Embed Size (px)
Citation preview

Clinical Microbiology Newsletter I
Vol. 16, No. 1
Radiologic Tests for Infectious Disease Diagnosis Giles W. Boland, M.D. Department of Radiology Massachusetts General Hospital Harvard Medical School Boston, MA 02114
Advances in the microbiologic inves- tigation and diagnosis of infectious dis- ease have been paralleled in the last two decades by the rapid development of new radiologic techniques. These newer imaging modalities have signifi- cantly improved the sensitivity in the detection of the source and type of in- fection in sepsis patients. Imaging tests frequently provide the fh-st objective evidence that infection is present. Radi- ologic tests, therefore, play a key role in the diagnosis and follow-up of many infectious disease processes.
Despite the dependence of clinicians on radiologic tests for the diagnosis of infectious disease, there are no truly specific imaging techniques for infec- tions. All tests available to the radiolo- gist either detect the presence of inflammation or detect macroscopic evi- dence of disease. Although this may suggest infection, other specific disease processes may have similar appear- ances. It is therefore essential that any abnormality detected by a radiologic test be correlated with the clinical f'md- ings and results from other investiga- tions. A further caveat to the use of imaging techniques is the trend toward the use of more expensive technology when basic radiologic tests may suffice. A computed tomographic (CT) scan of the chest may identify precise pncu- monic infiltration in the lung, but a chest x ray will provide similar informa-
tion at minimal cost and inconvenience to the patient. In addition, an under- standing of the radiation doses involved in some of the newer technologies should lead to caution on behalf of the referring physician. For instance, the ra- diation dose received during a chest CT is over 1130 times that of a chest x ray (1). Therefore, the newer technologies should be applied with caution and in cases where they are likely to provide significant additional information that may alter the management of the pa- tient.
Each available imaging test has in- herent limitations in its clinical applica- bility. Imaging methods such as plain film radiography, contrast studies, CT, ultrasound, and magnetic resonance im- aging (MRI) can generally detect only macroscopic anatomical changes. Ra- dionuclide tests, in contrast, detect in- flammation even if it is not associated with structural change. This article will discuss the radiologic tests available and their applications for investigating infection in specific organs.
Radiologic Techniques For infections occurring outside the
brain, the initial radiologic test when in- dicated is the plain radiograph. Although it can provide accurate information about the type and site of infection in areas such as the chest, in other organs it is relatively insensitive--large struc- tural or destructive changes need to have occurred before an abnormality is detected. It can, however, act as a base- line measure in the follow-up of diag- nosed disease. The use of contrast agents can enhance detection and local-
l
Jammry 1, 1994
ization of infection and further define its extent. These include barium studies of the abdomen, which provide nonspe- cific evidence of infection ~ the small or large intestine; injection of water-sol- uble contrast agents into abscess cavi- ties; and intravenous and intraarterial injection of contrast agents that can pro- vide evidence of infection in areas such as the kidney or brain.
Computed tomography has trans- formed the detection and management of infectious disease processes. It can provide precise cross-sectional informa- tion about the extent and site of infec- tion and is the modality of choice for abscess detection with a sensitivity greater than 95% (2). It also provides anatomic information for planning aspi- ration or drainage (either radiologic or surgical) of abscess formation in any or- gan including the brain. The administra-
In This Issue
Radioiogic Tests for Infectious D sease V i a g u i s . . . . . . . . . . . . . . . t
How newer imaging methods such as
computed tomographic ecan, ultra- sound, magnetic resonance imaging, and radionuclide tests can enhance the diagnosis o f infection
Bacteremia Caused by TsukamureUa Species . . . . . . . . . . . . 6
A case report
CMNEEJ 16(I)14,1994 Elsevier 0196-4399/94/$0.00 ÷ 06.00

tion of intravenous contrast media may increase the sensitivity for the detection of areas of inflammation by identifying either a marked vascular component or an increase in capillary permeability into surrounding areas of inflammation.
Ultrasound allows rapid noninvasive evaluation of the patient and it is most useful in abdominal imaging, particu- larly for suspected abscess collections. However, the sound beam is attenuated by overlying air in lung and bowel and by bony structures and is therefore lim- ited for investigations within lung pa- renchyma and the brain and for deep inWaabdominal collections.
Magnetic resonance imaging (MRI) is the newest and most expensive radi- ologic test available and is most useful for detection of abnormalities in the brain or musculoskeletal system. In other areas its use is limited by motion artifact from the lung, great vessels, and bowel. Compared with other imaging modalities, it provides superior defini- tion of the extent of edema associated with infection. The administration of in- travenous contrast media can be useful in a similar fashion to contrast-en- hanced CT scans.
Scintigraphic imaging of infection rests on identification of inflammation and cannot differentiate between infec- tious and noninfectious inflammatory disease. However, radiouuclide studies are generally more sensitive than other imaging modalities at detecting infec- tion because they depend on white cell migration or changes in blood flow or permeability to show inflammation. The distribution of radioisotope paral- Iris the acute inflammatory response as- sociated with infection and tends to he greater in acute sites of inflammation than in areas of chrouic inflammation. This high sensitivity is the chief strength of nuclear imaging. It is par- ticularly helpful in the detection of in- fection in a patient with a fever of
unknown origin because it then directs attention to that region. To arrive at a meaningful clinical diagnosis, the site of the inflammation must then be corre- lated with an anatomic structure that may require additional imaging modali- ties such as CT or MRI. Radioisotopes available include 67Gallium, which af- ter injection binds to circulating pro- teins (3) and is rapidly localized in areas of inflammation through in- creased capillary permeability. Leuko- cytes can be labeled with radioisotopes, and if there is marked white cell migra- tion into a region of infection, radiola- beled white cells will provide a pictorial representation of the inflamma- tory response. White cells axe usually labeled with indium- 111 although 99mTechnetium-HMPAO-labeled white cells have recently been investigated but the ultimate role of this method is still uncertain. Finally, radionuclide-la- heled antibodies to bacteria have been investigated. Only indium-111-labeled IgG has proved useful and further stud- ies are awaited.
Radiologic Imaging of Infections in Specific Organs
The Brain There have been extensive recent re-
ports as to the radiologic manifestations of HIV in the brain. In HIV encephali- tis, CT and MR scans may be normal or show atrophy or white matter lesions. White matter lesions are hypodense on CT or hyperintense on T2-weighted MR images reflecting edematous changes. Normal MR scans are much more com- mon in neurologically intact patients than in those with neurologic symptoms (87% versus 54%) (4). Symptomatic pa- tients had more white matter lesions in- volving a larger area of the brain and involving infratentorial portions of the brain (4). Early recognition by MRI of HIV encephalitis is, however, diffieult at present and it is generally accepted
that radiologic findings lag behind clini- cal fmdings. Radioiogic findings that suggest demyelination are thought to be the result of a secondary inflammatory reaction to the basic pathological proc- ess of microglial nodule formation.
The CT evaluation of HIV encephali- tis is less sensitive than MRI, but AIDS patients show significantly enlarged ventricles and a trend toward sulcal en- largement compared with healthy con- trol patients (5). In HIV-positive patients who do not have AIDS, focal lesions are found only in patients with focal neurologic signs or symptoms. Nonfocal clinical findings are associ- ated with either a normal CT scan, hy- drocephalus, or atrophy (6). MRI is generally considered the best imaging method for examining AIDS patients with possible intracranial disease. A re- cent study has shown that MRI was 44% more sensitive than CT at detect- ing AiDS-related abnormalities (7).
Other AIDS-related opportunistic in- fections are also more readily detected by MRI than CT. MR scans of patients with Cryptococcus neoformans can identify mass lesions (cryptococcoma), mihary disease, leptomeningeal nod- ules, and distention of Virchow-Robin spaces. Up to 50% of HIV patients will develop spinal cord infections with cy- tomegalovirus and herpes simplex vi- rus. These infections can cause abnormal enhancement on CT and MR scans, although MRI is usually more sensitive.
Bacterial infectious in the brain can manifest through meningeal involve- ment that can be detected by meningeal enhancement on CT- and MR-enhanced scans. Infectious aneurysms associated with meningitis, bacterial endocarditis, or fungal infection can be detected by angiographic studies. In patients not un- dergoing surgery, repeated studies are usually required to follow the progress of such lesions (8). Brain abscesses are
NOTIg: No n~spousibility is assumed by the Publisher for any injury and/or damage to pemorm or propmty as a matter of products liability, negligence or otherwise, or from any me or operation of aay methods, products, instructions or ideas contained in the mate~al bemin. No enuested test or prcoedme should be carried oat unless, in the reader's judgment, its risk is justified. Became of rapid advances in medical sciences, we recommend th~ the independ•t verification of diagnoses end drag dosages should be made. Discussions, views, and recommendations as to medical procedures, choice o f d m ~ and dm 8 dosages arc the responsibility of the authors.
Ch'~cal Microbwlogy Nm, e/ctl~" (ISSN 0196-4399) is issued twice monthly in one indexed volume per year by Elsevi~ Science Inc., 655 Avenue of the Americas, New York, NY 10010. Sub~ription pt~e per year:. $155.00 including p~tage rout handling in the United States, Cmmde, and Mexico. Add $59.00 for pcetage in the rest of the world. Scared-chum pmtMe paid at New York, NY and at additional mailing o f f i ~ . Postmaster:. Send address changes to Cfinicai Microblolo&y NewMef;er, Elsevier Science Inc., 655 Avenue of the Americas, New York, NY 10010.
2 01964399/94/~.00 + 06.00 © 1994 Elsevier Science Inc. Clinical Microbiology Newsletter 16:1,1994

readily identified on both CT and MRI scans. On CT they show a hypodense center with smooth thin walls that strongly enhance after adminisW~on of intravenous contrast Metastatic disease and lymphoma can give similar appear- ances. Indium-I I 1-1abeled white cell scans have been shown to have a high degree of specificity for the detection of brain abscesses and can be per- formed when a differentiation of ab- scess from neoplasm cannot be made by either CT or MRI.
Use of enhanced CT in the evalu- ation of tuberculosis of the brain has identified meningeal involvement in 18% of cases, pure parenchymal in- volvement in 71%, and mixed men- ingeal involvement in 1 I% (9). Parenchymal tuberculosis can be subdi- vided into parenchymai and granuloma- tons disease and tuberculous abscess. The former is more common and is characterized by edema surrounding an area of ring enhancement with irregular walls on intravenous contrast-enhanced CT or by solid enhancement. Tubercu- lous abscesses, which can be single or multiloculated, have alvemances identi- cal to pyogenic abscesses on CT scans.
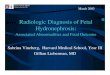
Parasitic infections, such as neuro- cysticercosis, may show enhancement on MR imaging (Figure 1) following gadolinium administration, with edema identified on T2-weighted images. Larva that are still alive do not produce a host reaction, produce little edema, and in general do not enhance. MR has been shown to be more sensitive than CT scanning at detecting amebic (Enta- moeba histolytica) infection with thick- walled enhancement in some patients and nodular enhancement in others. CT and MRI studies can detect fungal infec- tions, including aspergillosis, blastomy- cosis, and histoplasmosis. The appear- a n o n , h o w e v e r , a r e US~mlly nonspec i f i c .
The Chest The mainstay for detecting infection
within the chest is still the chest x ray. Plain radiographs identify most disease processes, including pneumonia, lung abscess, empyema, and med_~inal ab- scess. The hallmark of exudative infec- tions in the chest x ray is air-space disease chaxaeterized by bronchi out- lined by opacified alveoli f'dled with
Figure 1.Axial MRI of the head. This demonstrates multiple lesions throughout the brain (arrow) in a patient with diffuse headache. These lesions were a result o f toxoplasmosis.
exudative material. However, other dis- ease processes such as pulmonary edema and lymphoma can produce simi- lax appearances and therefore the find- ings must be taken in clinical context. Although CT is more sensitive than the chest x ray in identifying air-space dis- ease, the patient will usually present af- ter readily identifmble changes are visualized on the chest x ray. However, some opportunistic infections may pre- sent with nonspecific clinical disease and without overt changes on the chest x ray. In these circumstances, a Cl" scan of the chest, although not routinely indicated, may identify changes not vlsnaliTed by chest x ray, including air- space disease, "ground glass" appear- ances, an interstitial pattern, and a "patchwork pattern" of air-space and in- terstitial disease (10).
CT can provide additional informa-
tion beyond plain radiography in the evaluation of lung abscess. These in- clude delineation of pleural-abscess re- lationships, characterization of paxenchymal consolidation, visualiza- tion of internal contents of the abscess, improved visualization of vessels, and enhanced resolution of these abnormali- ties. CT is of particular benefit in differ- entiating lung abscess from empyema. Abscesses tend to be round and demon- strate thick, irregular walls. Bronchi and pulmonary vessels terminate abruptly at the advancing wall of an ab- scess and are not compressed or dis- torted (11). Empyemas, in contrast, have lenticular shapes surrounded by a fibrin peel that forms the basis for the most reliable radiographic feature of an empyema, which has been called the "split pleura" (11) sign.
Radionnclide studies age generally
Clinical Microbiology Newsletter 16:1,1994 © 1994 Elsevier Science Inc. 01964399/94/$0.1)0 + O6.OO 3

Figure 2. Axial CT scan of the lower pelvis demonstrating an abscess posteriorly (arrow). This patient had undergone an abd~maino-perineal resection 6 d previously and now presented with recurrent fever.
not helpful in detecting lung infection but are particularly useful in the evalu- ation of acute diffuse pneumonia such as Pneumocystis carinii infection. This and other opportunistic infections may cause either focal or diffuse uptake in the lung. The chest x ray is normal in the early stages at a time that gallium scanning reveals profound disease. An abnormal gallium scan in an immuno- compromised patient with pulmonary symptoms is good evidence for infec- tion. Unfortunately, this may not be suf- ficient information to institute treatment because there are many potentially pathogenic microorganisms, each of which requires a different antlmicrobial regimen. Additional diagnostic studies such as bronchoscopy are often neces- sary.
Ultrasound, although of no benefit for parenchymal lung disease, readily identifies pleural collections resulting from pneumonia. Ultrasound is ideal for providing image-guidance needle aspi- ration when secondary infection of a Imrapneumonic effusion is suspected. CT further defines the extent of em- pyema and is usually required for fol- low-up observation after surgical or radiologic drainage.
The Abdomen Plain films of the abdomen can sug-
gest the location of an abscess in up to 50% of cases (12). These films may be of less value in the immediate post-op-
i
4 0196-4399/94/$0.00 + 06.00
erative period if a paralytic ileus with excessive bowel gas creates confusing patterns. The cardinal plain film feature of an abscess is an extraluminal, abnor- mal gas collection. Less common find- ings include reactive pleural effusion or elevation of the diaphragm or a mass may be detected if it causes displace- ment of adjacent bowel loops. How- ever, many of these signs may be appreciated only in retrospect. In addi- tion, once an abscess is identified, fur- ther imaging studies are usually required to def'me it more clearly. A contrast study is particularly useful in detecting a suspected abscess that has originated from a perforation of the gas- Ilointestinal tract. Studies must usually be performed with water-soluble con- trast media rather than barium because extravasation of barium is higMy toxic to the peritoneum, with up to a 50% mortality resulting from barium-induced peritonitis. Furthermore, barium will degrade subsequent CT examinations whose result is probably more useful than that of the contrast study.
Ultrasound is of particular benefit in the evaluation of abdominal abscesses in the upper abdomen and pelvis where air-filled bowel is less likely to attenu- ate the sound beam. The liver provides a window for the evaluation of intra- hepatic, perihepatic, and subphrenic fluid collections. Similar appearances can be identified in the spleen. The kid-
© 1994 Elsevier Scim-,ce lnc.
neys can be clearly identified using the liver or spleen as windows and anatomic changes resulting from ab- scess formation can be identif~L In the mid-abdomen, ultrasound is generally effective only if an abscess cavity lies against the abdominal wall. In the pel- vis the urine-filled bladder provides an ideal sonic window with over 90% sen- sitivity for the detection of pelvic ab- scesses (13). Abscesses generally appear as round or oval fluid collec- tions that are generally hypoechoeic but frequently contain internal echoes, al- though the pattern may range from com- pletely anechoeic to highly echogenic (2). Gas-filled abscesses may be diffi- cult to identify, although abscesses that contain multiple small bubbles will be identified as multiple small echogenic foci, creating a coarse echogenic pnt- tern. The apIrarance of an abscess on ultrasound is nonspecific because any fluid collection within the abdomen could give similar appearances. There- fore, as with all radiologic tests, de- tected abnormalities should be correlated with clinical findings.
CT is the primary modality for ab- scess detection within the abdomen, with reported sensitivity over 95% (2). The CT scan (Figure 2) must be planned and conducted so that it will provide the diagnostic information re- quired. The bowel must be opacified with oral/rectal contrast because
Clinical Microbiology Newsletter 16:1,1994
?

unopacified bowel can have an appear- ance similar to that of an abscess. Addi- tional information may be acquired because the CT scan images the entire abdomen, including soft tissues and bone. The CT signs of an abscess in- clude a well-defined area of low attenu- ation, obliteration of surrounding fat planes, extraluminal gas collections, and displacement of surrounding vis- cera (2). Infection without abscess for- marion can be identified as an area of edema within the fat planes, which is more specific if localized to an area of suspected infection. Occasionally, ad- ministration of intravenous contrast may increase the sensitivity for abscess detection by delineating an enhancing rim to an abscess due to the intense vas- cular supply to the wall of the abscess.
Radionuclide imaging in the abdo- men plays a role only when other imag- ing m~aliries fail to show an abnor- mality. Gallium scanning, which detects most significant abdominal collections, is nonspecitic and is readily excreted into normal bowel. Administration of indium-11 l-labeled leukocytes has an advantage because they are not nor- really excreted into the bowel. Other than that of the liver or spleen, there should be no activity within the normal abdomen or pelvis. After CT scanning, indium-11 I-labeled leukocyte imaging is probably the radiologic investigation of choice for the detection of an occult abdominal infection (Figure 3).
The Muscuioskeletal System Plain films are us~mlly the initial di-
agnostic study used for the investiga- tion of osteomyeliris. If deep, soft tissue swelling, periosteal reaction, cortical ir- regularities, and demineralization sag- gest osteomyelitis, additional studies may not be required. However, it may be 3 to 4 wk before plain films show evidence of disease, by which rime ex- tensive destruction may have occurred. Therefore, if clinical suspicion of acute osteomyelitis is present, additional im- aging tests will be required. CT can demonstrate almormalities earlier than plain bone films and is particularly use- ful in the spine, pelvis, and sternum, which are difficult to visnalize on the plain film. Early findings include in- creased marrow density and surround-
Figure 3. Radionucleide study showing an ab- scessin the right lower quadrant (arrow) in a patient with Crohn's disease.
ing soft tissue edema. Chronic osteo- myelitis shows sclerosis, demineraliza- tion, periosteal reaction, and sequesca (14). However, as with plain films, the diagnosis of active infection is difficult or impossible with CT. MRI is inher- ently more sensitive than CT for mar- row and soft tissue abnormalities. Active osteomyelitis is identified by a decreased signal on Tl-weighted im- ages and a bright or increased signal on T2-weighted images, which represents replacement of marrow fat with water secondary to edema, exudate, hypere- mia, and ischemia (14). Findings on MRI appear much earlier in the course of the disease than on CT or plain films and reported sensitivities approach 95% (15). MRI is of particular value in ex- amining the spine where osteomyelitis shows a characteristic pattern of conflu-
ent vertebral body and disk involve- ment. However, MRI signal charac- teristics that reflect osteomyeliris are intrinsically nonspecif'lc as tumors, frac- tures, and a variety of inCa- or extra- medullary inflammatory processes can show similar appearances (14). In addi- tion, the diagnostic sensitivity of MRI is fimited by the presence of a metal prosthesis and is a cosily technique. For these reasons, the initial diagnostic im- aging study may remain the conven- tional planar bone scan.
The overall sensitivity of conven- tional bone scan performed with in- jected 99~Technetium-MDP approaches 100% (14) and most nuclear medicine practitioners would argue that a nega- tive bone scan in an otherwise healthy adult essentially rules out bone infec- tion. A conventional bone scan is the first radiologic test that will detect evi- dence of osteomyelitis, often within the first few days of the disease. With the recent addition of single photon emis- sion computed tomography (SPECT) imaging, it is possible to image in the axial plane, similar to a CT scan, which therefore improves spatial resolution and may increase sensitivity. Classi- cally, osteomyelitis presents as a region of increased blood flow and appears as an area of increased tracer activity on initial blood flow (dynamic) and on de- layed (equilibrium) images. Photopenic defects are less common but may repre- sent osteomyelitis, particularly in the early stages. Positive bone scans, al- though extremely sensitive, are rela- tively nonspecific, and thus gallium scanning and indium-111 scanning are sometimes used. There is tittle normal white cell accumulation in noninflam- matory regions of increased bone turu- over. This contrasts sharply with gallium imaging and lxovides a real ad- vantage in patients with complicated or- thopedic problems. Indium- 111 scanning is therefore more commonly applied in the search for osteomyeliris in previously traumatized bone and ad- jacent to joint prostheses. Indium-leuko- cyte scanning is also useful in the evaluation of celluliris and suspected soft tissue abscesses and is useful to dis- tinguish between cellulitis alone and osteomyelitis with overlying soft tissue
Clinical MierobiololD' Newsletter 16:1,1994 © 1994 Elsevier Science Inc. 0196-4399/94/$0.00 + 06.00 5

infection. This is a common problem in the diabetic foot, particularly in regions overlying neurolmthic joints. Unfortu- nately, the limitations of s ~ ' a l resolu- tion may obscure the distinction between bone and soft tissue and correlation with conventional radiographic studies and clinical findings are required.
Conclus ion A variety of radioiogic tests are
available to the physician for the diag- nosis and follow-up of infection. Each tests has its merits and limitations and should be tailored to the diagnosis in question. Abnormal findings are often nonspecific and should always be corre- lated with clinical disease. Recent ad- vances in radiologic technology have improved the sensitivity for detection of disease but problems of cost, r~iia- tion dosages, and availability continue to limit their applicability. For these rea- sons, the plain radiograph will con- tinue to be the initial radiologic examination in most cases. Further im- aging should be performed if the plain film identifies a nonspecific abnormal- ity or if the clinical index of suspicion is h igh.
References 1. Mayo, J. R., S. A. Jackson, and N. L.
Muller. 1993. High resolution CT of the chest: radiation dose. A JR 160:479-481.
2. Gerzof, S. G. and M. E. Oates. 1988. Imaging techniques for infections in the surgical patient. Surg. Clin. North Am. 68:147-165.
3. Palmer, E. L., J. A. Scott, and H. W. Strauss. 1992. Chapter 9, p. 343-364. In: Practical nuclear medicine. 1st edi- tion. WB Saunders Company, Philadel- phia.
4. Post, M. J. D., J. R. B~ger, and R. M. Quencer 1991. Asymptomatic and neurologically symptomatic HlV-posi- tive individuals: prospective evaluation with cranial MR imaging. Radiology 178:131-139.
5. MoeUer, A. A. and H. C. Backmund. 1990. Ventricle brain ratio in the clini- cal course of HIV infection. Acta Neurol. Scand. 42:164-165.
6. Rauch, R. A., C. Bazan, and J. R. Jink- ins. 1992. Imaging of infections of the central nervous system. Curr. Opin. Ra- diol. 4:43-51.
7. McArthur, J. C. et al. 1989. Low preva- lence of neurological and neuropsy- chological abnormalities in otherwise healthy HIV-I infection: association with AIDS-related complex but not asymptomatic HIV-1 infection. Ann.
Neurol. 26:582--600.
8. Barrow, D. L. and A. R. Prats. 1990. In- fectious intracranial aneurysms: com- parison of groups with and without endocarditis. Neurosurgery 27:562-573.
9. Jinkins, J. R. 1991. Computed tomogra- phy of intracranial tuberculosis. Neuroradiology 33:126-135.
10. Kuhlman, J. E. et al. 1990. Pnewnocys- tis carinii pneumonia: spectrum of parenchymal CT findings. Radiology 175:711-714.
11. Stark, D. D., M. P. Federle, and P. C. Goodman. 1983. Differentiating lung abscess and empyema: radiography and computed tomography. A JR 141:163-167.
12. Conneil, T. R. et al. 1980. Upper ab- dominal abscesses: a continuing and deadly problem. AJR 134:759-765.
13. Taylor, K. J. W. et al. 1980. Accuracy of gray scale ultrasound diagnosis of ab- dominal and pelvic abscesses in 220 pa- tients. Lancet 1:83-84.
14. Wegener, W. A. and A. Alavi. 1991. Di- agnostic imaging of musculoskeletal in- fection. Orthoped. Clin. North Am. 22:401-418.
15. Schauwecker, D. S., Braunstein, and E. M., L. J. Wheat. 1990. Diagnostic imag- ing of ostcomyelitis. Infect. Dis. Clin. North Am. 4:441-463.
C a s e R e p o r t
Bacteremia Caused by Tsukamurella Species
Carla Clausen, Ph.D. Department of Laboratories Children's Hospital and Medical Center Seattle, WA 98105
Carolyn K. Wallis, R.M.(AAM) Department of Laboratory Medicine Harborview Medical Center University of Washington, Seattle, WA 98104
The patient, a 5-yr-old female, had received an muelatod bone marrow transplant 5 mo after a diagnosis of
acute myelogenous leukemia. Her clini- cal course after transplantation was complicated by graft versus host dis- ease and cytomegalovirus (CMV) gas- troenteritis. After discharge from the hospital, her health had been stable for about 2 mo when she developed fever, nausea, vomiting, diarrhea, and abdomi- nal pain. Her private physician obtained blood for culture ~ h the Hicknum catheter and began treatment with oral ~ - s u i f a m e t h o x a z o l e (TMP-
SMZ) . Her symptoms persisted over the next 2 d and she was therefore admitted to the hospital.
On admission, the patient had a tem- perature of 39.5"C, a while blood count of 5700/ram 3 with 7% p o l e - clear leukocyte, and slisht toxic granu- lation. Blood for cullme was drawn through a periphend vein, and empirical treatment with ceftazadime and gen- tamicin was begun. Later on the day of admission, a report was received that
6 01964399/94/$0.00 + 06.00 © 1994 Elsevier Science Inc. Clinical Microbiology ~ r 16:1.1994