Embed Size (px)
Citation preview

Racial, Ethnic and Socioeconomic Health Disparities in the US
Richard Lichtenstein Ph.D., MPH
University of Michigan
School of Public Health
June, 2010

Why is the health status of African Americans worse than the health status of Caucasian
Americans?

Health Status is a Function of:
• Biology/Genetics
• Lifestyle/Behavior
• Social/Societal Characteristics
• Physical Environment (“Total Ecology”)
• Medical Care
Tarlov, A.R. “Public Policy Frameworks for Improving Population Health.” Annals of the New York Academy of Sciences 896:281-293 (1999)

Impact of Various Domains on Early Deaths in a Population
Behavioral Patterns
40%
Medical Care10%
Genetics30%
Environment 5%
Social Circumstances
15%Source
McGinnis, et al, Health Affairs 21: 78.
March/April 2002

A major area of research on Health Disparities today is called:
THE SOCIAL DETERMINANTS OF HEALTH
(SDOH)

GENERAL MODEL OF SOCIAL DETERMINANTS
Discrimination
Quality of living area
Access to Services
Social Factors
Social Support
Stress
Fundamental Factors: Money, Power, Prestige
Health
Disease
Self Regulation/Management
Adoption of Preventive Behavior
Individual risk factors
Personal Factors
CUES, NYAM, 2000
Outcomes

Diagram by Whitehead M and Dahlgren C, in “What can be done about inequities and health?”, The Lancet, 338, 8774, 26 October 1991, 1059-1063.

Poverty is the Major Factor in Health Disparities
Which Racial or Ethnic Group Accounts for the Most People in Poverty in the US?

Number of Persons Below Poverty Level By Race, 2007
0
10,000
20,000
30,000
40,000
All races White Black Asian Hispanic
Source: Health, United States, 2009, Table 3
In T
hou
sand
s

Percent of Persons Below Poverty Level By Race, 2007
Source: Health, United States, 2009, Table 3
Per
cen
t b
elow
pov
erty

Why is there a relationship between socioeconomic status
and race?

What is Race?

What is Race?
• Race is not a biological determinant
• “Race is a social construct, a social classification based on phenotype, that governs the distribution of risks and opportunities in our race-conscious society.”
Camara Phyllis Jones, Am J Epidemiol, 154: 299-304 (2001)

What is Race?
• “Although ethnicity reflects cultural heritage, race measures a societally imposed identity and consequent exposure to the societal constraints associated with that particular identity.”
Camara Phyllis Jones

Race Varies by Country• “This assigned race varies among countries…In the
United States I am clearly labeled Black, while in Brazil I would be just as clearly labeled White and in South Africa I would be clearly labeled "colored." It is likely that, if I stayed long enough in any one of these settings, my health profile would become that of the group to which I had been assigned, even though I would have the same genetic endowment in all three settings.”
Camara Phyllis Jones

Beware of treating Race and Ethnicity as Monolithic Concepts
• Is everyone who is black poor?
• Do all Latino sub-groups experience the same degree of unequal health compared to whites?

What are Health Disparities?

Health Disparities or Health Inequalities are inequities that
are related to differences in health status or medical
treatment that are unfair to disadvantaged people and that
are avoidable
Braverman and Tarimo, Soc Sci and Med:54:1621-1635 (2002).

“Pursuing equity in health care means striving to reduce avoidable disparities in physical and psychological well-being—
and in the determinants of that well-being—that are systematically observed between groups of people with different levels of underlying social privilege, i.e.,
wealth, power or prestige.”
Braverman and Tarimo, Soc Sci and Med:54:1621-1635 (2002).

Demographic and Health Characteristics of People on the
Eastside of Detroit

Table 1: Socio-Demographic Characteristics of Eastside and Central Detroit in Comparison to City of
Detroit and the National Average
Source: 1U.S. Bureau of the Census, 2006-2008 American Community Survey 3-Year Estimates2Detroit data from www.CHIMart.org, 1999-2001 data

Table II: Health Status Characteristics of the Eastside in Comparison to the City of Detroit and the
U.S. Population
Detroit data from www.CHIMart.org, 1999-2001 data*2006 Data from Health, United States, 2009 Table 26**Infant deaths/1000 live births, Health, United States, 2009, Table 19

Health Disparities

Life Expectancy at Birth by Race and Sex, 1970-2006
55
60
65
70
75
80
85
1970
1980
1990
1992
1994
1996
1998
2000
2002
2004
2006
Yea
rs
White Male
White Female
Black Male
Black Female
Source: Health, United States, 2009, Table 24

0200400600800
10001200
Age
-Adj
uste
d D
eath
Rat
e
White Black Am. Indian or Alaskan Asian/Pacific Islander Hispanic
Age-Adjusted Death RatesDue to All Causes,
by Race and Hispanic Origin, 2006
Source: Health, United States, 2009, Table 25

Age-adjusted Death Rates by Race, 2006
0
50
100
150
200
250
300
350
All Race & Sex White Black
Dea
ths
per
100,
000 Disease of Heart
Ischemic Heart Disease
Cerebrovascular Disease
Prostate Cancer
Breast Cancer
Diabetes Mellitus
Homicide
Source: Health, United States, 2009, Table 26

New York Times, December 2, 2009
Native American Death Rates Compared to All Races

YEARS OF POTENTIAL LIFE LOST
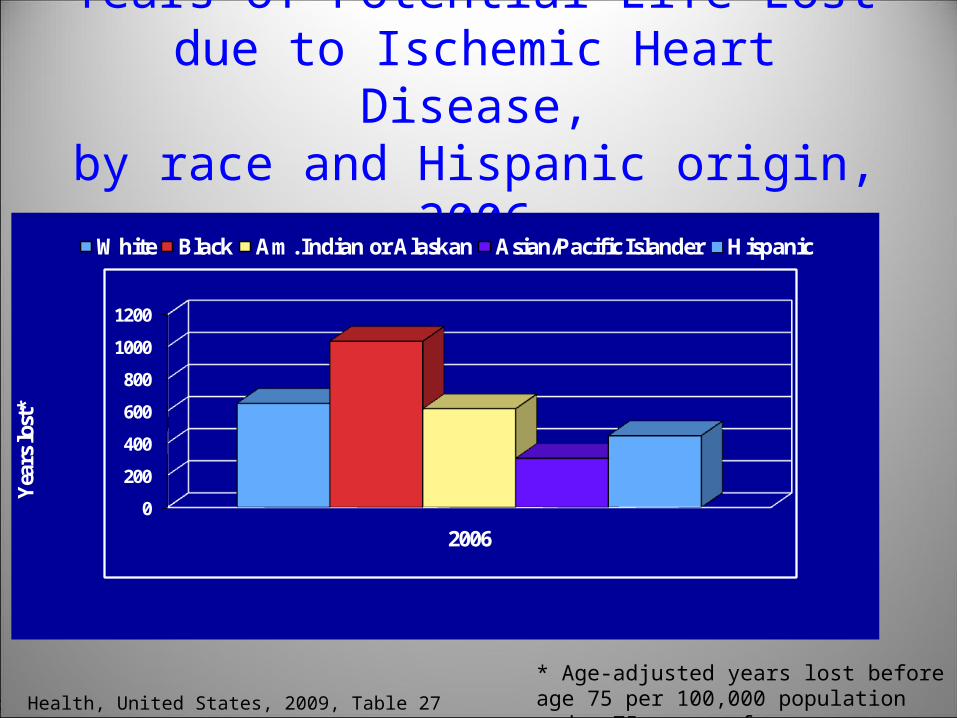
Years of Potential Life Lostdue to Ischemic Heart Disease,
by race and Hispanic origin, 2006
0
200
400
600
800
1000
1200
2006
Yea
rs lo
st*
White Black Am. Indian or Alaskan Asian/Pacific Islander Hispanic
Source: Health, United States, 2009, Table 27
* Age-adjusted years lost before age 75 per 100,000 population under 75 years of age.

Years of Potential Life Lostdue to Diabetes Mellitus,
by race and Hispanic origin, 2006
0
100
200
300
400
Yea
rs lo
st*
White Black Am. Indian or Alaskan Asian/Pacific Islander Hispanic
2006
Source: Health, United States, 2009, Table 27
* Age-adjusted years lost before age 75 per 100,000 population under 75 years of age.

Years of Potential Life Lostdue to Homicide,
by race and Hispanic origin, 2006
0
200
400
600
800
1000
Yea
rs lo
st*
White Black Am. Indian or Alaskan Asian/Pacific Islander Hispanic
2006
Source: Health, United States, 2009, Table 27
* Age-adjusted years lost before age 75 per 100,000 population under 75 years of age.

5 Year Relative Survival Rates for Breast Cancer
50
60
70
80
90
100
1974-79 1980-82 1983-85 1986-88 1989-91 1992-94 1996-1998 1999-2005
White Female
Black Female
Per
cent
of
Pat
ient
s (%
)
Source: Health, United States, 2009, Table 50

Infant Mortality Rates by Race*United States, 1970-2006
0
10
20
30
40
1970
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
All races
White
Black
Source: Health, United States, 2009, Table 19
Dea
ths
per
1,0
00 L
ive
Bir
ths
*Race of mother

0 2 4 6 8 10 12 14 16
Black, not Hispanic
Hispanic (total)
Puerto Rican
White, not Hispanic
Cuban
MexicanCentral and South American
Infant mortality rates by detailed race and Hispanic origin of mother: United States, 2005
NOTES: Infant is defined as under 1 year of age. Persons of Hispanic origin may be of any race. The race groups, Asian or Pacific Islander and American Indian or Alaska Native, include persons of Hispanic and non-Hispanic origin. See Data Table for data points graphed and additional notes.
Infant per 1,000 live births
Other Hispanic
Centers for Disease Control and Prevention, National Center for Health Statistics. Health, United States, 2009
Asian or Pacific Islander (total)
American Indian or Alaska Native

Infant Mortality Rate by Race (of mother), 2001-2006
0
5
10
15
20
25
1980 1985 1990 1995 2000 2003 2005 2006
Infa
nt M
orta
lity
Rat
e
White
Black
Source: Health, United States, 2009, Table 19
IMR: Deaths of infants under 1 year per 1,000 live births

International Rankings for Infant Mortality1960 and 2006
1960 2006
Hong Kong 26 1
Singapore 21 2
Japan 19 2
Finland 6 4
Norway 3 6
Czech Republic 4 7
Portugal 35 7
Belgium 11 -
Austria 24 9
Greece 25 10
Ireland 18 10
Germany 22 12
France 16 12
Spain 28 12
Denmark 8 12
Israel 20 16
Switzerland 7 17
Italy 27 -
1960 2006
Netherlands 2 17
Australia 5 20
England and Wales 9 21
New Zealand 10 23
Scotland 13 19
Canada 15 -
Cuba 23 24
Hungary 31 25
Northern Ireland 14 22
Poland 32 26
United States 12 28
Slovakia 17 27
Chile 36 29
Puerto Rico 27 -
Costa Rica 35 30
Russian Federation --- 31
Bulgaria 30 -
Romania 36 32Source: Health, United States, 2009, Table 22

IMR - International Rankings 2009
Source: CIA – The World Factbook: (accessed May 14, 2010)
Country Infant Mortality Rate (deaths/1000 live births)
Rank
Angola 180.21 1
Afghanistan 153.14 2
Liberia 138.24 3
Niger 116.66 4
Mali 115.86 5
-- -- --
United States 6.22 180
-- -- --
France 3.33 217
Iceland 3.23 218
Macau 3.22 219
Hong Kong 2.92 220
Japan 2.79 221
Sweden 2.75 222
Bermuda 2.46 223
Singapore 2.31 224

Infant Mortality Rates by mother’s education, race, and Hispanic origin, 2003-2005
0
3
6
9
12
15
IMR
Less than 12 years 12 years 13+ years
Years of Education
White, non-Hispanic Black, non-HispanicHispanic American Indian or Alaska NativeAsian or Pacific Islander
Source: Health, United States, 2008, Table 19

Low Birth Weight* by Race and Ancestry of Mother, 2007
0
4
8
12
16
Per
cen
t L
ow B
irth
W
eigh
t B
irth
s
White Black Arab Ancestry HispanicAncestry
City of DetroitWayne CountyWayne County Health Dept.Michigan
Source: Division for Vital Records and Health Statistics, Michigan Department of Community Health, 2007
*less than 2500 grams

Activities of Daily Living (ADL) and Instrumental ADL (2008)
0
1
2
3
4
5
6
7
8
ADL IADL
Per
cent
age
18+
yrs
Exp
erie
ncin
g Im
pair
men
t
<$35,000 $35,000-$49,999 $50,000-$74,999 $75,000-$99,999 $100,000 or more
Source: National Health Interview Survey, 2008

Percent with Fair or Poor Self-Rated Health Status, 2007
0 5 10 15 20 25 30
TotalWhiteBlack
PoorNear-PoorNon-Poor
<18 years65+
Male Female
MetropolitanNon-Metropolitan
Source: Health, United States, 2009, Table 57
Percent

Fair or Poor Health among Adults18 years and older by family income, race,
and Hispanic origin, 2007
0
5
10
15
20
25
White, non-Hispanic Black, non-Hispanic Hispanic
Per
cen
t
Poor Near Poor Non-Poor
Source: Health, United States, 2009, Table 57

For Want of a Dentist
Pr. George's Boy Dies After Bacteria From Tooth Spread to Brain
By Mary Otto
Washington Post Staff WriterWednesday, February 28, 2007; Page B01
Twelve-year-old Deamonte Driver died of a toothache
Sunday.
A routine, $80 tooth extraction might have saved him.
If his mother had been insured.
If his family had not lost its Medicaid.
If Medicaid dentists weren't so hard to find.
If his mother hadn't been focused on getting a dentist for his brother, who had six rotted teeth.
Deamonte's death and the ultimate cost of his care, which could total more than $250,000, underscore an often-overlooked concern in the debate over universal health coverage: dental care.

Utilization of ServicesHealth Insurance is important to Access,
but it is not the only factor

No Health Insurance Coverage among persons under 65, by race and Hispanic origin, 2004
05
10152025303540
White, non-Hispanic
Black, non-Hispanic
AmericanIndian and
AlaskanNative
Asian Hispanic orLatino
Per
cent
uni
nsur
ed
Source: Health, United States, 2006, Table 135.

Percentage With Access Problems
0
5
10
15
20
25
30
35
All Persons
Medicare
Private
Medicaid
Uninsured

Percent of Children under 18 with No Usual Source of Care
by Insurance Type, 2006-2007
33.6
5.2 3
0
5
10
15
20
25
30
35
40
Uninsured Medicaid Private
Per
cen
t w
ith
no
usu
al s
ourc
e of
car
e
Source: Health United States, 2009, Table 75

Vaccinations among Children 19-35 months old by Poverty Status and Race, 2007
60
65
70
75
80
85
White, non-Hispanic Black, non-Hispanic Hispanic
Per
cen
t re
ceiv
ing
com
bin
ed s
erie
s
Poor
Non-Poor
Source: Health, United States, 2009, Table 82

Proportion of Live Births with Late* or No Prenatal Care, by Race and Ethnicity of
Mother, 2006
3.2
5.7
8.1
3.1
5
0
1
2
3
4
5
6
7
8
9
White Black American Indian or Alaskan Native
Asian or Pacific Islander
Hispanic Origin
Per
cent
of
Liv
e B
irth
s
Source: Health, United States, 2009, Table 7 (37 states, DC and NYC)
*third trimester*third trimester

Children under 6 with no physician contactswithin last year, by race, and Hispanic origin,
and poverty status, 2005-2006
0
2
4
6
8
10
12
Per
cent
wit
hout
a v
isit
All race White, non-Hispanic
Black, non-Hispanic*
Hispanic
Poor
Near Poor
Nonpoor
AVERAGE all children under 6 without a health care visit in 2005-6 – 6.1%* Estimates are for 2004/2005 (data not available for 2005-2006)Source: Health, United States, 2008, Table 82

Persons with Hospital Stay in the Past Year*, By Poverty and Insurance Status, 2007
Source: Health, United States, 2009, Table 98
* Persons under 65 years of age* Persons under 65 years of age
0
2
4
6
8
10
12
Poor Near Poor Non-Poor
Per
cent
of
pers
ons
Poverty and Insurance Status
Insured
Uninsured >12 mths

Avoidable Hospitalizations - Adults 18-64 yrs old by household income* and race, 1989-1991
0
2
4
6
8
10
12
14
16
18
20
Dis
char
ges
per
1,00
0 po
pula
tion
All races White Black
<$20,000$20,000-$29,999$30,000-$39,999$40,000+
Source: Health, United States, 1998, Figure 48
* Median household income in Zip code of residence

Asthma Hospitalizations - Children 1-14 yrs of age by household income* and race, 1989-
1991
0
1
2
3
4
5
6
7
8
Dis
char
ges
per
1,00
0 po
pula
tion
All races White Black
<$20,000$20,000-$29,999$30,000-$39,999$40,000+
Source: Health, United States, 1998, Figure 24
*Median household income in Zip code of residence

UNEQUAL TREATMENT

Black/White and SES Differences When Patients Have
Same Diagnosis

“The health system is less responsive to black patients then
to white patients.” (Epstein and Ayanian, 2001)
The same is true for low vs. high income patients.

Institute of Medicine ReportUnequal Treatment
“Racial and ethnic minorities tend to receive a lower quality of healthcare than non-minorities,
even when access-related factors, such as patients’ insurance status
and income, are controlled.”IOM, IOM, Unequal Treatment, 2002Unequal Treatment, 2002

Studies have shown this to be true for patients with:
• Heart attacks and heart disease (PTCA and CABGS)
• Peripheral vascular disease of the lower extremities (amputation vs. re-vascularization)
• ESRD (transplants vs. dialysis)• Small-cell carcinoma of the lungs• Psychiatric problems• Many more diagnoses

Racial Disparities In Early Stage Lung Cancer Treatment
34.9
26.4
0
10
20
30
40
50
60
70
80
Per
cen
t or
rat
e
White Black
Rate of Surgery5yr Survival Rate
Source: Bach et. al,. Racial differences in the treatment of early-stage lung cancer. N Engl J Med. 1999 Oct 14;341(16):1198-205.

Racial Disparities In Rehabilitation Services after Hip Fracture (odds ratio)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Rat
io
Acute Rehab SNU Rehab No Rehab
WhiteBlack
Source: Harada et. al,. Patterns of rehabilitation utilization after hip fracture in acute hospitals and skilled nursing facilities. Med Care. 2000 Nov;38(11):1119-30.

Will the Passage of Health (Insurance) Reform, which will
provide insurance coverage to 32 Million more Americans,
eliminate Health Disparities?
![Lichtenstein v. Lichtenstein · [Cite as Lichtenstein v.Lichtenstein, 2020-Ohio-5080.] COURT OF APPEALS OF OHIO EIGHTH APPELLATE DISTRICT COUNTY OF CUYAHOGA RYAN LICHTENSTEIN, : Plaintiff-Appellee,](https://img.dokumen.tips/doc/110x75/60903f096995511fe42a0d9e/lichtenstein-v-cite-as-lichtenstein-vlichtenstein-2020-ohio-5080-court-of.jpg)




























