Embed Size (px)
Citation preview
RADIOTHERAPY RISK PROFILETechnical Manual

Radiotherapy Risk Profile WHO/IER/PSP/2008.12
© World Health Organization 2008
All rights reserved. Publications of the World Health Organization can be obtained from:
WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications - whether for sale or fornoncommercial distribution - should be addressed to:
WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not implythe expression of any opinion whatsoever on the part of the World Health Organizationconcerning the legal status of any country, territory, city or area or of its authorities, orconcerning the delimitation of its frontiers or boundaries. Dotted lines on maps representapproximate borderlines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply thatthey are endorsed or recommended by the World Health Organization in preference to others ofa similar nature that are not mentioned. Errors and omissions excepted, the names of proprietaryproducts are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify theinformation contained in this publication. However, the published material is being distributedwithout warranty of any kind, either expressed or implied. The responsibility for theinterpretation and use of the material lies with the reader. In no event shall the World HealthOrganization be liable for damages arising from its use.
Designed by 22 DesignPrinted in Switzerland
Radiotherapy Risk Profile
Foreword 3
This document is divided into two parts:
1. An international review of patient safety measures in radiotherapy practice 4
Executive Summary 4Introduction 5
Radiotherapy treatment 5Risk management and quality assurance in radiotherapy 6Radiotherapy treatment errors 6
An evidence-based review of current practice 10Aim 10Materials and methods 10
Summary of literature 11Radiotherapy incidents 11Radiotherapy incidents in developing countries 21Emerging issues 21Costing 22
Conclusion 27
Stages of radiotherapy treatment 28-29
2. WHO patient safety Radiotherapy Risk Profile 30
Radiotherapy treatment process 30Risks inherent in the radiotherapy process 32
1. Assessment of the patient 322. Decision to treat 333. Prescribing treatment protocol 344. Positioning and immobilization 355. Simulation, imaging and volume determination 366. Planning 377. Treatment information transfer 388. Patient setup 399. Treatment delivery 4010. Treatment verification and monitoring 41
Risk reduction interventions 42Continuing to learn 42
Annex I Literature search strategy and results 44
Annex II Data form used to collect information on accidents, incidents and errors 45
References 46
Acknowledgements 49
CONTENTS

2
“Radiotherapy is widelyknown to be one of thesafest areas of modernmedicine, yet, for some, this essential treatment can bring harm, personaltragedy and even death”
Radiotherapy saves lives, prolongs lives andimproves the quality of life. For these reasons,millions of patients around the world, theirfamilies and the healthcare professionals whoserve them have reason to be truly thankful.It is widely known to be one of the safestareas of modern medicine, yet, for some, thisessential treatment can bring harm, personaltragedy and even death.
There is a long history of documentingincidents and examining adverse events inradiotherapy. From the study of theseincidents and the factors underlying them ithas been possible to map the risks.
When these serious incidents of harm wereexamined, slowly but surely a pattern becameevident. Each of the incidents was associatedwith one or more particular steps in theprocess of care. From this, it was possible toidentify a core process of care that wascommon to most radiotherapy treatment. Onto that, the common and rarer risks could bemapped as a first step to reducing oreliminating them. This is the world’s first riskprofile developed by the World HealthOrganisation World Alliance for Patient Safety.
In this risk profile, an assessment of theextent of harm caused by radiotherapyinternationally has been made. Manycountries have suffered the same types ofincidents in different places and at differenttimes. In response, an international expertgroup was convened representing all thosewho participate in daily radiotherapy delivery.Other agencies, such as the InternationalAtomic Energy Agency, that has a long andsuccessful history of ensuring the safestpractice in radiotherapy were also co-optedto the task. We are indebted to all of themfor their work on this risk profile.
We hope that it will assist regulatoryagencies, hospitals and individualdepartments to recognise and understandwith clarity the risks inherent in radiotherapy.We hope that this healthcare risk profile willstimulate interest in the concept worldwide.
Sir Liam DonaldsonChair, World Alliance for Patient Safety
Radiotherapy Risk Profile
Foreword by Sir Liam Donaldson
3
EXECUTIVE SUMMARY
4
• The literature in the area of radiationsafety is limited, and relates mainly todeveloped countries, or is the result ofinvestigations of major errors.
• Review of available literature showed thatin the years 1976 to 2007, 3125 patientswere reported to be affected byradiotherapy incidents that led to adverseevents. About 1% (N=38) of the affectedpatients died due to radiation overdosetoxicity. Only two reports estimated thenumber of deaths from under-dosage.
• In the years 1992 to 2007, more than 4500near misses (N=4616) were reported in theliterature and publically availabledatabases.
• Misinformation or errors in data transferconstituted the greatest bulk of incidentsin modern radiotherapy services. Of allincidents without any known adverseevents to patients, 9% (N=420) wererelated to the ‘planning’ stage, 38%(N=1732) were related to transfer of
information and 18% (N=844) to the‘treatment delivery’ stage. The remaining35% of the incidents occurred in acombination of multiple stages.
• More system or equipment-related errorsdocumented by medical physicists werereported, as compared to errors that occurduring initial choice of treatment, doseprescription and other random errors notrelated to equipment or system faults.
• International safety guidelines have beendeveloped and are regularly updated todeal with radiotherapy errors related toequipment and dosimetry. There is noconsensus as yet as to how best to dealwith errors not covered by regular systemquality assurance checks.
• Initiatives are proposed to develop a set ofpatient safety interventions addressing thehigh risk areas in the radiotherapy processof care, especially those involving patientassessment and clinical decisions.
AN INTERNATIONAL REVIEW OF PATIENT SAFETYMEASURES IN RADIOTHERAPY PRACTICE1
INTRODUCTION
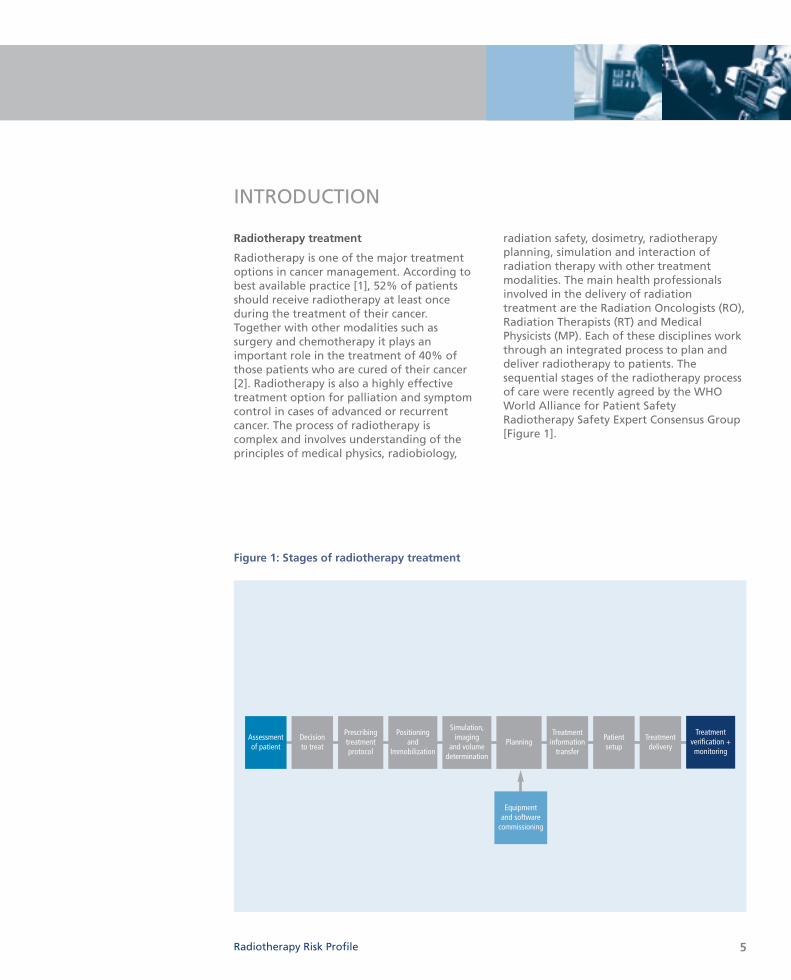
Figure 1: Stages of radiotherapy treatment
Radiotherapy Risk Profile
Radiotherapy treatment
Radiotherapy is one of the major treatmentoptions in cancer management. According tobest available practice [1], 52% of patientsshould receive radiotherapy at least onceduring the treatment of their cancer.Together with other modalities such assurgery and chemotherapy it plays animportant role in the treatment of 40% ofthose patients who are cured of their cancer[2]. Radiotherapy is also a highly effectivetreatment option for palliation and symptomcontrol in cases of advanced or recurrentcancer. The process of radiotherapy iscomplex and involves understanding of theprinciples of medical physics, radiobiology,
radiation safety, dosimetry, radiotherapyplanning, simulation and interaction ofradiation therapy with other treatmentmodalities. The main health professionalsinvolved in the delivery of radiationtreatment are the Radiation Oncologists (RO),Radiation Therapists (RT) and MedicalPhysicists (MP). Each of these disciplines workthrough an integrated process to plan anddeliver radiotherapy to patients. Thesequential stages of the radiotherapy processof care were recently agreed by the WHOWorld Alliance for Patient SafetyRadiotherapy Safety Expert Consensus Group[Figure 1].
5
Equipment and software
commissioning
Decision to treat
Prescribingtreatmentprotocol
Positioning and
Immobilization
Simulation,imaging
and volumedetermination
Treatmentdelivery
Patient setup
PlanningTreatment
verification +monitoring
Assessment of patient
Treatment information
transfer

Risk management and quality assurance inradiotherapy
Radiotherapy treatment is a multi-stage,complex, process that involves treatment of awide range of cancer conditions throughutilization of various technologies andrelated professional expertise. A high level ofaccuracy is needed at every step so that themaximum tumour control is produced withminimal risk to normal tissue. Risks should bemanaged prospectively and dose errorsshould be maintained within acceptabletolerances; the radiation dose should bedelivered within 5% of the prescribed dose[3]. Several studies have concluded that, forcertain types of tumours, the accuracy shouldbe even better (up to 3.5%) [4-6]. Accordingto WHO guidelines:
Quality assurance (QA) in radiotherapy is allprocedures that ensure consistency of themedical prescription, and safe fulfilment ofthat prescription, as regards to the dose tothe target volume, together with minimaldose to normal tissue, minimal exposure ofpersonnel and adequate patient monitoringaimed at determining the end result of thetreatment [7].
It is imperative that proper QA measures arein place in order to reduce the likelihood ofaccidents and errors occurring, and increasethe probability that the errors will berecognized and rectified if they do occur.Radiation treatment-specific quality assuranceguidelines have been issued by a number ofworldwide organizations such as the WorldHealth Organization (WHO), the InternationalAtomic Energy Agency (IAEA), and theInternational Commission on RadiologicalProtection (ICRP) [7-10]. Radiation safetyprotocols should be adhered to for all stagesof radiation treatment delivery, namely,tumour localization, patient immobilization,field placement, daily patient setup, dosecalibration, calculation, treatment deliveryand verification, as well as for equipmentcommissioning and maintenance. Skills andcompetences in radiation protectionrequirements are essential for all radiationtreatment health professionals. Radiationprotection includes the conceptual
framework of radiation protection ofpatients, staff and the public, internationalradiation safety standards, safety andaccuracy of equipment, radiation hazards inradiotherapy facilities, dosimetric andgeometric quantities for accuracy inradiotherapy, radiobiology and radiationrisks, treatment planning for optimizingdelivery of radiation dose, optimal and safeuse of different radiation sources inradiotherapy, radiation emergencies, physicalprotection and security of sources [11].
Protocols for individual countries have beendeveloped, based on relevance to the workenvironment of the local departments [12-15]. Quality initiative reports published inEurope [13] recommend that QA should notbe confined to physical and technical aspectsof the treatment process only, but should alsoencompass all activities in a radiationoncology centre from the moment a patiententers until the time they leave, and shouldcontinue throughout the follow-up period.However, all of these aspects may not be thefocus of individual facilities. As such, specificguidelines have also been developed inresponse to major radiotherapy incidents,highlighting individual issues to preventfuture adverse events [16-17].
Radiotherapy treatment errors
Accidental exposures in radiotherapy mayresult from an accident, an event or asequence of events, including equipmentfailures and operating errors [18]. Thepotential for errors in radiotherapy is high, asit involves a complete patient pathway withmany links in the chain. At each link in thechain there are hand-overs between differenthealth-care groups. The interaction of manyhealth-care workers collaborating on highlytechnical measurements and calculations canin itself present a risk of error. Modernradiotherapy departments are multisystem-dependent environments that rely heavily ontransfer of patient data between differentunits, systems and staff of differentdisciplines. The data transfer process inradiotherapy extends from diagnosis, toplanning initiation and review, further
6
Database
Checking Diagnostics
TreatmentReviewPlanning
Hospital management system
02
05 01
0603
07
04
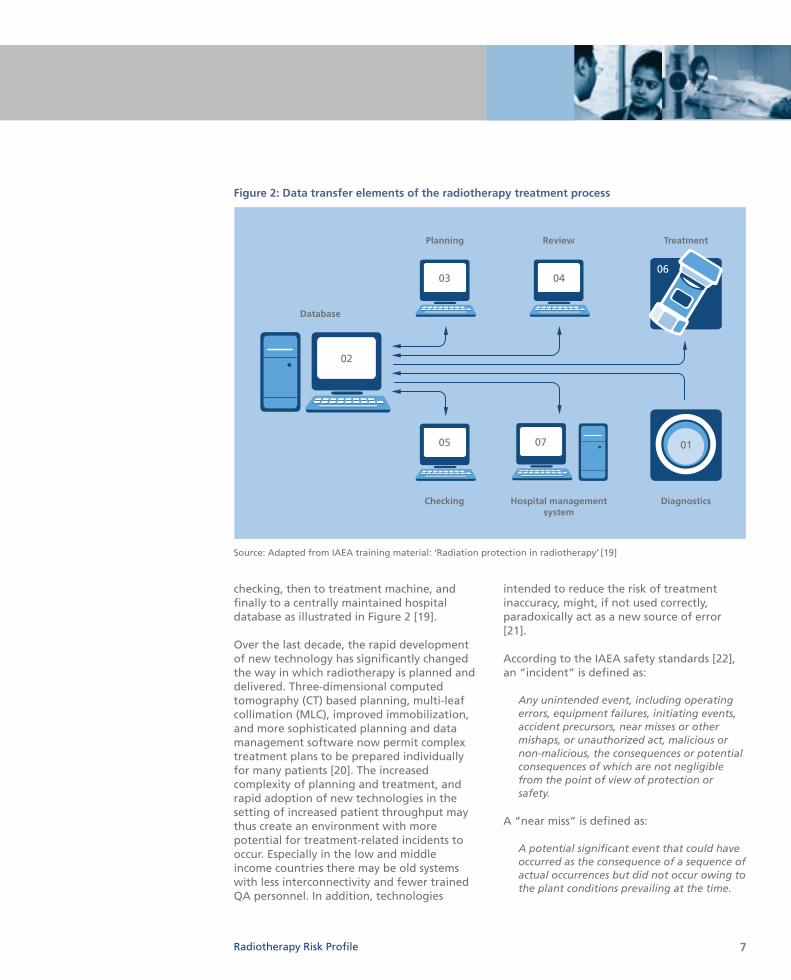
Figure 2: Data transfer elements of the radiotherapy treatment process
7
checking, then to treatment machine, andfinally to a centrally maintained hospitaldatabase as illustrated in Figure 2 [19].
Over the last decade, the rapid developmentof new technology has significantly changedthe way in which radiotherapy is planned anddelivered. Three-dimensional computedtomography (CT) based planning, multi-leafcollimation (MLC), improved immobilization,and more sophisticated planning and datamanagement software now permit complextreatment plans to be prepared individuallyfor many patients [20]. The increasedcomplexity of planning and treatment, andrapid adoption of new technologies in thesetting of increased patient throughput maythus create an environment with morepotential for treatment-related incidents tooccur. Especially in the low and middleincome countries there may be old systemswith less interconnectivity and fewer trainedQA personnel. In addition, technologies
intended to reduce the risk of treatmentinaccuracy, might, if not used correctly,paradoxically act as a new source of error[21].
According to the IAEA safety standards [22],an “incident” is defined as:
Any unintended event, including operatingerrors, equipment failures, initiating events,accident precursors, near misses or othermishaps, or unauthorized act, malicious ornon-malicious, the consequences or potentialconsequences of which are not negligiblefrom the point of view of protection orsafety.
A “near miss” is defined as:
A potential significant event that could haveoccurred as the consequence of a sequence ofactual occurrences but did not occur owing tothe plant conditions prevailing at the time.
Radiotherapy Risk Profile
Source: Adapted from IAEA training material: ‘Radiation protection in radiotherapy’ [19]

Other terms for medical errors include “events”, “mistakes”, “misadministrations”,“unusual occurrences”, “discrepancies”, and“adverse events”.
The WHO World Alliance for Patient Safetygeneral patient safety taxonomy containedwithin the International Classification forPatient Safety uses the following definitions[23]:
A patient safety incident is an event orcircumstance which could have resulted, ordid result, in unnecessary harm to a patient.
An adverse event is an incident which resultsin harm to a patient.
A near miss is an incident that did not causeharm (also known as a close call).
An error is a failure to carry out a plannedaction as intended or application of anincorrect plan, and may manifest by doingthe wrong thing (an error of commission) orby failing to do the right thing (an error ofomission), at either the planning or executionphase.
We have used “incident” and “near miss”wherever possible within this report.However, this needs further discussion withinthe radiotherapy community to determinewhether a uniform terminology as in othermedical fields could be used in relation toradiotherapy safety.
Although there are detailed reports on somemajor clinical radiation incidents thathappened over the last 30 years [24], it islikely that many more incidents have occurredbut either went unrecognized, were notreported to the regulatory authorities, orwere not published in the literature [10].
Research on radiotherapy safety focuses onanalyses of adverse events and near misses[25–26] as these might lead to identificationof latent problems and weak links within asystem that lie dormant for some time, andthen combine with a local trigger to create anincident [27]. A health service research group
in Canada developed a model for clinicalincident monitoring specifically addressingthe radiotherapy treatment service incidents.This model suggests an emphasis of incidentinvestigation on causal analysis and correctiveactions to improve care process performanceso that identification and response toincidents occurs in a systematic way thatsupports organizational learning [28]. Thereporting of near misses has been identifiedas a valuable tool in preventing seriousincidents in the non-medical domain [29].
Studies in radiotherapy practice have shownthat development of a comprehensive QAsystem, including an explicit and uniformprotocol for implementation and timelyassessment of error rate, may reduce the levelof incidents [20, 30]. A recent evaluation at acancer centre in the United Kingdom [31]reported a significant decrease in the numberof recorded incidents over the past eightyears. Changes in working practices duringthat time included: relocation of differentprocedures, increased use of specialist staff,and adaptation of working practices toreflect the requirements of new technologythrough regular discussion amongst staff.These factors were identified as factorspromoting incident reduction [31]. In anotherinstitution, real time audits of 3052 treatmentplans for a period of eight years providedimportant direct and indirect patient benefitsthat went beyond normal physical QAprocedures, and addressed issues related tophysician prescriptions [32].
The United States Nuclear RegulatoryCommission (NRC) maintains a large databaseof radiotherapy incidents, and has estimatedthat about 60% or more of radiotherapyincidents are due to human error [33]. Humanerror can be reduced through education andtraining and changes in working practicewithin radiotherapy departments [Figure 3]1.These findings, together with the fact thatradiotherapy quality activities requireinvolvement of a large group of professionalsusing a cooperative approach, justify thepriority for developing a globally acceptablepatient-centred safety guideline.
8

Individual
Machine
Human
Systematic
X
X X XXXX X
X XX
XX
XX
X
X
X
X
X
XX
XXX
XX
XX
X
XXX
Figure 3: A conceptual framework to prioritize high-risk areas in radiotherapy practice1
Source: Dr. Claire Lemer, the WHO World Alliance for Patient Safety
Radiotherapy Risk Profile
Presented overleaf is a collation and synthesisof evidence on radiation incidents and therecommended safety measures. Bothpublished literature and unpublished datasources have been reviewed. The riskiestareas in the process of care for radiotherapyhave been identified. These require furtherattention, especially those relating to humanerror rather than to equipment and systemfailure.
1. A conceptual framework of work in radiotherapy has beendesigned by the WHO World Alliance for Patient safety thatprovides a framework for thinking about where work hasoccurred (black) and where less work has occurred (red). Thismay aid categorization of errors and influence development ofan appropriate safety protocol.
9
Aim
To conduct an evidence-based review ofcurrent practice of patient safety measures inradiotherapy treatment facilities, including ananalysis of previous incidents in radiotherapydelivery and identification of high-risk areas.
Materials and methods
Worldwide incidents of accidental errorsduring radiotherapy treatment in the lastthirty years (from 1976 to 2007) were reviewedthrough appraisal of published materials(technical reports, journal articles, guidelines)and unpublished sources of information(departmental incident reports). A computer-based search of ‘Google’ and ‘Google Scholar’search engines and a ‘PubMed’ search of the e-journal collections on radiotherapy, medicalphysics and nuclear medicine was performedusing the key words: ‘radiotherapy accident/s’,‘radiotherapy incident/s’, ‘radiotherapyoverexposure’, ‘radiation protection’, ‘patientsafety’, ‘quality assurance’, ‘safety measures’and variations of these terms in combination.In addition, a broader search was performedfor developing countries using the above keywords combined with the terms ‘developingcountries’, ‘low income countries’ ‘Asia’,‘Africa’, and ‘Latin America’. ‘Grey literature’(material which is not formally published), suchas working papers, organizational reports (e.g.IAEA and ICRP web/print publications) andconference proceedings were obtainedelectronically and through personalcommunication. The bibliography of theindividual literature retrieved was iterativelysearched for additional citations. For articlespublished in other languages (e.g. French,Japanese), the translated abstracts wereidentified and verified with the study findingsfrom other sources in English (if available). Adetailed search strategy and the search resultsare presented in Annex I.
Radiotherapy safety-related incidents and nearmisses that were reported to local andinternational databases were also reviewed,
including the ‘Radiation Oncology SafetyInformation System’ (ROSIS) database, avoluntary web-based safety informationdatabase for radiotherapy, set up by a groupof medical physicists and radiation therapytechnicians in Europe and the Australian State-based Department of Radiation Oncologyannual incident reports collection [34-35].While reviewing the literature, a data form(Annex II) was used as a template to ensureuniformity and completeness of information.
The incidents were recorded according to thefollowing categories: • Description
• Direct cause(s)
• Contributing factors
• Stage of the treatment process duringwhich the incident happened (as describedin Figure 1)
• Reported impact or outcome
• Corrective actions and prevention of futureincidents
The data available from all sources werereviewed and synthesized to determine: thestage at which most accidents or incidentsoccurred, what were the existing deficienciesand contributing factors that led to the errors,and how these errors could have beenprevented. The incidents were groupedaccording to the income level of the countries(high income, middle and low incomecountries) as categorized in the World Bank listof economies [36]. Economies were dividedamong income groups according to the 2006Gross National Income (GNI) per capita intolow income: US$ 905 or less; lower middleincome: US$ 906–US$ 3595; upper middleincome: US$ 3596–US$ 11 115; and highincome: US$ 11 116 or more. The overallsummary of incidents, in terms of mostcommon stage of occurrence and identifiedareas of need were drawn; a similar approachhas been suggested in the 2006 Annual Reportof the Chief Medical Officer for theDepartment of Health, United Kingdom [37].
10
AN EVIDENCE-BASED REVIEW OF CURRENT PRACTICE
Radiotherapy incidents
A summary of all widely reported majorradiotherapy incidents that led to significantadverse events to patients (such as radiationinjury and death) and which have occurred inthe last three decades (1976-2007) ispresented in Table 1. The countries ofoccurrence were middle and high incomecountries in the United States of America,Latin America, Europe and Asia. In total, 3125patients were affected and of them 38 (1.2%)patients were reported to have died due toradiation overdose toxicity. The number ofincidents that occurred in the planning stagewas 1702 (55%), and of the remaining 45%,incidents were due to errors that occurredduring the introduction of new systemsand/or equipment such as megavoltagemachines (25%), errors in treatment delivery(10%), information transfer (9%) or inmultiple stages (1%).
In the years from 1992 to 2007, 4616 incidentsthat led to near misses and which resulted inno recognizable patient harm were identifiedfrom the published literature andunpublished incident reporting databasesfrom Australia, United Kingdom, otherEuropean countries, Canada and the UnitedStates (Table 2). A major source (N=854) ofthe recent incidents was the ROSIS database[34], a voluntary web-based safetyinformation database for radiotherapyincidents in Europe, which had been set up bytwo radiation therapists and two medicalphysicists. Of all such incidents without anyknown adverse events to patients, 9%(N=420) were related to the ‘planning’ stage;38% (N=1732) were related to transfer ofinformation and 18% (N=844) to the‘treatment delivery’ stage. The remaining35% of the incidents occurred in thecategories of prescription, simulation, patientpositioning or in a combination of multiplestages.
Radiotherapy Risk Profile
SUMMARY OF LITERATURE
11

12
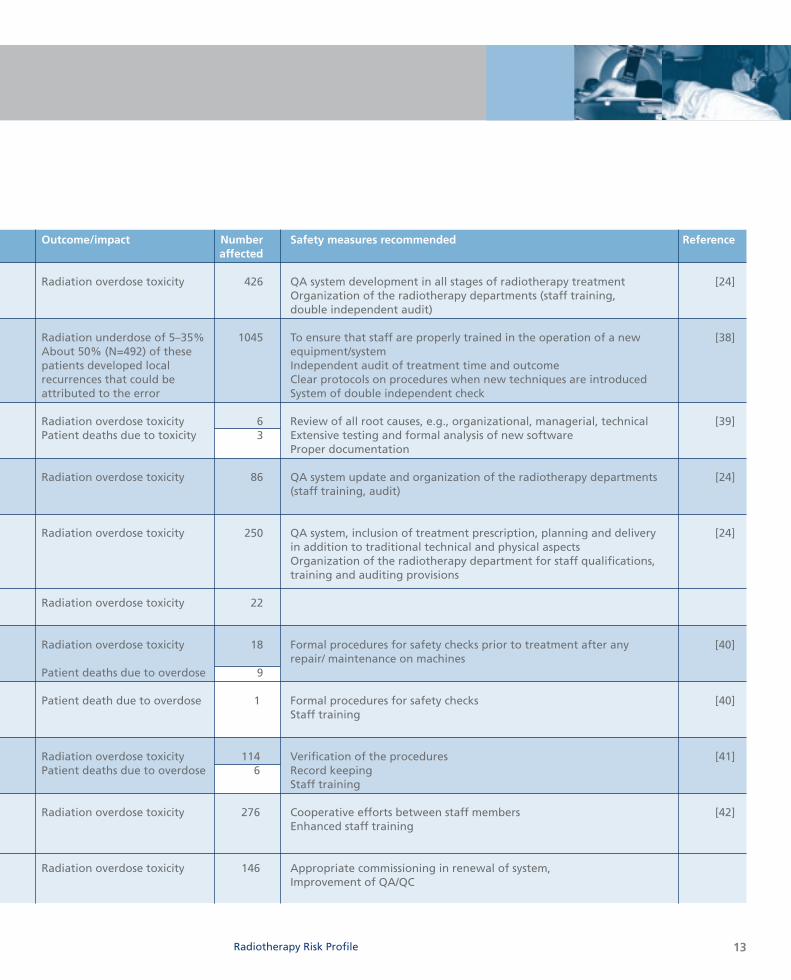
Table 1: Chronological summary of radiotherapy incidents with adverse events by country and stage of treatment [white box indicates number of reported deaths from this incident]
Year(s) Country Economic group Stage of therapy Cause/contributingfactors of error
1974– 1976 USA High income Commissioning Calibration error of a Cobalt-60Teletherapy unit and falsified documentation
1982–1991 UK High income Planning Introduction of a new technique of treatment planning leading to miscalculation of radiation doses
1985–1987 USA & High income Treatment Therac-25 Software Canada delivery programming error
1986–1987 Germany High income Planning Cobalt-60 dose calculations based on erroneous dose tables(varying overdoses)
1988 UK High income Commissioning Error in the calibration of a Cobalt-60 therapy unit
1988–1989 Treatment Error in the identification of delivery Cs-137 Brachytherapy sources
1990 Spain High income Treatment Errors in maintenance and delivery calibration of a linear accelerator
combined with procedural violations
1992 USA High income Treatment Brachytherapy source (High delivery Dose Rate) dislodged
and left inside the patient
1996 Costa Rica Upper middle Commissioning Miscalibration of a Cobalt-60 income unit resulting in incorrect
treatment dose
1990–1991, Japan High income Information Differences of interpretations for 1995–1999 transfer prescribed dose between RO & RT,
lack of their communication
1998–2004 Planning Wedge factor input error in renewalof treatment planning system
13Radiotherapy Risk Profile
Outcome/impact Number Safety measures recommended Referenceaffected
Radiation overdose toxicity 426 QA system development in all stages of radiotherapy treatment [24]Organization of the radiotherapy departments (staff training, double independent audit)
Radiation underdose of 5–35% 1045 To ensure that staff are properly trained in the operation of a new [38]About 50% (N=492) of these equipment/systempatients developed local Independent audit of treatment time and outcomerecurrences that could be Clear protocols on procedures when new techniques are introducedattributed to the error System of double independent check
Radiation overdose toxicity 6 Review of all root causes, e.g., organizational, managerial, technical [39]Patient deaths due to toxicity 3 Extensive testing and formal analysis of new software
Proper documentation
Radiation overdose toxicity 86 QA system update and organization of the radiotherapy departments [24](staff training, audit)
Radiation overdose toxicity 250 QA system, inclusion of treatment prescription, planning and delivery [24]in addition to traditional technical and physical aspectsOrganization of the radiotherapy department for staff qualifications, training and auditing provisions
Radiation overdose toxicity 22
Radiation overdose toxicity 18 Formal procedures for safety checks prior to treatment after any [40]repair/ maintenance on machines
Patient deaths due to overdose 9
Patient death due to overdose 1 Formal procedures for safety checks [40]Staff training
Radiation overdose toxicity 114 Verification of the procedures [41]Patient deaths due to overdose 6 Record keeping
Staff training
Radiation overdose toxicity 276 Cooperative efforts between staff members [42]Enhanced staff training
Radiation overdose toxicity 146 Appropriate commissioning in renewal of system,Improvement of QA/QC
14
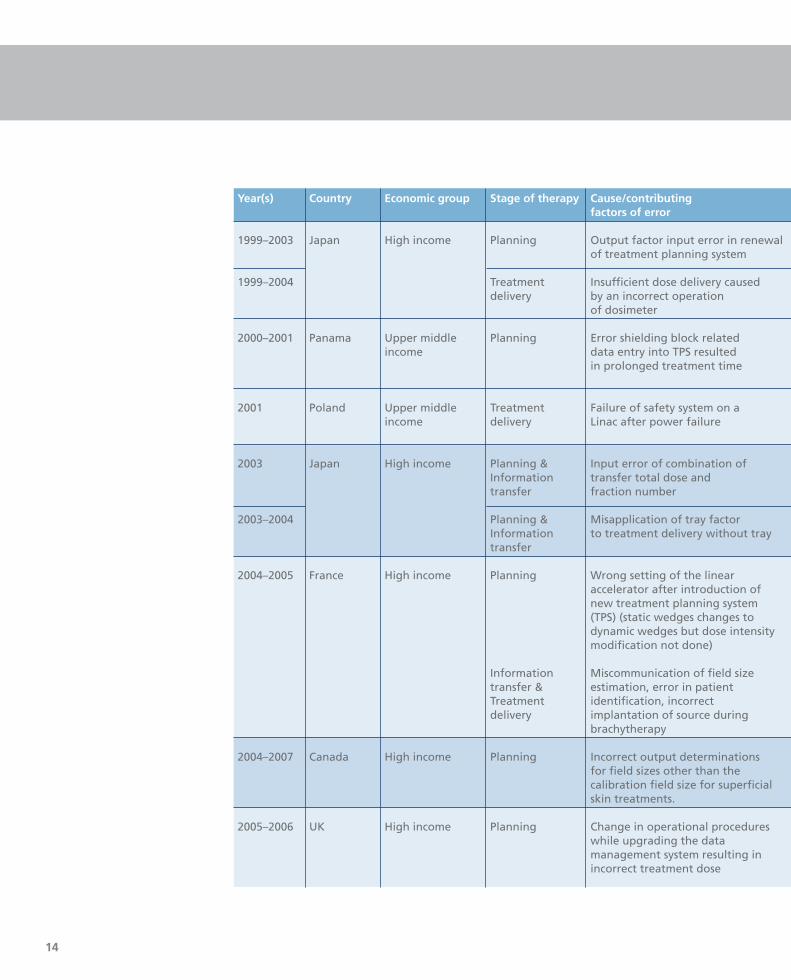
Year(s) Country Economic group Stage of therapy Cause/contributingfactors of error
1999–2003 Japan High income Planning Output factor input error in renewal of treatment planning system
1999–2004 Treatment Insufficient dose delivery caused delivery by an incorrect operation
of dosimeter
2000–2001 Panama Upper middle Planning Error shielding block related income data entry into TPS resulted
in prolonged treatment time
2001 Poland Upper middle Treatment Failure of safety system on a income delivery Linac after power failure
2003 Japan High income Planning & Input error of combination of Information transfer total dose andtransfer fraction number
2003–2004 Planning & Misapplication of tray factorInformation to treatment delivery without traytransfer
2004–2005 France High income Planning Wrong setting of the linear accelerator after introduction of new treatment planning system (TPS) (static wedges changes to dynamic wedges but dose intensity modification not done)
Information Miscommunication of field size transfer & estimation, error in patientTreatment identification, incorrectdelivery implantation of source during
brachytherapy
2004–2007 Canada High income Planning Incorrect output determinations for field sizes other than the calibration field size for superficial skin treatments.
2005–2006 UK High income Planning Change in operational procedures while upgrading the data management system resulting in incorrect treatment dose
15Radiotherapy Risk Profile
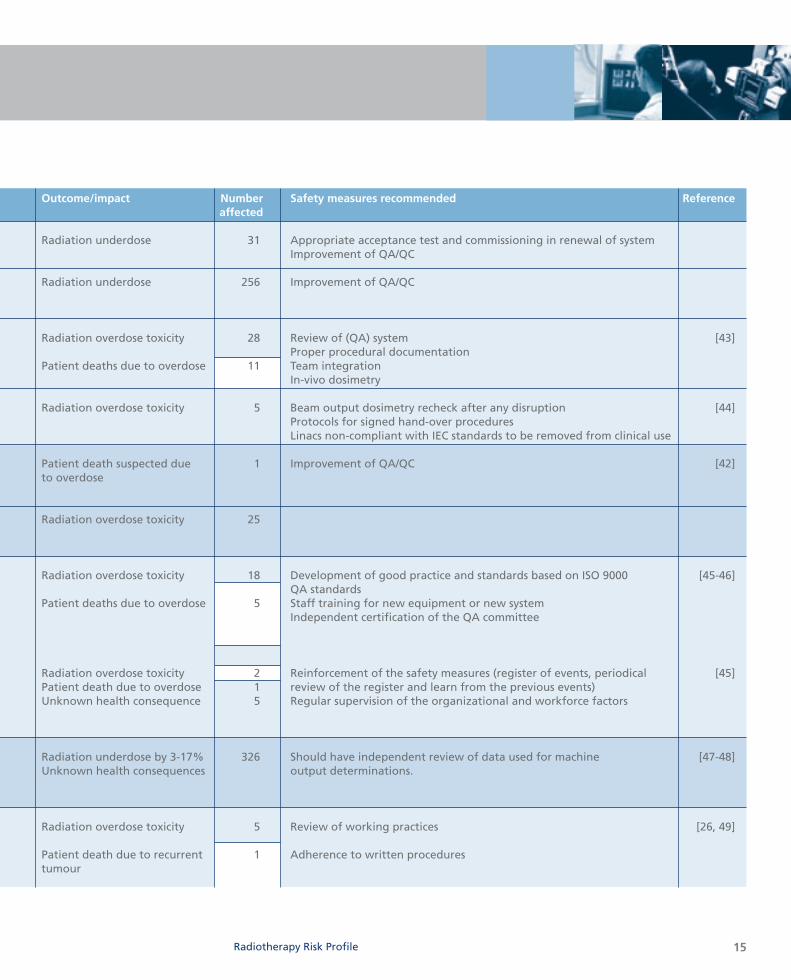
Outcome/impact Number Safety measures recommended Referenceaffected
Radiation underdose 31 Appropriate acceptance test and commissioning in renewal of systemImprovement of QA/QC
Radiation underdose 256 Improvement of QA/QC
Radiation overdose toxicity 28 Review of (QA) system [43]Proper procedural documentation
Patient deaths due to overdose 11 Team integration In-vivo dosimetry
Radiation overdose toxicity 5 Beam output dosimetry recheck after any disruption [44]Protocols for signed hand-over proceduresLinacs non-compliant with IEC standards to be removed from clinical use
Patient death suspected due 1 Improvement of QA/QC [42] to overdose
Radiation overdose toxicity 25
Radiation overdose toxicity 18 Development of good practice and standards based on ISO 9000 [45-46]QA standards
Patient deaths due to overdose 5 Staff training for new equipment or new systemIndependent certification of the QA committee
Radiation overdose toxicity 2 Reinforcement of the safety measures (register of events, periodical [45]Patient death due to overdose 1 review of the register and learn from the previous events)Unknown health consequence 5 Regular supervision of the organizational and workforce factors
Radiation underdose by 3-17% 326 Should have independent review of data used for machine [47-48]Unknown health consequences output determinations.
Radiation overdose toxicity 5 Review of working practices [26, 49]
Patient death due to recurrent 1 Adherence to written procedurestumour
16
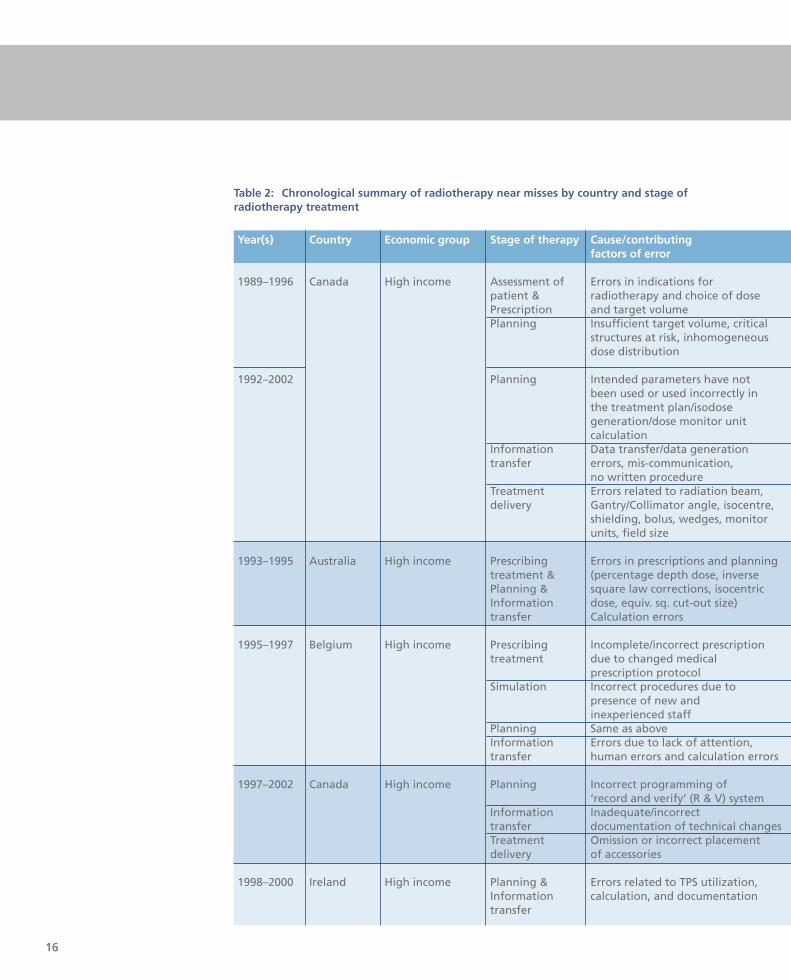
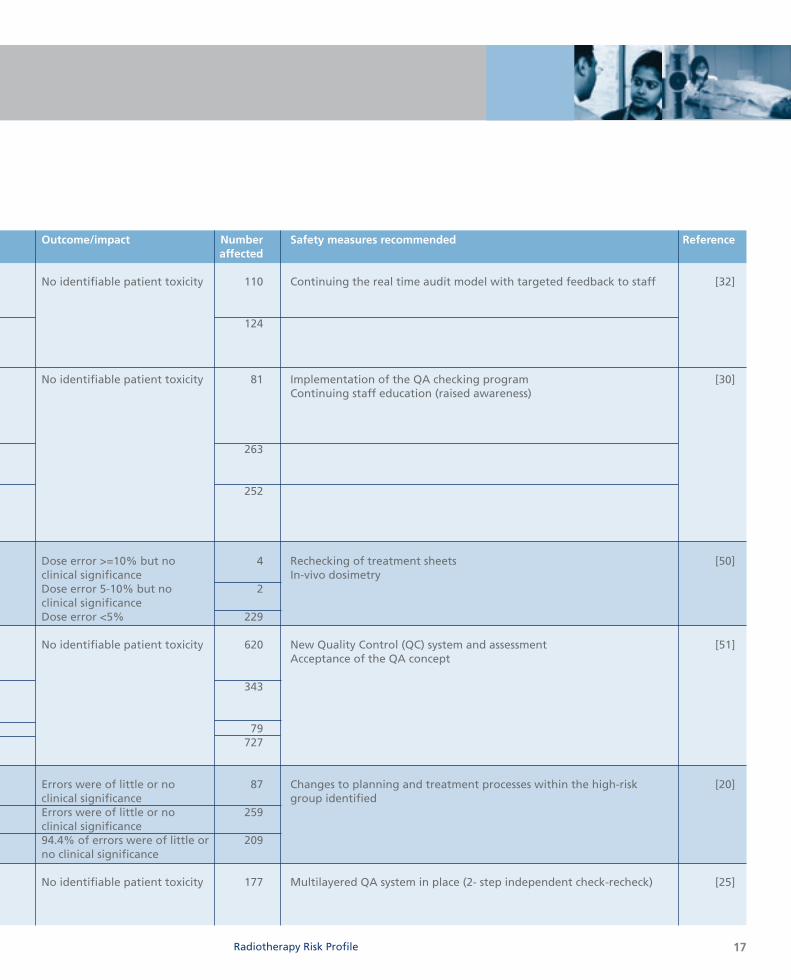
Table 2: Chronological summary of radiotherapy near misses by country and stage of radiotherapy treatment
Year(s) Country Economic group Stage of therapy Cause/contributingfactors of error
1989–1996 Canada High income Assessment of Errors in indications for patient & radiotherapy and choice of dose Prescription and target volumePlanning Insufficient target volume, critical
structures at risk, inhomogeneous dose distribution
1992–2002 Planning Intended parameters have not been used or used incorrectly in the treatment plan/isodose generation/dose monitor unit calculation
Information Data transfer/data generationtransfer errors, mis-communication,
no written procedure Treatment Errors related to radiation beam,delivery Gantry/Collimator angle, isocentre,
shielding, bolus, wedges, monitor units, field size
1993–1995 Australia High income Prescribing Errors in prescriptions and planningtreatment & (percentage depth dose, inversePlanning & square law corrections, isocentric Information dose, equiv. sq. cut-out size)transfer Calculation errors
1995–1997 Belgium High income Prescribing Incomplete/incorrect prescriptiontreatment due to changed medical
prescription protocolSimulation Incorrect procedures due to
presence of new and inexperienced staff
Planning Same as aboveInformation Errors due to lack of attention,transfer human errors and calculation errors
1997–2002 Canada High income Planning Incorrect programming of ‘record and verify’ (R & V) system
Information Inadequate/incorrect transfer documentation of technical changes Treatment Omission or incorrect placementdelivery of accessories
1998–2000 Ireland High income Planning & Errors related to TPS utilization, Information calculation, and documentationtransfer
17Radiotherapy Risk Profile
Outcome/impact Number Safety measures recommended Referenceaffected
No identifiable patient toxicity 110 Continuing the real time audit model with targeted feedback to staff [32]
124
No identifiable patient toxicity 81 Implementation of the QA checking program [30]Continuing staff education (raised awareness)
263
252
Dose error >=10% but no 4 Rechecking of treatment sheets [50]clinical significance In-vivo dosimetryDose error 5-10% but no 2clinical significanceDose error <5% 229
No identifiable patient toxicity 620 New Quality Control (QC) system and assessment [51]Acceptance of the QA concept
343
79727
Errors were of little or no 87 Changes to planning and treatment processes within the high-risk [20]clinical significance group identifiedErrors were of little or no 259clinical significance94.4% of errors were of little or 209no clinical significance
No identifiable patient toxicity 177 Multilayered QA system in place (2- step independent check-recheck) [25]

18
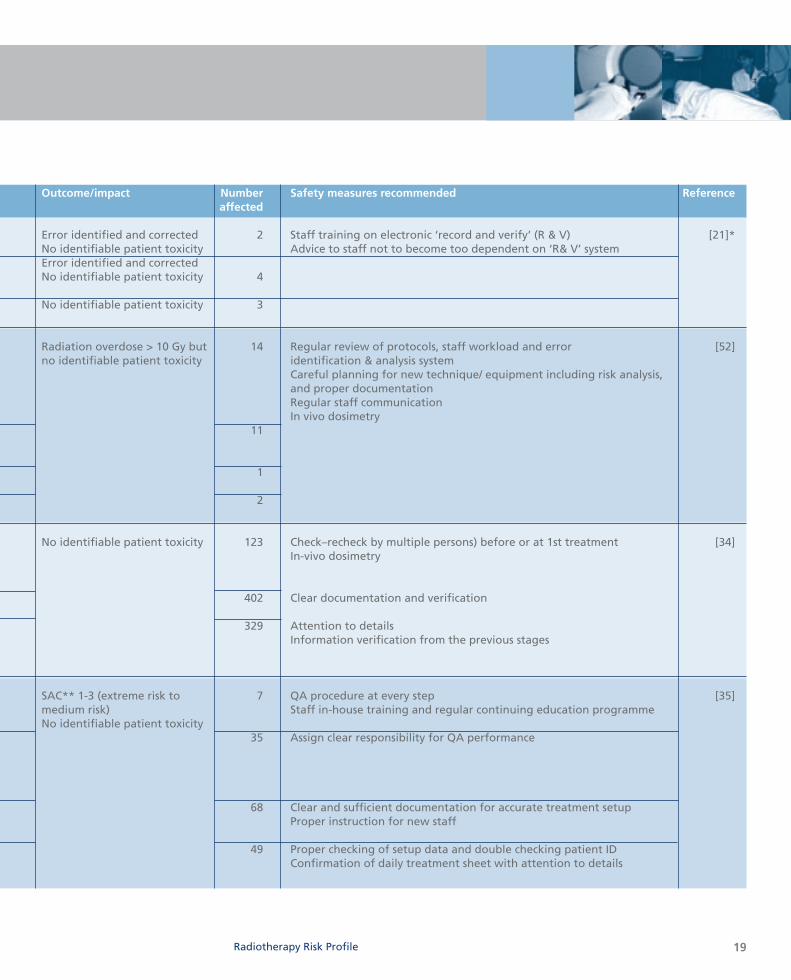
Year(s) Country Economic group Stage of therapy Cause/contributingfactors of error
1999-2000 USA High income Information Incorrect data entry leading totransfer incorrect treatment parametersPatient Incorrect placement of positioning positioning device, error in placement of
shielding blocksTreatment Patient identification error, delivery staff miscommunication
2000–2006 UK High income Planning Incorrect setup details, calculation errors, errors in prescription interpretation, incorrect data/dose per fraction into the planning computer.Wrong side/site being planned
Information Incorrect patient setup details,transfer Incorrect data entry into the
‘Record & Verify’ (R&V) systemPatient Patient changing position positioning after setup Treatment Technical complexity and overlap delivery of concomitant treatment areas
2001–2007 Europe High income Simulation Mould room error, incorrect virtual(Not & Planning simulation protocol, incorrect specified) calculation of monitoring unit (mu),
couch distance, pacemaker etc.Information Errors in data transfer, inadequatetransfer communicationTreatment Errors related to patient delivery identification, radiation beam,
isocentre, shielding, bolus, and wedges, field size etc.
2005 Australia High income Simulation Simulation/virtual simulation error due to lack of attention to details while simulating
Planning Errors in which intended parameters have not been used or used incorrectly in the treatment plan/isodose generation/dose monitor unit calculation
Information Unclear documentation, incorrecttransfer data generation, and inadequate
communicationTreatment Errors related to radiation beam,delivery port film/EPI use, shielding, bolus,
wedges, monitor units, field size
*The incidents described were the ones only related to the computerized ‘record and verify’ system **Severity Assessment Code (SAC) is a numerical score applied to an incident based on the type of event, its likelihood of recurrence and its consequence. The scale ranges from 1 (extreme) to 4 (low) [53].
19Radiotherapy Risk Profile
Outcome/impact Number Safety measures recommended Referenceaffected
Error identified and corrected 2 Staff training on electronic ‘record and verify’ (R & V) [21]*No identifiable patient toxicity Advice to staff not to become too dependent on ‘R& V’ systemError identified and corrected No identifiable patient toxicity 4
No identifiable patient toxicity 3
Radiation overdose > 10 Gy but 14 Regular review of protocols, staff workload and error [52]no identifiable patient toxicity identification & analysis system
Careful planning for new technique/ equipment including risk analysis, and proper documentationRegular staff communicationIn vivo dosimetry
11
1
2
No identifiable patient toxicity 123 Check–recheck by multiple persons) before or at 1st treatment [34]In-vivo dosimetry
402 Clear documentation and verification
329 Attention to detailsInformation verification from the previous stages
SAC** 1-3 (extreme risk to 7 QA procedure at every step [35]medium risk) Staff in-house training and regular continuing education programmeNo identifiable patient toxicity
35 Assign clear responsibility for QA performance
68 Clear and sufficient documentation for accurate treatment setupProper instruction for new staff
49 Proper checking of setup data and double checking patient IDConfirmation of daily treatment sheet with attention to details
0
500
1000
1500
2000
1750
1250
750
250
0
500
1000
1500
2000
1750
1250
750
250
Ass
essm
ent o
f pat
ient
&
deci
sion
to tr
eat &
pre
scrip
tion
Posit
ioni
ng &
imm
obili
zatio
nSi
mul
atio
n &
imag
ing
Com
miss
ioni
ng
Plan
ning
Trea
tmen
t inf
orm
atio
ntr
ansf
erPa
tient
setu
p Tr
eatm
ent d
eliv
ery
Trea
tmen
t rev
iew
Mul
tiple
stag
es
20
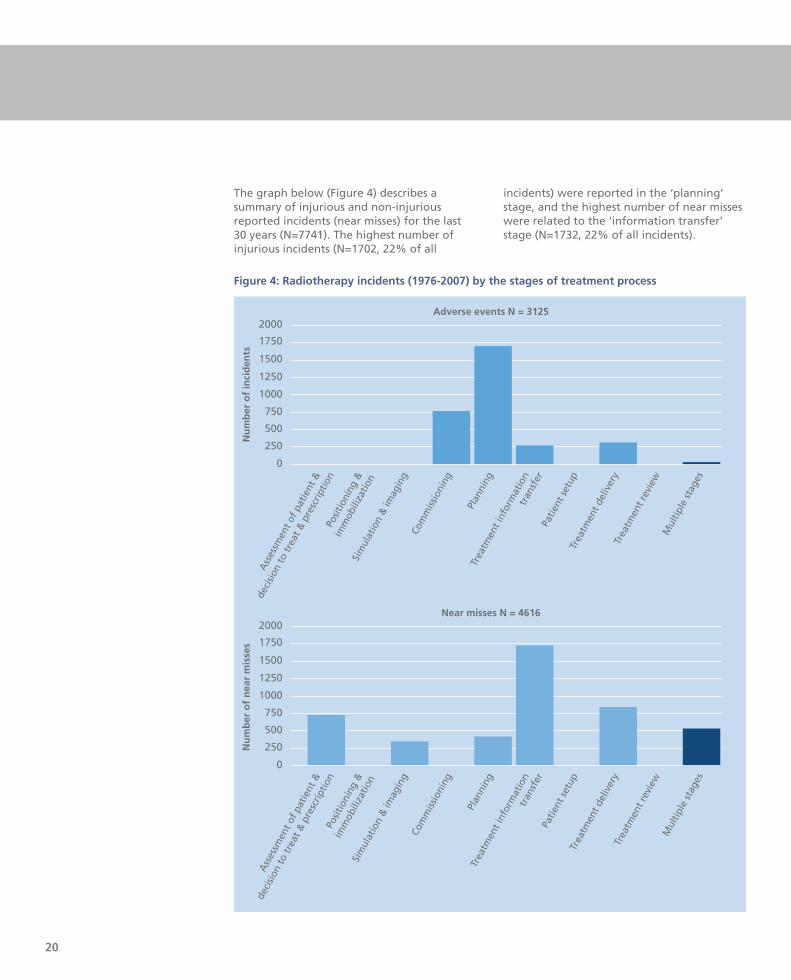
The graph below (Figure 4) describes asummary of injurious and non-injuriousreported incidents (near misses) for the last30 years (N=7741). The highest number ofinjurious incidents (N=1702, 22% of all
incidents) were reported in the ‘planning’stage, and the highest number of near misseswere related to the ‘information transfer’stage (N=1732, 22% of all incidents).
Ass
essm
ent o
f pat
ient
&
deci
sion
to tr
eat &
pre
scrip
tion
Posit
ioni
ng &
imm
obili
zatio
n
Sim
ulat
ion
& im
agin
gCo
mm
issio
ning
Plan
ning
Trea
tmen
t inf
orm
atio
ntr
ansf
erPa
tient
setu
p Tr
eatm
ent d
eliv
ery
Trea
tmen
t rev
iew
Mul
tiple
stag
es
Near misses N = 4616
Adverse events N = 3125
Nu
mb
er o
f in
cid
ents
Nu
mb
er o
f n
ear
mis
ses
Figure 4: Radiotherapy incidents (1976-2007) by the stages of treatment process
Radiotherapy Risk Profile
Radiotherapy incidents in developingcountries
No detailed reports on radiotherapy-relatedadverse events were available from Asia orAfrica. The only published studies are theevaluation of the dosimetry practices inhospitals in developing countries through theIAEA and World Health Organization (WHO)-sponsored Thermoluminescent Dosimetry(TLD) postal dose quality audits carried out ona regular basis [54, 55]. These studiesreported that facilities that operateradiotherapy services without qualified staffor without dosimetry equipment have poorerresults than those facilities that are properlystaffed and equipped. Strengthening ofradiotherapy infrastructure has beenrecommended for under-resourced centres,such as those in South America and theCaribbean, to improve their audit outcomesas comparable to those of developedcountries [54].
An external audit of an oncology practice inAsia was able to identify ‘areas of need’ interms of gaps in knowledge and skills of thestaff involved. The study found that abouthalf (52%) of the patients audited receivedsuboptimal radiation treatment, potentiallyresulting in compromised cure/palliation orserious morbidity. Inadequate knowledge andskills and high workload of the radiationoncology staff were described as the reasonsfor poor quality of service [56].
Emerging issues
From our literature review, it is apparent thatin the early 1990s major radiotherapyincidents occurred mainly due to inexperiencein using new equipment and technologyduring radiotherapy treatment (Table 1), andthese types of incidents are now much lessfrequent. More recently, misinformation orerrors in data transfer constituted thegreatest bulk of radiotherapy-relatedincidents (Table 2). The incidents that occurdue to transcription errors, rounding offerrors, forgotten data or interchange of dataare mostly due to human mistakes or
inattention [57]. It is now a well-recognizedchallenge in radiotherapy, and a largenumber of preventative guidelines and safetyprotocols have been established by theradiation safety-related authorities at thelocal and international level [58-64]. In someof the centres around the world, strictadherence to the radiotherapy QA protocolshas resulted in reduction in the number oferrors and related consequences [20, 30, 50].It has also been suggested that continuousreporting and evaluation of incidents inradiotherapy is an effective way to preventmajor mishaps, as demonstrated in the highratio of near misses per adverse events (14 to1) [25]. Thus, regular frequent QA review atthe local level should be ensured, withadequate funding and expertise.
Another important initiative in preventingradiotherapy errors in decision-making andpoor, or incorrect, work practice, could bebehavioural modification, achieved throughfrequent audit and regular peer review of thespecialist’s protocols, processes, proceduresand personnel involved [8, 65]. Shakespeareet al [56] observed that their audit acted asan informal learning needs assessment for theradiation oncology staff of the auditedcentre. They became more aware of theirknowledge and skills gaps, and implementedpeer review of all patients simulated.Additionally they implemented weeklydepartmental continuing medical educationactivities, a portal film review process, andhave been performing literature search andpeer discussion of difficult cases [56].
The incidents in radiotherapy that are mainlyrelated to patient assessment prior totreatment involve history/physicalexamination, imaging, biochemical tests,pathology reviews and errors duringradiotherapeutic decision-making includingtreatment intent, tumour type, individualphysician practice and type of equipmentused [66]. Comprehensive QA protocols havebeen developed that include medical aspectsof the radiotherapy treatment, such asclinician decision and patient assessment [8],
21
and have been adopted in several centres inEurope. However, these protocols have notbeen widely adopted in radiotherapy centresworldwide.
An evaluation of radiotherapy incidentreporting using three well known incidentdata sources, namely, IAEA, ROSIS and NRCdatasets, reported relatively fewer incidentsin the ‘prescription’ domain than in the‘preparation’ and ‘treatment’ domains [67].According to the report of a QA meeting inthe UK in 2000 [68], much effort has beendirected at QA of system and equipment-related components of radiotherapy, such asplanning computers, dosimetry audit andmachine performance. Little effort has beenmade so far to standardize medical processes,including target drawing, the application ofappropriate margins and the verification ofsetup involved in radiotherapy. These errorscause variations in time–dose–fractionationschedules, leading to changes in thebiological doses that have the potential for asignificant impact on patient safety. Europeanexperts also suggested that taking initiativesto improve the culture of clinical governance,and setting the standards of practice throughmedical peer review of target drawing anddose prescription, would be a significantpositive step in improving quality inradiotherapy services [8, 68].
A summary of potential ‘risk’ areas in theradiotherapy process, and the suggestedpreventive measures is presented in Table 3.The ‘risk’ areas and the proposed preventivemeasures have been generated throughconsultation with radiotherapy professionalsand review of recommendations of bothpublished and unpublished radiotherapyincident reports.
Costing
It is evident in the literature that theradiation treatment incidents are mostlyrelated to human error. Hence, the safetyinterventions, such as regular training, peerreview process, and audit of the QA protocolsat various points of therapy, would involveinvestment in workforce resources (e.g. time,personnel, and training). The cost ofworkforce would vary from country tocountry because of the variability of thesalary levels of the treatment personnelbetween high, low and middle incomecountries [69]. A detailed cost–benefitanalysis however is beyond the scope of this report.
22
23Radiotherapy Risk Profile

Table 3: Potential risk areas (•) in radiotherapy treatment
Stages Patient factors Equipmentsystem factors
History Clinical Pathologyexamination
Assessment of patient & • • •decision to treat
Prescribing
• •treatment protocol
Positioning & • • •immobilization
Simulation & imaging •
Planning
•
Treatment
•information transfer
Patient setup • • • •
Treatment delivery • • • •
Treatment review • • •
24

25Radiotherapy Risk Profile
Staff factors Suggested preventive measures
Communication Guidelines/ Training No. of staffprotocol
• • • • Peer review processEvidence-based practice
• • •Peer review processStandard protocol Competency certificationConsultation with seniors
• • • • Competency certificationQA check & feedbackIncident monitoring
• • • • Competency certificationQA check & feedbackIncident monitoring
• • • •QA check & feedbackNew staff & equipment orientationCompetency certificationIncident monitoring
• • • •Clear documentationTreatment sheet check‘Record & verify’ system In vivo dosimetry
• • • • Competency certificationIncident monitoringSupervisor audit
• • • • Incident monitoringImaging/Portal filmIn-vivo dosimetry
• • • • Competency certificationIncident monitoringIndependent audit

26
27Radiotherapy Risk Profile
Radiotherapy-related errors are notuncommon, even in the countries with thehighest level of health-care resources, but theradiotherapy-related error rate comparesfavourably with the rate of other medicalerrors. The risk of mild to moderate injuriousoutcome to patients from these errors wasabout 1500 per million treatment courses,which was much lower than the hospitaladmission rates for adverse drug reactions(about 65 000 per million) [70]. It is unrealisticto expect to reduce the error rate to zero, butevery effort should be taken to keep the rateslow. Risk model researchers Duffy and Saullcomment:
Errors can always be reduced to the minimumpossible consistent with the accumulatedexperience by effective error managementsystems and tracking progress in errorreduction down the learning curve [33].
This can also lead to identification ofincidents earlier in the process with lessserious consequences.
Through our review we were able to confirmthe stages of radiotherapy treatment wheremost incidents occur. Although a largeproportion of reported incidents were relatedto system failures due to incorrect use ofequipment and setup procedures, for anumber of them the contributing factorswere incorrect treatment decisions, incorrecttreatment delivery and inadequateverification of treatment, due to inexperienceand inadequate knowledge of the staffinvolved. These errors were not as wellreported as the system-related errors
documented predominantly by the medicalphysicists, as observed in our review. Hence,development of a set of standardshighlighting the patient-centred ‘risk’ areas inradiotherapy treatment, together withsuggested improvements tailored to the needof individual countries and specificdepartments may be relevant for allstakeholders.
The WHO World Alliance for Patient Safetyhas started an initiative to address the high-risk areas in the radiotherapy process of care,that is complimentary to the IAEA-developedsafety measures and other previouslydeveloped standards, to address non-equipment, non-system faults associated withradiotherapy delivery. An expert groupfacilitated by the WHO World Alliance forPatient Safety has developed a risk profile toidentify high-risk practices in radiotherapyand suggest specifically targetedinterventions to improve patient safety (Part2 of this document).
CONCLUSION
28
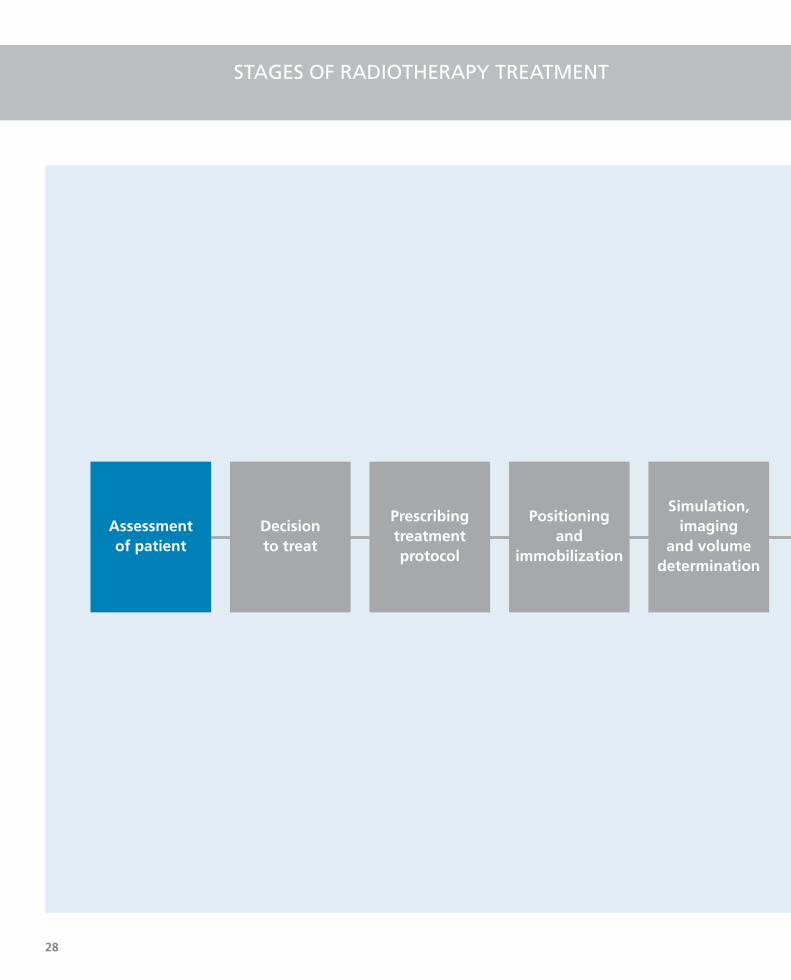
STAGES OF RADIOTHERAPY TREATMENT
Decision to treat
Prescribingtreatmentprotocol
Positioningand
immobilization
Simulation,imaging
and volumedetermination
Assessment of patient
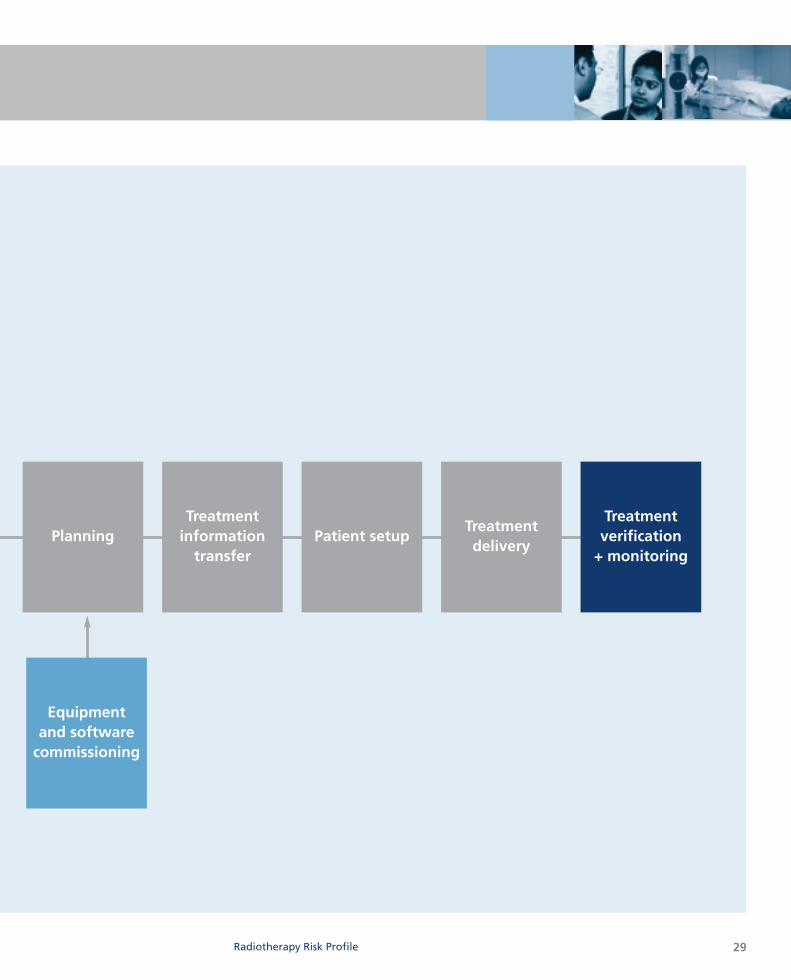
29Radiotherapy Risk Profile
Equipment and software
commissioning
Treatmentdelivery
Patient setupPlanningTreatment verification
+ monitoring
Treatment information
transfer
30
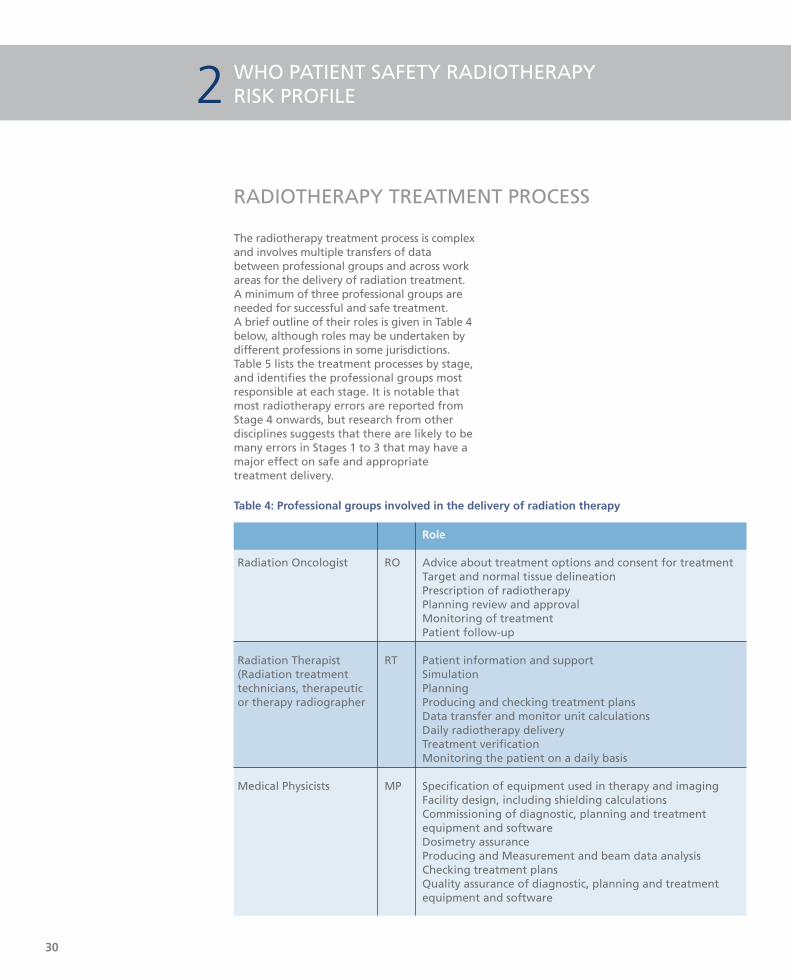
Role
Radiation Oncologist RO Advice about treatment options and consent for treatmentTarget and normal tissue delineationPrescription of radiotherapyPlanning review and approval Monitoring of treatmentPatient follow-up
Radiation Therapist RT Patient information and support(Radiation treatment Simulationtechnicians, therapeutic Planningor therapy radiographer Producing and checking treatment plans
Data transfer and monitor unit calculationsDaily radiotherapy deliveryTreatment verificationMonitoring the patient on a daily basis
Medical Physicists MP Specification of equipment used in therapy and imagingFacility design, including shielding calculationsCommissioning of diagnostic, planning and treatment equipment and softwareDosimetry assuranceProducing and Measurement and beam data analysis Checking treatment plansQuality assurance of diagnostic, planning and treatment equipment and software
WHO PATIENT SAFETY RADIOTHERAPY RISK PROFILE2
The radiotherapy treatment process is complexand involves multiple transfers of databetween professional groups and across workareas for the delivery of radiation treatment. A minimum of three professional groups areneeded for successful and safe treatment. A brief outline of their roles is given in Table 4below, although roles may be undertaken bydifferent professions in some jurisdictions.Table 5 lists the treatment processes by stage,and identifies the professional groups mostresponsible at each stage. It is notable thatmost radiotherapy errors are reported fromStage 4 onwards, but research from otherdisciplines suggests that there are likely to bemany errors in Stages 1 to 3 that may have amajor effect on safe and appropriatetreatment delivery.
Table 4: Professional groups involved in the delivery of radiation therapy
RADIOTHERAPY TREATMENT PROCESS

31
Note: Professions responsible for process stages vary between countries
Radiotherapy Risk Profile
Stage Description ResponsibilityRO RT MP
1 Assessment of patient History taking, physical examination, •review of diagnostic material
2 Decision to treat Consideration of guidelines, patient •wishes
3 Prescribing treatment protocol Determination of site, total dose,
•fractionation and additional measuressuch as dental review or concurrent chemotherapy
4 Positioning and immobilization Setting up the patient in a •reproducible position for accurate
daily treatment
5 Simulation, imaging and Determining region of the body to be
• •volume determination treated using diagnostic plain X-ray unit with the same geometry as a treatment unit (simulator) or dedicated CT scanner
6 Planning Determining X-ray beam arrangement • •and shielding then calculating dose to
achieve prescription
7 Treatment information transfer Transfer beam arrangement and• •dose data from treatment plan to
treatment machine
8 Patient setup Placing patient in treatment position •for each treatment
9 Treatment delivery Physical delivery of radiation dose • •
10 Treatment verification and Confirmation of treatment delivery
• • •monitoring using port films and dosimeters
Monitoring of the daily setupMonitoring of tolerance by regular patient review
Table 5:Treatment processes and identification of the professional groups responsible for each process.
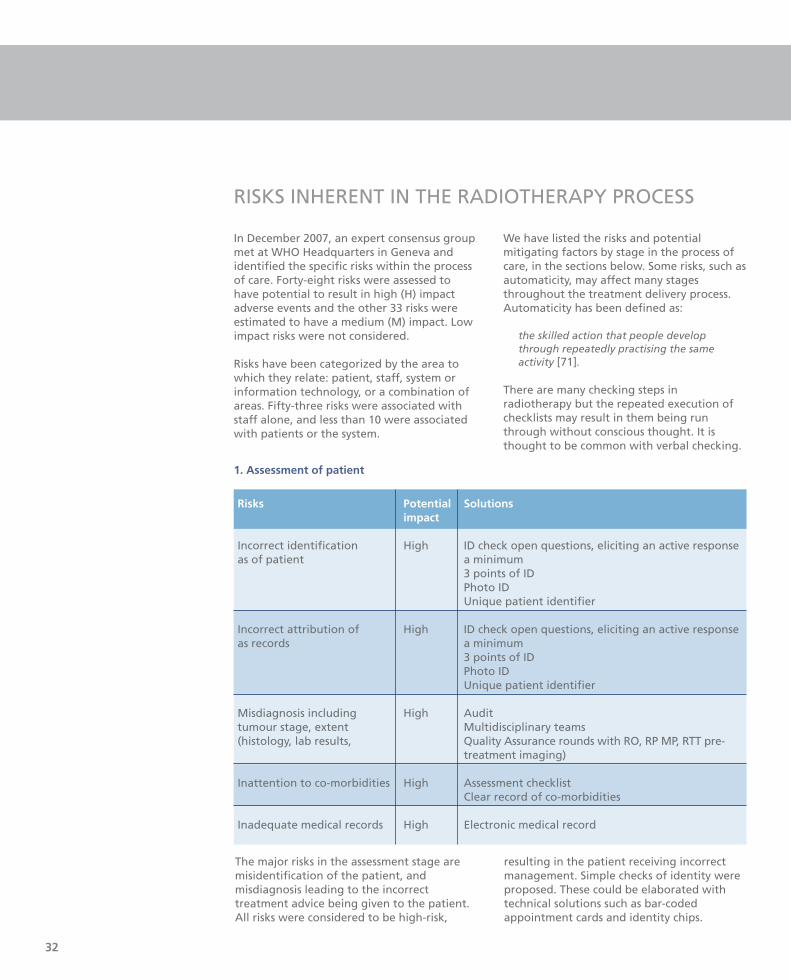
In December 2007, an expert consensus groupmet at WHO Headquarters in Geneva andidentified the specific risks within the processof care. Forty-eight risks were assessed tohave potential to result in high (H) impactadverse events and the other 33 risks wereestimated to have a medium (M) impact. Lowimpact risks were not considered.
Risks have been categorized by the area towhich they relate: patient, staff, system orinformation technology, or a combination ofareas. Fifty-three risks were associated withstaff alone, and less than 10 were associatedwith patients or the system.
We have listed the risks and potentialmitigating factors by stage in the process ofcare, in the sections below. Some risks, such asautomaticity, may affect many stagesthroughout the treatment delivery process.Automaticity has been defined as:
the skilled action that people developthrough repeatedly practising the sameactivity [71].
There are many checking steps inradiotherapy but the repeated execution ofchecklists may result in them being runthrough without conscious thought. It isthought to be common with verbal checking.
32
1. Assessment of patient
Risks Potential Solutionsimpact
Incorrect identification High ID check open questions, eliciting an active responseas of patient a minimum
3 points of IDPhoto IDUnique patient identifier
Incorrect attribution of High ID check open questions, eliciting an active responseas records a minimum
3 points of ID Photo IDUnique patient identifier
Misdiagnosis including High Audittumour stage, extent Multidisciplinary teams (histology, lab results, Quality Assurance rounds with RO, RP MP, RTT pre-
treatment imaging)
Inattention to co-morbidities High Assessment checklist Clear record of co-morbidities
Inadequate medical records High Electronic medical record
RISKS INHERENT IN THE RADIOTHERAPY PROCESS
The major risks in the assessment stage aremisidentification of the patient, andmisdiagnosis leading to the incorrecttreatment advice being given to the patient.All risks were considered to be high-risk,
resulting in the patient receiving incorrectmanagement. Simple checks of identity wereproposed. These could be elaborated withtechnical solutions such as bar-codedappointment cards and identity chips.
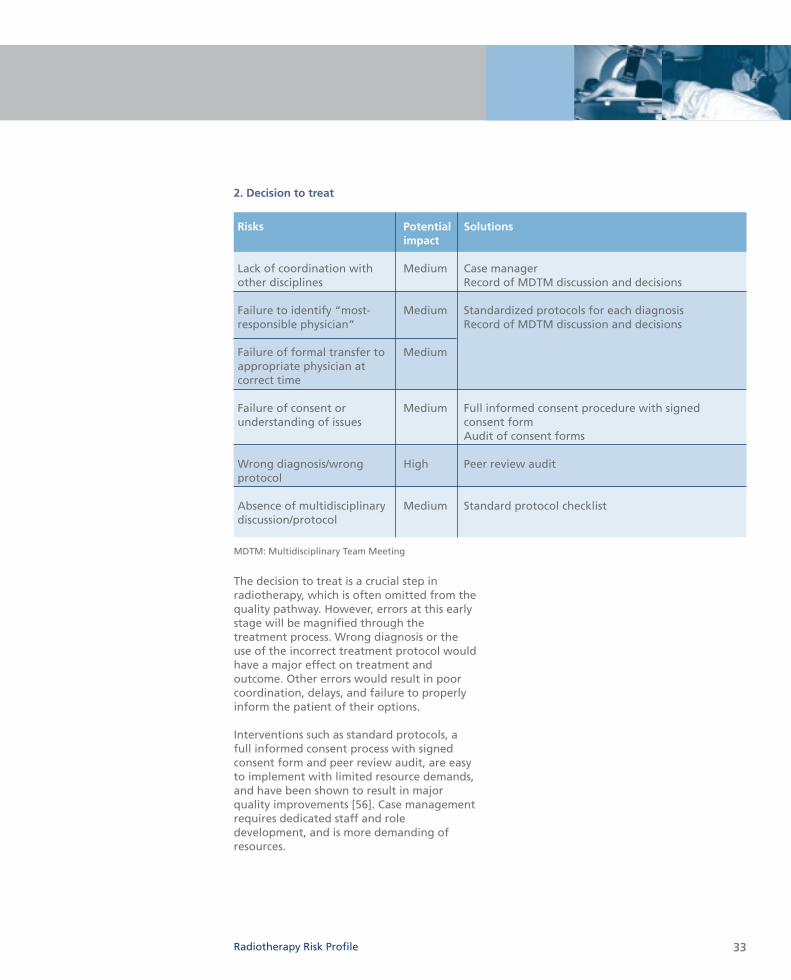
2. Decision to treat
Risks Potential Solutionsimpact
Lack of coordination with Medium Case managerother disciplines Record of MDTM discussion and decisions
Failure to identify “most- Medium Standardized protocols for each diagnosisresponsible physician” Record of MDTM discussion and decisions
Failure of formal transfer to Mediumappropriate physician at correct time
Failure of consent or Medium Full informed consent procedure with signed understanding of issues consent form
Audit of consent forms
Wrong diagnosis/wrong High Peer review auditprotocol
Absence of multidisciplinary Medium Standard protocol checklistdiscussion/protocol
33
The decision to treat is a crucial step inradiotherapy, which is often omitted from thequality pathway. However, errors at this earlystage will be magnified through thetreatment process. Wrong diagnosis or theuse of the incorrect treatment protocol wouldhave a major effect on treatment andoutcome. Other errors would result in poorcoordination, delays, and failure to properlyinform the patient of their options.
Interventions such as standard protocols, afull informed consent process with signedconsent form and peer review audit, are easyto implement with limited resource demands,and have been shown to result in majorquality improvements [56]. Case managementrequires dedicated staff and roledevelopment, and is more demanding ofresources.
Radiotherapy Risk Profile
MDTM: Multidisciplinary Team Meeting
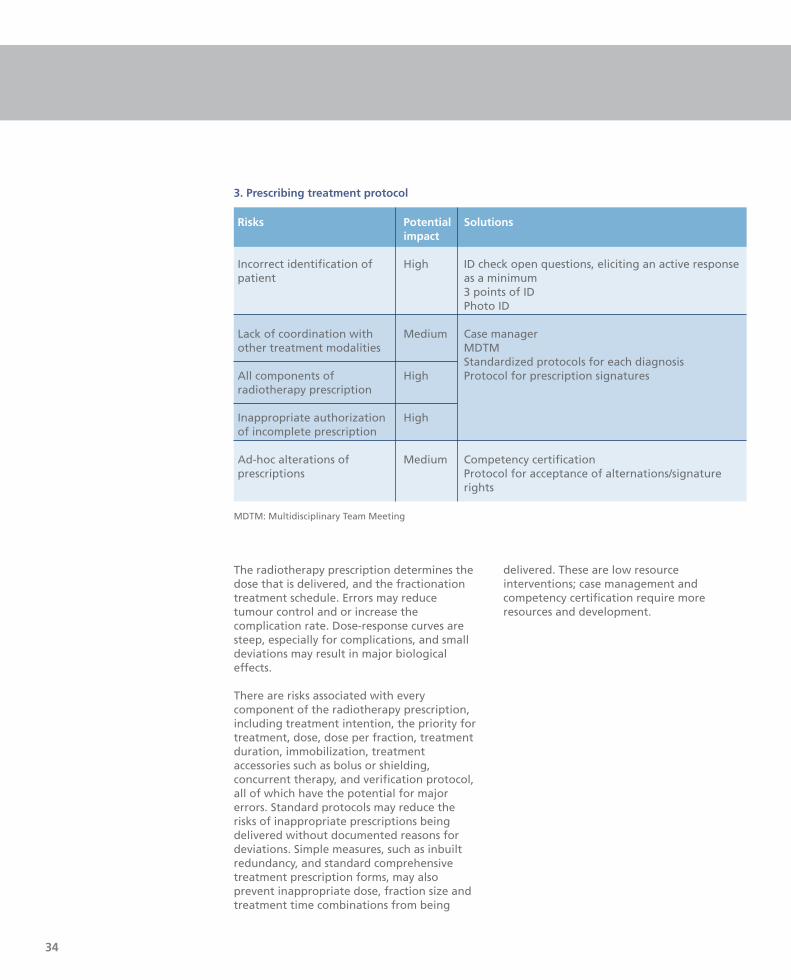
Risks Potential Solutionsimpact
Incorrect identification of High ID check open questions, eliciting an active responsepatient as a minimum
3 points of IDPhoto ID
Lack of coordination with Medium Case managerother treatment modalities MDTM
Standardized protocols for each diagnosisAll components of High Protocol for prescription signatures radiotherapy prescription
Inappropriate authorization Highof incomplete prescription
Ad-hoc alterations of Medium Competency certificationprescriptions Protocol for acceptance of alternations/signature
rights
MDTM: Multidisciplinary Team Meeting
3. Prescribing treatment protocol
34
The radiotherapy prescription determines thedose that is delivered, and the fractionationtreatment schedule. Errors may reducetumour control and or increase thecomplication rate. Dose-response curves aresteep, especially for complications, and smalldeviations may result in major biologicaleffects.
There are risks associated with everycomponent of the radiotherapy prescription,including treatment intention, the priority fortreatment, dose, dose per fraction, treatmentduration, immobilization, treatmentaccessories such as bolus or shielding,concurrent therapy, and verification protocol,all of which have the potential for majorerrors. Standard protocols may reduce therisks of inappropriate prescriptions beingdelivered without documented reasons fordeviations. Simple measures, such as inbuiltredundancy, and standard comprehensivetreatment prescription forms, may alsoprevent inappropriate dose, fraction size andtreatment time combinations from being
delivered. These are low resourceinterventions; case management andcompetency certification require moreresources and development.

Risks Potential Solutionsimpact
Patient-related factors – Medium Patient selection Comprehensive assessment and co-morbid disease, inability documentation of difficulties to comply with instructions
Incorrect patient positioning High Planning protocol checklistIndependent checking
Different positioning for Medium Adequate staffing levels and education different imaging modalities In vivo dosimetry
Incorrect immobilization Mediumposition
Wrongly applied Mediumimmobilization device
Inaccurate transfer of Highprescription
4. Positioning and immobilization
Radiotherapy Risk Profile
Radiotherapy is given daily and a full coursemay take up to seven weeks or longer.Patients are positioned and immobilized sothat they will be in the correct position fortreatment during the course of radiotherapy.Incorrect positioning or poor immobilizationwill result in the tumour not receiving theintended dose, resulting in a greater risk ofrecurrence or in sensitive normal tissues beingtreated beyond tolerance. High-precisiontechniques such as radiosurgery and intensitymodulated radiation treatment place greatdemands on accurate and reproduciblepatient positioning and immobilization.
Patients need to be able to comply with therequirements of positioning, and manyfactors may impede their ability to becorrectly positioned and immobilized,including co-morbidities such as pain andorthopnoea, inability to comply withinstructions due to poor communication orconfusion, and psychological barriers such asclaustrophobia. These are generally difficultto overcome and often reflect poor patient
selection or poor choice of radiotherapymodality, and failure to identify patient-related problems at the time that thetreatment decision is made.
All other risks identified could be reduced bythe development and implementation of aplanning protocol checklist, which wouldhave low resource demands. Checklists areused in many departments, and somejurisdictions have developed checklists for thispurpose [72].
35
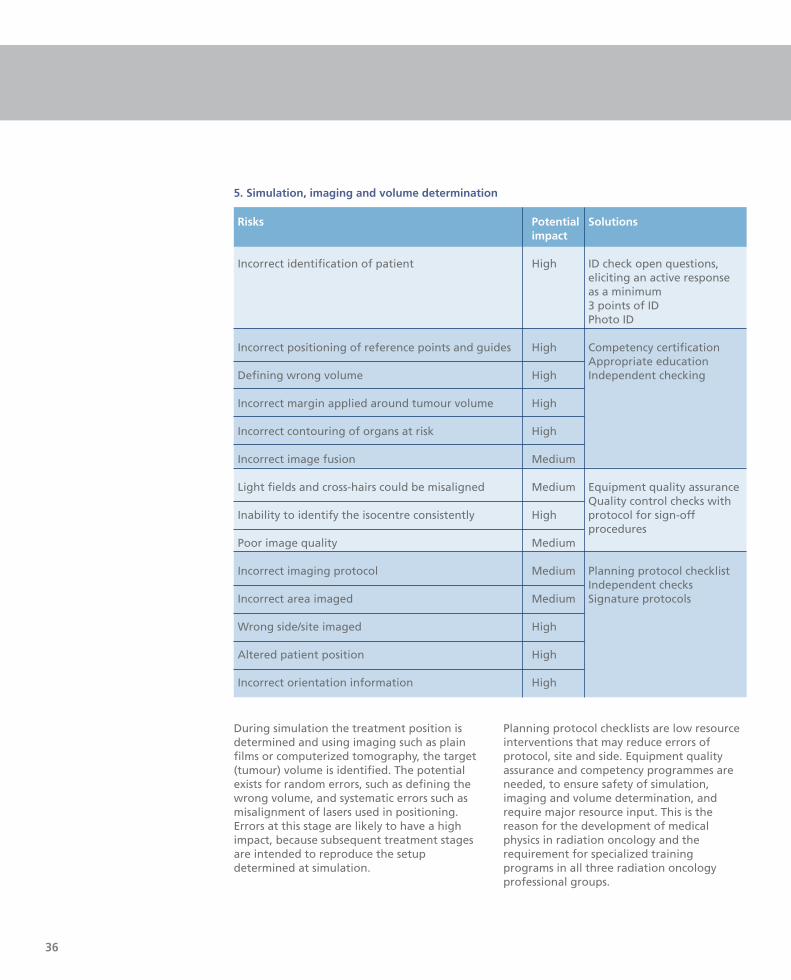
During simulation the treatment position isdetermined and using imaging such as plainfilms or computerized tomography, the target(tumour) volume is identified. The potentialexists for random errors, such as defining thewrong volume, and systematic errors such asmisalignment of lasers used in positioning.Errors at this stage are likely to have a highimpact, because subsequent treatment stagesare intended to reproduce the setupdetermined at simulation.
Planning protocol checklists are low resourceinterventions that may reduce errors ofprotocol, site and side. Equipment qualityassurance and competency programmes areneeded, to ensure safety of simulation,imaging and volume determination, andrequire major resource input. This is thereason for the development of medicalphysics in radiation oncology and therequirement for specialized trainingprograms in all three radiation oncologyprofessional groups.
36
Risks Potential Solutionsimpact
Incorrect identification of patient High ID check open questions, eliciting an active responseas a minimum3 points of IDPhoto ID
Incorrect positioning of reference points and guides High Competency certificationAppropriate education
Defining wrong volume High Independent checking
Incorrect margin applied around tumour volume High
Incorrect contouring of organs at risk High
Incorrect image fusion Medium
Light fields and cross-hairs could be misaligned Medium Equipment quality assuranceQuality control checks with
Inability to identify the isocentre consistently High protocol for sign-offprocedures
Poor image quality Medium
Incorrect imaging protocol Medium Planning protocol checklistIndependent checks
Incorrect area imaged Medium Signature protocols
Wrong side/site imaged High
Altered patient position High
Incorrect orientation information High
5. Simulation, imaging and volume determination

37
During radiotherapy planning, a softwaremodel is used to design treatment beamarrangements, shielding, and calculate dose.Software is individualized for each treatmentmachine to model the beam characteristics.Errors can arise in the commissioning processthat will affect every treatment or, becausethe software is misused, to producetreatment plans under conditions it is notable to accurately model [43, 45-46]. Inaddition, random errors may occur due toincorrect inputs into individual plans. Thereare many steps in the planning and
calculation of patient treatments. Anexhaustive list can be found in the IAEAQATRO protocol [8].
Commissioning Quality Assurance andcompetency certification are needed toprevent major systematic errors. Protocolsshould be in place and checking should beundertaken by independent professionalgroups.
Planning protocol checklists will reduce therandom errors in individual plans.
Radiotherapy Risk Profile
Risks Potential Solutionsimpact
Incorrect calibration or incorrect output data High Equipment quality assurancegeneration External independent
dosimetry comparison audits Protocols and sign-off procedures and audits
Incorrect physical data such as decay curves and High Independent checkstables of constants Planning protocols
In vivo dosimetry
Faulty planning software High Commissioning Quality Incorrectly commissioned planning software High Assurance Sign-off procedures
In vivo dosimetry
Misuse of planning software High Competency certificationErroneous monitor unit calculation High Manual check by
independent professionalIn vivo dosimetry
Lack of independent cross-checking High Departmental policy
Incorrect treatment modalities and beam positioning High Planning protocol checklistIncorrect beam energy High Signature protocols and Incorrect beam size High independent checkingIncorrect normalizations HighIncorrect prescription point MediumIncorrect inhomogeneity correction MediumIncorrect use of bolus in calculation HighWrongly sited blocks HighPoorly constructed blocks HighWrong depth dose chart for wrong machine High
Utilization of non-standard protocols Medium Standard protocol checklist
6. Planning

Risks Potential Solutionsimpact
Incorrect identification of patient High ID check open questions, eliciting an active response as a minimum3 points of ID Photo ID
Manual data entry Medium Automated data transferIn vivo dosimetry
Incompatible chart design Medium Clear documentation and protocols
Illegible handwriting for manual transfers High
No independent check High
Incorrect or inadequate data entry on ‘record & High Independent checkingverify’ system
Ambiguous or poorly designed prescription sheet High Model prescription sheet
Sending unapproved plan Medium Protocol checklist
Failure to communicate changes in plans Medium ‘Record and verify’ systemsIndependent checks
Incorrect number of monitor units, accessories, High In vivo dosimetrywedges
The transfer of information from the plan tothe treatment machine is a critical step. Itmay require software from different vendorsto interface correctly, or require correctmanual data entry. Random and systematicerrors may occur. Protocol checklists willprevent the implementation of unauthorizedplans, and clear documentation standards willreduce errors from poor record keeping andhandwriting. Signature policies should be inplace and audited.
Independent checking is a mainstay of errorreduction from transcription andcommunication errors, but is subject toautomaticity errors. Modern ‘‘record andverify’’ systems reduce random transcriptionerrors, but require quality assurance regimensto prevent systematic errors.
7. Treatment information transfer
38
39
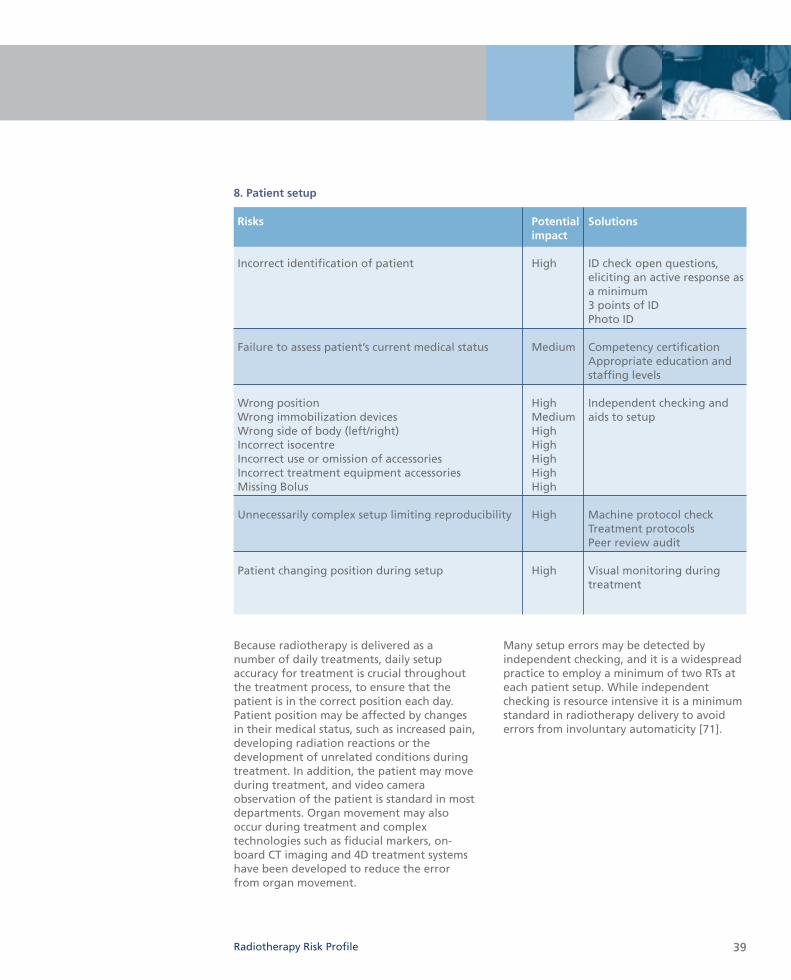
Because radiotherapy is delivered as anumber of daily treatments, daily setupaccuracy for treatment is crucial throughoutthe treatment process, to ensure that thepatient is in the correct position each day.Patient position may be affected by changesin their medical status, such as increased pain,developing radiation reactions or thedevelopment of unrelated conditions duringtreatment. In addition, the patient may moveduring treatment, and video cameraobservation of the patient is standard in mostdepartments. Organ movement may alsooccur during treatment and complextechnologies such as fiducial markers, on-board CT imaging and 4D treatment systemshave been developed to reduce the errorfrom organ movement.
Many setup errors may be detected byindependent checking, and it is a widespreadpractice to employ a minimum of two RTs ateach patient setup. While independentchecking is resource intensive it is a minimumstandard in radiotherapy delivery to avoiderrors from involuntary automaticity [71].
Radiotherapy Risk Profile
Risks Potential Solutionsimpact
Incorrect identification of patient High ID check open questions, eliciting an active response asa minimum3 points of ID Photo ID
Failure to assess patient’s current medical status Medium Competency certificationAppropriate education and staffing levels
Wrong position High Independent checking and Wrong immobilization devices Medium aids to setupWrong side of body (left/right) HighIncorrect isocentre HighIncorrect use or omission of accessories HighIncorrect treatment equipment accessories HighMissing Bolus High
Unnecessarily complex setup limiting reproducibility High Machine protocol check Treatment protocolsPeer review audit
Patient changing position during setup High Visual monitoring during treatment
8. Patient setup

Risks Potential Solutionsimpact
Undetected equipment failure High Machine protocol checkIn vivo dosimetry
Operating equipment in physics mode rather than High Machine protocol checkclinical mode In vivo dosimetry
Incorrect identification of patient High ID check open questions, eliciting an active response as a minimum3 points of ID Photo ID
Poor patient handling and care Medium Competency certification
Incorrect beam energy High In vivo-dosimetry
Incorrect field size and orientation High Independent checkingIn vivo dosimetry
Too many fractions or too few Medium
Inadequate checking of treatment parameters High
Failure to follow machine start up procedures Medium Machine protocol check
The major risk in treatment delivery isincorrect beam output due to incorrectcalibration of the beam at commissioning orat a later date, or the generation of incorrectdata used to calculate treatment time ormonitor units. This would result in asystematic error [38, 47] that could affecthundreds or thousands of patients.Considerable effort is dedicated to ensuringand maintaining beam output in high incomecountries [73]. An IAEA postal survey [54] oflow and middle income countries showedthat 84% of centres were within the 5%tolerance limit. Centres without radiationmeasurement devices and qualified physicsstaff were more likely to have doses outsidethe tolerance limits. Equipment qualityassurance programmes are resource intensiveand require specialist personnel (medicalphysicists and engineers), specializedequipment and replacement parts.
The other risks identified relate to randomerrors that may affect individual treatmentsor courses. Independent checking reduces therisk of many of these errors [71]. In vivodosimetry using radiation detectors, such asdiodes or thermoluminescent dosimetry, mayreveal incorrect beam energy or incorrectcalibration. In addition, if used systematicallynear the start of treatment, for the majorityof patients it can provide an independentfinal check of many of the proceduresinvolved in treatment planning and patientdose delivery, provided that it has not beencalibrated with the same beam that it issupposed to be checking.
40
9. Treatment delivery
Risks Potential Solutionsimpact
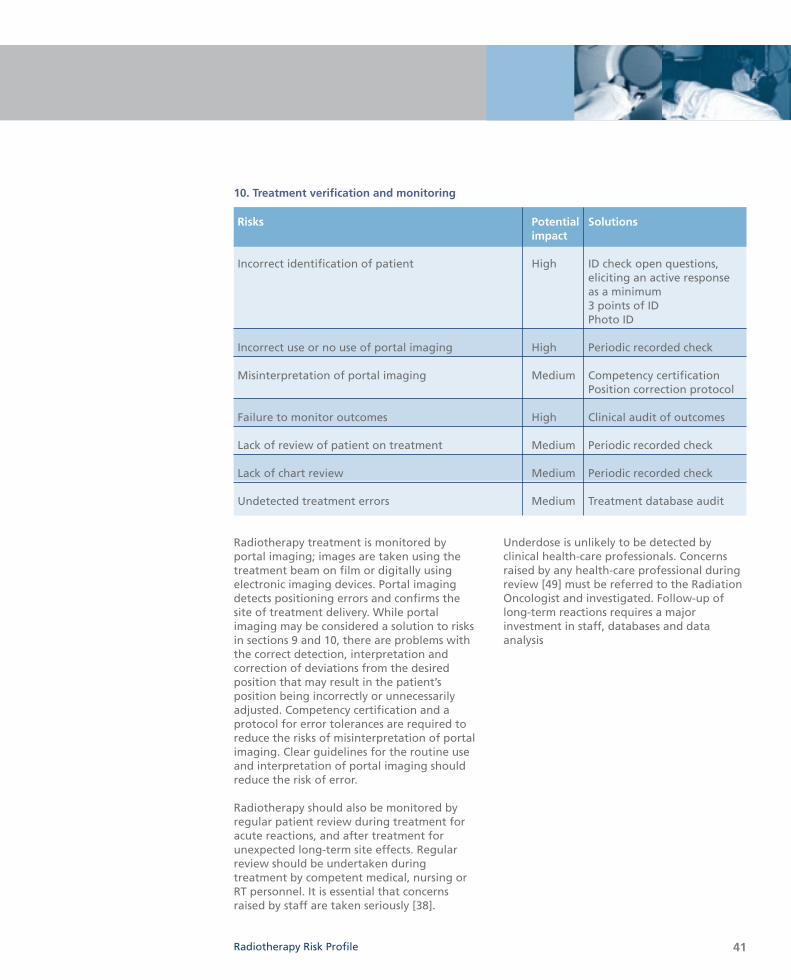
Incorrect identification of patient High ID check open questions, eliciting an active response as a minimum3 points of IDPhoto ID
Incorrect use or no use of portal imaging High Periodic recorded check
Misinterpretation of portal imaging Medium Competency certificationPosition correction protocol
Failure to monitor outcomes High Clinical audit of outcomes
Lack of review of patient on treatment Medium Periodic recorded check
Lack of chart review Medium Periodic recorded check
Undetected treatment errors Medium Treatment database audit
10. Treatment verification and monitoring
Radiotherapy Risk Profile
Radiotherapy treatment is monitored byportal imaging; images are taken using thetreatment beam on film or digitally usingelectronic imaging devices. Portal imagingdetects positioning errors and confirms thesite of treatment delivery. While portalimaging may be considered a solution to risksin sections 9 and 10, there are problems withthe correct detection, interpretation andcorrection of deviations from the desiredposition that may result in the patient’sposition being incorrectly or unnecessarilyadjusted. Competency certification and aprotocol for error tolerances are required toreduce the risks of misinterpretation of portalimaging. Clear guidelines for the routine useand interpretation of portal imaging shouldreduce the risk of error.
Radiotherapy should also be monitored byregular patient review during treatment foracute reactions, and after treatment forunexpected long-term site effects. Regularreview should be undertaken duringtreatment by competent medical, nursing orRT personnel. It is essential that concernsraised by staff are taken seriously [38].
Underdose is unlikely to be detected byclinical health-care professionals. Concernsraised by any health-care professional duringreview [49] must be referred to the RadiationOncologist and investigated. Follow-up oflong-term reactions requires a majorinvestment in staff, databases and dataanalysis
41

Several interventions are likely to be effectiveat reducing risks at multiple stages in theradiotherapy treatment process. Planningprotocol checklists are relevant to 20identified risks, independent checking to 12risks, and specific competency certification to11 risks (Table 6). This may be because thereare more risks in these areas or because theindividual risks have been better identified.
Other high impact interventions include:
• Equipment quality assurance to reducethe risk of systematic errors such asmiscalibration that may affect very largenumbers of patients.
• Peer review audit to improve decisionmaking that will have flow-on effectsthroughout the treatment process.
• In vivo dosimetry may mitigate 24identified risk areas and provide animportant independent check of theplanning, calculation and deliveryelements of the pathway and address 12of 16 risks in planning, 5 of 10 intreatment transfer, 4 of 11 in patient set-up and 3 of 7 in treatment delivery. Thecosts of establishing and maintaining aprogram of routine in vivo dosimetry forall treatments is likely to be high andresource intensive, which may place itbeyond the reach of services in somecountries.
In addition there are safety processes thatapply to all stages of the delivery ofradiotherapy:
1. Patient identification
2. Audit of equipment commissioning andprocesses
3. Staff competency assessment
4. Process and equipment quality assurance
5. Information transfer with redundancy
6. Process governance
7. Error reporting and quality improvement
8. External checking
9. Adequate staffing
Continuing to learn
This risk profile for the first time quantifiesthe process of care in radiotherapy, andsystematically addresses the risks at eachstage. Putting this knowledge to work willrequire innovative strategies on behalf ofmanagers and health-care professionals alike.
Redesigning systems to reduce risk involvesengaging policy-makers, managers andpatients [74]. Central to this is an adequateand competent workforce, supported by anappropriate reporting and learningframework. Several efforts have beenattempted, both nationally andinternationally to this end, including theRadiation Oncology Safety InformationSystem (ROSIS) [34], the Calgary incidentlearning system [28] and the recentlydescribed United Kingdom framework [52].
Technical solutions offer hope for the future,including in vivo dosimetry, which offers theopportunity to reduce some risk, but must beput in the context of an overall approach topatient safety in radiotherapy.
The use of simple checklists has been provedto be successful in other areas of patientsafety as a way of systematically reducing risk[75]. Similar systems have been suggested inradiotherapy and should be further promotedand developed [76].
42
RISK REDUCTION INTERVENTIONS
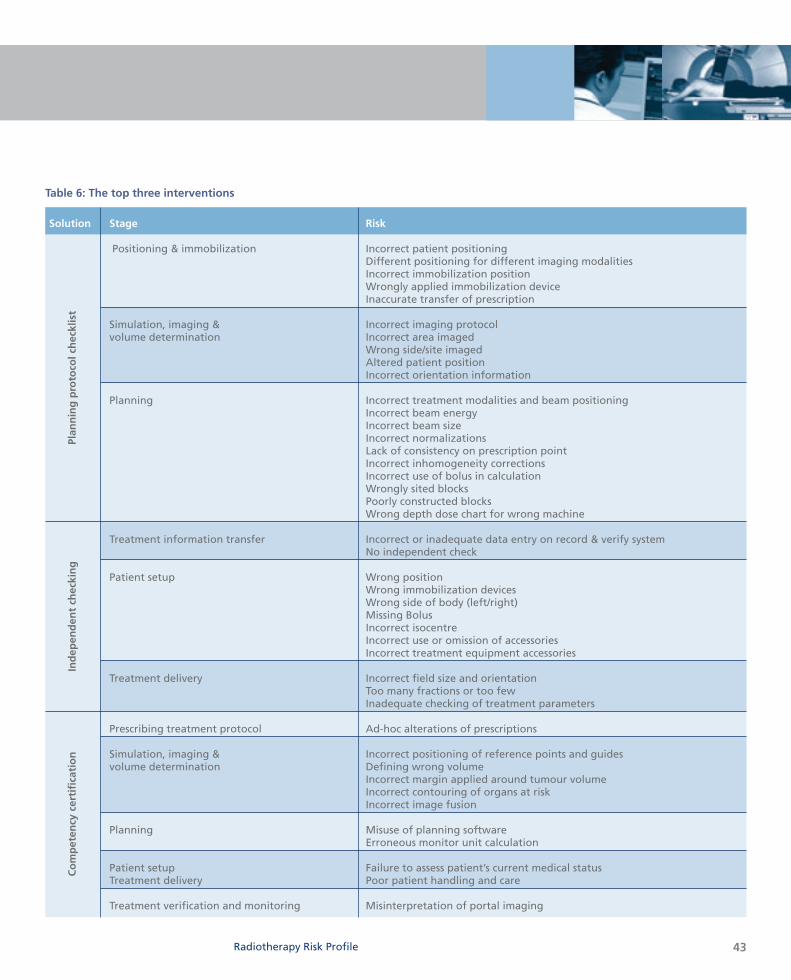
Solution Stage Risk
Positioning & immobilization Incorrect patient positioningDifferent positioning for different imaging modalitiesIncorrect immobilization positionWrongly applied immobilization deviceInaccurate transfer of prescription
Simulation, imaging & Incorrect imaging protocolvolume determination Incorrect area imaged
Wrong side/site imagedAltered patient positionIncorrect orientation information
Planning Incorrect treatment modalities and beam positioningIncorrect beam energyIncorrect beam sizeIncorrect normalizationsLack of consistency on prescription pointIncorrect inhomogeneity correctionsIncorrect use of bolus in calculationWrongly sited blocksPoorly constructed blocksWrong depth dose chart for wrong machine
Treatment information transfer Incorrect or inadequate data entry on record & verify systemNo independent check
Patient setup Wrong positionWrong immobilization devicesWrong side of body (left/right)Missing Bolus Incorrect isocentreIncorrect use or omission of accessoriesIncorrect treatment equipment accessories
Treatment delivery Incorrect field size and orientationToo many fractions or too fewInadequate checking of treatment parameters
Prescribing treatment protocol Ad-hoc alterations of prescriptions
Simulation, imaging & Incorrect positioning of reference points and guidesvolume determination Defining wrong volume
Incorrect margin applied around tumour volumeIncorrect contouring of organs at riskIncorrect image fusion
Planning Misuse of planning softwareErroneous monitor unit calculation
Patient setup Failure to assess patient’s current medical statusTreatment delivery Poor patient handling and care
Treatment verification and monitoring Misinterpretation of portal imaging
Table 6: The top three interventions
Plan
nin
g p
roto
col c
hec
klis
tIn
dep
end
ent
chec
kin
gC
om
pet
ency
cer
tifi
cati
on
Radiotherapy Risk Profile 43

An extensive search of the ‘Google’ and‘Google Scholar’ search engines wasconducted for online publications and asearch of the ‘PubMed’ database wasconducted for relevant journal publications,supplemented by searches of ‘relevant links’for appropriate citations and articlebibliographies for further relevant sources.Articles published in all languages between1976 and 2007 were included. Unpublishedmaterials (e.g. ROSIS database, Liverpool
Hospital incident report collection) werecollected from personal communication withthe radiotherapy professionals locally andinternationally. The summary of the mostrelevant search engines, search terms withnumber of hits and the search results (carriedout in August-September 2007) are asfollows:
Annex I: Literature search strategy and results
Search terms Google PubMed Search resultsScholar ‘review’
articlesNo. of hits As a “Phrase” No. of
anywhere in hitstext
Radiotherapy incident/s 7410/8130 4/4 24/11 Total no. sites searched: 1330Radiotherapy overexposure 670 1 3 ⇓
Radiation protection AND 462000 26 358 No. of abstract reading ofradiotherapy relevant references: 86Patient safety AND 234000 3 4 ⇓
radiotherapyQuality assurance AND 7670 199 526 No. of full text/executive radiotherapy summary readings of most
relevant references (articles, reports, websites): 68
QA AND radiotherapy 7940 20 12 ⇓
Safety measures AND 8880 12 10 References included in this radiotherapy report
References for incident data:26Other references: 47Total references: 73
Radiotherapy accidents 2200 2 2AND developing countries
ANNEX I: LITERATURE SEARCH STRATEGY AND RESULTS
44
SEARCH STRATEGY FOR ARTICLES
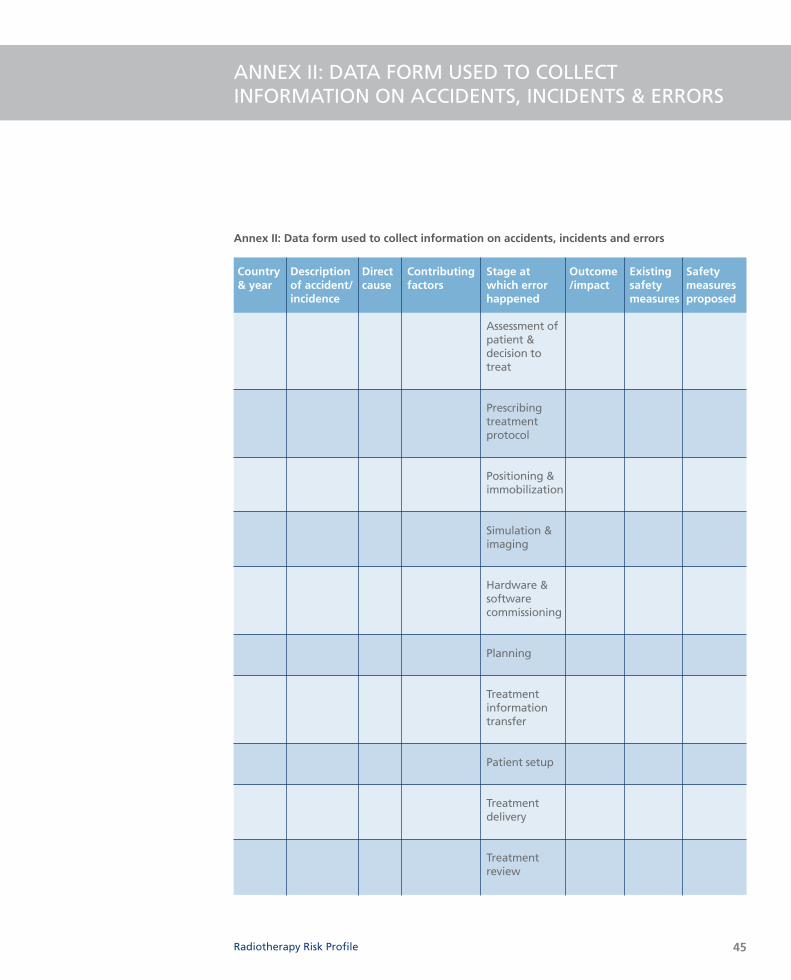
ANNEX II: DATA FORM USED TO COLLECTINFORMATION ON ACCIDENTS, INCIDENTS & ERRORS
Annex II: Data form used to collect information on accidents, incidents and errors
Country Description Direct Contributing Stage at Outcome Existing Safety & year of accident/ cause factors which error /impact safety measures
incidence happened measures proposed
Assessment of patient & decision to treat
Prescribing treatment protocol
Positioning & immobilization
Simulation & imaging
Hardware & software commissioning
Planning
Treatment information transfer
Patient setup
Treatment delivery
Treatment review
Radiotherapy Risk Profile 45
REFERENCES
46
References
1. Delaney G et al. The role of radiotherapy in cancertreatment: Estimating optimal utilization from areview of evidence-based clinical guidelines. Cancer,2005, 104:1129–1137.
2. The Swedish Council on Technology Assessment inHealth Care (SBU). Systematic Overview ofRadiotherapy for Cancer including a ProspectiveSurvey of Radiotherapy Practice in Sweden 2001 –Summary and Conclusions. Acta Oncologica, 2003,42:357–365.
3. International Commission on Radiation Units andMeasurements (ICRU). Determination of AbsorbedDose in a Patient Irradiated by Beams of X orGamma Rays in Radiotherapy Procedures. ICRUReport 24. Bethesda, MD: ICRU, 1976.
4. Brahme A et al. Accuracy requirements and qualityassurance of external beam therapy with photonsand electrons. Acta Oncologica, (Suppl. 1) 1988.
5. Mijnheer BJ, Battermann JJ, Wambersie A. Whatdegree of accuracy is required and can be achievedin photon and neutron therapy? Radiotherapy andOncology, 1987, 8:237–252.
6. Mijnheer BJ, Battermann JJ, Wambersie A. Reply to:Precision and accuracy in radiotherapy.Radiotherapy and Oncology, 1989, 14:163–167.
7. World Health Organization (WHO). QualityAssurance in Radiotherapy. Geneva: WHO, 1988.
8. Comprehensive audits of radiotherapy practices: atool for quality improvement: Quality AssuranceTeam for Radiation Oncology (QUATRO) — Vienna:International Atomic Energy Agency, 2007.
9. Setting up a radiotherapy programme: clinical,medical physics, radiation protection and safetyaspects. — Vienna: International Atomic EnergyAgency (IAEA), 2008.
10. International Commission on RadiologicalProtection (ICRP). Radiological Protection and Safetyin Medicine. ICRP 73. Annals of the ICRP, 1996, Vol.26, Num. 2.
11. European Commission. Guidelines on education andtraining in radiation protection for medicalexposures. Radiation Protection 116. EnvironmentDirectorate-General, Office for Official Publicationsof the European Communities, Luxembourg, 2000.
12. Kutcher GJ et al. Comprehensive QA for radiationoncology: report of AAPM Radiation TherapyCommittee Task Group 40. Medical Physics, 1994,21:581–618.
13. Leer JW et al. Practical guidelines for theimplementation of a quality system in radiotherapy.ESTRO Physics for Clinical Radiotherapy Booklet No.4. Brussels, Belgium: European Society forTherapeutic Radiology and Oncology (ESTRO), 1998.
14. Novotny J et al. A Quality assurance network inCentral European countries: RadiotherapyInfrastructure. Acta Oncologica, 1998, 37(2),159–165.
15. Thwaites DI et al. Quality assurance in radiotherapy,Radiotherapy and Oncology, 1995, 35:61–73.
16. International Atomic Energy Agency (IAEA). Lessonslearned from accidents in radiotherapy. Vienna,Austria: IAEA, 2000. (Safety Reports Series 17).
17. Prevention of accidental exposures to patientsundergoing radiation therapy: A report of theInternational Commission on Radiological Protection(ICRP). Annals of the ICRP, 2000, 30(3):7–70.
18. Holmberg O. Accident prevention in radiotherapy.Biomedical Imaging and Intervention Journal, 2007,3(2):e27. (http://www.biij.org/2007/2/e27, accessed18 June 2007)
19. IAEA Training Material on Radiation Protection inRadiotherapy. Part 7: Design of facilities and shielding.(http://rpop.iaea.org/RPoP/RPoP/Content/Documents/TrainingRadiotherapy/Lectures/RT07_shield1_Facilitydesign_WEB.ppt, accessed 30 October 2007)
20. Huang G et al. Error in the delivery of radiationtherapy: results of a quality assurance review.International Journal of Radiation Oncology BiologyPhysics, 2005, 61(5):1590–1595.
21. Patton G, Gaffney D, Moeller J. Facilitation ofradiotherapeutic error by computerized record andverify systems. International Journal of RadiationOncology Biology Physics, 2003, 56(1):50–57.
22. IAEA safety glossary: Terminology used in nuclearsafety and radiation protection. 2007 Edition.Available at: http://www-pub.iaea.org/MTCD/publications/PDF/Pub1290_web.pdf. accessed 30 July 2008.
23. International Classification for Patient Safety (ICPS).World Health Organisation (WHO). Available at:http://www.who.int/patientsafety/taxonomy/en/.Accessed 24th June 2008.
24. Ortiz P, Oresegun M, Wheatley J. Lessons frommajor radiation accidents. IAEA publication.(http://www.irpa.net/irpa10/cdrom/00140.pdf,accessed 11 October 2007)
25. Holmberg O, McClean B. Preventing treatmenterrors in radiotherapy by identifying and evaluatingnear-misses and actual incidents. Journal ofRadiotherapy in Practice, 2002, 3:13–25.
26. Williams MV. Improving patient safety inradiotherapy by learning from near-misses, incidentsand errors. British Journal of Radiology, 2007,80(953):297–301.
27. Hamilton C, Oliver L, Coulter K. How safe isAustralian radiotherapy? Australasian Radiology,2003, 47(4):428–433.
28. A reference guide for learning from incidents inradiation treatment: HTA Initiative #22. AlbertaHeritage Foundation for Medical Research, 2006. (http://www.ihe.ca/documents/hta/HTA-FR22.pdf,accessed 27 July 2008)
29. Barach P, Small SD. Reporting and preventingmedical mishaps: lessons from non-medical near-miss reporting systems. British Medical Journal,2000, 320:759–763.
30. Yeung TK et al. Quality assurance in radiotherapy:evaluation of errors and incidents recorded over a10 year period. Radiotherapy and Oncology, 2005,Mar;74(3):283–291.
31. Lawrence G et al. The Impact of changingtechnology and working practices on errors at theNCCT. 1998–2006. Clinical oncology (Royal Collegeof Radiologists), 2007;19(3):S37.
32. Brundage MD et al. A real-time audit of radiationtherapy in a regional cancer center. InternationalJournal of Radiation Oncology Biology Physics,1999;43(1):115–124.
33. Duffey RB, Saull JW. Know the risk: Learning fromerrors and accidents: Safety and risk in today’stechnology. US: Butterworth-HeinemannPublications, 2003
34. ROSIS database: a voluntary safety reporting systemfor Radiation Oncology. (www.rosis.info, accessed 10September 2007)
35. Sydney South West Cancer Services, Radiationoncology treatment related incident reportdatabase 2005. (Unpublished)
36. World Bank List of Economies.(http://siteresources.worldbank.org/DATASTATISTICS/Resources/CLASS.XLS, accessed 23 August 2007)
37. UK Department of Health. Radiotherapy: Hiddendangers (Chapter 5). In: On the state of publichealth: Annual report of the Chief Medical Officer2006, London: Department of Health, 2007:61–68.
38. Ash D, Bates T. Report on the clinical effects ofinadvertent radiation underdosage in 1045 patients.Journal of Clinical Oncology, 1994, 6:214–225.
39. Leveson NG, Turner CS. An investigation of theTherac-25 accidents. IEEE computer. 1993;26(7):18–41.
40. International Atomic Energy Agency. Informationfor Health Professionals: Radiotherapy Accidentprevention.(http://rpop.iaea.org/RPoP/RPoP/Content/InformationFor/HealthProfessionals/2_Radiotherapy/AccidentPrevention.htm#_9._HDR_unit, accessed 20 September2007)
41. International Atomic Energy Agency. Theoverexposure of radiotherapy patients in San José,Costa Rica. Vienna, Austria: IAEA, 1998.(STI/PUB/1180)
42. Ikeda H et al. How do we overcome recentradiotherapy accidents? – a report of the symposiumheld at the 17th JASTRO Annual Scientific Meeting,Chiba, 2004. Journal of JASTRO (Japanese Societyfor Therapeutic Radiology and Oncology) 2005,17(3):133–139. (in Japanese) (Abstract at:http://sciencelinks.jp/j-east/article/200523/000020052305A0872711.php,accessed 13 November 2007)
43. International Atomic Energy Agency. Investigationof an accidental exposure of radiotherapy patientsin Panama. Vienna, Austria: IAEA, 2001.(STI/PUB/1114)
44. International Atomic Energy Agency. The accidentaloverexposure of radiotherapy patients in Bialystok.Vienna, Austria: IAEA, 2002. (STI/PUB/1027)
45. Autorité De Surate Nucleaire (ASN). Annual report2006. ( http://annual-report.asn.fr/cancer-radiotherapy.html, accessed 11 October 2007)
46. Summary of ASN report no. 2006 ENSTR 019 – IGASno. RM 2007-015P on the Epinal radiotherapyaccident, submitted by Guillaume WACK (ASN, theFrench Nuclear Safety Authority) and Dr FrançoiseLALANDE, member of the Inspection Générale desAffaires Sociales (General inspectorate of SocialAffairs), in association with Marc David SELIGMAN.(http://www.asn.fr/sections/main/documents-available-in/documents-available-in-english/downloadFile/attachedFile_unvisible_3_f0/ASN_report_n_2006_ENSTR_019_-_IGAS.pdf?nocache=1174581960.71, accessed 23October 2007)
47. MacLeod I. Cancer patients get wrong dose at CivicCampus. .The Ottawa Citizen, 21 July 2008.
48. Gandhi U. 326 skin cancer patients underdosedbecause of hospital error. The Globe and Mail, 22July 2008. Page A6.
49. Unintended overexposure of patient Lisa Norrisduring radiotherapy treatment at the BeatsonOncology Centre, Glasgow in January 2006. Reportof the investigation by Inspector appointed by theScottish Ministers for the Ionising Radiation(Medical Exposures) Regulations 2000.(http://www.scotland.gov.uk/Publications/2006/10/27084909/0, accessed 11 October 2007)
50. Duggan L et al. An independent check of treatmentplan, prescription and dose calculation as a QAprocedure. Radiotherapy and Oncology, 1997,42(3):297–301.
51. Bate MT et al. Quality control and error detection inthe radiotherapy treatment process. Journal ofRadiotherapy in Practice, 1999, 1:125–134.
Radiotherapy Risk Profile 47
52. The Royal College of Radiologists. Towards SaferRadiotherapy. The Royal College of Radiologists,BCFO(08)1,London.2008http://www.rcr.ac.uk/publications.aspx?PageID=149&PublicationID=281
53. The Clinical Excellence Commission of New SouthWales. Patient safety clinical incident managementin NSW. Analysis of 1st year of IIMS (IncidentInformation Management System) data; Annualreport 2005–2006. Sydney, 2006.
54. Izewska J et al. The IAEA/WHO TLD postal dosequality audits for radiotherapy: a perspective ofdosimetry practices at hospitals in developingcountries. Radiotherapy and Oncology, 2003,69(1):91–97.
55. Izewska J, Vatnitsky S, Shortt KR for IAEA. Postaldose audits for radiotherapy centres in LatinAmerica and the Caribbean: trends in 1969–2003.Rev Panm Salud Publica, 2006, 20(2–3):161–172.
56. Shakespeare TP et al. External audit of clinicalpractice and medical decision making in a newAsian oncology center: results and implications forboth developing and developed nations.International Journal of Radiation Oncology BiologyPhysics, 2006, Mar 1;64(3):941–947.
57. Leunens G et al. Human errors in data transferduring the preparation and delivery of radiationtreatment affecting the final result: “garbage in,garbage out”. Radiotherapy and Oncology, 1992,23:217–222.
58. International Atomic Energy Agency (IAEA). Designand implementation of a radiotherapy programme:Clinical, medical physics, radiation protection andsafety aspects. Vienna, Austria: IAEA, 1998. (IAEA-TECDOC-1040).
59. International Atomic Energy Agency (IAEA).Applying Radiation Safety Standards inRadiotherapy. Vienna, Austria: IAEA, 2006. (SafetyReports Series No. 38)
60. International Atomic Energy Agency (IAEA).Radiation Oncology Physics: A Handbook forTeachers and Students. Vienna, Austria: IAEA, 2005.ISBN 92-0-107304-6
61. Nath R et al. AAPM code of practice forradiotherapy accelerators. Medical Physics, 1994,21(7):1093–1121.
62. American Association of Physicists in Medicine(AAPM). Quality assurance for clinical radiotherapytreatment planning. College Park (MD): AAPM,1998. (AAPM Report 62)
63. Canadian Association of Provincial Cancer Agencies.Standards for Quality Control at Canadian RadiationTreatment Centres: Kilovoltage X-ray RadiotherapyMachines.(http://www.medphys.ca/Committees/CAPCA/Kilovoltage_X-ray_Radiotherapy_Machines.PDF, accessed29 October 2007)
64. Clinical Oncology Information Network, RoyalCollege of Radiologists. Guidelines for externalbeam radiotherapy, Clinical Oncology, 1999,11:S135–S172.
65. Shakespeare TP et al. Design of an internationallyaccredited radiation oncology training programincorporating novel educational models.International Journal of Radiation Oncology BiologyPhysics, 2004, 59:1157–1162.
66. Esik O et al. External audit on the clinical practiceand medical decision-making at the departments ofradiotherapy in Budapest and Vienna. Radiotherapyand Oncology, 1999, 51:87–94.
67. Ekaette EU et al. Risk analysis in radiationtreatment: application of a new taxonomicstructure. Radiotherapy and Oncology, 2006,80(3):282–287.
68. McNee SG. Clinical governance: risks and qualitycontrol in radiotherapy. Report on a meetingorganized by the BIR Oncology Committee, held atthe British Institute of Radiology, London, on 9February 2000 [Commentary]. The British Journal ofRadiology, 2001, 74:209–212.
69. Van Der Giessen PH, Alert J, et al. Multinationalassessment of some operational costs of teletherapy.Radiotherapy and Oncology, 2004, 71(3):347–355.
70. Munro AJ. Hidden danger, obvious opportunity:error and risk in the management of cancer. BritishJournal of Radiology, 2007, 80:955-966.
71. Toft B, Mascie-Taylor H. Involuntary automaticity: awork-system induced risk to safe health care. HealthServices Management Research, 18: 211–216.
72. RANZCR Maintenance of Certification / RevalidationAudit Instrument. (www.ranzcr.edu.au/documents,accessed 4 August 2008)
73. Ibbott G et al. Anniversary paper: fifty years ofAAPM involvement in radiation dosimetry. MedicalPhysics, 2008, 35(4):1418-1427.
74. Katharine Tylko and Mitzi Blennerhassett: How theNHS could better protect the safety of radiotherapypatients. Health Care Risk Report p18–19 September2006.
75. World Health Organization World Alliance forPatient Safety(http://www.who.int/patientsafety/challenge/safe.surgery/launch/en/index.html, accessed 29 May 2008)
76. Australian Commission on Safety and Quality inHealthcare. Expanding the Ensuring correct patient,correct site, correct procedure protocol: Draftpatient matching protocols for radiology, nuclearmedicine, radiation therapy and oral health.Consultation Paper. 14 January 2008.
48
49Radiotherapy Risk Profile
Developed by the Radiotherapy Safety Team within the World Alliance for Patient Safety underthe editorial leadership of Michael Barton and Jesmin Shafiq of the South Western Clinical School,University of New South Wales, Australia and the Collaboration for Cancer Outcomes Researchand Evaluation, Liverpool Health Service, Sydney, Australia, with support and contributions from:
Raymond P Abratt Dept of Radiation Oncology, Groote Schuur Hospital, South AfricaCharlotte Beardmore The Society and College of Radiographers, London, United KingdomZhanat Carr Radiation and Environmental Health Programme, World Health Organization,
Geneva, SwitzerlandMary Coffey University of Dublin Trinity College, Dublin, IrelandBernard Cummings Princess Margaret Hospital, Toronto, CanadaRenate Czarwinski International Atomic Energy Agency, Vienna, AustriaJake Van Dyk London Regional Cancer Program, London Health Sciences Centre,
London, Ontario, CanadaMahmoud M El-Gantiry National Cancer Institute, Cairo University, Cairo, Egypt Akifumi Fukumura National Institute of Radiological Sciences, Chiba-Shi, JapanFuad bin Ismail Department of Radiotherapy and Oncology, Hospital University Kebangsaan
Malaysia, Kuala Lumpur, MalaysiaJoanna Izewska International Atomic Energy Agency, Vienna, AustriaAhmed Meghzifene International Atomic Energy Agency, Vienna, AustriaMaria Perez Radiation and Environmental Health Programme, World Health Organization,
Geneva, SwitzerlandMadan Rehani International Atomic Energy Agency, Vienna, AustriaJohn Scarpello National Patient Safety Agency, London, United KingdomKen Shortt International Atomic Energy Agency, Vienna, AustriaMichael Williams Oncology Centre, Addenbrooke’s NHS Trust, Cambridge, United KingdomEduardo Zubizarreta International Atomic Energy Agency, Vienna, Austria
World Alliance for Patient Safety Secretariat
(All teams and members listed in alphabetical order following the team responsible for the publication)
Radiotherapy:
Michael Barton, Felix Greaves, Ruth Jennings, Claire Lemer, Douglas Noble, Gillian Perkins, JesminShafiq, Helen Woodward
Blood Stream Infections:
Katthyana Aparicio, Gabriela García Castillejos, Sebastiana Gianci, Chris Goeschel, Maria Teresa Diaz Navarlaz, Edward Kelley, Itziar Larizgoitia, Peter Pronovost, Angela Lashoher
Central Support & Administration:
Sooyeon Hwang, Sean Moir, John Shumbusho, Fiona Stewart-Mills
Clean Care is Safer Care:
Benedetta Allegranzi, Sepideh Bagheri Nejad, Pascal Bonnabry, Marie-Noelle Chraiti, NadiaColaizzi, Nizam Damani, Sasi Dharan, Cyrus Engineer, Michal Frances, Claude Ginet, WilcoGraafmans, Lidvina Grand, William Griffiths, Pascale Herrault, Claire Kilpatrick, Agnès Leotsakos,Yves Longtin, Elizabeth Mathai, Hazel Morse, Didier Pittet, Hervé Richet, Hugo Sax, KristineStave, Julie Storr, Rosemary Sudan, Shams Syed, Albert Wu, Walter Zingg
ACKNOWLEDGEMENTS
50
Communications & country engagement:
Vivienne Allan, Agnès Leotsakos, Laura Pearson, Gillian Perkins, Kristine Stave
Education:
Bruce Barraclough, Gerald Dziekan, Benjamin Ellis, Felix Greaves, Helen Hughes, Ruth Jennings,Itziar Larizgoitia, Claire Lemer, Douglas Noble, Rona Patey, Gillian Perkins, Samantha VanStaalduinen, Merrilyn Walton, Helen Woodward
International Classification for Patient Safety:
Martin Fletcher, Edward Kelley, Itziar Larizgoitia, Fiona Stewart-Mills
Patient safety prize & indicators:
Benjamin Ellis, Itziar Larizgoitia, Claire Lemer
Patients for Patient Safety:
Joanna Groves , Martin Hatlie, Rachel Heath, Helen Hughes, Anna Lee, Peter Mansell, MargaretMurphy, Susan Sheridan, Garance Upham
Reporting & Learning:
Gabriela Garcia Castillejos, Martin Fletcher, Sebastiana Gianci, Christine Goeschel, Helen Hughes,Edward Kelley, Kristine Stave
Research and Knowledge Management:
Maria Ahmed, Katthyana Aparicio, David Bates, Helen Hughes, Itziar Larizgoitia, Pat Martin,Carolina Nakandi, Nittita Prasopa-Plaizier, Kristine Stave, Albert Wu
Safe Surgery Saves Lives:
William Berry, Mobasher Butt, Priya Desai, Gerald Dziekan, Lizabeth Edmondson, Luke Funk, AtulGawande, Alex Haynes, Sooyeon Hwang, Agnès Leotsakos, Elizabeth Morse, Douglas Noble,Sukhmeet Panesar, Paul Rutter, Laura Schoenherr, Kristine Stave, Thomas Weiser, Iain Yardley
Solutions & High 5s:
Laura Caisley, Gabriela Garcia-Castillejos, Felix Greaves, Edward Kelley, Claire Lemer, AgnèsLeotsakos, Douglas Noble, Dennis O'Leary, Karen Timmons, Helen Woodward
Tackling Antimicrobial Resistance:
Gerald Dziekan, Felix Greaves, David Heymann, Sooyeon Hwang, Sarah Jonas, Iain Kennedy,Vivian Tang
Technology:
Rajesh Aggarwal, Lord Ara Darzi, Rachel Davies, Gabriela Garcia Castillejos, Felix Greaves, EdwardKelley, Oliver Mytton, Charles Vincent, Guang-Zhong Yang,
Vincristine Safety:
Felix Greaves, Helen Hughes, Claire Lemer, Douglas Noble, Kristine Stave, Helen Woodward
50
51Radiotherapy Risk Profile Radiotherapy Risk Profile 51





























