Embed Size (px)
Citation preview

Quality of Life in Patients With Barrett’s EsophagusUndergoing SurveillanceDeborah Fisher, M.D., M.H.S., Amy Jeffreys, M.Stat., Hayden Bosworth, Ph.D., Jennifer Wang,Joseph Lipscomb, Ph.D., and Dawn Provenzale, M.D., M.S.Durham Veterans Affairs Medical Center, Institute for Clinical and Epidemiological Research, Durham,North Carolina; Duke University Medical Center, Division of Gastroenterology, Durham, North Carolina;and National Cancer Institute, Bethesda, Maryland
OBJECTIVES: Practice guidelines recommend surveillancefor Barrett’s esophagus (BE) because of the risk of esoph-ageal cancer. The quality of life of patients undergoingsurveillance is unknown. The objectives of this study wereto develop a new utility instrument to measure quality of lifeof patients undergoing BE surveillance and determine ifQuality of Life in Reflux and Dyspepsia (QOLRD) scorescorrelate with utility ratings.
METHODS: Fifteen patients were administered 16 scenariosdescribing possible BE surveillance outcomes. Each sce-nario was rated from 0 (equivalent to being dead) to 10(equivalent to being in perfect health). Each patient alsocompleted the QOLRD, a validated instrument. At test wasperformed to compare the QOLRD means with publishedmeans. The Spearman’s rank correlation coefficient wascalculated for the median QOLRD score and the medianutility rating.
RESULTS: QOLRD means ranged from 5.80 to 6.65 (previ-ously published means 4.3–5.4). Lower scores denoted aworsened quality of life. The difference was significant (p �0.001). The correlation coefficient of median QOLRD score(6.8) and median utility rating (4.0) was 0.10 (p � 0.71).
CONCLUSIONS: This population of BE patients had signifi-cantly higher QOLRD scores than a previously publishedpopulation referred for endoscopy. Quality of life using theutility measure was reduced. The utility measure did notcorrelate with the disease-specific instrument, suggestingthat the concerns of patients undergoing surveillance aredistinct from their reflux symptoms. (Am J Gastroenterol2002;97:2193–2200. © 2002 by Am. Coll. of Gastroenter-ology)
INTRODUCTION
Barrett’s esophagus (BE), intestinal metaplasia of the esoph-ageal epithelium, carries an associated risk of esophagealcancer (1). Endoscopic surveillance is recommended to de-tect dysplasia and diagnose cancer while at an early andpossibly treatable stage (2). There are no controlled trialsdemonstrating that surveillance decreases mortality from
esophageal cancer. Previous studies suggest that patientswith BE have decreased health-related quality of life(HRQL) compared with population norms (3). There are nostudies assessing HRQL in BE patients enrolled in surveil-lance programs. Such information would be valuable inadvising patients and providers of expected outcomes ofsurveillance.
There are several types of instruments for measuringHRQL. Utilities measure the perceived worth of a givenhealth state. Patients responding to utility measures comparehealth states to death. In utilities, HRQL is usually measuredon a scale from death or the equivalent in preference todeath (0.0) to full health (1.0 or 10) (4). Utilities can be usedto calculate quality-adjusted life-years for economic analy-sis. For chronic conditions, such as type 2 diabetes or BE, atreatment path may include multiple health states. In thesecases, the overall quality-adjusted life-years for a giventreatment path can be estimated. The treatment path isdivided into discrete health states,e.g., diabetes, diabeteswith complications, etc, which are separately evaluated byutility measurement. The overall utility measure is recon-structed by multiplying the discrete health state utilities bythe duration of that health state and taking the sum. Thistechnique assumes a constant rate of scoring and indepen-dence of individual utilities (5, 6). The holistic scenariomethod is an alternative to the traditional utility assessment.Respondents consider the value of the entire treatment pathat once. This method has the advantages of freedom fromrestrictive assumptions and may be more valid for chronicconditions such as diabetes or BE (7, 8). Limited data areavailable comparing the two techniques, and no studies haveused holistic scenario-based methods in BE patients.
The Quality of Life in Reflux and Dyspepsia (QOLRD) isa validated disease-specific HRQL instrument with 25 ques-tions in five dimensions (emotions, vitality, sleeping, eating/drinking, physical/social functioning) using a Likert scale(9). Lower scores denote a worsened HRQL (9). The QOL-RAD was initially tested in a cohort of patients who hadbeen referred for endoscopy because of upper GI symptoms.Sixty-eight percent were on medication for their GI symp-toms at the time of the study. Gender differences, with
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 9, 2002© 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00Published by Elsevier Science Inc. PII S0002-9270(02)04329-0

women scoring lower, were noted in all dimensions of theQOLRAD (9). The minimally relevant change is 0.5 units.An important change as defined by the patient is estimatedat one (1) unit and a very important change by 1.5 units (10).
Initial pilot testing of a new utility instrument, using 16scenarios related to possible outcomes of BE surveillance,included 10 patients who completed preferences for the 16scenarios and the Short Form-36 (SF-36). The SF-36 is ageneral HRQL instrument validated in several populationsincluding elderly veterans (11–13). The protocol was thenchanged to include the disease-specific QOLRAD becausethe new utility instrument was disease specific. The firstanalysis of the feasibility of administrating the new utilityinstrument pooled the 10 patients who had also completedthe SF-36 and the first seven patients who completed thenew protocol (with the QOLRAD) because only the utilityinstrument was assessed (unpublished data). In that analysisof 17 patients by the median, utility scores for the scenariosranged from 1 to 8 (on the 0–10 scale). There were nosignificant differences by age (�65, �65 yr), education(�12, �12 yr), or ethnicity (minority, white) for the highestscoring and lowest scoring scenarios. The highest scoringscenarios described situations involving only the inconve-nience of regular endoscopy or a minor complication ofendoscopy. The lowest scoring scenarios described devel-opment of cancer and/or fatal complications of esophagec-tomy. We concluded that: 1) scenarios that had more favor-able outcomes at face value scored higher than those withless favorable outcomes indicating face validity; and 2)these results support the comprehensibility of the instrumentand its applicability to patients of different ages acrossvaried educational and ethnic backgrounds.
Thus, measuring the HRQL of patients undergoing BEsurveillance can provide valuable information. In particular,the holistic scenario method can measure utilities, which canbe used in future economic analysis, and has advantagesover traditional quality-adjusted life-years for evaluatingHRQL in chronic diseases, such as BE. Also using a vali-dated disease-specific questionnaire may contribute to es-tablishing validity of the new utility instrument and wouldallow assessment of the impact of reflux symptoms on theHRQL of BE patients undergoing surveillance.
The objectives of this study were:
1. To develop an instrument to measure HRQL by utilityassessment of patients with BE undergoing surveillance.
2. To determine if the QOLRAD questionnaire results cor-relate with the utility rating.
MATERIALS AND METHODS
Inclusion criteria for subjects enrolled in this study weredocumented Barrett’s epithelium on endoscopic biopsy,candidate for surveillance, English speaking, and telephoneaccess. Exclusion criteria included cognitive impairmentprecluding cooperation or a score of �8 on Pfeiffer short
portable mental status questionnaire. The study was ap-proved by the Human Subjects Subcommittee and the Re-search Committee of the Durham Veterans Affairs MedicalCenter. Following a scripted introduction (Appendix 1), aconvenience sample of 15 patients were administered 16scenarios related to possible outcomes of BE surveillance(Appendix 2). Each scenario was rated from 0 (equivalent tobeing dead) to 10 (equivalent to being in perfect health) ona visual analog scale. The instrument’s readability was ap-proximately at an eighth grade level by Flesch-Kincaidgrade level. The Flesch-Kincaid formula was developed toestimate the ease of reading and understanding based onsyllables per word and words per sentence (14). In addition,baseline sociodemographic and comorbidity data were col-lected, and each patient completed the QOLRAD. MeanQOLRAD scores for each dimension were compared by ttest with published means for a gender-matched cohort ofpatients referred for endoscopy for upper GI symptoms (9).The Spearman’s rank correlation coefficient for the medianQOLRAD score and the median utility rating was calcu-lated.
RESULTS
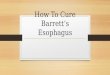
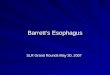
Patients enrolled in the study were aged 50–78 yr (medianage 67), 93% were white, and all were men. Fifty-threepercent were high school graduates, and all subjects weretaking a proton pump inhibitor. Table 1 lists the meanQOLRAD score for our study cohort, the previously pub-lished cohort of male patients (9), and the difference inmean scores. This difference was statistically significant foreach dimension (p � 0.001) (Fig. 1). In addition, the dif-ference in mean scores was greater than 1 unit supporting aclinical significance as well (10). The median utility forindividual scenarios ranged from 0 to 8 (Table 2, Fig. 2).The median QOLRAD was 6.80 (scale of 0–7), the medianutility was 4 (0 equivalent to being dead, 10 equivalent tobeing in perfect health) and their correlation coefficient was0.10 (p � 0.71).
DISCUSSION
Although many have studied the effect of gastroesophagealreflux disease (GERD) on HRQL, few studies have focused
Table 1. Mean QOLRAD Scores by Dimension
DimensionBE CohortMean (SD)
ComparisonCohort (9)Mean (SD)
Differencein Scores
Emotional distress 6.1 (1.15) 4.5 (1.6) 1.6†Sleep disturbance 6.2 (1.15) 4.7 (1.6) 1.5†Food and drink problems 5.8 (1.25) 3.8 (1.6) 2.0†Physical/social functioning 6.6 (0.54) 4.9 (1.5) 1.7†Vitality 6.0 (1.22) 3.7 (1.6) 2.3†
* 1 unit � important change (10).† 1.5 units � very important change (10).
2194 Fisher et al. AJG – Vol. 97, No. 9, 2002

on HRQL of patients with BE. Of these BE studies, mostaddress HRQL after surgical intervention: fundoplicationfor GERD (15) or esophagectomy for adenocarcinoma (16–18). Using the SF-36, Eloubeidi and Provenzale (3) com-pared the HRQL in a cohort of veteran patients with histo-logically documented BE to veteran patients with GERD butno BE. The HRQL of the BE and GERD patients was notsignificantly different, but for both groups it was reduced(lower SF-36 scores) compared with age and gender-ad-justed population norms. The duration and frequency ofheartburn symptoms was not different between the twogroups, but BE patients were less likely to have severeversusmild heartburn and less likely to have nocturnalsymptoms. Of note, the comorbidity index and proton pumpinhibitor use did not differ significantly between the twogroups (3).
We have tested veteran patients. Patients with BE are onaverage 55–63 yr at diagnosis, predominantly white andmale (19). Patients followed within the veteran medicalsystem are also predominantly older white men. Althoughthis does not preclude psychometric evaluation of the newinstrument for other populations, veterans represent a validstudy population for this condition.
Although the preferences given for many of the BE sur-veillance scenarios in the new instrument were reduced, theHRQL as measured by the QOLRAD was relatively high.To provide a context for the QOLRAD results in our BEcohort, these were compared with scores from a previouslypublished cohort of gender-matched patients referred forupper endoscopy. The QOLRAD scores in the BE cohort
Figure 1. The vertical axis denotes the QOLRAD score on a scale of 1 (lowest HRQL) to 7 (highest HRQL). The horizontal axis denoteseach dimension of the QOLRAD (emotions, sleeping, eating/drinking, physical/social functioning, vitality) and the mean total QOLRADscore. The black vertical bars represent the mean QOLRAD scores for the study cohort of veterans with BE for each dimension and themean total. The gray vertical bars represent the mean QOLRAD score for the previously published cohort of men referred for endoscopyfor GI symptoms (9). The difference is significant for each dimension (p � 0.001).
Figure 2. The vertical axis denotes the utility score on a scale of 0(equivalent to being dead) and 10 (equivalent to being in perfecthealth). The vertical bars represent the median utility score for eachof the 16 scenarios (labeled A through P).
Table 2. Median Utility Scores by Scenario
Scenario MedianInterquartile
Range
1 8 8–102 7 5–83 4 0–74 5 3–85 5 5–86 3 0–67 5 3–78 2 0–59 5 3.5–510 2 0–511 4 3–512 1 0–213 2 0–314 0 0–215 5 4–816 3 0–5
2195AJG – September, 2002 Quality of Life in BE Surveillance Patients

were significantly higher than the comparison cohort in eachof the five dimensions (9). Although both cohorts were100% male and predominantly white, there are differencesbetween the populations, which are detailed in Table 3.Although confounding is possible, particularly because ofthe differential rates of medication use for GI symptoms,there is other evidence that BE patients may be less symp-tomatic from GERD than patients without Barrett’s epithe-lium (2, 20). Using a symptom scale, Iascone et al. found atrend toward decreased incidence and severity of heartburnand regurgitation in BE patients compared with patientswith esophagitis (21). Winters et al. documented statisti-cally greater frequency of daytime heartburn reported bypatients with reflux esophagitis compared with those withBE or normal mucosa (22). Johnson et al. demonstrateddecreased sensitivity to acid in patients with BE comparedwith patients with reflux esophagitis (20). In Eloubeidi andProvenzale’s study, similar proportions of patients in the BEgroup and GERD without BE group were taking medication,and BE patients were still less symptomatic although not asdramatically so (3).
No disease-specific HRQL instruments exist to evaluatepatients with BE. We have developed a new instrument tomeasure HRQL of patients with BE undergoing surveillanceand found the HRQL to be reduced. As with our prior study,scenarios with more favorable outcomes scored higher thanthose with less favorable outcomes, which supports the facevalidity and comprehensibility of the instrument. TheHRQL using the utility instrument did not correlate with thedisease-specific HRQL measured by the QOLRAD. Thisfinding suggests that the new instrument does not merelymeasure the impact of reflux symptoms and contributes toits discriminant validity. The component or components ofthe surveillance paths responsible for the reduced patientpreferences, i.e., the decline in HRQL as measured by thenew instrument are unknown. Future work includes testingthe instrument in larger numbers of patients, formally ana-lyzing the discrete components of the scenarios to determinethe cause of the decrement in HRQL of patients with BEundergoing surveillance and establishing convergent–diver-gent validity by factor analysis of these components.
This instrument has both research and clinical applica-tions. Given the uncertain mortality benefit of BE surveil-lance, patient preferences should impact decision making.This instrument can help capture patient-centered informa-tion regarding, for example, the value of diagnosing cancerat an early stage balanced against patient preferences for therisks of surveillance or surgical intervention. Although theinstrument itself is not practical for administration in a clinicsetting, the information obtained from this and future studiescan improve the dialogue between patient and practionersby highlighting the risks and benefits of surveillance. Im-portantly, the results of these utility assessments can beapplied to decision analysis by incorporation into a Markovmodel. For example, the scenario describing BE portrays thestate of health of an individual with BE who undergoessurveillance and has no complications. It outlines a 20-yrlife expectancy and what the patient can expect related to hisBE over that time period. Likewise, there are scenarios thatdescribe BE with dysplasia, surveillance with perforationrequiring surgery, surveillance with perforation resulting indeath, etc. Each of these scenarios will map to a state ofhealth in a recursive BE decision model. Results from sucha model can further clarify the costs and benefits of surveil-lance and improve clinical care.
ACKNOWLEDGMENTS
Deborah Fisher, M.D., M.H.S., is supported by an Agencyfor Healthcare Research and Quality, Health Services Re-search Fellowship. Dawn Provenzale, M.D., M.S., is sup-ported by a National Institutes of Health grant (K-24 DK-02926-02) and a National Cancer Institute grant (263-MQ-10167). Hayden Bosworth, Ph.D., is supported in part by aVeterans Affairs Health Services Development grant (11R-20-034).
Reprint requests and correspondence: Deborah Fisher, M.D.,508 Fulton Street, Building 16, Room 70, GI Outcomes Research,Durham, NC 27705.
Received Nov. 6, 2001; accepted Apr. 9, 2002.
REFERENCES
1. Spechler SJ, Goyal RK. Barrett’s esophagus. N Engl J Med1986;315:362–71.
2. Sampliner RE. Practice guidelines on the diagnosis, surveil-lance and therapy of Barrett’s esophagus. Am J Gastroenterol1998;93:1028–32.
3. Eloubeidi MA, Provenzale D. Health-related quality of lifeand severity of symptoms in patients with Barrett’s esophagusand gastroesophageal reflux disease patients without Barrett’sesophagus. Am J Gastroenterol 2000;95:1881–7.
4. Guyatt GH, Feeny DH, Patrick DL. Measuring health-relatedquality of life. Ann Intern Med 1993;118:622–9.
5. Bleichrondt H, Johannesson M. The validity of QALYs: Anexperimental test of constant proportional tradeoff and utilityindependence. Med Decis Making 1997;17:21–32.
6. Johannesson M. The ranking properties of healthy-year equiv-
Table 3. Comparison of Study Cohort and Previously PublishedCohort
BE CohortComparisonCohort (9)
Male 100% 100%Age (yr) mean 66.9
(SD 8.5)mean 48.4(SD 15.2)
White 93% 86%Country U.S.A. U.S.A., U.K., Canada,
AustraliaTaking medication
for GIsymptoms (%)
100% 68%
Inclusion criteria Biopsy-provenBE
Referral for endoscopyfor upper GI symptoms
2196 Fisher et al. AJG – Vol. 97, No. 9, 2002

alents and quality-adjusted life-years under certainty and un-certainty. Int J Technol Assess Health Care 1995;11:40–8.
7. Mackeigan LD, O’Brien BJ, Oh PI. Holistic versus compositepreferences for lifetime treatment sequences for type 2 diabe-tes. Med Decis Making 1999;19:113–21.
8. Johannesson M, Pliskin JS, Weinstein MC. Are healthy-yearequivalents an improvement over quality-adjusted life years?Med Decis Making 1993;13:281–92.
9. Wiklund IK, Junghard O, Grace E, et al. Quality of life inreflux and dyspepsia patients psychometric documentation ofa new disease-specific questionnaire (QOLRAD). Eur J Surg1998;583(suppl):41–9.
10. Talley NJ, Fullerton S, Junghard O, et al. Quality of life inpatients with endoscopy-negative heartburn: Reliability andsensitivity of disease-specific instruments. Am J Gastroenterol2001;96:1998–2004.
11. Stewart AL, Greenfield S, Hays RD, et al. Functional statusand well-being of patients with chronic conditions. Resultsfrom the Medical Outcomes Study. JAMA 1989;262:907–13.
12. Stewart AL, Hays RD, Ware JE Jr, et al. The MOS short-formgeneral health survey. Reliability and validity in a patientpopulation. Med Care 1988;26:724–35.
13. Weinberger M, Samsa GP, Hanlon JT, et al. An evaluation ofa brief health status measure in elderly veterans. J Am GeriatrSoc 1991;39:691–4.
14. Klare GR. Readability. In: Person PD, Barr R, Kamil ML, eds.Handbook of reading research. New York: Longman, 1984:681–744.
15. Farrell TM, Smith CD, Metreveli RE, et al. Fundoplicationprovides effective and durable symptom relief in patients withBarrett’s esophagus. Am J Surg 1999;178:18–21.
16. Stein HJ, Feith M, Mueller J, et al. Limited resection for earlyadenocarcinoma in Barrett’s esophagus. Ann Surg 2000;232:733–42.
17. Kuster GG, Foroozan P. Early diagnosis of adenocarcinomadeveloping in Barrett’s esophagus. Arch Surg 1989;124:925–7.
18. Provenzale D, Schmitt C, Wong JB. Barrett’s esophagus: Anew look at surveillance based on emerging estimates ofcancer risk. Am J Gastroenterol 1999;94:2043–53.
19. Katzka DA, Rustgi AK. Gastroesophageal reflux disease andBarrett’s esophagus. Adv Gastroenterol 2000;84:1137–61.
20. Johnson DA, Winters C, Spurling TJ, et al. Esophageal acidsensitivity in Barrett’s esophagus. J Clin Gastroenterol 1987;9:23–7.
21. Iascone C, DeMeester TR, Little AG, et al. Barrett’s esopha-gus functional assessment, proposed pathogenesis, and surgi-cal therapy. Arch Surg 1983;118:543–9.
22. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’sesophagus a prevalent, occult complication of gastroesopha-geal reflux disease. Gastroenterology 1987;92:118–24.
APPENDIX 1
Appendix 1 is the script provided for patients (in italics)explaining the scenarios and their rating.
IntroductionBE is a condition that results from having heartburn for along time. This condition increases a person’s risk fordeveloping cancer of the esophagus. Because of this risk ofcancer, periodic endoscopy and biopsy are recommended.Although cancer may develop 10 or more yr in the future,surveillance is recommended now to detect changes such as
dysplasia. Dysplasia is a condition that leads to cancer, andit is one of the stages before cancer of the esophagusdevelops.
Upper EndoscopyThe person must report to the Veterans Affairs for upperendoscopy. Upper endoscopy involves placing a lighted tubeinto the esophagus and taking biopsies of small tissue sam-ples to evaluate for any changes that could lead to cancer.The person will have nothing to eat or drink after midnightthe night before his upper endoscopy. Then he reports to theVeterans Affairs the morning of the procedure. His throat issprayed with medication to numb the area, but there may bemild discomfort as he swallows the tube. He will have an i.v.line placed in his arm through which he will receive med-ications for sedation and pain. The procedure lasts approx-imately 20 min. He will need to stay at the Veterans Affairsfor approximately 1 h afterwards while he recovers from themedications. He will then be allowed to go home, butbecause he had received sedation for the procedure, he willnot be able to drive or return to work the day of theprocedure. He will be able to eat and drink normally as soonas he leaves the hospital. He may return to work and hisusual activities the day after the procedure.
PerforationPerforation is a small hole in the esophagus that may occuras a result of an endoscopic procedure. This will requirethat he has an operation to repair the hole in the esophagus.The operation will involve a 2-wk hospitalization. At the endof that time, he will be discharged from the hospital.
SurveillanceYou are going to read about a series of situations related toBE. The imaginary individuals in the situations below havebeen invited to participate in a surveillance program. Sur-veillance is a program of periodic upper endoscopy withbiopsy. The purpose is to detect changes in the esophagusthat could lead to cancer or that is early cancer and toprovide treatment for them if these changes are found. Youwill read about several situations related to surveillance.
RatingI would like your opinion about these situations and will askyou as part of this study to rate them. You will be asked toplace this card on a line to show the value you give thesituation described. In other words, if you think it is as badas being dead you would give the value 0. If you think thesituation described is as good as being in perfect health,then you would give it a score of 10. Please rate eachperson’s health on a scale of 0 to 19 with 0 being the worstpossible state of health from your perspective and 10 beinggood health, no limitations at all. You may use the samenumber more than once. You may mark between numbers,for example halfway between 2 and 3 is 2.5 or 21⁄2.
2197AJG – September, 2002 Quality of Life in BE Surveillance Patients

APPENDIX 2
Appendix 2 lists the 16 scenarios in the utility instrument.
Person A● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● There will be no complications from the endoscopy.● Upper endoscopy will be performed every 2 yr from now
until he dies.● He will live 20 more yr.
Person B● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● During an endoscopy 5 yr from now, he will sustain a
perforation of the esophagus.● This will require that he has an operation to repair the hole
in the esophagus. The operation will involve a 2-wkhospitalization.
● He will be discharged from the hospital.● As a result, he will be able to eat but may have some
difficulty with swallowing and food getting stuck and willgradually be able to return to his usual activities.
● He will continue to need upper endoscopy every 1–5 yr toevaluate for dysplasia or cancer.
● He will live for 20 more yr.
Person C● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● Approximately 10 yr from now, he will sustain a perfo-
ration (hole) of the esophagus during one of those endos-copies.
● As a result of the complication during the operation torepair this perforation, he will die.
Person D● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● He has just been diagnosed with low-grade dysplasia,
which was found on one of his biopsies during his mostrecent endoscopy last week. Low-grade dysplasia repre-sents a progression toward cancer. Patients who are di-agnosed with low-grade dysplasia need to undergo morefrequent endoscopy to evaluate for any further progres-sion toward cancer.
● He will have to undergo more frequent endoscopy withbiopsy every 6–12 months for the rest of his life.
● He will live 20 more yr.
Person E● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months for the rest of
his life.● During one of those endoscopies 10 yr from now, he will
sustain a perforation (hole) of the esophagus.● This will require that he has an operation to repair the hole
in the esophagus. The operation will involve a 2-wkhospitalization.
● He will be discharged from the hospital.● He will be able to eat but may have some difficulty with
swallowing and food getting stuck and will gradually beable to return to his usual activities.
● Once he has been discharged from the hospital, he willnot require upper endoscopy for BE again.
● He will live 10 more yr after this perforation.
Person F● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months for the rest of
his life.● During one of those endoscopies 7 yr from now, he will
sustain a perforation (hole) of the esophagus.● This will require that he has an operation to repair the hole
in the esophagus.● He will suffer a complication of the operation and will
die.
Person G● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months for the rest of
his life.● During one of those endoscopies 5 yr from now, the
biopsies determine that he has cancer.● He must undergo surgical removal of his esophagus.
2198 Fisher et al. AJG – Vol. 97, No. 9, 2002

● He will stay in the hospital for approximately 2 wk aftersurgery.
● Once he has recovered from surgery: He may continue toexperience some difficulty swallowing and the feelingthat food is getting stuck. He may feel that he gets fullmore easily than he did before.
● Although he is cured of his cancer, he will live theremainder of his life in this condition.
● He will not require any more endoscopies for BE again.● He will live for 10 yr after his surgery.
Person H● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months for the rest of
his life.● During one of those endoscopies 3 yr from now, the
biopsies determine that he has cancer.● He must undergo surgical removal of his esophagus.● He will suffer a complication of surgery and will die.
Person I● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months for the rest of
his life.● During one of those endoscopies, he sustains a performa-
tion (hole) of the esophagus.● In addition, the biopsy results determine that he has can-
cer.● He will require an emergency operation for which he will
be in the hospital for approximately 3 wk.● Most of his esophagus is removed.● At the end of this time, he is likely to have some difficulty
in swallowing and food getting stuck and he gets fullmore easily that before.
● Although he is cured of his cancer, he will live theremainder of his life—approximately 10 more yr—in thiscondition.
Person J● Has BE and low-grade dysplasia. Low-grade dysplasia
represents a progression toward cancer. Patients who arediagnosed with low-grade dysplasia need to undergomore frequent endoscopy to evaluate for any further pro-gression toward cancer.
● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 6–12 months.● During one of those endoscopies 7 yr from now, he
sustains a perforation (hole) of the esophagus.● In addition, the biopsy results determine that he has can-
cer.● He will require an emergency operation.● He will suffer a complication of the operation and will
die.
Person K● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● High-grade dysplasia, which usually progresses to cancer
if not removed, is diagnosed during his most recent en-doscopy last week.
● He must undergo surgery for removal of his esophagus.● After that time, he finds that he has difficulty swallowing
and food getting stuck. Although he does not have cancer,he must live the remainder of his life—approximately 10more yr—in this condition.
Person L● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● Last week, an upper endoscopy diagnosed high-grade
dysplasia.● High-grade dysplasia usually progresses to cancer if not
removed.● He must undergo surgery for removal of his esophagus.● He suffers a complication of surgery and dies.
Person M● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● He was diagnosed with low-grade dysplasia 3 yr ago.
Low-grade dysplasia represents a progression toward can-cer. Patients who are diagnosed with low-grade dysplasianeed to undergo more frequent endoscopy to evaluate forany further progression toward cancer.
● He has been undergoing upper endoscopy with biopsyevery 6–12 months.
● Cancer is found on his most recent endoscopy.● He must undergo surgery with removal of his esophagus.● He must stay in the hospital for 3 wk.● At the end of that time, he will have some difficulty
swallowing, and it may feel as though food is gettingstuck and that he gets full more easily than before.
● Unfortunately, his cancer is not cured.
2199AJG – September, 2002 Quality of Life in BE Surveillance Patients

● His difficulties with swallowing will continue to getworse.
● He will find that he will be able to eat less and less.● He will remain in that condition for the rest of his life,
which will be approximately 1 yr from now.
Person N● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● He was diagnosed with low-grade dysplasia 3 yr ago.● Since then, he has been undergoing upper endoscopy with
biopsy every 6–12 months.● Cancer was found on the most recent endoscopy.● He must now undergo surgery, which requires removal of
his esophagus.● He suffers a complication of surgery and dies.
Person O● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.
● Undergoes endoscopy every 2 yr.● During one of the endoscopies, 2 yr from now, he devel-
ops a complication, which requires hospitalization for 1wk. It does not require surgery.
● While in the hospital:● He receives i.v. antibiotics● He has a tube that goes from his nose to his stomach for
2 days● He is unable to eat for this period of time.● Once the tube is removed, he is able to eat and drink
normally.● He is discharged from the hospital after 1 wk.● He can return to his usual activities.● For the remainder of his life, approximately 10 yr, he
must continue undergoing endoscopy every 2 yr.
Person P● Has BE.● Has daily heartburn for which he takes medicine.● Has no other symptoms related to BE.● Undergoes endoscopy every 2 yr.● During one of the endoscopies, 4 yr from now, he devel-
ops a complication of endoscopy and dies.
2200 Fisher et al. AJG – Vol. 97, No. 9, 2002