Embed Size (px)
Citation preview

Rational Physician Coding for E/M Consult Services
Peter R. Jensen, MD, CPC www.EMuniversity.com

Peter R. Jensen, MD, CPC
For clinically driven E/M coding education, go to www.EMuniversity.com
Rational Physician Coding for E/M Consult
Services
Goals
Know the definition of a consultLearn the documentation requirements for consult servicesUnderstand how to identify the highest ethical level of careStreamline your documentation to save timeMaintain the focus on patient care
1

What is a Consult?
Occurs at the request of a physician or qualified NPP Asks another physician or qualified NPP for advice about the evaluation and treatment of a patientConsultant has expertise in a specific medical area beyond the requesting professional’s knowledge
The Three “R”s
There must be a documented REQUESTThere must be a clearly identifiable REASONThere must be formally documented REPORT
2

Types of Consults
Inpatient ConsultsOutpatient ConsultsConfirmatory ConsultsFollow-up Consults
Outpatient Consults
3 out of 3 key components must qualify
80HighCompComp99245
60ModCompComp99244
40LowDetailedDetailed99243
30SFEPFEPF99242
15PFPFPF99241TimeMDMExamHistoryE/M Code
3

Office patientsUse the outpatient consult codes for hospital patients who are not inpatients– Observation patients– ER consultsSubsequent visits are reported using the codes for established office patients (99211 – 99215)
Outpatient Consults
Inpatient Consults
3 out of 3 key components must qualify
110HighCompComp99255
80ModCompComp99254
55LowDetailedDetailed99253
40SFEPFEPF99252
20SFPFPF99251TimeMDMExamHistoryE/M Code
4

Hospital inpatientsResidents of nursing facilitiesInpatient consults can be reported only once per consultant per patient per facility admissionSubsequent care is reported using the codes for hospital progress notes (99231 – 99233)
Inpatient Consults
Inpatient Consults12.5 million encounters1.6 billion5.6% E/M spending
Outpatient Consults
Outpatient vs. Inpatient
13.1 million encounters$1.9 billion6.7% E/M spending
5
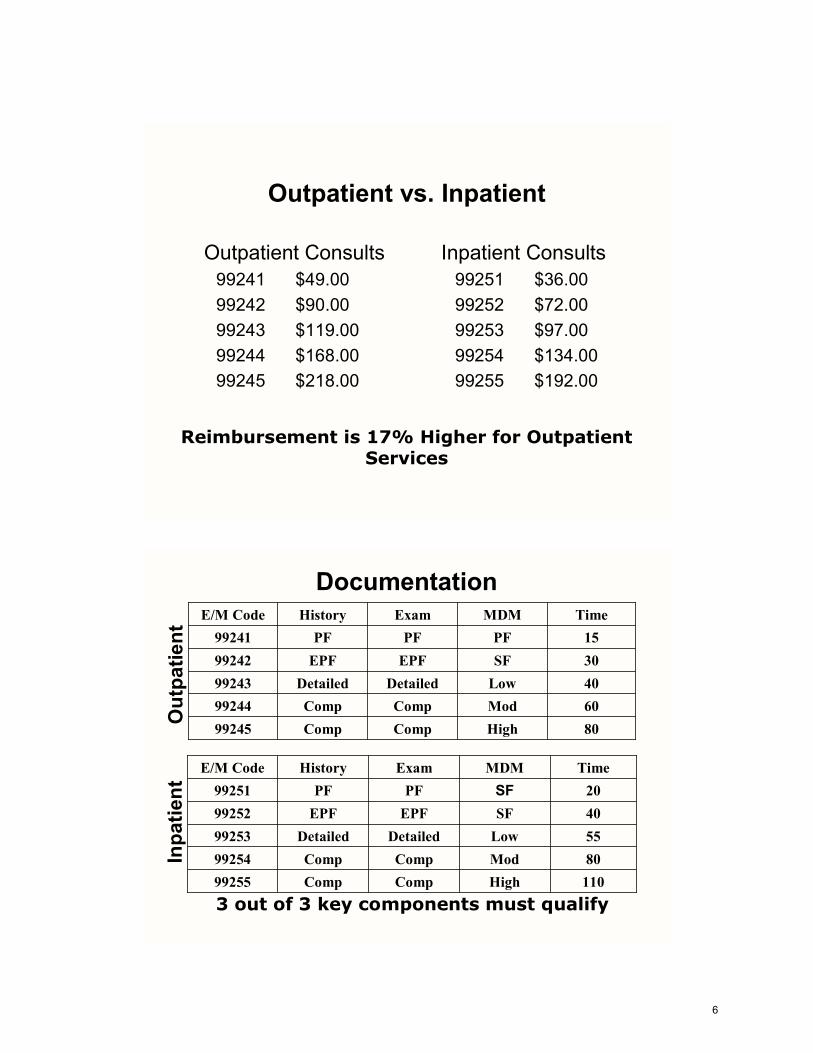
Inpatient Consults99251 $36.0099252 $72.0099253 $97.0099254 $134.0099255 $192.00
Outpatient Consults99241 $49.0099242 $90.0099243 $119.0099244 $168.0099245 $218.00
Outpatient vs. Inpatient
Reimbursement is 17% Higher for Outpatient Services
110HighCompComp9925580ModCompComp9925455LowDetailedDetailed9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
80HighCompComp9924560ModCompComp9924440LowDetailedDetailed9924330SFEPFEPF9924215PFPFPF99241
TimeMDMExamHistoryE/M Code
Inpa
tient
Out
patie
nt
3 out of 3 key components must qualify
Documentation
6
110HighCompComp9925580ModCompComp9925455LowDetailedDetailed9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
80HighCompComp9924560ModCompComp9924440LowDetailedDetailed9924330SFEPFEPF9924215PFPFPF99241
TimeMDMExamHistoryE/M CodeIn
patie
ntO
utpa
tient
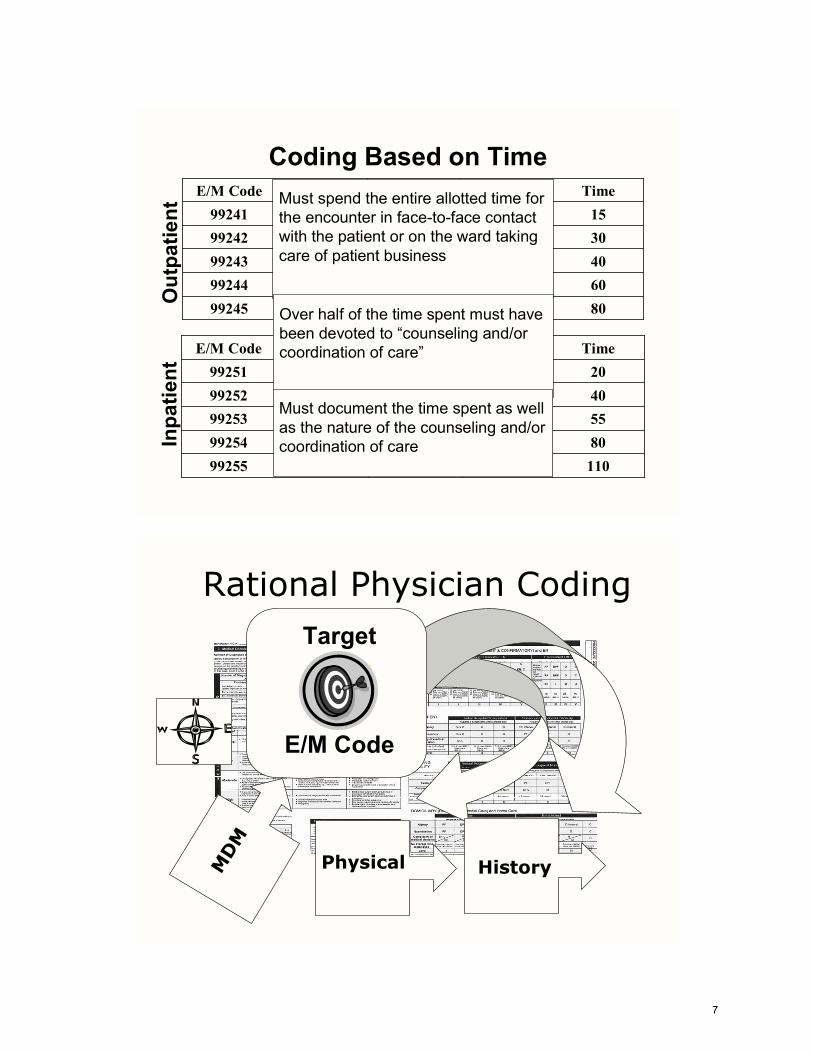
Coding Based on TimeMust spend the entire allotted time for the encounter in face-to-face contact with the patient or on the ward taking care of patient business
Over half of the time spent must have been devoted to “counseling and/or coordination of care”
Must document the time spent as well as the nature of the counseling and/or coordination of care
Rational Physician Coding
2Target
E/M Code
MD
M
Physical History
7
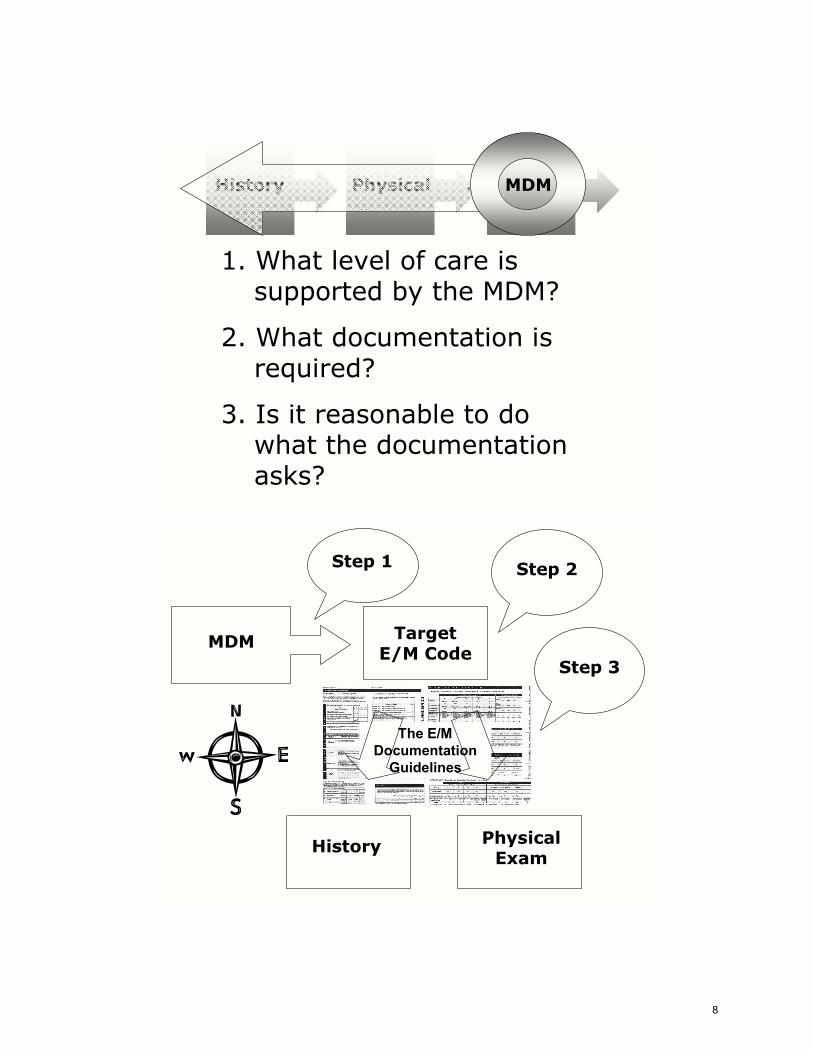
1. What level of care is supported by the MDM?
2. What documentation is required?
3. Is it reasonable to do what the documentation asks?
History Physical MDM
MDM Target E/M Code
History Physical Exam
Step 1 Step 2
Step 3
The E/M Documentation
Guidelines
8

3 out of 3 key components must qualify
99255
110HighCompComp99255
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
Comprehensive History Comprehensive Exam High Complexity MDM
Third most frequently used code for these encountersReimbursement is about $192.00
Time required would be 110 minutes
99255
110HighCompComp99255
TimeMDMExamHistoryE/M Code
99251 2.0%99252 8.1%99253 26.2%99254 41.5%99255 22.2%
9

What Does a 99255 Look Like?
You are consulted by an orthopedic surgeon for pre-op clearance of a patient scheduled to undergo hip surgeryActive problems include diabetes as well as stable hypertension and CAD
You order an echo and routine labsYou also stop Metformin and start the patient on sliding scale insulin Finally, you add a beta blocker and continue other BP medications and nitrates unchangedThe entire encounter, including documentation takes about 55 minutes
1363.8
23614
24 0.8
101 1237
10
MDM Target E/M Code
History Physical Exam
Step 1 Step 2
Step 3
The E/M Documentation
Guidelines
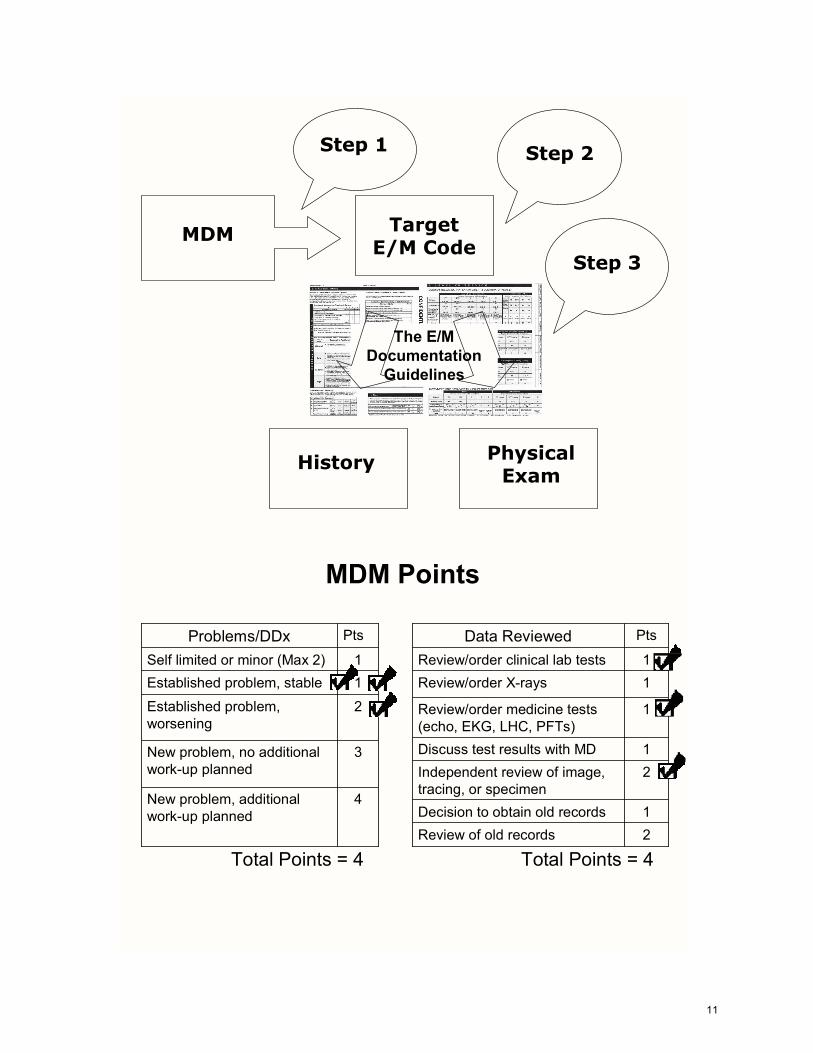
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 4Total Points = 4
11

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
12

110HighCompComp9925580ModCompComp9925455LowDetDet9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
Inpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
Internists selected this level of care was for 22.2 % of inpatient consults in 20032,693,993 encounters in 2004 for a total of $513,865,109 of allowed chargesTime: 110 minutes
3 out of 3 key components must qualify
99255
This exam requires only 2 bullets from EACH of NINE organ systems
This history requires an Extended HPI, 10 ROS and 3/3 elements of PFSH &
HighCompComp99255MDMExamHistoryTarget Code
13

E/M Insight: Comprehensive History
Requires an extended HPI (four or more HPI elements or the status of three or more problems), review of at least 10 systems and at least one item from all three components of past medical, family and social history.
This example qualifies as follows: HPI: Status of three problem (HTN, DM, CAD) PFSH: Includes least one item from all three components of the PFSH ROS: All systems were reviewed. The most clinically relevant systems are recorded. The rest were documented using the accepted E/M short-cut, “All other systems reviewed and are negative.”
HPI: This is a 77 YOWM with multiple medical problems, including well controlled HTN, stable NIRDM and CAD who fell and fractured his right hip early this morning. He is being admitted for right hip ORIF by the orthopedic service. Medical consult was requested for pre-op clearance and risk assessment.
SH: Married; non-smoker; drinks social ETOH
ROS: Pulm: Negative for cough/hemoptysis/SOBARGI: Negative for N/V/D, consitpationCV: Negative for SSCP/orhthopnea/PND
FH: Mother died at 85 of “old age”; father at 77 of acute MI; three grown children IGH
Current MedicationsLisinopril 10 mg QD Metformin 500 mg BID Imdur 30 mg QD Lipitor 20 mg QD
Reason for consult: Pre-op clearance Requesting Physician: John Doe, MD
3 out of 3 key components must qualify
PMH: per HPI, plus dyslipidemia, GERD and CABG in 1999
All other systems reviewed and are negative
3/310ExtendedCompPFSHROSHPIHistory
HighCompComp99255MDMExamHistoryTarget Code
History
14

Physical ExamConstitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
Requires AT LEAST 2 bullets from EACH of NINE organ systems
1 2 3 4 5 6 7 8 9 10 11 12 13 14
15 16
17 18
19
Vitals: 125/75, 82, 22, 98.6General: Pleasant and conversant; looks younger than stated ageEyes: anicteric sclerae, moist conjunctiva with no lid-lag; PERRLAHENT: AT/NC; oropharynx clear; MMM; normal hard/soft palate Neck: Trachea midline; FROM, supple; no thyromegalyLungs: CTA and percussionCV: RRR, no MRGs, healed sternotomy; normal PMI in the MCLAbd: Soft, non-tender; no masses or HSMExt: No digital cyanosis or clubbingSkin: Normal temperature/turgor/texture; no rash/ulcers/nodules Psych: Appropriate affect; A&O X 3
HighCompComp99255MDMExamHistoryTarget Code
Exam
E/M Insight: Comprehensive Exam
Requires at least two bullets from EACH of NINE organ systems.
The example above qualifies based on the following bullets and organ systems:
Constitutional • Three vital signs • General appearance Eyes • Exam of sclerae/lids • Exam of pupils/irises ENMT • Exam of oropharynx • External appearance of ears/nose Neck • Exam of neck • Exam of thyroid Lungs • Auscultation of lungs • Percussion of lungs
CV • Auscultation of heart • Palpation of heart Abdomen • Abdominal Exam • Exam of liver/spleen Musculoskeletal • Exam of digits Skin • Inspection of skin • Palpation of skin Psyche • Assessment of affect • Assessment of orientation
15

E/M Insight: High Complexity MDM Requires two out of three: • Four or more problem points • Four or more data points • High risk The example above qualifies based on four problem points and four data points, even though the level of risk is only moderate.
Plan: 1. Will draw one set of troponins2. Start atenolol and continue post-op3. D/C metformn and start sliding scale insulin4. Continue current BP meds and nitrates 5. Start enoxaprin 30 mg SQ bid 12 hours post-op 6. Echo today7. Ok for surgery in a.m.
Assessment: 1. Uncontrolled diabetes 2. Stable HTN3. CAD with no active chest pain4. Fractured right hip
3 out of 3 key components must qualify
EKG: NSR; no diagnostic ST changes
0.8
1363.8
23614
24101
HighCompComp99255MDMExamHistoryTarget Code
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
1237
Medical Decision-Making
16

Vitals: 125/75, 82, 22, 98.6 Gen: Pleasant and conversant; looks younger than stated age Eyes: Anicteric sclerae; moist conjunctivae, no lid-lag, PERRLA HENT: NC/AT; oropharynx clear; MMM, normal hard/soft palate Neck: Trachea midline; FROM, supple, no thyromegaly Lungs: Clear to auscultation and percussion CV: RRR, no MRGs; PMI in the MCL Abd: Soft, non-tender; no masses or HSM Ext: No digital cyanosis or clubbing Skin: Normal temp/turgor; no rash/lesions/nodules
Reason for consult: Hyperglycemia Requesting Physician: John Doe, MD
HPI: This is a 77 YOWM with multiple medical problems including well con-trolled HTN, stable NIRDM and CAD who fell and fractured his right hip early this morning. He is being admitted for right hip ORIF by the orthope-dic service. Medical consult was requested for pre-op clearance and risk assessment.
PMH: Per HPI, plus dyslipidemia, GERD and CABG in 1999 FH: Mother died at 85 of “old age” father at 77 of AMI SH: Married non-smoker; drinks social ETOH.
ROS Pulm: Negative for cough/hemoptysis/SOBAR GI: Negative for N/V/D, constipation CV: Negative for SSCP/orthopnea/PND
All other systems reviewed and are negative
0.8
136 236
14
24
12 37
101 3.8
EKG: NSR; no diagnostic ST changes
99255
Assessment: 1. Uncontrolled diabetes 2. Stable HTN 3. CAD with no active chest pain 4. Fractured right hip
Plan:
1. Will draw one set of troponins 2. Start atenolol 3. D/C METFORMIN and start SSI 4. Continue current BP meds and nitrates 5. Enoxaparin 30 mg SQ BID 6. Echo today 7. Okay for surgery in a.m.
Current Medications Lisinopril 10 mg QD Metformin 500 mg BID Imdur 30 mg QD Lipitor 20 mg QD
17

Third most frequently used code for these encountersReimbursement is about $218.00
Time required would be 80 minutes
99245
80HighCompComp99245
TimeMDMExamHistoryE/M Code
99241 1.4%99242 8.2%99243 29.7%99244 40.9%99245 19.8%
3 out of 3 key components must qualify
99245
80HighCompComp99245
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
Comprehensive History Comprehensive Exam High Complexity MDM
18

Outpatient Renal Consult
You see a diabetic male referred for elevated creatinine and proteinuria. BP is 180/90.
After reviewing records, you order a renal U/S, adjust medications and schedule a follow-up visit in one month.The entire encounter takes about 60 minutes.
1424.1
12418
19 2.4
101 9.829
Urine Prot/Cr = 3650 mg/G
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 4Total Points = 11
19

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
20

80HighCompComp9924560ModCompComp9924440LowDetDet9924330SFEPFEPF9924215SFPFPF99241
TimeMDMExamHistoryE/M Code
Outpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
1.9 million encounters in 2004 for a total of $411 million of allowed chargesReimbursement is about $218.00Time: 80 minutes
3 out of 3 key components must qualify
99245
This exam requires only 2 bullets from EACH of NINE organ systems
This history requires an Extended HPI, 10 ROS and 3/3 elements of PFSH &
HighCompComp99245MDMExamHistoryTarget Code
21

Reason for Consult: CKD Requesting MD: Richard Hayes
HPI: Pt is a 57 YOM with IRDM and dyslipidemia, both of which have been well controlled. He also has a history of HTN, which has worsened recently despite increasing doses of BP medications. He is referred for evaluation and management of elevated creatinine and proteinuria. He has no spontaneous somatic complaints.
ROS: Complete ROS was performed and documented using a questionnaire. Pertinent findings include intermittent lower extremity edema and paresthesias and occasional orthopnea. No recent hematuria, obstructive symptoms, rash, joint pain or dysuria. For more details, please refer to today’s ROS questionnaire in the chart.
Complete PFSH was reviewed and documented using a questionnaire. Note is made of a remote history of nephrolithiasis and a 20 pack-year history of smoking. He has no first degree relatives on dialysis and there is no evidence of hereditary renal disease. For details, please refer to the intake form in the chart dated today.
3 out of 3 key components must qualify
HighCompComp99245MDMExamHistoryTarget Code
3/310ExtendedCompPFSHROSHPIHistory
E/M Insight: Comprehensive History
Requires an extended HPI (four or more HPI elements or the status of three or more problems), 10 ROS and one item from all three components of the past medical, family and social history.
This example qualifies as follows: HPI: Status of three problem (HTN, DM, Dyslipidemia) ROS: Completed using a questionnaire. You must say you reviewed the information and comment on any pertinent findings. You must also note the date and location of the form. Finally, the questionnaire must remain in the chart as a permanent part of the medical record. PFSH: Also completed using a questionnaire. Same rules apply.
History
22

Constitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
Requires AT LEAST 2 bullets from EACH of NINE organ systems
1 2 3 4 5 6 7 8 9 10 11 12 13 14
15
17 18
19
Vitals: 180/90, 111, 99.6General: Well nourished male in NAD; looks stated ageEyes: anicteric sclerae, moist conjunctiva with no lid-lag; PERRLA,HENT: AT/NC; oropharynx clear; MMM; normal hard/soft palate Neck: Trachea midline; FROM, supple; no thyromegaly
CV: RRR, no MRGs, normal PMI in the midclavicular lineLungs: Clear to auscultation and percussion
Abd: Soft, non-tender; no masses or HSMExt: No digital cyanosis or clubbingSkin: Normal temp/texture/turgor; no rash/lesions/nodules Psych: Oriented to person/place/time; appropriate affect
3 out of 3 key components must qualify
HighCompComp99245MDMExamHistoryTarget Code
16
E/M Insight: Comprehensive Exam
Requires at least two bullets from EACH of NINE organ systems.
The example above qualifies based on the following bullets and organ systems:
Constitutional • Three vital signs • General appearance Eyes • Exam of sclerae/lids • Exam of pupils/irises ENMT • Exam of oropharynx • External appearance of ears/nose Neck • Exam of neck • Exam of thyroid Lungs • Auscultation of lungs • Percussion of lungs
CV • Auscultation of heart • Palpation of heart Abdomen • Abdominal Exam • Exam of liver/spleen Musculoskeletal • Exam of digits Skin • Inspection of skin • Palpation of skin Psyche • Assessment of orientation • Assessment of affect
Exam
23

Assessment1. Stage IV CKD with estimated GFR of 29 mls/min2. Poorly controlled HTN 3. Significant normocytic anemia4. Nephrotic range proteinuria
Plan1. Increase lisinopril to 40 mg QD2. Check iron stores and start empiric Procrit3. Check RUS 4. Start NaHCO3 650 mg BID5. RTC in one month with renal profile, spot prot/creat and CBC
Review of old records: We have a note from Dr. Hayes’ office dated sixmonths ago, which showed a creatinine of 1.9. At that time, the patient’s
BP was 160/80. Lisinopril was increased from 10 to 20 mg QD. Patient was last hospitalized in December of 2004 for lobar pneumonia. Creatinine during that admission was 1.5 to 1.8. BP was well controlled.
2.4
1424.1
12418
19101 9.8
29
Prot/Creat: 3650 mg/G
3 out of 3 key components must qualify
HighCompComp99245MDMExamHistoryTarget Code
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
E/M Insight: High Complexity MDM Requires two out of three: • Four or more problem points • Four or more data points • High risk The example above qualifies based on all three dimensions of medical decision-making.
Medical Decision-Making
24

Vitals: 180/90, 111, 99.6 Gen: Well-nourished WM; looks state age Eyes: Anicteric sclerae; moist conjunctivae, no lid-lag, PERRLA HENT: NC/AT; oropharynx clear; MMM, normal hard/soft palate Neck: Trachea midline; FROM, supple; no thyromegaly Lungs: Clear to auscultation and percussion CV: RRR, no MRGs; PMI in the MCL Abd: Soft, non-tender; no masses or HSM Ext: No digital cyanosis or clubbing Skin: Normal temp/turgor; no rash/lesions/nodules Psych: Oriented to person/place/time; appropriate affect
Reason for consult: CKD Requesting Physician: Richard Hayes, MD
HPI: 57 YOM with IRDM and dyslipidemia both of which have been well con-trolled. He also has a history of HTN which has worsened recently despite increasing doses of BP medications. He is referred for evaluation and man-agement of elevated creatinine and proteinuria. He has no spontaneous so-matic complaints.
ROS: Complete ROS was performed and documented using a questionnaire. Pertinent findings include intermittent lower extremity edema and orthopnea. No recent hematuria, obstructive symptoms, rash, joint pain or dysuria. For more details please refer to today’s ROS questionnaire in the chart. PFSH: Complete PFSH was reviewed and documented using a question-naire. Note is made of a remote history of nephrolithiasis and a 20 pack-year history of smoking. He has no first degree relatives on dialysis and there is no evidence of hereditary renal disease. For more details, please refer to the PFSH section of today’s intake form located in the chart.
99245
Assessment: 1. Stage IV CKD with GFR of 29 mls/min 2. Poorly controlled HTN 3. Significant normocytic anemia 4. Nephrotic range proteinuria
Plan:
1. Increase lisinopril to 40 mg PO QD 2. Check iron stores and start empiric Procrit 3. Check renal ultrasound 4. Start NaHCO3 650 mg PO BID 5. RTC in one month with renal profile, CBC and spot prot/creat
2.4
142 124
18
19
9.8 29
101 4.1
Prot/Creat: 3650 mg/G
25

Most frequently used code for these encountersReimbursement is about $134.00
Time required would be 80 minutes
99254
80ModCompComp99254
TimeMDMExamHistoryE/M Code
99251 2.0%99252 8.1%99253 26.2%99254 41.5%99255 22.2%
3 out of 3 key components must qualify
99254
80ModCompComp99254
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
Comprehensive History Comprehensive Exam High Complexity MDM
26

What Does a 99254 Look Like?You are consulted by a general surgeon to evaluate a patient for confusionHe is post-op day #2 following laproscopiccholecystectomy
You diagnose metabolic encephalopathy due to hypernatermia and start D5W at 150 cc/hr with 20 mEq of KCL/Liter along with a.m. labsTotal time, including documentation is about 50 minutesWhat’s the correct code and documentation?
1543.3
10814
24 0.8
101 1237
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 1Total Points = 4
27

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
28

110HighCompComp9925580ModCompComp9925455LowDetDet9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
Inpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
Internists selected this level of care was for 41 % of inpatient consults in 20035,296,789 encounters in 2004 for a total of $730,819,429 of allowed chargesTime: 80 minutes
3 out of 3 key components must qualify
99254
This exam requires only 2 bullets from EACH of NINE organ systems
This history requires an Extended HPI, 10 ROS and 3/3 elements of PFSH &
ModCompComp99254MDMExamHistoryTarget Code
29

HPI: The patient is a 57 YOWM who develped sudden confusion following laprascopiccholecystectomy. His wife states he has had progressive and constant confusion since yesterday which she describes as quite severe. The only associated symptom has been intermittent nausea without vomiting.
SH: Married non-smoker; social ETOH
ROS: Cannot be reliably obtained due to the patient’s confusion
FH: Negative for premature CVAs in first degree relatives; father is alive at age 80, mother is 79. Two grown kids IGH
Current MedicationsNorvasc 5 mg QD Lipitor 20 mg QD
Reason for consult: Altered mental status Requesting Physician: Jane Doe, MD
3 out of 3 key components must qualify
PMH: Dyslipidemia and essential HTN
3/310ExtendedCompPFSHROSHPIHistory
ModCompComp99254MDMExamHistoryTarget Code
E/M Insight: Comprehensive History
Requires an extended HPI (four or more HPI elements or the status of three or more problems), 10 ROS and one item from all three components of the past medical, family and social history.
This example qualifies as follows: HPI: Five HPI elements are recorded (context, timing, duration, severity, associated signs/symptoms). PFSH: Includes at least one item from all three components of PFSH ROS: Cannot be completed due to the patient’s confusion. In these cases, the examiner is not penalized for not including this information, but you must state the reason why it could not be obtained. .
History
30

Physical ExamConstitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
1 2 3 4 5 6 7 8 9 10 11 12 13 14
15 16
17 18
19
Vitals: 120/80, 28, 111, 99.6General: Well nourished middle-aged WM; confusedEyes: anicteric sclerae, moist conjunctiva with no lid-lag; PERRLA,HENT: AT/NC; oropharynx clear; MMM; normal hard/soft palate Neck: Trachea midline; FROM, supple; no thyromegaly
CV: RRR, no MRGs; hyperdynamic PMI in the MCLLungs: Anterior rhonchi; no crackles; clear to percussion
Abd: Soft, non-tender; no masses or HSMExt: No digital cyanosis or clubbingSkin: Decreased turgor; some tenting; no rash/lesions/nodules
Requires AT LEAST 2 bullets from EACH of NINE organ systems
ModCompComp99254MDMExamHistoryTarget Code
3 out of 3 key components must qualify
Psych: Not oriented to person/place/time; insight/judgment impaired
E/M Insight: Comprehensive Exam
Requires at least two bullets from EACH of NINE organ systems.
The example above qualifies based on the following bullets and organ systems:
Constitutional • Three vital signs • General appearance Eyes • Exam of sclerae/lids • Exam of pupils/irises ENMT • Exam of oropharynx • External appearance of ears/nose Neck • Exam of neck • Exam of thyroid Lungs • Auscultation of lungs • Percussion of lungs
CV • Auscultation of heart • Palpation of heart Abdomen • Abdominal Exam • Exam of liver/spleen Musculoskeletal • Exam of digits Skin • Inspection of skin • Palpation of skin Psyche • Assessment of orientation • Assessment of affect
Exam
31

Plan: 1. D5W with 20 mEq/L KCL at 150 cc/hr2. Renal profile later today3. Repeat renal profile in a.m.
Assessment: 1. Acute encephalopathy due to hypernatremia2. Mild hypokalemia3. Post-op day #2, laprascopic cholecystectomy
0.8
1543.3
10824101 12
37
3 out of 3 key components must qualify
14
ModCompComp99254MDMExamHistoryTarget Code
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
E/M Insight: Moderate Complexity MDM Requires two out of three: • Three or more problem points • Three or more data points • Moderate risk The example above qualifies based on four problem points and the pres-ence of moderate risk. Since only two out of three dimensions are re-quired, it doesn’t matter that the encounter produced only one data point.
Medical Decision-Making
32

Vitals: 120/80, 28, 111, 99.6 Gen: Well-nourished middle-aged WM; confused Eyes: Anicteric sclerae; moist conjunctivae, no lid-lag, PERRLA HENT: NC/AT; oropharynx clear; MMM, normal hard/soft palate Neck: Trachea midline; FROM, supple; no thyromegaly Lungs: Anterior rhonchi; clear to percussion CV: RRR, no MRGs; PMI in the MCL Abd: Soft, non-tender; no masses or HSM Ext: No digital cyanosis or clubbing Skin: Normal temp/turgor; no rash/lesions/nodules Psych: Not oriented to person/place/time; judgment/insight impaired
Reason for consult: AMS Requesting Physician: Jane Doe, MD
HPI: 57 YOM who developed sudden confusion following laparoscopic cholecystectomy. His wife states that he has had progressive and con-stant confusion since yesterday, which she describes as quite severe. The only associated symptom has been intermittent nausea and vomit-ing.
PMH: Dyslipidemia and essential HTN SH: Married non-smoker; social ETOH FH: Negative for premature CVAs in first degree relatives. Father is alive at 80; mother is 79. Two grown kids IGH. ROS: Cannot be reliably obtained due to the patient’s confusion.
99254
Assessment: 1. Acute encephalopathy due to hypernatremia 2. Mild hypokalemia 3. Post-op day #2 laparoscopic cholecystectomy Plan:
1. D5W with 20 mEq KCL/L at 150 cc/hr 2. Renal profile later today 3. Repeat renal profile in a.m.
0.8
154 108
14
24
12 37
101 3.3
33

Most frequently used code for these encountersReimbursement is about $97.00
Time required would be 55 minutes
99253
55LowDetDet99253
TimeMDMExamHistoryE/M Code
99251 2.0%99252 8.1%99253 26.2%99254 41.5%99255 22.2%
3 out of 3 key components must qualify
99253
55LowDetDet99253
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
Detailed History Detailed Exam Low Complexity MDM
34

What Does a 99253 Look Like?
You are consulted for HTN in a post-op TKR patientBP is 148/90The patient also has dyslipidemia and GERD which are not active problemsYou increase amlodipine from 5 to 10 mg PO qd and order routine labsTotal time spent is 35 minutes
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 1Total Points = 2
35

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
36

110HighCompComp9925580ModCompComp9925455LowDetDet9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
Inpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
Internists selected this level of care was for 26.2% of inpatient consults in 20033,287,293 encounters in 2004 for a total of $313,143,374 of allowed chargesTime: 55 minutes
3 out of 3 key components must qualify
99253
This exam requires only 12 bullets from ANY organ systems
This history requires an Extended HPI, 2 - 9 ROS and 1/3 elements of PFSH &
LowDetDet99253MDMExamHistoryTarget Code
37

ROS CV: Negative for SSCP/orthopnea/PNDNeuro: Negative for numbness/tingling/TIAs/blurry vision/pounding HA’s
Pertinent PFSH: Remarkable for ongoing tobacco abuse; 1 PPD times 30 years
HPI: The patient is a pleasant a 55 YOWM with a history of OA for which he underwent TKR on the right yesterday. He has long-standing HTN, which has been easy to control on routine medications as an outpatient. There is also a history of stable GERD for which he takes OTC H2 blockers. Aside from incisional knee pain, he has no spontaneous somatic complaints.
Reason for consult: Post-op HTN Requesting physician: John Doe, MD
3 out of 3 key components must qualify
LowDetDet99253MDMExamHistoryTarget Code
1/32 – 9ExtendedDetailedPFSHROSHPIHistory
E/M Insight: Detailed History
Requires an extended HPI (four or more HPI elements or the status of three or more problems), two through nine ROS and at least one item from one of the three components of PFSH.
This example qualifies as follows: HPI: Comments on the status of the three problems, OA, HTN, GERD. PFSH: Includes at least one item from all three components of PFSH ROS: Two clinically relevant systems are recorded (CV, neuro). .
History
38

Physical Exam
Lungs: Clear to auscultation and percussion
Constitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
Vitals: 148/90, 18, 82, 98.6
Neck: FROM, supple; no thyromegaly; no carotid bruits
CV: RRR, no MRGs; normal PMI in the MCL
Ext: No peripheral edema or digital cyanosis
1 2 37 8
9 1011
12
Requires AT LEAST 12 bullets from ANY organ systems
64 5
General: NAD, conversant, well nourished WM looks stated age
Abd: Soft, non-tender; NABS
3 out of 3 key components must qualify
LowDetDet99253MDMExamHistoryTarget Code
E/M Insight: Detailed Exam
A detailed exam requires 12 bullets from any organ systems. The exam-ple above contains the following bullets:
• Three vital signs • General appearance • Exam of neck • Exam of thyroid • Exam of carotids • Auscultation of lungs • Percussion of lungs • Auscultation of heart • Palpation of heart • Exam of abdomen • Assessment of extremity edema • Exam of digits
Exam
39

Assessment: Sub-optimally controlled essential HTN
3 out of 3 key components must qualify
Plan: 1. Increase amlodipine to 10 mg PO qd2. Decrease intervals between PO pain meds 3. Renal profile and CBC in a.m.
LowDetDet99253MDMExamHistoryTarget Code
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
E/M Insight: Low Complexity MDM
Low complexity MDM requires two out of three of the following: • Two problem points • Two data points • Low risk The example above qualifies based on two problem points (for the sub-optimally controlled HTN) and the presence of moderate risk (based on prescription drug management). Only one data point is tallied, but that’s okay because only two out of three dimensions of MDM are needed to qualify for any given level of complexity.
Medical Decision-Making
40

Vitals: 148/90, 18, 82, 98.6 Gen: NAD, conversant, well-nourished WM; looks staged age Neck: FROM, supple; no thyromegaly; no carotid bruits Lungs: Clear to auscultation and percussion CV: RRR, no MRGs; PMI in the MCL Abd: Soft, non-tender; NABS Ext: No peripheral edema or digital cyanosis
Reason for consult: Post-op HTN Requesting Physician: John Doe, MD
HPI: 55 YOM with a history of OA who underwent TKR on the right yes-terday. He has longstanding HTN which has been easy to control with routine medications as an outpatient. There is also a history of stable GERD for which he takes OTC H2 blockers. Aside from incisional knee pain, he has no spontaneous somatic complaints.
PFSH: Remarkable for ongoing tobacco abuse; 1 PPD for 30 yrs ROS: CV: Negative for SSCP/orthopnea/PND Neuro: Negative for numbness/tingling/TIAs/blurry vision
99253
Assessment: 1. Sub-optimally controlled essential HTN 2. Mild hypokalemia 3. Post-op day #2 laparoscopic cholecystectomy Plan:
1. Increase amlodipine to 10 mg PO QD 2. Decrease intervals between PO pain meds 3. Repeat renal profile and CBC in a.m.
41

Second least frequently used code for these encountersReimbursement is about $72.00
Time required would be 40 minutes
99252
40SFEPFEPF99252
TimeMDMExamHistoryE/M Code
99251 2.0%99252 8.1%99253 26.2%99254 41.5%99255 22.2%
3 out of 3 key components must qualify
99252
40SFEPFEPF99252
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
EPF History EPF Exam Straightforward MDM
42

What Does a 99252 Look Like?
Suppose you are consulted to see the same post-op patient with HTN from our previous exampleBut this time the BP is already optimally controlledYou make no changes in medications and order no labsTotal time spent is 15 minutes
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 0Total Points = 1
43

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
44

110HighCompComp9925580ModCompComp9925455LowDetDet9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
Inpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
Internists selected this level of care was for 8.1% of inpatient consults in 20031,176,712 encounters in 2004 for a total of $81,531,641 of allowed chargesTime: 40 minutes
3 out of 3 key components must qualify
99252
This exam requires only 6 - 11 bullets from ANY organ systems
This history requires a brief HPI, and review of ONE system &
SFEPFEPF99252MDMExamHistoryTarget Code
45

ROS CV: Negative for SSCP/orthopnea/PND
HPI: The patient is a pleasant a 55 YOWM with a history of OA which caused severe right hip pain. He underwent TKR on the right yesterday. He also has long-standing HTN, which has been easy to control on routine medications as an outpatient.
Reason for consult: Management of HTN Requesting physician: John Doe, MD
3 out of 3 key components must qualify
None1BriefEPFPFSHROSHPIHistory
SFEPFEPF99252MDMExamHistoryTarget Code
E/M Insight: Expanded Problem Focused History
An expanded problem focused history requires a brief HPI (with one to three HPI elements or the status of one to three problems), plus one ROS. No elements of PFSH are required. The example above qualifies as follows: HPI: Comments on the status of the two problems, OA and HTN. ROS: One clinically relevant system is reviewed (CV)
History
46

Lungs: Clear to auscultation
Constitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
Vitals: 125/75, 18, 82, 98.6
Neck: FROM, supple; no JVD
CV: RRR, no MRGs
1 2 3
Requires only 6 - 11 bullets from ANY organ systems
64 5
General: NAD, conversant, well nourished WM looks stated age
Abd: Soft, non-tender; NABS
SFEPFEPF99252MDMExamHistoryTarget Code
3 out of 3 key components must qualify
E/M Insight: Expanded Problem Focused Exam You can see that it doesn’t take much to qualify for an expanded problem focused exam. All you need is six to 11 bullets from any organ systems. In this case the following six bullets were documented: 1. A brief description of the patient 2. Three vital signs 3. Exam of the neck 4. Auscultation of the lungs 5. Auscultation of the heart 6. Abdominal exam This adds up to exactly six bullets which is the minimum required for an ex-panded problem focused exam.
Exam
47

Assessment: Optimally controlled essential HTN
3 out of 3 key components must qualify
Plan: Continue amlodipine 10 mg PO qd
SFEPFEPF99252MDMExamHistoryTarget Code
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
E/M Insight: Straightforward MDM
Straightforward MDM requires two out of three of the following: • One problem point • One data point • Minimal risk The example above qualifies based on all three dimensions of MDM. (The risk is actually more then enough.)
Medical Decision-Making
48

Vitals: 125/75, 18, 82, 98.6 Gen: NAD, conversant, well-nourished WM; looks staged age Neck: FROM, supple; no JVD Lungs: Clear to auscultation CV: RRR, no MRGs Abd: Soft, non-tender; NABS
Reason for consult: HTN Requesting Physician: John Doe, MD
HPI: 55 YOM with a history of OA which caused severe hip pain. He un-derwent TKR on the right yesterday. He has longstanding HTN which has been easy to control with routine medications as an outpatient.
ROS: CV: Negative for SSCP/orthopnea/PND
99252
Assessment: Optimally controlled essential HTN Plan: Continue amlodipine to 10 mg PO QD
49

Least frequently used code for these encountersReimbursement is about $36.00
Time required would be 20 minutes
99251
20SFPFPF99251
TimeMDMExamHistoryE/M Code
99251 2.0%99252 8.1%99253 26.2%99254 41.5%99255 22.2%
3 out of 3 key components must qualify
99251
20SFPFPF99251
TimeMDMExamHistoryE/M Code
6 – 11 from any systemsEPF
12 from any systemsDet
1 – 5 from any systemsPF
2 from 9 systemsComp
BulletsExam
None1BriefEPF
1/32 – 9ExtDet
NoneNoneBriefPF
3/310ExtComp
PFSHROSHPIHx
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
Problem Focused History Problem Focused Exam Straightforward MDM
50

99251 Example
You are asked to evaluate a patient for “persistent hypocalcemia”Serum calcium is 7.0 mg/dlSerum albumin is 2.2You calculate the corrected calcium (8.4) and make the diagnosis of pseudohypocalcemia which requires no further treatmentTotal time spent is 10 minutes
MDM Points
1Self limited or minor (Max 2)
4New problem, additional work-up planned
3New problem, no additional work-up planned
2Established problem, worsening
1Established problem, stable
PtsProblems/DDx
1Decision to obtain old records
2Independent review of image, tracing, or specimen
1Review/order clinical lab tests
2Review of old records
1Discuss test results with MD
1Review/order medicine tests (echo, EKG, LHC, PFTs)
1Review/order X-rays
PtsData Reviewed
Total Points = 1Total Points = 1
51

•Parenteral controlled substances•Drug therapy requiring intensive monitoring for toxicity•Obtain DNR or de-escalate care
•Cardiovascular imaging, with contrast, with identified risk factors•Cardiac EP studies•Diagnostic endoscopies, with identified risk factors
•One or more chronic illness, with severe exacerbation•Acute or chronic illness or injury, which poses a threat to life or bodily function•An abrupt change in neurological status
High
•Prescription drug management•IV fluids, with additives
•Cardiac stress test•Cardiovascular imaging studies, with contrast, with no identified risk factors
•One chronic illness, with mild exacerbation•Two stable chronic illnesses•Undiagnosed new problem, with uncertain prognosis
Moderate
•Over the counter drugs•Minor surgery, with no risk factors•PT/OT•IV fluids, without additives
•Physiologic tests not under stress, e.g., PFTs•Non-cardiovascular imaging studies with contrast•ABG•Skin biopsies
•Two or more self-limited or minor problems•One stable chronic illness•Acute uncomplicated injury or illness, e.g., cystitis, allergic rhinitis, sprain
Low
•Rest•Gargles•Superficial dressings
•Laboratory tests •Chest X-rays•EKG/EEG, Echocardiogram
•One self-limited or minor problem, e.g., cold, insect bite, tinea corporis.
Minimal
Management Options
Diagnostic ProceduresPresenting ProblemsRisk
Calculating the Overall MDM
High44HighMod33ModerateLow22LowMin0 - 11SF
RiskData Problems MDM Complexity
Need 2 out of 3 to qualify for given level of MDM
52

110HighCompComp9925580ModCompComp9925455LowDetDet9925340SFEPFEPF9925220SFPFPF99251
TimeMDMExamHistoryE/M Code
Inpatient Consults
3 out of 3 key components must qualify
Selecting the Target Code
Internists selected this level of care was for 2.0% of inpatient consults in 2003The documentation required for this level of care is extremely minimalTime: 20 minutes
3 out of 3 key components must qualify
99251
This exam requires only 1 - 5 bullets from ANY organ systems
This history requires only a brief HPI. No elements of ROS or PFSH are required
&
SFPFPF99251MDMExamHistoryTarget Code
53

HPI: The patient has had hypocalcemia seen on routine labs for the past three days.
Reason for consult: Hypocalcemia Requesting physician: John Doe, MD
3 out of 3 key components must qualify
NoneNoneBriefPFPFSHROSHPIHistory
SFPFPF99251MDMExamHistoryTarget Code
History
E/M Insight: Problem Focused History
A problem focused history requires a brief HPI (with one to three HPI elements or the status of one to three problems), no ROS and no PFSH. The example above qualifies as follows: HPI: One HPI element (duration) is recorded.
54

Physical ExamConstitutional Eyes ENMT Neck
Chest/Breasts
CV
Skin
Musculoskeletal
Neurologic
Psychiatric
GI GULungs
Vitals: 125/75, 18, 82, 98.6
1 2
Requires only 1 - 5 bullets from ANY organ systems
General: NAD, conversant; looks stated age
SFPFPF99251MDMExamHistoryTarget Code
3 out of 3 key components must qualify
Exam
E/M Insight: Problem Focused Exam It is difficult (but not impossible not to qualify for this level of exam. All you need are one to five bullets from any organ systems. In this case the following two bullets were documented: 1. A brief description of the patient 2. Three vital signs This adds up more than enough bullets to qualify.
55

Plan: 1. No specific therapy needed 2. Consider dietary consult to improve nutrition
Assessment: Pseudohypocalcemia
Labs: Calcium 7.0, albumin 2.2
SFPFPF99251MDMExamHistoryTarget Code
3 out of 3 key components must qualify
High≥4≥4High
Mod33Mod
Low22Low
Min0 - 11SF
RiskData PtsProb PtsMDM
Requires two out of three
E/M Insight: Straightforward MDM
Straightforward MDM requires two out of three of the following: • One problem point • One data point • Minimal risk The example above qualifies based on all three dimensions of MDM.
Medical Decision-Making
56

Vitals: 125/75, 18, 82, 98.6 Gen: NAD, conversant; looks staged age Labs: Calcium 7.0, albumin 2.2 Assessment: Pseudohypocalcemia Plan: 1. No specific therapy needed 2. Consider dietary consult to improve nutrition
Reason for consult: Hypocalcemia Requesting Physician: John Doe, MD HPI: The patient has had hypocalcemia seen on routine labs for the last three days.
99251
57
History Physical MDM
Perform the documentation in a purpose-driven manner Don’t document more than is necessary to take care of the patient and maintain complianceThree out of three key components are always needed for consult servicesUse outpatient consult codes for observation and ER patients
Peter R. Jensen, MD, CPC
Online and On-site Physician-to-Physician E/M Coding Education
1-888-U-EM-CODE
Practical E/M Coding Education
www.EMuniversity.com
58





























