Observation of 500 metaphases in 2-2.5 days scoring The dicentric assay 48 h Cell culture Spreading Observation of 500 metaphases in 2-2.5 days scoring Dicentrics acentrics Blood Processing 2 x 5 ml blood collected on heparin This slide is a summary reminder of the steps in the dicentric assay which requires 3 days to produce an initial triage dose estimates followed later by full dose estimates. 3 days 500 cells 48 hours 1 day 1 hour 50 cells
Radiological Accidents in Georgia
Lecture Module 15 Lecture: Radiological accidents in Georgia
Purpose: To present case histories of two radiological accidents
that occurred in Georgia and the biodosimetry response Learning
objectives: Upon completion of this lecture the participants will
know: The background circumstances of the two accidents The
biodosimetry results The application of the G-function calculation
to compensate for dose protraction A comparison of the dose
estimates from the dicentric assay with, where available, results
from FISH and electron spin resonance An illustration of follow-up
studies showing the relative declines with time of the dicentric
and translocation frequencies Duration: 1 hour Observation of 500
metaphases in 2-2.5 days scoring
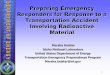
The dicentric assay 48 h Cell culture Spreading Observation of 500
metaphases in days scoring Dicentrics acentrics Blood Processing 2
x 5 ml blood collected on heparin This slide is a summary reminder
of the steps in the dicentric assay which requires 3 days to
produce an initial triage dose estimates followed later by full
dose estimates. 3 days 500 cells 48 hours 1 day 1 hour 50 cells
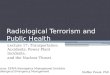
Dose effect curves WHOLE BODY DOSE
Yield of dicentrics and centric rings per cell 0,5 1 1,5 2 2,5 3
3,5 4 4,5 5 6 7 8 9 Dose (Gy) Bare source (n/g=0.86) Lead shield
(n/g=5.6) CH2 shield (n/g=0.12) 0,0 0,2 0,4 0,6 0,8 1,0 1,2 1,4 1,6
1,8 Cobalt-60 (0.1 Gy/min) Cobalt-60 (0.5 Gy/min) X-Ray (0.1
Gy/min) Caesium (0.5 Gy/min) These are examples of the laboratorys
standard acute dose effect curves for various qualities of high and
low LET radiation. The most appropriate curve is chosen for
converting the aberration frequency obtained from the patients into
estimates of absorbed dose. WHOLE BODY DOSE Biological tests
(hematological analysis, biochemical data, HLA, etc.)
Summary of the different strategies for dealing with a few or many
patients Expertise (Priority to the dose assessment) Emergency w/o
population triage (Priority to the medical evaluation) Emergency w
population triage (Priority for the distribution in categories)
Clinical symptoms Biological tests (hematological analysis,
biochemical data, HLA, etc.) Physical dosimetry Biological
dosimetry quick but not precise Biological dosimetry very precise
Medical team All persons are firstly assessed for clinical signs of
overexposure. This is supplemented by a series of blood tests
usually available as routine procedures in most clinics and
hospitals. Where possible, physical dosimetry by measurements and /
or calculations are carried out. At the same time blood samples are
taken for biological dosimetry.For events involving just one or a
few patients precise biological dosimetry is performed. All
information from biological dosimetry, routine blood tests and
physics is reported back to the medical team to assist in their
clinical decision taking. In the case a large number of patients
biological dosimetry will be operated firstly in triage mode, to
produce initial dose estimates. Together with the other information
that is then available the patients can be prioritised for
extending the biological dosimetry to precise dose estimates.
Biological dosimetry more precise Clinical decision & treatment
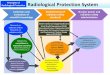
Time Time 4 Influence of the number of cells analysed on the
precision of dose estimation
Confidence intervals at 95 %: include the true value of the dose
The precision of the dose measurement is dependent on the number of
cells scored and the number of chromosome aberrations found in the
blood sample. This graph illustrates how the 95% confidence limits
on the same dose estimate of Gy are reduced by scoring more cells.
In triage mode where 50 cells are quickly scored the confidence
interval is about 1Gy, sufficient for a first triage. A full dose
estimate is based classically on the examination of 250 to 500
cells which takes more time. In this example for 500 cells
examined, the confidence interval is about 0.2 Gy. Triage based on
50 cells: 1 hour More precise dose estimation: 2-3 days Dose
reconstruction by biological dosimetry for the accident at Lilo
(Georgia, 1997)
Between 1997 and 2001 there were 3 radiation accidents in Georgia
involving either soldiers or members of the general public. These
accidents had a common cause: many radioactives sources were
abandoned in some former military camps when the Russian army left
Georgia. All 3 accidents were dealt with by an IAEA mission help by
a French delegation. Each individual involved in the accidents was
assessed for biological dosimetry by cytogenetics. Because, for
biological dosimetry, the most interestingevents were the first two
in 1997 and 1998 just these are summarized in this presentation.
Location in Georgia LILO, 1997
Lilo is a small city located 25 km east of the capital Tbilisi.
Lilo military training center
1997: 11 Georgian soldiers developed radiation induced skin lesions
and acute radiation syndrome 12 radioactive sources (Cs-137, Co-60,
Ra-226) abandoned at different locations in a former training
Russian military camp, some in this underground shelter. The most
irradiated victim (33 patches on his body) LILO: accident
circumstances (1)
Source container seems to have been opened by patient AN, but the
source remained inside for some time. Then the source was placed in
pocket of EPs coat. The coat was borrowed regularly leading to
irradiation of other persons. TK and CG shared the same room with
AN and EP and all used the coat, with the source in a pocket, as a
night time bed blanket. Irradiation occurred from mid 1996 to April
1997 Discovery of the exposures was in August 1997 Fuller details
of the circumstances and the patients clinical conditions can be
found in the IAEA book (2002) describing this event. LILO: accident
circumstances (2)
11 people with different levels of expsoure The 4 most exposed
people were hospitalized in France, the 7 others in Germany All
patients in France suffered from lymphopenia and nausea AN suffered
from contractures affecting the hands and lesions on the abdomen TK
displayed a deep lesion on the right thigh EP displayed 33 patches
on the trunk and thighs CG had hand and thigh lesions Fuller
details of the circumstances and the patients clinical conditions
can be found in the IAEA book (2002) describing this event. Results
of the dicentric analyses
First dose estimations obtained in October 1997 for the 4 most
seriously irradiated soldiers hospitalized in the Curie Institute
and Percy Hospital , Paris (cases 1 to 4) and for the 7 others
hospitalized in Ulm University Clinic (cases 5 to 11). Estimates of
averaged whole body doses were made by reference to Co-60
calibration curves. Patients 1 and 2 showed significant
overdispersion of their dicentric distributions (the u- test
statistic). Analyses made in October 1997 Details of biological
dosimetry by cytogenetics for the 4 most irradiated patients
4 patients hospitalized in France Analyses performed by 23/10/1997
Dicentric distribution Case Cells DicCrAce u-test Adu Eli God Kak
Dic = dicentrics; Cr = centric rings; Ace = excess acentrics
Lymphopenia was already present before the patients' arrival in
France. Consequently, the integrated equivalent whole-body doses
may be underestimations of the true doses because the dicentric
aberration is unstable and is removed more rapidly with
lymphopenia. For the first two patients the u-test indicated
overdispersion, consistent with heterogeneous irradiation, even
though the proportion of cells with several anomalies was
relatively low. Moreover, there was a lot (13% and 14%) of cells
with dicentrics without an accompanying acentric. This percentage
is abnormally high for acute irradiations and may be explained by
the fact that during cell division, dicentrics have a 50% chance of
passing from the mother cell to one of the two daughter cells. The
accompanying acentric fragments, on the other hand, are lost during
the division. This suggests that an exposure of relatively low
intensity took place, either continuously or at repeated intervals
for several days, weeks, or months, thus allowing partial
replenishment of the lymphocyte population. For patients 3 and 4
who also had received heterogeneous exposure, as shown by their
skin lesions, the dicentric distributions surprisingly showed no
evidence of overdispersion.It is possible that the lymphopaenia led
to the most highly irradiated cells being lost first and by the
time that they came to analysis lymphocytes containing only a
single aberration were seen. 12 Protracted/chronic exposure :
correction by the G-function
Initial dose-effect curve : Y= c + D +D2 For a protracted exposures
the acute curve is modified by the G-function G(x) = 2/x2
[x-1+exp(-x)] where x= t/t0 t= the actual exposure time t0=2h The
circumstances of the event were clearly that the men had been
irradiated on many different occasions, i.e.,fractionated exposures
and many single events were likely to have been protracted,
typically over several hours. This non-acute nature of their
exposures therefore needs to be considered in arriving at more
realistic dose estimates. The acute in vitro calibration curve is
modified by the G-function which is applied to the D2 term of the
yield equation which represents the dose rate and dose
fractionation sensitive component of the induced aberrations (see
the lecture on statistical techniques). However this procedure in
practice only operates for exposures of a few hours duration. For
longer times G(x) tends to zero so that the dose-effect curve
becomes simply linear Y = D as shown by the blue curve in the
graph. . Modified dose-effect curve : Y= c + D +G(x)D2 Correction
of cytogenetics results and comparison with ESR data
Initial Doses (Gy) 1 1.2 2 1.6 3 0.7 4 0.5 5 0.1 6 0.3 7 8 9 10 11
Corrected Doses (Gy) 4.2 5.9 1.5 1.1 0.2 0.6 0.7 4.1 Doses by ESR
(Gy) ND 4.5 1.4 1.5 0.7 1.3 0.1 0.4 Taking into account the
probable mix between chronic and repeated exposure during several
months, a simplifying assumption was made that the most appropriate
dose response to use for dose estimation was Y = D and not to
attempt a more sophisticated analysis involving the G function, as
duration information on the protracted individual exposures was
inadequate. The table shows the initial averaged whole body doses
based on the acute dose response curve and then the recalculated
(corrected) values based on the linear term only. It became
possible in some cases to obtain teeth and /or bone samples which
were sent to the Institute of Biophysics, Moscow for measurement by
electron spin resonance (ESR). This technique provides an
integrated total dose received by the tooth or piece of bone and is
not subject to dose rate modification. It is analagous to a
monitoring badge permanently worn in the same place and therefore
provides a measurement of dose at that point. Given that exposures
were heterogeneous the point dose estimate is also an approximation
of the true integrated dose. Nevertheless it was gratifying to note
that particularly for the most severe cases the corrected
cytogenetic values were closer than the initial values to the ESR
results. Nevertheless, regarding the very complex story of
irradiation, it is better to consider the results obtained by the
application of G-function and the ESR as a working hypothesis
rather thantrue values. ND = not done Some follow-up data An
occasional follow-up blood sampling of the 4 patients treated in
France was possible and this demonstrated the well known decline
with time in the frequency of the dicentric type of aberration.
Each was sampled 4 times and there was a complete disappearance of
dicentrics for three of the patients occuring either in the 3rd or
4th samples, whereas in person Eli the dicentrics were more
persistent. This is a good illustration of the variability in
dicentric persistence and the unsuitability of the dicentric as a
biological dosemeter long after irradiation. Comparison of
dicentric and translocation yields when patients were first
sampled
The figure shows the respective level of dicentrics, reciprocal and
total translocations scored in October 1997 in the blood
lymphocytes of the 4 most irradiated victims. Overall there is a
good level of agreement. For God no difference was seen in the
doses estimated by dicentric or translocation yields. For Kak and
Eli, a higher dose was assessed using translocations, but the
difference was not statistically significant. For patient Adu
however, a higher dose was estimated using dicentrics. To explain
these discrepancies, one can assume that the heterogeneity of
exposure differed from one patient to another. This has modified
the distribution of translocations in unstable cells and
consequently the relative disappearance of dicentrics compared to
translocations during the time from first exposure to first blood
sampling, exacerbated by the lymphopaenia FISH follow-up More
interesting is the FISH follow-up which was made with the 4
patients. The translocations in stable cells were scored. In
contrast to the dicentric persistence presented in a previous
slide, no decline in the frequency of two-way translocations was
observed for three of the 4 patients. For patient Kak, the
frequency of translocations decreased two months after the first
blood sample was taken, but the confidence interval included the
initial value of the translocations yield. This has illustrated
that generally there is a better persistence of translocations
which makes them better suited for retrospective dosimetry. After
four years, and considering the initial lymphopenia, it is assumed
that the blood was repopulated by lymphocytes coming from bone
marrow. Therefore these results suggest that in 3 cases the
irradiation of bone marrow was relatively homogeneous and the dose
was similar to that of the peripheral blood lymphocyte pool.
Conclusion Complex exposure scenario Exposures protracted
Delayed discovery Dicentric assay still possible Linear dose
response curve used Reasonable agreement with ESR Follow-up
dicentrics reduced with time Greater stability of translocations
Translocations probably reflect the bone marrow dose The second
accident Dose reconstruction by biological dosimetry for the
accident at Matkhoji (Georgia, 1998) The location MATKHOJI, 1998
Matkhoji is a small village, 300 km west of the capital,Tbilisi.
Key-dates in the IAEA mission to Georgia 1.
4 August 1998 : Georgia requested assistance from the IAEA for
radioactives sources found in and near Matkhoji. 10~14 August :
IAEA teamidentified problems and needs. ThreeCs-137 sources found:
150 GBq in a pit in a field 65 m from the main road dose rate: 0.15
mSv/h at 1 m. 3.3 GBq in an empty yard 4 m of the same road; dose
rate: 0.3 mSv/h at 1 m. 0.17 GBq in a barn; dose rate: 15 Sv/h at 1
m. The pit was used as a swimming pool mainly by children and the
empty yard as a playground. In the barn, the source was found close
to the place where cows were milked each day. Key-dates 2. 13
August :IAEA requested France to perform biodosimetry. 14 August :
Difficulties for local medical team to identify thecritical
individuals. 18 August : France offered to send a physicist and a
physician to help the Georgian medical team to identify thecritical
persons. 16 September: Hematological screening by local medical
team on 800 suggested that 60 people could have received 0.2 Gy.
12~17 October 1998 :Georgia requested help through IAEA anda French
team of two physicians, a physicist and a translator went to
Georgia. French teams decisions
To collect information about the circumstances of the exposure
directly from the Matkhoji people and the Georgian authorities. To
make blood cell counts on local people, to detect leucopaenia. To
blood sample some tens of people for biological dosimetry. People
sampled: children using the pit and playground and people living in
the barn. Timetable of the biodosimetry in Paris
Quick triage: 50 cells per case: Saturday 17th October (day 0) 85
blood samples arrive in Paris First blood cultures Sunday 18th
October (d1) Second blood cultures Monday 19th October (d2) Mitotic
block and harvesting of the first cultures after 48 h Tuesday 20th
October (d3) Mitotic block and harvesting of the second cultures
after 50 h Wednesday 21st October (d4) Staining slides and starting
triage scoring Thursday 22nd October to Monday 26 October (d5 - 7)
Completed scoring, using six observers and an image analysis system
Full analyses: increased scoring to 250 cells per case: From
Tuesday 27th October to Thursday 17th December 1998 In view of the
need to assess 85 people promptly, the biodosimetry was firstly
made in triage mode.Processing all the blood samples and the triage
scoring was completed in 7 days. The second phase was to increase
the statistical precision by increasing the number of cells scored
to 250 per case. This was achieved for all patients but two. The
blood samples had been transportedbadly and so there was
considerable variation in the mitotic indices. Summary of
biodosimetry results
First triage step : 85 individuals, mainly children On a basis of
50 cells scored per individual 1 blood sample with two cells
carrying one dicentrics each; 1 blood sample with a cell carrying
one dicentric; 1 blood sample with a cell carrying two dicentrics.
82 blood samples with no dicentrics Conclusion : the dose
estimation is within the Gy range The triage data showed few
dicentrics. This seemed to be in accord with the normal
haematological data obtained in Matkhojiby the IAEA mission. The
second phase of dose examination confirmed the triage phase. The
Paris laboratorys spontaneous dicentrics frequency in a normal
population is about 1 dicentrics per 2000 cell. Therefore in the
lymphocytes scored in these 85 people one would expect to observe
10 or 11 dicentrics. The number of dicentrics observed was
significantly higher than the control value suggesting that the
group had been irradiated. In addition,in the person with the most
dicentrics a tricentric was observed. Dicentric yields
distribution
The majority (68 ) persons had no dicentrics in 250 cells. Nine had
1 dicentric (0.004 / cell) which falls essentially on the 95th
percentile on the population mean. Three people had 2 dicentrics
and 5 people, including one with a tricentric, had 4 dicentrics
(0.012 / cell). Matkhojl - Conclusions
Biodosimetry indicated no individual whole-body dose above0.3Gy.
The highest doses were mostly to children who played in theformer
military camp close to the radioactive sources. From the local
investigations it was impossible to reconstructprecise individual
exposures. The haematology was normal, but this would only exclude
doses >1 Gy. The biodosimetry was the most quantitative
technique possible andthe results were good news for the people
examined and moregenerally the whole population of Matkhoji.
Publications on the Georgian accidents: An IAEA book on the Lilo
event: The Radiological Accident in Lilo STI/PUB/1097, 103 pp.; 39
figures; 2000, ISBN Two journal papers: Suspicion of radiological
overexposures in Georgia (1998): The role of IPSN- P. Voisin, L.
Lebaron-Jacobs, J.-F. Bottollier-Depois and P. Gourmelon.
Radioprotection Volume 36, Numro 2, 2001. Study of the tools
available in biological dosimetry to estimate the dose in case of
accidental complex overexposure to ionizing radiation: the Lilo
accident - Roy L., Gregoire E., Durand V., Buard V., Delbos M.,
Paillole N., Sorokine-Durm I., Gourmelon P., Voisin P.. Int. J.
Rad. Biol.,1-10, 2006.