-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
1/6
Papers
Randomised controlled trial of ultrasonography indiagnosis of
acute appendicitis, incorporating theAlvarado scoreCharles D
Douglas, Neil E Macpherson, Patricia M Davidson, Jonathon S
Gani
Abstract
ObjectivesTo determine whether diagnosis bygraded compression
ultrasonography improvesclinical outcomes for patients with
suspected
appendicitis.DesignA randomised controlled trial
comparingclinical diagnosis (control) with a diagnostic
protocolincorporating ultrasonography and the Alvaradoscore
(intervention group).SettingSingle tertiary referral
centre.Participants302 patients (age 5-82 years) referred tothe
surgical service with suspected appendicitis. 160patients were
randomised to the intervention group,of whom 129 underwent
ultrasonography.Ultrasonography was omitted for patients
withextreme Alvarado scores (1-3, 9, or 10) unlessrequested by the
admitting surgical team.Main outcome measuresTime to operation,
durationof hospital stay, and adverse outcomes,
includingnon-therapeutic operations and delayed treatment
inassociation with perforation.ResultsSensitivity and specificity
of ultrasonographywere measured at 94.7% and 88.9%,
respectively.Patients in the intervention group who
underwenttherapeutic operation had a significantly shortermean time
to operation than patients in the controlgroup (7.0v10.2 hours, P =
0.016). There were nodifferences between groups in mean duration
ofhospital stay (53.4v54.5 hours, P = 0.84), proportionof patients
undergoing a non-therapeutic operation(9%v11%, P = 0.59) or delayed
treatment inassociation with perforation (3%v1%, P =
0.45).ConclusionGraded compression ultrasonography is
an accurate procedure that leads to the promptdiagnosis and
early treatment of many cases ofappendicitis, although it does not
prevent adverseoutcomes or reduce length of hospital stay.
Introduction
Acute appendicitis is one of the commonest surgicalemergencies.
Simple appendicitis can progress to per-foration, which is
associated with a much highermorbidity and mortality, and surgeons
have thereforebeen inclined to operate when the diagnosis
isprobable rather than wait until it is certain. 1 A clinical
decision to operate leads to the removal of a normalappendix in
15% to 30% of cases (although the figuremay be higher or lower in
certain demographicgroups).1 This proportion may be reduced by
observing equivocal cases for a period of time, a prac-tice that
seems to be safe for most patients.2 Some casesof appendicitis may
resolve spontaneously.3 4 None theless, if a period of observation
culminates in thediagnosis of a ruptured appendix, the patient may
havesuffered a poor outcome that was avoidable. Reduc-tions in the
number of unnecessary or non-therapeutic operations should not be
achieved at theexpense of an increase in number of
perforations.5
It has been claimed that diagnostic aids candramatically reduce
the number of appendicectomiesin patients without appendicitis, the
number ofperforations, and the time spent in hospital. 1
Methodsadvocated to assist in the diagnosis of appendicitisinclude
laparoscopy,6 7 scoring systems,8 9 computer
programs,10 ultrasonography,11 computed tomogra-phy,12 and
magnetic resonance imaging.13 Imagingtechniques have been shown to
be particularlyaccurate.14 Graded compression ultrasonography is
theleast expensive and least invasive of these and has beenreported
to have an accuracy of 71% to 95%,14 butdoubts have been raised
about the influence ofultrasonography on patient outcomes.15
Furthermore,it has been argued that findings at sonography
shouldnot supercede clinical judgment in patients with a
highprobability of appendicitis.16 This raises questionsabout
whether sonography should be performed at allin patients at high
risk and whether there is some reli-able means of selecting those
who can benefit from
imaging.The Alvarado score is a 10 point scoring system forthe
diagnosis of appendicitis based on clinical signsand symptoms and a
differential leucocyte count (seetable 5). In his original paper
Alvarado recommendedan operation for all patients with a score of 7
or moreand observation for patients with scores of 5 or 6.8
Subsequent prospective studies have suggested thatthe Alvarado
score alone is inadequate as a diagnostictest,17 18 but it has been
advocated as a means of select-ing patients who should undergo
imaging.19
We designed a diagnostic protocol incorporatinggraded
compression ultrasonography and the
Department ofSurgery, JohnHunter Hospital,NSW 2310,Australia
Charles D Douglas
surgical registrar
Faculty of Medicineand HealthSciences, Universityof
Newcastle,Callaghan NSW2308, Australia
Neil E Macphersonmedical student
Patricia M Davidsonassociate professor of
paediatric surgery
Jonathon S Ganisenior lecturer
Correspondence to:CD [email protected]
BMJ 2000;321:17
1BMJ VOLUME 321 14 OCTOBER 2000 bmj.com
-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
2/6
Alvarado score on the basis of work in our own institu-tion.20
We then undertook a randomised controlledtrial to assess whether
the information provided by theprotocol improved clinical outcomes.
We tested thehypotheses that compared with standard
treatmentpatients assigned to the diagnostic protocol wouldhave a
shorter mean duration of hospital stay; a lowerrate of unnecessary
(non-therapeutic) operations; ashorter mean time to surgery for
those undergoing
therapeutic operations; and an equal or lower rate ofdelayed
treatment in association with perforation.
Methods
Ethics committee approval was obtained for this trial.Patients
were considered for inclusion in the study ifthey were referred to
the surgical service at JohnHunter Hospital and John Hunter
Childrens Hospitalwith a provisional diagnosis of acute
appendicitisbetween October 1997 and October 1998. All
generalsurgeons (six), paediatric surgeons (three), and
theirregistrars (seven) at the participating hospital wereinvolved
in the study.
Patients were excluded from randomisation if theyfulfilled any
of the following criteria: age less than 5years; evidence of
generalised peritonitis; palpablemass in the right iliac fossa;
evidence of acuteconfusional state or dementia; graded
compressionultrasonography already performed. All other
patientswere met by the project officer, a third year
medicalstudent, who explained the study and obtainedconsent. The
project officer randomly allocatedpatients by coin toss to control
(standard treatment) ordiagnostic protocol (intervention) groups.
He organ-ised a leucocyte count and performed a structuredclinical
assessment from which he calculated theAlvarado score (modified
only by using percussiontenderness in the place of rebound
tenderness).
For patients in the control group, members of theadmitting
surgical team were not informed of theAlvarado score. They
proceeded with appropriateclinical assessment and management. They
wererequested not to organise graded compressionultrasonography for
36 hours.
For patients in the intervention group, the projectofficer
advised the admitting team of the Alvaradoscore. Ultrasonography
was then organised if theAlvarado score was between 4 and 8,
inclusive. AnAlvarado score of 9 or 10 was taken to be a
relativeindication for surgery, but the admitting team wasgiven the
option of organising graded compressionultrasonography; patients
with an Alvarado of 3 or lesswere not eligible for ultrasonography.
The admitting
team was advised of the result of ultrasonographywhen this was
done.
UltrasonographyGraded compression ultrasonography results
weredesignated positive, negative, or equivocal by theattending
sonographer by using the following criteria:positiveappendix
identified, tender and non-compressible or appendiceal phlegmon or
abscessseen; negativeappendix not identified, no otherrelevant
abnormality seen; equivocalappendix notidentified but abnormal
amount of free fluid seen withthickened, dilated, or
non-peristaltic bowel in the
region of the caecum. In our experience these latterfindings are
often associated with perforation, and wesuggested to participating
surgeons and registrars thatit was safest to consider such a report
as a positiveresult.
In the few cases when the appendix was identifiedbut was
compressible or not tender we asked thesonographer to make a
judgment on the basis of his orher experience and any other
sonographic infor-
mation, including appendiceal dimensions and bloodflow. This
reporting system was based on the results ofa prospective study at
our hospital (unpublished).
Ultrasonography was unavailable at this institutionbetween the
hours of 10 pm and 8 am, and patientsentered in the study between
these times had theirexamination at 8 am, unless the admitting
surgicalteam deemed an immediate operation to be necessary.
SurgeryAll patients who underwent laparotomy or laparos-copy for
suspected appendicitis had an appendicec-tomy. The diagnosis of
appendicitis was made onhistological grounds on the basis of
infiltration of themuscularis propria by neutrophil
granulocytes.
A patient was considered to have had an operationif laparotomy
or laparoscopy was performed. Opera-tions were considered to be
therapeutic if disease wasfound, when the disease seemed to be the
cause for thepatients pain, and when surgery was the
appropriatetreatment for that disease. All other operations
wereclassed as non-therapeutic operations. Operationswere
considered to be non-therapeutic if the onlyabnormality was a
non-inflamed appendix containinga faecolith.
PerforationsThe appendix (or bowel) was considered to
beperforated if the surgeon clearly identified a perfora-tion or a
peritoneal swab grew at least one definite
bowel organism or the histopathologist identified aperforation
in association with gangrene or full-thickness necrosis.
Delayed treatment in association with perforationFor patients
with perforation, treatment was consid-ered to be delayed if
surgery had not started within 10hours of randomisation.
Follow upPatients were reviewed at one week and three monthswith
a pro-forma assessment. When direct review wasnot possible, details
were obtained from the patientsgeneral practitioner or surgeon.
Outcomes
We identified four outcome measures.Time to operation for
therapeutic operations was
defined as the time in hours from randomisation toskin
preparation.
Duration of stay was defined as the time in hoursfrom
randomisation to discharge from hospital. Whena patient was
discharged and then readmitted forongoing management of a
complication of acuteappendicitis the duration of the subsequent
admissionwas added to the first.
Rate of non-therapeutic operationsThis was thenumber of
non-therapeutic operations (see above) as aproportion of the total
number in each group.
Papers
2 BMJ VOLUME 321 14 OCTOBER 2000 bmj.com
-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
3/6
Rate of delayed treatment in association with perforationwas the
number of cases of delayed treatment inassociation with perforation
(as defined above) dividedby the total number in each group.
PowerThis sample had a power of 80% to detect a
differencebetween groups of 3.3 hours for mean time to theatre,15.2
hours for mean duration of stay, and a reduction
in the non-therapeutic operation rate from 11% to 2%.
Data analysisData were analysed on an intention to treat basis.
Forcalculation of sensitivity and specificity of graded
com-pression ultrasonography we included cases only if
ahistological diagnosis was available. Diagnoses otherthan
appendicitis were ignored. Equivocal ultrasonog-raphy reports were
counted as positive. Thus if theresults of graded compression
ultrasonography werereported as positive or equivocal for
appendicitis but aperforated diverticulum and normal appendix
werefound at operation, the test was counted as a false posi-tive,
even though the operation was consideredtherapeutic.
Two by two contingency tables were analysed byPearsons 2 test
(or Fishers exact test when stated), andcomparisons of means were
analysed by a two tailedttest. Confidence intervals for single
proportions werecalculated with the Wilson procedure without
correc-tion for continuity.21
Results
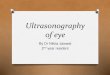
Figure 1 shows the trial profile. In total 306 patientswere
referred for inclusion; two patients failed to meetinclusion
criteria and two patients refused consent,thus 302 patients were
enrolled in the study, with 160in the intervention group and 142 in
the controlgroup. The mean age was slightly lower in the
intervention group (20.2 v 23.5 years); 202 patientswere aged 14
years and over and 100 were aged under14 years. There was little
difference between groupswith respect to sex, mean Alvarado score,
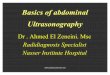
orproportion with Alvarado score greater than 6. Figure2 shows the
distribution of Alvarado scores. Table 1summarises the results.
Subgroup analysis by age isshown in table 2.
Sixteen patients were in breach of the trial protocolbecause the
admitting surgeon in each case thoughtthat this was in the patients
interests. All were includedin the reported analysis on an
intention to treat basis.The results of a secondary analysis with
these patientsexcluded were not substantially different with
respectto adverse outcomes (intervention 17/154 (11%; 95%
confidence interval 7% to 17%) v control 16/132(12.1%; 8% to
19%); P = 0.8) or duration of stay (inter-vention 53.1 (46 to 60)
hours vcontrol 53.0 (44 to 62)hours; P = 0.99).
UltrasonographyGraded compression ultrasonography was
performedin 139 patients (see table 3). The sensitivity and
specifi-city of ultrasonography for diagnosing appendicitiswas
94.7% and 88.9%, respectively. There were threefalse negative
results. Six patients with a positive orequivocal result on
ultrasonography recovered withoutsurgery.
SurgeryThere were 170 operations performed: 95 of the
160patients in the intervention group underwent surgerycompared
with 75 of the 142 patients in the controlgroup (59.4%v52.8%, P =
0.25). Appendicitis was con-firmed histologically in 128 patients:
73 (45.6%; 38% to53%) in the intervention group and 55 (38.7%; 31%
to47%) in the control group (P = 0.23). There were 13patients with
other conditions that met the criteria fora therapeutic operation
(see table 4). Twenty nine
operations were non-therapeutic: 14 (8.8%; 5.3% to14.2%) in the
intervention group and 15 (10.6%; 6.5%to 16.7%) in the control
group (P = 0.59).
PerforationsTwenty four patients had perforations, 19 had a
perfo-rated appendicitis (14.8% (10% to 22%) of all cases of
Referred to surgical servicewith suspected appendicitis
n=306
Randomisedn=302
Intervention groupn=160
Alvarado 4-8n=106
(one incomplete score)
Alvarado 8n=50
Ultrasonographyn=101
(5 protocol breach)
2 patients lost to follow up at three months(both had had
appendicectomy)
2 patients lost to followup at three months
(one appendicectomy,one negative result
on ultrasonography)
Ultrasonographyn=1
(protocol breach)
Ultrasonographyn=27
Ultrasonographyn=10
(all protocol breach)
Control groupn=142
Refusals n=2Exclusions n=2
Fig 1 Profile of trial of graded compression ultrasonography and
Alvarado score comparedwith clinical methods in diagnosis of
appendicitis
Table 1 Demographics and results according to allocation to
diagnosis with graded
compression ultrasonography and Alvarado score or clinical
diagnosis only. Results are
given with 95% confidence intervals unless stated otherwise
Intervention (n=160) Control (n=142)
No male 87 69
Mean age (years) 20.2 23.5
Alvarado score
Mean score 7.18 6.93
No (%) with score >6 99 (61.9) 86 (60.6)
Hospital data
Total No (%) of operations 95 (59.4; 52 to 67) 75 (52.8; 45 to
61)
No (%) of therapeutic operations 81 (50.6; 43 to 58) 60 (42. 3;
34 to 50)
Me an ti me t o t he ra pe uti c o pe ra ti on ( ho ur s) 7. 0 (
5. 9 to 8. 1) 1 0. 2 ( 7. 9 t o 1 3)
Mean duration of stay (hours) 53.4 (47 to 60) 54.5 (46 to
63)
N o ( %) of no n- the ra pe uti c o pe ra ti on s 14 ( 8. 8; 5.
3 t o 14 ) 15 ( 10 .6; 6. 5 to 17 )
No (%) with delayed treatment in association withperforation
5 (3.1; 1.3 to 7.1) 2 (1.4; 0.4 to 5.0)
Total (%) adverse outcomes (delayed treatment inassociation with
perforation and non-therapeuticoperations)
19 (11.9; 7.7 to 18) 17 (12.0; 7.6 to 18)
Papers
3BMJ VOLUME 321 14 OCTOBER 2000 bmj.com
-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
4/6
appendicitis) and five had other bowel perforations. Ofall
perforations, 14 were in the intervention group and10 in the
control group (perforations/number ingroup of 8.8% (5.3% to 14%)
and 7.0% (3.9% to 12%),respectively, P = 0.58).
Delayed treatment in association with perforationThere were
seven cases of delayed treatment in associ-ation with perforation
(six cases of appendicitis andone of perforation of a caecal
carcinoma). Five of thesewere in the intervention group and two
were in the
control group (3.1% v1.4%, P = 0.45, Fishers exacttest).
Follow upThere were no readmissions with appendicitis duringthe
follow up period. Two patients required readmis-sion for
complications: one in the intervention groupfor drainage of an
abscess and one in the controlgroup for an early small bowel
obstruction. Ninepatients had minor wound infections diagnosed
oneweek after discharge (4v5, P = 0.51, Fishers exact test).Four
patients were lost to follow up at three months,three of whom had
had their appendix removedduring their admission (and were
therefore able to beanalysed for all end points); the fourth, in
the control
group, had had a negative result on ultrasonographybefore
discharge.
Discussion
We have confirmed the high sensitivity and specificityof graded
compression ultrasonography in thediagnosis of appendicitis. All
our patients whounderwent surgery after a positive result on
ultra-sonography proved to have appendicitis. Patients
withequivocal signs of appendicitis are usually admitted tohospital
for a day or night of observation. If the resulton graded
compression ultrasonography is positive,however, the surgeon can
operate immediately. In ourstudy, this lead to a significant
reduction in mean time
to therapeutic operation.As some cases of appendicitis seem to
resolve with-
out surgery,3 4 however, graded compression ultra-sonography
could lead to an increase in therapeuticoperations (by correctly
diagnosing appendicitis inpatients who may have recovered during a
period ofobservation). Our results are consistent with this, with
ahigher proportion of therapeutic operations occurringin the
intervention group, although the difference wasnot significant.
This is despite the fact that Alvaradoscores were similarly
distributed between groups.
The reduced time to operation in the inter ventiongroup did not
result in a reduced duration of hospital
25
20
15
10
5
01
0.7 0.60.7
1.9
3.5 3.8
7.7
16.9
14.8 14.4
12.0
14.4
13.4
16.3
22.5 22.5
16.9
8.8
7.7
2 3 4 5 6 7 8 9 10
Alvarado score
Proportionofgroup(%)
Intervention
Control
Fig 2 Distribution of Alvarado scores in patients with
suspectedappendicitis allocated to diagnosis with graded
compressionultrasonography and Alvarado score (intervention group)
or clinicaldiagnosis only (control)
Table 2 Primary outcomes in adults (>14 years) and children
(14 years)
No of patients 94 108
Mean t ime to therapeut ic operation (hours) 7.1 (5.8 to 8.4)
9.7 (7.2 to 12) 0.068
Mean duration of stay (hours) 59.3 (49 to 69) 59.2 (49 to 69)
0.99No (%) of non-therapeutic operations 11 (11.7; 6.7 to 20) 12
(11.1; 6.5 to 18) 0.90
No (%) with delayed treatment in associationwith perforation
2 (2.1; 0.6 to 7.4) 1 (0.93; 0.2 to 5.1) 0.60*
Total (%) adverse outcomes (delayedtreatment in association with
perforationand non-therapeutic operations)
13 (13.8; 8.3 to 22) 13 (12.0; 7.2 to 20) 0.70
Children (
-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
5/6
stay. There was a trend towards shorter stays in theintervention
group for patients undergoing therapeu-tic operations but because a
larger proportion of thecontrol group was managed non-operatively
(andtherefore discharged early) there was no differenceoverall.
Adverse outcomesThere are two outcomes that surgeons seek to
avoid incases of suspected appendicitis. The first is
anon-therapeutic operation. The second is delayed
treatment in a patient who is subsequently found tohave
perforation (delayed treatment in association withperforation). In
this study, the proportion of patients ineach group who had an
adverse outcome (either anon-therapeutic operation or delayed
treatment) wassimilar. The occurrence of a number of cases of
delaywith perforation, despite a low rate of perforatedappendicitis
(14.8%), suggests that rate of delayedtreatment in association with
perforation is a moreappropriate measure of the consequences of
delayeddiagnosis than overall perforation rate.
In the intervention group, many adverse outcomeswere associated
with a clinical management decisionthat was at odds with a correct
diagnosis under theintervention protocol.Of particular note is the
fact that
11 patients had a non-therapeutic operation after anegative
result on graded compression ultrasonogra-phy. If surgeons had
relied on the results of the proto-col these unnecessary operations
would have beenavoided. But what would have happened to
otherpatients in the study?
The protocol, if allowed to override clinicaljudgment, would
have led to operations in at least sixpatients who recovered
without surgery and in twopatients who did in fact undergo
non-therapeuticoperations (one with an Alvarado score of 10 and
onewith an incorrect sonographic diagnosis of ovariancyst). More
importantly, rigid adherence to themanagement indicated by the
protocol would haverequired that no patient with a negative result
could
have an operation. There were three patients withappendicitis
who had a negative result on ultrasonog-raphy, and in each case the
appendix was gangrenousor perforated. Had graded compression
ultrasonogra-phy been relied on, these patients would have had
anindefinite delay in treatment.
Use of the Alvarado score to select patients forimagingWe used
the Alvarado score as an objective means ofstratifying patients
according to risk so that those witha high or low probability of
appendicitis need not haveunnecessary imaging. The Alvarado score
(table 5) is
based on a simple and largely objective assessment thatrequires
minimal clinical experience, neverthelessNEM had an intensive
period of training before thestudy began, and we ensured that he
was elicitingsymptoms and signs in a consistent and objective
way.We believe that having one person perform the sameobjective
assessment on all occasions was a reliable andreproducible method
of risk stratification.
Whether the Alvarado score or some other form of
risk stratification is used, selection of patients for imag-ing
is an issue that cannot be ignored. Had weperformed graded
compression ultrasonography onall patients in the intervention
group the results wouldprobably have been worse. We would still
have hadthree false negative tests, all in patients with a
gangre-nous or perforated appendicitis, and possibly more. Ofthe 31
patients in the intervention group who did notundergo graded
compression ultrasonography therewere 23 with Alvarado scores of 9
or 10, three withscores of 3 or less, and five breaches of
protocol(because the surgeon was not prepared to wait
forultrasonography). Of these 31 patients, 27 underwentsurgery and
25 (93%) had a therapeutic operation, witha mean time to operation
of 5.6 hours. Our diagnosticprotocol incorporating the Alvarado
score was, if any-thing, safer, faster, and more accurate than
gradedcompression ultrasonography alone,but it still failed
toproduce better outcomes than unaided clinicaldiagnosis.
Possible biasesDistributions of Alvarado scores in each group
weresimilar, and the proportions of each group with anAlvarado
score of greater than 6 (that is, patients whowould be predicted to
have appendicitis on the basis ofAlvarados original paper) were
almost identical.Therefore the disparity between groups in number
of
Table 5 Alvarado score for diagnosis of acute appendicitis
Symptom/sign/test Score
Migration of pain 1
Anorexia 1
Nausea-vomiting 1
Tenderness in right iliac fossa 2
Rebound pain 1
Raised temperature (>37.3C) 1
Leucocyte count>
10
10
9
/l 2Differential white cell count with neutrophils >75% 1
Total 10
What is already known on this topicUltrasonography is an
accurate test for thediagnosis of acute appendicitis
Few studies have examined the effect of
diagnosticultrasonography on clinical outcomes, and therehave been
no randomised controlled trials
What this study adds
This study confirmed the accuracy ofultrasonography and found a
reduction in meantime to operation for patients
undergoingtherapeutic operation
There was no benefit of ultrasonography in termsof length of
hospital stay, rate of non-therapeuticoperations, or rate of
delayed treatment inassociation with perforation
False negative tests occurred in patients withgangrenous and
perforated appendixes
Ultrasonography remains a test of unprovedbenefit and should not
be used by those who areinexperienced in the clinical diagnosis
ofappendicitis
Papers
5BMJ VOLUME 321 14 OCTOBER 2000 bmj.com
-
8/12/2019 Randomised Controlled Trial of Ultrasonography in
Diagnosis of Acute Appendicitis_incorporating the Alvarado Scor
6/6
therapeutic operations performed is unlikely to reflecta
difference in disease prevalence.
To ensure that our results were not biased by
thenon-availability of the imaging service to after 10 pm,we
performed a secondary analysis on the 231 patientswho were enrolled
in the study before this time. Thedifference in mean time to
theatre was marginallyshort of significance and there was still no
differencebetween groups in duration of hospital stay or in
adverse outcomes.
General commentsWhen performed by experienced
sonographers,graded compression ultrasonography is an accuratetest.
In this trial the accuracy was over 93%, equal tothat of computed
tomography without coloniccontrast.14 False negative reports,
however, do occur: inour study 5% of negative results were
incorrect. Thereis no certain way of determining which negative
resultis a false negative, and the consequences of not operat-ing
may be serious. Patients cannot be safely sent homeafter a negative
result unless there are also clinicalgrounds for their discharge.
It is therefore inappropri-ate for graded compression
ultrasonography to be
used by those who lack experience in the clinical diag-nosis of
appendicitis.
ConclusionThe diagnosis of acute appendicitis aided by
gradedcompression ultrasonography has not been shown toproduce
better outcomes than clinical diagnosis alone.Further studies of
graded compression ultrasonogra-phy and other diagnostic methods in
suspected appen-dicitis should be randomised trials.
We thank Dr John Bear and Dr Jan Bishop for assistance
withsonographic and histopathological diagnosis. We also
thanksonographers Sue Mullen, Jenny Gosling, Warren Jones,
BrettRoworth, and Darrin Gray for their excellent
technicalassistance. In addition we thank Professor Michael
Hensley, whoreviewed the proposal for study design and gave advice
about
data interpretation and analysis, and Dr Brian Draganic, whogave
statistical advice and reviewed and edited the drafted paper.
Contributors: CDD initiated the study, formulated the
studyhypotheses, proposed the study design, analysed the data,
wasthe principal author of the paper, and is the guarantor.
NEMmanaged the running of the trial, contributed to study
design,
collected the data, initiated and participated in data analysis,
andhelped to write the paper. PMD initiated the research
inultrasonography, supervised the running of the trial,
facilitatedand coordinated involvement of different departments,
contrib-uted to data interpretation, and helped to edit the paper.
JSGcontributed to study design, supervised the running of the
trial,contributed to data interpretation and analysis, and helped
towrite and edit the paper.
Funding: None.Competing interests: None declared.
1 Hoffmann J, Rasmussen OO. Aids in the diagnosis of acute
appendicitis.Br J Surg1989;76:774-9.
2 Jones PF. Active observation in the management of acute
abdominal painin childhood.BMJ1976;ii:551-3.
3 Ooms HW, Koumans RK, Ho-Kang-You PJ, Puylaert JB.
Ultrasono-graphy in the diagnosis of acute appendicitis. Br J
Surg1991;78:315-8.
4 Heller MB, Skolnick ML. Ultrasound documentation of
spontaneouslyresolving appendicitis.Am J Emerg Med1993;11:51-3.
5 Velanovich V, Savata R. Balancing the normal appendectomy rate
withthe perforated appendicitis rate: implications for quality
assurance. AmSurg1992;58:264-9.
6 Olsen JB, Myren CJ, Haahr PE. Randomized study of the value of
lapar-oscopy before appendicectomy.Br J Surg1993;80:822-923.
7 Moberg AC, Ahlberg G, Leijonmarck CE, Montgomery A, Reiertsen
O,Rosseland AR, et al. Diagnostic laparoscopy in 1043 patients
withsuspected appendicitis.Eur J Surg1998;164:833-40.
8 Alvarado A. A practical score for the early diagnosis of acute
append-icitis.Ann Emerg Med1986;15:557-64.
9 Teicher I, Landa B, Cohen M, Cabnick LS, Wise L. Scoring
system to aidin the diagnosis of appendicitis. Ann
Surg1983;198:753-9.
10 de Dombal FT, Leaper DJ, Staniland JR, McCann AP, Horrocks
JC.Computer-aided diagnosis of acute abdominal pain.
BMJ1972;ii:9-13.
11 Puylaert JBCM. Acute appendicitis: US evaluation using
gradedcompression.Radiology1986;158:355-60.
12 Balthazar EJ. Appendicitis: prospective evaluation with
high-resolutionCT.Radiology1991;180:21-4.
13 Incesu L, Coskun A, Selcuk MB, Akan H, Sozubir S, Bernay F.
Acuteappendicitis: MR imaging and sonographic correlation. Am J
Roentgenol1997;168:669-74.
14 Rao PM,Boland GWL. Imaging of acute right lower abdominal
quadrantpain. Clin Radiol1998;53:639-49.
15 Ford R, Passinault W, Morse M. Diagnostic ultrasound for
suspectedappendicitis: Does the added cost produce a better
outcome? Am Surg1994;60:895-8.
16 Sivit C. Imaging children with acute right lower quadrant
pain. PediatrClin North Am1997;44:575-89.
17 Ohmann C, Yang Q, Franke C. Diagnostic scores for acute
appendicitis.Eur J Surg1995;161:273-81.
18 Macklin CP, Radcliffe GS, Merei JM, Stringer MD. A
prospectiveevaluation of the modified Alvarado score for acute
appendicitis in chil-dren.Ann R Coll Surg Engl1997;79:203-5.
19 Tobias M, Samuel E. Ultrasound and the Alvarado score. J R
Soc Med
1992;85:585-6.20 Davidson PM, Douglas CD, Hosking CS, Graded
compressionultrasonography in the assessment of the tough decision
acuteabdomen in childhood.Pediatr Surg Int1999;15:32-5.
21 Newcombe R. Two-sided confidence intervals for the single
proportion:comparison of seven methods.Stat Med1998;17:857-72.
(Accepted 18 May 2000)
Papers
6 BMJ VOLUME 321 14 OCTOBER 2000 bmj.com