Embed Size (px)
Citation preview

R. Riener, H. Vallery, A. Duschau-WickeETH Zurich, Balgrist University Hospital, Hocoma
Z. Rymer & Y. DhaherRehabilitation Institute of Chicago
MARS-RERC Advisory Board Meeting18/19 August 2009
D1: Cooperative Control for Robot-Aided Gait TherapyD1: Cooperative Control for Robot-Aided Gait Therapy

Zurich NetworkZurich Network
R. Riener & V. Dietz & G. Colombo
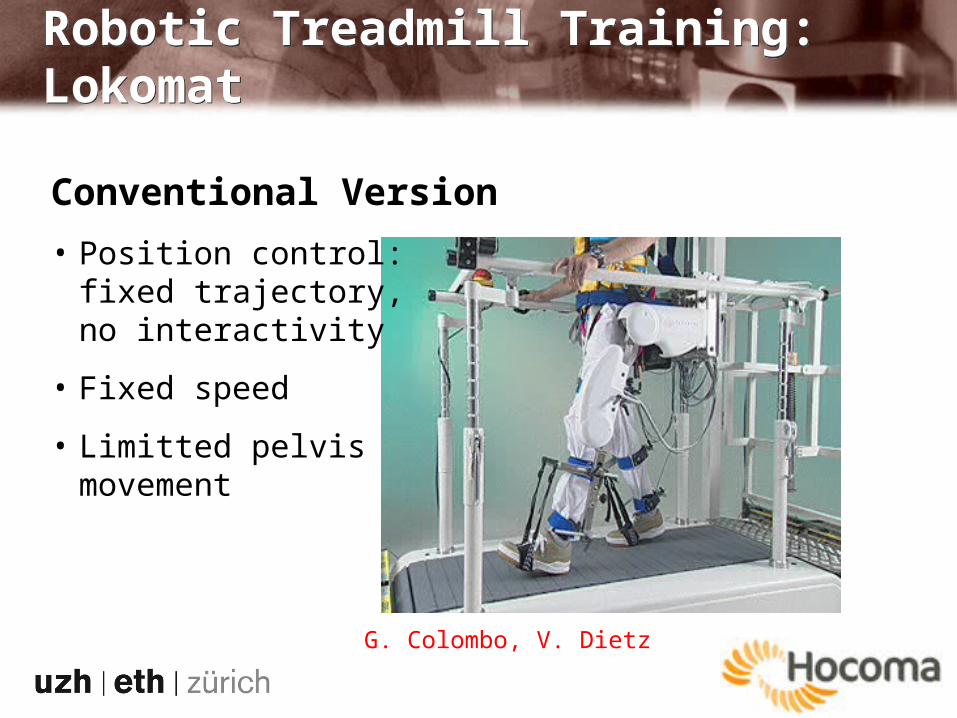
Robotic Treadmill Training: LokomatRobotic Treadmill Training: Lokomat
Conventional Version
• Position control: fixed trajectory, no interactivity
• Fixed speed
• Limitted pelvis movement
G. Colombo, V. Dietz
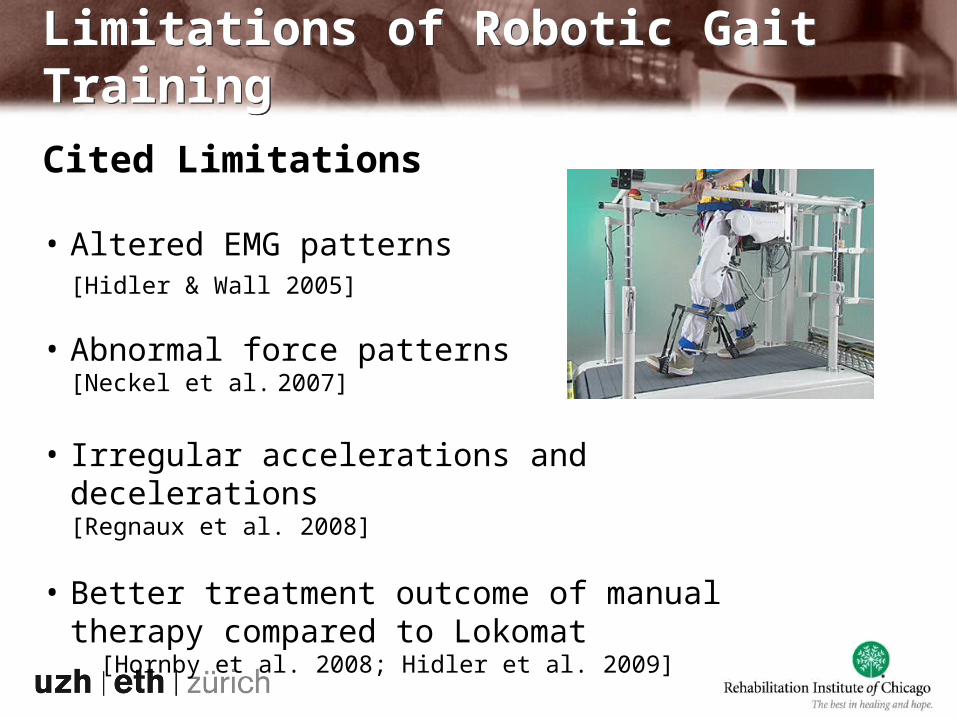
Cited Limitations
• Altered EMG patterns [Hidler & Wall 2005]
• Abnormal force patterns[Neckel et al. 2007]
• Irregular accelerations and decelerations [Regnaux et al. 2008]
• Better treatment outcome of manual therapy compared to Lokomat
[Hornby et al. 2008; Hidler et al. 2009]
Limitations of Robotic Gait TrainingLimitations of Robotic Gait Training
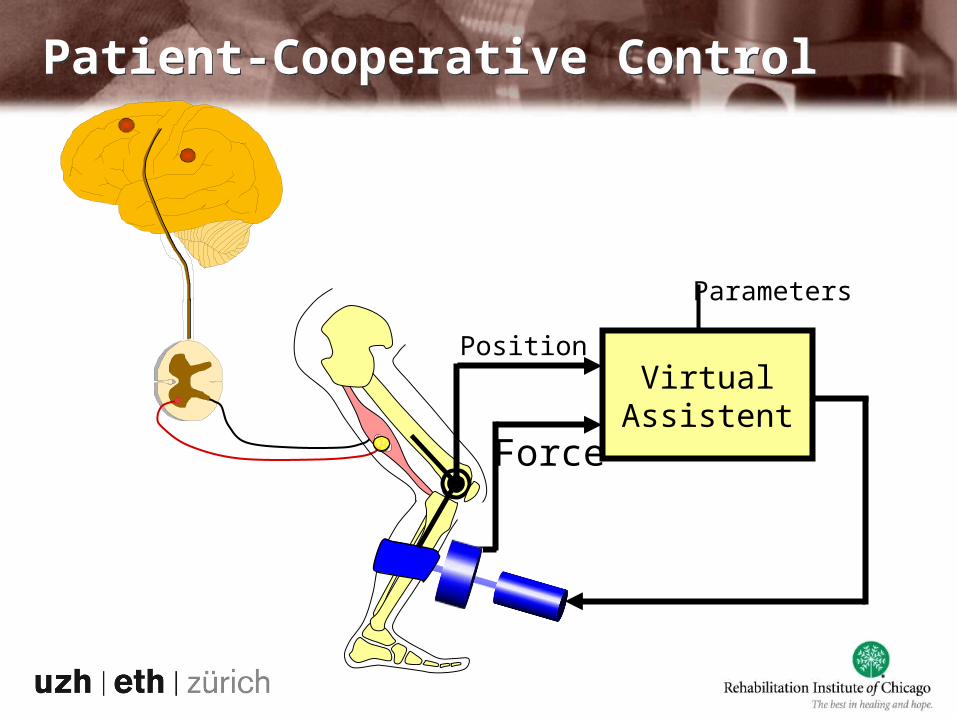
Parameters
VirtualAssistent
Position
Force
Patient-Cooperative ControlPatient-Cooperative Control
Design and evaluate cooperative control strategies that provide more freedom and participation by the patients, while still guaranteeing functional gait training
Assess the effects of cooperative control strategies on stroke patients using quantitative and qualitative measures of gait performance
D1 ObjectivesD1 Objectives

Patient-Cooperative ControlPatient-Cooperative Control
Goal: Active patient participation
Prerequisites-Transparency: “Hide” the robot
when not needed
-Constraints: Keep patient
within safe domain
Goal: Active patient participation
Prerequisites-Transparency: “Hide” the robot
when not needed
-Constraints: Keep patient
within safe domain
Patient-Cooperative ControlPatient-Cooperative Control
Transparency: Task FormulationTransparency: Task Formulation
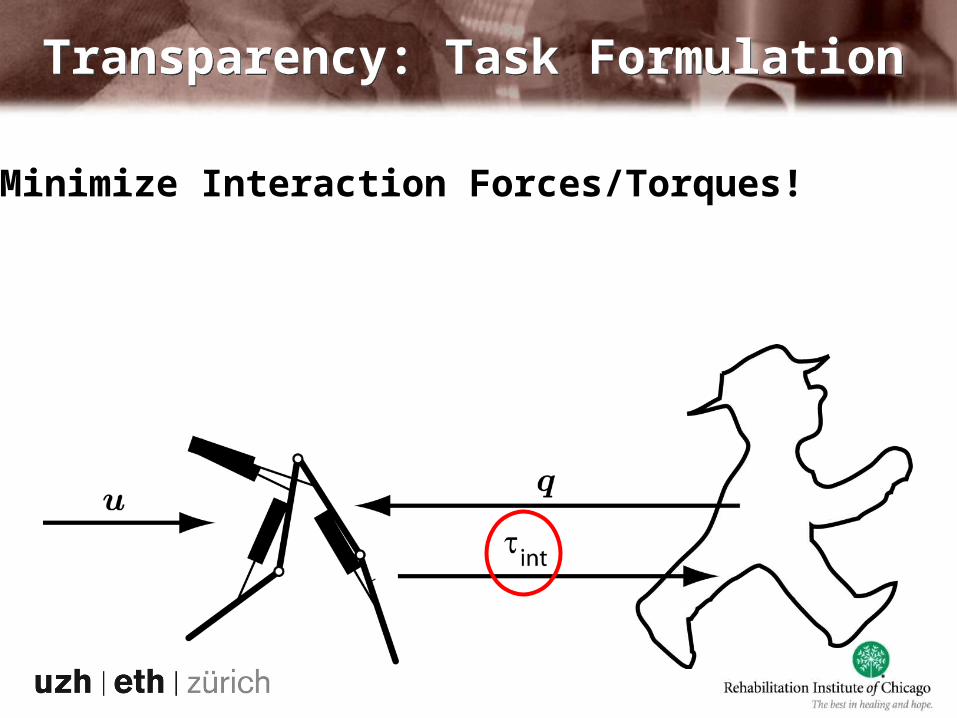
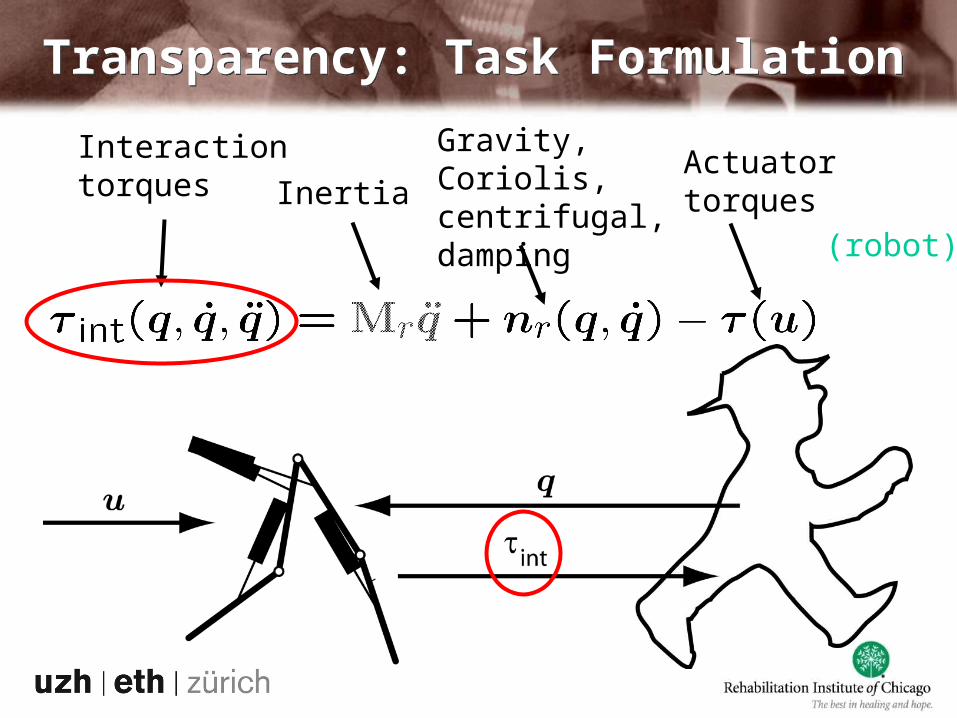
Minimize Interaction Forces/Torques!
Transparency: Task FormulationTransparency: Task Formulation
Interactiontorques Inertia
Gravity, Coriolis,centrifugal,damping
Actuatortorques
(robot)
Example: Mass with 1 DOFExample: Mass with 1 DOF
1. Given Mass (Robot) Connected to Operator (Human)

2. Given Movement of the Operator (Human)
3. Calculate Forces to Let Mass (Robot) Follow
Example: Mass with 1 DOFExample: Mass with 1 DOF
4. Find Optimal Conservative (Elastic) Force Field as Function of Position
5. Apply Force Field by Actuators (Robot)
Example: Mass with 1 DOFExample: Mass with 1 DOF

Multi-Joint Robot: Optimal Force FieldMulti-Joint Robot: Optimal Force Field
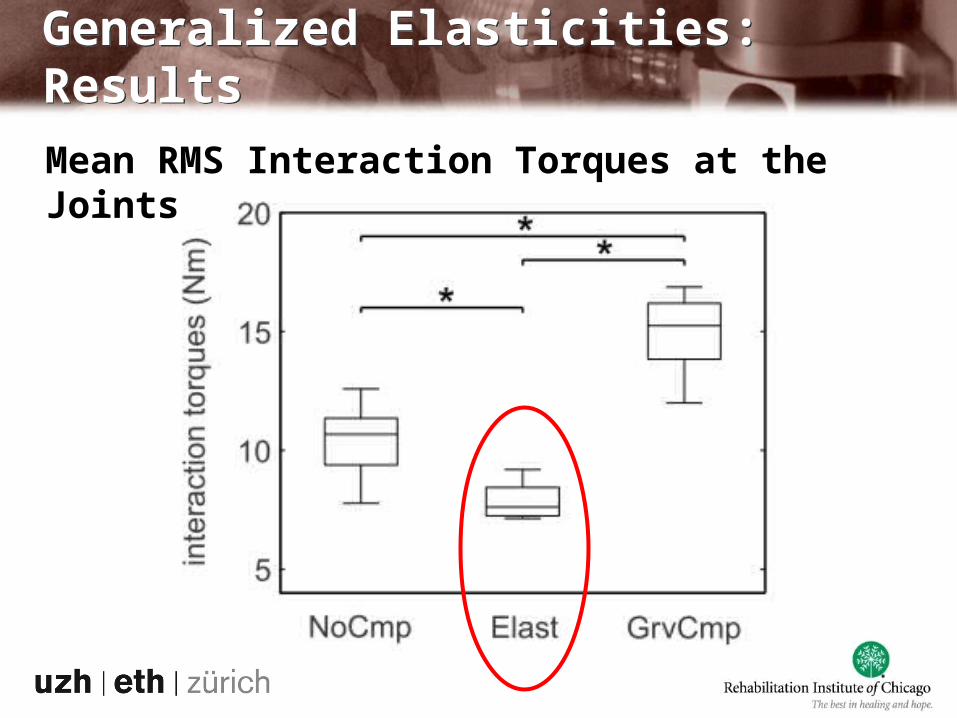
Generalized Elasticities: ResultsGeneralized Elasticities: Results
Mean RMS Interaction Torques at the Joints
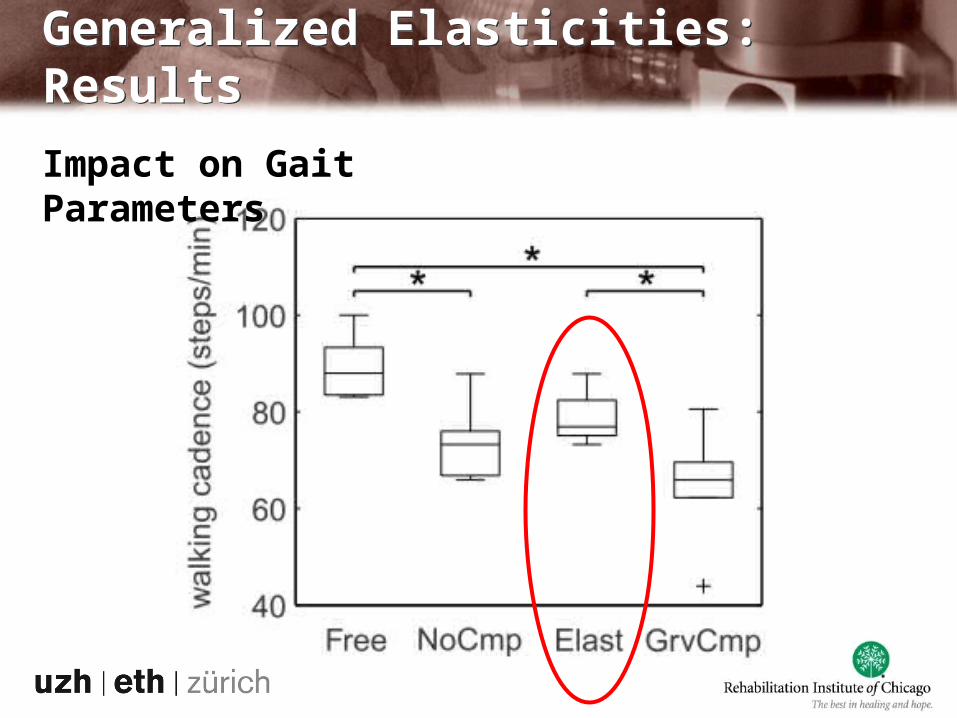
Generalized Elasticities: ResultsGeneralized Elasticities: Results
Impact on Gait Parameters
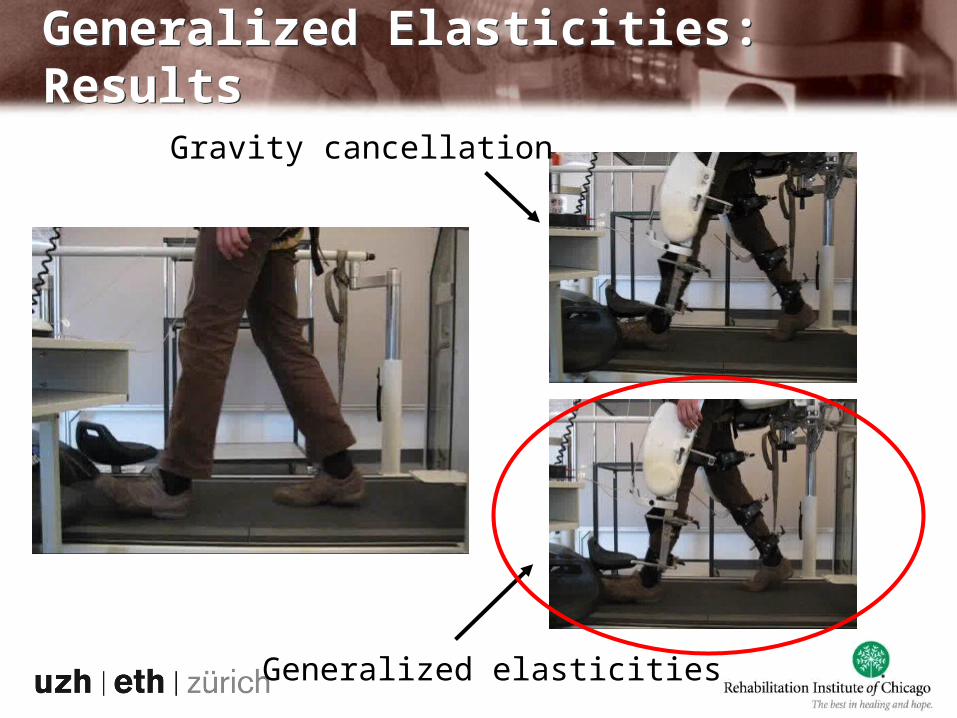
Generalized Elasticities: ResultsGeneralized Elasticities: Results
Gravity cancellation
Generalized elasticities
Goal: Active patient participation
Prerequisites:-Transparency: “Hide” the robot
when not needed
-Constraints: Keep patient
within safe domain
Patient-Cooperative ControlPatient-Cooperative Control
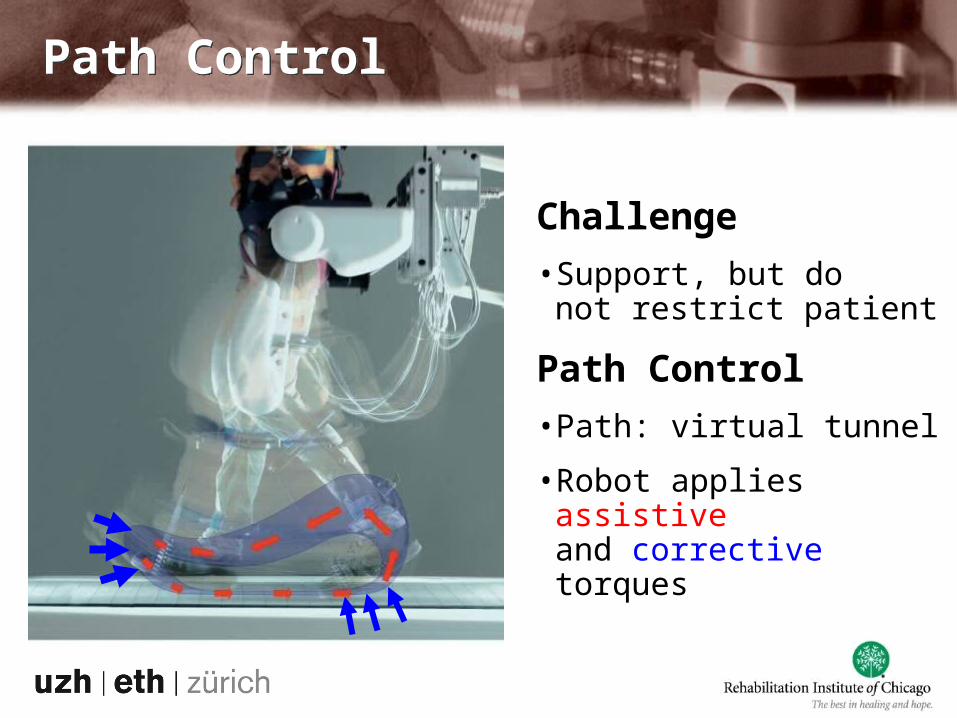
Challenge
•Support, but do not restrict patient
Path Control
•Path: virtual tunnel
•Robot applies assistive and corrective torques
Path ControlPath Control

Path ControlPath Control
1 (hip angle)
2 (
knee a
ng
le)
φrefφact
F
allowed region
reference pathIdeaCombine free timing with spatial guidance
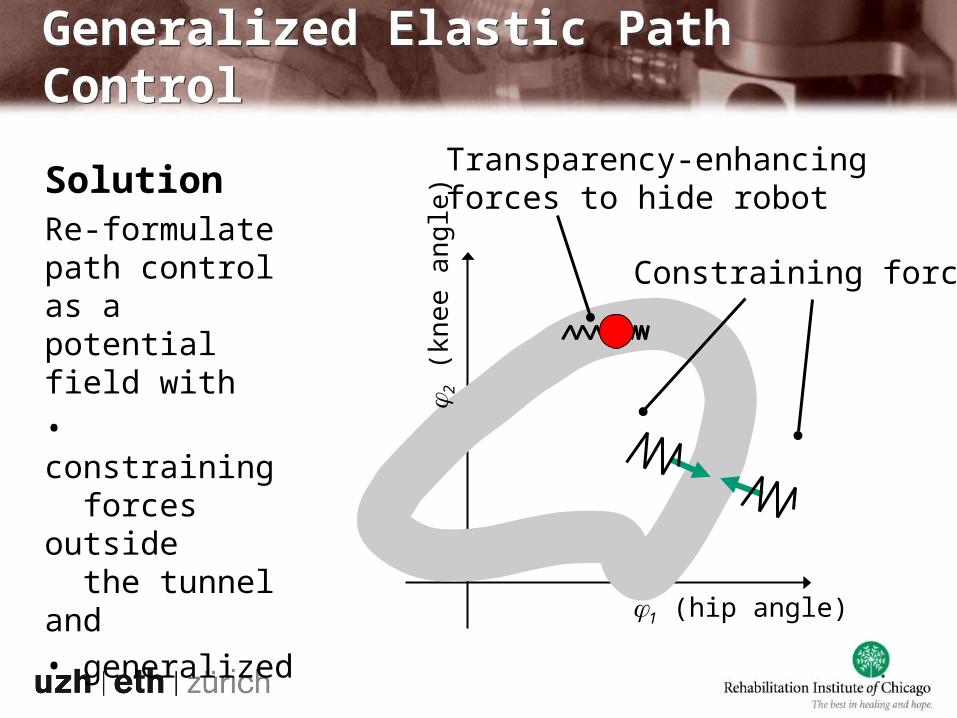
Generalized Elastic Path ControlGeneralized Elastic Path Control
Solution
Re-formulate path control as a potential field with• constraining forces outside the tunnel and• generalized elasticities inside the tunnel.
1 (hip angle)
2 (
knee a
ng
le)
Constraining forces
Transparency-enhancing forces to hide robot
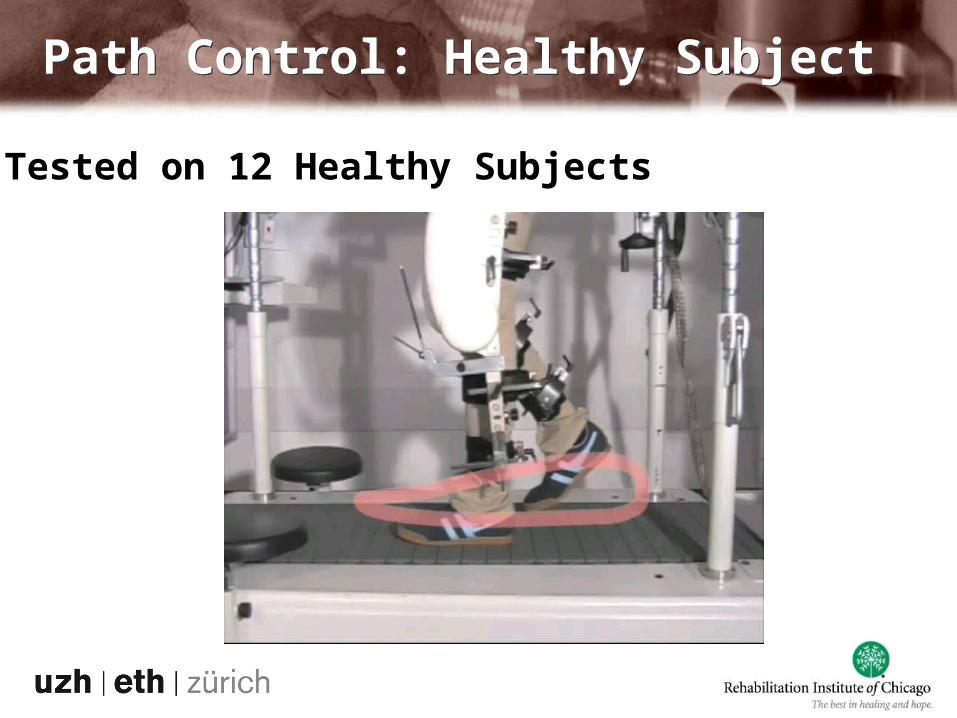
Path Control: Healthy SubjectPath Control: Healthy Subject
Tested on 12 Healthy Subjects

Path Control: iSCI SubjectPath Control: iSCI Subject

Pos Path_a Path_b Imp
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Hf rz
*
Muscle Activity Heart Rate
Pos.contr.Path contr.
0.06
0.08
0.1
0.12
0.14
0.16
0.18
0.2
0.22
0.24
Init. loading
Mid stance
Term. stance
Pre swing
Init. swing
Mid Swing
Term. swing
Nor
mal
ized
mus
cle
activ
ity (
BF
)
Position controlPath control
Rela
tive incr
ease
of
heart
rate
14 incomplete SCI subjects
Path Control Increases ParticipationPath Control Increases Participation
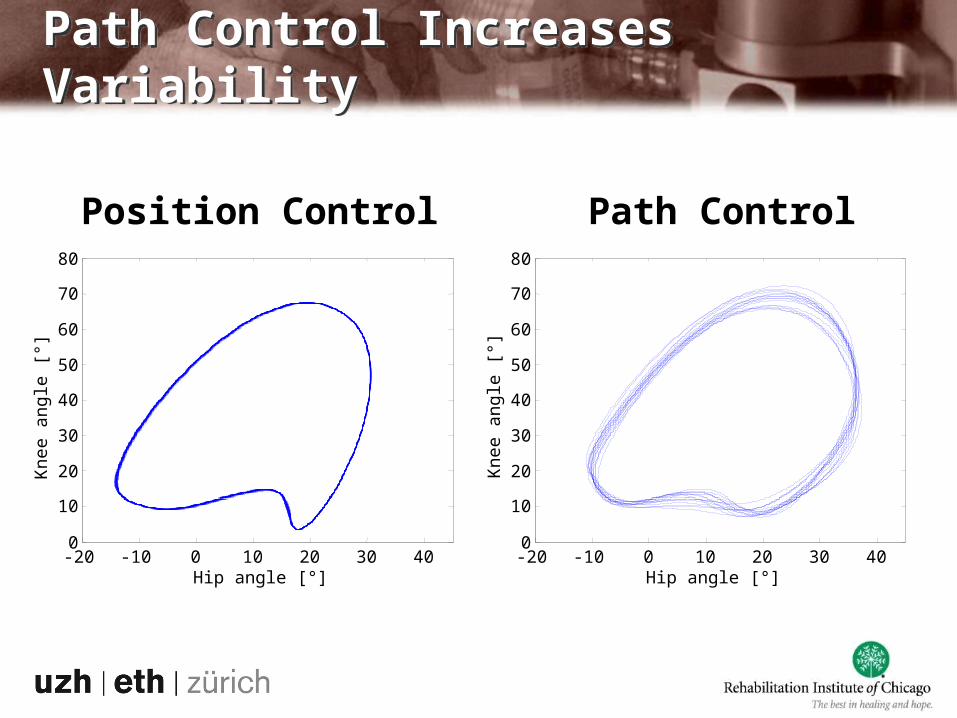
Path Control Increases VariabilityPath Control Increases Variability
Position Control
-20 -10 0 10 20 30 400
10
20
30
40
50
60
70
80
Hip angle [°]
Kne
e an
gle
[°]
Path Control
-20 -10 0 10 20 30 400
10
20
30
40
50
60
70
80
Hip angle [°]
Kne
e an
gle
[°]
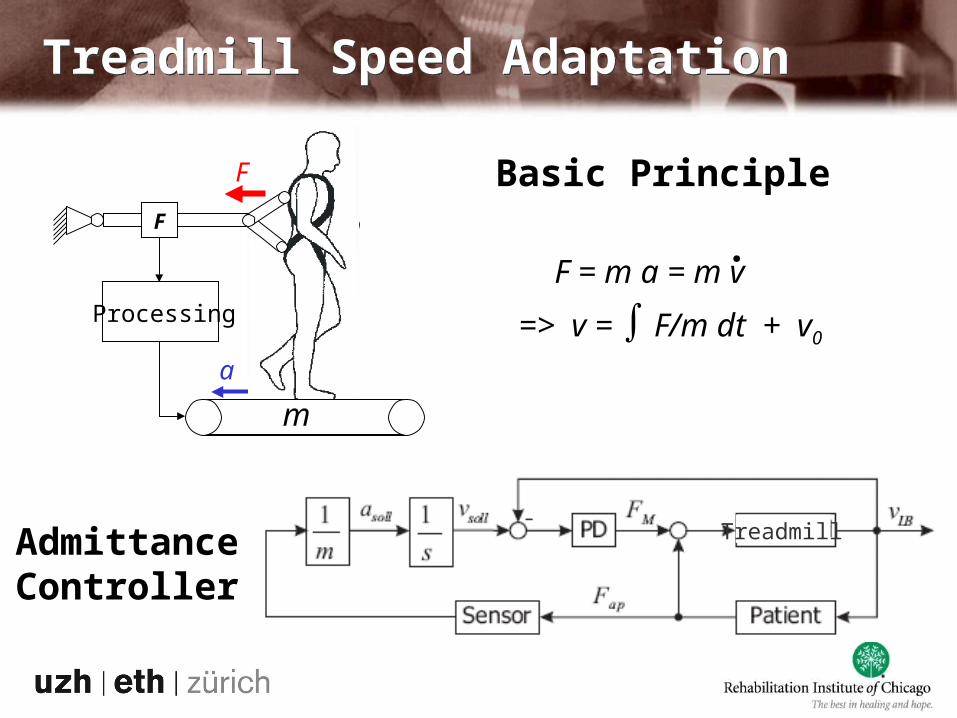
Treadmill Speed AdaptationTreadmill Speed Adaptation
Basic Principle
F = m a = m v.
Admittance Controller
Treadmill
F
a
a
mF
Processing
F
m
=> v = ∫ F/m dt + v0
Is that enough?Is that enough?
Video courtesy of Klinik Valens

Lokomat Extension from 4 to 7 DoFLokomat Extension from 4 to 7 DoF
4 active DoF
1 1
11
7 active DoF
1 1
2 21

Components of 7DoF ControlComponents of 7DoF Control
5 DoF Generalized Elastic Path Control:Hip and knee flexion+ pelvis translation
6 DoF collision avoidance:Hip and knee flexion+ hip abduction
2 x 1 DoF abduction limitation:Abduction only
Evaluation on Stroke Patients at the RIC Evaluation on Stroke Patients at the RIC

Shift to Clinical EvaluationShift to Clinical Evaluation
2009 2010
Balgrist, 4 DoFHealthy; SCI pilot
RIC, 4 DoFStroke pilot
Balgrist, 7 DoFTests on healthies
RIC, 7 DoF Stroke pilot
RIC,Stroke study
today
Balgrist, 7 DoF Multicenter RCT with iSCI?










![Robot for Coaching during Gait Training with Lokomat ... · Nowadays, Lokomat (Hocoma, Switzerland) is the gold standard device in these sessions [21]. The Lokomat is a robotic orthotic](https://img.dokumen.tips/doc/110x75/6007770419c94942d320f0db/robot-for-coaching-during-gait-training-with-lokomat-nowadays-lokomat-hocoma.jpg)


















