Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) 62, 108e111
CASE REPORT
Reconstruction of an enterocutaneous fistula usinga superior gluteal artery perforator flap
M. Sakuraba a,*, T. Asano a, T. Yano a, S. Yamamoto b, Y. Moriya b
a Division of Plastic and Reconstructive Surgery, National Cancer Center Hospital East, Chiba, Japanb Division of Colorectal Surgery, National Cancer Center Hospital, Tokyo, Japan
Received 22 August 2006; accepted 11 September 2007
KEYWORDSEnterocutaneous fistula;Superior gluteal arteryperforator flap;Perforator flap;Colorectal cancer
* Corresponding author. Address: NaEast, Division of Plastic and Reconstrunoha Kashiwa-city, Chiba 277-8577, Jfax: þ81 471 31 4724.
E-mail address: [email protected]
1748-6815/$-seefrontmatterª2008Bridoi:10.1016/j.bjps.2007.09.009
Summary Enterocutaneous fistula is an uncommon complication of surgery for colorectalcancer. However, once a fistula has developed, treatment is complicated by previous treat-ments. Here, we describe an enterocutaneous fistula that developed after multiple treatmentsfor rectal cancer in a 62-year-old woman. The woman had previously undergone several colo-rectal surgeries, radiation therapy and five courses of chemotherapy. Four years after the finalsurgery, an enterocutaneous fistula developed between the small intestine and the sacral skin.The fistula was resected, and the resulting defect was successfully reconstructed with a supe-rior gluteal artery perforator flap.ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Else-vier Ltd. All rights reserved.
Case report
A 62-year-old woman presented with an enterocutaneousfistula that developed 4 years after ablative surgery forrecurrent rectal cancer. Her past medical history was asfollows: initial treatment for rectal cancer was carried outwith low anterior resection of the rectum in 1998. Eightmonths later, a Miles’ operation was carried out for re-current rectal cancer. However, the tumour recurred, and
tional Cancer Center Hospitalctive Surgery, 6-5-1 Kashiwa-apan. Tel.: þ81 471 33 1111;
c.go.jp (M. Sakuraba).
tishAssociationofPlastic,Reconstruc
additional treatments, including two additional surgeries,radiation therapy up to 40 Gy and five courses of chemother-apy, were carried out at another hospital. Finally, magneticresonance imaging showed a recurrent tumour at the ante-rior aspect of the sacrum, and the patient was transferred tothe division of colorectal surgery of our hospital in July2001. The final surgery for tumour ablation in August 2001included total pelvic exenteration and partial resection ofthe sacrum. The patient was free of tumour recurrencefor the next 4 years.
Discharge from an abscess of the skin over the sacrum wasobserved in April 2005. A fistulogram and a computed tomo-gram indicated the presence of an enterocutaneous fistulabetween the small intestine and the sacral skin (Figures 1,2).The distal opening of the fistula was pinhole-sized, and
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
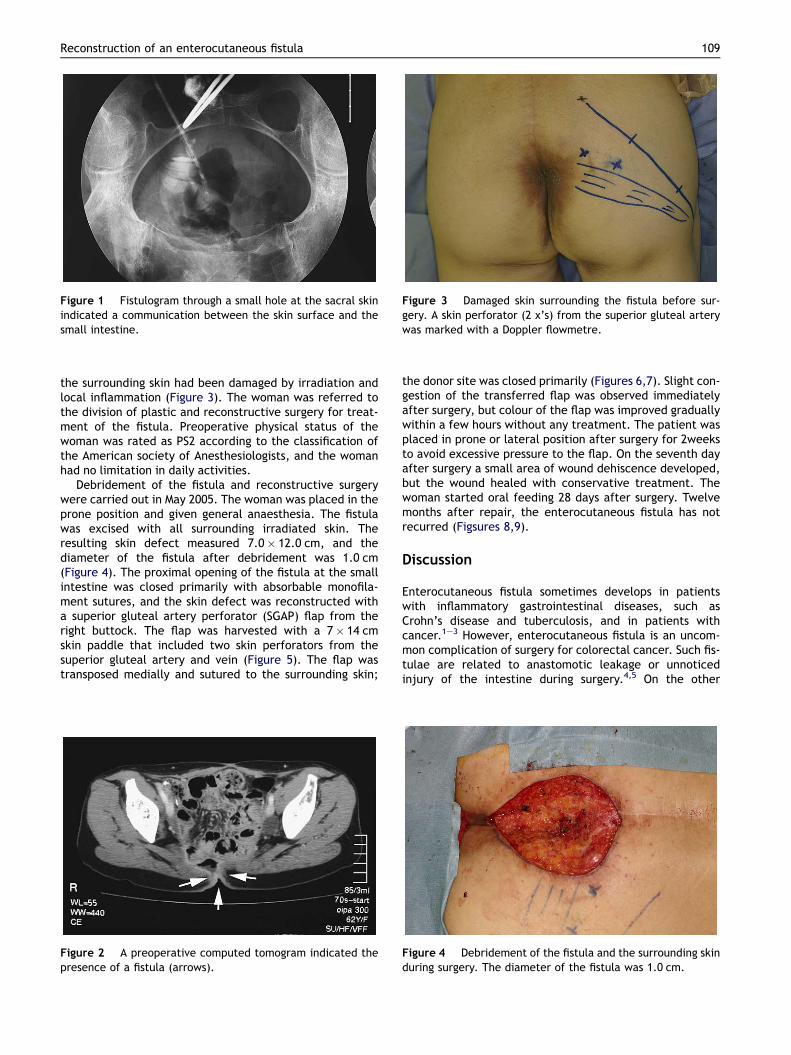
Figure 1 Fistulogram through a small hole at the sacral skinindicated a communication between the skin surface and thesmall intestine.
Figure 3 Damaged skin surrounding the fistula before sur-gery. A skin perforator (2 x’s) from the superior gluteal arterywas marked with a Doppler flowmetre.
Reconstruction of an enterocutaneous fistula 109
the surrounding skin had been damaged by irradiation andlocal inflammation (Figure 3). The woman was referred tothe division of plastic and reconstructive surgery for treat-ment of the fistula. Preoperative physical status of thewoman was rated as PS2 according to the classification ofthe American society of Anesthesiologists, and the womanhad no limitation in daily activities.
Debridement of the fistula and reconstructive surgerywere carried out in May 2005. The woman was placed in theprone position and given general anaesthesia. The fistulawas excised with all surrounding irradiated skin. Theresulting skin defect measured 7.0� 12.0 cm, and thediameter of the fistula after debridement was 1.0 cm(Figure 4). The proximal opening of the fistula at the smallintestine was closed primarily with absorbable monofila-ment sutures, and the skin defect was reconstructed witha superior gluteal artery perforator (SGAP) flap from theright buttock. The flap was harvested with a 7� 14 cmskin paddle that included two skin perforators from thesuperior gluteal artery and vein (Figure 5). The flap wastransposed medially and sutured to the surrounding skin;
Figure 2 A preoperative computed tomogram indicated thepresence of a fistula (arrows).
the donor site was closed primarily (Figures 6,7). Slight con-gestion of the transferred flap was observed immediatelyafter surgery, but colour of the flap was improved graduallywithin a few hours without any treatment. The patient wasplaced in prone or lateral position after surgery for 2weeksto avoid excessive pressure to the flap. On the seventh dayafter surgery a small area of wound dehiscence developed,but the wound healed with conservative treatment. Thewoman started oral feeding 28 days after surgery. Twelvemonths after repair, the enterocutaneous fistula has notrecurred (Figsures 8,9).
Discussion
Enterocutaneous fistula sometimes develops in patientswith inflammatory gastrointestinal diseases, such asCrohn’s disease and tuberculosis, and in patients withcancer.1e3 However, enterocutaneous fistula is an uncom-mon complication of surgery for colorectal cancer. Such fis-tulae are related to anastomotic leakage or unnoticedinjury of the intestine during surgery.4,5 On the other
Figure 4 Debridement of the fistula and the surrounding skinduring surgery. The diameter of the fistula was 1.0 cm.
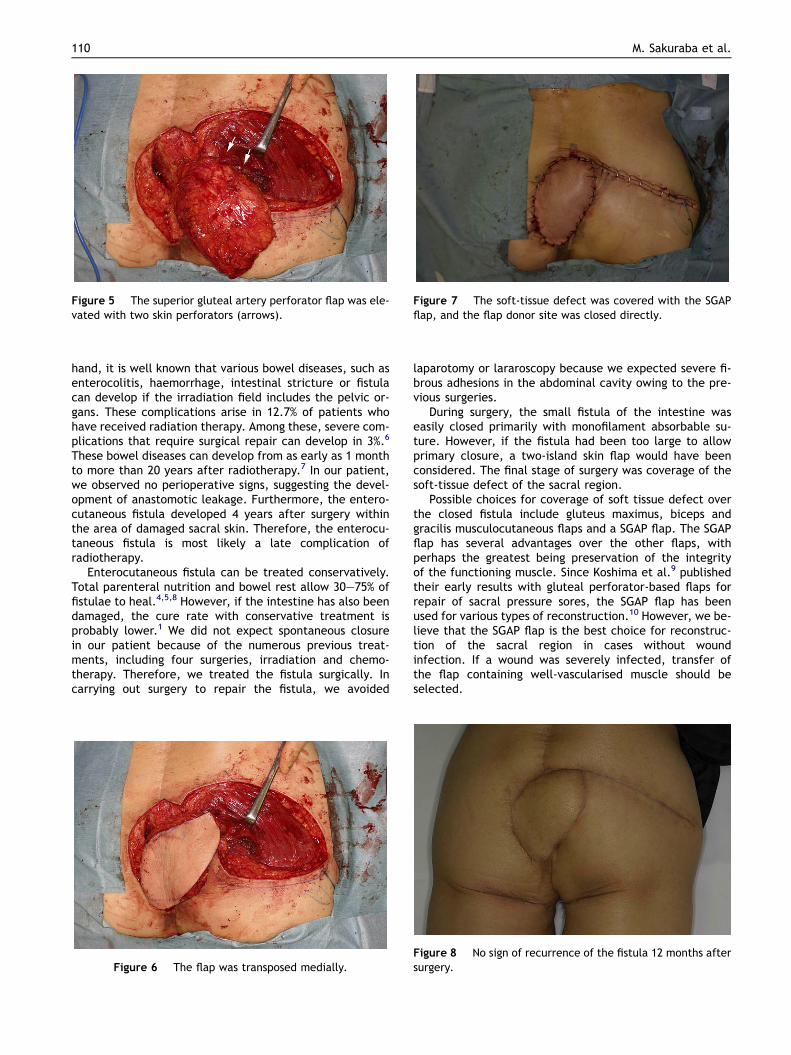
Figure 5 The superior gluteal artery perforator flap was ele-vated with two skin perforators (arrows).
Figure 7 The soft-tissue defect was covered with the SGAPflap, and the flap donor site was closed directly.
110 M. Sakuraba et al.
hand, it is well known that various bowel diseases, such asenterocolitis, haemorrhage, intestinal stricture or fistulacan develop if the irradiation field includes the pelvic or-gans. These complications arise in 12.7% of patients whohave received radiation therapy. Among these, severe com-plications that require surgical repair can develop in 3%.6
These bowel diseases can develop from as early as 1 monthto more than 20 years after radiotherapy.7 In our patient,we observed no perioperative signs, suggesting the devel-opment of anastomotic leakage. Furthermore, the entero-cutaneous fistula developed 4 years after surgery withinthe area of damaged sacral skin. Therefore, the enterocu-taneous fistula is most likely a late complication ofradiotherapy.
Enterocutaneous fistula can be treated conservatively.Total parenteral nutrition and bowel rest allow 30e75% offistulae to heal.4,5,8 However, if the intestine has also beendamaged, the cure rate with conservative treatment isprobably lower.1 We did not expect spontaneous closurein our patient because of the numerous previous treat-ments, including four surgeries, irradiation and chemo-therapy. Therefore, we treated the fistula surgically. Incarrying out surgery to repair the fistula, we avoided
Figure 6 The flap was transposed medially.
laparotomy or lararoscopy because we expected severe fi-brous adhesions in the abdominal cavity owing to the pre-vious surgeries.
During surgery, the small fistula of the intestine waseasily closed primarily with monofilament absorbable su-ture. However, if the fistula had been too large to allowprimary closure, a two-island skin flap would have beenconsidered. The final stage of surgery was coverage of thesoft-tissue defect of the sacral region.
Possible choices for coverage of soft tissue defect overthe closed fistula include gluteus maximus, biceps andgracilis musculocutaneous flaps and a SGAP flap. The SGAPflap has several advantages over the other flaps, withperhaps the greatest being preservation of the integrityof the functioning muscle. Since Koshima et al.9 publishedtheir early results with gluteal perforator-based flaps forrepair of sacral pressure sores, the SGAP flap has beenused for various types of reconstruction.10 However, we be-lieve that the SGAP flap is the best choice for reconstruc-tion of the sacral region in cases without woundinfection. If a wound was severely infected, transfer ofthe flap containing well-vascularised muscle should beselected.
Figure 8 No sign of recurrence of the fistula 12 months aftersurgery.

Figure 9 A computed tomogram shows successful coverageof the small intestine with sufficient flap volume.
Reconstruction of an enterocutaneous fistula 111
In conclusion, we report a rare case of enterocutaneousfistula developing after treatment of recurrent colorectalcancer. The enterocutaneous fistula was successfullytreated with an SGAP flap. The SGAP flap is a useful choicefor treatment of enterocutaneous fistulae of the sacralregion.
References
1. Poritz LS, Gagliano GA, McLeod RS, et al. Surgical managementof enter and colocutaneous fistulae in Crohn’s disease: 17year’s experience. Int J Colorectal Dis 2004;19:481e5.
2. Kaur N, Minocha VR. Review of hospital experience of entero-cutaneous fistula. Trop Gastroenterol 2000;21:197e200.
3. Chamberlain RS, Kaufman HL, Danforth DN. Enterocutaneousfistula in cancer patients: etiology, management, outcome,and impact on further treatment. Am Surg 1998;64:1204e11.
4. Tassiopoulos AK, Baum G, Halverson JD. Small bowel fistulas.Clin North Am 1996;76:1175e81.
5. Berry SM, Fisher JE. Enterocutaneous fistulas. Curr Probl Surg1994;31:474e566.
6. Bosh A, Frias Z. Complications after radiation therapy forcervical carcinoma. Acta Radiol 1977;16:53e62.
7. Schofield PF, Holden D, Carr ND. Bowel disease after radiother-apy. J R Soc Med 1983;76:463e6.
8. Sitges-Serra A, Jaurrieta E, Sitges-Creus A. Management ofpostoperative enterocutaneous fistulas: the roles of parenteralnutrition and surgery. Br J Surg 1982;69:147e50.
9. Koshima I, Moriguchi T, Soeda S, et al. The gluteal perforator-based flap for repair of sacral pressure sores. Plast ReconstrSurg 1993;91:678e83.
10. Blondeel P, Van Landuyt K, Hamdi M, et al. Soft tissue recon-struction with the superior gluteal artery perforator flap.Clin Plast Surg 2003;30:371e82.





























