Embed Size (px)
Citation preview

SKULL BASE SURGERY/NOLUME 5, NUMBER 2 APRIL 1995
TECHNICAL REPORT
Reconstructing Complex Cranial Defectswith a Preformed Cranial ProsthesisT.C. Origitano, M.D., Ph.D., Ricardo Izquierdo, M.D.,
and Louis B. Scannicchio, D.D.S.
The closure of cranial defects has a long and colorfulhistoryl-3: multiple autologous bone, metal, and polymer-based implants have been used. In the past, the impetusfor development has generally been injuries related towar. Today, an increase in the use and caliber of civilianweapons, the increased frequency of reoperation forpathologic intracranial processes (especially after radia-tion therapy), and the improved survival of patients withtraumatic head injuries provide new and more complexneeds for this procedure.
The goals of cranioplasty are to restore cosmeticaesthetics, protect the underlying brain, and restore intra-cranial pressure relationships. As the size and geometriccomplexity of the defect increases, the ability to meetthese goals decreases. The loss of overlying soft tissue(muscle) and contracture or skin necessary for closure are
often associated with large cranial defects. This can be ofspecial concern when old skin edges must be debrided.We have utilized a combined, staged approach to closecranial defects that are large and geometrically complex.
PATIENTS
Ten patients (six men and four women; ages 18 to 65years) with large cranial defects (mean, 105 cm2) were
treated with a combined staged cranioplasty of preformedpolymethyl methacrylate (Fig. 1; Table 1). Figure 2 showstypical preoperative patients presenting with large de-fects.
TECHNIQUE
Initially, the patient must be examined for construc-tion of a cranial prosthesis.48 Zero magnification x-rays
in both posteroanterior and lateral views are obtained toallow for accurate sizing and identification of bony irreg-ularities. A moulage of the defect is made with alginate.From this, a reverse model is made of hydrocal-105 stone,which serves as the working cast for the maxillofacial
109
Skull Base Surgery, Volume 5, Number 2, April 1995 Department of Neurological Surgery and Physiology (T.C.O.) and Division of Plastic Surgery(R.I.), Loyola University Medical Center, Maywood, Illinois, and Department of Oral and Maxillofacial Surgery (L.B.S.) Oak Park Hospital, OakPark, Illinois Reprint requests: Dr. Origitano, Department of Neurological Surgery, Loyola University Medical Center, 2160 South First Avenue,Maywood, IL 60153 Copyright © 1995 by Thieme Medical Publishers, Inc., 381 Park Avenue South, New York, NY 10016. All rights reserved.

SKULL BASE SURGERY/VOLUME 5, NUMBER 2
case 2
case 7 case 8
case 9 case 0
case 7 case 8
case 9 case 10Figure 1. Cranial defects.
Table 1. Complex Cranioplasty Cases
Case Sex Age Defect (cm2) Pathology*1 F 30 100 Post-operative osteomyelitis (redo craniotomy for meningioma)t2 M 37 105 Motorcycle trauma3 M 35 125 Recreational rocket injury4 M 45 75 Motor vehicle accident5 F 50 50 Post-operative osteomyelitis (cerebral aneurysm)6 M 22 1220 Gunshot wound7 F 65 95 Previous cranioplasty with intra-operative abscesst; (multiple reoperations for
recurrent meningioma)8 M 32 100 Post-radiation osteonecrosist (malignant astrocytoma)9 M 18 100 Gunshot wound1 0 F 56 60 Post-operative wound infectiont (cerebral aneurysm)
*Primary pathology resulting in bone loss0 Primary pathology for which (raniotomy perforrmecl
110 tReferred chronic defect > 1 year old
APRIL 1995
11
case 1

RECONSTRUCTING COMPLEX CRANIAL DEFECTS-ORIGITANO ET AL.
Figure 2. A: Preoperative defect, including the right frontal-parietal-temporal region and bilateral supraorbi-tal ridges (case 7). B: Preoperative defect, including the bifrontal region with severe skin contracture from loss ofvolume (case 3).
prosthodontist. A wax model is then constructed (Fig.3A). The wax imprint is tailored and contoured and thepatient has a final fitting. The methylmethacrylate pro-thesis is generated from the final stone cast (Fig. 3B) andthis is delivered to the operating room in a gas sterilizedpackage (Fig. 3C).
In 5 of the 10 patients, the skin available for closurewas deemed unsatisfactory and required cutaneous tissueexpansion before the cranioplasty. Indications for tissueexpansion included severe contracture associated withcutaneous changes induced by radiation, prolonged vol-ume loss (Fig. 2B), or large eschar at the suture linerequiring debridement to viable tissue. A Silastic subcuta-neous tissue expander4'9'10 (Fig. 4A) was placed undernormal tissues adjacent to the cranial defect over the boneand under the galea. The tissue expands over 4 to 6 weeks.Once each week, saline was injected into a remote portaccording to the patient's ability to tolerate pain. Thepatient was scheduled for definitive cranioplasty whentissue expansion was sufficient for closure (Fig. 4B to D).
The actual cranioplasty was straightforward. Thecranial incision was opened and the tissue expander re-moved. Any eschar was debrided if necessary, and theprothesis was laid in position. Final tailoring was doneaway from the operating table, thereby eliminating poten-
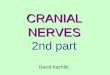
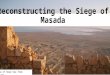
tial contamination at the implant site. The plate was ap-proximated with sutures, wire, or microplate. Our prefer-ence for the microplate is based on the rapid and rigidfixation of the prosthesis (Fig. 5). Surgical time was about1 hour per patient. Postoperatively, excellent cosmesiswas obtained (Fig. 6). No complications were encoun-tered with a mean follow-up of more than 1 year.
CONCLUSIONS
The use of a combined staged cranioplasty for pa-tients with large, geometrically complex defects allowsfor definitive, safe reconstruction that fulfills the goals ofcranioplasty. This technique is especially useful for pa-tients with anatomically complex defects in cosmeticallychallenging areas, such as the supraorbital rims, andwhere soft tissue defects lead to volume loss. The use ofsubcutaneous tissue expanders allows for adequate, via-ble, full-thickness skin closure, which is critical whencovering foreign bodies in previously injured, radiated, orinfected areas. Form-fitting the prothesis to the defectshortens the operating time. Processing the acrylic mou-lage before surgery eliminates the need to expose under-lying tissue (dura, brain) to the exothermic reaction and
B
111

SKULL BASE SURGERYNOLUME 5, NUMBER 2 APRIL 1995
A
B9
.~~~~~~~~~~~~~~~~~~Fgr 3. A:. Th wax pattr.~~~~~~~~~~~~~~~~~~~oe of potei. B: Th,ewa pat
B~~~~~~~~~~~~~~~~~~~mtarlt prothesis insere int
.~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~ ~h cast C: Th_opeedpohss
_g d
C._ ~ tion.
i_
__ . . ....
__ ~~~~~~~~~~~~~~~~~~Figure3. A: The wax pattern_ ~~~~~~~~~~~~~~~~~~~modelof prosthesis. B: The wax pat-
__ ~~~~~~~~~~~~~~~~~~ternprocessed in clear polymethyl
the cast. C: The complete prtessC _ ~~~~~~~~~~~~~~~~~~~~~~gas sterilIized, and ready for implanta-
112

RECONSTRUCTING COMPLEX CRANIAL DEFECTS-ORIGITANO ET AL.
A
Figure 4. A: The subcutaneous tissue expander. B,C: The tissue expander fully expanded in place (case 7).Note expander just behind the cranial defect. (Figure continued on the next page.)
C
113

SKULL BASE SURGERYNOLUME 5, NUMBER 2 APRIL 1995
Figure 4. (Continued). D: Case 3 with a fully ex-panded subcutaneous tissue expander. The remote injectionsite can be seen as a frontal bubble.
A
Figure 5. Prosthesis in place fixated with microplates: A: Case 7. (Figure continued on the next page.)
D
114
RECONSTRUCTING COMPLEX CRANIAL DEFECTS-ORIGITANO ET AL.
Figure 5. (Continued). B: case 3.
Figure 6. A: Early postoperative results (case 7). B: Late postoperative (1 year postoperative) results (case 3).B115

SKULL BASE SURGERYNOLUME 5, NUMBER 2 APRIL 1995
absorption of chemical radicals into surrounding soft tis-sue. Volumetric reconstruction of the cranial defect andoverlying soft tissue enhances the symmetry of the recon-struction, ensuring a cosmetically pleasing result.
REFERENCES
1. Delashaw JB, Persing JA: Cranial defects and their repair. InYoumans JR, ed: Neurological Surgery. Philadelphia: WB Saun-ders, 1990, pp 2290-2304
2. Prolo DJ: Cranial defects and cranioplasty. In Wilkins RH, Ren-gachary SS, eds: Neurosurgery. New York: McGraw-Hill, 1985,pp 1647-1656
3. Shaffrey ME, Persing JA, Shaffrey CI, Delashaw JB, Jane JA:
Craniofacial reconstruction. In Apuzzo MLJ, ed: Brain Sur-gery: Complication Avoidance and Management. New York:Churchill Livingstone, 1993, pp 1373-1398
4. Argenta LC: Controlled tissue expansion in reconstructive sur-gery. Br J Plast Surg 37:520-529, 1984
5. Blatt IM, Failla A: Acrylic implants for frontal bone defects. MilitMed 137:22-25, 1972
6. Cipcic JA: Silicone implant correction of facial deformities. Lar-yngoscope 78:565-585, 1968
7. Firtell DN, Beumer J III: Cranial and facial implants. In CullenJW, ed: Maxillofacial Rehabilitation. St. Louis: CV Mosby,1979, pp 372-397
8. Firtell DN, Moore DJ, Bartlett SO: A radiographic grid for con-touring cranial prostheses. J Prostet Dent 25:439-445, 1971
9. Radovan C: Tissue expansion in soft-tissue reconstruction. PlastReconstr Surg 74:482-490, 1984
10. Sasaki GH: Scalp repair by tissue expansion. In Brent B, ed: TheArtistry of Reconstructive Surgery: Selected Classic CaseStudies. St Louis: CV Mosby, 1987, pp 459-464
116
![Anterior Cranial Base Reconstruction with a Reverse ......346 Kwon SG et al. Cranial base reconstruction cranial base defects [1-5]. A variety of approaches have been used to cover](https://img.dokumen.tips/doc/110x75/6125c7c137a0983a040d4895/anterior-cranial-base-reconstruction-with-a-reverse-346-kwon-sg-et-al-cranial.jpg)