella-femoral joint utilized a kinetic communicator machine (Kin-Com 500H,Chattecx, Chattanooga, TN, USA) revealed still mild extension insufficiency. How-ever, the patient reported that he was able to perform normal daily activitieswithout difficulty at 5-year follow-up.ª 2006 British Association of Plastic, Reconstructive and Aesthetic Surgeons.Published by Elsevier Ltd. All rights reserved.
Reconstruction of a complex knee trauma withknee joint exposure and composite soft tissue andpatellar tendon deficiency remains a challengingtask. To prevent knee joint infection and promotewound healing, the soft tissue defect of theexposed knee joint is first conventionally covered.Then, the continuity of the extensor apparatus isrestored during the second stage. Options for flapreconstruction are local transposition muscleflaps,1e6 local fasciocutaneous flaps,7e9 and freemuscle flaps.10e13 Autogenous tendon grafts andallografts are options for re-establishing extensorapparatus continuity when a ligament defectexists.14,15 However, multiple-stage reconstructionis time-consuming and produces considerablesuffering for patients. Early mobilization followingknee reconstruction has achieved good out-comes. Consequently, one-stage reconstructionis preferred.1,4,5,10
In experience at Chang Gung Memorial Hospitalat Kaohsiung, the versatile anterolateral thigh(ALT) flap had been widely applied for reconstruc-tion of various soft tissue defects.16,17 An ALT flapwith vascularized fascia lata has been utilized toreconstruct the Achilles tendon and adjacent softtissue.18 The ALT flap with vascularized fascia latahas also been employed to reconstruct complicat-ed abdominal wall defects without peri-operativecomplications.19 Based on these experiences, anALT flap was utilized for one patient with a largecomplex knee soft tissue defect, knee joint expo-sure and segmental deficiency of the patellartendon. Reconstructed knee joint function wasassessed using a kinetic communicator machine(Kin-Com 500H, Chattecx, Chattanooga, TN, USA).
Figure 1 Right knee joint defects included segmentaldeficiency of the patellar tendon (6 cm in length) andsoft tissue defect (15� 10 cm).
Case report
A 65-year-old male sustained severe crushinginjury and patella fracture to his right knee ina work-related incident. The patellar open frac-ture was graded type IIIA using the classificationsystem developed by Gustilo et al. for openfractures.20,21 Open reconstruction of the patellarbone with tension band wiring was performedimmediately. Unfortunately, synovitis with severewound infection resulting in a septic knee
demonstrated postoperatively. Extensive synovec-tomy, sequestrectomy of the upper third of thepatella bone was preformed; tension band wireswere removed and overlying necrotic soft tissuewas trimmed. Following serial debridement, theexposed knee joint with patellar tendon deficiencyof 6 cm in length and a soft tissue defect15� 10 cm were observed (Fig. 1). One-stage re-construction with an ALT myocutaneous flap withvascularized fascia lata was performed. The ALTwas harvested as described previously.16e18 Theperforators were located via ultrasound Dopplerexamination. The pedicle from the descendingbranch of the lateral circumflex femoral artery(LCFA) was dissected between the septum ofthe rectus femoris and vastus lateralis muscle.A composite ALT myocutaneous flap measuring18� 12 cm with a 10� 6-cm vascularized fascialata sheet was harvested from the ipsilateral thigh(Fig. 2). The fascia lata sheet with sub-fascialplexus blood supply was rolled to mimic a patellartendon. The proximal section of fascia lata was

Figure 2 The flap design of the composite ALT myocu-taneous flap with a vascularized fascia lata. The skinpaddle measured 18� 12 cm and the vascularized fascialata was 10� 6 cm. The pedicle vessel was raised fromthe descending branch of lateral circumflex femoralartery (LCFA). ASIS: antero-superior iliac spine.
Anterolateral thigh flap and patellar tendon defect reconstruction 197
sutured to the patellar tendon remnant and at-tached to the tibial tuberosity; the distal sectionwas sutured to the patellar tendon remnant overthe residual patellar bone using 1/0 Ethibond(Ethicon, Cornelia, GA, USA). The knee joint waskept tense at its maximum extension during whilethe vascularized fascia lata was implanted. Theexposed knee joint was obturated by the vastuslateralis muscle of the ALT myocutaneous flap.The skin and soft tissue defect was reconstructedusing the skin paddle of the ALT flap. The pediclewas anastomosed end-to-end to the anterior tibialartery and its venae comitantes.
The patient’s postoperative course was un-eventful and the splint was removed at postoper-ative week 8. Physiotherapy was initiated withpassive and active range of motion (ROM) trainingand intensive leg muscle strengthening exercises.An MRI examination, which was performed duringthe sixth postoperative month, demonstrated goodcontinuity of the reconstructed patellar tendon(Fig. 3A). No maltracking of the patella was ob-served. The patient currently has mild limitation
in range of motion due to the patella alta at 12-month follow-up (Fig. 3B). Active movement ofthe patella extensor mechanism had extensor lagwith 20� deficiency; however, passive movementwas 10� extensor lag at 5-year follow-up. The ac-tive ROM of the injured knee reached 100� (exten-sion deficiency 20� and flexion 120�) at 5 years(Fig. 4A and B). Objective functional assessmentof the patella-femoral joint utilized a kinetic com-municator machine (Kin-Com 500H, Chattecx,Chattanooga, TN, USA) at postoperative month 6.The isometric power test at 30� knee flexion re-vealed a 24% deficit of the right injured knee com-pared with that of the contralateral normal knee.The isometric power test at 30� extension of thequadriceps indicated an 80% deficit. However,the patient could squat and climb steps withoutsupport. At 5-year follow-up, the patient reportedthat he was able to perform normal daily activitieswithout difficulty except scarring and mild exten-sion insufficiency (Fig. 4C).
Discussion
A complex soft tissue defect with knee jointexposure resulted from trauma, infection andcomplications of total knee arthroplasty.11e13 Tocover a soft tissue defect, a local muscle flap (gas-trocnemius muscle flap) or free muscle flaps (latis-simus dorsi muscle and rectus abdominis muscleflaps) have been applied to cover the exposedknee joint during the first stage of reconstruc-tion.1,2,5,12,13 Although these muscle flaps provideeffective obliteration of dead space, good vascu-larity for resisting wound infection, a thin skingraft is required. Scar contracture and poor dura-bility of skin graft are typical concerns. In thiscase, the complicated patellar tendon deficiencyand the exposed knee joint and extensor apparatusneeded to be covered and knee function restoredsimultaneously.
Conventionally, the patellar tendon is restoredusing an autogenous tendon graft (semitendinoustendon, gracilis tendon and fascia lata) or anallograft.14,15 However, delayedhealing, late failureand infection can occur when utilizing a non-vascularized tendon graft. Medial or lateral gastroc-nemius myotendinous flaps with Achilles tendongrafts achieved reported good healing and allowedfor early rehabilitation; however, residual donorleg function was frequently compromised.1,4,5
In this case, a composite ALT myocutaneous flapwith vascularized fascia lata was utilized success-fully for one-stage reconstruction. This compositeflap has durable skin, good vascularity of the
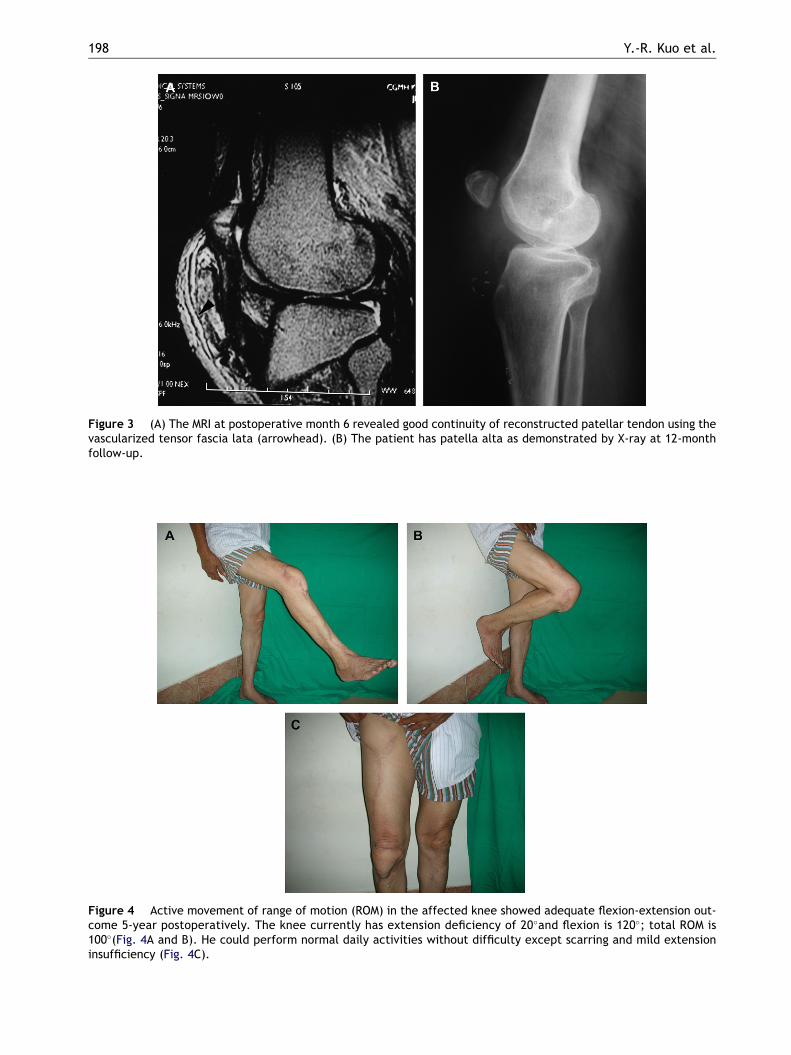
Figure 3 (A) The MRI at postoperative month 6 revealed good continuity of reconstructed patellar tendon using thevascularized tensor fascia lata (arrowhead). (B) The patient has patella alta as demonstrated by X-ray at 12-monthfollow-up.
Figure 4 Active movement of range of motion (ROM) in the affected knee showed adequate flexion-extension out-come 5-year postoperatively. The knee currently has extension deficiency of 20�and flexion is 120�; total ROM is100�(Fig. 4A and B). He could perform normal daily activities without difficulty except scarring and mild extensioninsufficiency (Fig. 4C).
198 Y.-R. Kuo et al.

Anterolateral thigh flap and patellar tendon defect reconstruction 199
vastus lateralis muscle and a well-vascularizedfascia lata. The skin island of ALT flap providesgood coverage without need for skin grafts. Thevastus lateralis muscle mimicked the local muscleflap in obliterating the knee synovium space andprevented wound infection. The vascularized fas-cia lata provided adequate tensile strength andthe good vascularity of the fascia effectivelyreplaced the deficiency of the patellar tendon.10,17
The functional assessment indicated that flex-ion strength of the reconstructed knee was 80% ofthat of normal knee. However, the reconstructedknee had 80% extension insufficiency. The patientcurrently has mild limitation in ROM during theknee flexion-extension cycle. This limited ROMindicates that this approach may not be a dynamicreconstruction, but rather function as an internalbrace against limited knee flexion. However, dur-ing kneeling, the patient was able to squat andstand up without support. The patient was able towalk and resume daily activities without difficulty.Although tension strength was unable to provide anextensor mechanism as strong as the originalpatella tendon, these outcomes indicated thatthe vascularized fascia lata is an alternative forpatellar tendon reconstruction.
In summary, composite ALT flap with vascular-ized fascia lata is a good option for one-stagereconstruction of complex knee joint soft tissueand patella tendon defect.
References
1. Rhomberg M, Schwabegger AH, Ninkovic M, et al. Gastroc-nemius myotendinous flap for patella or quadriceps tendonrepair, or both. Clin Orthop 2000;377:152e60.
2. Nahabedian M, Orlando JC, Delanois RE, et al. Salvageprocedures for complex soft tissue defect of the knee.Clin Orthop 1998;356:119e24.
3. Manushakian HS, McDiarmid JGM. Reconstruction of a largeanterolateral knee defect using a delayed distally basedtotal sartorius flap and a medial gastrocnemius flap. PlastReconstr Surg 1998;101:1065e9.
4. Chiou HM, Chang MC, Lo WH. One-stage reconstruction ofskin defect and patellar tendon rupture after total kneearthroplasty. J Arthroplasty 1997;12:575e9.
5. Leung KS, Yip KMH, Shen WY, et al. Reconstruction of exten-sor mechanism after trauma and infection by transposition
of the Achilles tendon: report of technique and four cases.J Orthop Trauma 1994;8:40e4.
6. Swartz WM, Ramasastry SS, McGill JR, et al. Distal basedvastus lateralis muscle flap for coverage of wounds aboutthe knee. Plast Reconstr Surg 1987;80:255e65.
7. Shaw AD, Ghosh SJ, Quaba AA. The island posterior calffasciocutaneous flap: an alternative to the gastrocnemiusmuscle for cover of knee and tibial defects. Plast ReconstrSurg 1998;101:1529e36.
8. Tsai CC, Lin SD, Lai CS, et al. Reconstruction of the upperleg and knee with a reversed flow saphenous island flapbased on the medial inferior genicular artery. Ann PlastSurg 1995;35:480e4.
9. Hayashi A, Maruyama Y. The lateral genicular artery flap.Ann Plast Surg 1990;24:310e7.
10. Yagi Y, Ueda M, Shirakabe M, et al. Reconstruction of kneeligaments with a free tensor fascia lata myocutaneous flaptransfer. Br J Plast Surg 2002;55:155e7.
11. Hallock GG. Utility of both muscle and fascia flaps in severelower extremity trauma. J Trauma 2000;48:913e7.
12. Yuen JC. Free-muscle-flap coverage of exposed knee jointsfollowing fulminant meningococcemia. Plast Reconstr Surg1997;99:880e4.
13. Yuen JC, Zhou AT. Free flap coverage for knee salvage. AnnPlast Surg 1996;37:158e66.
14. Zanotti RM, Freiberg AA, Matthews LS. Use of patellarrallograft to reconstruct a patellar tendon e deficient kneeafter total joint arthroplasty. J Arthroplasty 1995;10:271e4.
15. Cadambi A, Engh GA. Use of a semitendinous tendonautogenous graft for rupture of the patellar ligament aftertotal knee arthroplasty. J Bone Joint Surg 1992;74(A):974e9.
16. Kuo YR, Jeng SF, Kuo MH. Free anterolateral thigh flap forextremity reconstruction: clinical experience and functionalassessment of donor site. Plast Reconstr Surg 2001;107:1766e70.
17. Kuo YR, Jeng SF, Kuo MH. Versatility of the free anterolat-eral thigh flap for reconstruction of soft-tissue defect:review of 140 cases. Ann Plast Surg 2002;48:161e6.
18. Kuo YR, Kuo MH, Chou WC, et al. One-stage reconstructionof soft tissue and Achilles tendon defects using a compositefree anterolateral thigh flap with vascularized fascia lata:clinical experience and functional assessment. Ann PlastSurg 2003;50:149e55.
19. Kuo YR, Kuo MH, Lutz BS, et al. One-stage reconstruction oflarge midline abdominal wall defects using a composite freeanterolateral thigh flap with vascularized fascia lata. AnnSurg 2004;239:352e8.
20. Gustilo RB, Anderson JT. Prevention of infection in thetreatment of one thousand and twenty-five open fracturesof long bones: retrospective and prospective analyses.J Bone Joint Surg 1976;58A:453e8.
21. Gustilo RB, Mendoza RM, Williams DN. Problems in themanagement of type III (severe) open fractures: a newclassification of type III open fractures. J Trauma 1984;24:742e6.





























