Embed Size (px)
Citation preview

RCCSURGERY IN METASTATIC DISEASE
Prof. Alessandro Volpe
University of Eastern Piedmont
Maggiore della Carità Hospital, Novara, Italy
DISCLOSURE OF INTEREST
None



• Tumour resection is curative only if all tumour
deposits are excised. This includes patients
with the primary tumour in place and single-
or oligo-metastatic resectable disease
• For most patients with metastatic disease,
cytoreductive nephrectomy (CN) is palliative
and systemic treatments are necessary

Evidence of a ‘stage shift’
• Sweden: from 23 % in 2005 to 15 % in 20101
• Germany: 17 % in 20131
• Netherlands: 18 % in 20111
• USA: 11 % in 20152 (National Cancer Database)
1 Thorstenson et al. Scand J Urol 2013, Report of Dutch Integral Cancer Centres 2013, RCC working group Germany,
SEER data USA 2 Patel et al,, Clinical stage migration and survival for RCC in the United States, Eur Urol Oncol 2018
Flanigan, Clin Cancer Res 2004: “Up to one third of patients with
renal cell carcinoma will present with metastatic disease”

15 years ago
just after SWOG 8949 and EORTC 30947
• N=94 with primary mRCC
• N=38 (40 %) considered irresectable
• N=36 (38 %) had a WHO ≥2
• N=20 (21 %) underwent CN
“ Only 1/5th fulfilled criteria for CN”
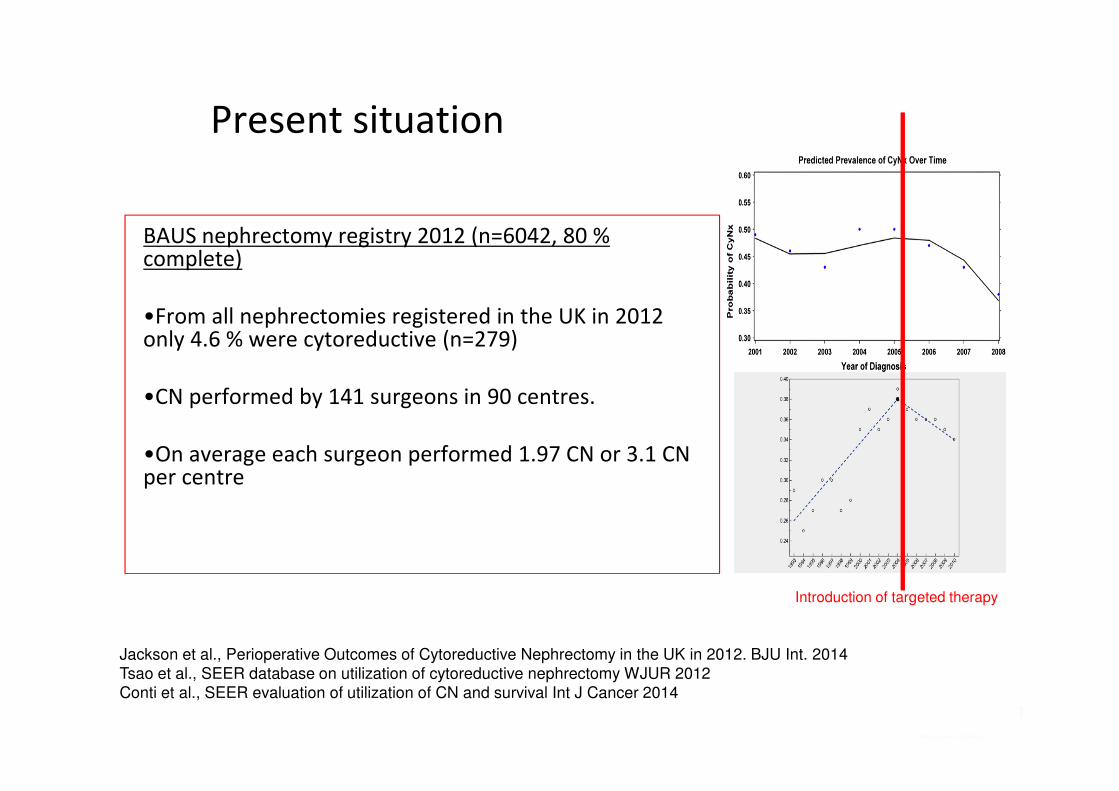
Present situation
BAUS nephrectomy registry 2012 (n=6042, 80 % complete)
•From all nephrectomies registered in the UK in 2012 only 4.6 % were cytoreductive (n=279)
•CN performed by 141 surgeons in 90 centres.
•On average each surgeon performed 1.97 CN or 3.1 CN per centre
Jackson et al., Perioperative Outcomes of Cytoreductive Nephrectomy in the UK in 2012. BJU Int. 2014
Tsao et al., SEER database on utilization of cytoreductive nephrectomy WJUR 2012
Conti et al., SEER evaluation of utilization of CN and survival Int J Cancer 2014
Introduction of targeted therapy

Morbidity of CN
• Individual prediction of 30-day mortality after partial or radical
nephrectomy according to age and stage strata (n=12,283)
T1-2N0M0
% 30 day mortality
(95%CI)
T3-4N0-2M0
% 30 day mortality
(95%CI)
T1-4N0-2M1
% 30 day mortality
(95%CI)
Age (years)
≤49 0.1 (0–0.4) 0.6 (0.1–1.9) 2.9 (1.2–5.9)
50–59 0.1 (0–0.5) 0.6 (0.2–1.8) 2.9 (1.4–5.6)
60–69 0.2 (0.05–0.5) 0.8 (0.3–1.6) 3.6 (2.0–6.3)
70–79 0.4 (0.1–0.7) 1.5 (0.7–2.6) 7.0 (4.0–11.0)
≥80 0.6 (0.1–1.5) 2.4 (0.8–4.9) 10.5 (4.3–23.0)
Cloutier, et al. Eur Urol 2008

4 months
20 %
SWOG trial of nephrectomy plus interferon
versus interferon alone
20 % of patients who underwent
surgery died within the first 4 months !
Figure from: Flanigan et al., Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for
metastatic renal-cell cancer. NEJM 345(23):1655-1659, 2001

• Multi-Institutional retrospective analysis of 141
patients after CN
• Systemic therapy 70% (98/141)
• No Systemic therapy due to* 15 % (20/141)
(*rapid progression & perioperative death)
Kutikov et al, Use of systemic therapy and factors affecting survival for patients undergoing
cytoreductive nephrectomy. BJUI 106(2):218-223, 2010.

Retrospective studies published until 2016 on survival
after CN versus no CN
Bex et al., Eur Urol 70: 901-905, 2016
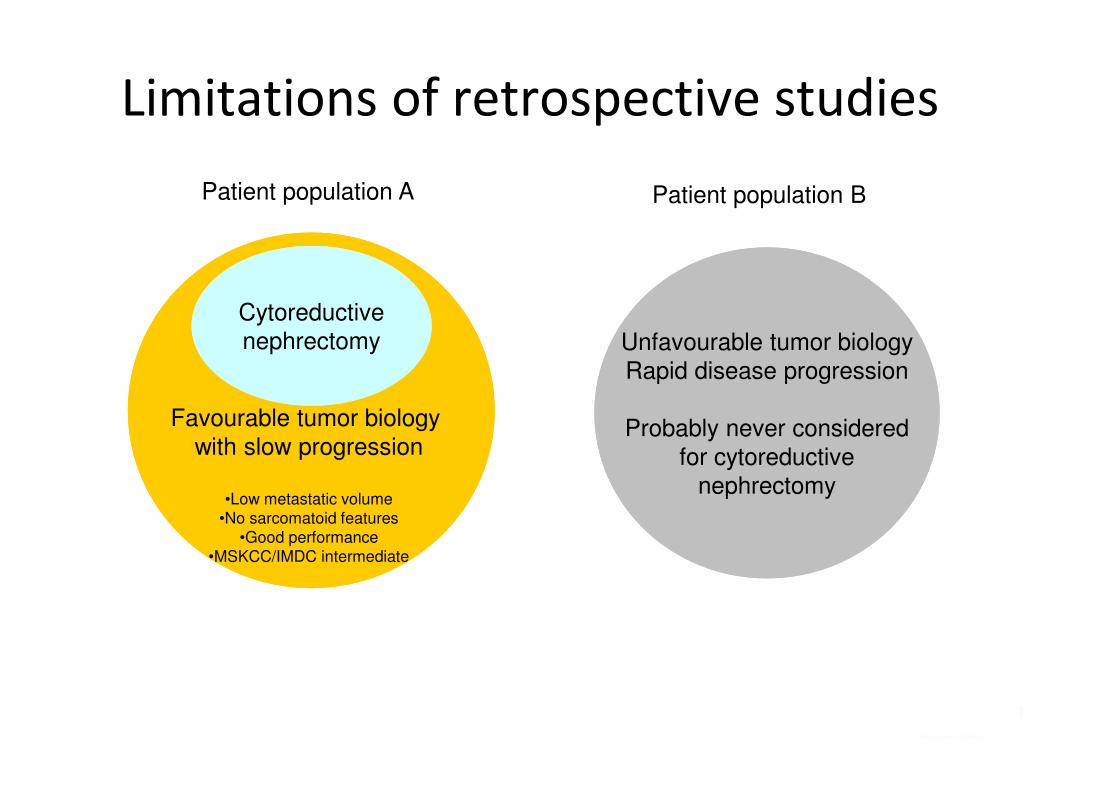
Limitations of retrospective studies
Unfavourable tumor biology
Rapid disease progression
Probably never considered
for cytoreductive
nephrectomy
Cytoreductive
nephrectomy
Favourable tumor biology
with slow progression
•Low metastatic volume
•No sarcomatoid features
•Good performance
•MSKCC/IMDC intermediate
Patient population A Patient population B
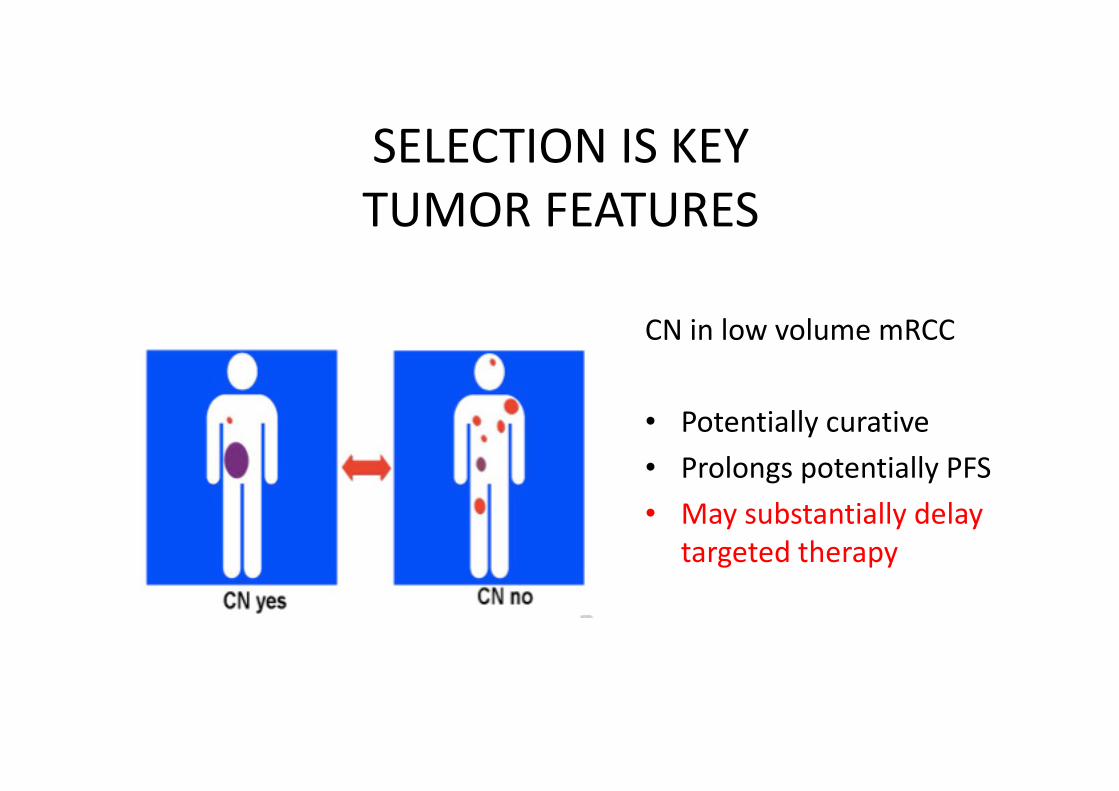
SELECTION IS KEY
TUMOR FEATURES
CN in low volume mRCC
• Potentially curative
• Prolongs potentially PFS
• May substantially delay
targeted therapy
ECOG Performance status
• A preoperative ECOG status ≥ 2 was the only
significant risk factor associated with failure to
undergo cytoreductive nephrectomy followed by
immunotherapy (P = 0.043).
Walther et al., Cytoreductive surgery prior to IL-2 based therapy in patients with mRCC. Urology 42(3):250-7, 1993
SELECTION IS KEYPATIENT FEATURES

Heng et al., External validation and comparison of the IMDC prognostic model with other models
The Lancet Oncology 14 (2)141-8, 2013
Individual factors• Karnofsky performance < 80 %• anemia• thrombocytosis• neutrophilia• hypercalcemia• time from diagnosis to treatment < 1 year
SELECTION IS KEYVALIDATED PROGNOSTIC SCORES

No survival benefit in poor risk patients
Noe et al., J Clin Oncol 31, 2013 (suppl; abstr e15525)
2-year OS:
Intermediate:
25.5% (95% CI 18-34%)
Poor:
2.9% (95 % CI 0.05-14%)
Courtesy Dr Daniel Heng, presented at ASCO GU 2014
Pretreatment MSKCC IMDC in primary mRCC (n=1658)
(n=154 patients at the NKI)
Median OS
- intermediate risk:
17 months (95% CI 11.3-22.6)
- poor risk:
6 months (95% CI 3.4-8.5)

Estimate life expectancy
Adequate life expectancy turnspotential significance into relevance
Courtesy Dr Daniel Heng, presented at ASCO GU 2014

SURTIME, a EORTC-GU 30073 Phase III Study
Investigating the Sequence of Nephrectomy and Sunitinib
� Primary end point: PFS
� Secondary end points: OS, association with prognostic gene
and protein expression profiles
Nephrectomy
Sunitinib
50 mg/day
(schedule 4/2)
Nephrectomy
Sunitinib
50 mg/day
(schedule 4/2)
Patients with
synchronous
mRCC and
primary tumor
in situ
RANDOMIZATION
N = 458
Biswas et al, 2009; US NIH, 2010d.

esmo.org
IMMEDIATE VERSUS DEFERRED CYTOREDUCTIVENEPHRECTOMY IN PATIENTS WITH SYNCHRONOUS
METASTATIC RENAL CELL CARCINOMA (MRCC) RECEIVING SUNITINIB.
The European Organization for Research and Treatment of Cancer (EORTC) randomized trial 30073 SURTIME.
A. Bex*, P. Mulders, M. Jewett, J. Wagstaff, R. Van Velthoven, P. Laguna, L. Wood, H.H.E. van Melick, P. Soetekouw,
J.B. Lattouf, T. Powles, I. De Jong, S. Rottey, B. Tombal, S. Marreaud, S. Collette, L. Collette, J. Haanen
*The Netherlands Cancer Institute, Amsterdam, The Netherlands, on behalf of the EORTC Genitourinary Cancer Group
Clinical trial identification NCT01099423

OBJECTIVE / ENDPOINTS / SAMPLE SIZE (2)
• Due to poor accrual (64 patients after 3 years recruitment), a revised statistical design had been submitted before the end of accrual to the Independent Data Monitoring Committee (IDMC) and approved the following changes:
• Primary endpoint: Progression-free rate (PFR) at 28 weeks, using RECIST v1.1
• Sample size: Based on the PFR at 7 months (28 weeks) in the sunitinib arm in the pivotal trial comparing sunitinib and interferon-alpha, in which 90% of the patients had a nephrectomy1, a PFR at 28 weeks of 70% was assumed for the immediate arm in trial 30073. To show an increase in the PFR at 28 weeks from 70% in the immediate arm to 90% in the deferred arm (H0: no difference versus H1: increase of 20% in the PFR), based on a one sided Fisher Exact test at 5% with 80% power in the intention-to-treat population, 98 patients were needed.
1Motzer et al.,N Engl J Med 2007; 356: 115-124.
21

STUDY DESIGN
Progression status at week 16
Progression status at week 28
NEPHRECTOMY
NEPHRECTOMY
Cycle 1 (6 wk) Cycle 2 Cycle 3 Cycle 4
NEPHRECTOMY
NEPHRECTOMY
Progression
status every
12 weeks
Cycle 4 Cycle 5Cycle 1 (6 wk) Cycle 2 Cycle 3 (4 wk)
R
Immediate Nephrectomy
DeferredNephrectomy
22
= Progression status 4 weeks after CN
= Sunitinib

RECRUITMENTRandomized patients
N=99
Immediate surgery
N=50
Deferred SurgeryN=49
NephrectomyN=46
NephrectomyN=34
Pre-surgical sunitinibN=48
Postop sunitinib N=40
Postop sunitinib N=26
Allocated treatment not started (n=1)
Allocated treatment not started (n=4)
No postop sunitinib (n=8)
No postop sunitinib (n=6)
Treatment stopped (n=22)Treatment ongoing (n=4)
Treatment stopped (n=34)Treatment ongoing (n=6)
No Surgery (n=8)Surgery off protocol (n=6)
10 not eligible 8 not eligible
23
• From 14/07/2010 to 24/03/2016 (ie 5.7 years):
• 99 patients randomized
• by 19 institutions
• from 4 countries (the Netherlands, Canada, United Kingdom, Belgium).
• As of May 5, 2017, median follow-up is 3.3 years (95% CI: 2.8, 3.8).

ADVERSE EVENTS AND SAFETY (1)
24
Immediatenephrecto
my(N=46)
Deferrednephrecto
my(N=48)
Number of patients with AE’s*
- grade ≥1 45 (97.8%) 48 (100.0%)
- grade ≥3 24 (52.2%) 28 (57.3%)
Number of patients with SAE’s
17 (37.0%) 17 (35.4%)
Number of SAE’s 32 24
*ALL adverse events, recorded according to CTCAE, version 4.0SAE were reported according ICH GCP and the EU Directive 2001/20/EC definition and requirements $ arterial embolization due to hematuria
Safety of pre-surgical sunitinib
Deferrednephrect
omy(N=48)
Delay of nephrectomy > 2 weeks- Logistical reasons- Treatment unrelated comorbidity- Sunitinib related
8 (16.6%)5 (10.4%)1 (2.0%)2 (4.2%)
Inability to perform surgery due to progression of primary tumour
-
Emergency intervention duringpretreatment$
1

25
SAFETY (2) - SURGICAL ADVERSE EVENTS
Immediatenephrecto
my
Deferrednephrecto
my$
Type of surgical complication:
- In-hospital mortality 2* 1
- Number of patients with prolongation of hospitalization (>20days) and/or readmission (within 30 days after
surgery)
6 3
- Number of patients (events) with intraoperative complication (including
vascular and organ damage# and
blood-loss grade 3)
• Grade ≥3
• Grade 5
14 (23)
8 (11)
1 (1)
9 (11)
6 (6)
-
- Number of patients with postoperative adverse events within 30 days after surgery#
• Grade ≥3
• Grade 5
7
1
7
1
$median days after sunitinib 4.5 (range 1.0-63.0), *1 death during surgery; # grade 3 or more according to CTCAE, version 4.0 and judged by physicians as likely related to surgery

PROGRESSION-FREE SURVIVAL - INTENTION TO TREAT -
Progression-free status at w 28 (±15 days)
Immediate
nephrectomy
(N=50)
Deferrednephrect
omy(N=49)
Progression-free at week 28
21 (42.0%)
21 (42.9%)
[95% CI][28.2% –
56.8%]
[28.8% –
57.8%]
p-value (Fisher exact test) >0.99
Progression before or at week 28, or treatment failure
25 (50.0%)
24 (49.0%)
Not assessable 4 (8.0%) 4 (8.2%)
26
Deferred
Immediate
HR [95% CI]: 0.88 [0.59-1.37]P=0.569 stratified by PS 0 vs 1

OVERALL SURVIVAL - INTENTION TO TREAT-
Immediate
nephrectomy
(N=50)
Deferrednephrect
omy(N=49)
Survival status
Dead 35 (70.0) 28 (57.1)
Reason of death
Progression 30 25Surgery related toxicity 1 0Progression and surgery
related toxicity 1 0
Cardiovascular disease (not due to toxicity or progression)
1 0
Other (not due to toxicity or progression)
1 0
Unknown 1 327
Deferred
Immediate
HR [95% CI]: 0.57 [0.34-0.95]P=0.032 stratified by PS 0 vs 1

PROGRESSION-FREE SURVIVAL AND OVERALL SURVIVAL- PER PROTOCOL -
28
Per protocol population: All patients who are eligible and have started their allocated treatment (excluding 18 ineligible patients and 5 who did not proceed to allocated treatment).
Deferred
Immediate
HR [95% CI]: 0.99 [0.60-1.62]P=0.965 stratified by PS 0 vs 1
Deferred
Immediate
HR [95% CI]: 0.71 [0.40-1.24]P=0.225 stratified by PS 0 vs 1

CONCLUSIONS
29
• The trial accrued poorly and therefore results are mainly exploratory.
• The sequence of CN and sunitinib did not affect the PFR at 28 weeks.
• The sample size precludes definitive conclusions from other endpoints, although an OS signal
was seen for deferred CN.
• The survival in the deferred arm is comparable to data reported from previous single-arm
phase II studies of presurgical sunitinib or pazopanib 1-3.
• The deferred CN approach appears to select out patients with inherent resistance to systemic
therapy. This confirms previous findings from single-arm phase II studies1-3.
• The deferred CN approach initiates therapy quickly, does not lead to inability to perform CN
and surgery appears safe after sunitinib.
1Powles et al., JAMA Oncol 2016, 10:1303-130; 2Powles et al., Eur Urol 2011, 60:448-5 ; 3Bex et al., Urology2011, 78:832-7

2018 Version

CARMENA Phase III Study of Sunitinib Only vs.
Nephrectomy Followed by Sunitinib
� Primary objective: Is sunitinib alone non-inferior to nephrectomy plus sunitinib in terms of OS?
� Note: NO stratification in MSKCC or IMDC risk
Nephrectomy
Sunitinib
50 mg/day
(schedule 4/2)
Sunitinib
50 mg/day
(schedule 4/2)
R
A
N
D
O
M
I
Z
A
T
I
O
N
N = 576
Metastatic
clear cell RCC
ECOG 0-1

Patient characteristics (1)
Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

Overall <br />survival (ITT)
Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

Overall survival (ITT)
Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

Secondary nephrectomy in Arm B (sunitinib alone)
Presented By Arnaud Mejean at 2018 ASCO Annual Meeting
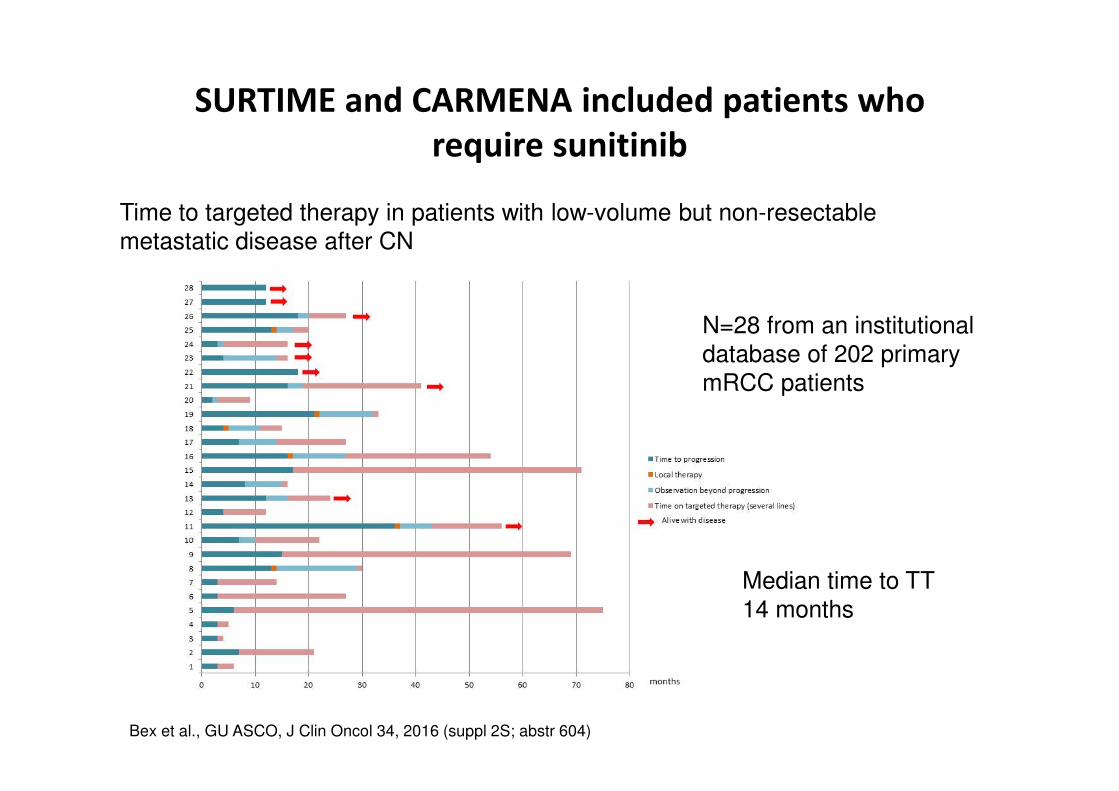
SURTIME and CARMENA included patients who
require sunitinib
N=28 from an institutional
database of 202 primary
mRCC patients
Bex et al., GU ASCO, J Clin Oncol 34, 2016 (suppl 2S; abstr 604)
Median time to TT
14 months
Time to targeted therapy in patients with low-volume but non-resectable
metastatic disease after CN




Which are the current indications for cytoreductive
nephrectomy?

Role of surgery for metastases

Does CN have a future ?
• VEGFR-TKI
Indication Frequency Rationale
Patients with solitary or
oligometastasis not requiring
immediate systemic therapy
low
(in NKI dataset 40/244 =16.4 %)
• Cure
• Delay of systemic therapy
Intermediate risk patients
without systemic progression
during immediate TKI
probably 80 % of intermediate
risk pts who constitute 60 %
of RCC risk groups
• Identification of long-term
survivors
• Potentially longer OS
Courtesy of Dr. A. Bex
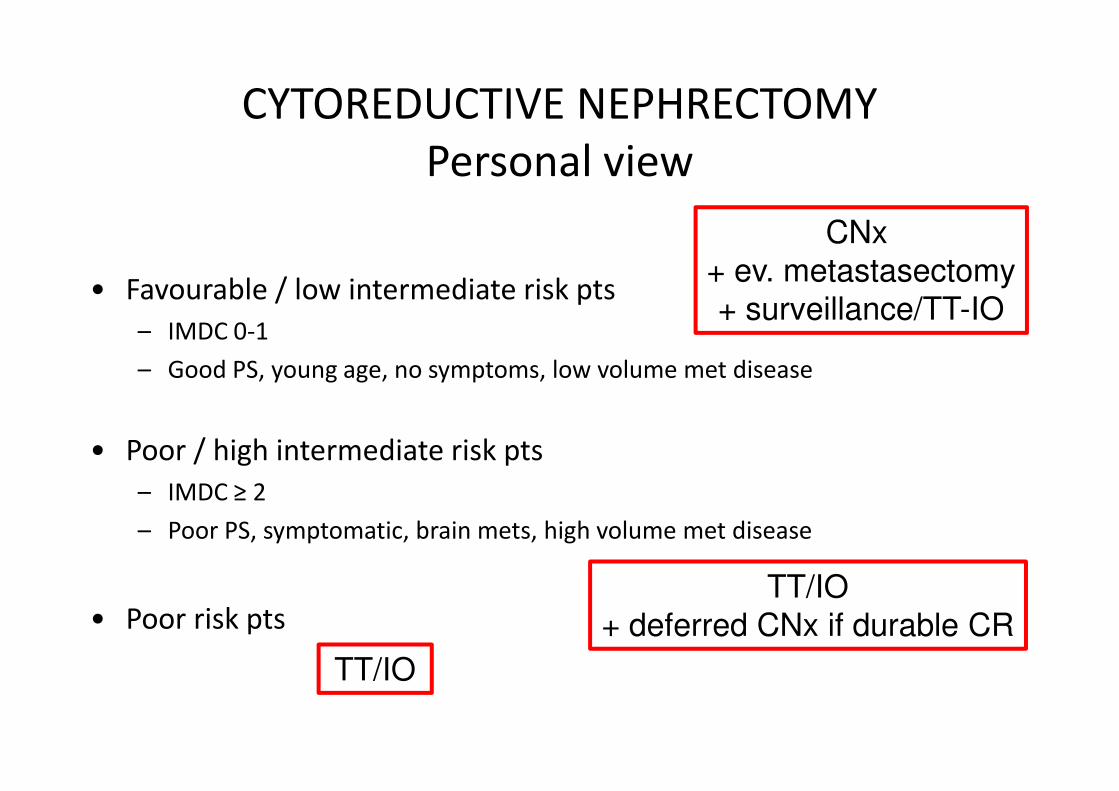
CYTOREDUCTIVE NEPHRECTOMY
Personal view
• Favourable / low intermediate risk pts
– IMDC 0-1
– Good PS, young age, no symptoms, low volume met disease
• Poor / high intermediate risk pts
– IMDC ≥ 2
– Poor PS, symptomatic, brain mets, high volume met disease
• Poor risk pts
CNx
+ ev. metastasectomy
+ surveillance/TT-IO
TT/IO
+ deferred CNx if durable CR
TT/IO



Does CN have a future ?
• Immunotherapy
Scenario Rationale of CN Probability
CR of primary and
metastases
CN not required unlikely
CR at metastatic sites only CN advised in all instances:
•to stop treatment
•potentially curative
May occur in a few cases
SD or PR but median OS
substantially longer than in
VEGFR-TT era with 10-20%
‘cured’
CN may be of benefit:
•in case of symptoms
•potentially curative
likely
CR=complete remission; PR=partial remission; SD=stable disease; OS=overall survival; TT=targeted therapy
Courtesy of Dr. A. Bex

� Primary objective: Is IO + X alone superior to nephrectomy plus IO +
X or IO + X plus nephrectomy in terms of OS?
� Stratification by IMDC risk factors
Nephrectomy
IO + X
IO + X
R
A
N
D
O
M
I
Z
A
T
I
O
N
N = 1500 + each new arm
Metastatic
clear cell RCC
ECOG 0-1
IO + X Nephrectomy
Courtesy of Dr. A. Bex

CONCLUSIONS
• Primary mRCC is heterogenous and selection is key
• Immediate and deferred cytoreductive nephrectomy
after systemic treatment is safe and effective in selected
cases
• Systemic therapy is the maynstay of therapy for the
majority of patients
• Patients with poor/intermediate prognosis are best
treated primarily with targeted agents/IO
• Stratification of intermediate risk category is warranted
• Further RCTs on cytoreductive nephrectomy + TT/IO are
awaited





























