Embed Size (px)
Citation preview

Central Journal of Clinical Nephrology and Research
Cite this article: Ayar Y, Sayılar EI, Ersoy A, Göktaş SY, Akalın EH, et al. (2014) Rapidly Progressive Mucormycosis and Aspergillus Infection after Kidney Transplantation: Two Casereports. J Clin Nephrol Res 1(2): 1007.
*Corresponding authorYavuz Ayar, Uludag University School of Medicine, Gorukle-Nilufer, Bursa, Turkey, Tel: +905055416075; Fax: +902242951451; Email:
Submitted: 20 October 2014
Accepted: 27 October 2014
Published: 29 October 2014
Copyright© 2014 Ayar et al.
OPEN ACCESS
Keywords•Renal transplantation•Mucor•Aspergillus
Case Report
Rapidly Progressive Mucormycosis and Aspergillus Infection after Kidney Transplantation: Two Case ReportsYavuz Ayar1*, Emel Işıktaş Sayılar1, Alparslan Ersoy1, Sibel Yorulmaz Göktaş2, Emin Halis Akalın2, Uygar Levent Demir3, Mahmut Yavuz1 and Mustafa Güllülü1
1Department of Nephrology, Uludag University School of Medicine, Turkey2Department of ClinicalMicrobiologyand InfectionDiseases, Uludag University School of Medicine, Turkey3Department of Otorhinolaryngology, Uludag University School of Medicine, Turkey
Abstract
Invasive fungal infections are reasons of increased morbidity and mortality after solid organ transplantations like kidney transplantation. Aspergillussupp and Mucoralessupp are invasive infections which are common in hematologic diseases, diabetic ketoacidosis, neutropenic patients, immunocompromised patients such as HIV and organ transplant recipients. Rhinocerebral form is the most common Mucor type, and it may be accompanied by pulmonary involvement. Aspergillus involves sinopulmonary tract and it causes invasive sinus and pulmonary infections. Clinical manifestations and radiological views of Mucor and Aspergillus are similar to each other and can be seen together. We reported 53 and 51 year-old cadaveric renal transplant recipients who were complicated with post-transplant Mucor and Aspergillus infections.
IntroductIonMucoralesspp and Aspergillusspp are the most common
invasive fungal infections like Candidaspp and Cryptococcus. The incidence of these infections varies according to the type of organ transplantation, 5 to 17% in heart transplantation, 14 to 22% in simultaneous heart-lung transplantation, 2 to 42% in liver transplantation and 2 to 14 % in kidney transplantation [1-3]. Aspergillus incidence is 0.5-2.2% in renaltransplant recipients and mortality is nearly 88% [4,5].The incidence of invasive fungal infections with Mucor is 0.2-1.2% and mortality rate is 60 to 100 % [6] (Table 1).
Mucormycosis (Zygomycosis) sub-types are Rhizopus, Mucor, Rhizomucor, Absidia, Apophysomyces, Saksenaea, Cunninghemalla, Cokeromyces and Syncephalastrum.The most common forms are rhinocerebral and pulmonar types [1,7]. Aspergillus involves more sinopulmonary tract and leads to primary and secondary infections [8,9].The sub-types of Aspergillus are Allergic Bronchopulmonary Aspergillosis (ABPA), fungus ball, acuteinvasive aspergillosis and cronic necrotizing aspergillosis
[10]. Bothinfections are common in hematological diseases, neutropenia, immunocompromised patients (such as HIV), diabetes, renalfailure, organ transplantation and solid organ tumors [9].Patients, who have Aspergillusspp infections, present with dyspnea, fever, haemoptysis and cough. Involvement of nasal and paranasal cavities, orbita, palate, pharynx is seen commonly and this situation causes vision loss, swelling of face, edema and pain originating from orbita and spreading to head [7, 9-14].
Inour report we have twopatients with Mucoralesspp and Aspergillusspp infections which are diagonised in the early period of cadaveric kidney transplantion.The frequency of these two infections increases especially in the first six months after transplantations [8-11].
case 1
The first patient is 53 year-old female with chronic renal failure which has unknown etiology. She was receiving hemodialysis 3 times a week since eight years old. [12] Before cadaveric renal transplantation she had no signs and
Central
Ayar et al. (2014)Email:
J Clin Nephrol Res 1(2): 1007 (2014) 2/5
symptoms. Physical examination of the patient was normal. In post-transplant immunosuppressive therapy 100 mg/day of cyclosporin A (CsA), 1 g/day of mycophenolatemofetil (MMF), basiliximab (20mg on transplantation day) and prednisolone were used. The patient had sudden dyspnein postoperative first day. An image like pleural effusion in the right side was viewed in Chest X-RAY after placement of internal jugular catheter. Right hemothorax was diagnosed in the image of Computed tomography (CT) of thorax. After she had fever we used empirical intravenous (IV) Ceftriaxone (2 g/day) for 8 days. CsA was discontinued and MMF dose was increased to 2 g/day. Right chest tube was inserted. The patient had 2 L/day urine in the fourth day of hospitalization. Renal function of graft did not get better (urea 262 mg/dl and creatinine 6.2 mg/dl) and she had to continue to receive hemodialysis. Anti-thymocyte globulin (ATG) prophylaxis (100 mg/day) was given for 2 days. The patient’s chest tube was withdrawn after x-ray findings were resolved. In the sixth day after ceasing anti biotherapy the patient had fever, temperature of 38.7 0C. One urine and two blood cultures were positive with extended spectrum beta-lactamase (ESBL) E.coli 2g/day of meropenem was administered intravenously. In the postoperative eighth day renal function of graft returned normal ranges.
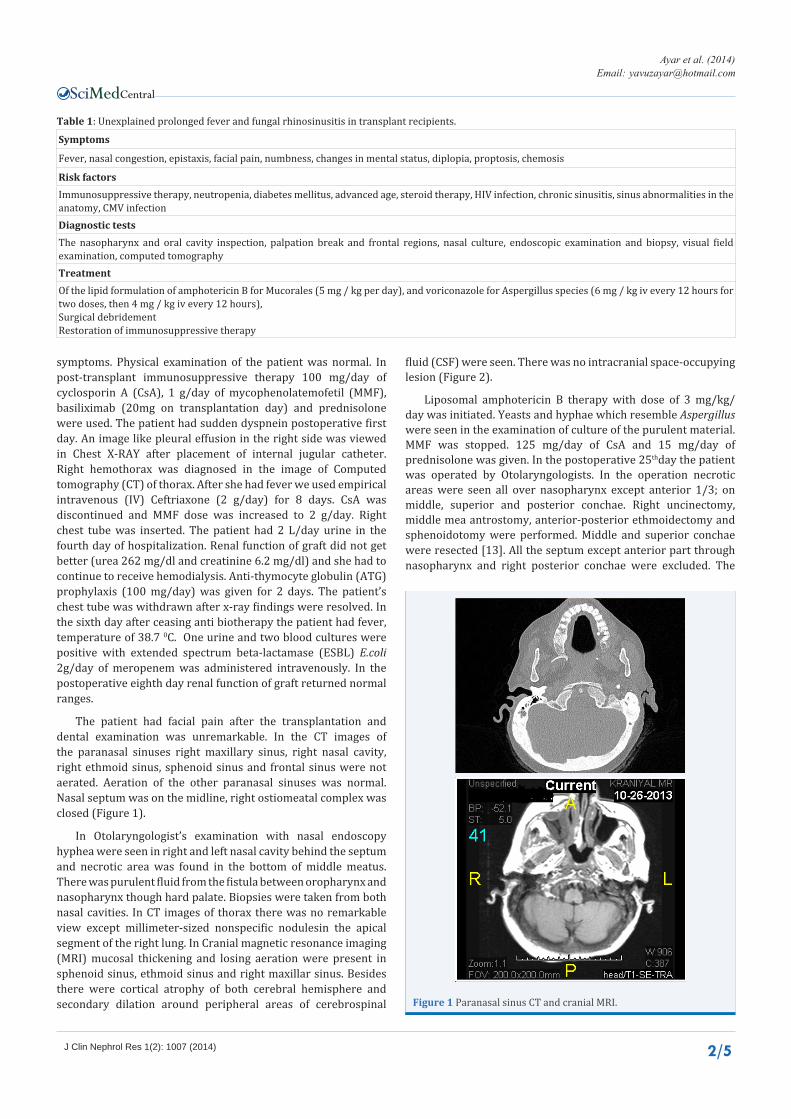
The patient had facial pain after the transplantation and dental examination was unremarkable. In the CT images of the paranasal sinuses right maxillary sinus, right nasal cavity, right ethmoid sinus, sphenoid sinus and frontal sinus were not aerated. Aeration of the other paranasal sinuses was normal. Nasal septum was on the midline, right ostiomeatal complex was closed (Figure 1).
In Otolaryngologist’s examination with nasal endoscopy hyphea were seen in right and left nasal cavity behind the septum and necrotic area was found in the bottom of middle meatus. There was purulent fluid from the fistula between oropharynx and nasopharynx though hard palate. Biopsies were taken from both nasal cavities. In CT images of thorax there was no remarkable view except millimeter-sized nonspecific nodulesin the apical segment of the right lung. In Cranial magnetic resonance imaging (MRI) mucosal thickening and losing aeration were present in sphenoid sinus, ethmoid sinus and right maxillar sinus. Besides there were cortical atrophy of both cerebral hemisphere and secondary dilation around peripheral areas of cerebrospinal
fluid (CSF) were seen. There was no intracranial space-occupying lesion (Figure 2).
Liposomal amphotericin B therapy with dose of 3 mg/kg/day was initiated. Yeasts and hyphae which resemble Aspergillus were seen in the examination of culture of the purulent material. MMF was stopped. 125 mg/day of CsA and 15 mg/day of prednisolone was given. In the postoperative 25thday the patient was operated by Otolaryngologists. In the operation necrotic areas were seen all over nasopharynx except anterior 1/3; on middle, superior and posterior conchae. Right uncinectomy, middle mea antrostomy, anterior-posterior ethmoidectomy and sphenoidotomy were performed. Middle and superior conchae were resected [13]. All the septum except anterior part through nasopharynx and right posterior conchae were excluded. The
Symptoms
Fever, nasal congestion, epistaxis, facial pain, numbness, changes in mental status, diplopia, proptosis, chemosis
risk factorsImmunosuppressive therapy, neutropenia, diabetes mellitus, advanced age, steroid therapy, HIV infection, chronic sinusitis, sinus abnormalities in the anatomy, CMV infectiondiagnostic testsThe nasopharynx and oral cavity inspection, palpation break and frontal regions, nasal culture, endoscopic examination and biopsy, visual field examination, computed tomographytreatmentOf the lipid formulation of amphotericin B for Mucorales (5 mg / kg per day), and voriconazole for Aspergillus species (6 mg / kg iv every 12 hours for two doses, then 4 mg / kg iv every 12 hours), Surgical debridement Restoration of immunosuppressive therapy
table 1: Unexplained prolonged fever and fungal rhinosinusitis in transplant recipients.
Figure 1 Paranasal sinus CT and cranial MRI.

Central
Ayar et al. (2014)Email:
J Clin Nephrol Res 1(2): 1007 (2014) 3/5
dose of liposomal amphotericin B was increased to 5 mg/kg/day. Therapy was continued with debridement. Mucormycosis was seen in histopathological examination from the surgical specimens of inferior conchae, septum and right nasal bone. After all these therapy renal function of graft was normal (serum urea 42 mg/dL, serum creatinine 0.7 mg/dL). Urine output of the patient was between 3-3.5 L. In control visits the lessions in nose and nasopharynx healed.
case 2
The second patient is a 51-year-old woman with end-stage renal disease due to chronic pyelonephritis. She had cadaveric renal transplantation in 2013 after 9 years of hemodialysis. Her immunosuppressive therapy was consisted of mycophenolatemofetil (MMF) and methylprednisolone after basiliximab induction. She had delayed graft function in the postoperative period. Renal imaging studies showed normal renal perfusion; severely decreased renal concentration in Mag-3 renal scintigraphy and elevated resistive index in doppler ultrasound. Renal allograft biopsy revealed normal histopathological findings except mild interstitial edema, intratubular calcification and vacuolar degeneration in tubular epithelial cells. [14] CD4d staining was negative. The patient was diagnosed with Acute tubular necrosis and rabbit anti-thymocyte globulin (ATG) was given for rejection prophylaxis. ATG was discontinued on fourth day because of leukopenia (1360/mm3). During this period, blood glucose levels were between180 to 230 mg/dL. On 10th
day, daily urine output increased to 500 cc. Then the patient had fever and hypotension. Laboratory findings of patients showed pyuria, high level of C-reactive protein (CRP) (22 mg/dL) and procalcitonin (>32.00 ng/mL). The patient was diagnosed with urosepsis. MMF was discontinued and teicoplanin, meropenem and fluconazole were initiated as antibiotherapy. Urine and blood cultures were positive with Extended Spectrum Beta-Lactamase (ESBL) E. coli. CMV-DNA (PCR) and serum galactomannan tests were negative. The chest high-resolution CT scan did not confirm findings of pulmonary infection in the both lungs. On 12th day she was transferred to intensive care unit (ICU) due to hypoxia and hypotension. Continuous veno venous hemo dia filtration (CVVHDF) was started. Tracheal aspirates yielded Acinetobacter baumannii. Colimycin was added to antibiotherapy. On 28th day a dark blue eschar due to zygomycosis was detected on the skin of the nose (Figure 3). Ecchymotic lesions were appeared on periorbital area including eyelids, back of nose and frontal area. Fluconazole was discontinued by considering possible invasive fungal infections and liposomal amphotericin-B with dose of 3 mg/kg/day was initiated. The lesions worsened, exophthalmia and chemosis were developed after 24 hours. Therefore dose of liposomal amphotericin-B was increased to 5 mg/kg/day and trimetoprimsulfametoxazol was added. In CT imaging of paranasal sinuses massive loss of sinus aeration and high density soft tissue shadow were seen in the paranasal sinus. Reduced discrimination between cortex-subcortex parts was seen on cranial CT, discrimination between gray matter and white matter could not be done and significant brain edema was observed. Similar findings were also reported for cerebellum and brain stem. In Otolaryngologist’s examination with nasal endoscopy showed a necrotic areas on left and right nasal cavities. The mycological examination of sample showed hyphae and spors on direct preparation; Aspergillus fumigatus, Aspergillus niger and Mucoralesspp were isolated from fungal culture. Necrosis on back of nose was more prominent on 31st day (Figure 4). The patient died in 36th day because of multi organ failure.
Figure 2 Mucor infection.
Figure 3 Necrosis Postoperative 28th day after transplantation.

Central
Ayar et al. (2014)Email:
J Clin Nephrol Res 1(2): 1007 (2014) 4/5
dIScuSSIonWe reported kidney transplant recipients developing
invasive fungal infections of Mucor and Aspergillus, in the early period after transplantation. Especially in the first six months after transplantation incidence of opportunistic invasive fungal infections is high. In this period clinical course progresses rapidly. In a study, Bodro et al. [15] in 9 liver, 8 kidneys and 3 heart transplant patients invasive fungal infection was seen. Fungal infections were observed in between 103 and 1195 days. Aspergillus was observed in two of these eight patients with renal transplantation. These patients had medical history of renal failure and medication with intensive antibiotics at last three months and high-dose steroid. Moulodi and his colleagues [16] reported that the incidence of Aspergillus pneumonia was 14.8%and the incidence of invasive Aspergillus was 3.7% among renal transplant recipients requiring ICU admissions during average of 10-month. In a study of Turkey 5 (4 living donor, 1 cadaveric donor) kidney transplant patients were complicated with Aspergillus pneumonia after the first 30-45 days of transplantation [17]. In another study conducted from China, 7 of the 89 patients were infected by Aspergillus in an average of 46 days after transplantation. 4 of them (57%) were died [18].
Jimenez et al. [19] made a study with 13 patients who had simultaneous pancreas-kidney transplantation. Two of them were diagnosed as Rhinocerebral Mucor infectionin an average of 65 day. After debridement of necrotic tissue and antibiotherapy of liposomal amphotericin B with dose of 3 mg/kg/day the patients were cured completely.In two studies from Korea and Iran 3 subjects, who were complicated by Mucor infection, were identified in 24 renal transplants. Although debridement and treatment with amphotericin B mortality rate were high. These patients were died [20,21]. A cadaveric renal transplant patient, who had intensive immunosuppressive medication with CsA, prednisolone, azothioprin and daclisumab induction, was diagnosed as acute rejection. After this subject got ATG,sirolimus,
MMF, prednisolone for rejection treatment Mucor infection was diagnosed in sixth week of transplantation. It was totally cured by debridement and amphotericin B with dose of 1 mg/kg/day [22]. In United State of America 116 patients with Mucor infection were reported. 73 of them were kidney recipients; 2 of them were simultaneous pancreas-kidney recipients. About half of these cases were died although amphotericin B and local surgical treatment [23].
Singh et al. [24] 50 of 100 patients with solid organ transplantation (16 renal transplant) were infected with Zygomycesin first sixth month of transplantation between 2003-2007. These patients had medical history of diabetes mellitus, organ transplantation, using intensive immunosuppressive drugs and antifungal drugs (voriconasole, caspofungin) 60% of patients were healed with local debridement and antifungal therapy (amphotericin B and posaconasole). Yassin et al. [25] reported a 41 year-old patient with hypertension and diabetes mellitus was infected with Rhizopus oryzae one week later after living donor kidney transplantation. In other study a living kidney transplant recipient, who was accepted as acute rejection, was reported and treated with10 sessions of plasmapheresis and rituximab 375 mg/m2/day [26]. In this case Mucor infection was identified after fever and headache one month later. After debridement and Amphotericin B treatment graft function was normal.
Diabetes mellitus, renal failure, haematological diseases, renal transplantation and immunocomprimisation are the major risk factors for invasive fungal infections. The time of operation, contamination of transplant kidney during transfer, latency of infection in donor kidney and immune comprimizing therapy after transplantation are the facilitating factors [3,9,11]. In our patients, renal failure, transplantation and immunosuppressive therapy are the facilitating factors for fungal infections.
Infection is one of the major causes of morbidity and mortality in renal transplant recipients. Invasive fungal infections such as Mucorale spp and Aspergillus spp are so difficult to be diagnosed and treated. As a result these infections have high mortality. Fungal infections are more common between first and sixth month after transplantation but they may appear earlier.
Our cases had early headache. After a few weeks fever began fungal infections were diagnosed. We think early persistent headache after transplantation may be alert symptom for fungal infection. Infections, caused by Mucorales spp and Aspergillus spp in early period, progress rapidly. As result early diagnosis of such fungal infections after transplantations has prognostic importance.
reFerenceS1. Prabhu RM, Patel R. Mucormycosis and entomophthoramycosis: a
review of the clinical manifestations, diagnosis and treatment. Clin Microbiol Infect. 2004; 10 Suppl 1: 31-47.
2. Eucker J, Sezer O, Graf B, Possinger K. Mucormycoses. Mycoses. 2001; 44: 253-260.
3. Patel R, Paya CV. Infections in solid-organ transplant recipients. Clin Microbiol Rev. 1997; 10: 86-124.
4. Ergin F, Arslan H, Azap A, Demirhan B, Karakayali H, Haberal M. Invasive aspergillosis in solid-organ transplantation: report of eight cases and review of the literature. Transpl Int. 2003; 16: 280-286.Figure 4 Necrosis Postoperative 31st day after transplantation.

Central
Ayar et al. (2014)Email:
J Clin Nephrol Res 1(2): 1007 (2014) 5/5
Ayar Y, Sayılar EI, Ersoy A, Göktaş SY, Akalın EH, et al. (2014) Rapidly Progressive Mucormycosis and Aspergillus Infection after Kidney Transplantation: Two Casereports. J Clin Nephrol Res 1(2): 1007.
Cite this article
5. Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature. Clin Infect Dis. 2001; 32: 358-366.
6. Godara SM, Kute VB, Goplani KR, Gumber MR, Gera DN, Shah PR, et al. Mucormycosis in renal transplant recipients: predictors and outcome. Saudi J Kidney Dis Transpl. 2011; 22: 751-756.
7. Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005; 41: 634-653.
8. Denning DW, Evans EG, Kibbler CC, Richardson MD, Roberts MM, Rogers TR, et al. Guidelines for the investigation of invasive fungal infections in haematological malignancy and solid organ transplantation. British Society for Medical Mycology. Eur J Clin Microbiol Infect Dis. 1997; 16: 424-436.
9. Linden E, Restrepo D, Dikman S, Murphy B, Huprikar S. Aspergillus infection limited to renal allograft: case report and review of literature. Transpl Infect Dis. 2006; 8: 177-181.
10. Koselj-Kajtna M, Kandus A, Rott T, Zver S, Zupan I, Koselj M, et al. Aspergillus infection in immunocompromised patients. Transplant Proc. 2001; 33: 2176-2178.
11. Paya CV. Fungalinfections in solid-organ transplantation. Clin Infect Dis. 1993; 16: 677-688.
12. Grossi P, Farina C, Fiocchi R, Dalla Gasperina D. Prevalence and outcome of invasive fungal infections in 1,963 thoracic organ transplant recipients: a multicenter retrospective study. Italian Study Group of Fungal Infections in Thoracic Organ Transplant Recipients. Transplantation. 2000; 70: 112-116.
13. Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in human disease. Clin Microbiol Rev. 2000; 13: 236-301.
14. Severo CB, Guazzelli LS, Severo LC. Chapter 7: zygomycosis. J Bras Pneumol. 2010; 36: 134-141.
15. Bodro M, Sabé N, Gomila A, Ayats J, Baliellas C, Roca J, Melilli E. Risk factors, clinical characteristics, and outcomes of invasive fungal infections in solid organ transplant recipients. Transplant Proc. 2012; 44: 2682-2685.
16. Mouloudi E, Massa E, Georgiadou E, Iosifidis E, Katsika E, Rembelakos
G, et al. Infections related to renal transplantation requiring intensive care admission: a 20-year study. Transplant Proc. 2012; 44: 2721-2723.
17. Usta M, Kahvecioglu S, Akdag I, Gullulu M, Ozdemir B, Ener B, et al. Aspergillus pneumonia in renal transplant recipients at a medical center in Turkey. Transplant Proc. 2004; 36: 2703-2707.
18. Zhang XD, Hu XP, Yin H, Wang W, Zhang X, Ma LL, et al. Aspergillus pneumonia in renal transplant recipients. Chin Med J (Engl). 2008; 121: 791-794.
19. Jiménez C, Lumbreras C, Aguado JM, Loinaz C, Paseiro G, Andrés A, et al. Successful treatment of mucor infection after liver or pancreas-kidney transplantation. Transplantation. 2002; 73: 476-480.
20. Lee EJ, Chung JW, Choi S, Kim YS, Woo JH. [Forefront of diagnosis and treatment of deep-steam mycology in Korea--rhinoorbitocerebral zygomycosis]. Nihon Ishinkin Gakkai Zasshi. 2009; 50: 229-233.
21. Hosseini SM, Borghei P. Rhinocerebral mucormycosis: pathways of spread. Eur Arch Otorhinolaryngol. 2005; 262: 932-938.
22. Lakshminarayana G, Rajesh R, Kurian G, Unni VN. Zygomycosis in a renal allograft recipient. Indian J Nephrol. 2009; 19: 30-33.
23. Almyroudis NG, Sutton DA, Linden P, Rinaldi MG, Fung J, Kusne S. Zygomycosis in solid organ transplant recipients in a tertiary transplant center and review of the literature. Am J Transplant. 2006; 6: 2365-2374.
24. Singh N, Aguado JM, Bonatti H, Forrest G, Gupta KL, Safdar N, et al. Zygomycosis in solid organ transplant recipients: a prospective, matched case-control study to assess risks for disease and outcome. J Infect Dis. 2009; 200: 1002-1011.
25. Yassin MA, Taj-Aldeen SJ, Khan FY, Errayes M, Aref E. Rhino-orbital zygomycosis secondary to Rhizopus oryzae in a renal transplant recipient successfully treated with liposomal amphotericin B. Chang Gung Med J. 2008; 31: 407-411.
26. Bakr A, Wafa E, Fouda A, Elagroudy A, Gheith O, Sobh M, et al. Successful treatment of mucormycosis in a renal allograft recipient. Clin Exp Nephrol. 2008; 12: 207-210.





























