Embed Size (px)
Citation preview

Jennifer A. Harvey, MDViktor E. Bovbjerg, PhD
Index terms:Breast, density, 00.92Breast neoplasms, diagnosis, 00.30Breast neoplasms, radiography,
00.11, 00.1215, 00.30Radiography, digital, 00.1215Review
Published online before print10.1148/radiol.2301020870
Radiology 2004; 230:29–41
Abbreviations:BI-RADS � Breast Imaging Reporting
and Data SystemHRT � hormone replacement
therapy
1 From the Departments of Radiology(J.A.H.) and Health Evaluation Sci-ences (V.E.B.), University of Virginia,Box 800170, Charlottesville, VA22908. Received July 18, 2002; revi-sion requested August 27; revision re-ceived October 23; accepted January8, 2003. Address correspondence toJ.A.H. (e-mail: [email protected]).© RSNA, 2003
Quantitative Assessment ofMammographic BreastDensity: Relationship withBreast Cancer Risk1
Increased mammographic breast density is a moderate independent risk factor forbreast cancer, with findings of published studies in which quantitative methods ofassessment were used showing a positive association. Breast density may be quan-tified by using visual assessment or planimetry. Although the category definitionsvary, the odds ratio for developing breast cancer for the most dense compared withthe least dense breast tissue categories ranges from 1.8 to 6.0, with most studiesyielding an odds ratio of 4.0 or greater. Plausible explanations for the association ofbreast density with increased breast cancer risk may be the development of prema-lignant lesions such as atypical ductal hyperplasia, elevated growth factors, orincreased estrogen production within the breast due to overactive aromatase. Theamount of breast density may be due in part to genetic heredity. However, unlikeother risk factors, breast density may be influenced. Specifically, breast density isvery hormonally responsive and potentially may be influenced by lifestyle factorssuch as alcohol intake and diet. Assessment of breast density may become useful inrisk assessment and prevention decisions.© RSNA, 2003
Breast density is perhaps the most undervalued and underutilized risk factorin studies investigating the causes of breast cancer.
Celia Byrne (1)
In 1976, Wolfe published an article that demonstrated a relationship between breastdensity and breast cancer risk (2). However, investigators of subsequent studies either didnot reproduce the association (3,4) or did not show the association to be as strong as thatin the Wolfe original report (5–7). Reader inconsistency issues also caused doubt as to theusefulness of the Wolfe density classification scheme (6,8), which fell into disuse in thiscountry in the 1980s, although it is still commonly used outside of the United States.
Beginning in the early 1980s, more precise quantitative methods of measuring breastdensity were developed. Since 1982, to our knowledge 12 studies (9–20) in which quan-titative methods were used for assessing breast density have been performed; findings of allthese studies showed a positive moderate association with breast cancer risk. The risk ofbreast cancer for women with increased breast density in most of these studies is four tosix times that for women with less dense tissue, a relative risk greater than most traditionalrisk factors such as nulliparity and early menarche. Unlike most other breast cancer riskfactors, breast density may be influenced by hormonal agents, alcohol use, and possiblyother means.
In this article, we review normal changes in breast composition over time, methods ofmeasuring breast density, the association of breast density measured with quantitativemethods to breast cancer risk, alternative explanations for the association, how hormonaland other factors are associated with breast density, and plausible reasons that increasedbreast density increases breast cancer risk. Last, we examine potential future directions foruse of quantitative assessment of breast density in relation to breast cancer risk.
Review
29
Ra
dio
logy

CHANGES IN BREASTCOMPOSITION OVER TIME:NORMAL PHYSIOLOGY
Premenopause
The mature breast undergoes cyclicchanges during the menstrual cycle. Es-trogen increases cell proliferation andprogesterone enhances this effect. Dur-ing the follicular phase, cell proliferationincreases and is further enhanced duringthe luteal phase (21). There is also anincrease in breast volume and water con-tent during the luteal phase of the cycle(22). Hypertrophy, or enlargement of in-dividual cells, may also contribute to theincrease in breast volume during this por-tion of the menstrual cycle, although lit-tle information exists regarding cellularhypertrophy during the menstrual cycle.Acute deprivation of estrogen and pro-gesterone causes an increase in celldeath, or apoptosis, which peaks duringthe time of menstrual bleeding (23). Onmammograms, these changes are re-flected by greater breast density duringthe luteal phase than during the follicu-lar phase (24,25).
As women near menopause, the men-strual cycle shortens. Specifically, the fol-licular phase shortens, with no signifi-cant change in the length of the lutealphase. This continues until the onset ofoligomenorrhea. During the perimeno-pausal years, preovulatory estradiol levelstend to be higher than they are inyounger women, while progesterone lev-els remain similar. Breast cysts are themost common form of breast lumps be-tween ages 40 and 49 years, possibly dueto the shortened follicular phase and el-evated estrogen levels during this time.The breasts continue to become lessdense, with about 50% of women in their40s and about 65% of women in their 20shaving 50% or greater breast density (26).
Menopause
With the reduction of estrogen andprogesterone levels after menopause, thecyclic proliferative process becomes qui-escent. Lobular tissue regresses, while themore proximal portions of the ductal sys-tem remain. The mammographic appear-ance of the breasts becomes increasinglyradiolucent (26), with about 34% ofwomen aged 75–79 years having fat-re-placed breasts compared with only 11%of women aged 25–29 years. Likewise,only 30% of women aged 75–79 yearshave 50% or greater breast density (26).
METHODS OF MEASURINGBREAST DENSITY
Wolfe applied a method of classificationof parenchymal patterns that used qual-itative, as well as quantitative criteria.The following are the descriptions pro-vided by Wolfe (2): N1 category refers toparenchyma composed primarily of fatwith, at most, small amounts of dyspla-sia; no ducts are visible. P1 category refersto parenchyma composed chiefly of fat,with prominent ducts in the anterior por-tion up to one-fourth the volume ofbreast; also may be a thin band of ductsextending into a quadrant. P2 categoryrefers to severe involvement, with prom-inent ductal pattern occupying morethan one-fourth the volume of breast. DYcategory refers to severe involvementwith dysplasia, often obscures an under-lying prominent ductal pattern.
The Wolfe classification has been ap-plied inconsistently. In a 1993 review,Oza and Boyd (27) found that the Wolfeclassification had an interobserver agree-ment of 52%–97% and an intraobserveragreement of 69%–97%. Authors of case-control and cohort studies have found anassociation between increased breast can-cer risk and the Wolfe P2 and DY catego-ries, although no association was as highas that in the original report by Wolfe(28). Findings of cross-sectional studieshave shown a weak association or no as-sociation (27).
Attempts to develop a reproduciblequantitative method of assessing breastdensity began in the early 1980s (9). Vi-sual estimation of the percentage of thebreast occupied by breast tissue has beenused frequently, with the number of cat-egories varying from five (9) to 20 (29),with the most frequently used method asproposed by Boyd et al (10) having sixcategories. Agreement for visual assess-ment was very good, with intrareader re-liability estimation of 0.82 reported inone 20-category study (30) and � value of0.89 (31) and intraclass correlation coef-ficient of 0.94 (10) reported in the six-category studies.
In the United States, the Breast Imag-ing Reporting and Data System (BI-RADS)was developed to standardize mammog-raphy reporting terminology and the as-sessment and recommendation catego-ries (32). BI-RADS density classification isincluded in the report to inform referringphysicians of the decline in sensitivity ofmammography with increasing breastdensity. It was not intended to serve as amethod of measuring breast density. The
four-category system (almost entirely fat;scattered fibroglandular densities; hetero-geneously dense, may lower the sensitivityof mammography; extremely dense, whichcould obscure a lesion on mammogra-phy) is based on quantitative assessment,although the categories are not definedby the percentage of density. The lack ofwell-defined categories likely accounts forthe only moderate interobserver agree-ment seen with the use of BI-RADS densitycategories, with an overall � value of 0.43–0.59 (33,34). However, the advantage of theBI-RADS classification is that it is widelyused in the United States and allows anal-ysis of large study populations (18).
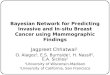
More consistent computer-assisted mea-surements of breast density have been de-veloped. All methods use planimetry insome way. Computer-assisted planimetrywas used as early as 1987 (11). With thismethod, an acetate overlay was placed overthe mammogram, and the outline of thebreast and breast tissue was made by usinga wax pencil. A computerized compensat-ing planimeter was then used to obtain thetotal area of the breast and the total area ofthe breast tissue (11–13). The percentage ofdensity is then calculated by dividing thearea of the breast tissue by the total area ofthe breast. Agreement with this method is70%–94% (11,12). More recently, filmmammograms have been digitized, andthe area of the breast parenchyma and thetotal area of the breast are outlined by us-ing either a mouse (25) or a digital segmen-tation of the mammogram (35,36). Withthe digital segmentation method, the his-togram of the digitized mammogram is di-vided into fatty tissue and parenchyma byusing interactive thresholding (35) (Fig 1).Agreement with this method is reported tobe 90% or greater (35). Other investigators(37–40) are developing automated calcula-tion of the percentage of density by usingsegmentation, with promising results, andmost recent methods yielded 80%–90%agreement with radiologist assessment ofdensity (38–40).
A limitation of the current planimetrymethods is that the pixels are used in abinary fashion (fat or parenchyma) with-out the actual depth of the pixel beingtaken into account. Thus, a pixel con-taining a small amount of breast tissue isconsidered the same as one with a largeamount of breast tissue. Taking pixel depthinto account would add some three-di-mensional information about the breast.An additional limitation of any methodthat may be very important when assessinga change in density over time is variationin film exposure factors. Changes in expo-sure, compression, and processor chemis-
30 � Radiology � January 2004 Harvey and Bovbjerg
Ra
dio
logy

try may influence the background densityof the film and potentially the measuredbreast density.
Another problem receiving increasingattention is that use of the percentage ofmammographic density represents only atwo-dimensional representation of athree-dimensional phenomenon. Womenwith large breasts may have a substantialamount of glandular breast tissue yet havelow breast density percentages. On theother hand, women with small breasts andreduced amounts of glandular tissue mayhave a higher percentage of breast density.A number of investigators are trying to de-vise a means of determining the total glan-dular content from three-dimensional re-construction of breast (Shephard J, oralcommunication, July 2002). It may be thatthis parameter would be a better predictorof breast cancer than quantification of
density based on current two-dimensionaltechniques. Further studies are ongoing toaddress this issue in a meaningful way(Cummings S, oral communication, July2002).
Other investigators are exploring the useof magnetic resonance imaging (41,42)and ultrasonography (43) for quantifyingbreast density, although these methodsmay not prove as useful for widespread useas density information already obtained onthe mammogram. Shephard et al (44) arealso investigating the use of dual x-ray ab-sorptiometry for measuring breast density.
RELATIONSHIP OF BREASTDENSITY AND BREASTCANCER RISK
In 1976, Wolfe proposed the positive as-sociation of qualitatively assessed breast
density and breast cancer risk (2). How-ever, subsequent reports primarily showedan association with case-control studiesbut it was not reproduced in many prev-alence studies, and the association wasquestioned. In 1987, Saftlas and Szklo(28) reviewed the studies that were per-formed to that date by using the Wolfecriteria and concluded that the mostcarefully conducted studies supported anassociation of breast cancer risk and theWolfe classification, but that lack of con-sistency in applying the parenchymalpattern classification was a major prob-lem when findings between investigatorswere compared.
Since 1982, authors of at least 12 stud-ies have reported an association of breastdensity with breast cancer risk by usingquantitative methods (Table) (9–20).Findings of all these studies have showna moderate to strong positive associationof increased breast cancer risk withhigher levels of breast density. All wereeither population-based or clinic-basedcase-control studies, and several werenested within large cohort populations.All studies were substantial in size, withmore than 150 cases, and half of thestudies had two or more controls for eachcase. In all studies, radiologists wereblinded to the case or control status.
Findings of all 12 studies in whichquantitative methods were used in as-sessing breast density showed a signifi-cant increase in breast cancer risk forwomen with the highest levels of breastdensity. Although the category defini-tions vary, the odds ratio for the mostdense compared with the least dense cat-egories ranges from 1.8 to 6.0, with moststudies yielding an odds ratio of 4.0 orgreater. The Maskarinec and Meng study(20) had the lowest risk and was com-posed of an ethnically diverse populationin Hawaii that included Asian and NativeHawaiian women known to be at lowerrisk of breast cancer.
Eight of these studies used both theWolfe classification and quantitative as-sessment of breast density; in all but theWolfe et al (11) and Kato et al (13) stud-ies, the quantitative analysis showed astronger association with breast cancerrisk than did the Wolfe classification,which suggests that quantitative meth-ods may be more useful in identifyingwomen at increased risk for developingbreast cancer.
Sala et al (45) report a positive associa-tion with higher histologic grade tumorsand mammographic density assessed byusing Wolfe criteria. In this issue of Radi-ology, Roubidoux et al (46) report a
Figure 1. Quantitative assessment of breast density with a computerized thresholding method(35). The computer interface is demonstrated. With this technique, the digitized mammogram isdisplayed. The red line marks the skin edge and is controlled by the bar labeled “Edge Threshold”in the threshold panel. The green line marks the breast parenchyma and is controlled by the barlabeled “Density Threshold.” The user can move either bar to select the appropriate skin line andthe area of breast tissue. The user draws a line to denote the boundary of the pectoralis muscle andthat area is excluded. Two other masks can be used to exclude markers, et cetera. The total, densearea, and percentage of density are then calculated. In this example, the breast is 26.5% dense.(Image courtesy of Martin Yaffe, University of Toronto).
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 31
Ra
dio
logy

Sum
mar
yo
fSt
udie
sEv
alua
tin
gB
reas
tD
ensi
tyb
yQ
uan
tita
tive
Ass
essm
ent
and
Bre
ast
Can
cer
Ris
k
Stud
yan
dYe
arSt
udy
Typ
eSt
udy
Pop
ulat
ion*
No.
ofC
ases
/C
ontr
ols
Tim
ebe
twee
nD
ensi
tyM
easu
rean
dC
ase
Asc
erta
inm
ent
Wol
feO
dds
Ratio
†Q
uant
itativ
eO
dds
Ratio
95%
CI
Qua
ntita
tive
Met
hod
Thre
shol
d(%
)A
djus
tmen
ts
Boyd
etal
,19
82(9
)C
ase-
cont
rol
Wom
en’s
Col
lege
Hos
pita
l,To
ront
o,C
anad
a
183/
183
Sim
ulta
neou
s1.
9–3.
7‡2.
8–6.
0‡1.
4,5.
62.
5,14
.1Vi
sual
�10
vs�
75A
geat
first
birt
h,p
arity
,fa
mily
hist
ory
Bris
son
etal
,19
82(1
4)C
ase-
cont
rol
Two
Bost
onho
spita
ls(1
972–
1978
)
408/
1,02
10–
12m
o4.
03.
8–5.
4§1.
6,8.
72.
5,11
.4Vi
sual
0vs
�60
Parit
y,ag
eat
first
birt
h,fa
mily
hist
ory,
age
atm
enop
ause
,ho
rmon
eus
eBr
isso
net
al,
1984
(15)
Cas
e-co
ntro
lTh
ree
Bost
onho
spita
ls(1
978–
1982
)
362/
686
0–12
mo
2.7
2.0–
4.4§
2.5,
7.9
Visu
al0
vs�
60W
eigh
t,he
ight
Wol
feet
al,
1987
(11)
Cas
e-co
ntro
lH
utze
lHos
pita
l,D
etro
it,M
ich
(197
9–19
82)
160/
160
Sim
ulta
neou
s12
.24.
31.
8,10
.4M
anua
lp
lani
met
ry�
25vs
�70
Parit
y
Bris
son
etal
,19
89(1
6)C
ase-
cont
rol
Que
bec
City
(198
2–19
84)
290/
645
Sim
ulta
neou
s3.
75.
5§2.
3,13
.2Vi
sual
0vs
�60
Age
,p
arity
,ed
ucat
ion,
wei
ght,
heig
htSa
ftas
etal
,19
91(1
2)C
ase-
cont
rol
nest
edin
coho
rt
BCD
DP
(197
3–19
75)
260/
301
5y
2.6
4.3
2.1,
8.8
Man
ual
pla
nim
etry
�5
vs�
65A
ge,
wei
ght,
par
ity
Boyd
etal
,19
95(1
0)C
ase-
cont
rol
nest
edin
coho
rt
NBS
S35
4/35
41–
5y
NA
NA
6.0
4.0
2.8,
13.0
2.1,
7.7
Visu
alC
omp
uter
ized
(thr
esho
ldin
g)
0vs
�75
Age
,p
arity
,ag
eat
first
birt
h,w
eigh
t,he
ight
,ag
eat
men
arch
e,fa
mily
hist
ory
Kato
etal
,19
95(1
3)C
ase-
cont
rol
nest
edin
coho
rt
NYU
Wom
en’s
Hea
lthSt
udy
(198
5–19
91)
197/
521
0–5.
5y
10.5
(pre
men
opau
sal)
0.7
(pos
tmen
opau
sal)
3.6
(pre
men
opau
sal)
2.1
(pos
tmen
opau
sal)
1.7,
7.9
1.1,
3.8
Man
ual
pla
nim
etry
�48
vs�
65(p
rem
enop
ausa
l)�
28vs
�44
(pos
tmen
opau
sal)
Body
mas
sin
dex,
par
ity,
men
opau
sals
tatu
s
Byrn
eet
al,
1995
(17)
Cas
e-co
ntro
lne
sted
inco
hort
BCD
DP
(197
3–19
80)
1,88
0/2,
152
1–16
y2.
74.
33.
1,6.
1C
omp
uter
ized
pla
nim
etry
0vs
�75
Wei
ght,
age
atfir
stbi
rth,
fam
ilyhi
stor
y,ed
ucat
ion,
alco
holu
se,
prio
rbi
opsi
es,
rep
rodu
ctiv
eye
ars
Lam
etal
,20
00(1
8)C
ase-
cont
rol
nest
edin
coho
rt
VBC
SS(1
996–
1997
)52
9/2,
116
6m
oto
2y
NA
4.5
1.9,
10.6
BIRA
DS
Entir
ely
fatt
yvs
extr
emel
yde
nse
Wei
ght
Van
Gils
etal
,19
99(1
9)C
ase-
cont
rol
nest
edin
coho
rt
Nijm
egen
Brea
stC
ance
rSc
reen
ing
Prog
ram
(198
5–19
94)
108/
400
10y
NA
3.3
1.5,
7.2
Com
put
eriz
ed(a
utom
ated
)�
5vs
�25
Men
opau
sals
tatu
s,Q
uete
let
inde
x
Mas
karin
ecan
dM
eng,
2000
(20)
Cas
e-co
ntro
lKa
iser
Perm
enen
teH
awai
i(19
91–
1997
)
647/
647
85%
with
in1
y(m
ean,
6m
o)
NA
1.8
1.1,
3.0
Com
put
eriz
ed(t
hres
hold
ing)
�10
vs�
50A
geat
men
arch
e,m
enop
ausa
lsta
tus,
par
ity,
age
atfir
stbi
rth,
fam
ilyhi
stor
y,ho
rmon
eus
e,p
revi
ous
brea
stp
robl
ems
*BC
DD
P�
Brea
stC
ance
rD
etec
tion
Dem
onst
ratio
nPr
ojec
t,N
BSS
�C
anad
ian
Nat
iona
lBre
ast
Can
cer
Scre
enin
gSt
udy,
NYU
�N
ewYo
rkU
nive
rsity
,VBC
SS�
Verm
ont
Brea
stC
ance
rSu
rvei
llanc
eSy
stem
.†
NA
�no
tap
plic
able
.‡
Rang
eof
thre
ere
adin
gra
diol
ogis
ts.
§Pe
rcen
tage
ofno
dula
ror
duct
altis
sue
occu
pyi
ngth
ebr
east
.
32 � Radiology � January 2004 Harvey and Bovbjerg
Ra
dio
logy

higher incidence of invasive breast can-cers that are estrogen-receptor negative,are of higher histologic grade, and are oflarger size in women with dense breasttissue that had negative clinical andmammographic screening findings within17 months of diagnosis. However, authorsof the study found that only tumor sizewas independent of age. The authors pos-tulate that the association between largertumor size and dense tissue at mammogra-phy may be due to either more rapidgrowth in glandular breasts or increaseddifficulty in detection due to the dense tis-sue.
Attributable Risk
Higher levels of breast density are fairlycommon, since 50% of women betweenthe age of 40 and 49 years and 30% ofwomen aged 70–79 years have breaststhat are at least 50% dense (26). If breastdensity is a moderate risk factor and therisk factor is fairly common, breast can-cers attributable to increased breast den-sity could potentially account for an im-portant percentage of total breast cancercases. In two studies, attributable riskfrom increased breast density was 28%–30% for 50% or greater density and 40%–44% for any breast density (10,17). Incomparison, less than 5% of breast can-cers are attributable to breast cancer gene(BRCA1 and BRCA2) mutations.
Breast cancers attributable to densebreast tissue may become more prevalentin the future. Blane et al (47) have foundthat for women aged 50–59 years, breastdensity on screening mammograms ob-tained in the 1990s did not decline withage as rapidly as that seen in the 1980s,even in those women not undergoinghormone replacement therapy (HRT).Authors of that study did not control forsuch factors as parity, age at first birth, orweight; therefore, slower involution ofthe breast may be due to these or othercauses. Regardless of the cause, findingsof the study suggest that if breast densityis a moderate risk factor for developingbreast cancer, then the attributable riskdue to density may become more signif-icant in our population.
Dose Response
If high breast density is a risk factor forbreast cancer compared to fat-replacedbreasts, then increasing density shouldbe associated monotonically with in-creasing risk. Boyd et al (48) reviewed theearliest nine of the 12 studies cited in theTable and found a positive trend in all
but the Wolfe study (11). In four studies(10,12,13,17), statistical evaluation fortrend was significant (P � .001 to P �.0001). This implies that the breast can-cer risk increases in proportion to thedegree of breast density.
In addition, if the relationship be-tween breast density and risk is propor-tional, then changing density shouldchange risk. Investigators of one studyhave found a trend of changes in riskwith changes in density (19). In thatstudy, women with 5%–25% density ini-tially had an odds ratio of 5.7 (95% CI:2.2, 15.2) for developing breast cancer iftheir density did not change over an8-year interval. However, if their breastdensity decreased to less than 5% duringthe interval, then the odds ratio for de-veloping breast cancer was only 1.9 (95%CI: 0.6, 6.1), while those with an increasein density to 25% or greater had an oddsratio of 6.9 (95% CI: 2.1, 22.9) (19). Thiswas a small study with wide CIs, and thefindings should be confirmed in largerstudies.
ALTERNATIVE EXPLANATIONSFOR THE LINK BETWEENBREAST DENSITY ANDCANCER RISK
Density Is a Marker but Not anIndependent Risk Factor
Breast density may reflect increasedrisk due to other causes or it may be anindependent risk factor. While weight,body mass index, age, menopausal sta-tus, age at first birth, nulliparity, familyhistory, hormone use, and previousbreast biopsy may all influence breastdensity, breast density is identified con-sistently as an independent risk factorafter adjustment for other variables asso-ciated with both density and breast can-cer risk (17,18). Regardless of the ulti-mate cause of breast density and itsassociation with risk, if density is a mod-erate predictor of risk, it may be a usefulmarker for disease risk even if it is only amore proximal link in a longer chain ofcausality.
“Masking” Explains the ApparentAssociation of Density toIncreased Risk
Egan and Mosteller (49) proposed themasking hypothesis to explain the appar-ent relationship of breast density andbreast cancer risk. Because cancers aremore difficult to detect in dense breasttissue, prevalent cancers may be morelikely to be missed at the first screening
among women with dense tissue. Whenthe tumors are detected later as apparentincident cancers, a spurious associationmay arise between the breast cancer riskand tissue density. Evaluation of a rela-tionship between density and breast can-cer risk from mammograms obtained inthe 1st year or 2 years after initial screen-ing may artificially suggest that density isa risk factor for breast cancer. However, ifbreast density was not a risk factor forbreast cancer, then at some future pointafter the initial screening, cancer inci-dence in women with dense and in thosewith fatty breasts should become similar.In addition, findings in studies in whichcancer diagnosis is evaluated at the timeof the initial screening examinationshould show fewer cancers in womenwith dense breast tissue than in womenwho have fat-replaced breast tissue.
A small study (50) was performed ex-amining the possible effect of maskingon the relationship of breast density andcancer risk. Authors of the study foundthat increased density defined as morethan 25% of the breast occupied by fi-broglandular tissue was associated with arelative risk of 1.4 at the initial screeningexamination, 1.2 at 1–2 years, 3.3 at 3–4years, and 1.2 at 5–6 years (50). Thesefindings are consistent with the hypoth-esis that masking of cancers in densebreast tissue does occur, although the ef-fect is small and peaks 3–4 years after theinitial screening examination. Masking,however, does not explain the increasedrelative risk of breast cancer for womenwith dense breast tissue at study entry,since cancers that are masked within thedense tissue should result in a lower de-tection and therefore lower apparent rel-ative risk. Of note, the study (50) usedmammograms obtained in the 1970s,which were much lower in contrast thanare those obtained by using more mod-ern techniques.
Masking bias was less likely to occur instudies that had an initial period duringwhich tumors were excluded from thestudy (10,17) or had a longer period be-tween initial screening and case statusascertainment (12,19). Studies performedon the basis of cohorts with long-termfollow-up that examine density and riskusing mammograms obtained in a regu-larly screened population should also beless affected by masking (10–13,17,19).Findings of three nested case-controlstudies (10,12,17) have shown that riskremains elevated for at least 5–10 years offollow-up. Byrne et al (17) reported find-ings for women with 10 or more yearsbetween density assessment and case-
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 33
Ra
dio
logy

control determination; among womenwith 0% density, there were 17 cases and42 controls, while among women withdensity greater than 75%, there were 45cases and 29 controls. Therefore, 45(73%) of 62 cases had dense tissue andonly 29 (40%) of 71 controls had densetissue. For masking of prevalent cancersto account for this large difference at 10years after initial screening, the effectwould have to be substantial and long-lived. We estimate that about 75% ofprevalent cancers in women with densebreasts would have been missed and sub-sequently diagnosed 10 or more yearslater to account for this difference, whichis highly unlikely.
Masking has been shown to introducesome bias in the detection of breast can-cer in dense tissue in one small study inwhich older mammograms were used(50). However, the association betweenbreast cancer risk and increased breastdensity was consistent in every quantita-tive study reviewed, from those in whichdensity and disease were ascertainednearly simultaneously (9,11,16) to thosewith up to a decade between density anddisease ascertainment (17,19). Given thefindings of these studies, masking biasdoes appear to occur but likely has only asmall and short-lived effect.
Current but Not Past Density IsAssociated with Increased Risk
In an editorial about breast density,White stated that “disagreement also ex-ists over whether current or past breastdensity serves as the better risk predictor”(51). Since the effect of breast density oncancer risk persists for at least 5–10 yearsafter assessment (10,12,17), past breastdensity appears to be important. On theother hand, findings of one study suggestthat changes in density change risk (19).In that study, reduction of breast densityover time lowered breast cancer risk butnot to the extent as in women with com-parable density at baseline. This impliesthat increased density has some persis-tent effect. Their data also suggest thatduring the 8 years of follow-up, strikingchanges in density were relatively un-common in both cases and controls. Thestudies reviewed here have widely vary-ing times between disease detection anddensity determination (Table), and allshow associations between density andbreast cancer risk. It appears likely thatboth past and current breast density areassociated with risk.
RELATIONSHIP BETWEENNONHORMONAL FACTORSAND BREAST DENSITY ANDBREAST CANCER RISK
Age and Menopausal Status
The association of breast density andbreast cancer risk may be greater for olderwomen. Byrne et al (17) found a greatereffect of breast density on breast cancerrisk in postmenopausal women (odds ra-tio, 5.8; 95% CI: 3.0, 11.3) comparedwith that in premenopausal women(odds ratio, 3.8; 95% CI: 2.3, 6.2). Boyd etal (10) also found a higher risk, withwomen aged 50–59 years having a rela-tive risk of 7.1 (95% CI: 2.0, 25.5) com-pared with women aged 40–49 yearshaving a relative risk of 6.1 (95% CI: 1.5,24.2). Findings of both studies, however,show significant overlap in the CIs,which indicates that neither study find-ings show a strong association betweenincreased breast density and cancer riskaccording to menopausal status. Kato etal (13) found the opposite effect, al-though their study was smaller.
The association of breast density withcancer risk seems counterintuitive giventhat breast cancer risk increases with ad-vancing age at the same time that breastdensity decreases. However, other age-as-sociated factors besides breast density arelikely driving the age-associated increasein breast cancer risk. A parallel situationmay be seen with smoking and the inci-dence of heart disease. As people age,they are more likely to quit smoking (52).However, an 80-year-old nonsmoker ismore likely to die of heart disease than a40-year-old smoker. This does not implythat smoking does not increase the risk ofheart disease, only that other factors be-sides smoking increase the risk of heartdisease. Likewise, other factors besidesbreast density contribute to breast cancerrisk. The association between decreasingbreast density and increasing breast can-cer risk with aging does not negate theassociation between increased breastdensity and breast cancer risk.
Weight and Body Mass Index
Obesity is a known risk factor for breastcancer. Lam et al (18) specifically exam-ined the relationship between weightand body mass index on the associationof breast density and breast cancer risk.They found that women with higherbody weight and body mass index wereless likely to have dense breasts. The un-adjusted odds ratio for developing breastcancer for women who weighed more
than 81 kg compared with those weigh-ing less than 63 kg was 1.7 (95% CI: 1.2,2.6). However, after adjusting for density,the odds ratio increased to 2.1 (95% CI:1.3, 3.2). This increase indicates that den-sity is an independent risk factor and thatwomen who are obese and have densebreasts are at higher risk. Likewise, theunadjusted odds ratio for women withextremely dense breasts was 3.2 com-pared with that in women with predom-inantly fatty breasts. However, when ad-justed for weight and body mass index,the odds ratio increased to 4.5 (95% CI:1.9, 10.6). Sala et al (53) found similarfindings and noted that “this negativeconfounding of two positive risk factorsmeans that the effect of parenchymalpatterns on risk will tend to be underes-timated when not adjusted for body massindex and waist hip ratio and vice versa.”
Parity
Increased breast density is associatedwith nulliparity and late age at first birth(54). van Gils et al (55) examined therelationship of parity and breast densitywith breast cancer risk. In that study, nul-liparous women with fatty breasts werenot at increased risk compared with par-ous women. However, women who werenulliparous with greater than 25% den-sity were 6.6 times more likely (95% CI:2.6, 16.5) to develop breast cancer, whileparous women with greater than 25%density were only 3.6 times (95% CI: 1.7,7.7) more likely develop breast cancer.
Family History
Boyd et al (56) performed a subanalysiswithin the Canadian National BreastScreening Study by examining breastdensity and the influence of family his-tory on breast cancer risk. For womenwith at least one affected first-degree rel-ative, the relative risk of breast cancerwas 11.1 (95% CI: 1.5, 80.4) for womenwith dense breasts compared with thosewith less than 10% density. The authorsconcluded that mammographic densitymay be strongly associated with the riskof breast cancer in women with a familyhistory of the disease. Likewise, Ziv et al(57) have found that women with ex-tremely dense breast tissue were morelikely to have first-degree relatives withbreast cancer.
Benign Breast Disease
Women with benign breast diseasehave a greater risk of breast cancer if theyalso have dense breast tissue than if they
34 � Radiology � January 2004 Harvey and Bovbjerg
Ra
dio
logy

have less dense breast tissue. In patientsparticipating in the Breast Cancer Detec-tion Demonstration Project, an increasedrelative risk of breast cancer was seenwith nonproliferative (relative risk, 5.8;95% CI: 1.8, 18.6) and proliferative (rel-ative risk, 3.2; 95% CI: 1.6, 6.6) benignbreast disease in women with greaterthan 75% density than in women withless than 50% density (58). However,atypical hyperplasia had a higher relativerisk in women with lower breast density(relative risk, 4.1; 95% CI: 2.1, 8.0) thanin women with dense breasts (relativerisk, 2.1; 95% CI: 0.6, 7.0). Therefore, therisk associated with benign breast diseaseis not explained by density alone andvice versa.
Race and Ethnicity
There are little data regarding the dif-ferences in breast density between differ-ent races and ethnic groups. Maskarinecand Meng (20) have found that the asso-ciation between density and breast can-cer risk for Asian women is similar to thatof Caucasian women.
Diet
The relationship between diet andbreast density is not well defined. Find-ings of two studies (16,59) have shownthat high intake of saturated fat is asso-
ciated with greater breast density, butfindings of another study (60) showedlower density. High intakes of vitamins Cand E have been associated with in-creased density (60), while high intake ofvitamin A has been associated with lowerdensity (16). Findings of a 2-year study(61) in which women were randomly as-signed to no intervention or a low-fathigh-carbohydrate diet did not show achange in density.
Intake of both soy protein and soyisoflavones has shown an inverse associ-ation with breast density in Chinesewomen in Singapore (62). Breast cancerrates are lower in Asian countries thanthey are in the United States and WesternEurope (63), and dietary differences, in-cluding soy intake, have been hypothe-sized to contribute to a lowered risk. Soyproducts are high in phytoestrogens,which may displace endogenous estro-gens at hormone-binding sites, decreas-ing the stimulatory effect of endogenousestrogens in the breast (62).
Alcohol
High alcohol intake is associated withincreased breast density (60). However,while white wine intake was associatedwith increased density in postmeno-pausal women, red wine intake was asso-ciated with lower breast density (60). No
difference was noted for premenopausalwomen and the type of alcoholic bever-age.
Exercise
Only two studies, to our knowledge,have addressed the relationship betweenexercise and breast density. Authors ofone study found no relationship (60),and authors of the other study found aweak inverse relationship between mod-erate exercise and breast density (64).
RELATIONSHIP BETWEENHORMONAL FACTORS ANDBREAST DENSITY ANDBREAST CANCER RISK
HRT
HRT slows normal breast involution(65–67) and causes an increase in mam-mographic density in 17%–73% ofwomen (67–72) (Fig 2). The increase indensity is most commonly diffuse butmay be focal or multifocal (68,69).
Mammographic changes vary with dif-ferent HRT regimens. Estrogen combinedwith progestin has a greater associationwith increase in density than the use ofestrogen alone (70–73). An increase inbreast density is also more commonly ob-served with continuous use of combinedHRT, where both estrogen and progester-one are taken daily, than with a cycledHRT, where estrogen is used daily butprogesterone is only used during part ofthe month (70,73). In one study, 28% ofwomen undergoing continuous com-bined therapy had an increase in densitycompared with 10% of women using cy-clic therapy, 5% of women using estra-diol alone, and 3% of controls (71). Sim-ilar results were found in womenparticipating in the Postmenopausal Es-trogen/Progestin Interventions, or PEPI,trial (73). Use of androgenic norpro-gestins, which is common in Europe, haseffects similar to those of medroxypro-gestrone acetate, which is commonlyused in the United States (74,75).
Breast density appears to be very re-sponsive to HRT. Investigators of thePEPI trial have found that the greatestchange in density occurs during the 1styear of use (73). The breast responds rap-idly to hormonal manipulation, with adecrease in density seen after just 2 weeksafter HRT cessation (Fig 3) (76). Colacurciet al (77) have found that women whostopped HRT for 3 weeks prior to theirannual mammography had no signifi-cant change from baseline, whereas
Figure 2. Mammograms demonstrate marked increase in density with HRT. A, Prior toHRT use, the breast is minimally dense. B, After 1 year, the breast is extremely dense andhas increased in size.
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 35
Ra
dio
logy

women who continued HRT had an in-crease in density.
Authors of three large cohort studieshave demonstrated a greater breast can-cer risk with use of estrogen and proges-terone than with use of estrogen alone(78–80). The estrogen-plus-progesteronearm of the Women’s Health Initiativetrial was halted before study completionbecause of an increased breast cancer risk(81). The estrogen-only arm of the studycontinues, because breast cancer risk wasonly slightly elevated in that group.
At histologic examination, benignbreast biopsies performed in women us-ing estrogen plus progestin had signifi-cantly higher proliferation indices com-pared with biopsies performed in womeneither using estrogen alone or not under-going HRT (82). In addition, the prolifer-ation noted in women using estrogenwith progestin in that study was localizedto the terminal duct lobular unit, whichis the site of the development of mostbreast cancers (82).
Selective Estrogen ReceptorModulators
Selective estrogen receptor modulatorsdecrease mammographic density pre-sumably due to the antiestrogen effect on
the breast (Fig 4). In a breast cancer pre-vention trial, 44% of women using ta-moxifen experienced a reduction inbreast density compared with 15% ofwomen randomly assigned to a placebo
(83). Raloxifene is another selective estro-gen receptor modulator that is approvedby the U.S. Food and Drug Administra-tion for treatment of osteoporosis. In theMultiple Outcomes of Raloxifene Evalua-
Figure 3. Mammograms obtained in a 65-year-old woman taking 1 mg estradiol daily. A, Right mediolateral oblique viewfrom a baseline mammogram shows heterogeneously moderate breast density. B, One year later, the right mediolateraloblique view from a screening mammogram shows that the breast density has undergone mild diffuse increase withdevelopment of a focal density (arrow). C, Right mediolateral oblique view from a diagnostic mammogram obtained afterstopping estrogen for 2 weeks shows that the focal density has resolved and the appearance is similar to that at baseline.Metallic marker identifies an incidental skin lesion.
Figure 4. Right craniocaudal mammographic views show a marked decrease in breast density atbaseline (left) and 2 years (right) after beginning treatment with tamoxifen for contralateralbreast cancer.
36 � Radiology � January 2004 Harvey and Bovbjerg
Ra
dio
logy

tion Trial, raloxifene significantly re-duced breast density compared with pla-cebo and estrogen (36).
Selective estrogen receptor modulatorsare associated with decreased breast can-cer risk (84,85). Tamoxifen reduces breastcancer risk by half in high-risk women(84). Raloxifene reduces breast cancer riskby 75% in postmenopausal women of av-erage risk (85). Of interest, only womenwith elevated serum estradiol levels re-duced breast cancer risk with raloxifeneuse, whereas women with undetectableestradiol levels had very low risk of breastcancer that was not changed with ralox-ifene use (86).
Other Hormonal Agents
Decrease in breast density has alsobeen reported with use of a gonadotro-pin-releasing hormone agonist that wasused in a clinical trial for birth control(87). The gonadotropin-releasing hor-mone agonist inhibits ovarian functionand is hypothesized to reduce breast can-cer risk (87). Tibolone is widely used inEurope for hormone replacement ther-apy but is not approved by the Food andDrug Administration in the UnitedStates. The precise mechanism of actionof this agent is not known since it hasmultiple metabolites, each of which canexert differing effects. Its major effectsare to inhibit sulfatase activity andthereby block estrogen synthesis from es-trone sulfate and to exert androgenic ef-fects (88). This compound increasesbreast density in a small number ofwomen (2%–6%) compared with womenwho use estrogen and progesterone daily(46%–50%) (89). No data are availableabout the effect of oral contraceptives orandrogens on breast density.
Changes in Breast Density withHRT and Selective EstrogenReceptor Modulator MirrorBreast Cancer Risk
Mammographic density appears tomirror the risk associated with hormonalagents (Fig 5). Since women with mam-mographically dense breasts have an in-crease in breast cancer risk, women whohave an increase in mammographic den-sity in response to HRT may be at higherrisk for developing breast cancer thanwomen who do not experience a changein density with use of HRT, although, toour knowledge, there are currently nostudies in this area. Decrease in breastdensity in response to selective estrogenreceptor modulators may also decreasebreast cancer risk, and further studies tothese points may be useful, particularlywith the suggestion in one study (19)that changes in density change breastcancer risk.
HISTOLOGIC EVALUATION OFMAMMOGRAPHICALLY DENSEBREASTS
In 1986, Page and Winfield (90) statedthat “true ducts make up little of the ra-diographic density found in any breast.The great mass of density seen on themammogram is due to the glandular lob-ules and their stroma.” The relative con-tribution of each to the mammographi-cally dense breasts has not beenquantified, although studies have inde-pendently evaluated stromal and epithe-lial differences in minimally dense versusdense breasts. Authors of two studies(91,92) in which quantitative measureswere used note an association betweenincreased stromal collagen and mammo-graphically highly dense breasts, whileothers (93,94) similarly note increased
stromal fibrosis in association with theWolfe P2 and DY patterns.
As to epithelial changes, authors ofseveral studies who correlated increaseddensity with quantitative analysis haveshown an increase in epithelial hyperpla-sia (58,91,95). Specifically, women par-ticipating in the Canadian NationalBreast Screening Study with extremebreast density have been shown to be12.2 times more likely to develop hyper-plasia without atypia (91). Of note, thesewomen were also found to be 9.7 timesmore likely to develop atypical hyperpla-sia or carcinoma in situ (91). Authors ofanother study (96) compared nipple aspi-rate fluid cytologic results to breast den-sity and found that women with mam-mographically dense breasts were fourtimes more likely to have cytologicatypia. The mammographically densebreasts are therefore likely caused by anincrease in both stromal and epithelialtissue. These changes may lead to devel-opment of the histologic precursors ofbreast cancer, as was seen with the in-creased incidence of atypia and carci-noma in situ in these studies (91,96).
PLAUSIBLE FACTORS THATMAY EXPLAIN THEASSOCIATION OF BREASTDENSITY WITH BREASTCANCER RISK
Increased Growth Factors
Although mammographically densebreasts are likely a result of an increase inboth stroma and epithelium, the cause ofthese changes is not clear but may be duein part to increased growth factors. Au-thors of a study (92) compared the tissuesurrounding benign breast lesions fromwomen with extremely dense breastswith tissue from women with little or nodensity and found that the tissue fromwomen with dense breasts had increasedinsulin-like growth factor 1, greater nu-clear area, and more total collagen. Au-thors of two studies, including one ofwomen in the Nurse’s Health Study, alsofound elevated serum insulin-like growthfactor 1 and lower insulin-like growthfactor binding protein-3 in premeno-pausal women with dense breast tissue,but the effect did not occur in postmeno-pausal women (97,98).
Estrogen Exposure
Breast density is clearly hormonally re-sponsive. Some investigators believe thatbreast density may reflect past exposureto estrogen (51). There is moderate evi-
Figure 5. Graphs demonstrate that the overall percentage of women with change in density(left) is similar to the relative risk of breast cancer (right) associated with the hormonal agents.Note that the relative risk of breast cancer with tamoxifen (white bar) use is reported for high-riskwomen (84), while raloxifene (striped bar) use is reported for average-risk women (85). Blackbar � estrogen; gray bar � estrogen plus progesterone.
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 37
Ra
dio
logy

dence to support the role of endogenousestrogens in the cause of breast cancer.Experimental evidence suggests that theestrogen metabolites 4-hydroxyestroneand 4-hydroxyestradiol are further me-tabolized to estradiol quinones (99).These compounds can bind directly toadenine and guanine and pull these basesoff segments of DNA. This is postulatedto be a mechanism for direct mutageniceffects of estrogens. Others postulate thatthe 2-hydroxymetabolites of estradiolcause stable DNA adducts or that the16-� estrogen metabolites can covalentlybind to the estrogen receptor and consti-tutively activate it (99).
Estrogen production may occur withinthe breast itself through the enzymes aro-matase and sulfatase. Aromatase convertsandrogens to estrogens, while sulfataseconverts biologically inactive estrone sul-fate into biologically active estrone. Asurprising finding is that estradiol levelswithin breast cancers and the surround-ing tissue are similar in pre- and post-menopausal women even though plasmaconcentrations are markedly higher inpremenopausal women (100). This obser-vation suggests that a major source ofestradiol in the breast tissue in post-menopausal women who develop breastcancer is the breast itself due to overac-tive aromatase or sulfatase (96,101). Fur-ther work regarding the biologic cause ofincreased breast density will be helpful.
Serum Prolactin Levels
Elevated serum prolactin levels havebeen associated with higher breast den-sity in postmenopausal women in a dose-response fashion (98). Findings of theNurses Health Study showed a significantpositive association between plasma levelof prolactin and the postmenopausalbreast cancer risk (highest vs lowest quar-tile; multivariate relative risk, 2.03; 95%CI: 1.24, 3.31) (102). Neither study find-ings showed an association of prolactinlevels with breast density or breast cancerrisk in premenopausal women. Thus,high mammographic breast density andbreast cancer risk may be related to ele-vated prolactin levels only in postmeno-pausal women.
Genetics
In a cohort study of families withbreast cancer, Pankow et al (30) evaluatedprimary relative relationships and corre-lation with breast density. The sister-sis-ter correlation was statistically signifi-cant (r � 0.16–0.27, P � .05), while the
mother-sister correlation was suggestive(r � 0.01–0.17). Paternal breast densityobviously cannot be assessed. Segrega-tion analysis suggests that a major auto-somal gene influences breast density,probably with Mendelian transmission ofa dominant gene. Further work with thiscohort suggests that the gene may be onchromosome 6 (29).
Authors of a recent study correlatedbreast density between 218 pairs ofmonozygotic twins and 134 pairs of dizy-gotic twins in the United States and Aus-tralia (103). According to the study find-ings, heritability accounted for 63% ofthe variation in breast density in all twinsstudied (103). Also of interest, womenwith known BRCA1 or BRCA2 mutationshave been shown to have denser breasttissue that is coarser and lower in con-trast than women at low risk for develop-ing breast cancer (104). Findings of thesestudies suggest that genetics plays astrong role in breast density.
FUTURE DIRECTIONS
Incorporation of Density in RiskAssessment Models
Current computerized methods ofquantitative assessment of breast densityare very reliable but time consuming andnot practical for everyday use. More prac-tical visual assessment methods are notas reproducible. Since there is no standardmethod of quantifying breast density, val-idation of density in risk assessment mod-els is difficult. Density assessment wouldbecome more practical if an automated,quantitative, and reproducible methodcould be developed. This may be an idealapplication for digital mammographysince the images are already in digitalformat.
Use of Density as an Entry Criterioninto Breast Cancer Prevention Trials
If density is a risk factor for breast can-cer, use of high breast density as an in-clusion criterion for breast cancer pre-vention trials may increase study powersuch that studies would require fewer pa-tients and be directed at women atgreater risk. For instance, a dietary inter-vention study recruiting women with50% or greater density from 1982 to 1994has noted a four to five times greater in-cidence of breast cancer than expected(105).
Use of Breast Density as a SurrogateMarker of Risk for Prevention Trialsand HRT Regimens
Since changes in breast density appearto reflect breast cancer risk, some inves-tigators have proposed using density as apreliminary surrogate marker in preven-tion trials. If a drug that is thought toreduce risk causes an increase in breastdensity, the risk may not be reduced. Fur-ther studies evaluating correlation ofcancer risk and changes in density arenecessary before this could be useful.Likewise, there is increasing interest fromdrug manufacturers regarding whethertheir particular HRT regimen is associ-ated with an increase in density becauseof the possible implications regardingbreast cancer risk. However, it should bestressed that currently there is only sug-gestive data that an increase in density isassociated with an increase in risk (19),and further studies need to be performedto investigate this concept.
The Mammogram as aPhysiologic Test
If future study findings do show thatchanges in density do correlate withchanges in risk, mammography maysomeday be viewed as a physiologic testin addition to its current screening anddiagnostic roles. Women may somedaybe given an estimate of their cancer riskbased on risk models that included breastdensity at the time of their mammogra-phy. They could use this informationto make decisions regarding HRT use,lifestyle changes, or chemoprevention.However, since breast cancer risk remainselevated for at least 5–10 years after themammogram showed increased density,lowering density may not change cancerrisk or may take 5–10 years after the in-tervention to affect breast cancer risk.This is an important area for investiga-tion.
SUMMARY
Across a number of studies in varied set-tings and populations, increased breastdensity as evaluated with quantitativemethods is a moderate independent riskfactor for breast cancer. Only genetic ab-normalities, age, prior breast cancer, andbiopsy findings showing lobular carci-noma in situ are associated with similaror greater relative risk of breast cancer.Breast density information is unlikely tobecome useful in risk assessment modelsuntil it can be measured in a reproduc-
38 � Radiology � January 2004 Harvey and Bovbjerg
Ra
dio
logy

ible, standardized, and automated fash-ion. Unlike most breast cancer risk fac-tors, breast density can be influenced.However, further studies must be per-formed to determine the use of includingdensity in risk assessment and preven-tion decisions and to evaluate whetherreducing breast density will reduce breastcancer risk.
Acknowledgments: We thank Martin Yaffe,PhD, for the instruction in and use of thebreast density program developed at the Uni-versity of Toronto. We thank Richard Santen,MD, for his assistance in reviewing this article.
References1. Byrne C. Studying mammographic den-
sity: implications for understandingbreast cancer. J Natl Cancer Inst 1997;89:531–533.
2. Wolfe JN. Breast patterns as an index ofrisk for developing breast cancer. AJRAm J Roentgenol 1976; 126:1130–1139.
3. Threatt B, Norbeck JM, Ullman NS, et al.Association between mammographicparenchymal pattern classification andincidence of breast cancer. Cancer 1980;45:2550–2556.
4. Witt I, Steen Hansen H, Brunner S. Therisk of developing breast cancer in rela-tion to mammography findings. Eur JRadiol 1984; 4:65–67.
5. Egan RL, McSweeney MB. Mammo-graphic parenchymal patterns and riskof breast cancer. Radiology 1979; 133:65–70.
6. Moskowitz M, Gartside P, McLaughlinC. Mammographic patterns as markersfor high-risk benign breast disease andincident cancers. Radiology 1980; 134:293–295.
7. Tabar L, Dean PB. Mammographic pa-renchymal patterns: risk indicator forbreast cancer? JAMA 1982; 247:185–189.
8. Carlile T, Thompson DJ, Kopecky KJ, etal. Reproducibility and consistency inclassification of breast parenchymal pat-terns. AJR Am J Roentgenol 1983; 140:1–7.
9. Boyd NF, O’Sullivan B, Campbell JE, etal. Mammographic signs as risk factorsfor breast cancer. Br J Cancer 1982; 45:185–193.
10. Boyd NF, Byng JW, Jong RA, et al. Quan-titative classification of mammographicdensities and breast cancer risk: resultsfrom the Canadian National BreastScreening Study. J Natl Cancer Inst1995; 87:670–675.
11. Wolfe JN, Saftlas AF, Salane M. Mammo-graphic parenchymal patterns andquantitative evaluation of mammo-graphic densities: a case-control study.AJR Am J Roentgenol 1987; 148:1087–1092.
12. Saftlas AF, Hoover RN, Brinton LA, et al.Mammographic densities and risk ofbreast cancer. Cancer 1991; 67:2833–2838.
13. Kato I, Beinart C, Bleich A, Su S, Kim M,Toniolo PG. A nested case-control studyof mammographic patterns, breast vol-ume, and breast cancer. Cancer CausesControl 1995; 6:431–438.
14. Brisson J, Merletti F, Sadowsky NL,
Twaddle JA, Morrison AS, Cole P. Mam-mographic features of the breast andbreast cancer risk. Am J Epidemiol 1982;115:428–437.
15. Brisson J, Morrison AS, Kopans DB, et al.Height and weight, mammographic fea-tures of breast tissue, and breast cancerrisk. Am J Epidemiol 1984; 119:371–381.
16. Brisson J, Verreault R, Morrison AS, Ten-nina S, Meyer F. Diet, mammographicfeatures of breast tissue, and breast can-cer risk. Am J Epidemiol 1989; 130:14–24.
17. Byrne C, Schairer C, Wolfe J, et al. Mam-mographic features and breast cancerrisk: effects with time, age, and meno-pause status. J Natl Cancer Inst 1995;87:1622–1629.
18. Lam PB, Vacek PM, Geller BM, Muss HB.The association of increased weight,body mass index, and tissue densitywith risk of breast carcinoma in Ver-mont. Cancer 2000; 89:369–375.
19. Van Gils CH, Hendricks JH, Holland R,et al. Changes in mammographic breastdensity and concomitant changes inbreast cancer risk. Eur J Cancer Prev1999; 8:509–515.
20. Maskarinec G, Meng L. A case-controlstudy of mammographic densities inHawaii. Breast Cancer Res Treat 2000;63:153–161.
21. Soderqvist G, Isaksson E, von SchoultzB, Carlstrom K, Tani E, Skoog L. Prolif-eration of breast epithelial cells inhealthy women during the menstrualcycle. Am J Obstet Gynecol 1997; 176:123–128.
22. Graham SJ, Stanchev PL, Lloyd-SmithJO, Bronskill MJ, Plewes DB. Changes infibroglandular volume and water con-tent of breast tissue during the men-strual cycle observed by MR imaging at1.5 T. J Magn Reson Imaging 1995;5:695–701.
23. Anderson TJ. Pathological studies of ap-optosis in the normal breast. Endocr Re-lat Cancer 1999; 6:9–12.
24. White E, Velentagas P, Mandelson MT,et al. Variation in mammographic breastdensity by time in menstrual cycleamong women aged 40–49 years. J NatlCancer Inst 1998; 90:906–910.
25. Ursin G, Parisky YR, Pike MC, Spicer DV.Mammographic density changes duringthe menstrual cycle. Cancer EpidemiolBiomarkers Prev 2001; 10:141–142.
26. Stomper PC, DSouza DJ, DiNitto PA.Analysis of parenchymal density onmammograms in 1353 women 25–79years old. AJR Am J Roentgenol 1996;167:1261–1265.
27. Oza AM, Boyd NF. Mammographic pa-renchymal patterns: a marker of breastcancer risk. Epidemiol Rev 1993; 15:196–208.
28. Saftlas AF, Szklo M. Mammographic pa-renchymal patterns and breast cancerrisk. Epidemiol Rev 1987; 9:146–174.
29. Vachon CM, King RA, Atwood LD, KuniCC, Sellers TA. Preliminary sibpair link-age analysis of percent mammographicdensity. J Natl Cancer Inst 1999; 91:1778–1779.
30. Pankow JS, Vachon CM, Kuni CC, et al.Genetic analysis of mammographicbreast density in adult women: evidence
of a gene effect. J Natl Cancer Inst 1997;89:549–556.
31. Lee-Han H, Cooke G, Boyd NF. Quanti-tative evaluation of mammographicdensities: a comparison of methods ofassessment. Eur J Cancer Prev 1995;4:285–292.
32. American College of Radiology. Breastimaging reporting and data system (BI-RADS). Reston, Va: American College ofRadiology, 1993.
33. Berg WA, Campassi C, Langenberg P,Sexton MJ. Breast Imaging Reportingand Data System: Inter- and intraob-server variability in feature analysis andfinal assessment. AJR Am J Roentgenol2000; 174:1769–1777.
34. Kerlikowski K, Grady D, Barclay J, et al.Variability and accuracy in mammo-graphic interpretation using the Ameri-can College of Radiology Breast ImagingReporting and Data System. J Natl Can-cer Inst 1998; 90:1801–1809.
35. Byng JW, Yaffe MJ, Jong RA, et al. Anal-ysis of mammographic density andbreast cancer risk for digitized mammo-grams. RadioGraphics 1998; 18:1587–1598.
36. Freedman M, San Martin J, O’Gorman J,et al. Digitized mammography: a clinicaltrial of postmenopausal women ran-domly assigned to receive raloxifene, es-trogen, or placebo. J Natl Cancer Inst2001; 93:51–56.
37. Karssemeijer N. Automated classifica-tion of parenchymal patterns in mam-mograms. Phys Med Biol 1998; 43:365–378.
38. Sivaramakrishna R, Obuchowski NA,Chilcote WA, Powell KA. Automatic seg-mentation of mammographic density.Acad Radiol 2001; 8:250–256.
39. Zhou C, Chan HP, Petrick N, et al. Com-puterized image analysis: estimation ofbreast density on mammograms. MedPhys 2001; 28:1056–1069.
40. Chang YH, Wang XH, Hardesty LA, et al.Computerized assessment of tissue com-position on digitized mammograms.Acad Radiol 2002; 9:899–905.
41. Lee NA, Rusinek H, Weinreb J, et al.Fatty and fibroglandular tissue volumesin the breasts of women 20–83 yearsold: comparison of x-ray mammographyand computer-assisted MR imaging. AJRAm J Roentgenol 1997; 168:501–506.
42. Graham SJ, Bronskill MJ, Byng JW, YaffeMJ, Boyd NF. Quantitative correlation ofbreast tissue parameters using magneticresonance and x-ray mammography.Br J Cancer 1996; 73:162–168.
43. Blend R, Rideout DF, Kaizer L, ShannonP, Tudor-Roberts B, Boyd NF. Parenchy-mal patterns of the breast defined by realtime ultrasound. Eur J Cancer Prev 1995;4:293–298.
44. Shephard JA, Kerlikowski KM, Smith-Bindman R, Genant HK, Cummings SR.Measurement of breast density withdual x-ray absorptiometry: feasibility.Radiology 2002; 223:554–557.
45. Sala E, Warren R, McCann J, Duffy S,Luben R, Day N. Mammographic paren-chymal patterns and breast cancer natu-ral history: a case-control study. ActaOncol 2001; 40:461–465.
46. Roubidoux MA, Bailey JE, Wray LA,Helvie MA. Invasive cancers detected af-
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 39
Ra
dio
logy

ter negative breast cancer screening re-sults: relationship of mammographicdensity to tumor prognostic factors. Radi-ology 2004; 230:42–48.
47. Blane CE, Fitzgerald JT, Gruppen LD, OhMS, Helvie MA, Andersson I. Decreasingrate of fatty involution at screeningmammography. Acad Radiol 2002; 9:895–898.
48. Boyd NF, Lockwood GA, Byng JW,Tritchler DL, Yaffe MJ. Mammographicdensities and breast cancer risk. CancerEpidemiol Biomarkers Prev 1998; 7:1133–1144.
49. Egan RL, Mosteller RC. Breast cancermammography patterns. Cancer 1977;40:2087–2090.
50. van Gils CH, Otten JD, Verbeek AL, Hen-dricks JH. Mammographic breast densityand risk of breast cancer: masking bias orcausality? Eur J Epidemiol 1998; 14:315–320.
51. White J. Breast density and cancer risk:what is the relationship? J Natl CancerInst 2000; 92:443.
52. Cigarette smoking among adults—United States, 2000. MMWR Morb Mor-tal Wkly Rep 2002; 51:642–645.
53. Sala E, Warren R, McCann J, Duffy S,Luben R, Day N. High-risk mammo-graphic parenchymal patterns and an-thropometric measures: a case-controlstudy. Br J Cancer 1999; 81:1257–1261.
54. Vachon CM, Kuni CC, Anderson K,Anderson VE, Sellers TA. Association ofmammographically defined percentbreast density with epidemiologic riskfactors for breast cancer. Cancer CausesControl 2000; 11:653–662.
55. van Gils CH, Hendricks JH, Otten JD,Holland R, Verbeek AL. Parity and mam-mographic breast density in relation tobreast cancer risk: indication of interac-tion. Eur J Cancer Prev 2000; 9:105–111.
56. Boyd NF, Lockwood GA, Martin LJ, et al.Mammographic densities and risk ofbreast cancer among subjects with afamily history of this disease. J Natl Can-cer Inst 1999; 91:1404–1408.
57. Ziv E, Shepherd J, Smith-Bindman R,Kerlikowske K. Mammographic breastdensity and family history of breast can-cer. J Natl Cancer Inst 2003; 95:556–558.
58. Byrne C, Schairer C, Brinton LA, et al.Effects of mammographic density andbenign breast disease on breast cancerrisk. Cancer Causes Control 2001; 12:103–110.
59. Knight JA, Martin LJ, Greenberg CV, etal. Macronutrient intake and change inmammographic breast density at meno-pause: results from a randomized trial.Cancer Epidemiol Biomarkers Prev1999; 8:123–128.
60. Vachon CM, Kushi LH, Cerhan JR, KuniCC, Sellers TA. Association of diet andmammographic breast density in theMinnesota breast cancer family cohort.Cancer Epidemiol Biomarkers Prev2000; 9:151–160.
61. Boyd NF, Greenberg C, Lockwood G, etal. Effects at 2 years of a low-fat, high-carbohydrate diet on radiologic featuresof the breast: results from a randomizedtrial. J Natl Cancer Inst 1997; 89:488–496.
62. Jakes RW, Duffy SW, Ng F, et al. Mam-
mographic parenchymal patterns andself-reported soy intake in SingaporeChinese women. Cancer EpidemiolBiomarkers Prev 2002; 11:608–613.
63. Parkin DM, Muir CS. Cancer incidencein five continents: comparability andquality of data. IARC Sci Publ 1992; 120:45–173.
64. Gram IT, Funkhouser E, Tabar L. Moder-ate physical activity in relation to mam-mographic patterns. Cancer EpidemiolBiomarkers Prev 1999; 8:117–122.
65. Kaufman Z, Garstin WIH, Hayes R,Michell MJ, Baum M. The mammo-graphic parenchymal patterns ofwomen on hormonal replacement ther-apy. Clin Radiol 1991; 43:389–392.
66. Sterns EE, Zee B. Mammographic den-sity changes in perimenopausal women:is the effect of hormone replacementtherapy predictable? Breast Cancer ResTreat 2000; 59:125–132.
67. Rutter CM, Mandelson MT, Laya MB,Taplin S. Changes in breast density as-sociated with initiation, discontinua-tion, and continuing use of hormonereplacement therapy. JAMA 2001; 285:171–176.
68. McNicholas MM, Heneghan JP, MilnerMH, Tunney T, Hourihane JB, MacEr-laine DP. Pain and increased mammo-graphic density in women receivinghormone replacement therapy: a pro-spective study. AJR Am J Roentgenol1994; 163:311–315.
69. Stomper PC, Van Voorhis BJ, RavnikarVA, Meyer JE. Mammographic changesassociated with postmenopausal hor-mone replacement therapy: a longitudi-nal study. Radiology 1990; 174:487–490.
70. Berkowitz JE, Gatewood OM, GoldblumLE, Gayler BW. Hormonal replacementtherapy: mammographic manifesta-tions. Radiology 1990; 174:199–201.
71. Persson I, Thurfjell E, Holmberg L. Effectof estrogen and estrogen-progestin re-placement regimens on mammographicbreast parenchymal density. J Clin On-col 1997; 15:3201–3207.
72. Laya MB, Gallagher JC, Schreiman JS,Larson EB, Watson P, Weinstein L. Effectof postmenopausal hormonal replace-ment therapy on mammographic den-sity and parenchymal pattern. Radiol-ogy 1995; 196:433–437.
73. Greendale GA, Reboussin BA, Sie A, et al.Effects of estrogen and estrogen-proges-tin on mammographic parenchymaldensity. Ann Intern Med 1999; 130:262–269.
74. Sendag F, Cosan Terek M, Ozsener S, etal. Mammographic density changes dur-ing different postmenopausal hormonereplacement therapies. Fertil Steril 2001;76:445–450.
75. Lundstrom E, Wilczek B, von Palffy Z,Soderqvist G, von Schoultz B. Mammo-graphic breast density during hormonereplacement therapy: differences ac-cording to treatment. Am J Obstet Gy-necol 1999; 181:348–352.
76. Harvey JA, Pinkerton JV, Herman CR.Short-term cessation of hormone re-placement therapy and improvement ofmammographic specificity. J Natl Can-cer Inst 1997; 89:1623–1625.
77. Colacurci N, Fornaro F, DeFranciscis P,
Mele D, Palermo M, delVecchio W. Ef-fects of a short-term suspension of hor-mone replacement therapy on mammo-graphic density. Fertil Steril 2001; 76:451–455.
78. Schairer C, Lubin J, Troisi R, Sturgeon S,Brinton L, Hoover R. Menopausal estro-gen and estrogen-progestin replacementtherapy and breast cancer risk. JAMA2000; 283:485–491.
79. Persson I, Weiderpass E, Bergkvist L, etal. Risks of breast and endometrial can-cer after estrogen and estrogen-proges-tin replacement. Cancer Causes Control1999; 10:253–260.
80. Ross RK, Paganini-Hill A, Wan PC, PikeMC. Effect of hormone replacementtherapy on breast cancer risk: estrogenversus estrogen plus progestin. J NatlCancer Inst 2000; 92:328–332.
81. Rossouw JE, Anderson GL, Prentice RL,et al. Risks and benefits of estrogen plusprogestin in healthy postmenopausalwomen: principal results from theWomen’s Health Initiative randomizedcontrolled trial. JAMA 2002; 288:321–333.
82. Hofseth LJ, Raafat AM, Osuch JR, PathakDR, Slomski CA, Haslam SZ. Hormonereplacement therapy with estrogen orestrogen plus medroxyprogesterone ace-tate is associated with increased epithe-lial proliferation in the normal post-menopausal breast. J Clin EndocrinolMetab 1999; 84:4559–4565.
83. Brisson J, Brisson B, Cote G, Maunsell E,Berube S, Robert J. Tamoxifen and mam-mographic breast densities. Cancer Epi-demiol Biomarkers Prev 2000; 9:911–915.
84. Fisher B, Costantino JP, Wickerham DL,et al. Tamoxifen for prevention of breastcancer: report of the National SurgicalAdjuvant Breast and Bowel Project P-1Study. J Natl Cancer Inst 1998; 90:1371–1388.
85. Cummings SR, Eckert S, Krueger KA,et al. The effect of raloxifene on riskof breast cancer in postmenopausalwomen: results from the MORE random-ized trial. JAMA 1999; 281:2189–2197.
86. Cummings SR, Duong T, Kenyon E, Cau-ley JA, Whitehead M, Krueger KA. Serumestradiol level and risk of breast cancerduring treatment with raloxifene. JAMA2002; 287:216–220.
87. Spicer DV, Ursin G, Parisky YR, et al.Changes in mammographic densities in-duced by a hormonal contraceptive de-signed to reduce breast cancer risk. J NatlCancer Inst 1994; 86:431–436.
88. van de Ven J, Donker GH, Sprong M,Blankenstein MA, Thijssen JH. Effect oftibolone (Org OD14) and its metaboliteson aromatase and estrone sulfatase ac-tivity in human breast adipose stromalcells and in MCF-7 and T47D breast can-cer cells. J Steroid Biochem Mol Biol2002; 81:237–247.
89. Lundstrom E, Christow A, KersemaekersW, et al. Effects of tibolone and contin-uous combined hormone replacementtherapy on mammographic breast den-sity. Am J Obstet Gynecol 2002; 186:717–722.
90. Page DL, Winfield AC. The dense mam-mogram. AJR Am J Roentgenol 1986;147:487–489.
40 � Radiology � January 2004 Harvey and Bovbjerg

91. Boyd NF, Jensen HM, Cooke G, Lee HanH. Relationship between mammo-graphic and histologic risk factors forbreast cancer. J Natl Cancer Inst 1992;84:1170–1179.
92. Guo YP, Martin LJ, Hanna W, et al.Growth factors and stromal matrix pro-teins associated with mammographicdensities. Cancer Epidemiol BiomarkersPrev 2001; 10:243–248.
93. Bright R, Morrison A, Brisson J, et al.Relationship between mammographicand histologic features of breast tissue inwomen with benign biopsies. Cancer1988; 61:266–271.
94. Arthur JE, Ellis IO, Flowers C, Roebuck E,Elston CW, Blamey RW. The relation-ship of “high risk” mammographic pat-terns to histological risk factors for de-velopment of cancer in the humanbreast. Br J Radiol 1990; 63:845–849.
95. Urbanski S, Jensen HM, Cooke G, et al.The association of histological and ra-diological indicators of breast cancerrisk. Br J Cancer 1988; 58:474–479.
96. Lee MM, Petrakis NL, Wrensch MR, KingEB, Miike R, Sickles E. Association of ab-normal nipple aspirate cytology andmammographic breast pattern and den-sity. Cancer Epidemiol Biomarkers Prev1994; 3:33–36.
97. Byrne C, Colditz GA, Willett WC,Speizer FE, Pollak M, Hankinson SE.Plasma insulin-like growth factor (IGF) I,IGF-binding protein 3, and mammo-graphic density. Cancer Res 2000; 60:3744–3748.
98. Boyd NF, Stone J, Martin LJ, et al. Theassociation of breast mitogens withmammographic densities. Br J Cancer2002; 87:876–882.
99. Jefcoate CR, Liehr JG, Santen RJ, et al.Tissue-specific synthesis and oxidativemetabolism of estrogens. J Natl CancerInst Monogr 2000; 27:95–112.
100. Pasqualini JR, Chetrite G, Blacker C, etal. Concentrations of estrone, estradiol,and estrone sulfate and evaluation ofsulfatase and aromatase activities in pre-and post menopausal breast cancer pa-
tients. J Clin Endocrinol Metab 1996;81:1460–1464.
101. Yue W, Santen RJ, Wang JP, HamiltonCJ, Demers LM. Aromatase within thebreast. Endocr Relat Cancer 1999;6:157–164.
102. Hankinson SE, Willett WC, MichaudDS, et al. Plasma prolactin levels andsubsequent risk of breast cancer in post-menopausal women. J Natl Cancer Inst1999; 91:629–634.
103. Boyd NF, Dite GS, Stone J, et al. Herita-bility of mammographic density, a riskfactor for breast cancer. N Engl J Med2002; 347:886–894.
104. Huo Z, Giger ML, Olopade OI, et al. Com-puterized analysis of digitized mammo-grams of BRCA1 and BRCA2 gene muta-tion carriers. Radiology 2002; 225:519–526.
105. Boyd NF, Fishell E, Jong R, et al. Mam-mographic densities as a criterion forentry to a clinical trial of breast cancerprevention. Br J Cancer 1995; 72:476–479.
Volume 230 � Number 1 Quantitative Assessment of Mammographic Breast Density � 41
Ra
dio
logy