Embed Size (px)
Citation preview

Inr. J. Radiation Onco/ogv Biol. Phys.. Vol. 7. pp. 1695-I 701 03~3016/81/121695~7~2.~/0
Printed in the U.S.A. All rights rcscrved. Copyright 0 198 I Pergamon Press Ltd.
0 Oncology Intelligence
RADIOBIOLOGICAL BASIS OF TOTAL BODY IRRADIATION WITH DIFFERENT DOSE RATE AND FRACTIONATION: REPAIR CAPACITY OF
HEMOPOIETIC CELLS
CHANG W. SONG, PH.D., TAE H. KIM, M.D., FAIZ M. KHAN, PHD., JOHN H. KERSEY, M.D. AND SEYMOUR H. LEVITT, M.D.
University of Minnesota Medical School, Box 494 Mayo, Minneapolis, MN 55455
Total body irradiation (TBI) followed by bone marrow transplantation is being used in the treatment of malignant or non-malignant hemopoietic disorders. It has been believed that the ability of hemopoietic cells to repair sublethal radiation damage is negligible. Therefore, several school of investigators suggested that TBI in a single exposure at extremely low dose rate (5 rad/min) over several hours, or in several fractions in 2-3 days, should yield a higher therapeutic gain, as compared with a single exposure at a high dose rate (26 rad/min). We reviewed the existing data in the literature, in particular, the response of hemopoietic cells to fractionated doses of irradiation and found that the repair capacity of both malignant and non-malignant hemopoietic cells might be greather than has been thought. It is concluded that we should not underestimate the ability of hemopoietic cells to repair sublethal radiation damage in using TBI.
Total body irradiation, Dose rate, Bone marrow transplantation, Hemopoietic stem cells, Leukemia.
Total body irradiation (TBI) followed by bone marrow transplantation is becoming an established modality in the treatment of malignant or non-malignant hemo- poietic disorders.2’,22.38 In the past, the most commonly used protocol for TBI was exposing patients to 1000 rad in a single dose at dose rate of 5-8 rad/min using a 6oCo radiotherapy unit.” It should be stressed that the use of such a low dose rate was not based on a radiobiological foundation, but it was the maximum dose rate that could be obtained from the conventional @‘Co unit. Delivery of 1000 rad at this low dose rate requires an arduous task of several hours and has a number of disadvantages. Because the already sick patients develop radiation syndrome during the treatment, the radiation process should be interrupted frequently. In addition, occupying a radiation source for several hours in the usual radio- therapy department severely restrains routine work. Since high dose rate machines, such as linear accelera- tors, became available, several medical centers have been using high dose rates to minimize the inconvenience imposed on the patient and to avoid the great ado with TBI for several hours at low dose rate.*‘***
Based on our animal experiments on the TBI with @Co and 10 MV X rays at different dose rates for bone marrow death,” we at the University of Minnesota devised a protocol in which the patients are irradiated
with 750 rad of 10 MV X rays at a midline dose rate of 26 rad/min in a single exposure. With this protocol, TBI can be completed within 30 min.
Presently, dose rates ranging from 2.5 rad/min to 45 rad/min are being used for TBI in a single or fraction- ated dose at various medical centers.22 The clinical effect of different TBI protocols has been a controversial subject in recent years. Several groups of investiga- tors23*24*26*29.30 have stated that the capacity of bone marrow stem cells and malignant hemopoietic cells (which are the targets of TBI) to repair sublethal radia- tion damage is quite limited as compared with that of other mammalian cells. It was concluded, therefore, that TBI in a single dose at a low dose rate (5-8 rad/min) or in fractions should yield a greater therapeutic gain when compared with single dose TBI at high dose rate (26 rad/min)*3v26-29,30 In support of their contention, the report by McCulloch and Til127 that the radiation survival curve of colony forming units (CFU) from mouse bone marrow had an extrapolation number (n) and quasithreshold dose (Dq) of 1.5 and 50 rad, respectively, is frequently mentioned. We reexamined a number of other reports on the radiation response of normal and malignant hemo- poietic stem cells and found that the repair capacity of these cells is substantial. It is our opinion that the theoretical therapeutic gain achieved by delivering TBI
Reprint requests to: C. W. Song, Ph.D. Supported by National Cancer Institute Grant # CA 15548.
Acknowledgment-The authors are indebted to Miss Peggy Teefy for help in manuscript preparation.
Accepted for publication 9 July I98 I.
1695

1696 Radiation Oncology 0 Biology 0 Physics December I98 I, Volume 7, Number 12
Table I. Radiation response of hemopoietic cells
Do Dq
Mouse bone marrow CFU
Mouse bone marrow CFU
Mouse splenic CFU Mouse femoral CFU Mouse bone marrow CFU Mouse bone marrow CFU Mouse bone marrow CFU
Mouse bone marrow CFU
Mouse bone marrow CFU Human lymphoid cell (T,) Human bone marrow CFU
Irradiation Rad
In vivo (100) In vitro 105 In vivo 95 In vivo 62 In vivo 70 In vitro 62 In vivo 73 In vivo. 105 R/min 72
I 1.6 R/min 79 5.37 R/min 85 2.86 R/min 99
In vitro, 1750 R/hr 90. I 190 R/hr 92.9
In vitro 160 In vitro 85 In vitro 137
Rad
(80) (100)
(50)
(80) (100)
(90) 60 48 45
(Z.2) (56.1)
0 175
0
n Refs
(2.0) 16 2.5 24 1.5 27
0.97 17 2.5 17 4.0 42 2.4 42 2.4 32 1.8 32 1.7 32 1.2 32 1.93 24 1.83 24 1.0 36 7.7 8 1.0 36
The numbers in parentheses are estimate values.
in several fractions at a high dose rate or in a single dose at 5-8 rad/min instead of a single treatment at 26 rad/min is overestimated by other investigators.
In Table 1, the parameters of the radiation survival curve of hemopoietic cells reported by a number of investigators are listed. The parameters of radiation survival curves for the hemopoietic cells in some of those studies are at considerable variance from those reported by McCulloch and Till.” For example, Van Putten reported that the n of the radiation survival curve for mouse bone marrow stem cells was as large as 4 and Dq was 100 rad. The Do of radiation survival curve of mouse marrow CFU was reported to be 160 rad, although the extrapolation number was only 1 .0.36 Pettersen et ~1.~’ reported that mouse bone marrow stem cell population is consisted of radiosensitive and radioresistant cells and that the Dq of the radioresistant population is greater than 200 rad. Drewinko et al.’ demonstrated that estab- lished human lymphoid cells (T,) had n and Dq of 7.7 and 175 rad, respectively; they concluded that the radia- tion response of these lymphoid cells is remarkably simi- lar to the response of other mammalian cells.
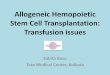
The capacity of mammalian cells to repair sublethal radiation injury can be best quantitated by split-dose or fractionated-dose experiments. In Fig. I, the repair capacity of lymphoid cells is compared with that of Chinese hamster cells and L cells of mice. It is clear that the survival of lymphoid cells, including hemopoietic stem cells, significantly increases when the radiation exposure is split into two doses, unequivocally demon- strating the sublethal damage caused by the first dose of radiation is repaired. In fact, the extent of recovery of T, ceils, an established human lymphoid cell line (curve A), is greater than that in Chinese hamster cells (curve E) or L cells of mice (curve F). Till and McCulloch3’ observed that survival of endogenous colony forming ceils in the mouse spleen increased by factors of 3-4 when radiation
was fractionated in 2 doses with a time interval of 5 hours (curve B); they concluded that “early repair processes occur after whole-body irradiation of the intact mouse.” The recovery factor was about 2 for exogenous colony forming cells from mouse bone marrow (curve C), as opposed to 3-4 recovery factor for endogenous cells (curve B), suggesting that perturbation of environment may diminish the repair capacity of hemopoietic cells. Till and McCulloch” concluded that “the survival ratio (recovery factor) at the j-hour maximum appears to be greater than would be expected from the extrapolation number of 1.5 for the single-exposure curve.” This could be taken to imply that the extrapolation number of a single dose radiation survival curve may not necessarily
30- I 1 I I I I
20- Hemopoietlc Cells
0 2 4 6 8 10 12 14
Hours after First Dose
Fig. 1. Recovery factor for hemopoietic cells as a function of time between two doses. (A) Tl cells, 350 rad + 350 rad.8 (B) Mouse splenic CFU (exogenous), 400 rad + 300 rad.j9 (C) Mouse bone marrow CFU, 200 rad + 200 rad.39 (D) Mouse splenic CFU (endogenous), 250 rad + 500 rad.6 (E) Chinese hamster cells, 791 rad + 731 rad.” (F) L cells, 700 rad + 509 rad.47

Repair capacity of hemopoietic cells ??C. W. SONG et al. 1697
present the repair capacity of sublethal radiation damage. In this context, Withers45 suggested that single dose survival curves tend to provide an underestimate of the repair capacity of a proportion of the cells.
Chaffey and Hellman observed that the survival of hemopoietic stem cells of mice increased by a factor of more than 2 when the irradiation was split into 2 fractions at an interval of several hours (curve D). The study by these investigators on the effect of fractionated irradiation on the endocolonies in the spleen of mice is more interesting. With fractionated radiation of 200 R per day, there was no further decrease in the endocolonies with the increase in total dose greater than 600 R; the efficacy of the fractionation of 250 R per day was significantly less than that of a single dose exposure in reducing endocolonies (Fig. 2). Hellman15 recently attributed the above results to repopulation of clonogenic cells between fractionations and repair of cellular damage. Whatever the mechanism might be, the unrefut- able fact is that fractionated radiation is significantly less effective in reducing hemopoietic stem cell survival than a single exposure.
Rubin and Scarantino33 detailed the factors related to bone marrow regeneration after irradiation and drug treatment. Indications are that there are at least three
50.0
1
a
10.0 1
2 5.0 -
8 .- 2 s 5 r" 1.0:
0.5 -
0.2 -
POOR/day
4/ ’ I I I I I
400 600 800 1000 1200 1400
Total Dose (RI Fig. 2. Radiation survival curves of endogenous CFU in spleen of C3H mice. The animals were irradiated in a single dose or daily dose of 200 R or 250 R, and the colonies in the spleens were counted. Redrawn from Chaffey and Hellman.”
different kinds of CFU and that fractionated irradiation is less effective than a single dose irradiation in sterilizing the CFU.
The study by Puro and Clark3* clearly demonstrated that the response of mouse bone marrow CFU to radia- tion is dose rate dependent as shown in Table 1. Kolb et aLz3 also studied the effect of TBI delivered with different dose rates on the peripheral blood counts of leukocytes, lymphocytes and platelets as well as on the bone marrow CFU in dogs. Irradiation at 5.5 rad/min was far less effective than that at 55 rad/min in reducing above blood cells. For example, TBI of 400 rad at 5.5 rad/min decreased the CFU to 36%) of the control, while TBI at 55 rad/min decreased the CFU to 0% of the control 35 days after the treatments. In the study by Krebs and Jones,24 no such dose rate effect was observed for the CFU from bone marrow of mice. Interestingly, however, there was a significant increase in LDS,,,3,, when the dose rate was reduced; the LD,,,,,, at 3.1 R/min and 20.9 R/min was 1359 R and 873 R, respectively. The difference was 486 R, which was a 55% increase over the LD so,30 for the higher exposure rate.
For a complete take of bone marrow transplanted after TBI, the host immune response should be suppressed as much as possible. There is unequivocal evidence that the immunosuppressive effect of TBI is strongly dependent of dose rate.7.‘2 Gengozian rt al.‘* irradiated mice at different dose rates and transplanted allogeneic or xeno- geneic bone marrow cells. A permanent marrow graft was obtained and the survival of mice was prolonged when the TBI was done at 39.7 R/min or 53.4 R/min, while the mice irradiated at 3.75 R/min rejected the graft. In the mice receiving TBI at the low exposure rate, formation of antibody directed against graft antigen was observed. It was concluded that “the lower the exposure rate, the greater the ability of the irradiated animal to mount an immune response leading to an incomplete take or loss of the graft and subsequent formation of anti- body.”
There is abundant evidence that normal or malignant hemopoietic cells are able to effectively carry out repair of DNA damage caused by ionizing radiation or ultravio- let light in common with other proliferating mammalian Cel]s,%25.35 The above observations are in direct contra- diction to the assertion that “there is often no split dose recovery” in hemopoietic stem cells,” “there should be relatively little effect on cell survival of dose fractionation or of dose rate” or “both LD50,30 assay and CFU assay indicate a limited to absent repair capacity.“30
With regard to malignant hemopoietic stem cells, Peters et ~1.~’ stated that the mean extrapolation number for 7 leukemias or lymphomas compiled by Whitmore and Til14’ was I .6 (our own calculation shows that it is not I .6, but 2.0) and concluded that “experimental leukemias or lymphomas share the property of their normal cells of origin, having smaller survival curve-shoulders.” Kolb et ~1.‘~ and Lichter ef ~1.~~ also expressed a similar opinion.

zn c .- > ._ >
f co
Radiation Oncology ??Biology 0 Physics December 198 1, Volume 7, Number I 2
E
I I I I I I
0 400 800 1200
Rad
Fig. 3. Radiation survival curves of malignant hemopoietic cells. (A) Ll2lO lymphoma cells in viva (hypoxic?).” (B) P-388 leukemia cells in vivo (1 day old).’ (C) WEHI AML cells in vitro, grown in 0.8% methylcel1ulose.‘3 (C’) WEHI- AML ceils in vitro, grown in plastic dish.13 (D) L5178Y lymphoma cells in virr~.‘~ (E) L12lO lymphoma cells in viva.” (F) Chinese hamster cells in vitro.” (G) Mastocytoma cells in vitro.”
In Fig. 3, we compared the radiation survival curve of several experimental malignant hemopoietic cells with that of Chinese hamster cells and mastocytoma cells of mouse. The detailed parameters of the radiation survival curves of various leukemia and lymphoma cells of mouse are summarized in Table 2. It is apparent that the n, Dq and Do of these malignant hemopoietic cells are not different from those for normal or other malignant cells, including human tumor cells,44 and are greater than those values cited by other investigators.23~26~29”0 In Fig. 4, the effect of split dose on the survival of malignant hemo- poietic cells of mice is compared with that of Chinese hamster cells and L cells of mice. It can be seen that the capacity of hymphoma or leukemia cells to repair suble- thal damage caused by the first dose is as great as that of other cells.
Recently, Weichselbaum et ~1.~~ studied the radiosen- sitivity of established human malignant hemopoietic cell lines. They observed that the radiosensitivity of these cells was heterogenous with Do and n respective of 45-165 rad and 1.1-4.0. It should be stressed that the radiobiological parameters of these malignant hemo- poietic cells were similar to the radiobiological param- eters of other human tumors (Do; 139 rad. n; 1.63) reported by Weichselbaum et a1.44 Unfortunately, the response of human malignant hemopoietic cells to split dose irradiation has not yet been examined. It is highly conceivable, however, that human malignant hemopoietic cells may also be able to repair radiation damage as are the other human malignant cells.
It is probable that the disassociation of tumors depleted the repair capacity of the cells in the experiment by Weichselbaum et a1.,44 and that the actual repair capacity of tumor cells in situ may be much greater than
Table 2. Radiation response of malignant hemopoietic cells
Do Do Irradiation
Ll210 lymphoma (spleen) In vivo (femur) In vivo
L1210 lymphoma (i.p.) In vivo LS 178 lymphoma In vitro L5 178 lymphoma In vitro Mouse leukemia In vivo AKR lymphoma In vitro P388 leukemia (6 day old) In vivo P388 leukemia (diploid) In vivo P288 leukemia (tetraploid) In vivo P388 leukemia In vivo P388 leukemia In vitro (1 day old) In vivo (7 day old) In viva 5774 In vitro WEHI- In vitro (methylcellulose)
In vitro (plastic dish) BNML In vivo
The numbers in parentheses are estimate values.
Rad
88 83
250 100 85
165 114
(300) 160 180 350 I51 110 411 116 104
(103) 68
Rad
(108) (102) (219)
134 130
(181)
(600) (75)
(204) 600
(226) (362) (230)
(268) (42) (89)
n Refs
3.4 17 3.4 17 2.4 19 3.8 34 4.7 49 3.0 18 0.7 5
(10.0) 20 1.6 3 3.1 3 8.0 4 4.5 1
26.9 1 1.75 1 0.67 13
13.2 13 1.5 13 3.7 14

Repair capacity of hemopoietic cells 0 C. W. SONG et al. 1699
30 I I I I I I
20 - Leukemia Ceils
0 2 4 6 8 10 12 14 Hours after First Dose
Fig. 4. Recovery factor for malignant hemopoietic cells as a function of time between two doses. (A) 1 day old P-388 cells, 500 rad + 500 rad.* (B) 6 day old P-388 cells, 1500 rad + 1500 rad.* (C) AKR mouse lymphoma cells, 374 rad + 188 rad.“’ (D) Chinese hamster cells, 791 + 731 rad.” (E) L cells, 700 rad + 500 rad.”
the parameters of radiation survival curve of single cells in vitro indicate. It has been reported that the self- replication of hemopoietic stem cells and certain leukemic cells occurs preferentially in the subendosteal area.” The relatively small extrapolation number of radiation survival curves for CFU reported by investiga- tors may be attributed, at least in part, to the disruption of microenvironment: i.e. culturing in agar media after removing from such a preferred area.
Using the parameters of a single dose radiation survival curve for mouse bone marrow stem ceils (Dq:50 rad. n: I .5) reported by McCulloch and Till*’ and the dose rate effect factors for mouse LDsolso, Peters*’ and Peters et a1.30 estimated the effectiveness of different TBI proto- cols to reduce the survival of hemopoietic stem cells of mouse. They concluded that a single dose of 750 rad at 26 rad/min would reduce the mouse hemopoietic stem ceils by 3.63 logs, and that fractionated TBI with total dose of 1200 rad or 1600 rad using 200 rad per fraction twice a day would reduce the survival by 4.43 logs and 5.9 I logs, respectively. Hagenbeek and Van Bekkum” used a rat model for human acute myelocytic leukemia (BNML) to investigate the efficacy of different TBI schedules (Table 3). TBI with 900 rad in a single dose reduced the survival of BNML cells by 4 logs and TBI of 900 rad in four daily fractions of 225 rad could reduce the survival by only I-2 logs. This significant difference in the efficacy of 900 rad in a single dose and in fractionated doses to reduce the survival of leukemic cells was apparently a result of the regeneration and repair of sublethal damage during the
Table 3. Decrease in survival (log death) of BNML leukemic cells of rats by different TBI schedules (14)
TBI schedules (I 1 S/rad/min)
1 x 900 rad/day x I 1 x 225 rad/day x 4 2 x 200 rad/day x 4
Total dose tad
900 900
1,600
Log death
4 l-2 3-4
fractionated irradiation. Fractionated TBI with a total dose of 1600 rad given by 200 rad per fraction twice a day reduced the survival of leukemic cells by 3-4 logs, which is substantially smaller than 5.91 logs killing estimated by Peters,” as mentioned above.
The lung is believed to be the dose-limiting tissue for TBI followed by bone marrow transplantation. A number of investigators pointed out that the repair capacity of the lung is greater than that of CFU of hemopoietic cells. It is probably improper to compare the damage in orga- nized whole lung with the depletion of the reproductive capacity of disassociated hemopoietic cells, which is assayed either by in vitro culture or by injection to other irradiated hosts. The repair capacity of endoclones in undisrupted mouse spleen as used by Chaffey and Helman (Fig. 2) may be a better choice for a compari- son. In this regard, it is of interest to note that dose- response curve for the depletion of proliferation function of type 2 lung epithelial cells in mice has recently been reported to be diphasic.28 The initial steeper portion of the curve was characterized by Do of 120 rad with the extrapolation number of I .O.
It is believe that repair of sublethal damage, redistri- bution of cells through the cell cycle, and regeneration of surviving cells both in normal tissues and tumors and reoxygenation of hypoxic cells in tumors take place during radiotherapy with conventional fractionated schedules.46 The relative importance of these four factors in the TBI in several fractions over 2-3 days is unknown. Nevertheless, it appears that the role of difference in the repair capacity between hemopoietic cells and other tissues in TBI may not be as substantial as has been believed.
It is not the contention of this discussion that normal or malignant hemopoietic cells are able to repair radiation damage as effectively as are other normal tissues such as the lung. Rather, it is intended to point out that the repair capacity of hemopoietic stem cells or immunocytes may have been underestimated. Further research on the repair capacity of normal and malignant human hemopoietic tissues and that of the lung is urgently needed.
REFERENCES 1. Andrews, R., Belli, J.A.: Relationship between tumor
growth and radiosensitivity. JNCI 31: 689-703, 1963. 2. Belli, J.A., Dicus, G.J., Nagle, W.: Repair of radiation
damage as a factor in preoperative radiation therapy. Front. Radiation. Ther. One. 5: 40-57, 1970.
3. Berry, R.J.: Quantitative studies of relationships between

1700 Radiation Oncology 0 Biology 0 Physics December 1981. Volume 7. Number I2
tumor cell ploidy and dose reponse to ionizing radiation in vivo. Radiat. Res. 18: 236-245, 1963.
4. Berry R.: Medication of radiation effects. Radio/. C‘lin. h’. Am. 3: 249-258, 1965.
5. Bruce, W.R., Bush, R.S.: The radiosensitivity of trans- planted lymphoma cells as determined by the spleen colony method. Radiat. Res. 21: 612-621, 1964.
6. Chaffey, J.T., Hellman. S.: Radiation fractionation as applied to murine colony-forming cells in differing prolifer- ative states. Radiol. 93: I I67- I 172, 1969.
7. Courtenay, V.D.: Studies on the protective efect of allo- geneic marrow grafts in the rat following whole-body irradiation at different dose-rates. Br. J. Radiol. 36: 440- 447. 1963.
8. Drewinko, B., Humphrey, R.M., Trujilio. J.M.: The radia- tion response of a long-term culture of human lymphoid cells. I. Asynchronous populations. Int. J. Radiat. Biol. 21: 36lL373, 1972.
9. Elkind, M.M.: DNA repair and cell repair: Are they related? Int. J. Radiat. Oncol. Biol. Phys. 5: 1089-1094. 1979.
IO. Elkind, M.M., Sutton, H.: Radiation response of mammal- ian cell growth in culture. I. Repair of X-ray damage in surviving Chinese hamster cells. Radiat. Res. 13: 556-593. 1960.
I I. Feola, J.M., Song, C.W.. Khan, F.M.. Levitt, S.H.: Lethal response of C57BL mice to MeV x-rays and to 6oCo gamma-rays. Int. J. Radiat. Biol. 26: 161-165, 1974.
12. Gengozian, N., Carison, D.E., Allen, E.M.: Transplanta- tion of allogeneic and xenogeneic (Rat) marrow in irra- diated mice as affected by radiation exposure rates. Trans- plantation 7: 259-273, 1969.
13. Greenberger, J.S., Weichselbaum, RR., Botnick, L.E.. Sakakenny, M., Molony, W.C.: Cell biological effects 01 total body irradiation on growth and differentiation of acute myelogenous leukemia cells compared to normal bone marrow. Exp. Hematol. 7( 5): 279-289. 1979.
14. Hagenbeek, A., Van Bekkum, D.W.: Comparison of different total body irradiation regimes combined with bone marrow transplantation in a rat model for human acute myelocytic leukemia. Int. J. Radiat. Biol 36: 412, 1979.
15. Hellman, S.: Improving the therapeutic index in breast cancer treatment: The Richard and Linda Rosenthal Foun- dation Award Lecture. Cancer Res. 40: 433554342, 1980.
16. Hellman, S., Hannon. E.: Effect of adriamycin on the radiation response of murine hematopoietic stem cells. Radiat. Res. 67: 162-167. 1976.
17. Hendry, J.H.: The response of haemapoietic colony-form- ing units and lymphoma cells irradiated in soft tissue (spleen) or a bone cavity (femur) with single doses of x-rays, rays or D-T neutrons. Br. J. Radiol. 45: 923-932, 1972.
18. Hewitt, H.B., Wilson, G.W.: The effect of tissue oxygen tension on the radiosensitivity of leukemia cells irradiated in situ in the livers of leukemic mice. Br. J. Cancer 13: 675-684,1959.
19. Hofer, K.G., Choppin, D.A., Hofer, M.G.: Effect of hyper- thermia on the radiosensitivity of normal and malignant cells in mice. Cancer 36: 279-287, 1976.
20. Johnson, R.K., Wodinsky, I., Swiniarski, J., Meaney, K.F., Clement, J.J.: Interaction of irradiation with two new antineoplastic agents, aziridinylbenzoquinone (AZW) and 4-(acridinylamino) methansulfon-m-anisidide (AMSA), in muring tumor in vivo. Int. J. Radiat. Oncol. Biol. Phys. 5: 160551609, 1979.
21. Kim, T.H., Kersey, J.H., Sewchand, W., Nesbit, M.E., Krivit, W., Levitt, S.H.: Total body irradiation with a high
dose rate linear accelerator for bone marrow transplanta- tion in aplastic anemia and neoplastic disease. Radio/. 122: 523-525, 1977.
22. Kim. J.H.. Khan, F.M.. Galvin, J.M.: A report of the work party: comparison of the total body irradiation techniques for bone marrow transplantation. Int. J. Radiat. Oncol. Biol. Phys. 6: 779- 784. 1980.
23. Kolb. H.J., Rieder. I., Bodenberger. U., Hetzel. B., Schaf- fer. E.. Kolb. H.. Thierfelder. S.: Dose rate and dose fractionation studies in total body irradiation of dogs. Pathol. Biol. 27: 370-372. 1979.
24. Krebs. J.S.. Jones. D.C.L.: The LD,, and the survival of bone-marrow colony forming cells in mice: Effect of rate of exposure to ionizing radiation. Radiat. Res. 51: 374-380, 1972.
25. I.ett, J.T., Caldwell. I.. Dean, C.J., Alexander. P.: Rejoin- ing of x-ray induced breaks in the DNA of leukemia cells. Nature 214: 790-792. 1967.
26. Lichter. A.S., Tracy. D., Lam, W.C., Order, S.E.: Total body irradiation in bone marrow transplantation: the influence of fractionation and delay of marrow infusion. Int. J. Radiat. Oncol. Biol. Phys. 6: 301-309, 1980.
27. McCulloch, E.A., Till, J.E.: The sensitivity of cells from normal mouse bone marrow to gamma radiation in vitro and in vivo. Radiat. Res. 16: 822-832, 1962.
28. Meyer, K.R.. Witsch, H.. Ullrich, R.L.: Proliferative response of type 2 lung epithelial cells after X-rays and fission neutrons. Radiat. Res. 82: 559-569, 1980.
29. Peters. L.: Discussion: The radiobiological bases of TBI. Int. J. Radiat. Oncol. Biol. Phys. 6: 785-787, 1980.
30. Peters, L.J.. Withers, H.R., CunditT, J.H., Dicke, K.A.: Radiobiological considerations in the use of total body irradiation for bone-marrow transplantation. Radio/. 131: 243-247. 1979.
3 I. Pettersen, E.O., Boyum, A.. Laane, B.F.M.: X-ray inacti- vation of murine bone marrow cells as measured by the spleen colony assay and the diffusion chamber technique. Radiat. Res 58: 409-416, 1974.
32. Puro, E.A., Clark, G.M.: The effect of exposure rate on animal lethality and spleen colony cell survival. Radiat. Res. 52: I I 5- 129, 1972.
33. Rubin, P., Scarantino, C.W.: The bone marrow organ: The critical structure in radiation-drug interaction. Int. J. Radiat. Oncol. Biol. Phys. 4: 3-23, 1978.
34. Sato, K., Hieda, N.: Isolation and characterization of a mutant mouse lymphoma cell sensitive so methyl methane- sulfonate and x rays. Radiat. Res. 78: 167-l 7 I, 1979.
35. Scaife. J.F.: DNA repair in thymus lymphocyte after irradiation. Int. J. Radiat. Biol. Phys. 21: 197-200, 1972.
36. Senn, J.S., McCulloch, E.A.: Radiation sensitivity of human bone marrow cells measured by a cell culture method. Blood 35: 56-60, 1970.
37. Song, C.W., Clement J.J.. Levitt, S.H.: Cytotoxic and radiosensitizing effects of 5-thio-D-glucose on hypoxic cells. Radiol. 123: 201-205, 1977.
38. Thomas, E.D., Storb, R., Clift, R.A., Fiefer, R., Johnson, L., Hieman, P.E., Lerner, K., Gluksberg, H., Buckner, C.D.: Bone marrow transplantation, I and II. N. Engl. J. Med. 292: 832-843 and 895-902, 1975.
39. Till, J.E., McCulloch, E.A.: Early repair process in marrow cells irradiated and proliferating in vivo. Radiat. Res 18: 96-105, 1963.
40. Tolmach, L.J.: Capacity for repair in nirmal and malignant tissues. Conference on “Time and dose relationships in radiation biology as applied to radiotherapy.” Carmel, California, Brookhaven National Laboratory 50203 (C- 57) 1969, pp. 65-66.
41. Van Bekkum, D.W., Prins, M.E.F., Hagenbeek, A.: The

Repair capacity of hemopoietic cells ??C. W. SONG et al. 1701
42.
43.
44.
45.
mechanism of inhibition of hemopoiesis in acute leukemia. Blood Cells (In press) 198 1. Van Putten, L.M.: The biology of dose-limiting tissues. Conference on “Time and dose relationships in radiation biology as applied to radiotherapy.” Carmel, California, Brookhaven National Laboratory 50203 (C-57) 1969, pp. 162-166.
46.
47.
Weichselbaum, R.R., Greenberger, J.S., Schmidt, A., Karpas, A., Moloney, W.C., Little, J.B.: In vitro radiosen- sitivity of human leukemia cell lines. Radiol. 139: 485-487, 1981.
48. Weichselbaum, R.R., Nove, J., Little, J.B.: X-ray sensitiv- ity of human tumor cells in vitro. Int. J. Radiat. Oncol. Biol. Phys 6: 437-440, 1980. Withers, H.R.: Capacity for repair in cell of normal and malignant tissues. Conference on “Time and dose relation- ships in radiation biology as applied to radiotherapy.”
49.
Carmel, California, Brookhaven National Laboratory 50203 (C-57), 1969, pp. 54-69. Withers, H.R.: The four R’s of radiotherpay. In Advances in Radiation Biology, Vol. 5, J.T. Lett and H. Adler (Eds.). N.Y., Academic Press. 1975, pp. 241-271. Whitmore, G.F., Gulyas, S., Botond, J.: Radiation sensitiv- ity throughout the cell cycle and its relationship to recov- ery. In Cellular Radiation Biology. 18th Annual Sympo- sium on Fundamental Cancer Research. The University of Texas. M.D. Anderson Hospital and Tumor Institute. William and Wilkins Co. 1965, pp. 423-441. Whitmore, G.F., Till, J.E.: Quantitation of cellular radio- biological response. Ann. Rev. Nucl. Sci. 14: 347-374, 1964. Yau, T.M., Kim, SC.: Local anaesthetics as hypoxic radio- sensitizers, oxic radioprotectors and potentiators of hyperthermic killing in mammalian cells. Br. J. Rudiol. 53: 687-692,198O.