Embed Size (px)
Citation preview
Pediatric Dennatology Vol. 10 No. 1 54-57
Rapp-Hodgkin Syndrome with Pili Canaliciili
Francisco Camacho, Juan Ferrando,* Antonio R. Pkhardo, Ismael Sotillo, andEnrique Jorquera
Departments of Medico-Surgical Dermatology and Venereology, Seviila, and *Barcelona, Spain
Abstract: A 20-year-old woman and her 12-year-ofd brother had hypo-hidrotic ectodermal dysplasia, cleft lip and palate, midfacial hypoplasiawith narrow nose Irom the nasal bridge to the tip, narrow dysplastic nails,and conical teeth and hypodontia, and hypospadias artd hypoplasticuvuia in the boy. The woman had major underdevelopment of intellectualcapacity. The most important hair anomalies in both siblings were sparseeyebrows, pili torti, and pili canalicuiL Some of the pili canalicuii had twocanals (pili bicanalicuii), and the cross section for scanning electron mi-croscopy had a quadrangular aspect. This is the seventh famiiy reportedwith Rapp-Hodgkin ectodermai dysplasia.
Since the original description of the Rapp-Hodgkin syndrome (RHS) as an uncommon, hered-itary, congenital condition in three members of anAmerican family in 1968 (I), six families and foursporadic cases have been reported, for a total of 22patients. We add a new family with two affectedmembers in whom, together with the typical fea-tures of ectodermal dysplasia (Table 1), structuralhair anomalies of pili torti and pili canalicuii werefound.
CASE REPORTS
A 20-year-old woman was first seen in our depart-ment when she was age 5 years for hypohidrotic ec-todermal dysplasia with cleft lip, corrected whenshe was 3. She also had cleft palate, snub nose withnarrowing from the nasal bridge to the tip, ble-pharophimosis, hypertelorism, auricular lobes withlow implantation, dental malocclusion, mental re-tardation, hypoplastic nails, eyebrow alopecia, andtightly curled, rough, brilliant, very difficult-to-
comb hair, which was diagnosed as spun-glass hair(Fig. 1). She had a normal female karyotype.
Among the laboratory studies done, the follow-ing had abnormal results: electroencephalogram,with overcharge activity of slow waves; radiographshowing bifid spine at the sacrum; and serum zinclevel of 248 fig/100 ml (normal 70-150 (xg/ml). Asweat test on the face and back with pilocarpineiontophoresis produced very little sweating.
We also saw her 12-year-old brother, whose cleftlip had been corrected seven years earlier. He had ashort cleft palate, hypoplasia of the uvula, midfacialhypoplasia with a Iow nasal bridge, narrow nasalopenings, short philtrum, thin vermilion border ofthe upper lip, more prominent lower lip, alopecia ofeyebrow ends, depapillated tongue, and misshapenteeth in the upper and lower jaws (Fig. 2). He had aglandular hypospadia that had been surgicallytreated four years earlier. His height was 124.5 cm(normal for age 12 yrs: 149.6 cm). His intellectualcapacity was normal. His nails had dysplasticchanges of hypotrophy, brittleness, and chromony-
Address correspondence to Prof. Francisco Camacho, De-partamento de Dermatologia Medico-Quirurgica y Venereologia,Hospital Universitario Virgen Macarena, Avda. Dr. Fedriani s/n,Sevffla 41075, Spain.
54
Camacho et al: Rapp-Hodgkin Syndrome 55
TABLE I. Clinical Features
Ciinical features of Rapp-Hodgkin syndromeCraniofacial anomalies; midfacial hypoplasia with
high forehead, small mouth, narrow nose, shortphiltrum, thin vermilion border of the upper lip.
Cleft lip or palateHypopiasia of the uvulaPoor dentition: hypodontia and conically shaped
teethPoor hair growth: sparseness of eyebrows and
eyelashes, pili torti, pili canalicuii.Dystrophic nails: hypertrophy, brittleness, narrow,
cbromonychia.HypohidrosisHypospadias in boys
Other ciinical feattires reportedErythrodermia and scaling skin at birthShort statureLow intellectual capacityDepapillated tongueConductive hearing lossHypoplastic maxillaAtretic ear canalsDysplastic eustachian orificesOphthalmologic complications: bilateral punctal
atresia, underdevelopment of lacrimal ducts,corneal scarring.
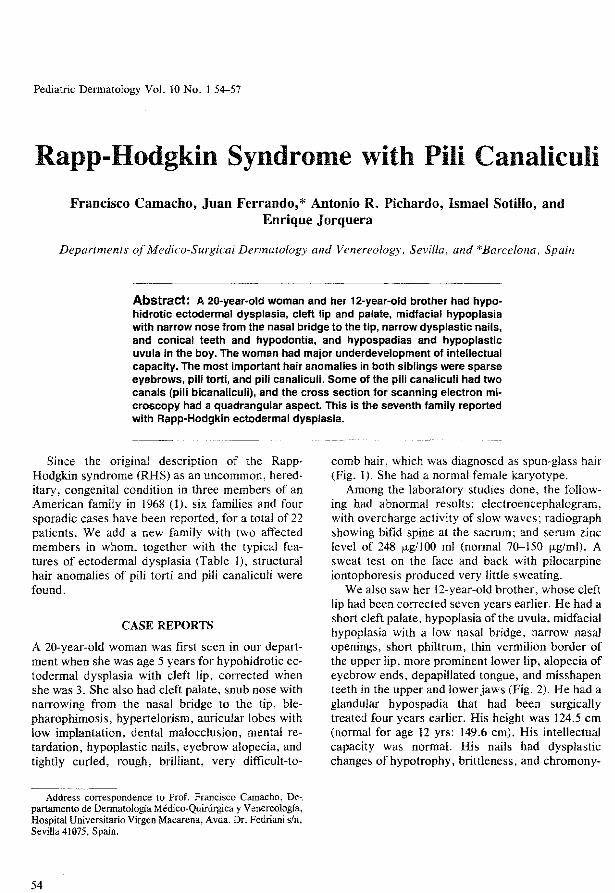
Figure 2. Brother with scar of cleft lip intervention onthe left half of lip, narrow nose, thin vermilion borderon upper lip, and malocclusion and loss of some teethin both upper and lower jaws.
chia. The hair was rough, brilliant, straight, and asimpossible to comb as his sister's. He was diag-nosed as having pili canalicuii in spun-glass or un-combable hair (Fig. 3).
Results of his blood count, electrolyte, atid met-abolic investigations were normal. He had a normalmale karyotype. A sweat test on his face was nega-tive and on his back produced little sweating.
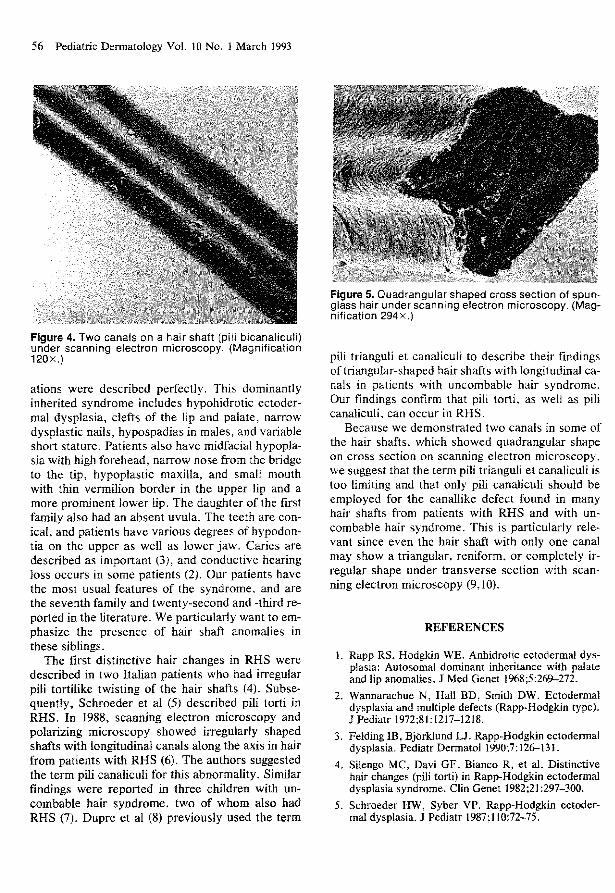
Hairs from both siblings were taken for study bylight microscopy and scanning electron micros-copy. Many of the hairs showed pili torti but themost frequently observed feattire was the longitudi-nal canal along the hair shaft, which, when singular,showed a triangular or kidney-shaped form, or oc-casionally a flattened ellipse in cross section. Somehairs had two longitudinal canals (Fig. 4) that oncross section were quadrangular (Fig. 5)
DISCUSSION
In the first publications on Rapp-Hodgkin ectoder-ma! dysplasia syndrome (1,2) the ectodermal alter-
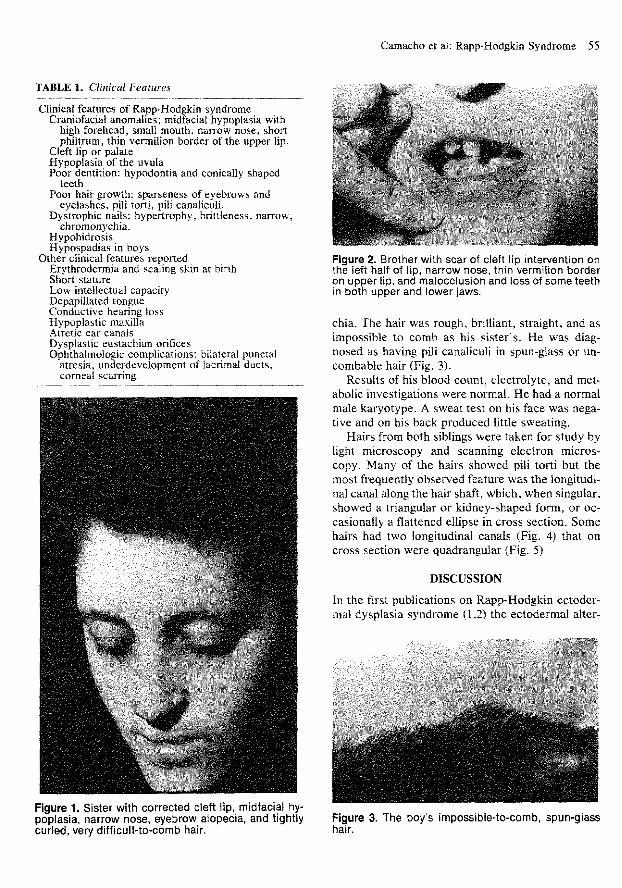
Figure 1. Sister with corrected cleft lip, midfacial hy-poplasia, narrow nose, eyebrow alopecia, and tightlycurled, very difficult-to-comb hair.
Figure 3. The boys impossible-to-comb, spun-glasshair.
56 Pediatric Dennatology Vol. 10 No. 1 March 1993
Figure 4. Two canals on a hair shaft (piii bicanalicuii)under scanning electron microscopy. (Magnification120x.)
ations were described perfectly. This dominantlyinherited syndrome includes hypohidrotic ectoder-mal dysplasia, clefts of the lip and palate, narrowdysplastic nails, hypospadias in males, and variableshort stature. Patients also have midfacial hypopla-sia with high forehead, narrow nose from the bridgeto the tip, hypoplastic maxilla, and small mouthwith thin vermilion border in the upper lip and amore prominent lower lip. The daughter of the firstfamily also had an absetit uvtila. The teeth are con-ical, and patients have various degrees of hypodon-tia on the upper as well as lower jaw. Caries aredescribed as important (3), and conductive hearingloss occurs in some patients (2). Our patients havethe most usual features of the syndrome, and arethe seventh family and twenty-second and -third re-ported in the literature. We particularly want to em-phasize the presence of hair shaft anomalies inthese siblings.
The first distinctive hair changes in RHS weredescribed in two Italian patients who had irregularpili tortilike twisting of the hair shafts (4). Subse-quently, Schroeder et al (5) described pili torti inRHS. In 1988, scanning electron microscopy andpolarizing microscopy showed irregularly shapedshafts with longitudinal canals along the axis in hairfrom patients with RHS (6). The authors stiggestedthe term pili canalicuii for this abnormality. Similarfindings were reported in three children with uo-combable hair syndrome, two of whom also hadRHS (7). Dupre et al (8) previously used the term
jrc 5
pili trianguli et canalicuii to describe their findingsof triangular-shaped hair shafts with longittidioai ca-nals in patients with uncombable hair syndrome.Our findings confirm that pili torti, as well as pilicanalicuii, can occur iti RHS.
Becatise we demotistrated two canals in some ofthe hair shafts, which showed quadrangular shapeon cross section on scanning electron microscopy,we suggest that the term pili trianguli et canalicuii istoo limiting and that only pili canalicuii should beemployed for the canallike defect found in manyhair shafts from patients with RHS and with un-combable hair syndrome. This is particularly rele-vant since even the hair shaft with only one canalmay show a triangular, reniform, or completely ir-regular shape under transverse section with scan-ning electron microscopy (9,10).
REFERENCES
1. Rapp RS, Hodgkin WE. Anhidrotic ectodermal dys-plasia: Autosomal dominant inheritance with palateand lip anomalies. J Med Genet 1968;5:26&-272.
2. Wannarachue N, Hall BD, Smith DW. Ectodermaldysplasia and multiple defects (Rapp-Hodgkin type).J Pediatr 1972;81:1217-1218.
3. Felding IB, Bjorklund LJ. Rapp-Hodgkin ectodermaldysplasia. Pediatr Dermatol 1990,7:126-131.
4. Silengo MC, Davi GF, Bianco R, et al. Distinctivehair changes (pili torti) in Rapp-Hodgkin ectodermaldysplasia syndrome. Clin Genet 1982;21:297-300.
5. Schroeder HW, Syber VP. Rapp-Hodgkin ectoder-mal dysplasia. J Pediatr 1987;n0:72-75.
Camacho et al: Rapp-Hodgkin Syndrome 57
6. Salinas CF, Montes GM. Rapp-Hodgkin syndrome:observation on ten cases and characteristic hairchanges (pili canalicuii). Birth Defects 1988;24:47-68.
7. Shelley WB, Shelley ED. Uncombable hair syn-drome: observations on response to biotin and occur-rence in siblings with ectoderma! dysplasias. J AmAcad Dermatol 1985;!3:97-102.
8. Dupre A, Bonafe JL, Litoux F, Victor M. Le syn-drome des cheveux incoiffables: pili trianguli et
10.
canalicuii. Ann Dermatol Venereol 1978;105:627-630.Ferrando J, Fontamau R, Gratacos MR, MascaroJM. Pili canalicuii ("cheveux incoiffables" ou "che-veux en fibre de verre"). Dix nouveaux cas avecetude au microscope electronique a balayage. AnnDennatol Venereol 1980; 106:243-247.Camacho-Martmez F, Ferrando J. Hair shaft dyspla-sias. Int J Dennatol 1988;27:71-80.