Embed Size (px)
Citation preview

Page 19 BJC Vol I No 2
IATED D I S O R D E R S ctic Associat ion 's Au tumn Confe rence 1 9 9 7
R a d i o l o g i c a l C a s e Stud ies : A s s e s s m e n t of C e r v i c a l Sp ine S t a b i l i t y
Jane Cook, DC, DACBR
When assessing the chiropractic patient who has received a hyperflexion/extension or 'whiplash' type of cervical spine injury, it is important Io eval- uate the cervical X-rays correctls:
If the patient does not exhibit any neurological sigms and symptoms and if their routine cervical series (lateral cervical neutral, anteroposterior lower cervical and anteroposterior open mouth) does not show an acute disruption in alignment or obvious fractures, flexion and extension cervical lateral views are not contraindicated and should bc taken.
The Hcnderson-Dormon method of assessing intersegmental movement of C2 to ('7 during flex- ion and extension of the cervical spree is a useful procedure, ellen emplyed m the teaching clinic at the Anglo European College of Chiropractic. The inter and intra-cxaminer reliability has been researched and has been fnnnd to bc very good. particularly from C2 to (/6.
The assessment requires the cxaminer to place a clear acetate sheet over lhe neutral lateral cerxi- cal views and trace around the vertebral bodies from C2 to ('7. The acetate is then placed oxer the flexion lateral view and the outline of ('7 (neutral) is positioned exactly over C7 on this viex~.
The exalniner then outlines the vcrtebral body (76 in the flexion view. It is caster if this is done in a difl;erent colour. The outline of the neutral posi- tion C6 is then moved exactly over (76 on the flex- ion view, and the C5 vertebral body on the flexion ~icw is outlined. This procedure continues tip to the C2 vertebral body. A similar process is used to outline each segment on the extension latenil views, again using a difli~rent colour.
The resulting diagram on the ticetaie i~ then assessed as tbllows: The anteroposterior vertebral mid-body diameter is measured at each level. The total excursion of each vertebral body is then mea- sured using the posterior superior corner of the bod~: The latter measurement is placed o~cr the fiwmcr and multiplied by I O0 to gain a pcrccntage figure.
Henderson and Dormon have Ibund thai 50", intersegmental nnovenlent is \~.ithin normal lilllils. Movement grealer than this is described as rela- tively hypermobile for movemenl of 50 to 6000: hypennobile from 60 to 72'!, and movement greater than this is regarded as demonstration of instability" Movement of 40 to 50'~ i, is termcd "rel- ati~ ely hypnmobility'. A "fixed' motioil segment is
one that has under 28% movement. These values obviously have implications to
the manipulating practitioner, and the Henderson- Dormon method is a quick, relaible and accurate method of localising hyper- or hypo-mobile motion segments that can be treated appropriately.
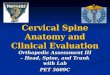
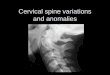
An example of the Henderson.Dormon method of assessment for cervical intersegmental motion in the sagital plane.
A Flexion
8
Extension
--~ ,7~ .4--
7_.; Adapted from Henderson and Dormon, 1985.
J
A: Completed template study. Solid line represent the vertebral alignment in the neutral ce~'ical view. hlierruptcd lines, depict the extreme flexed or extended positions in relation to the vertebral segment immediately below. B: Rocntgenometric analysis ofintersegmental motion ofC2-3 through C6-7. The ratio of estimated trans- lation I.vl to sagittal body diameter (v) provides motion values denoted percent sagittal body diameter (, .SBD)