Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Esophagus (2005) 2:21–23 © Japan Esophageal Society and Springer-Verlag 2005DOI 10.1007/s10388-004-0031-3
Atsunori Yorozu
Radiotherapy for nodal recurrence after chemoradiotherapy foresophageal carcinoma
Received: July 26, 2004 / Accepted: October 23, 2004
AbstractBackground. To evaluate the treatment outcome of radio-therapy for nodal recurrence after definitive chemoradio-therapy for esophageal carcinoma.Methods. Between 1996 and 2001, ten patients with isolatednodal recurrence after definitive chemoradiotherapy re-ceived radiotherapy with or without chemotherapy. Thesite of recurrence was the mediastinum in five patients, theceliac node in four patients, and the supraclavicular fossa inone patient. All sites of nodal recurrence were outside theprevious irradiated area and without local recurrence ordistant metastases. Radiotherapy was given with three-dimensional conformal technique, and an average totaldose was 60Gy. Eight patients received chemotherapy con-currently with radiotherapy. Chemotherapy consisted oftwo cycles of cisplatin and 5-FU.Results. The control rate of the irradiated region was eightof ten patients. The size of all controlled lesions was 3cm orless in diameter. In five patients, distant metastases devel-oped to other organs and caused death. Two patients sur-vived without disease for 5 years and three patients survived2 years or more. In four patients with an interval of 2 yearsor longer between the previous treatment and nodal recur-rence, three patients survived without disease. Improve-ment of clinical symptoms such as dysphagia or hoarsenesswas obtained in five of six patients.Conclusions. Radiotherapy for isolated nodal recurrence ofesophageal carcinoma after definitive chemoradiotherapy issuggested to be safe and effective. This treatment is pro-mising as well as palliative.
Key words Esophageal cancer · Radiotherapy · Recurrence· Chemoradiotherapy
A. Yorozu (*)Department of Radiology, Tokyo Medical Center, National HospitalOrganization, 2-5-1 Higashigaoka, Meguro-ku, Tokyo 152-8902,JapanTel. �81-3-3411-0111; Fax �81-3-3412-9811e-mail: [email protected]
Introduction
After chemoradiotherapy for esophageal carcinoma, nodalrecurrence without local failure or distant metastases occursin about 9% of total treatment failure [1]. When nodalrecurrence occurs outside the previous irradiated area,radiotherapy with or without chemotherapy might curethose isolated nodal recurrences. The outcome of treatmentfor isolated nodal recurrence has not been reported yet. Weretrospectively analyzed if radiotherapy was effective forthis type of recurrence.
Methods
Between 1993 and 2001, 112 patients with esophagealcarcinoma received radiotherapy, with or without chemo-therapy, with curative intent at Tokyo Medical Center,National Hospital Organization. All patients had squamouscell carcinoma. Ninety patients received chemoradio-therapy. The details of treatment have been reported pre-viously [2,3]. The site of first recurrence was the nodalregion in 10 patients, the esophagus in 28 patients, the dis-tant metastases in 11 patients, and combination of these in16 patients. We evaluated the 10 patients with regionalnodal recurrence alone; 5 patients had recurrence in themediastinum, 4 patients in the celiac node, and 1 patient inthe supraclavicular fossa. All sites of nodal recurrence weresolitary and outside the previous irradiated area.
Diagnosis of recurrence was based on regular checkupor follow-up computed tomography (CT) findings. Theinterval between follow-up CT was 6 months in the first2 years and 12 months after 2 years. The diagnosis ofmediastinal or abdominal recurrence was based on thenode growing larger than 2cm viewed via CT. Histopatho-logical examination was not done. In six patients, changes insymptoms were evaluated; hoarseness in three patients,dysphagia in two patients, and abdominal pain in onepatient.

22
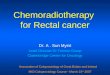
All ten patients with isolated regional recurrence re-ceived radiotherapy. A linear accelerator (10, 6, or 4MV)was used as the X-ray source. The radiation field was a localfield with a margin of 1–2cm from the tumor. In all patientswith mediastinal or celiac nodes, three-dimensional confor-mal radiotherapy was used to avoid overlapping with theprevious radiation field (Fig. 1). Conventional fractionation(2Gy/fraction, 1 fraction/day, five times per week) wasused. The median radiation total dose was 60Gy (range, 50–72Gy). Eight patients received chemotherapy concurrentlywith radiotherapy. Chemotherapy consisted of two cycles ofcisplatin (60mg/m2) and 5-fluorouracil (5-FU) (600mg/m2
per 24h, continuous infusion for 5 days). Response wasevaluated by CT scan or palpation. Complete response wascomplete resolution of all clinically detectable disease for aperiod of at least 1 month by definition. Partial responsewas a reduction in tumor dimensions of at least 50% main-tained for at least 1 month. No change was a response thatis less than a partial response or progression less than a 25%increase during the period of observation.
The last follow-up was performed in July 2004. Survivalperiods were calculated from the start of irradiation tonodal recurrence.
Results
Patient and treatment characteristics are shown in Table 1.The median survival period was 2 years. Five patients sur-vived more than 2 years, and two patients were alive with-out disease after 5 years. The disease-free survival periodwas 11 months.
Complete response and partial response were observedin seven and two of the patients, respectively. Regionalcontrol in the treated area was obtained finally in eightpatients of ten. All the controlled lesions were 3cm or lessin diameter. Regrowth of the tumor in the treated areaoccurred in the two other patients and finally caused death.Distant metastases to other organs developed in five pa-tients and caused death. Three patients were free from dis-ease at the last follow-up.
In five patients with 2 years or longer between previoustreatment and nodal recurrence, four patients survivedmore than 2 years after recurrence. In the other five pa-tients, only one patient survived 2 years.
Improvement in symptoms was observed in five of the sixpatients. No late complications were observed.
Fig. 1. Case example of isodose distributions. Three-dimensional conformal radiotherapy for metastatic celiac lymph node is presented. The 95%of 60-Gy isodose line includes a 3-mm margin around the tumor

23
Discussion
In the treatment of esophageal cancer with chemoradio-therapy, there is no consensus as to prophylactic irradiationto three fields: the neck, the mediastinum, and the abdomi-nal nodal region. Actually, the incidence of local failureafter chemoradiotherapy is still high [1,2] . Long-term se-vere complications of pulmonary or cardiac function havebeen reported [4]. In practice, the superior and inferiorborders of the radiation field are often 3cm or 5cm beyondthe primary tumor, or sometimes include regional nodes[1–3]. The number of patients with nodal recurrence with-out local disease or distant metasetases will increase in thenear future. Radiotherapy or surgery is anticipated to sal-vage the isolated nodal recurrence. We reported curabilitywith radical radiotherapy for this type of recurrence.
We treated metastatic lymph nodes sized between 2 and4cm. The size of tumor is important for radiotherapy, andlong-term follow-up must be important for those patients.The size of all controlled lesion was 3cm or less in diameter.We were unable to evaluate whether chemotherapy waseffective because of the small number of patients. Fivepatients developed distant metastases to other organs.Chemotherapy will be reexamined in the future. The timeinterval between surgery and the onset of recurrence wasreported to be the prognostic factor [5]. The time intervalbetween the initial treatment and onset of recurrence seemsthe prognostic factor for chemoradiotherapy as well. Wefound no complications of treatment.
In conclusion, radiotherapy with or without chemo-therapy for isolated nodal recurrence after definitive radio-therapy is effective. The prognosis of the patients who hadrecurrence after 2 years was good. Further investigation isrequired to confirm this result.
References
1. Minsky BD, Pajak TF, Ginsberg RJ, Pisansky TH, Martenson J,Komaki R, et al. INT 0123 (Radiation Therapy Oncology Group94-05) Phase III trial of combined-modality therapy for esophagealcancer: high-dose versus standard-dose radiation therapy. J ClinOncol 2002;20:1167–74.
2. Yorozu A, Dokiya T, Oki Y, Suzuki T. Curative radiotherapy withhigh-dose-rate brachytherapy boost for localized esophageal carci-noma: dose-effect relationship of brachytherapy with the balloontype applicator system. Radiother Oncol 1999;51:123–9.
3. Yorozu A, Dokiya T, Oki Y. High-dose-rate brachytherapy boostfollowing concurrent chemoradiotherapy for esophageal carcinoma.Int Radiat Oncol Biol Phys 1999;45:271–5.
4. Nemoto K, Ariga H, Kakuto Y, Matsushita K, Takeda C, TakahashiY, et al. Radiation therapy for loco-regionally recurrent esophagealcancer after surgery. Radiother Oncol 2001;61:165–8.
5. Ishikura S, Nihei K, Ohtsu A, Boku H, Hironaka S, Mera K, et al.Long-term toxicity after definitive chemoradiotherapy for squa-mous cell carcinoma of the thoracic esophagus. J Clin Oncol 2003;15:2697–702.
Tab
le 1
.C
hara
cter
isti
cs o
f pa
tien
ts a
nd t
umor
s
Pat
ient
Age
Sex
cTN
MT
umor
Site
of
noda
lT
ime
toSy
mpt
omSi
ze o
fR
adia
tion
Che
mot
hera
pyE
ffec
tR
elap
seP
rogn
osis
num
ber
loca
tion
recu
rren
cere
curr
ence
lesi
on (
cm)
dose
(G
y)
168
MT
3N1
Ut
Cer
vica
l4
year
sD
ysph
agia
3.5
60Y
esP
RR
egro
wth
Dea
d of
dis
ease
aft
erpa
raes
opha
geal
1 ye
ar2
70F
T1N
0M
tP
retr
ache
al3
year
sH
oars
enes
s2
72N
oC
RN
o re
curr
ence
Aliv
e w
itho
ut d
isea
seaf
ter
7 ye
ars
366
MT
2N0
Mt
Supr
acla
vicu
lar
1 ye
arN
one
250
Yes
CR
No
recu
rren
ceA
live
wit
hout
dis
ease
afte
r 5
year
s4
61F
T3N
0L
tU
pper
tho
raci
c3
year
sD
ysph
agia
366
Yes
CR
Met
asta
ses
to p
leur
a,D
ead
of d
isea
se a
fter
para
esop
hage
albo
ne, l
iver
aft
er 2
yea
rs3
year
s an
d 10
mon
ths
545
MT
1N0
Mt
Cel
iac
5 ye
ars
Non
e3
60N
oP
RM
etas
tase
s to
live
r,D
ead
of d
isea
se a
fter
para
aort
ic n
odes
aft
er1
year
and
6 m
onth
s1
year
656
MT
3N1
Mt
Cel
iac
11 m
onth
sN
one
250
Yes
CR
Met
asta
ses
to li
ver
Dea
d of
dis
ease
aft
eraf
ter
5 m
onth
s1
year
770
FT
3N1
Mt
Cel
iac
11 m
onth
sA
bdom
inal
pai
n3.
560
Yes
NC
Reg
row
thD
ead
of d
isea
se a
fter
1 ye
ar8
45F
T3N
1M
tC
elia
c2
year
sN
one
360
Yes
CR
No
recu
rren
ceA
live
wit
hout
dis
ease
afte
r 2
year
s9
70M
T3N
1M
tU
pper
10 m
onth
sH
oars
enes
s2.
560
Yes
PR
Met
asta
ses
to li
ver,
lung
Dea
d of
dis
ease
aft
erm
edia
stin
alaf
ter
4 m
onth
s8
mon
ths
1071
MT
3N1
Mt
Upp
er11
mon
ths
Hoa
rsen
ess
266
Yes
CR
Met
asta
ses
to lu
ng a
fter
Aliv
e w
ith
dise
ase
afte
rm
edia
stin
al6
mon
ths
2 ye
ars
Ut,
uppe
r th
orac
ic p
orti
on o
f in
trat
hora
cic
esop
hagu
s; M
t, m
iddl
e th
orac
ic p
orti
on; L
t, lo
wer
tho
raci
c po
rtio
n; P
R, p
arti
al r
espo
nse;
CR
, com
plet
e re
spon
se; N
C, n
o ch
ange





















![[C2] Preoperative radiotherapy and chemoradiotherapy for](https://img.dokumen.tips/doc/110x75/6159a52ce5e78c2242485b77/c2-preoperative-radiotherapy-and-chemoradiotherapy-for-.jpg)