Embed Size (px)
Citation preview

Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Radiologic Diagnosis of Radiologic Diagnosis of Thoracic Aortic AneurysmsThoracic Aortic Aneurysms
Patricia Tung, Harvard Medical School Year III
Gillian Lieberman, MD
2
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
BackgroundBackground
Incidence 6 cases per 100,000 patient years– Less common than AAA– Incidence increasing over last 30 years
Typically 6th-7th decadeMales 2-4 x > than femalesFamilial predispositionExpand less rapidly than AAA

3
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Risk FactorsRisk FactorsAtherosclerosisCT disordersInfection: salmonella, staph aureus, syphilisBicuspid Ao valve and coarctation => post-stenotic dilatationTrauma: deceleration injuriesTakayasu’s and Giant Cell arteritides

4
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
PathophysiologyPathophysiologyAtherosclerosis– Proteolytic factors in inflammatory plaques destroy
elastin and collagen, weakening vessel wallCystic medial degeneration – Elastic tissue fragmentation– Separation of elastic and muscular elements of media
by amorphous ECM– Provides substrate for HTN and other insults
5
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Categorization of TAA: by Categorization of TAA: by locationlocation
Ascending: Ao valve to innominate arteryArch: involving any of the branch vesselsDescending: distal to the left subclavianartery

6
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Complications of TAAComplications of TAARupture – universally fatal except in rare cases of containmentEmbolization – stroke, infarctDissection – stroke, infarct, renal failure, paralysisSepsis – undetected mycotic aneurysms and pseudoaneurysms
7
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
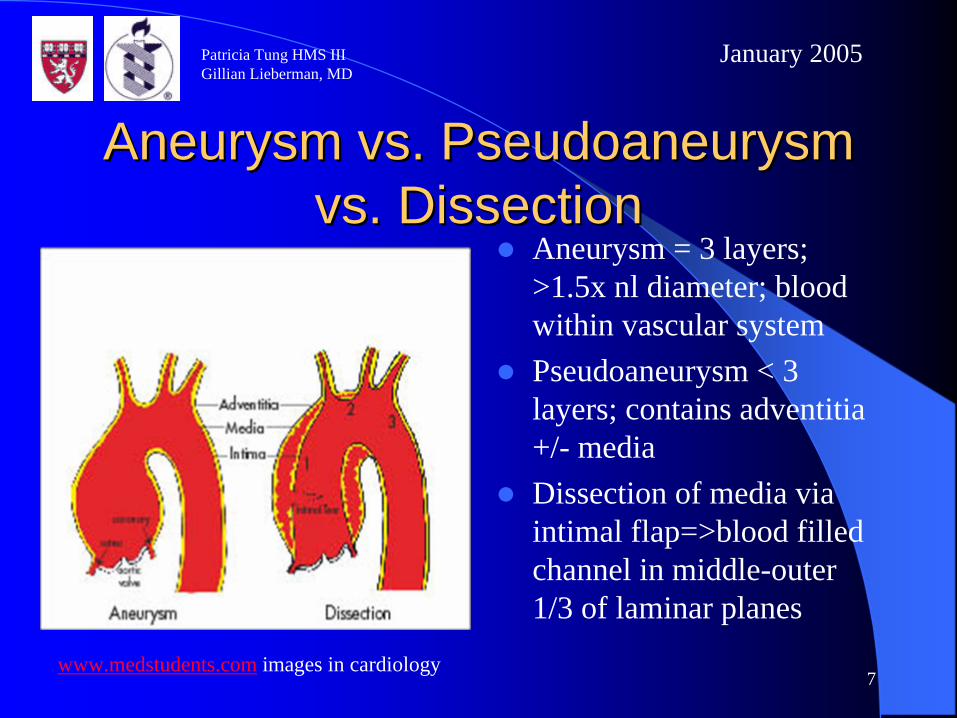
Aneurysm vs. Aneurysm vs. PseudoaneurysmPseudoaneurysm vs. Dissectionvs. Dissection
Aneurysm = 3 layers; >1.5x nl diameter; blood within vascular systemPseudoaneurysm < 3 layers; contains adventitia +/- mediaDissection of media via intimal flap=>blood filled channel in middle-outer 1/3 of laminar planes
www.medstudents.com images in cardiology

8
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
TreatmentTreatment
Size = 1° determinant of rupture; uncommon <5cm or expansion <1cm/yearSurgery if >5.5 cm or sxUntx TAA>6cm => risk rupture or dissection 6.9%, death 11.8%/year (Davies et al).
Perko et al. Unoperated Aortic Aneurysms: A Survey of 170 Patients. Ann Thorac Surg 1995; 59; 1204-9.
Survival for Untx TAA, T/AAA, AAA

9
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Clinical PresentationClinical PresentationAsx in absence of expansion or bleedingSx related to mass effect or circulatory compromiseUp to 13% patients have multiple aortic aneurysms
=>Most commonly detected as incidental finding on plain film

10
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
CXR: Radiologic FindingsCXR: Radiologic Findings
Not used for diagnosisAortic silhouette abnormal 80-90% cases– Diffuse widening mediastinum– Mediastinal mass– Pleural effusion– Displacement of NG tube to the right– change in aortic contour over time**

11
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
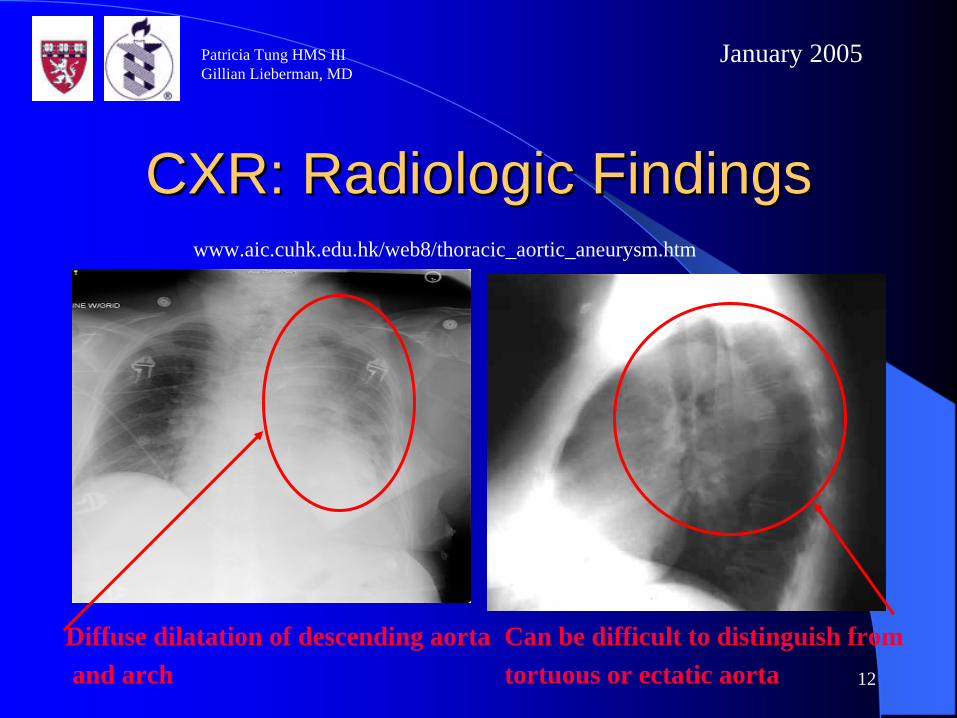
CXR: Radiologic FindingsCXR: Radiologic FindingsAneurysm seen as mediastinal mass adjacent to aortaCan be indistinguishablefrom 1° lung cancer
www.aic.cuhk.edu.hk/web8/thoracic_aortic_aneurysm.htm
12
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
CXR: Radiologic FindingsCXR: Radiologic Findings
Diffuse dilatation of descending aortaand arch
Can be difficult to distinguish from tortuous or ectatic aorta
www.aic.cuhk.edu.hk/web8/thoracic_aortic_aneurysm.htm

13
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
CXR: TAA RuptureCXR: TAA RuptureWidened mediastinumRight hemothoraxChange in aortic contour compared to previous CXR
www. Health.all-refer.com
=>With high clinical suspicion, more sophisticated study needed to confirm dx and size determination

14
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Primary Diagnostic ModalitiesPrimary Diagnostic Modalities
AortogramCT/CTAMRI/MRATEE
15
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
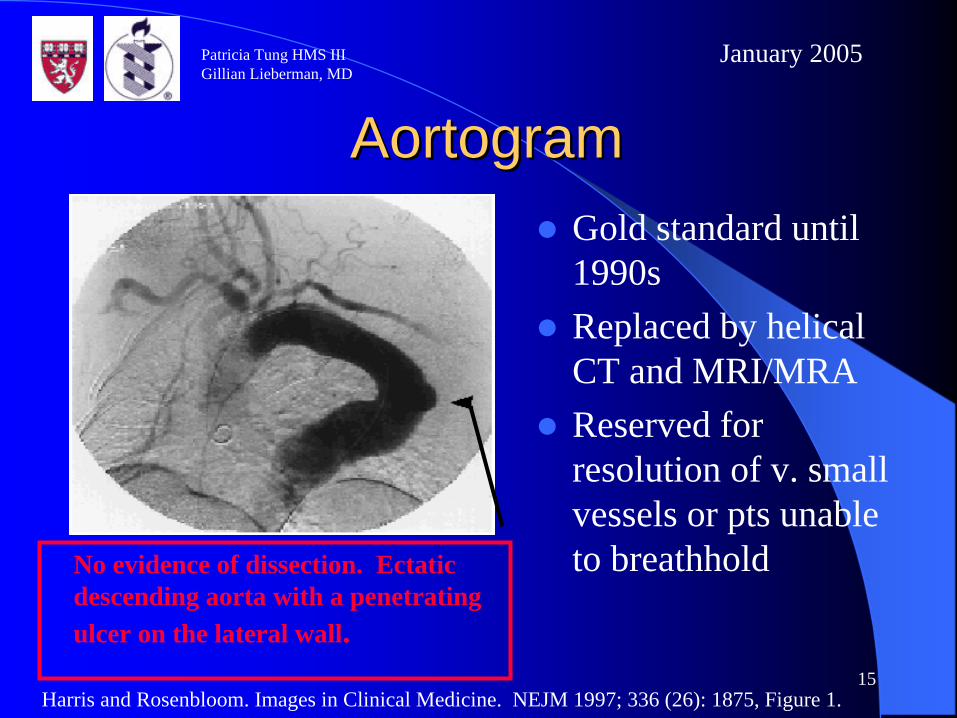
AortogramAortogramGold standard until 1990sReplaced by helical CT and MRI/MRAReserved for resolution of v. small vessels or pts unable to breathholdNo evidence of dissection. Ectatic
descending aorta with a penetrating ulcer on the lateral wall.
Harris and Rosenbloom. Images in Clinical Medicine. NEJM 1997; 336 (26): 1875, Figure 1.

16
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
CT: Descending Aortic AneurysmCT: Descending Aortic AneurysmBest for emergent settingsWidely available, less expensive than MRIDelineates morphology, pattern, distribution of thrombus and calcification
Harris and Rosenbloom. Images in Clinical Medicine. NEJM 1997; 336 (26): 1875, Figure 1.

17
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
CT: Additional BenefitsCT: Additional BenefitsHyperdensityidentifies acute injury Visualization of dissection and intimal flap
PACS, BIDMC

18
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
MRIMRIShows lumen and vessel wall; best assessment of true size Excellent vessel anatomy and surrounding structuresLeast renal toxicityTime consuming; not for unstable patients
www.medstudents.com images in cardiology

19
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
MRAMRA3D Gado MRA shows blood flowCINE imaging gives functional assessment of Ao valve; can show intimal flapDoes not visualize adventitia well
=>Differences in treatment make visualization of entire aorta critical.
home.earthlink.net/~radiologist/tf/060302.htm

20
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
MRI Coronal View: MRI Coronal View: Ascending Aortic AneurysmAscending Aortic Aneurysm
PACS, BIDMC
Signal loss in ascending aorta c/w stenosis
Aneurysmal dilatation 4.6 x 4.1 cm at main PA
Smooth dilatation
No lumenal irregularity
No coarctation
21
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
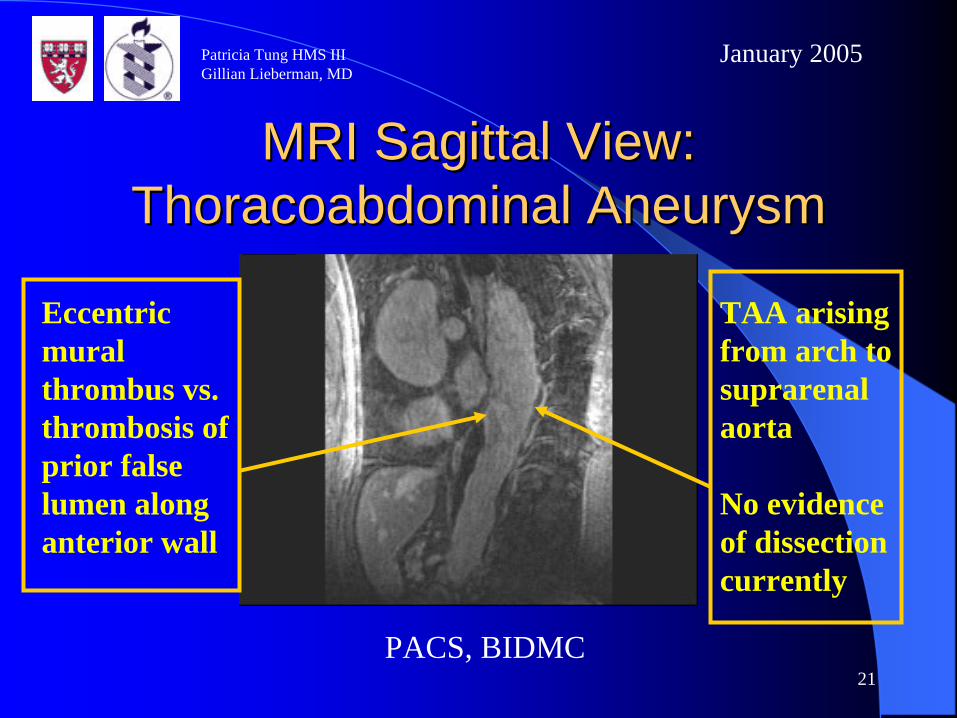
MRI MRI SagittalSagittal View: View: ThoracoabdominalThoracoabdominal AneurysmAneurysm
PACS, BIDMC
TAA arising from arch to suprarenal aorta
No evidence of dissection currently
Eccentric mural thrombus vs. thrombosis of prior false lumen along anterior wall

22
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
MRI: MRI: ThoracoabdominalThoracoabdominal AneurysmsAneurysms
PACS, BIDMC
Tortuous descending aorta
Infrarenal aneurysm
Multiple bilateral renal cysts
1.5 cm cyst left lobe liver
23
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
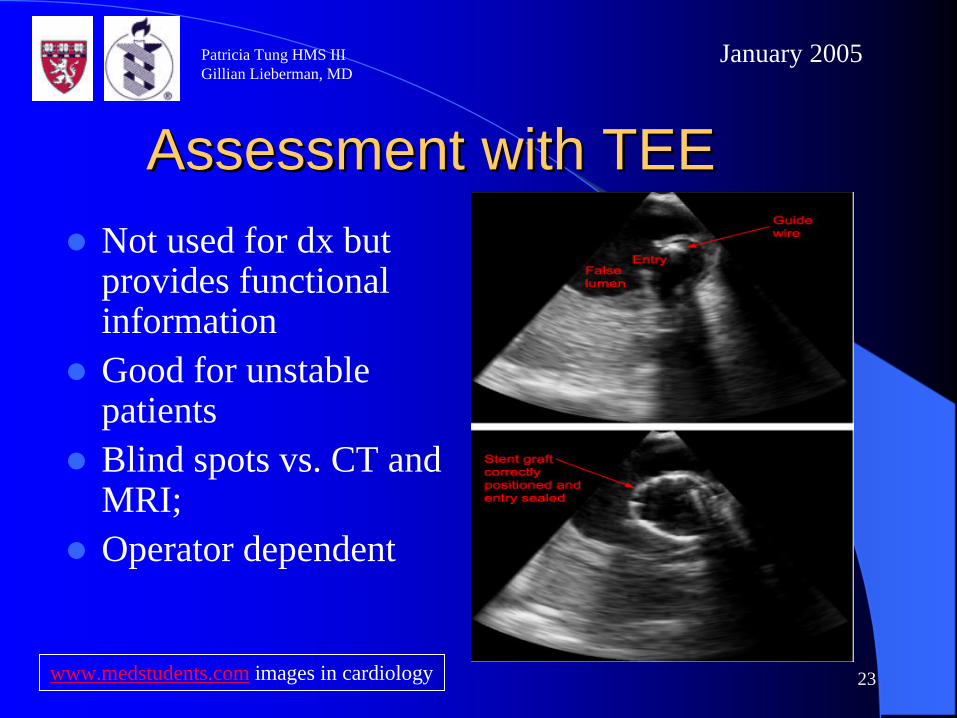
Assessment with TEEAssessment with TEENot used for dx but provides functional informationGood for unstable patientsBlind spots vs. CT and MRI; Operator dependent
www.medstudents.com images in cardiology

24
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
TEE: Radiologic FindingsTEE: Radiologic Findings
Harris and Rosenbloom. Images in Clinical Medicine. NEJM 1997; 336 (26): 1875, Figure 1.
Severe atherosclerosisMildly enlarged descending aortaEccentric thickening of one wall Echogenicity consistent with thrombus or IMH
25
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Patient J.D.Patient J.D.
77 year old male with chest discomfort, pressure between scapulae and hoarsenessPMH: COPD, prior asbestos exposure, PVD, HTNPSH: s/p aortobifemoral bypass graftElevated creatinine

26
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
ContrastContrast--enhanced CT at enhanced CT at PresentationPresentation
Disruption of inferior wall of aortic arch c/wpseudoaneurysm or contained ruptureAdjacent mediastinalhematomaPleural plaques c/wasbestos exposure
PACS, BIDMC

27
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
ContrastContrast--enhanced CT at enhanced CT at PresentationPresentation
Disruption of inferior wall of aortic arch c/wpseudoaneurysm or contained ruptureAdjacent mediastinalhematoma
PACS, BIDMC

28
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
ContrastContrast--enhanced CT 3 Days enhanced CT 3 Days LaterLater
PACS, BIDMC
Increased size of mediastinal hematoma adjacent to pseudoaneurysmIncreased pleural effusion, possible subacute hemothorax

29
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Take Home PointsTake Home PointsHelical CT gives rapid assessment of major pathology; good for:– Acutely symptomatic– Question of additional thoracoabdominal pathology
MRI gives excellent detail; good for: – Asymptomatic and hemodynamically stable– Surgical planning– Patient contraindications
30
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Take Home Points (cont’d)Take Home Points (cont’d)
TEE good for functional assessmentNon-angiographic modalities best for assessing non-lumenal anatomy
31
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
ReferencesReferencesRubin GD. CT Angiography of the Thoracic Aorta. Seminars in Roentgenology 2003 April; 38(2): 115-133.Miller, WT. Thoracic Aortic Aneurysms: Plain Film Findings. Seminars in Roentgenology 2001 Oct; 36(4): 288-294.Roberts, DA. Magnetic Resonance Imaging of Thoracic Aortic Aneurysm and Dissection. Seminars in Roentgenology 2001 Oct; 36(4): 295-308.Nguyen, BT. Computed Tomography Diagnosis of Thoracic Aortic Aneurysms. Seminars in Roentgenology 2001 Oct; 36(4): 309-324.Scott CH, Keane MG, Ferrari VA. Echocardiography Evaluation of the Thoracic Aorta. Seminars in Roentgenology 2001 Oct; 36(4): 325-333.Soulen MC. Catheter Angiography of Thoracic Aortic Aneurysms. Seminars in Roentgenology 2001 Oct; 36(4): 325-339.Marx, Hockberger, Walls. Rosen’s Emergency Medicine, 5th edition. Vol (1); 406.Davies RR et al. Yearly Rupture or Dissection Rates for TAA: Simple Prediction Based on Size. Ann Thorac Surg 2002 Jan; 73(1): 17-27.
32
Patricia Tung HMS IIIGillian Lieberman, MD
January 2005
Many thanks to:Many thanks to:
Atif Zaheer, MDGillian Lieberman, MDPamela LepkowskiLarry Barabas, our Webmaster