Embed Size (px)
Citation preview

Rapid HIV Tests
Norman Moore, Ph.D.
Director of Medical Affairs

A majority of the information in this lecture was taken from the CDC Lecture by Bernard Branson, M.D.
Associate Director for Laboratory DiagnosticsDivisions of HIV/AIDS Prevention
National Center for HIV, STD, and TB PreventionCenters for Disease Control and Prevention
The views of Dr. Branson are not necessarily the official views of the CDC.

HIV/AIDS Diagnoses among Adults and Adolescents, by Transmission Category — 33 States, 2001–2005
MSM63%
IDU15%
Heterosexual17%
MSM/IDU 5%
Other 1%
Males(n ≈133,000)
Females(n ≈52,000)
Heterosexual78%
IDU21%
Other 1%
HIV/AIDS Surveillance Report, 2005

Number HIV infected 1,039,000 – 1,185,000
Number unaware of their HIV infection 252,000 - 312,000 (24%-27%)
Estimated new infections annually 40,000
Awareness of HIV Status among Persons with HIV, United States
Glynn M, Rhodes P. 2005 HIV Prevention Conference

Late HIV Testing is CommonSupplement to HIV/AIDS Surveillance, 2000-2003
• Among 4,127 persons with AIDS*, 45% were first diagnosed HIV-positive within 12 months of AIDS diagnosis (“late testers”)
• Late testers, compared to those tested early (>5 yrs before AIDS diagnosis) were more likely to be:– Younger (18-29 yrs)– Heterosexual– Less educated– African American or Hispanic
MMWR June 27, 2003
*16 states

0%
20%
40%
60%
80%
100%
Illness Self/partnerat risk
Wanted toknow
Routinecheck up
Required Other
Late (Tested < 1 yr before AIDS dx)
Early (Tested >5 yrs before AIDS dx)
Reasons for testing: late versus early testersSupplement to HIV/AIDS Surveillance, 2000-2003

Previous Recommendations

Previous CDC RecommendationsAdults and Adolescents
• Routinely recommend HIV screening in acute-care hospital settings with HIV prevalence >1%
• Targeted testing based on risk assessment in clinical settings with lower HIV prevalence

HIV Testing Practices in EDs
• Survey of 154 ED providers– Average: 13 STD patients per week– Only 10% always recommend HIV test
• Reasons for not testing for HIV:– 51% concerned about follow up– 45% not a “certified” counselor– 19% too time-consuming– 27% HIV testing not available
-Fincher-Mergi et al, 2002: AIDS Pat Care STDs

Previous CDC RecommendationsPregnant Women
• Routine, voluntary HIV testing as a part of prenatal care, as early as possible, for all pregnant women
• Simplified pretest counseling
• Flexible consent process

Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant
Women in Health-Care Settings
MMWR 2006;55 (No. RR-14):1-17
Published September 22, 2006
http://www.cdc.gov/mmwr/pdf/rr/rr5514.pdf

Revised RecommendationsAdults and Adolescents - I
• Routine, voluntary HIV screening for all persons 13-64 in health care settings, not based on risk
• All patients with TB, or seeking treatment for STDs, should be screened for HIV
• Repeat HIV screening of persons with known risk at least annually

Revised RecommendationsAdults and Adolescents - II
• When acute retroviral infection is a possibility, use an RNA test in conjunction with an HIV antibody test
• Settings with low or unknown prevalence:– Initiate screening
– If yield from screening is less than 1 per 1000, continued screening is not warranted

Revised RecommendationsAdults and Adolescents - III
• Opt-out HIV screening with the opportunity to ask questions and the option to decline testing
• Separate signed informed consent should not be required
• Prevention counseling in conjunction with HIV screening in health care settings should not be required

Revised RecommendationsAdults and Adolescents - IV
• Screening is voluntary
• Inform patients orally, or in writing, that HIV testing will be performed unless they decline.
• Arrange access to care, prevention, and support services for patients with positive HIV test results

Rationale for Revising CDC Recommendations
• Many HIV-infected persons access health care but are not tested for HIV until symptomatic
• Effective treatment available
• Awareness of HIV infection leads to substantial reductions in high-risk sexual behavior
• Inconclusive evidence about prevention benefits from typical counseling for persons who test negative
• Great deal of experience with HIV testing, including rapid tests

Veterans Health System
• December 2008 – The Veterans’ Mental Health and Other Care Improvements Act of 2009 repealed the limitation on HIV screening.
• August 2009 Written consent is no longer required for HIV testing in the VHA– Patients only need to provide verbal informed consent prior
to HIV testing
• VHA National HIV Program Directive– HIV testing should be a part of routine medical care and pro

Criteria that Justify Routine Screening
1. Serious health disorder that can be detected before symptoms develop
2. Treatment is more beneficial when begun before symptoms develop
3. Reliable, inexpensive, acceptable screening test
4. Costs of screening are reasonable in relation to anticipated benefits
5. Treatment must be accessible
-WHO Public Health Paper, 1968Principles and Practice of Screening for Disease
Knowledge of HIV Infection and Behavior
Meta-analysis of high-risk sexual behavior in personsaware and unaware they are infected with HIV in the U.S. Marks G, et al. JAIDS. 2005;39:446
After people become aware they are HIV-positive, the prevalence of high-risk sexual behavior is reduced substantially.
Reduction in Unprotected Anal orVaginal Intercourse with HIV-neg partners: HIV-pos Aware vs. HIV-pos Unaware
68%


Effect of Counseling in Conjunction with HIV Testing
• Meta-analysis of 27 studies of HIV-CT:
– HIV-positive participants reduced unprotected intercourse and increased condom use.
– HIV-negative participants did not modify their behavior more than untested participants.
- Weinhardt et al, 1999: Am J Public Health

Opt-Out Screening
Prenatal HIV testing for pregnant women:• RCT of 4 counseling models with opt-in consent:
- 35% accepted testing- Some women felt accepting an HIV test indicated high
risk behavior
• Testing offered as routine, opportunity to decline- 88% accepted testing- Significantly less anxious about testing
Simpson W, et al, BMJ June,1999

Cost Effectiveness
• Expanded screening for HIV in the U.S. – an analysis of cost effectiveness. Paltiel AD, et al. NEJM 2005;352:586. “In all but the lowest-risk populations, routine,
voluntary screening for HIV once every 3 to 5 years is justified on both clinical and cost-effectiveness grounds. One-time screening in the general population may also be cost-effective.”

Cost Effectiveness
• Prenatal HIV screening– Averts ~1500 cases of neonatal HIV per year– Cost saving
• HIV antibody testing of 15 million blood donations– Averts ~1500 HIV infections per year– Costs $3,600 per QALY
• Pooled RNA screening for HIV and HCV– Averts 4 HIV and 56 HCV infections per year– Costs $4.3 million per QALY
HIV Rapid Tests

Role for Rapid HIV Tests
• Increase receipt of test results
• Increase identification of HIV-infected pregnant women so they can receive effective prophylaxis
• Increase feasibility of testing in acute-care settings with same-day results
• Increase number of venues where testing can be offered to high-risk persons

HIV Testing Can Be Done in Unusual Places

Rapid Lateral Flow Tests
• Capture antibody or antigen immobilized as a line on nitrocellulose
• Detector antibody or antigen is a gold particle or latex particle

Generations of Rapid Tests
• 1st Generation – Detect antibody to HIV with viral lysate
• 2nd Generation – Detect antibody to HIV with recombinant proteins or synthetic peptides
• 3rd Generation – Detect both IgG and IgM antibody to HIV
• 4th Generation – Detect antibody and viral protein

Detection of HIV by Diagnostic Tests

Uni-Gold Recombigen™
Multispot HIV-1/HIV-2
Reveal® G3
OraQuick Advance®
Clearview® COMPLETE HIV 1/2
Clearview® HIV 1/2 STAT-PAK®

FDA-approved Rapid HIV Tests
Sensitivity
(95% C.I.)
Specificity
(95% C.I.)
Whole blood
OraQuick Advance®
Uni-Gold Recombigen™
Clearview® HIV 1/2
STAT-PAK®
Clearview® COMPLETE
HIV 1/2
99.6 (98.5 - 99.9)
100 (99.5 – 100) 99.7 (98.9 – 100)
99.7 (98.9 – 100)
100 (99.7-100)
99.7 (99.0 – 100)
99.9 (98.6 – 100)
99.9 (98.6 – 100)
Serum/plasma
Reveal® G3
Multispot
99.8 (99.2 – 100)
100 (99.9 – 100)
99.9 (98.6 – 100)
99.9 (99.8 – 100)

OraQuick Advance® HIV-1/2
• CLIA-waived for finger stick, whole blood, oral fluid
• Store at room temperature
• Screens for HIV-1 and 2
• Read time 20-40 minutes
• Shelf life: 1 year

Collect oral fluid specimens by swabbing gums with test device.
Reduce hazards, facilitate testing in field settings.

Insert device; test develops in 20 minutes.

PositiveNegative
Reactive Control
Positive HIV-1/2
Read results in 20 – 40 minutes.

Uni-Gold Recombigen™
• CLIA-waived for finger stick, whole blood
• Store at room temperature
• Screens for HIV-1
• Detects IgG and IgM
• Read time 10-12 minutes
• Shelf life: 1 year

Fingerstick with disposable pipette

Add 1 drop specimen to well

Add 4 drops of wash solution

Read results in 10 minutes
Positive Negative
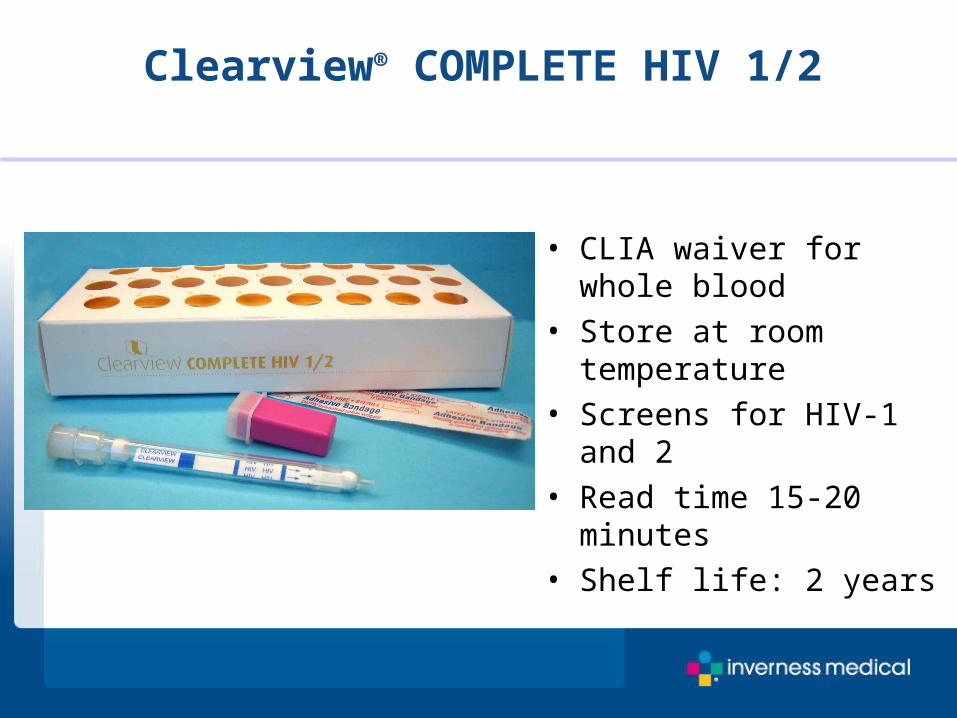
Clearview® COMPLETE HIV 1/2
• CLIA waiver for whole blood
• Store at room temperature
• Screens for HIV-1 and 2• Read time 15-20 minutes• Shelf life: 2 years

Obtain fingerstick blood sample

Insert device into buffer vial.

Read results in 15-20 minutes

Clearview® HIV-1/2 STAT-PAK®
• CLIA-waived for whole blood and fingerstick
• Store at room temperature
• Screens for HIV-1 and 2• Read time 15-20 minutes• Shelf life: 2 years

Obtain fingerstick specimen.

Add 5 microliters specimen.

Add 3 drops buffer to well.

Read results in 15-20 minutes.

Summary
• There is an urgent need to increase the proportion of persons who are aware of their HIV-infection status
• Expanded, routine, voluntary, opt-out screening in health care settings is needed
• Such screening is cost-effective• Revised recommendations: September 2006





























