Embed Size (px)
Citation preview
MEDICINE
Radiosurgery Techniques in the Treatment of Epilepsy Relatedto Hypothalamic Hamartomas (Systematic Review)
Sergiu Scobioala1 & Angela Brentrup2& Khaled Elsayad1
& Hans Theodor Eich1
Accepted: 8 February 2019# Springer Nature Switzerland AG 2019
AbstractVarious radiosurgery (RS) techniques are available for the therapy of epilepsy related to hypothalamic hamartomas (HH). Asshown in previous reports, each RS method can reduce the frequency of seizures, as well as behavioral and cognitive alterationsrelated to HH. This review summarizes the safety and efficacy of the most frequently used RS techniques for HH patients, with aparticular focus on the Gamma Knife RS, interstitial brachytherapy, and linear accelerator (LINAC) RS. Literature compilationwas achieved through use of a wide spectrum of information—namely, Cochrane Library, PubMed®, and the National Instituteof Health (NIH) clinical trials register. All identified reports were peer-reviewed and less than 20 years old. Relevant patientinformation, including RS method, follow-up, seizure outcome, and side effects, were selected from the above databases. Thirty-four reports with a total number of 123 patients, including 48 patients from singular randomized trial, were included in the review.The most common clinical presentations were gelastic seizures and cognitive dysfunctions. All RS techniques demonstrateapproximately the same seizure reduction outcomes achieving maximal values of 90%. The brachytherapy was reported to havea higher risk of brain edema or memory deterioration compared to the Gamma Knife or LINAC-based RS. Common limitationsfor the RS therapies included large sizes of hamartomas and their prolonged time latencies. RS is the least invasive curativetherapy with a lower rate of complications compared to surgery. RS can be considered the therapy of choice especially for smallor medium-sized HH.
Keywords Hamartoma . Epilepsy . Radiosurgery . GammaKnife . Brachytherapy
Introduction
Hypothalamic hamartomas (HH) are rare malformations thatare associated with seizures, hormonal, and behavioral dys-function. Most patients develop the condition in early child-hood, experiencing typical gelastic seizures which are usuallyresistant to anticonvulsive drugs. The evolution of this diseaseduring the following years may be characterized by a moregeneralized range of seizures, major cognitive disturbances,and psychiatric comorbidities [1–5].
A large spectrum of local treatment options that may po-tentially achieve complete ablation of HH has been proposed[6, 7]. The most widely practiced treatment includes differentsurgical techniques, as well as stereotactic radiosurgery (SRS).The advantage of SRS compared to microsurgery is in itsnoninvasive access. A series of SRS demonstrated low mor-bidity rates across various studies [8–13]. This review ana-lyzes both the efficacy and safety of different radiosurgerytechniques, such as the Gamma Knife, linear accelerator(LINAC)-based RS, and interstitial brachytherapy in the treat-ment of HH-related epilepsy.
Material and Methods
This systematic review was structured according to theBPRISMA^ reporting guidelines [14]. The Bseven-step model^was used to perform the literature search, as described in detail,by Onwuegbuzie and Friels and Williams [15, 16]. The flowchart of reports from the selection process is presented in
This article is part of the Topical Collection on Medicine
* Sergiu [email protected]
1 Department of Radiotherapy and Radiooncology, UniversityHospital of Muenster, Albert-Schweitzer-Campus 1, Gebäude A1,48149 Muenster, Germany
2 Department of Neurosurgery, University Hospital of Muenster,Muenster, Germany
SN Comprehensive Clinical Medicinehttps://doi.org/10.1007/s42399-019-00054-9
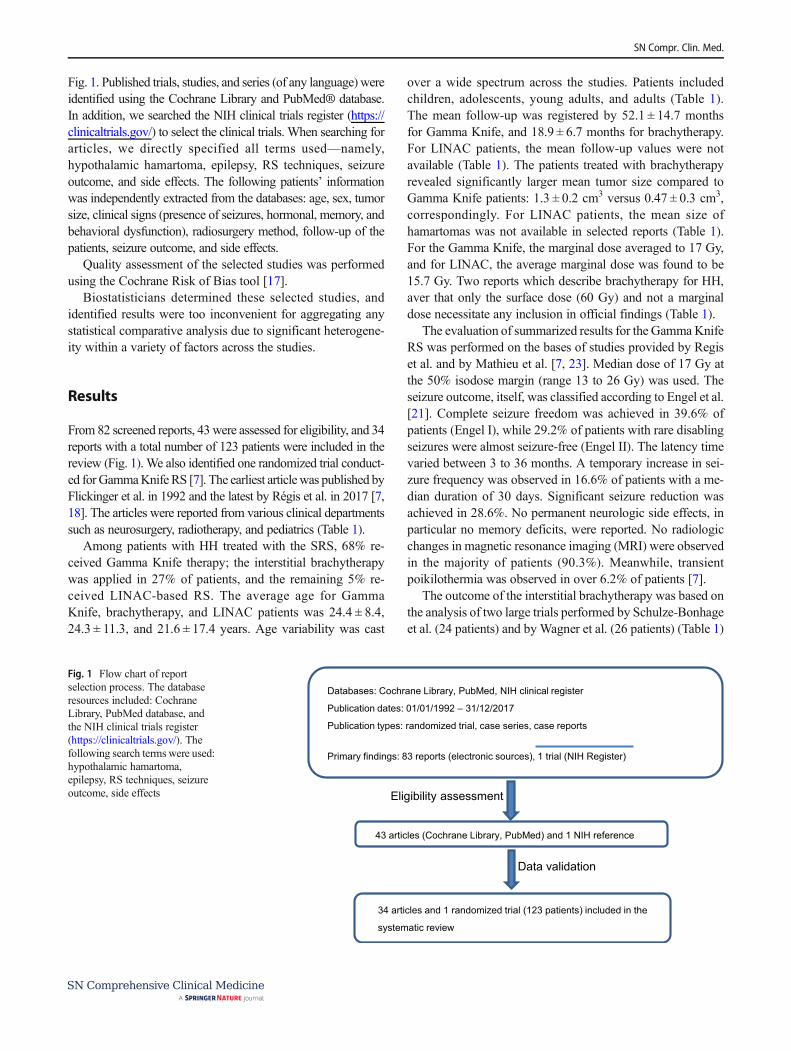
Fig. 1. Published trials, studies, and series (of any language) wereidentified using the Cochrane Library and PubMed® database.In addition, we searched the NIH clinical trials register (https://clinicaltrials.gov/) to select the clinical trials. When searching forarticles, we directly specified all terms used—namely,hypothalamic hamartoma, epilepsy, RS techniques, seizureoutcome, and side effects. The following patients’ informationwas independently extracted from the databases: age, sex, tumorsize, clinical signs (presence of seizures, hormonal, memory, andbehavioral dysfunction), radiosurgery method, follow-up of thepatients, seizure outcome, and side effects.
Quality assessment of the selected studies was performedusing the Cochrane Risk of Bias tool [17].
Biostatisticians determined these selected studies, andidentified results were too inconvenient for aggregating anystatistical comparative analysis due to significant heterogene-ity within a variety of factors across the studies.
Results
From 82 screened reports, 43 were assessed for eligibility, and 34reports with a total number of 123 patients were included in thereview (Fig. 1). We also identified one randomized trial conduct-ed for GammaKnife RS [7]. The earliest articlewas published byFlickinger et al. in 1992 and the latest by Régis et al. in 2017 [7,18]. The articles were reported from various clinical departmentssuch as neurosurgery, radiotherapy, and pediatrics (Table 1).
Among patients with HH treated with the SRS, 68% re-ceived Gamma Knife therapy; the interstitial brachytherapywas applied in 27% of patients, and the remaining 5% re-ceived LINAC-based RS. The average age for GammaKnife, brachytherapy, and LINAC patients was 24.4 ± 8.4,24.3 ± 11.3, and 21.6 ± 17.4 years. Age variability was cast
over a wide spectrum across the studies. Patients includedchildren, adolescents, young adults, and adults (Table 1).The mean follow-up was registered by 52.1 ± 14.7 monthsfor Gamma Knife, and 18.9 ± 6.7 months for brachytherapy.For LINAC patients, the mean follow-up values were notavailable (Table 1). The patients treated with brachytherapyrevealed significantly larger mean tumor size compared toGamma Knife patients: 1.3 ± 0.2 cm3 versus 0.47 ± 0.3 cm3,correspondingly. For LINAC patients, the mean size ofhamartomas was not available in selected reports (Table 1).For the Gamma Knife, the marginal dose averaged to 17 Gy,and for LINAC, the average marginal dose was found to be15.7 Gy. Two reports which describe brachytherapy for HH,aver that only the surface dose (60 Gy) and not a marginaldose necessitate any inclusion in official findings (Table 1).
The evaluation of summarized results for the GammaKnifeRS was performed on the bases of studies provided by Regiset al. and by Mathieu et al. [7, 23]. Median dose of 17 Gy atthe 50% isodose margin (range 13 to 26 Gy) was used. Theseizure outcome, itself, was classified according to Engel et al.[21]. Complete seizure freedom was achieved in 39.6% ofpatients (Engel I), while 29.2% of patients with rare disablingseizures were almost seizure-free (Engel II). The latency timevaried between 3 to 36 months. A temporary increase in sei-zure frequency was observed in 16.6% of patients with a me-dian duration of 30 days. Significant seizure reduction wasachieved in 28.6%. No permanent neurologic side effects, inparticular no memory deficits, were reported. No radiologicchanges in magnetic resonance imaging (MRI) were observedin the majority of patients (90.3%). Meanwhile, transientpoikilothermia was observed in over 6.2% of patients [7].
The outcome of the interstitial brachytherapy was based onthe analysis of two large trials performed by Schulze-Bonhageet al. (24 patients) and by Wagner et al. (26 patients) (Table 1)
Databases: Cochrane Library, PubMed, NIH clinical register
Publication dates: 01/01/1992 – 31/12/2017
Publication types: randomized trial, case series, case reports
Primary findings: 83 reports (electronic sources), 1 trial (NIH Register)
Eligibility assessment
43 articles (Cochrane Library, PubMed) and 1 NIH reference
Data validation
34 articles and 1 randomized trial (123 patients) included in the
systematic review
Fig. 1 Flow chart of reportselection process. The databaseresources included: CochraneLibrary, PubMed database, andthe NIH clinical trials register(https://clinicaltrials.gov/). Thefollowing search terms were used:hypothalamic hamartoma,epilepsy, RS techniques, seizureoutcome, side effects
SN Compr. Clin. Med.

[24, 25]. I125 seeds (sized 4.5 × 0.5 mm) were stereotacticallyimplanted into the target volume. Treatment plans were calcu-lated to a dose of 60Gy for the surface of hamartoma with amean energy dose rate of 10 cGy/h. Over 46% of patients wereseizure-free or achieved a seizure reduction of at least 90%(Engel classes I and II). Treatment effects appeared in themean time-period of 8 weeks after seeds implantation, andremained stable in the majority of patients. Due to unsatisfac-tory initial outcomes, treatment was repeated in 54% of pa-tients. In 29% of patients, tests revealed a radiological reduc-tion in HH volume. The interstitial brachytherapy was toler-ated well in most patients. Neither perioperative mortality norneurological deficits, as well as visual-filed impairments orendocrinologic dysfunction, were revealed. Weight gain ofmore than 5 kg was registered with four patients (17%).Transient radiation-related edema appeared in five patients(20.8%), and was not associated with further cognitive dys-function. Considering the rarity of the LINAC-based RS in thetherapy of epilepsy related to the HH, the information aboutefficacy and safety of this technique is very scare (Table 1).Patients received 11 Gy to 18 Gy (mean dose of 15.7Gy) in asingle fraction prescribed at the 90 to 95% isodose by using of6-MV linear accelerator (Novalis, BrainLAB, Germany). Inthe study of Golanov et al. (six patients), decreased frequencyof seizures was observed in 100% of cases, albeit withoutfurther clinical specification of seizure reduction [26]. Selchet al. (three patients) received two seizure-free patients (Engelclass IA). The third patient experienced a significant reductionin the seizure rate (Engel class II) without any improvement incognitive function [12]. The latency time varied between 7 to9 months. No changes in the tumor size or signal features wereobserved in the follow-up MRI. None of patients in both ev-idences developed neurologic or endocrinologic dysfunction.
Discussion
This systematic review is the first to assess the efficacy andsafety of different RS techniques in the therapy of HH-associated seizures. However, the heterogeneity of identifiedstudies or case series did not allow for a statistical analysis ofthe RS outcome. Even though the literature search was notrestricted with specific criteria for variables, identified reportsoverwhelmingly consisted of case series or case reports. Forthese reasons, our systematic review had some limitations:first, a great heterogeneity across studies/case series in suchvariables as age, estimation of seizure outcome, side effects,and follow-up; second, a high ratio of incompletely reportedoutcome (Table 1); third, lack of prospectively randomizedtrials, directly comparing different RS methods or RS withsurgical modalities for HH. To reiterate, it is due to thesereasons that we did not validate the efficacy of outcomes, asthey would ultimately suggest a significant risk for bias in anyobservable results. From this point of view, any interpretationsfor efficacy/safety ratios for RS methods are not altogetherexpressive enough.
Gamma Knife RS
Outcomes of Gamma Knife RS in the therapy of gelastic ep-ilepsy caused by HH were evaluated though use of a prospec-tive methodology performed by Regis et al. [7]. However, thissingle-arm study did not provide comparative assessment ofthe therapy outcome with surgical techniques or other RSmethods. Fifty-seven patients treated with Gammy Knife RSwere included for evaluation of the therapy outcome; 48 ofwhom exceeded 3 years of follow-up. Significant seizure re-duction was achieved in more than 50% of patients treated for
Table 1 Safety and efficacy of different SRS modalities in the therapy of gelastic epilepsy associated with hypothalamic hamartoma (summary ofreports limited with ≥ 3 patients)
Author Year Patients Medianage,years
Tumor size,(mean or range,cm3)
RS/dose (Gy) Follow-up(mean or range,Mo)
Seizure free(Engel I + II)
Transientmemoryinjury
Radiogenicedema
Schulze-Bonhage[19]
2008 24 21.9 1.2 Brachy/60 Gy(s.d.)
24 11/24(45.8%)
2/24 5/24(20.8%)
Wagner [20] 2014 26 26.7 1.4 Brachy/60 Gy(s.d.)
13.8 2/26 (7.7%) 20–50% 10/26(38.5%)
Regis [7] 2013 48 16.5 0.398 GK/17 Gy (meanm.d.)
71 30/48 (65%) 0 0
Mathieu [21] 2010 9 29.8 0.8 GK/17 Gy (meanm.d.)
27.3 55.6% 0 0
Drees [18] 2012 4 27 0.20 GK/dose NA 58 2/3 0 0
Selch [12] 2005 3 34.7 0.15–1.12 LINAC/15-18 Gy(m.d.)
13–17 2/3 0 0
Golanov [22] 2010 6 8.5 0.3–3 LINAC/15.7(mean m.d.)
3–50 NA* NA NA
SRS stereotactic radiosurgery, Brachy interstitial brachytherapy, GK Gamma Knife, LINAC linear accelerator, s.d. surface dose, m.d.marginal dose, NAnot available, NA* seizure outcome according to the Engel’s grading is not available in the study of Golanov et al.
SN Compr. Clin. Med.
HH. Beyond seizure reduction, a greater improvement of psy-chiatric, as well as cognitive comorbidities, was acknowl-edged. For comparison, the use of endoscopic surgical ap-proaches achieved a significant alleviation of seizures in 43–68% of HH patients. This finding, notably, came accompaniedby a major reduction in rates of surgery-related morbidity andmortality [27, 28]. For example, there were no recorded in-stances of severe long-lasting neurophysiological or endocri-nologic side effects (i.e. malignant obesity, diabetes insipidus,etc.) related to resective surgery after Gamma Knife treatment[6, 29]. A series of retrospective evidences that evaluated theefficacy of Gamma Knife RS demonstrated a seizure remis-sion rate from 27 to 66% across studies [8–13]. Drees et al.observed a similar efficacy between surgical or Gamma Knifeprocedures in adults with small HH occurrences, for instance,achieving complete seizure freedom in over one-third of pa-tients [30]. This, by comparison, is a worsened outcome forseizure control compared to that of younger patients, in whichthe seizure freedom rate after Gamma Knife treatment variesbetween 37 and 66% [11, 23, 31]. Interestingly, only the ab-sence of mental retardation was significantly associated withthe seizure-free outcome [30]. There are no prospective stud-ies directly comparing the outcome and safety of minimallyinvasive techniques, such as Gamma Knife with open surgery/microsurgery in the therapy of HH. However, the realizationof such prospective trials could be complicated due to therelative rarity of this disease. Regis et al. offered treatmentstrategies for the HH according to its topological type [29].Types I and II and small type III HH are good candidates forthe Gamma Knife RS. Types IV, V, and VI are frequentlyoperable or undergo the combined therapy including surgeryfollowing by Gamma Knife RS. An example of a large HH isshowed in Fig. 2. Some single-center reports showed low ratesof the primary morbidities after surgical treatment althoughthey remain significantly higher compared to the GammaKnife treatment [19, 32, 33]. According to Thom et al., therisk of death in surgery averaged to 0.24%; a chance of seriouspermanent complications averaged to 2%, and transient
complications averaged to 6% [33]. In the study of Dreeset al., only the patients who underwent resection suffered astroke (15%) and mortality rate averaged to 10% [30]. Oneadult patient treated with Gamma Knife RS experiencedweight gain (25%), although no weight gain was typicallyfound in younger populations [20, 23, 30]. The impairmentsin neurocognition related to open surgery remain significant,with patients experiencing occurrence rates upwards of 10–60% [20, 22, 27, 30]. Analysis of several evidences, includinga large prospective trial performed by Regis et al., revealed thecorrelation between margin radiation dose of HH in theGamma Knife RS and seizure remission rate. Patients whoreceived a dose of at least 17 Gy to the margin of HH demon-strated a higher outcome of seizure remission than those treat-ed with less than 13 Gy [7]. However, the efficacy of GammaKnife RS was found to be diminished in therapies for largehamartomas, as defined by stages V and VI, according to theclassification of Delalande et al. [7, 29, 34]. The combinedtherapy with resection of the part of hamartomas, as a firststep, and by using of Gamma Knife RS of the residue in asecond treatment step, was found to be more effective forlarger lesions [7, 29]. In the retrospective data reported byDrees et al., 70% of patients with a HH volume < 0.2 cm3
underwent either endoscopic resection or Gamma Knife RSwith similar efficacy concerning seizure control [30]. The sec-ond limitation factor of Gamma Knife treatment is its delayedoutcome. According to analyzed reports, the latency time var-ied between 3 to 36 months. Delayed efficacy of the GammaKnife RS may be problematic in patients with severe epilepsythat affects the psychiatric and cognitive functions. For thesepatients, primarily standard surgical treatments may be pre-ferred over Gamma Knife treatment. To summarize, theGamma Knife RS may have a superior seizure outcome inpatients if they are children rather than adults. Smaller occur-rences of HH, which are localized a sufficient distance fromthe optic chiasm, optic tracts, or fornices, may be favored fortheir therapy with Gamma Knife RS as compared to standardsurgical treatment.
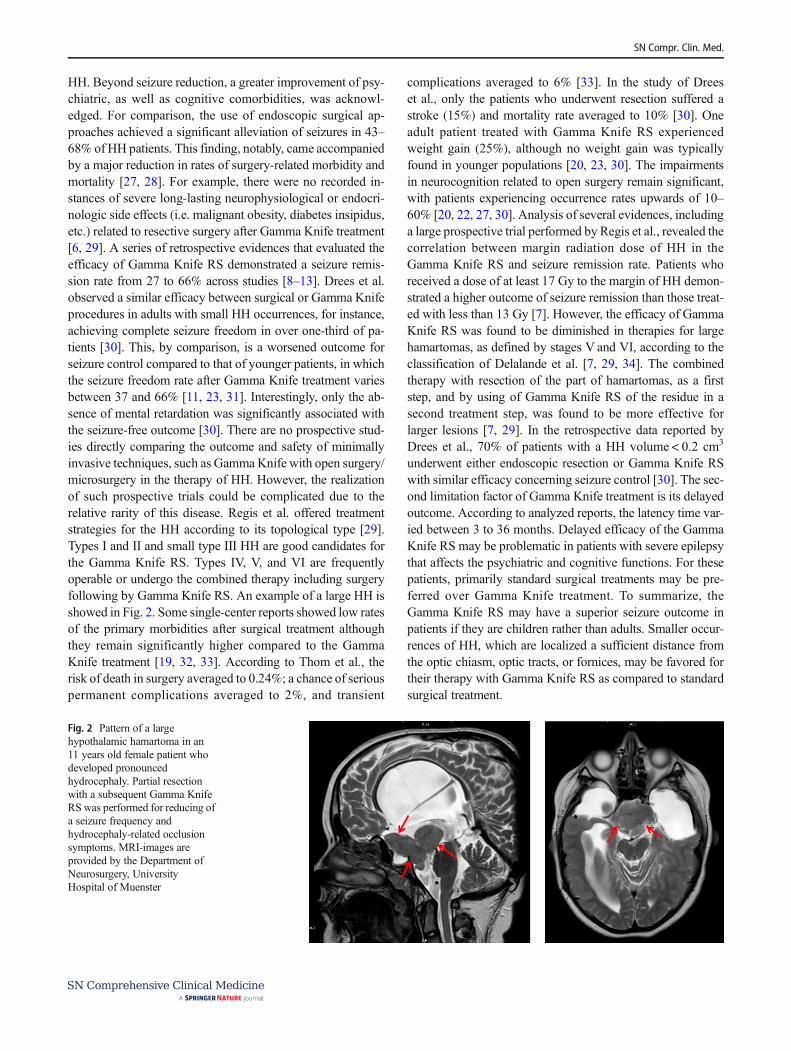
Fig. 2 Pattern of a largehypothalamic hamartoma in an11 years old female patient whodeveloped pronouncedhydrocephaly. Partial resectionwith a subsequent Gamma KnifeRSwas performed for reducing ofa seizure frequency andhydrocephaly-related occlusionsymptoms. MRI-images areprovided by the Department ofNeurosurgery, UniversityHospital of Muenster
SN Compr. Clin. Med.

Interstitial Brachytherapy
The first major evidence for interstitial brachytherapy ofgelastic epilepsy related to HH was published by Schulze-Bonhage et al. in 2008 [24]. Over 46% of patients wereseizure-free or achieved a seizure reduction of at least 90%(Engel classes I and II). The duration and severity of epilepsybefore therapy negatively affected the treatment outcome.Patients who achieved a significant seizure reduction oftendemonstrated positive behavioral effects and improvement incognitive function. In 29% of patients, tests revealed a radio-logical reduction in HH volume, suggesting seizure reductionwithout complete tumor destruction in most patients. Thetreatment outcome following seeds implantation ranged from2 up to 8 months, which is faster than after Gamma Knife RS,but ranks similar to results following microsurgical resection[6, 7, 28, 29]. Unlike external radiation by use of LINAC orGamma Knife, the smaller effective dose rate correspondingto hyperfractionated radiotherapy is applied with interstitialbrachytherapy. Moreover, the advantage in the dose distribu-tion of radiation to the surrounding organ at risk can be ex-pected for the interstitial RS compared to the external radia-tion modalities. The authors judged the risk for bleeding dur-ing seed implantation in about 0.6% of patients. Such sideeffects as hyperphagia, and treatment-related brain edema,appeared in a small number of patients (20.8%). This phenom-enon was accompanied by the transient appearance of head-aches, fatigue, and lethargy. The majority of patients, howev-er, showed a marked improvement in overall cognitive func-tionality. Similar to the Gamma Knife RS, a longer duration ofepilepsy and large hamartoma size were negatively associatedwith seizure control and cognitive function. On the contrary,there was a 1 to2% risk of haemorrhage associated with inser-tion of stereotactic probes into the brain during interstitialbrachytherapy. Wagner et al. took cognizance of memory out-come by use of a median follow-up at around 13.8 months[25]. Impairments appeared more often in declarative memoryfunction in 20 to 50% of the patients, while attentional func-tions were stable or revealed an improved performance in amore than 80% of patients. To summarize, in about half of allpatients treated with interstitial brachytherapy featured a sig-nificant reduction in seizures. A longer duration of epilepsyprior to interstitial brachytherapy is negatively correlated withseizure control. A larger hamartoma size, along with eccentricseeds positioning, were correlated with radiogenic edema.
LINAC-Based RS
The indication of LINAC RS for patients with medicallyrefractory gelastic seizures related to HH was rather excep-tional. In the literature, we find that only 13 patients withHH received the LINAC RS. For this reason, the meta-analysis of therapy efficacy and safety for LINAC-based
RS is actually not factful. The largest studies were per-formed by Selch et al. and by Golanov et al. [12, 26]. Theauthors showed significant reduction in the seizure rate;however, the therapy efficacy was delayed from 7 to9 months in these experiences. Similarly, the median laten-cy time reported in the large series with Gamma Knife RSwas 9 months [7]. Due to the limited number of patients, theauthors could not elucidate upon any prognostic factors fortherapy outcome. Additionally, any adequate radiationdoses for seizure control could not be determined due tothe small number of patients treated with LINAC RS.Munari et al. observed no effect after 18Gy delivered byLINAC [35]. Some relevant additional predictive factorsas number of gelastic seizures prior to treatment or tumorsize may affect the SRS outcome. Nonetheless, the study ofSelch et al. revealed that seizure-free patients experiencedtwo to six gelastic seizures per day [12]. Thus, the indepen-dent effects of radiation dose and seizure frequencies re-main uncertain and should be evaluated in a multivariateanalysis. The patients treated with LINAC-based RS didnot develop any neurological or endocrinological injury;however, a longer follow-up is needed to establish long-term RS side effects [36, 37]. Thus, the LINAC RS mayrepresent an alternative therapy approach for epilepsy relat-ed to HH. Extensive trials recruiting a large number of pa-tients with a longer follow-up are needed to evaluate theefficacy and tolerability of the LINAC-based RS.
Conclusion
This systematic review emphasizes both the safety and ef-ficacy of different radiosurgery techniques in the therapy ofgelastic epilepsy related to the HH. The literature demon-strates that all modern surgical and RS techniques achieveapproximately the same probability of seizure freedom andlower rate of therapy-related side effects, particularly, neu-ropsychological deterioration or endocrinologic toxicity.There are several common limitations for the RS therapies,such as the large size of hamartomas and its delayed effica-cy. For these reason, the treatment option must be individ-ually selected given the severity of epilepsy and the feasi-bility of the therapy method per each individual case.Considering the safety/efficacy profile, the RS can be con-sidered as a first-line treatment option in patients with bothsmall- or middle-sized HH and low seizure frequency priorto applied therapy.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
SN Compr. Clin. Med.

Ethical Approval This article does not contain any studies with humanparticipants performed by any of the authors.
Publisher’s Note Springer Nature remains neutral with regard to juris-dictional claims in published maps and institutional affiliations.
References
1. Freeman JL, Coleman LT, Wellard RM, Kean MJ, Rosenfeld JV,Jackson GD, et al. MR imaging and spectroscopic study of epilep-togenic hypothalamic hamartomas: analysis of 72 cases. AJNRAmJ Neuroradiol. 2004;25:450–62.
2. Kerrigan JF, Ng YT, Chung S, Rekate HL. The hypothalamichamartoma: a model of subcortical epileptogenesis and encepha-lopathy. Semin Pediatr Neurol. 2005;12:119–31. https://doi.org/10.1016/j.spen.2005.04.002.
3. Nguyen D, Singh S, Zaatreh M, Novotny E, Levy S, Testa F, et al.Hypothalamic hamartomas: seven cases and review of the litera-ture. Epilepsy Behav. 2003;4:246–58. https://doi.org/10.1016/S1525-5050(03)00086-6.
4. Quiske A, Frings L, Wagner K, Unterrainer J, Schulze-Bonhage A.Cognitive functions in juvenile and adult patients with gelastic ep-ilepsy due to hypothalamic hamartoma. Epilepsia. 2006;47:153–8.https://doi.org/10.1111/j.1528-1167.2006.00381.
5. Weissenberger AA, Dell ML, Liow K, et al. Aggression and psy-chiatric comorbidity in children with hypothalamic hamartomasand their unaffected siblings. J Am Acad Child AdolescPsychiatry. 2001;40:696–703. https://doi.org/10.1097/00004583-200106000-00015.
6. Quigg M, Harden C. Minimally invasive techniques for epilepsysurgery: stereotactic radiosurgery and other technologies. JNeurosurg. 2014;121:232–40. https://doi.org/10.3171/2014.8.GKS141608.
7. Régis J, Lagmari M, Carron R, Hayashi M, McGonigal A, DaquinG, et al. Safety and efficacy of gamma knife radiosurgery in hypo-thalamic hamartomas with severe epilepsies: a prospective trial in48 patients and review of the literature. Epilepsia. 2017;58:60–71.https://doi.org/10.1111/epi.13754.
8. Barajas MA, Ramírez-Guzman MG, Rodríguez-Vázquez C,Toledo-Buenrostro V, Cuevas-Solórzano A, Rodríguez-HernándezG. Gamma knife surgery for hypothalamic hamartomas accompa-nied by medically intractable epilepsy and precocious puberty: ex-perience in Mexico. J Neurosurg. 2005;102(Suppl):53–5.
9. Mathieu D, Kondziolka D, Niranjan A, Flickinger J, Lunsford LD.Gamma knife radiosurgery for refractory epilepsy caused by hypo-thalamic hamartomas. Stereotact Funct Neurosurg. 2006;84:82–7.https://doi.org/10.1159/000094036.
10. Régis J, Bartolomei F, de Toffol B, Genton P, Kobayashi T, Mori Y,et al. Gamma knife surgery for epilepsy related to hypothalamichamartomas. Neurosurgery. 2000;47:1343–51.
11. Régis J, Scavarda D, Tamura M, Nagayi M, Villeneuve N,Bartolomei F, et al. Epilepsy related to hypothalamic hamartomas:surgical management with special reference to gamma knife sur-gery. Childs Nerv Syst. 2006;22:881–95. https://doi.org/10.1007/s00381-006-0139-y.
12. Selch MT, Gorgulho A, Mattozo C, Solberg TD, Cabatan-AwangC, DeSalles AA. Linear accelerator stereotactic radiosurgery for thetreatment of gelastic seizures due to hypothalamic hamartoma.Minim Invasive Neurosurg. 2005;48:310–4. https://doi.org/10.1055/s-2005-915598.
13. Unger F, Schröttner O, Feichtinger M, Bone G, Haselsberger K,Sutter B. Stereotactic radiosurgery for hypothalamic hamartomas.Acta Neurochir Suppl. 2002;84:57–63.
14. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA group.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. J Clin Epidemiol. 2009;62:1006–12.https://doi.org/10.1016/j.jclinepi.2009.06.005.
15. Onwuegbuzie AJ & Frels R. Seven steps to a comprehensive liter-ature review. Los Angeles, 2015; CA: Sage.
16. Williams JK. A comprehensive review of seven steps to a compre-hensive literature review. Qual Rep. 2018;23:345–34 https://nsuworks.nova.edu/tqr/vol23/iss2/4.
17. Higgins J & Green S (Editors). Cochrane handbook for systematicreviews of interventions version 5.1.0 (updatedMarch 2011); http://www.cochrane-handbook.org (accessed 21 Dec 2017).
18. Flickinger JC, Lunsford LD, Kondziolka D, Maitz AH, EpsteinAH, Simons SR, et al. Radiosurgery and brain tolerance: an analy-sis of neurodiagnostic imaging changes after gamma knife radio-surgery for arteriovenous malformations. Int J Radiat Oncol BiolPhys. 1992;23:19–26.
19. Wyler AR, Hermann BP, Somes G. Extent of medial temporal re-section on outcome from anterior temporal lobectomy: a random-ized prospective study. Neurosurgery. 1995;37:982–90.
20. Anderson JF, Rosenfeld JV. Long-term cognitive outcome aftertranscallosal resection of hypothalamic hamartoma in older adoles-cents and adults with gelastic seizures. Epilepsy Behav. 2010;18:81–7. https://doi.org/10.1016/j.yebeh.2010.02.018.
21. Wieser HG, Blume WT, Fish D, et al. ILAE commission report.Proposal for a new classification of outcome with respect to epilep-tic seizures following epilepsy surgery. Epilepsia. 2001;42:282–6.https://doi.org/10.1046/j.1528-1157.2001.35100.
22. Harvey AS, Freeman JL, Berkovic SF, Rosenfeld JV. Transcallosalresection of hypothalamic hamartomas in patients with intractableepilepsy. Epileptic Disord. 2003;5:257–65.
23. Mathieu D, Deacon C, Pinard CA, et al. Gamma knife surgery forhypothalamic hamartomas causing refractory epilepsy: preliminaryresults from a prospective observational study. J Neurosurg.2010;113:215–21. https://doi.org/10.3171/2010.8.GKS101059.
24. Schulze-Bonhage A, Trippel M, Wagner K, Bast T, Deimling FV,Ebner A, et al. Outcome and predictors of interstitial radiosurgery intreatment of gelastic epilepsy. Neurology. 2008;71:277–82. https://doi.org/10.1212/01.wnl.0000318279.92233.82.
25. Wagner K, Buschmann F, Zentner J, Trippel M, Schulze-BonhageA. Memory outcome one year after stereotactic interstitial radiosur-gery in patients with epilepsy due to hypothalamic hamartomas.Epilepsy Behav. 2014;37:204–9. https://doi.org/10.1016/j.yebeh.2014.06.031.
26. Golanov AV, Kornienko VN, Trunin II, Kostiuchenko VV,Gorlachev GE, Gorelyshev SK, et al. Stereotactic radiosurgery intreatment of patients with hypothalamic hamartomas. Zh VoprNeirokhir Im N N Burdenko. 2010;1:24–9.
27. Miranda P, Esparza J, Cabrera A, Hinojosa J. Giant hypothalamichamartoma operated through subfrontal approach with orbitary rimosteotomy. Pediatr Neurosurg. 2006;42:254–7. https://doi.org/10.1159/000092365.
28. Palmini A, Chandler C, Andermann F, Costa da Costa J, Paglioli-Neto E, Polkey C, et al. Resection of the lesion in patients withhypothalamic hamartomas and catastrophic epilepsy. Neurology.2002;58:1338–47. https://doi.org/10.1212/WNL.58.9.1338.
29. Régis J, Scavarda D, Tamura M, Villeneuve N, Bartolomei F, BrueT, et al. Gamma knife surgery for epilepsy related to hypothalamichamartomas. Semin Pediatr Neurol. 2007;14:73–9. https://doi.org/10.1016/j.spen.2007.03.005.
30. Drees C, Chapman K, Prenger E, Baxter L, Maganti R, Rekate H,et al. Seizure outcome and complications following hypothalamichamartoma treatment in adults: endoscopic, open, and gamma knifeprocedures. J Neurosurg. 2012;117:255–61. https://doi.org/10.3171/2012.5.JNS112256.
SN Compr. Clin. Med.

31. Abla AA, Shetter AG, Chang SW, et al. Gamma knife surgery forhypothalamic hamartomas and epilepsy: patient selection and out-comes. J Neurosurg. 2010;113:207–14. https://doi.org/10.3171/2010.8.GKS101027.
32. Shamim S, Wiggs E, Heiss J, Sato S, Liew C, Solomon J, et al.Temporal lobectomy: resection volume, neuropsychological ef-fects, and seizure outcome. Epilepsy Behav. 2009;16:311–4.https://doi.org/10.1016/j.yebeh.2009.07.040.
33. Thom M, Mathern GW, Cross JH, Bertram EH. Mesial temporallobe epilepsy: how do we improve surgical outcome? Ann Neurol.2010;68:424–34. https://doi.org/10.1002/ana.22142.
34. Delalade O, Fohlen M. Disconnecting surgical treatment of hypo-thalamic hamartoma in children and adults with refractory epilepsy
and proposal of a new classification. NeurolMed Chir. 2003;43:61–8. https://doi.org/10.2176/nmc.43.61.
35. Munari C, Kahane P, Francione S, Hoffmann D, Tassi L, Cusmai R,et al. Role of the hypothalamic hamartoma in the genesis of gelasticfits (a video-stereo-EEG study). Electroencephalogr ClinNeurophysiol. 1995;95:154–60.
36. Tishler RB, Loeffler JS, Lunsford LD, Duma C, Alexander E III,Kooy HM, et al. Tolerance of cranial nerves of the cavernous sinusto radiosurgery. Int J Radiat Oncol Biol Phys. 1993;27:215–21.https://doi.org/10.1016/0360-3016(93)90230-S.
37. Voges J, Treuer H, Sturm V, Büchner C, Lehrke R, Kocher M, et al.Risk analysis of linear accelerator radiosurgery. Int J Radiat OncolBiol Phys. 1996;36:1055–63. https://doi.org/10.1016/S0360-3016(96)00422-1.
SN Compr. Clin. Med.





























