Embed Size (px)
Citation preview

Quality Tool Box Foot Pain
Dr. David Berbrayer
Division Head, Physiatry
Sunnybrook Health Sciences Centre
University of Toronto

Disclosures
• Dr. David Berbrayer has no financial or other disclosures.

Sunnybrook Health Sciences Centre

Learning Objectives
At the end of the presentation on foot evaluation, participants will be able to:• Describe constructs for core sets for foot pain
• Review assessment instruments for foot pain
• Reflect on quality metrics for foot pain
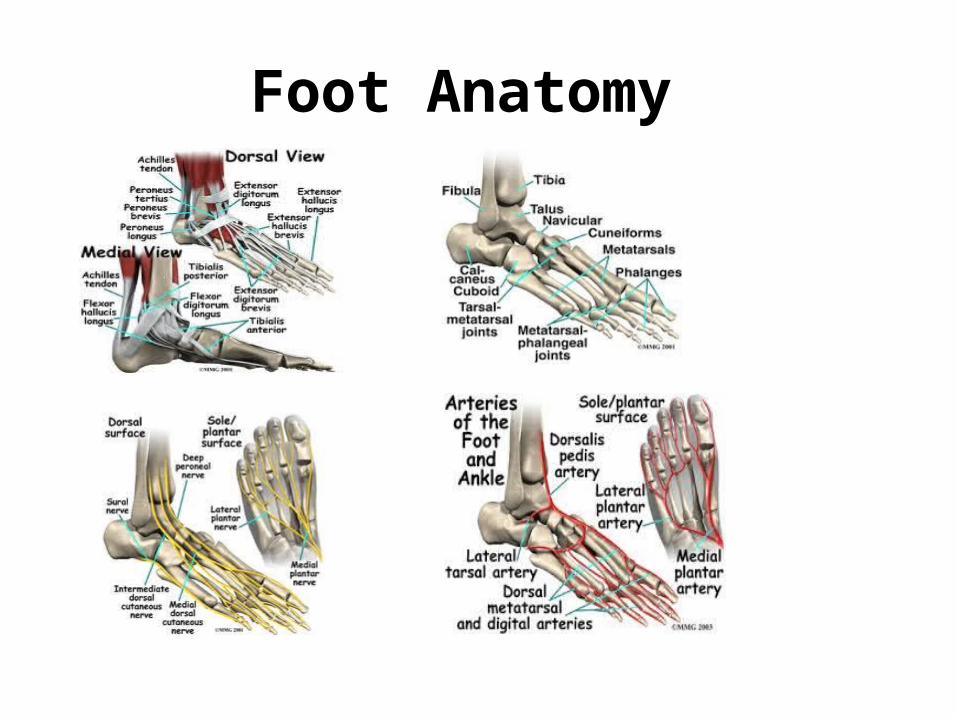
Foot Anatomy

Reflexology

Causes of Hind-foot pain
• Plantar fasciopathy• Calcaneal apophysitis• Calcaneal spur• Heel pad fat atrophy• Nerve entrapment• Achilles tendinitis• Arterial insufficiency• Jogger’s foot• Tarsal tunnel syndrome• Peripheral ischemia

Plantar Fasciopathy
• Plantar fasciopathy is a painful condition of the foot caused by inflammation (which produces acute symptoms) or degeneration (a source of chronic pain) of the plantar fascia, which is the thick connective tissue extending from the calcaneus to the metatarsal heads.
• Function: static-supports arch
Dynamic-medial arch flattens/ elevates
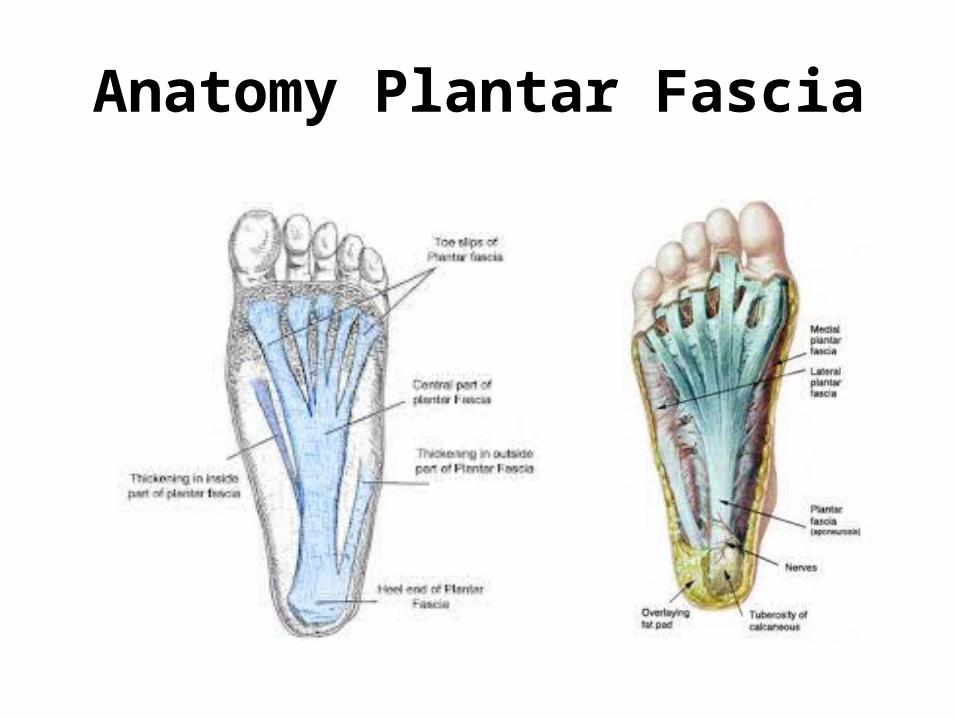
Anatomy Plantar Fascia

Foot Pain: Core Constructs
• Pain• Mobility- Walking, Moving, Transfer• Self-care• Participation• Life satisfaction

PBAs vs. PROs
• Provider based assessment instrument (PBA):
Foot Function Index
Rowan Foot Pain Assessment
Manchester Foot Pain Disability Index• Patient reported outcome measure (PRO):
Foot Health Status Questionnaire
Foot and Ankle Questionnaire –AAOS
(Disability indices for lower limb core, global foot and ankle functionality, and shoe comfort are included.)

Physical Examination of Foot Pain
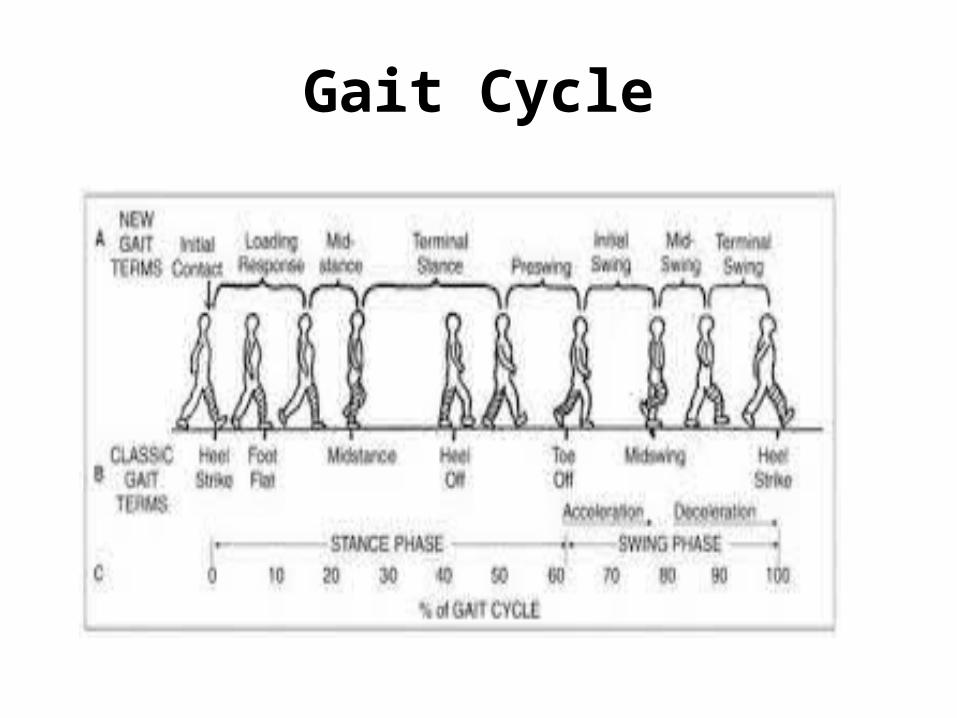
• Reduced Quality life / Abnormal Gait Cycle-decrease stance on affected foot
• Windlass Test • Restriction Ankle Dorsiflexion• Localized Pain over Calcaneus • Longitudinal Arch Impairment

Windlass Mechanism

Windlass Test
NON-WEIGHT BEARING
• With the patient sitting, the examiner stabilizes the ankle joint in neutral with 1 hand placed just behind the first metatarsal head.
• The examiner then extends the first metatarsophalangeal joint, while allowing the interphalangeal joint to flex.
• Passive extension (i.e., dorsiflexion) of the first metatarsophalangeal joint is continued to its end of range or until the patient’s pain is reproduced
Weight Bearing
• The patient stands on a step stool and positions the metatarsal heads of the foot to be tested just over the edge of the step.
• The subject is instructed to place equal weight on both feet.
• The examiner then passively extends the first metatarsophalangeal joint while allowing the interphalangeal joint to flex.
• Passive extension (i.e., dorsiflexion) of the first metatarsophalangeal joint is continued to its end of range or until the patient’s pain is reproduced.
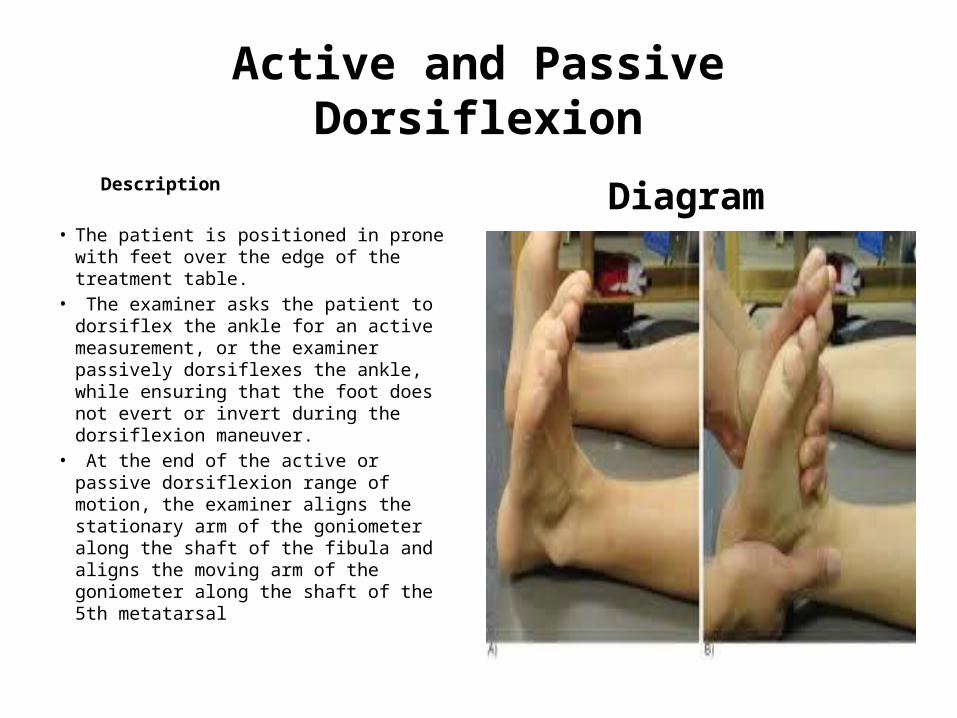
Active and Passive Dorsiflexion
Description
• The patient is positioned in prone with feet over the edge of the treatment table.
• The examiner asks the patient to dorsiflex the ankle for an active measurement, or the examiner passively dorsiflexes the ankle, while ensuring that the foot does not evert or invert during the dorsiflexion maneuver.
• At the end of the active or passive dorsiflexion range of motion, the examiner aligns the stationary arm of the goniometer along the shaft of the fibula and aligns the moving arm of the goniometer along the shaft of the 5th metatarsal
Diagram

Restriction Ankle Dorsiflection

Medial/Lateral Longitudinal Arch

Longitudinal Arch Test
Description• With the patient standing with
equal weight on both feet, the midpoint of the medial malleolus, the navicular tuberosity, and the most medial prominence of the first metatarsal head are identified using palpation and marked with a pen.
• A goniometer is then used to measure the angle formed by the 3 points with the navicular tuberosity acting as the axis point.
Measurement
Current Treatment Guidelines• Heel Pain-Plantar Fasciitis Guidelines link International Classification of
Functioning, Disability, and Health (ICF) body structures (ligaments, fascia of ankle and foot, neural structures of lower leg) and ICF body functions (pain in lower limb, radiating pain in a segment or region) with World Health Organization's International Statistical Classification of Diseases and Related Health Problems (ICD) health condition (plantar fascia fibromatosis/plantar fasciitis).
• Guidelines describe evidence-based physical therapy practice and provide recommendations for (1) examination and diagnostic classification based on body functions / structures, activity limitations, and participation restrictions, (2) prognosis, (3) interventions and (4) assessment of outcome, musculoskeletal disorders.
McPoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. Heel pain--plantar fasciitis: clinical practice guidelines linked to the International Classification of Function, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008 Apr;38(4):A1-18.

Assessment Measures for Activity/Participation
• The Foot Function Index (FFI) is a 0-10 scale of pain and foot function over time in standing, walking, etc.
• The Foot Health Status Questionnaire (FHSQ) is a 42-item questionnaire assessing quality of foot health.
• The Foot and Ankle Ability Measure (FAAM) is an activities-of-daily-living scale of foot health.

Foot Function Index
• Foot Pain in past week• Foot Stiffness past week• Difficulty walking past week• Difficulty ADL past week• Difficulty Activity limitation past week• Difficulty social issues past weekThe Foot Function Index: a measure of foot pain and disability.Budiman-Mak E, Conrad KJ, Roach KE. J Clin Epidemiol. 1991;44(6):561-70

Foot Health Status Questionnaire (FHSQ)
Assess 4 domains:• Foot Pain: type of pain, severity, duration• Foot function: walking, working, stairs• Footwear: lifestyle issues• General foot health: body imageDevelopment and Validation of a Questionnaire Designed to Measure Foot-Health Status Bennett et al. J Am Podiatr Med Assoc 88(9): 419-428, 1998

Foot and Ankle Ability Measure (FAAM)
• Measures: standing, walking uneven ground, hills, stairs, curbs
• Difficulty: home, ADL, personal care, work(light, moderate, heavy),and recreation
Martin, R; Irrgang, J; Burdett, R; Conti, S; Van Swearingen, J: Evidence of Validity for the Foot and Ankle Ability Measure. Foot and Ankle International. Vol.26, No.11: 968-983, 2005.
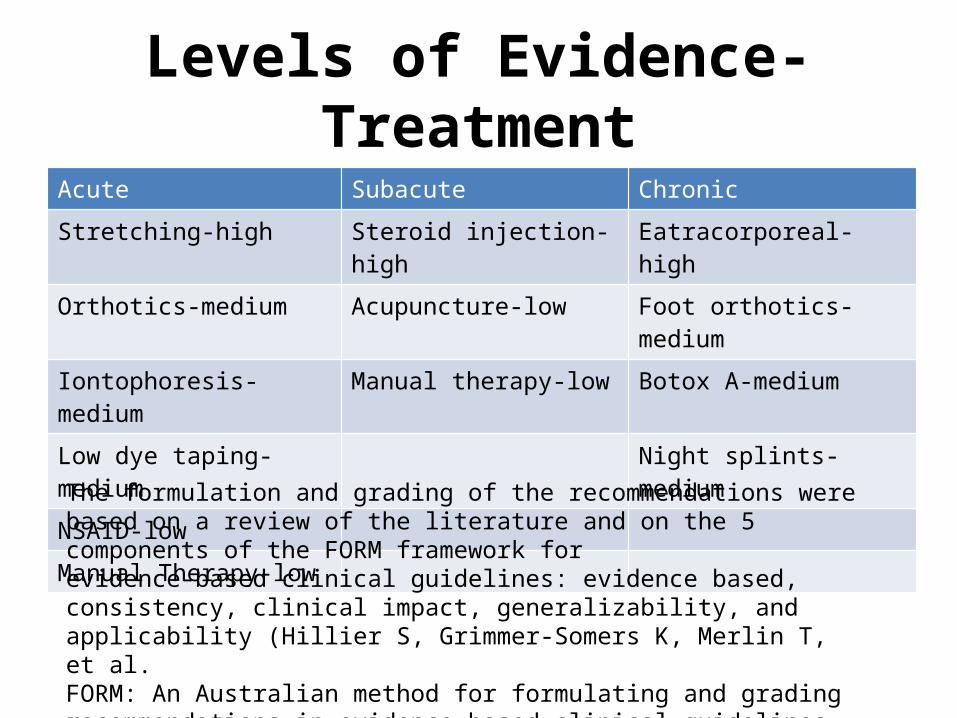
Levels of Evidence-TreatmentAcute Subacute Chronic
Stretching-high Steroid injection-high Eatracorporeal-high
Orthotics-medium Acupuncture-low Foot orthotics-medium
Iontophoresis-medium Manual therapy-low Botox A-medium
Low dye taping-medium Night splints-medium
NSAID-low
Manual Therapy-low
The formulation and grading of the recommendations were based on a review of the literature and on the 5 components of the FORM framework forevidence-based clinical guidelines: evidence based, consistency, clinical impact, generalizability, and applicability (Hillier S, Grimmer-Somers K, Merlin T, et al.FORM: An Australian method for formulating and grading recommendations in evidence-based clinical guidelines. BMC Med Res Method 2011;11:23).

Major Evidence Based References
1. Update on Evidence –Based Treatments for Plantar Fasciopathy
David Berbrayer MD, Michael Fredericson MD
PM&R 2014;6:159-169
2. Knowledge Now AAPM&R Plantar Fasciitis
David Berbrayer MD, FRCPC