Embed Size (px)
Citation preview
Radiothérapie Hypofractionnée et
Cancer de Prostate
JM Hannoun-Levi
Cercle des Oncologues Radiothérapeutes du Sud / Centre Antoine Lacassagne
2ème Congrès du CORS – Juan les Pins – 26/06/09
# fractions

# fractions
dose/fraction total dose

# fractions
Hypofractionated RT
dose/fraction total dose

# fractions
Hypofractionated RT
Accelerated
treatment time
dose/fraction total dose

# fractions
Hypofractionated RT
Accelerated Non Accelerated
treatment time treatment time =
dose/fraction total dose



# fractions
Hypofractionated RT
Accelerated Non Accelerated
dose/fraction total dose
treatment time treatment time =
Rationnal
Patient
Tumor
RT department
Quality of lifeTime for recovering professional life
Treatment coast
Biological considerationsDose escalation
Therapeutic index
linac time # treated pts
treatment delay
Rationnal
Patient
Tumor
RT department
Quality of lifeTime for recovering professional life
Treatment coast
Biological considerationsDose escalation
Therapeutic index
linac time # treated pts
treatment delay

Rationnal
Patient
Tumor
RT department
Quality of lifeTime for recovering professional life
Treatment coast
Biological considerationsDose escalation
Therapeutic index
linac time # treated pts
treatment delay

Rationnal
Patient
Tumor
RT department
Quality of lifeTime for recovering professional life
Treatment coast
Biological considerationsDose escalation
Therapeutic index
linac time # treated pts
treatment delay

Durée duTTT
Dose/fraction(Total dose)
Volume
3D Hypofractionnated RT

Overall Treatment Time
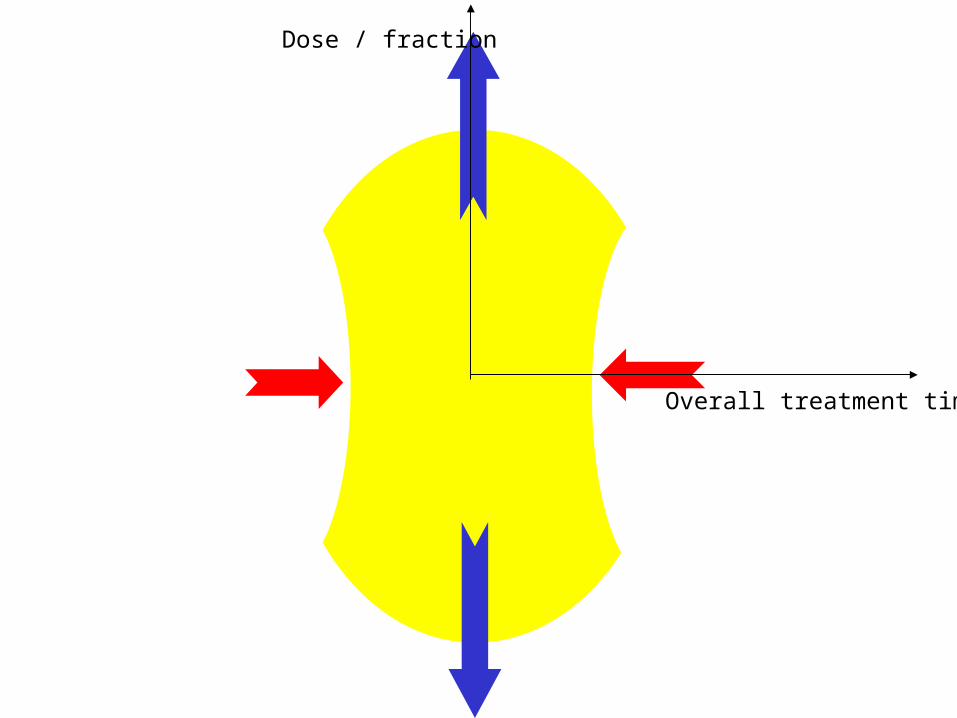
Overall treatment time
Dose / fraction

Volume

High doseSmall volume
Short time
Volume

Development
• Biological considerations
• Dose escalation in prostate cancer
• Small volume
• Clinical data
• Conclusion
Development
• Biological considerations
• Dose escalation in prostate cancer
• Small volume
• Clinical data
• Conclusion

Development
• Biological considerations
• Dose escalation in prostate cancer
• Small volume
• Clinical data
• Conclusion
Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusion
Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusion

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions
?=
Biological Equivalent Dose @ 2 Gy

?=
Biological Equivalent Dose @ 2 Gy
dose/fraction total dose

Sur
vivi
ng c
ell f
ract
ion
Dose (Gy)
Sur
vivi
ng c
ell f
ract
ion
Dose (Gy)
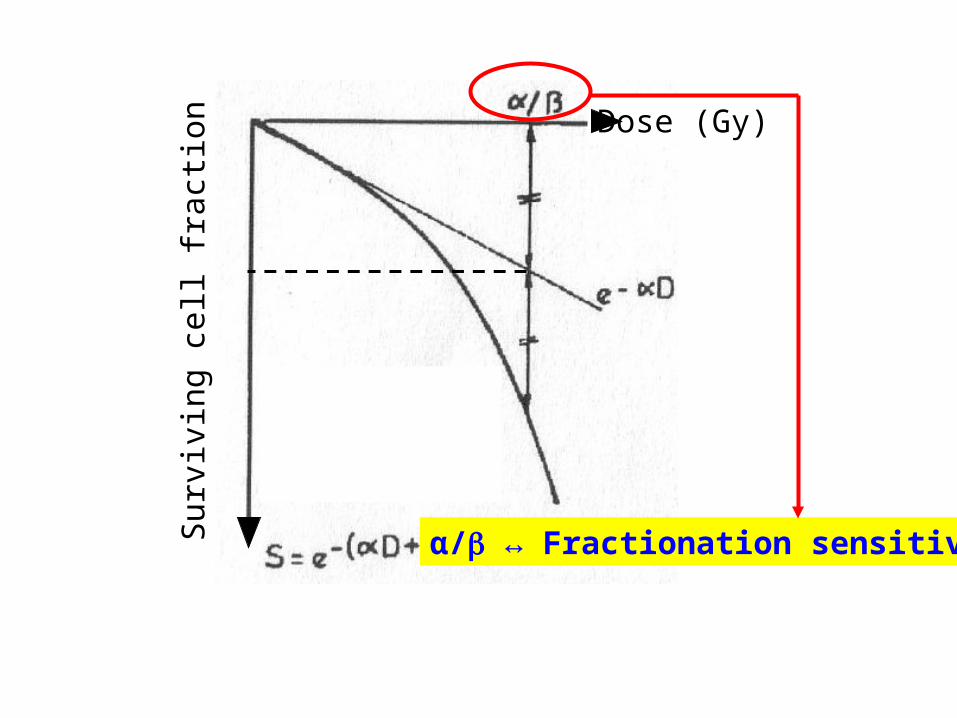
α/ ↔ Fractionation sensitivity

α/ Dose range
(Gy)
Normal Tissue
Response OTT* D/f**
Low
High
1 to 5
10 to 20
Late
Early
& Tumors
+
+++
+++
+
Sensitivity to
* OTT: Overall Treatment Time** D/f: Dose per fraction

α/ Dose range
(Gy)
Normal Tissue
Response OTT* D/f**
Low
High
1 to 5
10 to 20
Late
Early
& Tumors
+
+++
+++
+
Sensitivity to
* OTT: Overall Treatment Time** D/f: Dose per fraction

Efficacy
Toxicity

2///*' dDD
D’: biologic equivalent dose (Gy)D : physical delivered dose (Gy)d : dose per fraction for D (Gy)d’ : dose per fraction for D’ (Gy)
For dose/fraction < 8 GyFor dose/fraction < 8 Gy
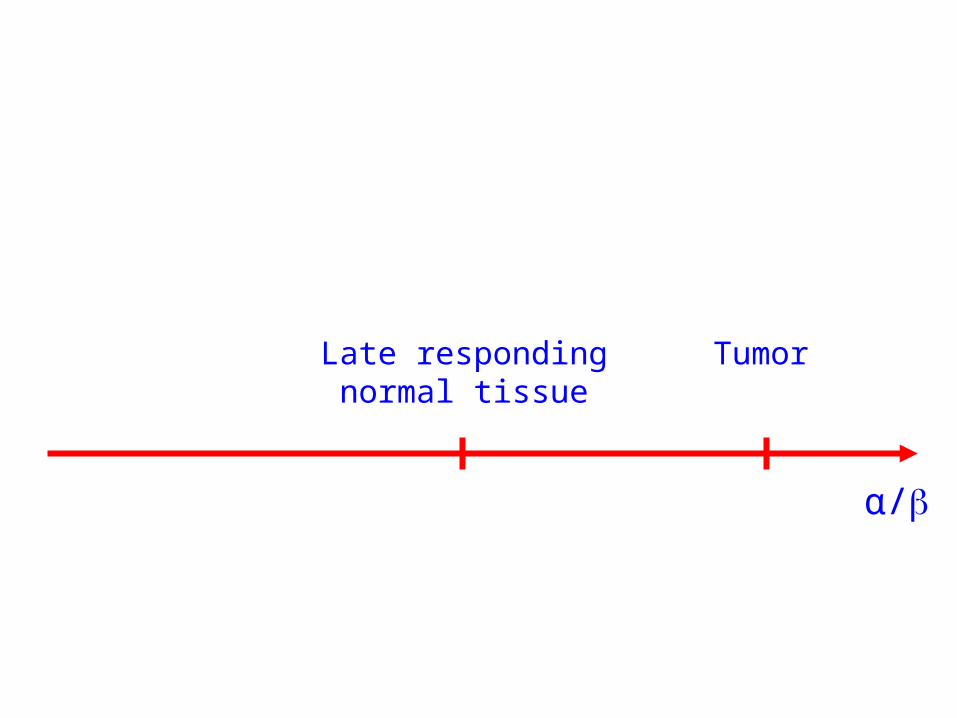
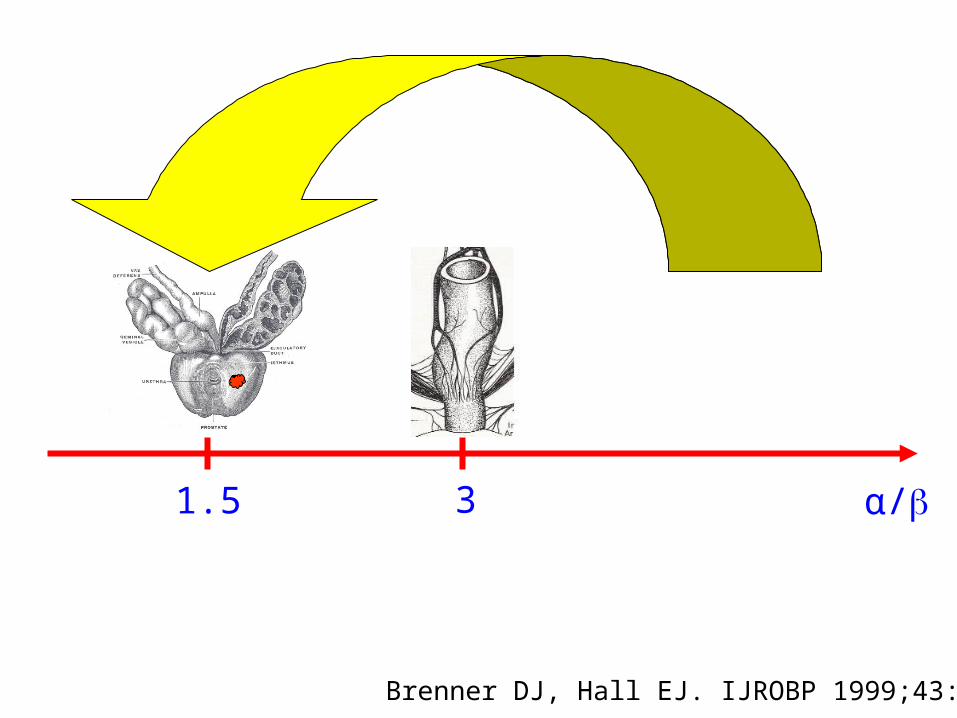
α/
Late respondingnormal tissue
Tumor

α/
Late respondingnormal tissue
Tumor
α/
Brenner DJ, Hall EJ. IJROBP 1999;43:1095
1.5 3
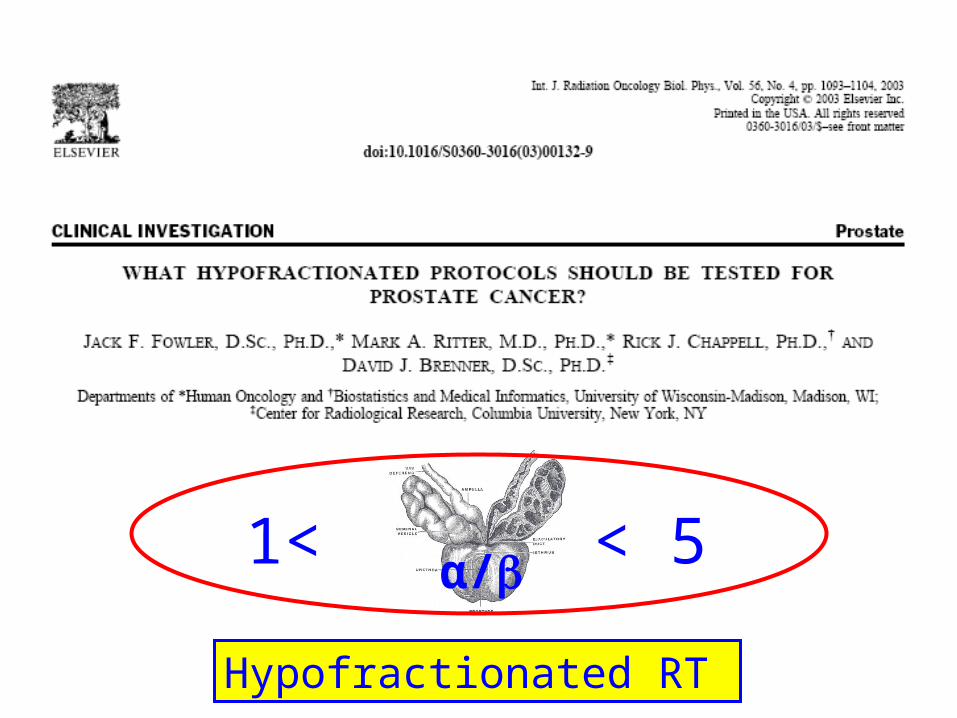
1< < 5α/
Hypofractionated RT

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions
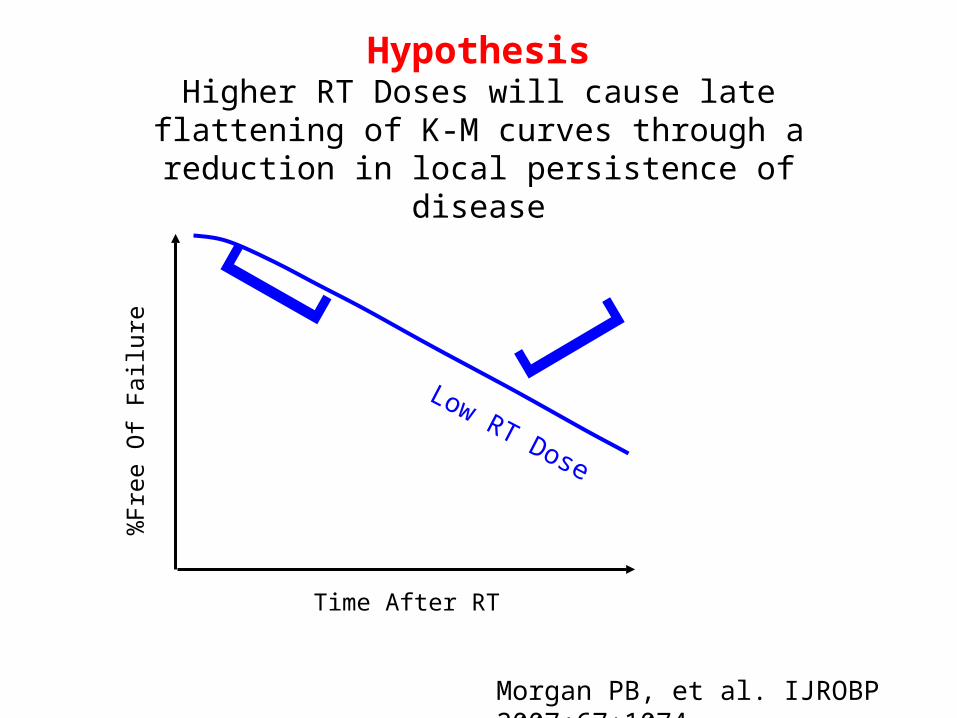
HypothesisHigher RT Doses will cause late flattening of K-M curves
through a reduction in local persistence of disease
Time After RT
%Fr
ee O
f Fa
ilure
Low RT Dose
[ [
Morgan PB, et al. IJROBP 2007;67:1074
Time After RT
%Fr
ee O
f Fa
ilure
Low RT Dose
[ [
Morgan PB, et al. IJROBP 2007;67:1074
Early drop due to
micrometastatic disease
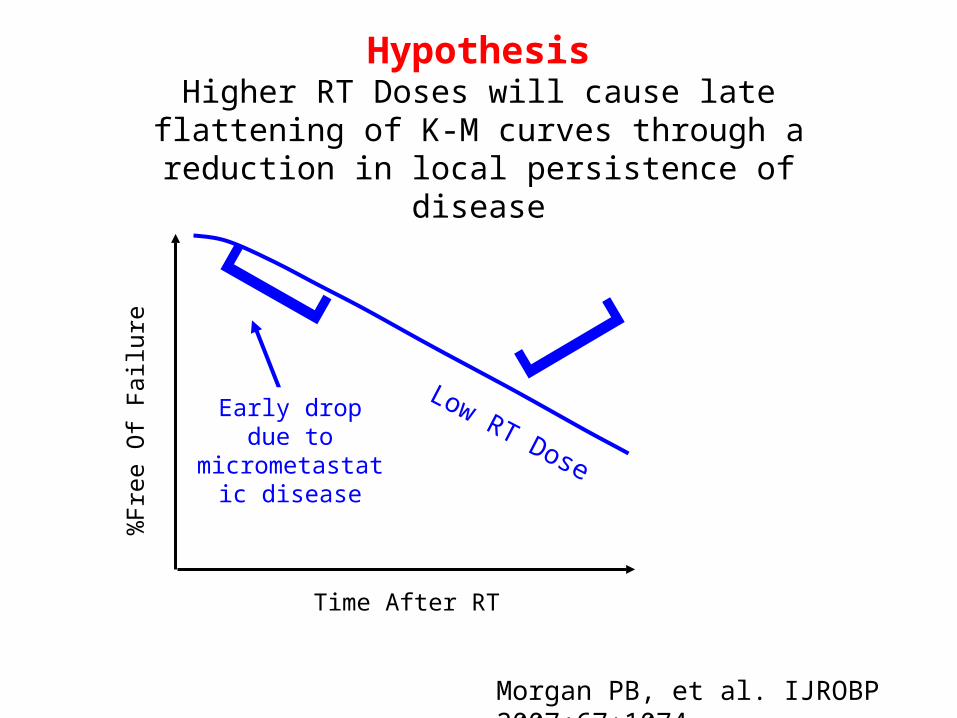
HypothesisHigher RT Doses will cause late flattening of K-M curves
through a reduction in local persistence of disease

Time After RT
%Fr
ee O
f Fa
ilure
Low RT Dose
[Late drop due
to local persistence of
disease
[
Morgan PB, et al. IJROBP 2007;67:1074
Early drop due to
micrometastatic disease
HypothesisHigher RT Doses will cause late flattening of K-M curves
through a reduction in local persistence of disease

HypothesisHigher RT Doses will cause late flattening of K-M curves
through a reduction in local persistence of disease
Time After RT
%Fr
ee O
f Fa
ilure
High RT Dose
Low RT Dose
[Late drop due
to local persistence of
disease
[
Morgan PB, et al. IJROBP 2007;67:1074
Early drop due to
micrometastatic disease
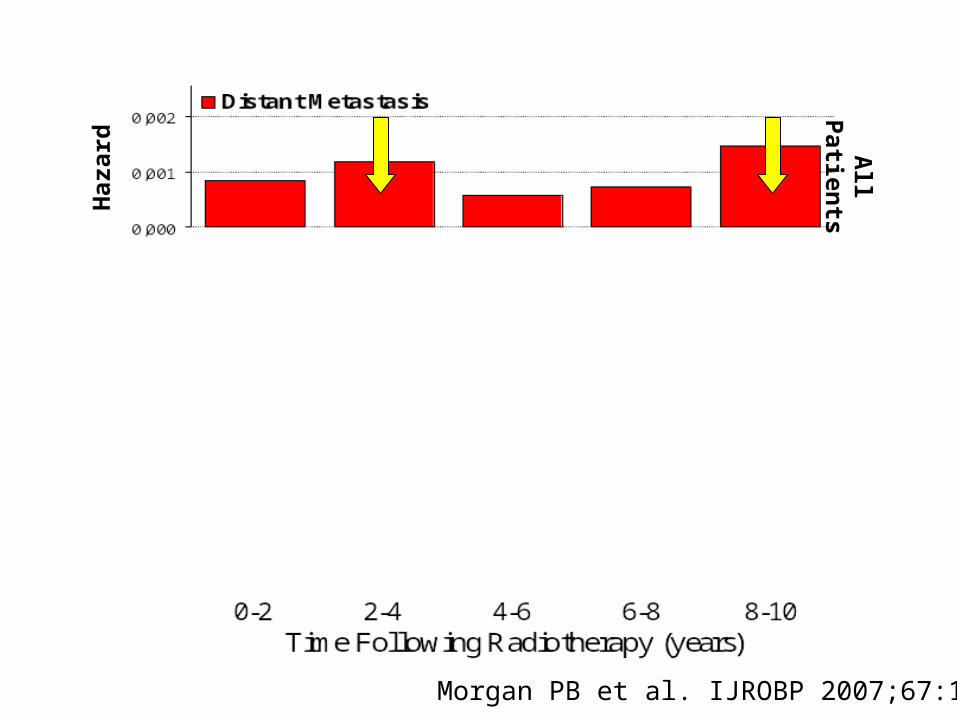
Haz
ard
Haz
ard
Haz
ard
All P
atients<
74 G
ray>
74 G
ray
Morgan PB et al. IJROBP 2007;67:1074

Haz
ard
Haz
ard
Haz
ard
All P
atients<
74 G
ray>
74 G
ray
Morgan PB et al. IJROBP 2007;67:1074

Haz
ard
Haz
ard
Haz
ard
All P
atients<
74 G
ray>
74 G
ray
Morgan PB et al. IJROBP 2007;67:1074

PSA Era Randomized Dose Escalation Trials
Authors (yr) # pts Dose (Gy) FFBF p-value
Kuban (2008)* 151 78 78%(10yr) 0.004150 70 59%(10yr)
Zietman (2005) 195 79.2 80%(5 yr) <0.001197 70.2 61%(5 yr)
Peeters (2006) 333 78 64%(5 yr) 0.02331 68 54%(5 yr)
Dearnaley (2007) 422 74 71%(5 yr) 0.0007421 64 60%(5 yr)
*Nadir+2 FFBF; Neoadjuvant AD 3-6 mo.

PSA Era Randomized Dose Escalation Trials
Authors (yr) # pts Dose (Gy) FFBF p-value
Kuban (2008)* 151 78 78%(10yr) 0.004150 70 59%(10yr)
Zietman (2005) 195 79.2 80%(5 yr) <0.001197 70.2 61%(5 yr)
Peeters (2006) 333 78 64%(5 yr) 0.02331 68 54%(5 yr)
Dearnaley (2007) 422 74 71%(5 yr) 0.0007421 64 60%(5 yr)
*Nadir+2 FFBF; Neoadjuvant AD 3-6 mo.
Hypofractionated RT

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions


Bladder & Rectal Volume Changes During RT
Antolak JA et al. IJROBP 1998;42:661
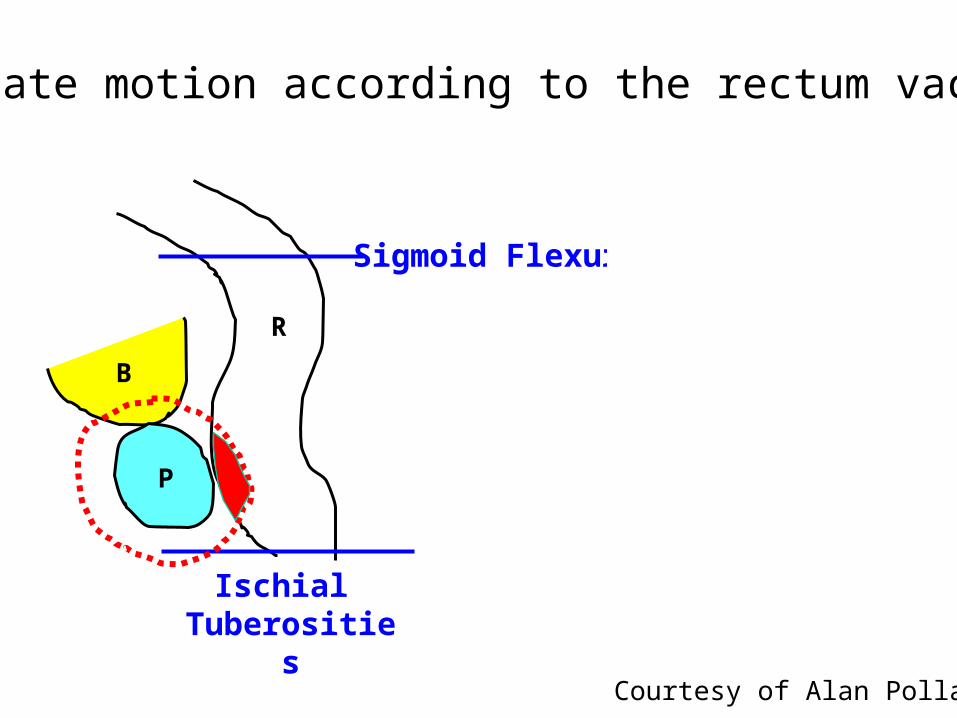
Sigmoid Flexure
Ischial Tuberosities
PP
R R
Not corrected for motion
B B
Prostate motion according to the rectum vacuity
Courtesy of Alan Pollack

Sigmoid Flexure
Ischial Tuberosities
PP
R R
Not corrected for motion
B B
Prostate motion according to the rectum vacuity
Courtesy of Alan Pollack

Consequences of prostate motion
de Crevoisier et al, IJROBP 2005;62:965
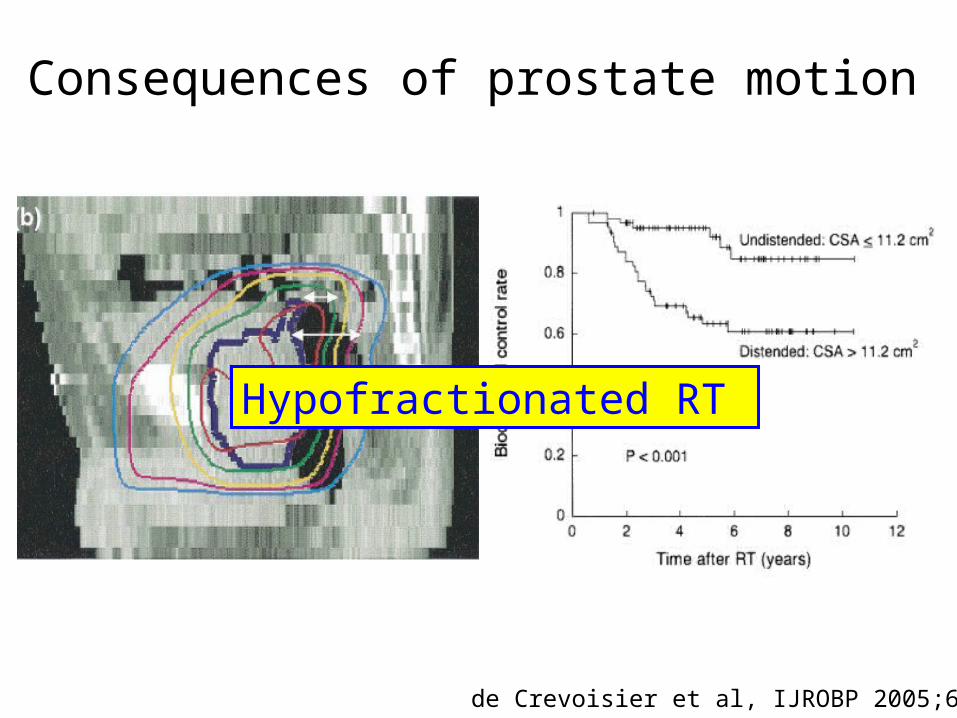
Consequences of prostate motion
de Crevoisier et al, IJROBP 2005;62:965
Hypofractionated RT

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions

Technical aspect

Technical aspect
RCMI +/- AT

Technical aspect
RCMI +/- AT CyberKnife
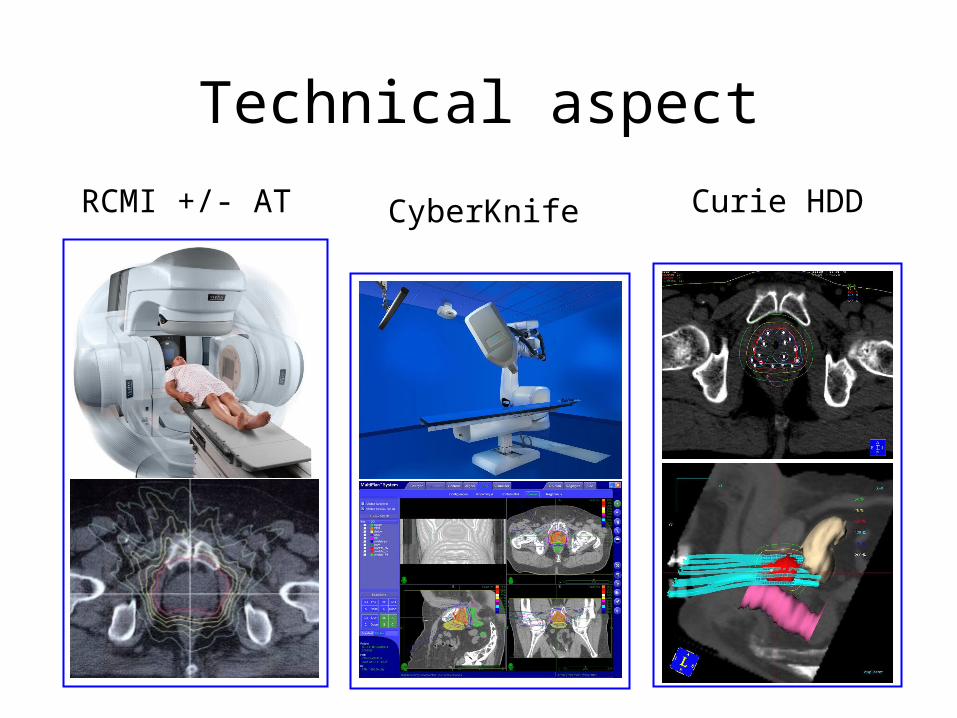
Technical aspect
RCMI +/- AT Curie HDDCyberKnife

Results of Prospective Phase II“Soft” Hypofractionation Studies (EBRT)
Miles EF et al. Semin Radiat Oncol 2008;18:41
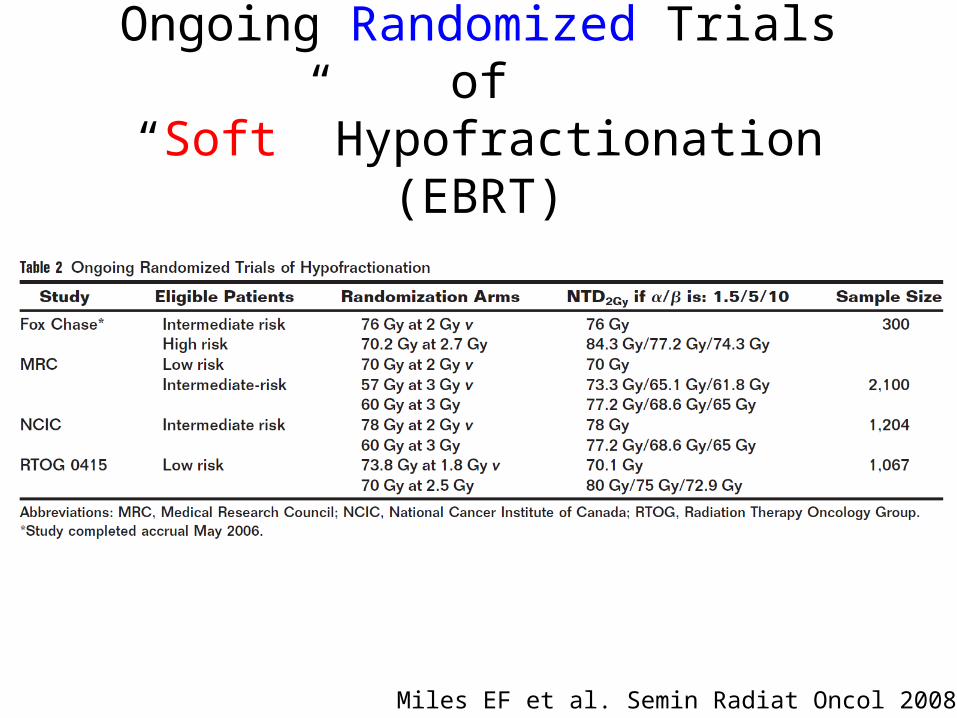
Ongoing Randomized Trials of“Soft” Hypofractionation (EBRT)
Miles EF et al. Semin Radiat Oncol 2008;18:41
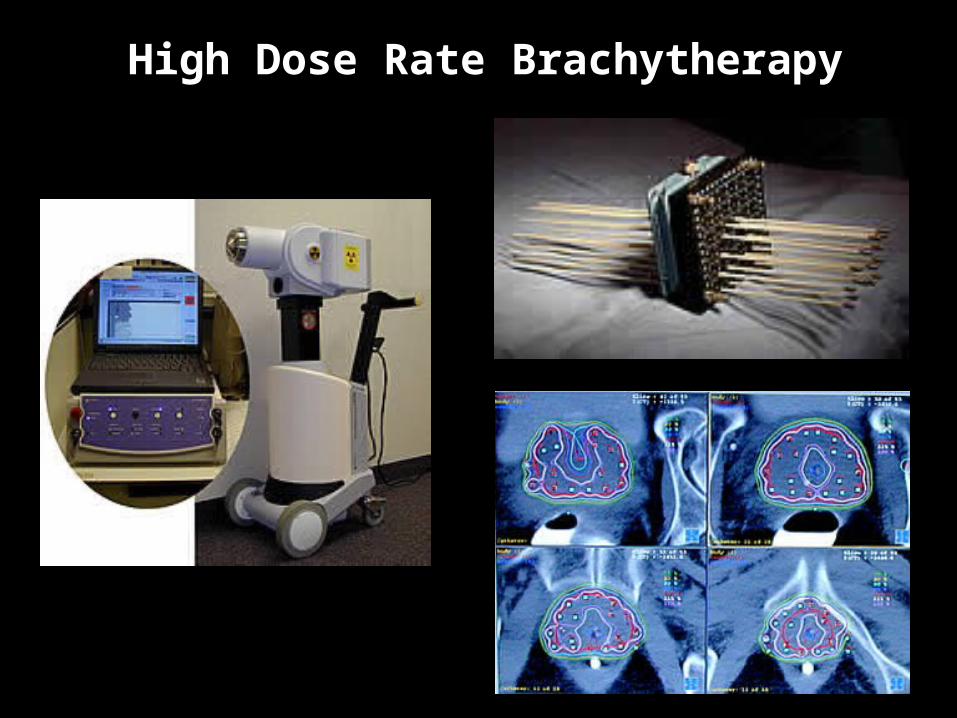
High Dose Rate Brachytherapy

Results of ProspectiveHypofractionation Boost Studies (HDR)
Risk Authors (yr) Groups Median Dose (Gy)
EBRT HDR
Median
follow-up (yr)
5-year
Biochemical
control rate (%)*
Low Elau (2000)
Galalae (2004)
Demanes (2005)
T1-2b, SG =6, PSA<10
T1-2b, SG =6, PSA<10
T1-2b, SG =6, PSA<10
50 12-16
46-50 16-30
36 22-24
6
5
7.25
96
96
90
Inter. & high Elau (2000)
Martinez (2002)
Galalae (2004)
Demanes (2005)
Martinez (2009)
T2c-3, SG 7-10, PSA >15
Intermediate : 1/2 factors
High : 3 factors
T2c-3, SG 7-10, PSA =10
T = 2b, SG =7, PSA =10
Intermediate : 1 factor
High : =2 factors
T2b-c, SG 7, 10<PSA =20
T3, SG 8-10, PSA > 20
T = 2b, SG =7, PSA =10
50 12-16
46 23
46-50 16-30
36 22-24
40 24
6
4
5
7.25
5.8
72
49
87
88
69
87
69
85 (82*)
*ASTRO definition** 10-year biochemical control rate

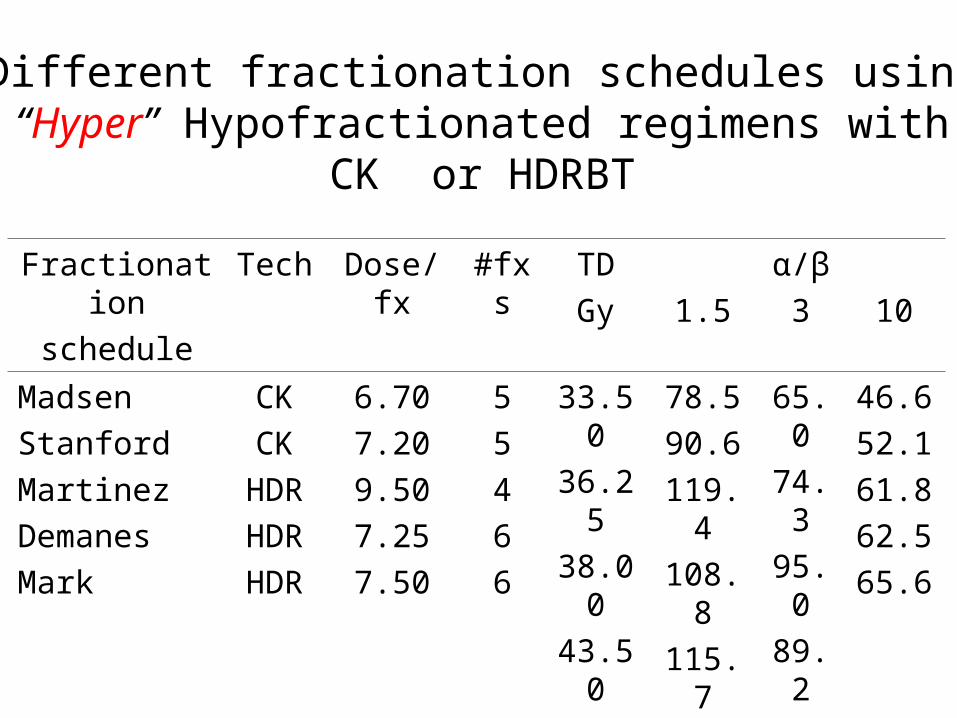
Fractionation
schedule
Tech Dose/fx #fxs TD
Gy 1.5
α/β
3 10
Madsen
Stanford
Martinez
Demanes
Mark
CK
CK
HDR
HDR
HDR
6.70
7.20
9.50
7.25
7.50
5
5
4
6
6
33.50
36.25
38.00
43.50
45.00
78.5
90.6
119.4
108.8
115.7
65.0
74.3
95.0
89.2
94.5
46.6
52.1
61.8
62.5
65.6
Different fractionation schedules using“Hyper” Hypofractionated regimens with
CK or HDRBT

Development
• Biological considerations
• Dose escalation in prostate cancer
• Prostate motion
• Clinical data
• Conclusions

Rationale for Accelerated and Hypofractionated Treatments for Prostate Cancer

Quality of lifeTime for recovering professional life
Treatment coast
Rationale for Accelerated and Hypofractionated Treatments for Prostate Cancer

Quality of lifeTime for recovering professional life
Treatment coast
Biological considerationsDose escalation
Therapeutic index
Rationale for Accelerated and Hypofractionated Treatments for Prostate Cancer

Biological considerations
1< < 5α/
= 3

Biological considerations
1< < 5α/
= 3
Dose escalation


Hypofractionated RT for Prostate Cancer
« Soft » « Hyper »?













![OFSEP MRI protocol: the need of good practice’s standardization …€¦ · Neurol. - FMC 7, 153–158 (2016).(French) [B] Cotton, F., Kremer, S., Hannoun, S., Vukusic, S. & Dousset,](https://img.dokumen.tips/doc/110x75/5fb4fa476709b63f1d0a255f/ofsep-mri-protocol-the-need-of-good-practiceas-standardization-neurol-fmc.jpg)







