Embed Size (px)
Citation preview

Recent Advances: Gingival Retraction and Fluid Control
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):105-109 105
JDSORJDSOR
Recent Advances: Gingival Retraction and Fluid Control1Bhuwneshwer Pandey, 2MK Singhal, 3Chandna Nair, 4Farah Ahmed, 5Zainab Khan
ABSTRACT
Restoration and periodontium are correlated to each other. The biological width is reformed by them. The main factor to achieve the biological width is gingival retraction/displacement at the time of recording impression of area of finish lines in fixed partial denture prosthodontics. In view of this, a crevicular fluid control is also very essential. The current article discusses the evaluation of clinical techniques for gingival retraction and fluid control and its recent advances in the view of material sciences. Data are collected from journals, text book, and global internet. Expasyl retraction paste, Magic FoamCord, and Matrix impres-sion system are newer ones and give very good result. Among them, Expasyl retraction paste has good clinical property, and it give good result and is less expensive while impregnated cotton cord is least effective.
Keywords: Cotton cord, Expasyl retraction paste, Fluid control, Gingival retraction, Mereocel.
How to cite this article: Pandey B, Singhal MK, Nair C, Ahmed F, Khan Z. Recent Advances: Gingival Retraction and Fluid Control. J Dent Sci Oral Rehab 2016;7(3):105-109.
Source of support: Nil
Conflict of interest: None
INTRODUCTION
For restorations to survive for a long-term, the periodon-tium must remain healthy. This harmony between a res-toration and the periodontium that surrounds the tooth should be the ultimate aim of any fixed prosthodontic treatment. Key to achieve such a relationship depends on an accurately made impression.1 Displacement of the gingival tissue is essential for obtaining accurate impressions for the fabrication of fixed restorations, particularly while the finish line is at or just within the gingival sulcus and cervical lesions are present. Tissue management includes placing the gingival tissues away from the preparation margins; so they can record the impression combined with providing hemostasis when the gingival tissues are susceptible to bleeding. This
REVIEW ARTICLE
1,4,5Postgraduate Student, 2Professor and Head, 3Professor1-5Department of Prosthodontics, Institute of Dental Sciences Bareilly, Uttar Pradesh, India
Corresponding Authors: Bhuwneshwer Pandey, Postgraduate Student, Department of Prosthodontics, Institute of Dental Sciences Bareilly, Uttar Pradesh, India, e-mail: [email protected]
10.5005/jp-journals-10039-1121
displacement is known as gingival retraction or gingival displacement. Gingival displacement is defined as the deflection of the marginal gingiva away from the tooth. This is performed to create sufficient vertical and lateral space between the prepared finish line and the gingival tissue to allow the injection of adequate bulk of the impression material into the expended crevice. Impres-sion along the subgingival margin is critical toward the marginal fit and emergence profile of the prosthesis.2 Historically, MJ Thompson started gingival retraction in 1959 and in 1986 BW Benson et al have done it by chemicomechanical method. Today’s gingival retrac-tion procedures have been evolved newer techniques and materials. The rationales of gingival retraction are to provide adequate reproduction of finish lines, to accurately duplicate subgingival margins, to provide the best possible condition for the impression material and fluid control, and to fabricate accurate restorations thereby preventing periodontal diseases.3
Procedure for gingival retraction can be mechanical method, chemicomechanical method, surgical method (gingival curettage, surgical diathermy). Recent advances in gingival retraction and fluid control are the ones silicone-based materials.
CLINICAL PROCEDURES
Mechanical Method
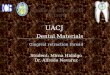
Among the gingival retraction methods, one of the method is mechanical method. In this method we do gingival retrac-tion either by-Rubber dam, copper tube or cotton cord (single-cord technique, double-cord technique) which may be depending on the configuration as twisted, knitted, plain, finished surfaced, waxed, unwaxed and chemical treatment, plain, or impregnated. Cotton cord comes in different thickness. According to the thickness or fineness we designate it as- 000(black), 00(yellow), 0(purple), 1(blue), 2(green), and 3(red), single-cord tech-nique is indicated when making impressions of one to three prepared teeth with healthy gingival tissues. It is relatively simple and efficient and is probably the most commonly used method of achieving gingival displace-ment.3 While making impression of multiple prepared teeth and tissue health is compromised, a double-cord technique is followed. In this procedure, a small-diameter cord is placed in sulcus. This cord is left in the sulcus during impression making. The second cord is (Fig. 1)
Bhuwneshwer Pandey et al
106
soaked with hemostatic agent of choice is placed in the sulcus above small-diameter cord. After waiting 8 to 10 minutes, the larger cord is removed and impression is recorded.3
MECHANICOCHEMICAL METHOD
Gel Cord (Fig. 2, 25% aluminum sulfate gel) and Stat Gel (Fig. 3, 15% ferric sulfate).
They aid in tissue retraction and hemostasis. Vasocon-strictors physiologically restricts the blood supply to the area by decreasing the size of the blood capillaries, tissue fluid seepage and consequently size of the free gingival, that is, epinephrine and norepinephrine.4
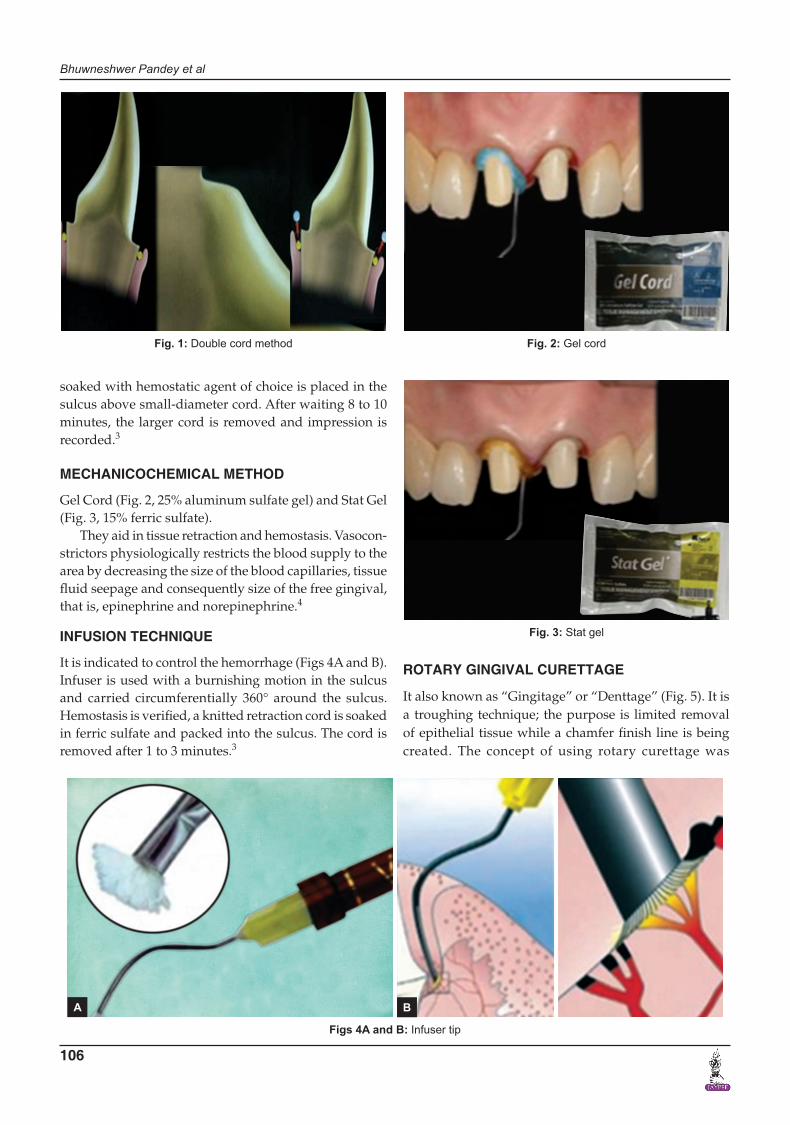
INFUSION TECHNIQUE
It is indicated to control the hemorrhage (Figs 4A and B). Infuser is used with a burnishing motion in the sulcus and carried circumferentially 360° around the sulcus. Hemostasis is verified, a knitted retraction cord is soaked in ferric sulfate and packed into the sulcus. The cord is removed after 1 to 3 minutes.3
Fig. 1: Double cord method Fig. 2: Gel cord
Fig. 3: Stat gel
Figs 4A and B: Infuser tip
ROTARY GINGIVAL CURETTAGE
It also known as “Gingitage” or “Denttage” (Fig. 5). It is a troughing technique; the purpose is limited removal of epithelial tissue while a chamfer finish line is being created. The concept of using rotary curettage was
A B

Recent Advances: Gingival Retraction and Fluid Control
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):105-109 107
JDSOR
described by Amsterdam in 1954. The technique was developed by Hansing and subsequently by Ingraham.5
ELECTROSURGERY UNIT
It is a high-frequency oscillator or radio transmitter that uses either a vacuum tube or a transistor to deliver a high-frequency electrical current at least 1.0 MHz (Fig. 6).5
LASERS
Lasers help in exposure of subgingival finish lines, con-trols the hemorrhage, and removes just enough epithelial attachment and periodontal ligament to facilitate the placement of retraction cord and minimum gingival reces-sion (Fig. 7). Laser tips are 400 to 600 micron in diameter. A featherlight stroke should be used. The laser handpiece should be kept moving. Along with the attached gingiva, approximately 1 mm of epithelial attachment should be removed and coagulated to achieve hemostasis and to expose the crown margins.6
Advantages
Minimum pain, inconvenience discomfort, less fear anxiety, minimum stress or no anesthesia, no drill sounds,
less chair time, reduced postoperative complications, minimum or no bleeding.
RECENT ADVANCES
Expasyl Retraction Paste
Noncord gingival retraction system (Fig. 8). Green- colored paste (combination of KAOLIN and 15% aluminum chloride) in glass cartridge (Figs 9A to D) is used to express
Fig. 5: Rotary curettage
Fig. 6: Electrosurgery unit with components Fig. 7: Gingival retraction with laser
Fig. 8: Expasyl-gingival retraction material

Bhuwneshwer Pandey et al
108
the paste through a disposable metal dispensing tip into the gingival sulcus prior to impression making or cemen-tation. This viscoelastic product is calculated to exert a stabilized pressure of 0.1 N/mm.2,7
Magic Foam Cord
Magic foam had been developed in a free partnership with Dr. Dumfahrt and is the first expanding polyvinyl siloxane material designed for easy and fast retraction of the sulcus without the potentially traumatic and time-consuming packing of the of retraction cord (Fig. 10). It is a nonhemo-static cordless retraction system and consists of foam and cartridges, mixing and intraoral tips, comprecaps (3 sizes).8
Merocel
New retraction strips have been proposed in dentistry to displace the gingival tissues prior to impression making
without damaging the tissues. The synthetic retraction material used is chemically extracted from a biocompat-ible polymer (hydroxyl polyvinyl polyacetate).8
Matrix Impression System
Gus J Livaditis9, in this system, is a matrix of polyether occlusal registration elastomeric material made over the tooth preparation.
DISCUSSION
Gingival retraction holds an indispensable place during soft tissue and fluid management before impression is made. Several problems that can arise from poor mar-ginal fit of fixed dental prostheses can be prevented if the margins of prepared tooth are recorded after adequate exposure by any of the gingival retraction methods.
Figs 9A to D: Clinical picture of gingival displacement, before and after use
Fig. 10: Magic FoamCord with comprecap
A
C
B
D

Recent Advances: Gingival Retraction and Fluid Control
Journal of Dental Sciences and Oral Rehabilitation, July-September 2016;7(3):105-109 109
JDSOR
Merocel is easily shaped and adapted around the tooth. It is highly effective in oral absorption of oral fluids and chemically pure and free from fragments, but it is time-consuming.8 Magic FoamCord is a nontraumatic, conser-vative method of temporary gingival retraction. It is easy and fast, applicable directly to the sulcus without pressure or packing, comfortable to the patient, and outstanding retraction for perfect impressions. Extensive rising is not required due to absence of hemostatic chemicals that could contaminate impression site; however, there is clinical indication, hemostasis cannot be achieved, rela-tively expensive compared to cord, and less effective on subgingival margins.8 Expasyl physically displaces the tissue for good marginal access, with minimum time and force needed compared with packing cord, and there is safe minimal pressure required and no danger of ruptur-ing the epithelial attachment.8 Swift increase in research work in the recent past leaves no option for a clinician, but to be updated and to possess optimum knowledge to rationalize the use of materials and techniques that are employed for gingival displacement in proximity to both teeth and implants.
Aforesaid discussed materials and techniques, the chemicomechanical technique (impregnated cotton cord) is least effective, time-consuming and more destructive to the gingival tissues. Sometime it causes necrosis of gingival tissues due to the presence of vasoconstrictors. Cord packing is least effective due to presence of saliva and patient uncooperation. This method does not even control the fluid.
CONCLUSION
Gingival retraction and fluid control play an indispens-able role in fixed partial denture fabrication. The choice of the technique and material depends on operator’s
judgment of the clinical situation apart from availability and cost of the materials. In view of material science, KAOLIN-based gingival retraction materials are good and provide ease of handling clinically.
ACKNOWLEDGMENTS
I acknowledge this article to my wife Dr Ankita Pandey and to my two small kids, Rishit and Rachit. I am also thankful to Dr Zainab Khan and Dr Farah Khan and, above all, to my respected head of department, Dr. MK Singhal, for his kind support and motivation.
REFERENCES
1. Padbury A Jr, Eber R, Wang HL. Interactions between the gingival and margin of the restoration. J Clin Periodontal 2003 May;30(5):379-385.
2. Al Hamad KQ, Azar WZ, Alwaeli HA, Said KN. A clinical study on the effects of cordless and conventional retraction techniques on the gingival and periodontal health. J Clin Periodontol 2008 Dec;35(12):1053-1058.
3. Donovan TE, Chee WW. Current concepts in gingival displace-ment. Dent Clin North Am 2004 Apr;48(2):433-444.
4. Benson BW, Bomberg TJ, Hatch RA, Hoffman W Jr. Tissue displacement methods in fixed prosthodontics. J Prosthet Dent 1986 Feb;55(2):175-181.
5. Shillingburg, HT. Jr.; Hobo, S.; Whitsett, LD.; Jacobi, R.; Brackett, SE. Fundamentals of fixed prosthodontics. 3rd ed. Quintessence Publishing; 1997. p. 269-275.
6. Rupali K, Sarandha DL, Gulab C. Advances in gingival retrac-tion. Int J Clin Dent Sci 2011;2(1):64-67.
7. Kazemi M, Memariam M, Loran V. Comparing the effective-ness of two gingival retraction procedures on gingival reces-sion and tissue displacement. Res J Biol Sci 2009;4(3):335-339.
8. Ferrari M, Cargidiaco M, Ercoli C. Tissue management with a new gingival retraction material. A preliminary clinical report. J Prosthet Dent 1996 Mar;75(3):242-247.
9. Livaditis G. Comparison of the new matrix system with tradi-tional fixed prosthodontic impression procedures. J Prosthet Dent 1998 Feb;79(2):248-253.