Embed Size (px)
Citation preview
CONTENTS
Preface xiAnthony P.C. Yim
Risk Acceptance and Risk Aversion: Patients’ Perspectives on Lung Surgery 287Samuel Cykert
Many patients diagnosed with early-stage, non small cell lung cancer do not acceptpotentially curative lung resection surgery. Decisions for and against surgery often areinfluenced by patients’ perceptions of risk and prognosis. This article reviews the litera-ture pertaining to risk acceptance and risk aversion and discusses the influence of theserisk attitudes on lung cancer surgery decisions. The concept of numeracy is introduced,and future directions that could optimize cancer treatment decisions are suggested.
Optimization of Lung Function Before Pulmonary Resection: Pulmonologists’Perspectives 295 Aymarah M. Robles and Deborah Shure
Pulmonary resection for lung cancer carries a significant risk for patients with under-lying lung disease. Determinations of predicted postoperative lung function and exerciseendurance can help to reduce morbidity and mortality through appropriate patientselection. Other methods of risk reduction for patients with significant chronic obstruc-tive pulmonary disease include inspiratory muscle training, treatment of pulmonaryinfections, bronchodilators, and corticosteroids if needed. Smoking cessation also shouldbe encouraged.
Methodology for Quality-of-Life Assessment: A Critical Appraisal 305Benny Chung-Ying Zee and Tony S.K. Mok
Technologic advancements have transformed diseases such as cancer from a usuallyfatal disease to a curable illness for some patients and a chronic condition for many more.This change has resulted in an increasing appreciation for the health-related quality of lifeof patients diagnosed with cancer and the quality of care they receive. Knowledge ofhealth-related quality of life provides helpful information to primary care providers,specialists, other health care providers, patients, and families to understand and explorefurther their role in symptom management and appropriate means for providing specialcare for patients throughout the course of cancer. Partly due to the realization of thisneed, academic research on quality of life has been active since the 1980s and 1990s.Health-related quality of life has become an important end point in cancer clinical trials,and it has presented methodologic issues that have been areas of active research. Thisarticle discusses several methodologic issues in the research for health-related quality of life.
QUALITY OF LIFE AFTER THORACIC SURGERY
VOLUME 14 • NUMBER 3 • AUGUST 2004 v

Acute and Chronic Reduction of Pulmonary Function After Lung Surgery 317Ibrahim Bulent Cetindag, William Olson, and Stephen R. Hazelrigg
Thoracic surgeons are facing an increased number of complicated and elderly patientsfor consideration of pulmonary resection. Preoperative prediction of pulmonary func-tion changes is important in marginal patients. Several variables (ie, surgical approach,extent of resection, and postoperative management) play roles in lung function changes,especially in the early postoperative period. Pulmonary rehabilitation is helpful in therecovery of cardiopulmonary function for patients who are left with marginal respira-tory volumes.
Acute Postoperative Compromise in Cardiovascular Function After Chest Surgery 325 Joseph LoCicero, III
Major chest operations place a significant strain on all physiologic systems in the body.Strain on the cardiovascular system can lead to the most serious problems or even death.The problems are not limited to ischemia, arrhythmias, or heart failure, but also includecardiac herniation and hypertensive crisis. Attention to preoperative cardiovascular riskfactors, appropriate preparation, early recognition, and treatment are essential to pre-vent potential catastrophic cardiac events from leading to life-threatening situations inthe postoperative period.
Shoulder Function After Thoracic Surgery 331Wilson W.L. Li, T.W. Lee, and Anthony P.C. Yim
Thoracic procedures are considered to be among the most painful surgical incisions andare associated with considerable postoperative pain and shoulder dysfunction, severelyaffecting mobility and activities of daily living. Improper patient positioning, muscledivision, perioperative nerve injury, rib spreading, and consequent postoperative paininfluence the patient’s postoperative shoulder function and quality of life. To reduceaccess trauma and postoperative morbidity, various alternative modalities have beenproposed to replace the standard posterolateral thoracotomy, including muscle-sparingtechniques and video-assisted thoracic surgery. Initial evaluations suggest that thesealternatives are associated with significantly better postoperative shoulder function.
Postthoracotomy Pain Syndrome 345Manoj K. Karmakar and Anthony M.H. Ho
Postthoracotomy pain syndrome occurs in some 50% of patients. It manifests as chronicneuropathic and myofascial pain. Preemptive analgesia prior to surgery might reduce itsincidence. Surgical techniques that minimize intercostal nerve injury show promise, butno technique has emerged as the definitive answer. Treatment is seldom totally satisfac-tory and might require long-term multidisciplinary pain management.
Quality of Life After Lung Cancer Resection 353Wilson W.L. Li, T.W. Lee, and Anthony P.C. Yim
Lung cancer is the most common cancer in the world, with the highest cancer mortalityrate by far. Although resection remains the treatment of choice in early-stage non small-cell lung cancer, the prognosis remains grim even after surgical treatment. In a patientpopulation with such a high mortality rate, evaluation and preservation of quality of life(QOL) after treatment is imperative. More prospective, longitudinal studies with largerstudy populations and a longer follow-up period are needed to more accurately portraythe course of QOL in lung cancer patients and improve postoperative care.
vi CONTENTS

Quality of Life After Esophageal Surgery 367Hiran C. Fernando and James D. Luketich
Quality of life measurement (QOL) is being reported with increasing frequency in thesurgical literature. The authors and others have found that the use of a generic instru-ment such as the SF36 used in combination with a disease-specific instrument will pro-vide the most comprehensive information. Gastroesophageal reflux disease (GERD) is asignificant health problem that primarily affects the QOL of a large segment of the pop-ulation. New therapies for GERD continue to be developed and introduced into clinicalpractice. QOL assessment should be an important part of the evaluation of these newtherapies. Similarly, the management of esophageal cancer and high-grade dysplasia isalso controversial. QOL assessment should be a crucial factor in determining which sur-gical or nonoperative approach is used for these patients.
Quality of Life After Lung Volume Reduction Surgery 375Douglas E. Wood
Emphysema produces disabling symptoms with an enormous impact on quality of life.Physiologic and functional variables used to evaluate outcomes of lung volume reduc-tion surgery are poor surrogates for the outcomes that are important to patients—reliefof symptoms and improvement in quality of life. Disease-specific and general measure-ments of health-related quality of life have been reported in several series of lung vol-ume reduction surgery outcomes and uniformly show the benefit of lung volume reductionsurgery in relieving the symptoms of dyspnea and improving quality of life in patientswith emphysema.
Quality of Life After Lung Transplantation 385Cliff K. Choong and Bryan F. Meyers
Lung transplantation is an accepted form of treatment for many end-stage lung diseases.Numerous studies have reported improvements in pulmonary function and exerciseperformance after lung transplantation. The survival of lung transplant recipients alsohas improved as a result of improved patient selection, perioperative care, surgical tech-niques, and immunosuppression regimens. Despite the potential differences in patientcharacteristics, study designs, and types of instruments used, this review of the literatureshowed several common findings. Important improvements in quality of life are reportedafter lung transplantation. These improvements were observed when cross-sectionalcomparisons were made across the cohort of candidates and recipients and during longi-tudinal follow-up of patients pretransplant and posttransplant. The improvements inquality of life after transplantation seem to be sustained for 1 to 3 years after transplant.Lung transplant recipients generally were satisfied with their decision to have under-gone transplantation.
Return to Work After Thoracic Surgery: An Overlooked Outcome Measure in Quality-of-Life Studies 409 Chuong D. Hoang, Marc C. Osborne, and Michael A. Maddaus
An important, but poorly defined and often unrecognized aspect of global quality of lifeafter undergoing thoracic surgery is the patient’s ability to return to work. Furtherimprovement in postoperative quality of life is unlikely without a better understandingof the factors that influence the ability to work. The available data on return to work afterthoracic surgery highlight the urgent need for comprehensive clinical investigations tobe performed.
CONTENTS vii

Chronic Respiratory Failure After Lung Resection: The Role of Pulmonary Rehabilitation 417 Bartolome R. Celli
Pulmonary rehabilitation has become the cornerstone of treatment of symptomaticpatients with chronic lung disease. In several published randomized trials, rehabilitationhas been compared with optimal medical therapy and has been shown to have moreimpact on outcomes of importance to patients than any other therapy. The NationalEmphysema Therapy Trial reaffirmed the central role of rehabilitation in the manage-ment of patients with chronic obstructive pulmonary disease. Rehabilitation now is anintegral part of the overall selection process and treatment of patients to be offered lungreduction surgery and lung transplant. This article describes major advances in pul-monary rehabilitation, explains and documents why rehabilitation should be included inthe evaluation of patients with lung disease, and expands on its role in patients beingconsidered for high-risk surgery.
Index 429
viii CONTENTS

FORTHCOMING ISSUES
October 2004
MesotheliomaDavid J. Sugarbaker, MD, andMichael Chang, MD, Guest Editors
February 2005
Thoracic Anesthesia and Pain ManagementJerome M. Klafta, MD, Guest Editor
RECENT ISSUES
May 2004
Aggressive Surgery for Lung Cancer Valerie W. Rusch, MD, Guest Editor
February 2004
Imaging Modalities in General Thoracic SurgeryNasser K. Altorki, MD, andDavid F. Yankelevitz, MD, Guest Editors
November 2003
Surgery for EmphysemaKeith S. Naunheim, MD, Guest Editor
August 2003
Lung TransplantationG. Alexander Patterson, MD, Guest Editor
May 2003
Tracheal SurgeryDouglas J. Mathisen, MD, Guest Editor
THE CLINICS ARE NOW AVAILABLE ONLINE!
Access your subscription at:http://www.TheClinics.com

Thorac Surg Clin 14 (2004) xi
Preface
Quality of Life After Thoracic Surgery
Anthony P.C. Yim, MD, FRCS, FACS, FCCP, FHKAM
Guest Editor
Traditionally, surgical mortality and major mor-
bidity have been the standard outcome parameters in
volume reduction surgery, and lung transplantation;
and the impact of functional impairment such as
studies involving chest operations. Although these
data continue to provide important information, with
the advances in anesthetic and surgical techniques
and technology, mortality and major morbidity fig-
ures alone are increasingly inadequate in meeting the
growing needs for detailed comparison of new sur-
gical approaches and rising expectations from
patients of surgery.
This issue of Thoracic Surgery Clinics of North
America focuses on the various aspects of post-
operative quality of life after thoracic surgery. The
carefully chosen topics cover preoperative patient
counseling and risk assessment; preoperative optimi-
zation of lung function; a critical appraisal of the
different health-related quality-of-life instruments
currently in use; impairment of pulmonary, cardio-
vascular, and shoulder functions after lung resection;
chronic pain syndrome; quality of life after different
procedures—lung resection, esophageal surgery, lung
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00027-1
chronic respiratory failure and loss of work on the
patients, their families, and society.
The articles in this issue have been written by
renowned experts in their fields. I would like to thank
all the authors for their contributions, which I trust
the readers will find both useful and educational.
I would also like to thank our consulting editor,
Dr. Mark Ferguson, for the privilege and opportunity
to put this issue together.
Anthony P.C. Yim, MD, FRCS, FACS, FCCP, FHKAM
Department of Surgery
Professor of Surgery and
Chief of Cardiothoracic Surgery
The Chinese University of Hong Kong
The Prince of Wales Hospital
Shatin, NT, Hong Kong SAR, China
E-mail address: [email protected]
s reserved.
Thorac Surg Clin 14 (2004) 287–293
Risk acceptance and risk aversion: patients’ perspectives on
lung surgery
Samuel Cykert, MDa,b,*
aDepartment of Medicine, Division of General Internal Medicine, The University of North Carolina School of Medicine,
Chapel Hill, NC USAbInternal Medicine Program, Moses Cone Hospital, 1200 North Elm Street, Greensboro, NC 27401, USA
Lung cancer is the leading cause of cancer death in exposure at some point in their lives and often are
the United States. Estimates derived from the National
Cancer Institute’s Surveillance Epidemiology and End
Results program suggested that during 2003, 172,000
new patients would be diagnosed with lung cancer,
and 157,000 attributable deaths would occur. Non–
small cell histology is the predominant lung cancer
type, representing 80% of all cases [1,2]. Surgical
resection during stage I and stage II disease remains
the only reliable cure, with a 5-year survival rate of
about 40% when considering all patients in these
clinical stages [3]. Patients who do not undergo ap-
propriate lung resection are limited to a median
survival of less than 1 year, during which time they
endure the consequences of progressive cancer and
death [4,5]. Despite the morbidity associated with the
choice against surgery, administrative data suggest
that 24% of white patients and 36% of black patients
who are diagnosed clinically with stage I or stage II
disease do not undergo surgery [3]. Despite facing
a rapidly progressive, fatal disease, many patients
and their physicians are deciding exclusively or mu-
tually that the only reliable curative treatment is not
worth pursuing.
By definition, patients diagnosed with non–small
cell lung cancer have experienced significant tobacco
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00016-7
This work was supported by the University of North
Carolina Project on Health Outcomes, the Education Com-
mittee of the Greensboro Area Health Education Center,
and the Moses Cone Health System.
* Internal Medicine Program, Moses Cone Hospital,
1200 North Elm Street, Greensboro, NC 27401.
E-mail address: [email protected]
affected by the pulmonary and cardiovascular con-
sequences of such exposure. Even with the high
prevalence of tobacco-associated comorbid conditions
among lung cancer patients, however, few have the
severe degree of these illnesses that represent absolute
contraindications to surgery. Many patients do not
pursue lung cancer surgery because of their physi-
cian’s clinical judgment or their own risk perceptions.
This article reviews the role of these risk perceptions
in decisions about lung cancer surgery. The following
questions relevant to this topic are addressed:
1. How accurately do patients understand con-
versations about risk?
2. How might risk aversion affect surgical
decisions?
3. Can prognostic accuracy alter patients’ treat-
ment decisions?
4. When patients’ preferences are measured for-
mally in a manner that takes risk attitudes into
account, what lung cancer outcomes do they
care about most?
5. What can clinicians tell patients about these
outcomes of interest?
6. What future directions should be pursued?
General risk perceptions and numeracy
The idea that numeracy (the construct that
describes facility with basic probability and numerical
concepts) affects the accuracy of patients’ risk per-
ceptions has been postulated and measured only more
s reserved.

S. Cykert / Thorac Surg Clin 14 (2004) 287–293288
recently. Schwartz et al [6] surveyed 287 female
veterans. Of these women, 96% were high school
graduates, and 36% had attended at least some col-
lege. Of the group, 85% had had a previous mammo-
gram. Numeracy of participants was tested using three
questions: (1) the number of times 1000 coin flips
would come up heads (about 500), the conversion of a
percentage (1%) to a proportion (10 of 1000), and a
proportion (1 in 1000) to a percentage (0.1%). Only
16% answered all three questions correctly compared
with 26% with two correct answers, 28% with one
correct answer, and 30% with no correct answers. The
participants were presented with data describing the
risk reduction of breast cancer death related to screen-
ing mammography. Of respondents who answered all
three numeracy questions correctly, 40% were able to
present accurately the breast cancer risk reduction,
compared with 9% who answered one question cor-
rectly and 6% who answered none correctly. Although
strong numeracy skills were associated with better
understanding of mammography benefit, most of
the high numeracy group still was not able to por-
tray accurately the effect of mammography on breast
cancer. The authors did not report the effect of
numeracy on the number of study participants who
then went on to get mammograms. Two other assess-
ments of numeracy have been published [7,8]. One
study showed that many highly educated patients have
numeracy difficulties [8], and the other study showed
that for patients with low numeracy scores, the mea-
surement of health preferences is less likely to be
reliable [7]. No reports connect level of numeracy to
real decisions concerning cancer or surgical care.
Authors of an article published in 2001 described
risk perceptions of 71 patients with symptomatic ca-
rotid artery disease who were awaiting endarterectomy
[9]. All patients in this study were given a scripted
presentation by the consulting surgeon. During the
presentation, patients were advised of the 3-year risk
of stroke without surgery, the reduction of risk attrib-
utable to surgery, and the immediate stroke risk during
operation. Numbers were quoted exactly and displayed
graphically during the consultation. Patients under-
stood that the operation would reduce their 3-year
stroke risk. The numbers quoted for risk without
surgery and the reduced risk after successful surgery
were markedly overestimated, however (57% versus
22% for baseline risk and 24% versus 8% for postsur-
gery risk). The risk of endarterectomy itself not only
was overestimated at initial survey (10% versus 2%),
but also when patients were resurveyed the day before
operation the surgical risk was quoted as even higher
(14%). There was a statistically significant correlation
of patients who perceived greater risk also perceiving
greater benefit. The authors did not offer a formal
analysis of the association of risk/benefit perceptions
with actual surgical decisions except to state that 15%
of patients who estimated surgical risk higher than
their baseline risk still opted for carotid endarterectomy.
The same authors now are investigating the use of
written pamphlets and computer aids to improve the
risk communication [9].
Risk aversion, risk acceptance, and patient
preferences
The role of risk aversion in surgical decisions has
been discussed in past reports. In a hypothetical
decision model used to evaluate transurethral prosta-
tectomy versus watchful waiting for benign prostatic
hypertrophy, Cher et al [10] showed that when the
complications of sexual dysfunction and urinary in-
continence were considered, risk-averse patients con-
sistently decided in favor of a watchful waiting
strategy rather than surgical intervention. For lung
cancer specifically, a similar analysis explored the
influence of risk aversion attitudes on the cost-effec-
tiveness of diagnostic algorithms for solitary pulmo-
nary nodules [11]. The base case used in this study
was a 50-year-old man with a 3-cm, peripheral pul-
monary nodule. The diagnostic strategies included im-
mediate thoracoscopy, sputum cytology followed by
thoracoscopy, fine-needle aspiration followed by thor-
acoscopy, sputum cytology followed by fine-needle
aspiration followed by thoracoscopy, and sputum
cytology followed by fine-needle aspiration; if strat-
egies were nondiagnostic, expectant management was
implemented. Besides the strategies themselves, com-
parisons also were made between patients who were
risk averse to procedures and patients who were
averse to waiting and worrying about cancer. The
results of the study are outdated in that positron
emission tomography was not a diagnostic option
for difficult cases, and the expectant management
strategy consisted of frequent chest x-rays at 3- to
6-week intervals with cost accounting for only a
2-month period. Despite these limitations, the authors
did show that whether a patient was more risk averse
toward procedures or more averse toward waiting for
and worrying about a diagnosis influenced cost-effec-
tiveness calculations and possibly actual decisions.
Another method used to assess the relationship of
risk aversion to surgical decisions is the measurement
of an individual’s perception of surgery as a treatment
alternative for a defined condition. The best example
of this method is the aversion to surgery score as
defined by Oddone et al [12] in their study pertaining

S. Cykert / Thorac Surg Clin 14 (2004) 287–293 289
to racial disparities in the use of carotid endarterec-
tomy. These investigators enrolled patients who had
at least a 50% carotid stenosis as shown by Doppler
ultrasound. As part of a predecision survey, partici-
pants were asked to ascertain the risk of immediate
death that they would be willing to accept to be
treated with a pill rather than an operation to reduce
10-year stroke risk by the same magnitude. Surgery
was assigned a fixed mortality risk of 5%. The
aversion to surgery score was determined using a
standard gamble approach in which the interviewer
determined the probability of death for taking the pill
to be indifferent compared with the 5% mortality risk
for surgery (probability of indifference [Pi]). The
surgical mortality risk was subtracted from Pi. This
percentage was converted to a decimal probability. If
the patient considered a 10% immediate death risk for
the pill to be equivalent to a 5% risk of surgery, Piwould be equal to 10%; the aversion to surgery score
would be 10% � 5% converted to the decimal score
of 0.05. Similarly, if Pi were 20%, the aversion to
surgery score would be 0.15, and if Pi were 5%, the
score would be 0. In the analysis, the aversion to
surgery score was divided into quartiles (0–0.025,
0.025–0.075, 0.075–0.250, and > 0.250). A logistic
regression model was used to identify predictors of
carotid endarterectomy while controlling for Rand
appropriateness rating and patient’s race, surgical
experience, self-rated health, Charlson comorbidity
score, evaluation site, and aversion to surgery quar-
tile. Patients in the highest aversion score quartile
(>0.250) were only 40% (95% confidence interval
20% to 90%) as likely to receive carotid endarterec-
tomy compared with the lowest quartile. These data
suggest that individuals who fear surgery are less
likely to accept invasive intervention. The author
used this concept in a pilot study of patients with
newly diagnosed stage I or II non–small cell lung
cancer (n = 29). The author was not able to show a
statistically significant effect ( P = 0.77) of the
aversion to surgery score on decisions for (n = 19,
aversion score 0.22) and against (n = 10, aversion
score 0.26) lung resection surgery (unpublished data).
As opposed to risk aversion, attitudes of risk
acceptance influence patient preferences toward more
aggressive therapies. Although most cancer patients
tend to be risk averse [13], Weeks et al [14] showed
that patients who overestimate their prognosis were
more accepting of aggressive life-extending therapy
compared with patients who did not overestimate
prognosis. Specifically the study population had meta-
static non–small cell lung cancer or metastatic colon
cancer. Patients who estimated their probability for
6-month survival as equal to or greater than 90%
were 2.6 times more likely to choose aggressive
treatments than patients who estimated this probabil-
ity as less than 90%. When patients in the overesti-
mation group were cared for by physicians whose
concomitant 6-month survival estimate for that pa-
tient was less than 10%, the odds ratio for aggressive
treatment increased to 8.5. These results suggest that
patients who do not understand the limitations of their
prognosis and treatment are more risk accepting and
pursue therapies that are overaggressive. The data
concerning discordant perceptions between patient
and physician pairs indicate that the larger the phy-
sician-patient communication gap, the more likely the
patient will choose potentially dangerous therapies
for minimal benefit. Because cancer patients often are
unjustifiably optimistic about their long-term survival
[15,16], these findings are likely important for pa-
tients making decisions about lung cancer surgery.
As these authors concluded, more accurate patient
perception of prognosis may be key to making
treatment decisions that are more consistent with
patients’ true values for risk and benefit.
Health utility scores (HUS) represent patient val-
ues assigned to potential outcomes of medical treat-
ments, including thoracic surgery. Classically, these
scores are anchored in such a way that 0 = death and
1 = normal health. The HUS is an indicator of the
quality of life that patients attach to a specific health
state. Although it is controversial which of the three
major methods of utility assessment is the most
accurate [17], the standard gamble approach is the
one that accounts most for patients’ risk attitudes [13].
The HUS derived from the standard gamble is deter-
mined in a manner similar to the aversion to surgery
score. The health state in question is presented, usu-
ally by a trained, face-to-face interviewer, as a guar-
anteed situation. To avert the guarantee, a patient is
asked the immediate risk of death that he or she would
accept to receive a therapy that would return the
patient to normal health. The concept of risk is
explained thoroughly, and patients are presented pos-
sible risk choices in a predefined manner. The percent
risk at which the patient is indifferent between imme-
diate death and the guaranteed health state determines
the HUS. The higher the risk the patient is willing to
take to avert the guaranteed health state, the lower the
value he or she places on that state. In a survey to
define patient values for possible outcomes of lung
resection surgery, the author and colleagues wanted to
determine the average HUS for progressive lung
cancer [18]. The following scenario was presented:
If you were to receive the diagnosis of lung cancer,
imagine that to cure the cancer and restore your

Table 1
Patients’ perception of possible outcomes of lung surgery as
represented by utility scores
Outcome
Utility score* (95%
confidence interval)
Pneumonia requiring
2 wk of hospitalization
0.81 (0.74–0.88)
Atelectasis requiring
bronchoscopic therapy
0.80 (0.72–0.88)
Ventilator dependence for 3 d 0.76 (0.68–0.84)
Ventilator dependence for 15 d 0.66 (0.57–0.75)
Ventilator dependence for 30 d 0.59 (0.49–0.69)
Permanent ventilator dependence
with estimated survival of 6 mo
0.10 (0.04–0.16)
Acute myocardial infarction 0.49 (0.40–0.59)
Can walk only 2 city blocks
without stopping
0.48 (0.40–0.56)
Current activity level reduced
by half
0.44 (0.37–0.51)
Oxygen dependence 0.33 (0.26–0.40)
Need assistance with activities
of daily living
0.19 (0.13–0.25)
Limited to bed-to-chair existence 0.17 (0.11–0.23)
Progressive lung cancer 0.17 (0.10–0.24)
Permanent nursing home placement 0.16 (0.10–0.22)
* Utility scores range from 0, representing death, to 1,
representing perfect health.
Adapted from Cykert S, Kissling G, Hansen C. Patients pre-
ferences regarding possible outcomes of lung resection: what
outcomes should pre-operative evaluation target? Chest
2000;117:1553; with permission.
S. Cykert / Thorac Surg Clin 14 (2004) 287–293290
normal life expectancy a hypothetical treatment is
available. The problem with this hypothetical treat-
ment is that there is a chance of dying immediately
when taking the treatment. If you do not have the
treatment, however, the cancer will progress, and
you likely will die in 18 months. The last 6 months
will involve physical weakening, such as an inability
to walk more than a few steps, and pain that some-
times requires narcotic medications for relief. In
other words, if you take no treatment, you are
guaranteed to live 18 months, but the last 6 would
involve weakness and pain. What percent risk of
dying right now are you willing to take to accept the
hypothetical treatment to cure the cancer and live a
normal life?
If the patient is indifferent between accepting a
70% risk of immediate death associated with taking
the treatment and remaining in the guaranteed health
state, the Pi is equal to 0.7. To calculate the HUS for
progressive lung cancer, Pi simply is subtracted from
1, yielding a value in this case of 0.3. If this Pi were
equal to 95%, the HUS for progressive lung cancer
would be 0.05. By forcing a decision on acceptable
death risk early on, a patient’s risk attitude is incor-
porated into the value placed on the given health state.
Patients can be risk averse concerning surgery but
may be risk accepting of surgery or any treatment
potentially causing immediate death if faced with the
prospect of progressive cancer. Somehow, these com-
peting patient attitudes and values need to be com-
bined into an approach that leads to the most rational
treatment decision.
Decisions about lung resection surgery
Most of the literature that describes preoperative
prediction for postoperative complications of lung
resection surgery uses a composite postoperative
complication outcome that largely includes transient
states, such as atelectasis, pneumonia, and prolonged
mechanical ventilation [19–27]. Using the standard
gamble approach, the author and colleagues docu-
mented that these transient complications were rela-
tively unimportant from a patient’s perspective
(Table 1) [18]. In Table 1, utility score decrements
for atelectasis, pneumonia, and time-limited ventila-
tor therapy apply only during periods that patients are
affected by these complications. Conversely, out-
comes that patients feared most—the outcomes for
which patients were willing to take an 80% risk of
immediate death to avoid—were limitation to a bed-
to-chair existence, the need for help in performance
of activities of daily living, permanent ventilator
dependence, and permanent nursing home placement.
Respondents believed that the HUS for progressive
cancer was just as poor, however, as the scores as-
signed to these severe treatment complications. After
expanding the respondent pool to 181, these HUS
data were used to construct a decision model to simu-
late the lung resection surgery decision for patients
who had stage I or stage II, non–small cell cancer
[28]. One of the goals of this decision analysis was to
identify factors in the decision process that most
powerfully sway patients away from surgery. Some
of the important results from this model output are
as follows:
1. Reasonable variation in the HUS for progres-
sive lung cancer affected the surgical decision
only if the patient was sure to have a disabling
complication combined with a life expectancy
of less than 8 months or if the patient faced a
perioperative mortality of 80% or greater.
2. If the patient was uncertain of the diagnosis or
believed in an alternate therapy for cure, he or
she was more apt to decide against surgery,
S. Cykert / Thorac Surg Clin 14 (2004) 287–293 291
particularly if there was a chance of disabling
complications. The higher the predicted com-
plication rate, the greater the certainty of
diagnosis a patient required to decide in favor
of surgery.
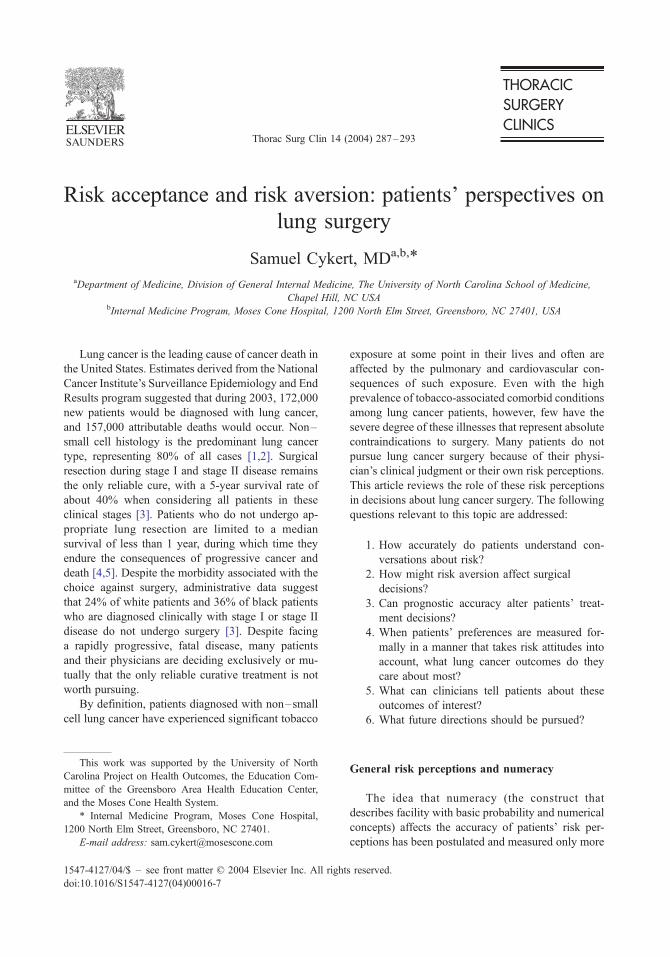
The two-way sensitivity analysis presented in
Fig. 1 graphically shows the relationships described
in the second statement. The pcurenosurg variable
pictured on the x-axis of Fig. 1 can represent either
uncertainty of diagnosis (eg, if there is a 20% chance
that you do not have lung cancer, then there is a 20%
chance you will be free of cancer without lung
surgery) or the belief that an alternative cure, such
as prayer, would work.
Although results from decision modeling are
hypothetical, pilot data derived from newly diag-
nosed lung cancer patients support these concepts
[29]. HUS for progressive lung cancer was no differ-
ent (P = 0.6) for patients who had surgery (n = 19,
HUS = 0.30) compared with patients who did not
(n = 10, HUS = 0.25). In bivariate analysis, patients
who believed that prayer alone could cure their dis-
ease (4 of 10) underwent surgery less often than those
who did not hold this belief (14 of 18; P = 0.05).
Also, of patients who were asked on a 0-to-100 scale
how certain they were about the diagnosis of lung
cancer, patients who answered less than 90% (4 of
12) were less likely to undergo surgery than patients
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
pnoc
omp
- P
roba
bilit
y of
NO
Per
iope
rativ
e C
ompl
icat
ions
0.0 0.1 0.2 0.3 0.4 0.5
pcurenosurg - Probability of Lung Cance
Fig. 1. Two-way sensitivity analysis on the probability of ‘‘cu
tive complications. (Adapted from Cykert S, Phifer N. Surgical d
racially sensitive perceptions of cancer are likely to explain rac
with permission.)
who conveyed a certainty of 90% or greater (15 of
17; P = 0.002). Although these data must be regarded
as preliminary, they re-emphasize the point that
misperception of diagnosis and prognosis potentially
can change risk attitudes and treatment decisions.
How does the interaction of patients’ risk attitudes
toward progressive cancer and debilitating surgical
complications affect acceptance of operative mortal-
ity risk? Using the survey and decision model, if
surgery was the only possible cure, and the diagnosis
of lung cancer was absolutely certain, the model
output suggests that, in the setting of a 100% com-
plication rate, patients would accept an operative
mortality rate of 60% [28]. Dowdie and Wildman
[30] projected the mortality rate to be 40%, but these
authors empirically used much higher values for life
with progressive cancer than the author and col-
leagues obtained from the HUS survey. Further
analysis of the model reveals that with the assumption
of a 30% cure for nonsurgical treatment, the accept-
able operative mortality decreases to 10%. If this
nonsurgical cure rate is fixed at 30% (eg, radiation
therapy for stage Ia non–small cell cancer) [31], and
if a patient is guaranteed not to have any long-term
postoperative debility, the acceptable operative mor-
tality risk becomes 20% or less. If a long-term
debility risk of 30% or greater is assigned, however,
the model output does not yield any acceptable opera-
tive mortality risk.
0.6 0.7 0.8 0.9 1.0
r Resolving Without Surgery
surgery
no surgery
re’’ without surgery and the probability of no periopera-
ecisions for early stage, non-small cell lung cancer: which
ial variation in surgery. Med Decis Making 2003;23:172;

S. Cykert / Thorac Surg Clin 14 (2004) 287–293292
Which patients subjected to lung resection surgery
develop the extent of permanent debility that is un-
acceptable according to patients’ preferences? Two
reports agree that patients who are treated with lobec-
tomy experience a mild-to-moderate decrement in
forced expiratory volume in 1 second (FEV1) 3months
postoperatively that returns to near-baseline 6 months
later [32,33]. The average preoperative FEV1 in both
studies was greater than 2 L. Patients with lower
baseline FEV1 might or might not fare as well. Pneu-
monectomy resulted in much more significant pulmo-
nary function reductions that did not recover over
time. The authors did not correlate the reduced breath-
ing capacity with actual functional status. Investiga-
tors led by Handy and Myrdal [34,35] attempted to fill
this void by reporting on postoperative functional
measurements, including the physical functioning
scale of the SF-36. Both groups found significant
reductions in SF-36 physical functioning scores with
absolute values in the range of 55 to 60. These scores
are statistically different compared with the normal
population but do not represent significant clinical
impairment. A group of pulmonary rehabilitation
patients improved their SF-36 physical functioning
score from 26 to 31, and these values correlated with
an improvement of 6-minute walk test distance from
470 to 536 m [36]. Even with dismally low SF-36
scores (half of age-matched population norms), these
data do not describe a population limited to a bed-to-
chair existence or confined to a nursing home.
Summary
Patients express risk aversion toward surgery,
particularly if surgery can lead to lifelong debility
and loss of independence. When faced with a guar-
antee of progressive lung cancer and no alternatives
for cure, however, patients are willing to take ex-
tremely high risks of postoperative complications and
surgery-related death. This result occurs because risk
aversion toward unrelenting cancer death supersedes
patients’ risk attitudes toward almost all other health
states. By adding conditions such as misunderstand-
ing of prognosis, diagnostic uncertainty, a patient’s
denial of diagnosis, an actual alternative cure such as
radiation therapy, or a perceived alternative cure such
as prayer, decisions can be shifted so that risk
aversion to surgery can predominate. In practical
terms, the following statements can be made:
1. For patients who surely have operable stage I
or stage II non–small cell lung cancer, if
patient risk preferences are taken seriously, the
pulmonary function level and comorbidities
that are acceptable for the offer of surgical care
probably need to be liberalized. Patients with
short life expectancies because of advanced age
or comorbid illness and patients with severe
preoperative functional debility (eg, bed-to-
chair limitation as defined earlier) should not
be candidates, however.
2. The diagnosis of cancer needs to be confirmed
absolutely as often as possible before lung re-
section surgery.
3. Physicians or a staff member must communi-
cate prognosis to a patient as precisely and
numerically as possible and ensure the patient’s
understanding of the data presented.
4. This communicator also must explore a pa-
tient’s trust in the diagnosis and probe for be-
liefs in alternative solutions.
Important areas for future study include the search
for methods that most accurately communicate risk
information to patients, especially patients with low
numeracy skills. Part of this communication effort
should involve the exploration and discussion of
patients’ alternative beliefs and ways of using these
belief systems to help them make the best possible
decisions for their long-term health and quality of
life. Also, clinicians must identify pulmonary and
other predictors of mortality rates and the debility
states that patients’ cite as most important according
to their risk preferences and give up the predictors of
transient postoperative complications that patients
find acceptable.
References
[1] Humphrey E, Smart C, Winchester D. National survey
of the pattern of care for carcinoma of the lung.
J Thorac Cardiovasc Surg 1990;100:837–43.
[2] Travis W, Travis L. Lung cancer. Cancer 1995;75:
191–202.
[3] Bach PB, Cramer LD, Warren JL, Begg CB. Racial
differences in the treatment of early-stage lung cancer.
N Engl J Med 1999;341:1198–205.
[4] Lin AY, Ihde DC. Recent developments in the treat-
ment of lung cancer. JAMA 1992;267:1661–4.
[5] Vrdoljak E, Mise K, Sapunar D, Rozga A, Marusic M.
Survival analysis of untreated patients with non-small-
cell lung cancer. Chest 1994;106:1797–800.
[6] Schwartz I, Woloshin S, Black W, Welch H. The role
of numeracy in understanding the benefit of screening
mamography. Ann Intern Med 1997;127:966–72.
[7] Woloshin S, Schwartz I, Moncur M, Gabriel S, Toste-

S. Cykert / Thorac Surg Clin 14 (2004) 287–293 293
son A. Assessing values for health: numeracy matters.
Med Decis Making 2001;21:382–90.
[8] Lipkus I, Samsa G, Rimer B. General performance on
a numeracy scale among highly educated samples.
Med Decis Making 2001;21:37–44.
[9] Lloyd A, Hayes P, Bell P, Naylor A. The role of risk
and benefit perception in informed consent for surgery.
Med Decis Making 2001;21:141–9.
[10] Cher D, Miyamato J, Lenert L. Incorporating risk atti-
tude into Markov-process decision models. Med Decis
Making 1997;17:340–50.
[11] Raab S, Hornberger J. The effect of a patient’s risk-
taking attitude on the cost-effectiveness of testing strat-
egies in the evaluation of pulmonary lesions. Chest
1997;111:1583–90.
[12] Oddone E, Horner R, Johnston D, et al. Carotid end-
arterectomy and race: do clinical indications and pa-
tient preferences account for differences? Stroke 2002;
33:2936–43.
[13] Stiggelbout A, Kiebert G, Kievit J, Leer J, Stoter G,
DeHaes J. Utility assessment in cancer patients: adjust-
ment of time tradeoff scores for the utility of life years
and comparison with standard gamble scores. Med
Decis Making 1994;14:82–90.
[14] Weeks J, Cook F, O’Day S, et al. Relationship between
cancer patients’ predictions of prognosis and their
treatment preferences. JAMA 1998;279:1709–14.
[15] Siminoff L, Fetting J, Abeloff M. Doctor-patient com-
munication about breast cancer adjuvant therapy. J Clin
Oncol 1989;7:1192–200.
[16] Eidenger R, Schapira D. Cancer patients’ insight into
their treatment, prognosis, and unconventional thera-
pies. Cancer 1984;53:2736–40.
[17] Torrance G, Thomas W, Sacket D. A utility maximi-
zation model for the evaluation of health programs.
Health Serv Res 1972;7:118–33.
[18] Cykert S, Kissling G, Hansen C. Patients preferences
regarding possible outcomes of lung resection: what
outcomes should pre-operative evaluation target?
Chest 2000;117:1551–9.
[19] Pierce R, Copland J, Sharpe K, et al. Preoperative risk
evaluation for lung cancer resection: predicted post-
operative product as a predictor of surgical mortality.
Am J Respir Crit Care Med 1994;150:947–55.
[20] Fergusen M, Little L, Rizzo L, et al. Diffusing capacity
predicts morbidity and mortality after pulmonary re-
section. J Thorac Cardiovasc Surg 1988;96:894–900.
[21] Bousamra II M, Presberg K, Chammas J, et al. Early
and late morbidity in patients undergoing pulmonary
resection with low diffusion capacity. Ann Thorac Surg
1996;62:968–75.
[22] Wang J, Olak J, Ultmann R, et al. Assessment of pul-
monary complications after lung resection. Ann Thorac
Surg 1999;67:1444–7.
[23] Kearney D, Lee T, Reilly J, et al. Assessment of oper-
ative risk in patients undergoing lung resection: impor-
tance of predicted pulmonary function. Chest 1994;
105:753–9.
[24] Nakahara K, Ohno K, Hashimoto J, et al. Prediction of
postoperative respiratory failure in patients undergoing
lung resection for lung cancer. Ann Thorac Surg 1988;
46:549–52.
[25] Busch E, Verazin G, Antkowiak J, et al. Pulmonary
complications in patients undergoing thoracotomy for
lung carcinoma. Chest 1994;105:760–6.
[26] Fergusen M, Reeder L, Mick R. Optimizing selection
of patients for major lung resection. J Thorac Cardio-
vasc Surg 1995;109:275–83.
[27] Epstein S, Faling J, Daly B, Celli B. Inability to per-
form bicycle ergometry predicts increased morbidity
and mortality after lung resection. Chest 1995;107:
311–6.
[28] Cykert S, Phifer N. Surgical decisions for early stage,
non-small cell lung cancer: which racially sensitive
perceptions of cancer are likely to explain racial vari-
ation in surgery. Med Decis Making 2003;23:167–76.
[29] Cykert S, Carey T. Surgical decisions for early non-
small cell lung cancer: a prospective pilot study [ab-
stract]. J Gen Intern Med 2003;18:281.
[30] Dowie J, Wildman M. Choosing the surgical mortality
threshold for high risk patients with stage Ia non-small
cell lung cancer: insights from decision analysis. Tho-
rax 2002;57:7–10.
[31] Gauden S, Ramsay J, Tripcony L. The curative treat-
ment of radiotherapy alone of stage I non-small cell
carcinoma of the lung. Chest 1995;108:1278–82.
[32] Nezu K, Kushibe K, Tojo T, et al. Recovery and limi-
tation of exercise capacity after lung resection for lung
cancer. Chest 1998;113:1511–6.
[33] Bolliger C, Jordan P, Soler M, et al. Pulmonary func-
tion and exercise capacity after lung resection. Eur
Respir J 1996;9:415–21.
[34] Handy J, Asaph J, Skokan L, et al. What happens to
patients undergoing lung cancer surgery? Outcomes
and quality of life before and after surgery. Chest
2002;122:21–30.
[35] Myrdal G, Valtysdottir S, Lambe M, Stahle E. Quality
of life following lung cancer surgery. Thorax 2003;58:
194–7.
[36] Benzo R, Flume P, Turner D, Tempest M. Effect of
pulmonary rehabilitation on quality of life in patients
with COPD: the use of SF-36 summary scores as out-
come measures. J Cardiopulm Rehabil 2000;20:231–4.
Thorac Surg Clin 14 (2004) 295–304
Optimization of lung function before pulmonary resection:
pulmonologists’ perspectives
Aymarah M. Robles, MD, FCCP, Deborah Shure, MD, Master FCCP*
4929 Travis, Houston, TX 77002, USA
Lung resection carries inherent risks for patients tobacco smoking. Tobacco smoking also is the major
with underlying pulmonary disease. Thoracotomy
alone, without resection, has long been known to
diminish lung volume postoperatively [1]. Resection
adds an additional burden depending on the extent of
the resection [1]. Lobectomy tends to decrease post-
operative forced expiratory volume in 1 second
(FEV1) by 10%, and pneumonectomy tends to de-
crease FEV1 by 33%, although exercise capacity does
not decrease proportionately to the loss in FEV1 [2].
Much attention has been focused on prediction of
postoperative lung function to determine an accept-
able level of risk, and although no single test can
determine definitively the safety of a surgical proce-
dure, much has been learned about relative risks. It
also is essential to understand the many risk factors
other than volume loss that relate to morbidity and
mortality from lung resection to prepare the patient
better preoperatively. Some risk factors are unalter-
able; the effects of others can be ameliorated. This
article reviews predictors of postoperative lung func-
tion, preoperative risk factors, and measures to opti-
mize lung function before surgery. The emphasis is
on chronic obstructive pulmonary disease (COPD)
because this disease has been the main area of
research. What information is lacking and needs for
further investigation also are reviewed.
Chronic obstructive pulmonary disease
Most lung resections are performed for broncho-
genic carcinoma, for which the major risk factor is
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00018-0
* Corresponding author.
E-mail address: [email protected] (D. Shure).
risk factor for the development of COPD. Most
candidates for resection for lung cancer have COPD
with its attendant functional impairment. Because the
only known cure for non–small cell bronchogenic
carcinoma currently is surgery, the concern of the
pulmonologist and the surgeon is determining which
patients can tolerate the necessary removal of lung
tissue without developing severe pulmonary disabil-
ity postoperatively.
Prediction of postoperative lung function
Currently a great deal is known about predictors
of postoperative lung function, but clinicians still are
in the same position they were in 1987, when Tisi [3]
observed that no single number or even combination
of numbers can predict a good individual outcome.
There is even no firm lower limit, although high risk
can be determined. Table 1 summarizes the results of
several studies since the 1980s and indicates the
variability among these studies.
Several methods have been used to predict post-
operative lung volumes. Quantitative lung perfusion
scans have been consistently reliable [4–7]. CT also
shows good correlation with actual results [6]. Three
other methods are based on anatomy: the postopera-
tive predicted remaining number of segments as a
percentage of total segments, the predicted remaining
segments as a percentage of total unobstructed seg-
ments (functional segments), and a similar method
based on the number of subsegments. Good correla-
tions have been claimed for all methods, but only one
prospective study has compared all five techniques
[6]. Lung perfusion scanning was found to be the
most accurate. Postoperative predicted FEV1 and
forced vital capacity (FVC) values were the same as
s reserved.

Table 1
Predictors of postoperative pulmonary function
Parameters Study design No. patients Method of prediction Results References
FEV1, FVC Prospective 35 Segments Actual postoperative values at 6 mo were lower than
predicted values for patients with main or lobar bronchial
obstruction; PPO values were accurate for segmental
obstruction
Foroulis et al [65]
FEV1 Prospective 32 Segments Actual postoperative values were higher than PPO values.
Actual values were much higher than PPO values with
inspiratory muscle training
Weiner et al [58]
FEV1, FVC,
TLC, DLCO, VO2max
Prospective 68 Lung scan Actual post-operative values at 6 mo were higher than
PPO values
Bolliger et al [4]
FEV1, DLCO, VO2max Prospective 25 Lung scan Actual postoperative FEV1 and VO2max were the same as
PPO values at 3 mo.
Bolliger et al [5]
Actual postoperative DLCO was higher than predicted.
All actual values were higher than PPO values at 6 mo
FEV1 Retrospective 60 Segments Actual FEV1 was higher than PPO values. Good
correlation for lobectomy, but not for pneumonectomy
Zeiher et al [66]
FEV1, FVC, DLCO,
VO2max
Prospective 44 Lung scan, CT,
segments, functional
segments, subsegments
Lung perfusion scanning was the most accurate followed by
CT. The segment method without regard for obstruction
was the least accurate.
Bolliger et al [6]
For lung scans, the predicted values were the same as the
actual values for all but the VO2max, for which the actual
values were higher than the PPO values.
For all other techniques, the actual values were higher than
PPO values.
The results were not influenced by the presence or absence
of COPD
FEV1, FVC Prospective 11 Lung scan Actual postoperative values 200 mL higher than PPO values Williams et al [7]
Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PPO, predicted postoperatives; TLC, total
lung capacity.
A.M
.Robles,
D.Shure
/ThoracSurg
Clin
14(2004)295–304
296

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304 297
the measured values. Only the postoperative pre-
dicted VO2max was higher than the predicted value.
CT was the next most accurate technique. The seg-
ment method without regard for obstruction was the
least accurate. For all techniques other than lung
scanning, the actual values were higher than the
predicted values. In another prospective study by
the same investigators [5], actual values for FEV1
and VO2max were the same as postoperative pre-
dicted values at 3 months postoperatively but were
higher than postoperative predicted values at
6 months. The DLCO was higher than postoperative
predicted at both times. In general, most prediction
methods underestimate actual postoperative function
but serve as reasonable guides to risk.
Preoperative predictors of postoperative morbidity
and mortality
Many factors have been examined as predictors of
morbidity and mortality with lung resection, and
there is a great deal of variation among study results
(Table 2). Some investigators have found the pres-
ence of COPD to be predictive of complications [8,9],
whereas others have not [10]. The same discrepancies
hold true for most parameters with the exception of
stair climbing and predicted postoperative DLCO as a
percentage of predicted normal (ppoDLCO%) derived
from lung scanning, which have been found uni-
formly to be predictive of complications [11,12].
These studies vary in their design (retrospective and
prospective), the numbers of patients studied, the
numbers of parameters studied, and the level of
sophistication of the statistical analysis. Despite these
differences, some general patterns have emerged and
are reviewed for pulmonary function tests, exercise
tests, scoring systems, and other risk factors.
Pulmonary function tests
The FEV1 is the best standardized pulmonary
function test available. It forms an important part of
the basis of the definition of COPD and is used
commonly as a measure of the severity of the disease
[13]. The preoperative FEV1 has not been the best
predictor, however, of postoperative morbidity and
mortality, and patients with FEV1 values less than 1 L
(traditionally assumed to prohibit resection) have
survived lung resection without complications [14].
It generally is acknowledged that surgery should not
be withheld on the basis of a low FEV1 alone [13].
Predicted postoperative FEV1 (ppoFEV1) has been
a better indicator of postoperative morbidity and
mortality, but no lowest value has been identified
definitively. Even ppoFEV1 values less than 1 L (but
�700 mL) have been found acceptable. Because
criteria involving absolute values of FEV1 can be
biased against women and people of short stature,
who have lower normal absolute values and lower
values with disease, ppoFEV1% (predicted postoper-
ative FEV1 expressed as a percentage of the predicted
normal value) has been investigated and found to be a
better predictor of morbidity and mortality than
absolute values [15–18]. Still, there is no one value
that has been found to be prohibitive. Although some
studies have identified cutoff values of 40% [19],
others have found acceptable risk at values of 25%
[18]. Other studies have not identified increased risk
with ppoFEV1% less than 33% [14].
The DLCO expressed as a percentage of predicted
and, in particular, the ppoDLCO% have been found to
be the most reliable predictors of postoperative mor-
bidity and mortality. A ppoDLCO% less than 40% of
predicted normal values has been shown to be a good,
and often the only, predictor of morbidity and mor-
tality [11,16,20].
Arterial carbon dioxide retention, as defined by
PaCO2 equal to or greater than 45 mmHg, although a
marker of severe COPD, has not been found to be
independently predictive of increased risk of lung
resection [14,21–23]. Hypoxemia also has not been
found to be a predictor of increased surgical risk,
although conflicting data exist with respect to oxygen
desaturation during exercise [18–20,24].
Exercise tests
Although the ppoFEV1 has been found to be
useful and the ppoDLCO% even more so, many
studies suggest that some form of exercise testing,
particularly for borderline patients, can determine
high risk better. Exercise testing is believed to reflect
cardiac and pulmonary function. Study results have
varied (see Table 2). VO2max derived from expired
gas analysis during exercise has been a good predic-
tor of morbidity and mortality. Most studies have
found unacceptable risk associated with VO2max less
than 10 mL/kg/min [5,25,26]. There seems to be no
risk associated with VO2max equal to or greater than
20 mL/kg/min and an intermediate risk with values
between 10 mL/kg/min and 15 mL/kg/min.
Formal cardiopulmonary exercise testing is not
widely available. A simple and less costly assessment
of endurance is the time-honored practice of stair
climbing. Although results have varied with respect
to the number of steps or number of flights climbed,
increased risk is associated with poorer performance.
The inability to climb two flights of stairs is asso-
ciated with worse postoperative outcomes [12,27].
The inability to perform any exercise carries a poor

Table 2
Preoperative prediction of postoperative morbidity or mortality
Category Predictive of increased morbidity or mortality
Not predictive of increased morbidity
or mortality
Pulmonary
function tests
FEV1 <80% [9]
FEV1 <70% [67]
FEV1 <60% [16]
Low FEV1 [68,69]
PPOFEV1 <700 mL [25]
PPOFEV1 <55% [15]
PPOFEV1 <40% [11,16,19,20]
PPOFEV1 <30% [17]
PPOFEV1 <25% [18]
PPOFVC <55% [15]
DLCO <60% [16,70]
PPODLCO <40% [11,16,20]
Low PPODLCO% [19,71]
PPODLCO% — lack of increase with exercise [72]
PPOFEV1% � PPODLCO% [73]
Low maximal expiratory pressure [42,60]
FEV1 [1,23,24,28,38,41,71,74]
FEV1 <70% [75]
FEV1 <40% [14]
PPOFEV1 <35% [38]
PPOFEV1 <33% [14]
DLCO [1]
PaCO2 �45 mm Hg [14,21–23]
Exercise tests VO2max <15 mL/kg/min [14,16] VO2max [12,38,69,70]
VO2max <10 mL/kg/min [5,25,26] Oxygen desaturation during exercise [18]
VO2max <1.25 L/min [39] 12-min walk [68]
VO2max <60% [74,76]
Stair climb <3 flights [25,38,77]
Stair climb <2 flights [12,27]
6-min walk <1000 ft [12]
Inability to perform exercise [26]
Oxygen desaturation during exercise [19,20,24]
Ventilatory reserve <25 L [39]
Scoring systems ASA score �3 [28] QLI [39]
Poor POSSUM score [23,29] Comorbid indices [18]
Poor EVAD score [31]
CPRI score �4 [26,30]
Comorbid indices �4 [9]
Diseases COPD [8,9] COPD [10]
Interstitial lung disease [32] Interstitial lung disease [33,34]
Cancer [9] Cardiac disease [38]
Other Male gender [36,78,79] Male gender [9,23,41]
Older age [9,67] Older age [9,18,22,36,38]
Age �60 y [80] Weight loss [9]
Age �65 y [41] Poor nutrition [23,41]
Age �75 y [39] Preoperative chemotherapy [9,23]
Age �84 y [10] Preoperative radiation therapy [23]
Poor performance status [40] Corticosteroids [9]
Weight loss [40] Race [41]
Poor nutrition [42] Obesity [10,41]
Smoking, current [39]
Advanced stage [41]
Hemoglobin V10 g/dL [41]
Preoperative chemotherapy [9,45–48]
Preoperative radiation therapy [45,46]
Low institutional surgical volume [49]
Abbreviations: ASA, American Society of Anesthesiology; COPD, chronic obstructive pulmonary disease; CPRI, Cardio-
pulmonary Risk Index; FEV1, forced expiratory volume in 1 second; FVCS, forced vital capacity; PPO, predicted postoperative;
POSSUM, Physiological Operative Severity Score for Enumeration of Morbidity and Mortality; QLI, Quality of Life Index.
A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304298

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304 299
prognosis [26]. Although other forms of exercise
testing have been advocated, such as the 6-minute
walk [12] and oxygen desaturation during exercise
[18,19], stair climbing or, if available, cardiopulmo-
nary exercise testing provides the most studied and
reliable assessment of cardiopulmonary function.
Scoring systems
Many scoring systems have been studied as
predictors of postoperative function (see Table 2).
American Society of Anesthesiology scoring and
Physiological Operative Severity Score for the Enu-
meration of Morbidity and Mortality scoring have
been used in general surgery and have been found to
be predictive in lung resection as well [23,28,29]. A
scoring system of comorbid indices also has been
found to be predictive of overall outcome [9]. A
cardiopulmonary index (Cardiopulmonary Risk In-
dex) and a pulmonary index (EVAD, using pulmo-
nary function data and age) also have been found
to be useful in prospective studies [26,30,31]. Al-
though these scoring systems can be useful, it is not
clear that they add information to that obtained by
exercise testing and ppoDLCO%.
Other risk factors
Many preoperative risk factors, other than those
related to pulmonary function, have been identified.
COPD itself has been found to be a risk factor in
some studies [8,9], but not all studies [10]. Similarly
the presence of interstitial lung disease was found to
increase the risk of resection in one study [32], but
not in others [33,34]. In these latter studies, mortality
and survival were the same as for lung cancer in
general or interstitial lung disease in general. Asthma
is not a risk factor, unless it is in exacerbation, in
which case preoperative treatment and control together
with good postoperative management reduce the
risk. Corticosteroids, a mainstay in the treatment of
asthma exacerbations, have been found to be safe in
the preoperative and perioperative periods [9]. They
do not lead to increase in infections and have no
clinically significant effect on wound healing [35].
Age has been a controversial issue in the past, but
it now seems clear that age is not an independent
predictor of significant risk of surgery [18,22,36–38].
Octagenarians have undergone resection for broncho-
genic carcinoma successfully [39,40].
Men seem to do worse than women with lung
cancer surgery. Men tend to present with more ad-
vanced disease, requiring pneumonectomy rather
than lobectomy, and have worse survival rates than
women [4,15,67]. This finding has not been borne out
in all studies, however [9,23,41]. Advanced stage of
disease is itself a risk factor for worse outcome [41].
Perhaps reflecting advanced disease or more aggres-
sive tumor biology, poor performance status, regard-
less of anatomic staging, is associated with increased
surgical morbidity and mortality [40].
Poor nutritional status also is associated with
increased risks [42]. This observation is important
because patients with COPD are known to have
poorer nutritional status; 25% to 50% of COPD
patients have been found to have impaired nutritional
status [43,44]. Another factor related to COPD is the
risk of current smoking. This risk decreases when
smoking has stopped 2 months or more before
surgery [39].
Preoperative chemotherapy and radiation therapy
have been associated with increased postoperative
morbidity and mortality [9,45–48]. These therapies
seem to inhibit bronchial stump healing by decreasing
bronchial mucosal blood flow [47].These findings
also are important because neoadjuvant therapy may
play a future role in the management of lung cancer
as new, more potent drugs become available. Ways
needs to be found to minimize their adverse effects on
surgical outcomes.
A particularly important risk factor is the lack
of institutional experience. One study found signifi-
cantly lower morbidity and mortality in institutions
with high volumes of lung resection [49].
Pulmonary hypertension has not been well studied
in this setting but has been assumed to be a contra-
indication to resection. Pulmonary hypertension as-
sociated with COPD is a contraindication to lung
volume-reduction surgery (LVRS) [50] and so can be
inferred to be a contraindication to resection for lung
cancer. What has not been well established is the
degree of pulmonary hypertension and whether or not
pulmonary hypertension is present only with exercise.
Preoperative optimization of function and
reduction of risk
With the understanding of the above-outlined
preoperative risk factors, measures can be taken to
reduce surgical risks. Focusing on COPD, several
areas can be optimized. Bronchitic infections, mani-
fested by increased cough and sputum production,
can be treated with a course of antibiotics with
improvement in postoperative outcomes [51,52].
Bronchospastic exacerbations of COPD or asthma
can be treated with bronchodilators and corticoste-
roids preoperatively, perioperatively, and postopera-

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304300
tively. Exacerbations should be controlled before
surgery, but treatment should continue during and
after surgery to decrease risks [51]. As mentioned
previously, corticosteroids do not increase the risk of
postoperative infection and may decrease morbidity
by decreasing inflammatory cytokine production
postoperatively [53].
Smoking is common in patients with lung cancer
and patients with COPD. Cessation has been shown
to decrease postoperative complications in coronary
artery bypass patients [54] and can be assumed to do
so in patients undergoing lung resection. This effect
can be inferred from the finding of increased post-
operative morbidity in current smokers, but not in
patients who have stopped smoking 2 months or more
before surgery [39]. Although it may not be practical
to defer surgery for 2 months, smoking cessation still
should be encouraged to decrease smoking-related
lung inflammation, which may have deleterious
effects in the postoperative period [55].
Although it commonly is believed that lung
function cannot be improved other than with bron-
chodilators if a reversible component is present,
inspiratory muscle training has been documented to
improve function and cause subjective improvement
in dyspnea [56,57]. One study of incentive spirome-
try and inspiratory muscle training initiated 2 weeks
preoperatively and continued for 3 months postopera-
tively found significant increases in postoperative
FEV1 over ppoFEV1 [58] compared with untrained
controls. The actual measured FEV1 was 570 mL
larger than the ppoFEV1 for lobectomies and 680 mL
for pneumonectomies. These numbers compare with
70 mL for lobectomies and 110 mL for pneumonec-
tomies in the controls. Actual lung function can be
improved. Pulmonary rehabilitation also may have
a role because it is known to improve function,
dyspnea scores, and quality of life [59]. It also is a
prerequisite for LVRS in the National Emphysema
Treatment Trial [50]. A full pulmonary rehabilitation
program may not be practical, however, in terms of
the imperative of surgery. Inspiratory muscle training
should be possible, however, in most cases.
Nutrition is another area worthy of attention.
Because poor nutrition is associated with worse sur-
gical outcomes [42,60], improvement in nutritional
status preoperatively may be helpful. This effect has
not been studied for lung resection, however.
As noted earlier, the volume of surgery performed
at an institution has been found in a large retrospec-
tive study (2116 operations) to be related to outcome
[49]. In this study, 5-year survival was highest at the
centers with the highest volume, 44% versus 33% at
the centers with lower volume. Differences also were
found in the incidence of postoperative complications
(20% versus 44%) and the 30-day mortality (3%
versus 6%). Choosing the most experienced center
may improve outcome.
Patient selection can be optimized in many in-
stances. Patients with no history of COPD and no
pulmonary symptoms are unlikely to be at signifi-
cantly increased risk. Pulmonary function tests are
recommended for patients undergoing resection [13].
If the FEV1 is equal to or greater than 60% of
predicted and the patient is asymptomatic, no further
evaluation is needed because the patient falls into a
low-risk category. If the FEV1 or the DLCO are less
than 60% or if the patient has pulmonary symptoms,
such as dyspnea (regardless of the FEV1), further
functional evaluation is needed to assess risk. Lung
scanning or CT is indicated to determine ppoFEV1%
and ppoDLCO. If these values are borderline or low
(<40%), some form of exercise testing is indicated
[61]. This testing can be the simple stair climb or the
more sophisticated VO2max. An inability to climb
two flights of stairs or a VO2max less than 10 mL/kg/
min or less than 40% of predicted indicates a high-
risk patient. Although high-risk patients have been
operated on successfully [14], the markedly increased
level of risk dictates that great caution be exercised in
recommending surgery in these individuals. Perhaps
the only exceptions to the VO2max level of less than
10 mL/kg/min would be the rare patient with the
simultaneous ability to stair climb or an adequate
ppoDLCO% (>40%). In these cases, the VO2max
expressed as a percentage of predicted is likely to
be a better indication of risk.
Possible exceptions to these guidelines have been
seen in patients who underwent LVRS and were
found incidentally to have lung cancers in the
resected tissue. Many of these patients experienced
improvement in function postoperatively as a result
of the LVRS despite having poor preoperative func-
tion [62]. The mean preoperative FEV1 was 654 mL
(21.7% predicted), and the mean postoperative FEV1
was 1097 mL (49% predicted). A subsequent study
examined patients with lung cancer who were candi-
dates for LVRS [63]. Patients with ppoFEV1 less than
40% had no change in FEV1 postoperatively, whereas
patients with ppoFEV1 greater than 40% experienced
a reduction postoperatively. The in-hospital mortality
was high in the group with worse preoperative
function, 14% versus 0% for the group with better
preoperative function, but the long-term survival rates
of the groups were the same. The finding of no
decrement in lung function in the group with the
lowest FEV1 is consistent with other studies that
have found a smaller proportional decrement in

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304 301
lung function in patients with the lowest preoperative
FEV1 [64].
Future research
Although much information has become available
with respect to COPD, comparable information is
needed for the effects of resection on patients with
interstitial lung disease. The need for prediction of
postoperative lung function and the accuracy of these
predictions in the presence of interstitial lung disease
are not known. The presence of significant pul-
monary hypertension can be assumed to present a
risk similar to that in COPD, but in both cases a
tolerable level (if any) of pulmonary hypertension is
not known.
The optimal timing and duration of inspiratory
muscle training are not known and may be a profit-
able area of research. The risks of delaying surgery to
achieve optimal training by specific muscle training
or pulmonary rehabilitation in patients with lung
cancer also are not known and perhaps would be
difficult to study directly. Similarly the risks of
delaying surgery to achieve adequate nutritional sta-
tus are not known.
Summary
Many risk factors for morbidity and mortality with
lung resection have been identified. Factors such as
age, gender, and cancer stage cannot be altered, but
lung function can be optimized by treating COPD or
asthma with bronchodilators, corticosteroids, or anti-
biotics (when indicated) and by inspiratory muscle
training. Although smoking cessation 2 months in
advance of surgery may not be feasible, cessation
nevertheless should be encouraged because it may
decrease postoperative inflammation and in the long-
term may decrease the risk of recurrence. In addition,
morbidity and mortality can be minimized by careful
patient selection using lung scanning or CT to deter-
mine predicted postoperative functions (FEV1% and
DLCO%) and some form of exercise testing, such
as cardiopulmonary exercise testing or simple stair
climbing. When the risk of surgery is high, any
benefit from possible cure must be weighed against
the risk of long-term disability or death. Although
much data are available to guide clinicians in these
decisions, there still is no one test that provides the
answer in individual cases. The art and science of
medicine must merge at this point.
References
[1] Nugent AM, Steele IC, Carragher AM, et al. Effect of
thoracotomy and lung resection on exercise capacity
in patients with lung cancer. Thorax 1999;54:334–8.
[2] Schuurmans MM, Diacon AH, Bolliger CT. Functional
evaluation before lung resection. Clin Chest Med 2002;
23:159–72.
[3] Tisi GM. Preoperative identification and evaluation of
the patient with lung disease. Med Clin North Am
1987;71:399–412.
[4] Bolliger CT, Jordan P, Soler M, et al. Pulmonary func-
tion and exercise capacity after lung resection. Eur
Respir J 1996;9:415–21.
[5] Bolliger CT, Wyser C, Roser H, Soler M, Perruchoud
AP. Lung scanning and exercise testing for the predic-
tion of postoperative performance in lung resection
candidates at increased risk for complications. Chest
1995;108:341–8.
[6] Bolliger CT, Guckel C, Engel H, et al. Prediction of
functional reserves after lung resection: comparison by
computed tomography, scintigraphy, and anatomy.
Respiration (Herrlisheim) 2002;69:482–9.
[7] Williams AJ, Cayton RM, Harding LK, Mostafa AB,
Matthews HR. Quantitative lung scintigrams and lung
function in the selection of patients for pneumonectomy.
Br J Dis Chest 1984;78:105–12.
[8] Sekine Y, Behnia M, Fujisawa T. Impact of COPD on
pulmonary complications and on long-term survival of
patients undergoing surgery for NSCLC. Lung Cancer
2002;37:95–101.
[9] Bernard A, Ferrand L, Hagry O, Benoit L, Cheyne IN,
Favre JP. Identification of prognostic factors determin-
ing risk groups for lung resection. Ann Thorac Surg
2000;70:1161–7.
[10] Naunheim KS, Kesler KA, D’Orazio SA, Fiore AC,
Judd DR. Lung cancer surgery in the octogenarian. Eur
J Cardiothorac Surg 1994;8:453–6.
[11] Beckles MA, Spiro SG, Colice GL, Rudd RM. The
physiologic evaluation of patients with lung cancer
being considered for resectional surgery. Chest 2003;
123(1 Suppl):105S–14S.
[12] Holden DA, Rice TW, Stelmach K, Meeker DP. Exer-
cise testing, 6-min walk, and stair climb in the evalua-
tion of patients at high risk for pulmonary resection.
Chest 1992;102:1774–9.
[13] Celli BR, Snider GL, Heffner J, et al. Standards for
the diagnosis and care of patients with chronic obstruc-
tive pulmonary disease. Am J Respir Crit Care Med
1995;152(5 Pt 2):S77–120.
[14] Morice RC, Peters EJ, Ryan MB, Putnam JB, Ali MK,
Roth JA. Exercise testing in the evaluation of patients
at high risk for complications from lung resection.
Chest 1992;101:356–61.
[15] Haraguchi S, Koizumi K, Hatori N, et al. Prediction
of the postoperative pulmonary function and compli-
cation rate in elderly patients. Surg Today 2001;31:
860–5.
[16] Datta D, Lahiri B. Preoperative evaluation of patients

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304302
undergoing lung resection surgery. Chest 2003;123:
2096–103.
[17] Nakahara K, Ohno K, Hashimoto J, et al. Prediction
of postoperative respiratory failure in patients under-
going lung resection for lung cancer. Ann Thorac Surg
1988;46:549–52.
[18] Varela G, Cordovilla R, Jimenez MF, Novoa N. Utility
of standardized exercise oxymetry to predict cardiopul-
monary morbidity after lung resection. Eur J Cardio-
thorac Surg 2001;19:351–4.
[19] Markios J, Mullan BP, Hillman DR, et al. Preoperative
assessment as a predictor of mortality and morbidity
after lung resection. Am Rev Respir Dis 1989;139:
902–10.
[20] Ribas J, Diaz O, Barbera JA, et al. Invasive exercise
testing in the evaluation of patients at high-risk for
lung resection. Eur Respir J 1998;12:1429–35.
[21] Kearney DJ, Lee TH, Reilly JJ, DeCamp MM, Sugar-
baker DJ. Assessment of perioperative risk in patients
undergoing lung resection: importance of predicted
pulmonary function. Chest 1994;105:753–9.
[22] Reilly Jr JJ. Evidence-based preoperative evaluation of
candidates for thoracotomy. Chest 1999;116:474S–6S.
[23] Brunelli A, Fianchini A, Gesuita R, Carle F. Physio-
logical and operative severity score for the enumera-
tion of mortality and morbidity. Ann Thorac Surg
1999;67:329–31.
[24] Rao V, Todd TR, Kuus A, Buth KJ, Pearson FG. Ex-
ercise oximetry versus spirometry in the assessment of
risk prior to lung resection. Ann Thorac Surg 1995;
60:603–8.
[25] Pate P, Tenholder MF, Griffin JP, Eastridge CE, Wei-
man DS. Preoperative assesment of the high-risk pa-
tient for lung resection. Ann Thorac Surg 1996;61:
1494–500.
[26] Epstein SK, Faling LJ, Daly BD, Celli BR. Inability to
perform bicycle ergometry predicts increased morbid-
ity and mortality after lung resection. Chest 1995;107:
311–6.
[27] Girish M, Trayner E, Dammann O, Pinto-Plata V, Celli
B. Symptom-limited stair climbing as a predictor of
post-operative cardiopulmonary complications after
high-risk surgery. Chest 2001;120:1147–51.
[28] Stephan F, Boucheseiche S, Hollande J, et al. Pulmo-
nary complications following lung resection: a compre-
hensive analysis of incidence and possible risk factors.
Chest 2000;118:1263–70.
[29] Brunelli A, Fianchini A, Xiume F, Gesuita R, Mattei
A, Carle F. Evaluation of the POSSUM scoring system
in lung surgery. Thorac Cardiovasc Surg 1998;46:
141–6.
[30] Epstein SK, Faling LJ, Daly BD, Celli BR. Predicting
complications after pulmonary resection: preoperative
exercise testing vs a multifactorial cardiopulmonary
risk index. Chest 1993;104:694–700.
[31] Ferguson MK, Durkin AE. A comparison of three
scoring systems for predicting complications after ma-
jor lung resection. Eur J Cardiothorac Surg 2003;23:
35–42.
[32] Chiyo M, Sekine EI. Impact of interstitial lung dis-
ease on surgical morbidity and mortality for lung
cancer: analyses of short-term and long-term out-
comes. 2004.
[33] Marinod E, Azorin JF, Sadoun D, et al. Surgical re-
section of lung cancer in patients with underlying in-
terstitial lung disease. Ann Thorac Surg 2002;74:
1004–7.
[34] Aubry MC, Myers JL, Douglas WW, et al. Primary
pulmonary carcinoma in patients with idiopathic pul-
monary fibrosis. Mayo Clin Proc 2002;77:763–70.
[35] Gracey DR, Divertie MM, Didier EP. Preoperative
preparation of patients with chronic obstructive pul-
monary disease: a prospective study. Chest 1979;76:
123–9.
[36] Pagni S, McKelvey A, Riordan C, Federico JA, Ponn
RB. Pulmonary resection for malignancy in the elder-
ly: is age still a risk factor? Eur J Cardiothorac Surg
1998;14:40–4.
[37] Filaire M, Mom T, Laurent S, et al. Vocal cord dys-
function after left lung resection for cancer. Eur J Car-
diothorac Surg 2001;20:705–11.
[38] Brunelli A, Al Refai M, Monteverde M, Borri A, Salati
M, Fianchini A. Stair climbing test predicts cardio-
pulmonary complications after lung resection. Chest
2002;121:1106–10.
[39] Dales RE, Dionne G, Leech JA, Lunau M, Schweitzer
I. Preoperative prediciton of pulmonary complications
following thoracic surgery. Chest 1993;104:155–9.
[40] Pater JL, Loeb M. Nonanatomic prognostic factors in
carcinoma of th elung: a multivariate analysis. Cancer
2004;50:326–31.
[41] Jazieh AR, Hussain M, Howington JA, et al. Prognos-
tic factors in patients with surgically resected stages I
and II non-small cell lung cancer. Ann Thorac Surg
2000;70:1168–71.
[42] Jagoe RT, Goodship TH, Gibson GJ. The influence of
nutritional status on complications after operations for
lung cancer. Ann Thorac Surg 2001;71:936–43.
[43] Braun SR, Keim NL, Dixon RM, Clagnaz P, Anderegg
A, Shrago ES. The prevalence and determinants of
nutritional changes in chronic obstructive pulmonary
disease. Chest 1984;86:558–63.
[44] Hunter ABM, Carey MA, Larsh HW. The nutritional
status of patients with chronic obstructive pulmonary
disease. Am Rev Respir Dis 1981;124:376–81.
[45] Regnard JF, Icard P, Deneuville M, et al. Lung resec-
tion after high doses of mediastinal radiotherapy (sixty
grays or more): reinforcement of bronchial healing
with thoracic muscle flaps in nine cases. J Thorac Car-
diovasc Surg 1994;107:607–10.
[46] Torre W, Sierra A. Postoperative complications of lung
resection after induction chemotherapy using Paclitaxel
(and radiotherapy) for advanced non-small lung cancer.
J Cardiovasc Surg 2002;43:539–44.
[47] Yamamoto R, Tada H, Kishi A, Tojo T. Effects of
preoperative chemotherapy and radiation therapy on
human bronchial blood flow. J Thorac Cardiovasc
Surg 2000;119:939–45.
A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304 303
[48] Roberts JR, Eustis C, Devore R, Carbone D, Choy H,
Johnson D. Induction chemotherapy increases perio-
perative complications in patients undergoing resec-
tion for non-small cell lung cancer. Ann Thorac Surg
2001;72:885–8.
[49] Bach PB, Cramer LD, Schrag D, Downey RJ, Gelfand
SE, Begg CB. The influence of hospital volume on
survival after resection for lung cancer. N Engl J Med
2001;345:181–8.
[50] The National Emphysema Treatment Trial Research
Group. Rationale and design of the National Emphy-
sema Treatment Trial: a prospective randomized trial
of lung volume reduction surgery. Chest 1999;116:
1750–61.
[51] Garibaldi RA, Britt MR, Coleman ML, Reading JC,
Pace NL. Risk factors for postoperative pneumonia.
Am J Med 1981;70:677–80.
[52] Celli B. Perioperative respiratory care of the patient
undergoing upper abdominal surgery. Clin Chest
Med 1993;14:253–61.
[53] Mitsuta K, Shimoda T, Fukishiima C, Obases Y, Ayabe
H, Matsuse H. Preoperative steroid therapy inhibits
cytokine production in the lung parenchyma in asth-
matics. Chest 2001;120:1175–83.
[54] Warner MA, Divertie MB, Tinker JH. Preoperative
cessation of smoking and pulmonary complications
in coronary artery bypass patients. Anesthesiology
1984;60:380–3.
[55] Retamales I, Elliott WM, Meshi B, et al. Amplification
of inflammation in emphysema and its association with
latent adenoviral infection. Am J Respir Crit Care
Med 2001;164:469–73.
[56] Harver A, Mahler DA, Daubenspeck JA. Targeted in-
spiratory muscle training improves respiratory muscle
function and reduces dyspnea in patients with chronic
obstructive pulmonary disease. Ann Intern Med 1989;
111:117–24.
[57] Dekhuizen PNR, Folgering HTM, van Herwaarden
CLA. Target flow inspiration muscle training during
pulmonary rehabilitation in patients with COPD. Chest
1991;99:128–33.
[58] Weiner P, Man A, Weiner M, et al. The effect of in-
centive spirometry and inspiratory muscle training on
pulmonary function after lung resection. J Thorac Car-
diovasc Surg 1997;113:552–7.
[59] Casaburi R. Exercise training in chronic obstructive
lung disease. In: Casaburi R, Petty TL, editors. Princi-
ples and practice of pulmonary rehabilitation. Philadel-
phia: Saunders; 1993. p. 204–24.
[60] Nwiloh J, Freeman H, McCord C. Malnutrition: an
important determinant of fatal outcome in surgically
treated pulmonary suppurative disease. J Thorac Car-
diovasc Surg 1989;81:525–9.
[61] Weisman IM. Cardiopulmonary exercise testing in the
preoperative assessment for lung resection surgery.
Semin Thorac Cardiovasc Surg 2001;13:116–25.
[62] McKenna RJ, Fischel RJ, Brenner M, Gelb AF. Com-
bined operations for lung volume reduction surgery
and lung cancer. Chest 1996;110:885–8.
[63] Edwards DG, Waller DA. Lobar volume reduction sur-
gery: a method of increasing the lung cancer resection
rate in patients with emphysema. Thorax 2001;56:
791–5.
[64] Larsen KR, Svendsen UG, Milman N, Brenoe J,
Petersen BN. Cardiopulmonary function at rest and
during exercise after resection for bronchial carcinoma.
Ann Thorac Surg 1997;64:960–4.
[65] Foroulis CN, Kotoulas C, Konstantinou M, Lioulias A.
Is the reduction of forced expiratory lung volumes pro-
portional to the lung parenchyma resection, 6 months
after pneumonectomy? Eur J Cardiothorac Surg 2002;
21:901–5.
[66] Zeiher BG, Gross TJ, Kern JA, Lanza LA, Peterson
MW. Predicting postoperative pulmonary function in
patients undergoing lung resection. Chest 1995;108:
68–72.
[67] Ploeg AJ, Kappetein AP, van Tongeren RB, Pahlplatz
PV, Kastelein GW, Breslau PJ. Factors associated
with perioperative complications and long-term
results after pulmonary resection for primary carci-
noma of the lung. Eur J Cardiothorac Surg 2003;
23:26–9.
[68] Bagg LR. The 12-min walking distance; its use in the
pre-operative assessment of patients with bronchial car-
cinoma before lung resection. Respiration (Herrlisheim)
1984;46:342–5.
[69] Colman NC, Schraufnagel DE, Rivington RN, Pardy
RL. Exercise testing in evaluation of patients for lung
resection. Am Rev Respir Dis 1982;125:604–6.
[70] Wang J, Olak J, Ultmann RE, Ferguson MK. Assess-
ment of pulmonary complications after lung resection.
Ann Thorac Surg 1999;67:1444–7.
[71] Ferguson MK, Reeder LB, Mick R. Optimizing selec-
tion of patients for major lung resection. J Thorac Car-
diovasc Surg 1995;109:275–83.
[72] Wang JS, Abboud RT, Evans KG, Finley RJ, Graham
BL. Role of CO diffusing capacity during exercise in
the preoperative evaluation for lung resection. Am J
Respir Crit Care Med 2000;162(4 Pt 1):1435–44.
[73] Pierce RJ, Copland JM, Sharpe K, Barter CE. Preop-
erative risk evaluation for lung cancer resection:
predicted postoperative product as a predictor of sur-
gical mortality. Am J Respir Crit Care Med 1994;150:
947–55.
[74] Brutsche MH, Spiliopoulos A, Bolliger CT, Licker M,
Frey JG, Tschopp JM. Exercise capacity and the extent
of resection as predictors of surgical risk in lung can-
cer. Eur Respir J 2000;15:828–32.
[75] Brunelli A, Al Refai M, Monteverde M, Sabbatini A,
Xiume F, Fianchini A. Predictors of early morbidity
after major lung resection in patients with and with-
out airflow limitation. Ann Thorac Surg 2002;74:
999–1003.
[76] Bolliger CT, Jordan P, Soler M, et al. Exercise capacity
as a predictor of postoperative complications in lung
resection candidates. Am J Respir Crit Care Med 1995;
151:1472–80.
[77] Olsen GN, Bolton JW, Weiman DS, Hornung CA.

A.M. Robles, D. Shure / Thorac Surg Clin 14 (2004) 295–304304
Stair climbing as an exercise test to predict the post-
operative complications of lung resection. Chest 1991;
99:587–90.
[78] Alexiou C, Onyeaka CV, Beggs D, et al. Do women
live longer following lung resection for carcinoma?
Eur J Cardiothorac Surg 2002;21:319–25.
[79] Whittle J, Steinberg EP, Anderson GF, Herbert R. Use
of Medicare claims data to evaluate outcomes in el-
derly patients undergoing lung resection for lung can-
cer. Chest 1991;100:729–34.
[80] de Perrot M, Licker M, Reymond MA, Robert J, Spi-
liopoulos A. Influence of age on operative mortality
and long-term survival after lung resection for bron-
chogenic carcinoma. Eur Respir J 1999;14:419–22.

Thorac Surg Clin 14 (2004) 305–315
Methodology for quality-of-life assessment:
a critical appraisal
Benny Chung-Ying Zee, PhDa,b,*, Tony S.K. Mok, MD, FRCPCc
aCentre for Clinical Trials, School of Public Health, Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, NT,
Hong Kong SAR, ChinabComprehensive Cancer Trials Unit, Department of Clinical Oncology, Chinese University of Hong Kong,
Prince of Wales Hospital, Shatin, NT, Hong Kong SAR, ChinacDepartment of Clinical Oncology, Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, NT,
Hong Kong SAR, China
Technologic advancements in surgery and medi- as pain, dyspnea, and fatigue, which can be clearly
cine have transformed diseases such as cancer from a
usually fatal disease to a curable illness for some
patients and a chronic condition for many more. This
change has resulted in an increasing appreciation
about the health-related quality of life (HRQOL) of
patients diagnosed with cancer and the quality of care
they receive. Knowledge of HRQOL provides helpful
information to primary care providers, specialists,
other health care providers, patients, and families to
understand and explore further their role in symptom
management and appropriate means for providing
special care for patients throughout the course of
cancer. Partly due to the realization of this need, the
academic research on quality of life (QOL) has been
active since the 1980s and 1990s. HRQOL is widely
considered as multidimensional constructs describing
how illness and treatment affect patients’ ability to
function and the potential burden of symptoms from
treatment [1–3]. HRQOL has become an important
end point in cancer clinical trials, and it has presented
many methodologic issues that have been areas of
active research. This article discusses several meth-
odologic issues in the research for HRQOL.
One issue in HRQOL research is the definition
and the associated clinical meaning associated with
the QOL domains [4,5]. In contrast to symptoms such
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00028-3
* Corresponding author.
E-mail address: [email protected]
(B.C.-Y. Zee).
defined, HRQOL sometimes refers to abstract con-
structs, such as social functioning. Instead of a mea-
surement of depression, HRQOL assesses emotional
functioning that may incorporate a much wider scope
of emotional distress due to the disease and treatment.
Within the clinical trial context, various methods
of symptom assessment have been studied exten-
sively with a long history of methodologic develop-
ment that has been accepted by regulatory agencies in
the drug approval process to deal with specific
symptoms. Some successful examples and future
directions of development for other HRQOL con-
structs are discussed.
Because HRQOL data usually are obtained through
patient self-administered questionnaires, missing val-
ues are common [6]. The way the data are processed
may make a difference in the analysis and may affect
the study conclusion. To deal with missing data, most
statistical software uses case-deletion method by
deleting cases with missing data, then applies stan-
dard complete-data methods for the analysis. A
disadvantage is that case-deletion method reduces
the sample size and produces less efficient and
possibly biased estimates leading to erroneous con-
clusions. This article discusses many commonly used
approaches in summarizing the QOL scores with
missing data.
Finally, the HRQOL outcome may have been
defined clearly with an optimal methodology of
dealing with missing data; however, the way the data
are analyzed may affect the conclusion. The difficulty
s reserved.

1
0.8
0.6
0.4
0.2
0
–0.2
–0.4
–0.6Phys Role Emot Cogn Glob
QOLNaus Appe
–0.32
–0.01–0.06
–0.27 –0.3
0.78
0.38
Fig. 1. Spearman correlations between average diary nausea
score and selected European Organization for Research and
Treatment of Cancer (EORTC) Core Quality of Life
Questionnaire (QLQ-C30) domains and symptoms. Phys,
physical functioning; Role, role functioning; Emot, emo-
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315306
encountered in the analysis is due to the longitudinal
nature of the HRQOL data coupled with practical
issues, such as appointment scheduling. The analysis
methods of using growth curve modeling are dis-
cussed and compared with the results of the analysis
of using a HRQOL response variable to summarize
longitudinal HRQOL data [7,8].
Throughout this article, a cancer-specific question-
naire, the European Organization for Research and
Treatment of Cancer (EORTC) Core Quality of Life
Questionnaire (QLQ-C30) is used for illustration
purposes [9]. This is a patient self-administered ques-
tionnaire with 30 items. It has been psychometrically
validated and used in many studies. Embedded in the
questionnaire are dimensions assessing physical func-
tioning, role functioning, emotional functioning, cog-
nitive functioning, social functioning, and overall or
global QOL. In addition, there are three symptom
domains, including fatigue, nausea and vomiting and
pain, and six single items on dyspnea, insomnia, ap-
petite loss, constipation, diarrhea, and financial diffi-
culties. The whole QLQ-C30 questionnaire normally
takes about 10 to 15 minutes to complete.
tional functioning; Cogn, cognitive functioning; Glob QOL,global quality of life; Naus, nausea and vomiting; Appe,
appetite loss.
Symptom assessment and health-related quality
of life
Clinical trials on symptom control have been
successful in the past. One example is in the area of
antiemetic drug development. Pharmaceutical com-
panies and academic institutions have done many
well-designed studies assessing the antiemetic effect
of treatments such as ondansetron and dexametha-
sone [10–13]. One reason for these successes is that
nausea and vomiting, although considered as a sub-
jective response, can be understood easily from a
clinical point of view, which facilitates the regulatory
approval process. In a study assessing chemotherapy-
induced nausea and vomiting [14], 5-day average
nausea scores captured by patient diary on a 100-mm
visual analogue scale was significantly correlated with
QLQ-C30 nausea and vomiting domain (P < .01),
appetite loss (P < .05), physical functioning (P < .05),
and global QOL (P < .05) (Fig. 1). An important
observation of this result is that the high correlation
between 5-day average of nausea scores from patient
diary and the one-time assessment of the HRQOL at
the end of day 5 implies that the assessment of nausea
and vomiting can be done at one point of time,
although it was believed that the daily assessment
of nausea and vomiting is more accurate, and daily
diary assessment has been a preferred end point in
antiemetic studies. Kaizer et al [11] captured daily
measurements of nausea and vomiting for 5 days and
a one-time measurement of HRQOL at day 8 after
starting chemotherapy; there was a significant differ-
ence between the maintenance ondansetron arm and
the no maintenance ondansetron arm with respect to
complete response (59.6% versus 42.1%; P = .012,
one-sided test). The 5-day average of severity of nau-
sea also was significant in favor of the ondansetron
maintenance arm, with a mean of 9.4 mm differ-
ence (P = .002). Similarly the comparison between
EORTC QLQ-C30 nausea and vomiting domain was
significant in favor of the maintenance ondansetron
arm (17.8 versus 29.2; P < .001). The benefit of
nausea and vomiting assessment for the maintenance
arm was not strong enough, however, to translate into
a global QOL benefit (53.9 versus 49.4; P = .217).
The above-mentioned observations have been
noted repeatedly in other studies. In a phase II,
prospective randomized study, patients with stage
IIIb/IV, histologically confirmed non–small cell lung
carcinoma with an age range of 18 to 75 and with
bidimensionally measurable disease were randomized
to receive either gemcitabine, 1 g/m2, on days 1, 8,
and 15 and cisplatin, 75 mg/m2, on day 15 (GP)
versus gemcitabine, 1 g/m2, on days 1, 8, and 15 and
oral etoposide, 50 mg, on days 1 to 14 (GE) [15].

B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315 307
Patient HRQOL was assessed using EORTC QLQ-
C30 at baseline and the beginning of each cycle.
After the first cycle of treatment, nausea and vomiting
(5.1 for GE versus 16.7 for GP; P = .004) was
significantly worse in the GP arm, and alopecia
(52.5 for GE versus 11.5 for GP; P < .001) was
significantly worse in the GE arm. Nausea and
vomiting as assessed by the common toxicity criteria
was not significantly different (38% versus 39%
grade 2 or greater; P = .93). These results showed
that symptoms measured by a patient self-adminis-
tered tool such as QLQ-C30 are more sensitive than
common toxicity criteria. The QOL questionnaire can
be used as a valid clinical trial end point; the amount
of information required to show improvement is
dramatically reduced compared with a patient diary.
Other symptoms of interest in these patients are
cough, hemoptysis, sore mouth, and pain. Interven-
tion that could alleviate these symptoms may have a
greater impact on global QOL.
Summarizing health-related quality-of-life scores
with missing data
The ease of interpretation for the symptom
domains within a HRQOL questionnaire and the
evidence that a less frequent measurement schedule
may be sufficient do not come without a price. The
most obvious problem of using a patient self-admin-
istered questionnaire is missing data. The types of
missing data in HRQOL studies include data missing
due to patients inadvertently missing the item or
choosing not to answer the item for a specific reason.
Another type of nonresponse may be due to the fact
that patients with poor QOL may have a higher
likelihood of missing items or may be incapable of
answering the whole questionnaire. In a study on
palliative therapy for patients with poor-prognosis
small cell lung cancer, the proportion of patients
completing the QOL assessments decreased from
92% to 31% in patients whom physicians rated as
normal compared with patients who were confined to
bed or a chair [16]. The consequence of this type of
missing data is that serious bias may be generated. To
choose an optimal method of handling missing data
in a HRQOL study, the authors formally evaluated
many different imputation approaches through a
simulation method.
Methods of imputation
Six methods were examined in this study: (1) case
deletion, (2) subscale mean, (3) subscale mean 50%,
(4) item mean, (5) single imputation, and (6) matched
item mean. The most primitive method of handling
missing data is the case-deletion method. In this
method, a complete data set is generated by deleting
all subjects with incomplete items. The subscale-
mean method can be applied to instruments with
domains or subscales that have multiple items. The
imputed value of a missing item is the average of all
the completed items in that subscale for a particular
subject. The major characteristic of this method is
that it does not depend on the availability of data
from other subjects. The subscale-mean 50% method
is similar to the previous subscale-mean method
except that it requires at least 50% of the items within
the imputing domain to be answered before an
average value can be computed and used as the
imputed value. The items-mean method imputes the
missing items of a subject by an average of the items
of the subjects who answered that particular item.
This method does not depend on the availability of
data in each domain or subscale, but rather it depends
on the availability of data from other subjects and is
suitable only for large studies. The next two methods
use sets of similar subjects to model the missing
data. The criteria for defining the set of similar sub-
jects are discussed subsequently. The single-imputa-
tion method imputes a randomly selected value
from the corresponding item in the set of similar
subjects for the missing item. The matched items-
mean method also uses the set of similar subjects, but
similar to the imputed items-mean method. Instead
of imputing a value randomly selected from the
corresponding items, as in single imputation, the
missing items are imputed by the mean of the cor-
responding items.
For single-imputation and matched items-mean
methods, the selection criteria include a series of
comparisons between pairs of subjects. The sum of
the absolute differences between all nonmissing
items, within each domain, is calculated, as follows:
0 V dijk ¼XNk
l¼1
j Iikl � Ijkl jnikðak � bkÞ
V1;
k ¼ 1; . . . ; 15; I ¼ 1; . . . ; n; j ¼ 1; . . . ; n; and iaj
where Iikl and Ijkl are the lth item values of the kth
domain for the ith and jth individuals, nik is the
number of nonmissing items in the kth domain for
the ith individual, and the values ak and bk are the
maximum and minimum of the item value for the kth
domain. Nk is the total number of items in the kth
domain, and n is the total number of subjects in the
study. After the standardized distances (dijk) for each

Table 1
Average deviations for random missing data (N = 177)
10% data missing 20% data missing 30% data missing
Imputation method SSD PMD SSD PMD SSD PMD
Case deletion Nil .0107 Nil .0176 Nil .0701
Subscale mean .0401 .0004b .0567b .0004a .0855b .0061b
Subscale mean 50% .0348a .0001a .0559a .0014b .0705a .0071
Item mean .0610 .0046 .1151 .0024 .1597 .0007a
Single imputation .0377b .0039 .0871 .0092 .1004 .0343
Matched item mean .0703 .0025 .1195 .0113 .1474 .0354
Abbreviations: PMD, population mean deviation; SSD, sum of squared deviation.a Refers to the smallest p-value among the imputation methods.b Refers to the second smallest p-value among the imputation methods.
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315308
of the domains are calculated, an average is taken,
as follows:
0V Dij ¼X15k¼1
dijk
!=15
" #V1;
i ¼ 1; . . . ; n; j ¼ 1; . . . ; n; and iaj
where Dij is the average standardized distance (ASD).
Based on ASD, a probability (prob = 1 � ASD) was
assigned to the compared subject, and this probability
represents the chance the subject will be included
in the set of similar subjects. Subjects with a small
ASD value have a high probability, which represents
a higher likelihood of being included in the set of
similar subjects.
Simulation study
A data set was used to evaluate the performance of
the imputation methods. The data set was obtained
Table 2
Average deviations for random missing data (N = 452)
10% data missing 20
Imputation method SSD PMD SS
Case deletion Nil .0114 N
Subscale mean .0372 .0001a .0
Subscale mean 50% .0368b .0005b .0
Item mean .0411 .0021 .1
Single imputation .0282a .0009 .0
Matched item mean .0806 .0008 .1
Abbreviations: PMD, population mean deviation; SSD, sum of sqa Refers to the smallest p-value among the imputation methodb Refers to the second smallest p-value among the imputation
from samples of two symptom control studies (SC.8
and SC.9) of the National Cancer Institute of Canada
Clinical Trials Group [11,17]. In this data set, a total of
820 subjects were obtained, and 673 had complete
QOL data. A sample of 177 patients and a larger set of
452 patients were chosen from the complete QOL data
set for performing the evaluation. Among the patients
with complete QOL data, a comparison of the day
8 QOL data between two treatment arms was used.
To evaluate the performance of various imputation
methods, missing data were generated from the
complete data set using random and nonrandom
processes. In a workshop on ‘‘Missing Data in
Quality of Life Research in Cancer Clinical Trials,’’
most cooperative groups reported that the baseline
compliance rates were greater than 90% [18]. The
compliance rate while patients were receiving treat-
ment was about 80% and after patients completed
treatment was in the 70% range. Based on these
generally acceptable ranges of missing data during
different phases, the proportion of missing items
% data missing 30% data missing
D PMD SSD PMD
il .0192 Nil .0255
675b .0046b .1144b .0023
648a .0058 .1027a .0014b
052 .0020a .1562 .0010a
748 .0070 .1148 .0121
469 .0053 .1816 .0090
uared deviation.
s.
methods.

Table 3
Average deviations for nonrandom missing data (N = 177)
10% data missing 20% data missing 30% data missing
Imputation method SSD PMD SSD PMD SSD PMD
Case deletion Nil .0136 Nil .0235 Nil .0282a
Subscale mean .0120 .0015b .0375 .0012b .0579b .0035b
Subscale mean 50% .0116b .0012a .0369b .0027 .0535a .0052
Item mean .0206 .0031 .0465 .0045 .0864 .0090
Single imputation .0113a .0015b .0294a .0008a .0604 .0052
Matched item mean .0357 .0046 .0988 .0071 .1465 .0086
Abbreviations: PMD, population mean deviation; SSD, sum of squared deviation.a Refers to the smallest p-value among the imputation methods.b Refers to the second smallest p-value among the imputation methods.
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315 309
generated for this study has been decided and set at
10%, 20%, and 30%. For the nonrandom process,
missing data were generated using a mechanism such
that the probability of a nonresponded item is a
function of the score of a patient’s global QOL,
which ranged from 1 to 7, and a predefined rate of
nonresponses, 10%, 20%, and 30%. The percentage
of nonresponse for ith subject is (NR)I, as follows:
ðNRÞi ¼ Rð8� GiÞ=7; i ¼ 1; . . . ; n
where R is the predefined rate of nonresponse, and Gi
is the global QOL score for the ith patient among a
total of n patients. Because a small Gi is associated
with poor global QOL, the percentage of nonresponse
is higher for a patient with poorer global QOL.
Evaluation criteria
In assessing the accuracy of the imputation meth-
ods, the precision of the imputed individual total
score is evaluated by the average sum of squared
Table 4
Average deviations for nonrandom missing data (N = 452)
10% data missing 20
Imputation method SSD PMD SS
Case deletion Nil .0135 N
Subscale mean .0188b .0026a .0
Subscale mean 50% .0188b .0026a .0
Item mean .0231 .0046 .0
Single imputation .0141a .0029b .0
Matched item mean .0351 .0048 .0
Abbreviations: PMD, population mean deviation; SSD, sum of sqa Refers to the smallest p-value among the imputation methodb Refers to the second smallest p-value among the imputation
deviation (SSD) between the imputed values and the
actual values, as follows:
SSD ¼XNi¼1
XKj¼1
ðYij � YijÞ2
nj
0BBBB@
1CCCCA;
i ¼ 1; . . . ; n; and j ¼ 1; . . . ;K
where Yij is the sum of the jth subscale of the ith
subject from the imputed data set, Yij is the total for
the individual subscale of complete data, nj is the
number of complete cases in the jth subscale, N is the
number of subjects in the data, and K is the number
of subscales.
Another evaluation index is the deviation of the
averaged population mean deviation (PMD) between
the imputed data set and the actual complete data set.
The accuracy of the imputation methods is measured
by the absolute difference between the sample mean
% data missing 30% data missing
D PMD SSD PMD
il .0184 Nil .0246
175a .0036b .0298a .0034a
177b .0057 .0298a .0051b
451 .0063 .0856 .0100
256 .0027a .0537b .0081
503 .0061 .1078 .0077
uared deviation.
s.
methods.

Table 5
Health-related morality-of-the data response rates
Worsened Stable Improved Fisher’s p-valueb MH c2 P valuec
Physical functioning GE 11 (32%) 12 (35%) 11 (32%) .346 .477
GP 11 (32%) 7 (21%) 16 (47%)
Role functioning GE 10 (29%) 4 (12%) 20 (59%) 1.000 .785
GP 9 (26%) 4 (12%) 21 (62%)
Emotional functioning GE 9 (26%) 25 (74%) 0 .369 .234
GP 5 (15%) 29 (85%) 0
Cognitive functioning GE 13 (38%) 8 (24%) 13 (38%) .321 .154
GP 7 (21%) 10 (29%) 17 (50%)
Social functioning GE 14 (41%) 7 (21%) 13 (38%) .574 .277
GP 10 (29%) 7 (21%) 17 (50%)
Global QOL GE 13 (38%) 11 (32%) 10 (29%) .215 .783
GP 15 (44%) 5 (15%) 14 (41%)
Fatigue GE 14 (41%) 2 (6%) 18 (53%) .409 .516
GP 10 (29%) 5 (15%) 19 (56%)
Nausea and vomiting GE 15 (44%) 15 (44%) 4 (12%) .022a .032a
GP 26 (76%) 5 (15%) 3 (9%)
Pain GE 12 (35%) 7 (21%) 15 (44%) .810 .496
GP 10 (29%) 6 (18%) 18 (53%)
Dyspnea GE 13 (38%) 13 (38%) 8 (24%) .106 .036a
GP 7 (21%) 11 (32%) 16 (47%)
Insomnia GE 13 (38%) 9 (26%) 12 (35%) .136 .049a
GP 7 (21%) 7 (21%) 20 (59%)
Appetite loss GE 21 (62%) 13 (36%) 0 1.000 .806
GP 20 (59%) 14 (41%) 0
Constipation GE 13 (38%) 14 (41%) 7 (21%) 1.000 1.000
GP 13 (38%) 14 (4%) 7 (21%)
Diarrhea GE 5 (15%) 29 (85%) 0 .003a .180
GP 7 (21%) 19 (56%) 8 (24%)
Financial difficulties GE 8 (24%) 19 (56%) 7 (21%) .003a .001a
GP 2 (6%) 12 (35%) 20 (59%)
Abbreviations: GE, gemcitabine plus etoposide; GP, gemcitabine plus cisplatin.a Refers to p <0.05.b Fisher’s exact test with 2 degrees of freedom.c Mantel-Haenszel test with 1 degree of freedom.
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315310
of the questionnaire when there are no missing data,
as follows:
lf ¼
XNi¼1
Xnjj¼1
ðYij=njÞ=N
where N is the total number of subjects, nj is the
number of items in the jth subscale, and Yij is the total
for the individual and subscale of complete data. The
sample mean of the questionnaire when the missing
data are handled by the imputation methods is
as follows:
l ¼XNi¼1
Xnyj¼1
ðYij=njÞ=N
where Yij is the total of the completed and imputed
values for subjects with missing items. The absolute
deviation of the population means is PMD.
Comparisons of results among methods
In the simulation, missing rates of 10%, 20%, and
30% were used. The precision of the imputed values
was evaluated using the average SSD method of
individual items and the method of PMD. In SSD
and PMD approaches, values that are closer to 0
indicate smaller differences between the imputed
and actual values. The smaller the value, the better
the performance of the corresponding imputation
method. Results for missing items generated using a
random process are shown in Tables 1 and 2. Results
for missing items generated using a nonrandom
process are shown in Tables 3 and 4. The results of
average deviations all were close to zero in the
average SSD and the PMD; multiple imputation has
shown its accuracy and ability to minimize potential
biases caused by the missing data.
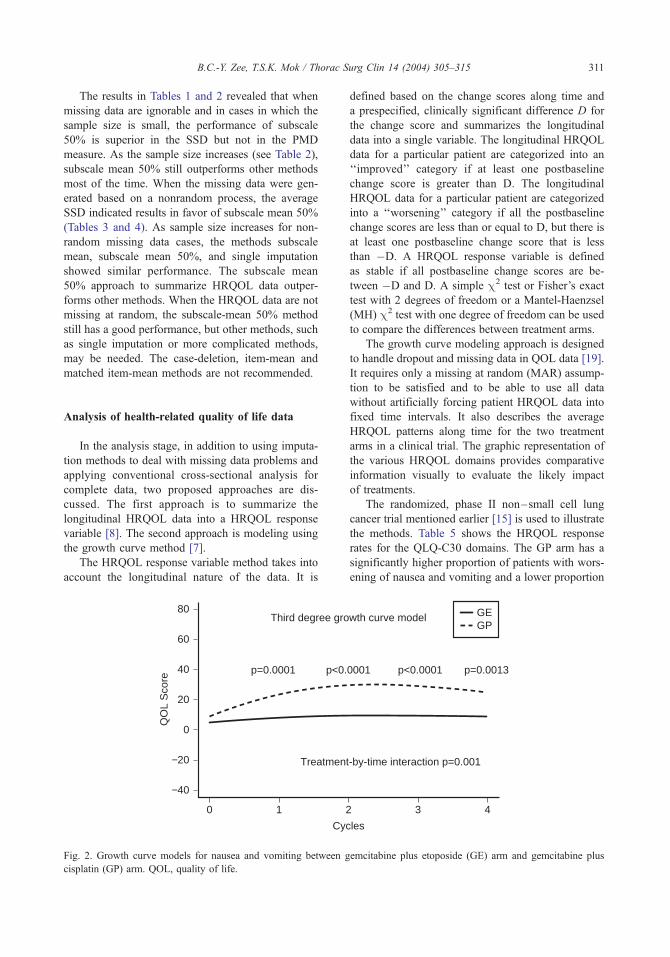
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315 311
The results in Tables 1 and 2 revealed that when
missing data are ignorable and in cases in which the
sample size is small, the performance of subscale
50% is superior in the SSD but not in the PMD
measure. As the sample size increases (see Table 2),
subscale mean 50% still outperforms other methods
most of the time. When the missing data were gen-
erated based on a nonrandom process, the average
SSD indicated results in favor of subscale mean 50%
(Tables 3 and 4). As sample size increases for non-
random missing data cases, the methods subscale
mean, subscale mean 50%, and single imputation
showed similar performance. The subscale mean
50% approach to summarize HRQOL data outper-
forms other methods. When the HRQOL data are not
missing at random, the subscale-mean 50% method
still has a good performance, but other methods, such
as single imputation or more complicated methods,
may be needed. The case-deletion, item-mean and
matched item-mean methods are not recommended.
Analysis of health-related quality of life data
In the analysis stage, in addition to using imputa-
tion methods to deal with missing data problems and
applying conventional cross-sectional analysis for
complete data, two proposed approaches are dis-
cussed. The first approach is to summarize the
longitudinal HRQOL data into a HRQOL response
variable [8]. The second approach is modeling using
the growth curve method [7].
The HRQOL response variable method takes into
account the longitudinal nature of the data. It is
1 20
80
60
0
20
40
−20
−40
QO
L S
core
Cyc
Treatmen
Third degree gro
p=0.0001 p<0.
Fig. 2. Growth curve models for nausea and vomiting between g
cisplatin (GP) arm. QOL, quality of life.
defined based on the change scores along time and
a prespecified, clinically significant difference D for
the change score and summarizes the longitudinal
data into a single variable. The longitudinal HRQOL
data for a particular patient are categorized into an
‘‘improved’’ category if at least one postbaseline
change score is greater than D. The longitudinal
HRQOL data for a particular patient are categorized
into a ‘‘worsening’’ category if all the postbaseline
change scores are less than or equal to D, but there is
at least one postbaseline change score that is less
than �D. A HRQOL response variable is defined
as stable if all postbaseline change scores are be-
tween �D and D. A simple c2 test or Fisher’s exact
test with 2 degrees of freedom or a Mantel-Haenzsel
(MH) c2 test with one degree of freedom can be used
to compare the differences between treatment arms.
The growth curve modeling approach is designed
to handle dropout and missing data in QOL data [19].
It requires only a missing at random (MAR) assump-
tion to be satisfied and to be able to use all data
without artificially forcing patient HRQOL data into
fixed time intervals. It also describes the average
HRQOL patterns along time for the two treatment
arms in a clinical trial. The graphic representation of
the various HRQOL domains provides comparative
information visually to evaluate the likely impact
of treatments.
The randomized, phase II non–small cell lung
cancer trial mentioned earlier [15] is used to illustrate
the methods. Table 5 shows the HRQOL response
rates for the QLQ-C30 domains. The GP arm has a
significantly higher proportion of patients with wors-
ening of nausea and vomiting and a lower proportion
3 4
les
t-by-time interaction p=0.001
wth curve model GEGP
p=0.00130001 p<0.0001
emcitabine plus etoposide (GE) arm and gemcitabine plus

1 2 30 4
100
80
60
0
20
40
−20
QO
L S
core
Cycles
Treatment-by-time interaction p=0.0125
Third degree growth curve modelGEGP
p=0.0291 p=0.0431p=0.0726 p=0.0356
Fig. 3. Growth curve models for dyspnea between gemcitabine plus etoposide (GE) arm and gemcitabine plus cisplatin (GP) arm.
QOL, quality of life.
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315312
of patients with stable response and improvement
(P = .022, 2 degrees of freedom). Dyspnea and
insomnia are significant only in the Mantel-Haenzsel
c2 test (P = .036 and P = .049 with 1 degree of
freedom) and not in Fisher’s exact test (P = .106 and
P = .136 with 2 degrees of freedom), showing that
GP has more improvement in both of these symptoms
and less in the stable and worsening categories. In
general, the Mantel-Haenzsel c2 test is more power-
ful at detecting linear trends and less powerful at
detecting nonlinear relationships.
10
80
60
0
20
40
−20
QO
L S
core
Cy
Treatme
Second degree gro
p=0.8850 p=0.
Fig. 4. Growth curve models for insomnia between gemcitabine
(GP) arm. QOL, quality of life.
When the results are assessed using growth curve
models, nausea and vomiting at baseline is close to 0,
indicating that there is no nausea and vomiting before
patients receive chemotherapy. There are significant
differences in each of the first four cycles, all of them
in favor of the GE arm after treatment started (Fig. 2).
For dyspnea, the sample size is relatively small for a
randomized phase II study with only 34 patients in
each of the two arms. The dyspnea score at baseline
for GE is 23.5 (SD = 25.33) and 46.1 (SD = 30.72)
for GP (P = .0026). The growth curve shows an
2 3 4
cles
nt-by-time interaction p=0.117
wth curve model GEGP
p=0.33977285 p=0.4701
plus etoposide (GE) arm and gemcitabine plus cisplatin
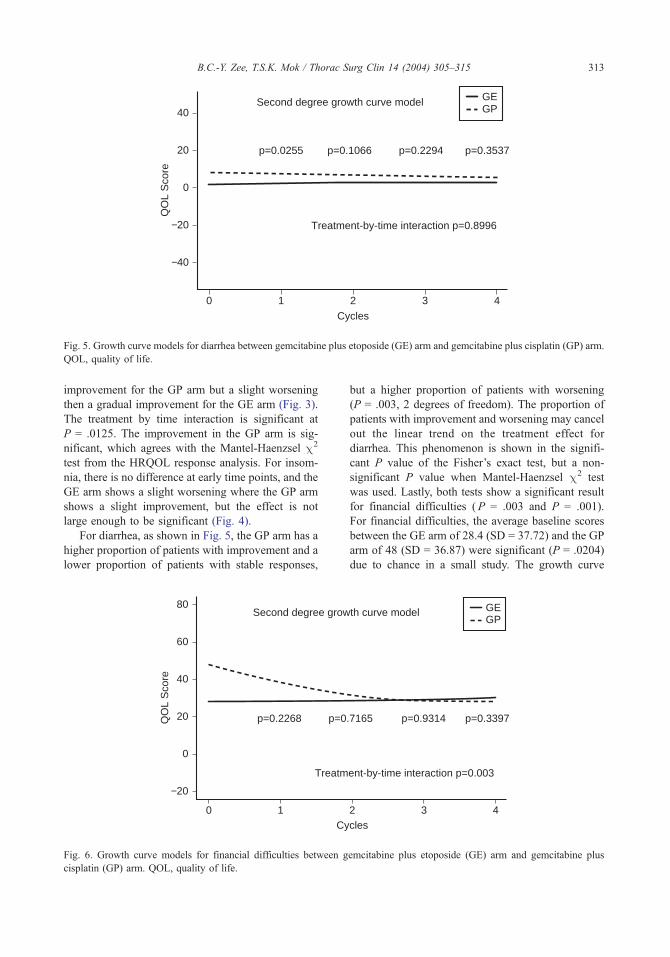
1 2 30 4
40
20
−20
0
−40
QO
L S
core
Cycles
Treatment-by-time interaction p=0.8996
Second degree growth curve model GEGP
p=0.0255 p=0.3537p=0.1066 p=0.2294
Fig. 5. Growth curve models for diarrhea between gemcitabine plus etoposide (GE) arm and gemcitabine plus cisplatin (GP) arm.
QOL, quality of life.
B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315 313
improvement for the GP arm but a slight worsening
then a gradual improvement for the GE arm (Fig. 3).
The treatment by time interaction is significant at
P = .0125. The improvement in the GP arm is sig-
nificant, which agrees with the Mantel-Haenzsel c2
test from the HRQOL response analysis. For insom-
nia, there is no difference at early time points, and the
GE arm shows a slight worsening where the GP arm
shows a slight improvement, but the effect is not
large enough to be significant (Fig. 4).
For diarrhea, as shown in Fig. 5, the GP arm has a
higher proportion of patients with improvement and a
lower proportion of patients with stable responses,
10
80
60
0
20
40
−20
QO
L S
core
Cy
Treatm
Second degree grow
p=0.2268 p=0
Fig. 6. Growth curve models for financial difficulties between g
cisplatin (GP) arm. QOL, quality of life.
but a higher proportion of patients with worsening
(P = .003, 2 degrees of freedom). The proportion of
patients with improvement and worsening may cancel
out the linear trend on the treatment effect for
diarrhea. This phenomenon is shown in the signifi-
cant P value of the Fisher’s exact test, but a non-
significant P value when Mantel-Haenzsel c2 test
was used. Lastly, both tests show a significant result
for financial difficulties (P = .003 and P = .001).
For financial difficulties, the average baseline scores
between the GE arm of 28.4 (SD = 37.72) and the GP
arm of 48 (SD = 36.87) were significant (P = .0204)
due to chance in a small study. The growth curve
2 3 4cles
ent-by-time interaction p=0.003
th curve model GEGP
p=0.3397.7165 p=0.9314
emcitabine plus etoposide (GE) arm and gemcitabine plus

B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315314
shows a clear difference in favor of the GE arm at
baseline; the GP arm is shown to improve quickly to
the same level of the GE arm after starting treatment
(Fig. 6). The difference in the rates of change
between the two arms is shown in the treatment by
time interaction test (P = .003).
In general, the Mantel-Haenzsel c2 test for the
HRQOL response shows the test of trend between the
two treatment arms with respect to the corresponding
domain. Fisher’s exact test provides an indication of
any differences between arms. The HRQOL response
approach is simple to understand and to carry out. It
lacks the visual presentation of the growth curve,
however, that provides more details to explain some
of the average patterns and potential disparity of
HRQOL scores at the baseline.
Summary
The methodology for QOL assessment covers a
wide range of topics. It involves a proper choice of
instruments with appropriate psychometric properties,
the administration of these instruments, frequency
of measurements, missing data problems, and the
method of analysis. There are currently debates on
the meaning and interpretation of the HRQOL
domains taking the form of arguing how to define
minimal clinically meaningful difference and whether
this can be used in regulatory approval for drug
development [20]. From a practical point of view,
the authors proposed that a disease-specific checklist
or symptom domains incorporated within a HRQOL
questionnaire may be a middle ground to gain general
agreements among academic institutions, manufac-
turers, and regulatory agencies to use a specific
symptom checklist or domain as the primary end
point for clinical trials together with other HRQOL
domains as ancillary data for the study. Antiemetic
trial with HRQOL assessments is an example. Most
would agree, however, that no matter what HRQOL
domains or symptoms are being studied, it should be
based on a patient self-administered questionnaire as
shown by the lack of sensitivity in the example in this
article [15]. Missing data are a problem in the data
collection and handling. The authors have examined a
few commonly used approaches and performed simu-
lation to study their properties. The subscale-mean
method when one has more than 50% of the infor-
mation on a subscale generally reflects the true
values. In practice, one still would have missing data
that cannot be handled completely by imputation. The
method of analysis must be flexible enough to
incorporate the nature of these data. Two approaches
have been discussed, and they are both flexible in
terms of using all available information being ob-
tained in a longitudinal fashion with variable visiting
schedules and potential missing data. The HRQOL
response variable approach is simple and easy to
understand. The growth curve models approach pro-
vides more detailed information on average trends
between treatment arms. In general, these two meth-
ods agree on the results of the example. They can be
used to report clinical trial results using HRQOL data
as end points.
References
[1] Ware Jr JE. Measuring functioning, well-being, and
other generic health concepts. In: Osoba D, editor.
Effect of cancer on quality of life. Boca Raton, FL:
CRC Press; 1991. p. 7–23.
[2] Kaasa S. Measurement of quality of life in clinical
trials. Oncology 1992;49:288–94.
[3] Bruner D. In search of the ‘‘quality’’ in quality-of-life
research. Int J Radiat Oncol Biol Phy 1995;31:191–2.
[4] Osoba D, Aaronson NK, Till JE. A practical guide for
selecting quality-of-life measures in clinical trials
and practice. In: Osoba D, editor. Effect of cancer on
quality of life. Boca Raton, FL: CRC Press; 1991.
p. 89–104.
[5] Beitz J, Gnecco C, Justice R. Quality of life endpoints
in cancer clinical trials: the Food and Drug Adminis-
tration perspectives. J Natl Cancer Inst Monogr 1996;
20:7–9.
[6] Osoba D, Zee B. Completion rates in health-related
quality-of-life assessment: approach of the National
Cancer Institute of Canada Clinical Trials Group. Stat
Med 1998;17:603–12.
[7] Zee B. Growth curve model analysis for quality of life
data. Stat Med 1998;17:757–66.
[8] Tu D, Liu J, Pater J. Analysis of the ordinal quality of
life response data: whither simple chi-square tests?
Controlled Clinical Trials 2003;24:229S.
[9] Fayers P, Aaronson N, Bjordal K, et al. EORTC QLQ-
C30 Scoring Manual. Brussels: EORTC Quality of
Life Study Group; 1999.
[10] Levitt M, Warr D, Yelle L, et al. A comparison of
ondansetron versus dexamethasone and metoclopra-
mide as antiemetics in the chemotherapy of breast
cancer with cyclophosphamide, methotrexate, and
5-fluorouracil: a study by the Clinical Trials Group
of the National Cancer Institute of Canada. N Engl J
Med 1993;328:1081–4.
[11] Kaizer L, Warr D, Hoskins P, et al. The effect of sched-
ule and maintenance on the antiemetic efficacy of
ondansetron combined with dexamethasone in acute
and delayed nausea and emesis in patients receiving
moderately emetogenic chemotherapy: a phase II trial

B.C.-Y. Zee, T.S.K. Mok / Thorac Surg Clin 14 (2004) 305–315 315
by the National Cancer Institute of Cancer Clinical
Trials Group. J Clin Oncol 1994 May;12(5):1050–7.
[12] Pater J, Lofters WS, Zee B, et al. The role of 5HT3
antagonists in the control of delayed onset of nausea
and vomiting in patients receiving moderately emeto-
genic chemotherapy. Ann Oncol 1997;8:181–5.
[13] Lofters WS, Pater J, Zee B, et al. A phase III Dou-
ble-blind comparison of dolasetron mesylate and on-
dansetron, and an evaluation of the additive role of
dexamethasone in the prevention of acute and delayed
nausea and vomiting due to moderately emetogenic
chemotherapy. J Clin Oncol 1997;15:2966–73.
[14] Zee B, Yeo W, Lai M, et al. Chemotherapy-induced
nausea affects patients’ quality of life (QOL) more
than vomiting. Presented at ISOQOL, November
12–5, 2003
[15] Mok TS, Zee B, Nguyen B, et al. A prospective ran-
domized study comparing toxicity and quality of life of
two gemcitabine-based regimens (with or without cis-
platin) for treatment of advanced non-small-cell lung
cancer. ASCO; 2002.
[16] Hopwood P, Stephens RJ, Machin D. Approaches to
the analysis of quality of life data: experiences gained
from a Medical Research Council Lung Cancer Work-
ing Party palliative chemotherapy trial. Qual Life Res
1994;3:339–52.
[17] Latreille J, Pater J, Johnston D, et al. Use of dexameth-
asone and granisetron in the control of delayed emesis
for patients who receive highly emetogenic chemother-
apy. J Clin Oncol 1998;16:1174–8.
[18] Bernhard J, Gelber RD, editors. Workshop on missing
data in quality of life research in cancer clinical trials:
practical and methodological issues. Stat Med 1998;
17:511–796.
[19] Fairclough D, Peterson H, Cella D, Bonomi P. Com-
parison of several model-based methods for analysing
incomplete quality of life data in clinical trials. Stat
Med 1998;17:781–96.
[20] Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Inter-
preting the significance of changes in health-related
quality-of-life scores. J Clin Oncol 1998;16:139–44.

Thorac Surg Clin 14 (2004) 317–323
Acute and chronic reduction of pulmonary function after
lung surgery
Ibrahim Bulent Cetindag, MDa, William Olson, MDa,Stephen R. Hazelrigg, MDb,*
aDivision of General Surgery, Southern Illinois University School of Medicine, 800 North Rutledge, Room D319,
Springfield, IL 62702, USAbDivision of Cardiothoracic Surgery, Southern Illinois University School of Medicine, 800 North Rutledge, Room D319,
Springfield, IL 62702, USA
Thoracic surgeons are facing an increased number mal disease requires the use of a combination of
of complicated and elderly patients for consideration
of pulmonary resection. In evaluating these patients,
surgeons continually must balance the benefits of
resection with the operative risks. Today the peri-
operative mortality rate for lung resection is low, but
it increases with the magnitude of the lung resection
planned. For pneumonectomies, reported periopera-
tive mortality and morbidity rates are 6% to 15%
and 36% to 70% [1–7], whereas for lobectomies,
mortality is much lower (3–7%) [1–7]. Respiratory
failure remains the leading cause of mortality and
morbidity after lung surgery, and the preoperative
estimation of pulmonary function is important to
aid in predicting the likelihood of postoperative
complications. The preoperative evaluation may
alter the extent of lung resection, preoperative pul-
monary preparation, surgical approach, or analgesic
strategy [8].
Many different tools are used simultaneously for
predicting the acute and long-term changes in pul-
monary functions after lung surgery (Box 1) [9–15].
This preoperative assessment can be done easily for
patients with good pulmonary function by using one
pulmonary function test, such as forced expiratory
volume in 1 second (FEV1). The decision with regard
to the type of resection for patients with severe
chronic obstructive pulmonary disease or parenchy-
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00019-2
* Corresponding author.
E-mail address: [email protected] (S.R. Hazelrigg).
several different tests. The surgeon strives to ensure
that the planned procedure will provide the patient a
reasonable outcome without chronic respiratory in-
sufficiency. This article reviews the literature pertain-
ing to acute and chronic lung function changes after
lung surgery.
Preoperative evaluation
The literature abounds with data and opinions on
the question of which pulmonary function test is most
predictive for postoperative outcome.
Spirometry is one of the oldest and most practical
tests for pulmonary mechanical function. Although
modern spirometry is able to report a multitude of
flows and volumes, the most often used parameters
for preoperative evaluation include forced vital ca-
pacity (FVC), FEV1, and the FEV1/FVC ratio. All
values are reported before and after bronchodilator
therapy, as milliliters, and as a percent predicted for
the patient’s age and body surface. A 15% improve-
ment with bronchodilators is considered a significant
improvement suggesting reactive airway disease.
Levels that have been associated with increased
pulmonary complications early after surgery are less
than 50% predicted for FVC and less than 60% for
FEV1/FVC ratio [16]. FEV1 has been studied exten-
sively and probably is the most common single
spirometric parameter used to predict postoperative
respiratory insufficiency [17–19]. The desired level
s reserved.

Box 1. Preoperative tools for prediction ofpostoperative lung function changes
1. Function testsSpirometry (FEV1)Parenchymal function (DLCO,arterial blood gasesCardiopulmonary function (exercisetolerance, VO2max, 6-minutewalk test)
2. Ventilation/perfusion scan3. CT or MRI4. Bronchoscopy
I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323318
of postoperative FEV1 is approximately 800 mL in an
average-size adult. The percent-predicted values
should be used in clinical practice because they
provide a more accurate assessment. Predicted post-
operative (PPO) FEV1 ideally should be greater than
30% to 40% predicted for the patient’s size and age.
The formula for PPO FEV1 is as follows [16]:
PPOFEV1
¼ preoperative FEV1ðas percent predicted valueÞ
� ð1�%functional lung tissue removed=100Þ
For patients with homogeneous lung parenchyma,
the right lung is considered roughly 10% larger than
the left, and the right upper and middle lobes can be
considered as one lobe [16]. The calculation for PPO
FEV1 is based on functional segments, with value
assigned as follows: Right upper lobe (RUL) is 6 (ap-
proximately 14%), right middle lobe (RML) is 4
(approximately 10%), right lower lobe (RLL) is 12
(approximately 30%), and left upper lobe (LUL) and
lower lobe (LLL) are 10 (approximately 23%) each.
A PPO FEV1 greater than 40% is a safe level to
prevent postoperative pulmonary complications. The
PPO FEV1 levels of 30% and less are associated with
a high incidence of prolonged postoperative ventila-
tory support due to respiratory insufficiency [17,18].
The overall condition of the patient always should be
considered with the FEV1. Gass and Olsen [19] in
their review showed 21% PPO FEV1 might be well
tolerated by young men, whereas 48% is the lower
limit for elderly women. Evaluating by the patient’s
exercise capacity along with their FEV1 is often
enough for surgical clearance with regard to the
preoperative evaluation of lung function in good-risk
patients. For patients with a marginal PPO FEV1 and
exercise capacity, other lung function and preopera-
tive evaluations should be performed.
The DLCO is another common lung function test
that is reported with spirometry results. Preoperative
DLCO less than 60% predicted is associated with an
increased incidence of pulmonary complications [20].
PPO DLCO of 40% or less also has a higher mortality
and morbidity [21,22]. PPO DLCO is calculated
similar to PPO FEV1 [23]. Patients with severe
emphysematous disease and lesions located in the
emphysematous parts of the lungs often can undergo
resection safely even with a preoperative DLCO less
than 60% predicted. Because these emphysematous
areas are not contributing to gas exchange (and they
may compress potentially functional lung), there
often is little change in postoperative pulmonary
function values [23].
The simplest and most important assessment is
cardiopulmonary function. A valuable and easy way
to assess cardiopulmonary function is with a careful
history pertaining to the patient’s exercise capacity.
A traditional test for ambulatory patients is the stair-
climbing test. Olsen et al [24], in their retrospective
review, found that patients unable to climb two flights
of stairs were more likely to have postoperative
pulmonary morbidity. Usually one flight is defined
as 20 steps with each step 6 inches in height [16].
Rao et al [25], in their retrospective study, investi-
gated the value of spirometry and exercise oximetry
in predicting postoperative home oxygen require-
ments. They found that simple exercise oximetry is
a better tool than FEV1 for predicting postoperative
home oxygen requirements and intensive care unit
admissions. They also showed the cost-effectiveness
of this method.
A more sophisticated laboratory test for cardio-
pulmonary function is VO2max. This test may be a
useful tool in marginal patients with pulmonary
insufficiency. Walsh et al [26] showed that patients
with VO2max of 15 mL/kg/min and greater with
marginal FEV1 could be operated on with a reason-
able risk of pulmonary morbidity and no mortality.
Another useful cardiopulmonary function test is the
6-minute walk distance test, which has been used as a
routine in the authors’ lung volume reduction
patients. A 6-minute walk 2000 feet and less is
associated with a higher incidence of postoperative
pulmonary insufficiency [27].
The ventilation/perfusion scan, bronchoscopy, and
imaging (CT and MRI) studies also may contribute to
a surgeon’s estimation of postoperative lung function.
Although predictive postoperative values of different
spirometry calculations is possible to predict based on
the formula explained earlier t, it can be predicted

I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323 319
more accurately in patients with significant bullous
disease by using the ventilation/perfusion scan [25].
Ventilation/perfusion scans can give accurate infor-
mation about the distribution of functional areas of
the lung [28]. Bronchoscopy may show bronchial
obstruction that would affect calculations of post-
operative pulmonary function. The lung segment
beyond these areas should not be taken into consid-
eration in the calculation. Tracheomalacia also can be
visualized with bronchoscopy in an awake setting.
Patients with tracheomalacia have an abnormally low
FEV1 but often tolerate the resection of the lung
beyond this area [16].
CTandMRI give information about nonfunctional,
air-filled bullous regions and the magnitude and num-
ber of lung masses. Patients with large tumors may
have little function loss after pulmonary resection
depending on how much functional lung needs to be
resected. Patients with significant emphysema may
improve after upper lobectomies because of the
removal of space-occupying nonfunctional lung. Se-
lected patients with lung cancer and disabling emphy-
sema (with suitable anatomy for lung volume
reduction) may benefit from a combined lobectomy
and lung reduction [23,29]. The degree of heteroge-
neous or homogeneous disease on high-resolution CT
scan can be assessed to predict how a resection would
be tolerated [30].
Surgical approach and postoperative lung
function changes
Pain and the amount of lung tissue removed are
the two most important factors in early postoperative
respiratory problems. Chest wall injuries affect the
compliance of the thoracic cage and lead to depres-
sion of total volumes for about 3 weeks. Chest wall
mechanics and pain are at their worst in the early
postoperative period and can result in significant
decreases in pulmonary volumes. The specific type
of thoracic incision can affect respiratory compro-
mise [31].
Thoracotomy is considered one of the more pain-
ful approaches among surgical incisions [32]. Several
different modifications of posterolateral thoracotomy
(PLT) have been suggested in the literature to dimin-
ish the pain and functional deterioration after this
approach [32–40]. These modifications include
limited lateral thoracotomy (LLT), muscle-sparing
thoracotomy (MST), anterior limited thoracotomy
(ALT), vertical axillary thoracotomy, anteroaxillary
thoracotomy (AAT), and axillary thoracotomy. Hazel-
rigg et al [40] evaluated the effects of MST versus
PLT on pulmonary function, pain, and muscle
strength. That prospective study concluded that the
MST is associated with improved postoperative pain
but no significant effects on postoperative FEV1 at
1 week and 1 month. Nomori et al [41] compared
ALT, AAT, video-assisted thoracoscopic surgery
(VATS), and PLT after lobectomy. The PLT approach
was associated with significantly lower vital capacity
between the first week and 24 months. These inves-
tigators also found better 6-minute walk distances in
the first postoperative week after ALT and VATS
approaches. There were no significant differences
between ALT and VATS in terms of 6-minute walk
and vital capacity at any time point after lobectomy.
The superiority of VATS in terms of preservation
of lung function in the immediate postoperative
period has been noted [42–52]. Outcome in lung
biopsy patients has been improved after VATS versus
open lung biopsy [42]. Similarly, there has been
better outcome in other patient populations using
VATS [45]. Reduced pain after VATS is associated
with a faster recovery in vital capacity and cardio-
pulmonary function [41,52]. Circulating cytokine
levels during and after surgery (which are associated
with systemic organ injury, such as adult respiratory
distress syndrome) have been shown to be signifi-
cantly lower with VATS compared with the conven-
tional approach [50]. Video-assisted thoracoscopic
procedures also may be associated with better oxy-
genation and diffusion capacity after surgery. Nomori
et al [41] compared the ALT approach with VATS in a
separate study. Their initial study (mentioned previ-
ously in the thoracotomy section) failed to show
significance between the two approaches. Their sec-
ond study showed superior 6-minute walk results
with the VATS approach. This difference did not
reach significance (P = .06), however [49]. Land-
reneau et al [48] reported similar findings; however,
in their study there was a change in FEV1 in the first
week that was significantly better with VATS versus a
limited thoracotomy.
Median sternotomy is another favorable approach
for preservation of lung function. It was noted that
patients who underwent sternotomy preserved their
total lung capacity [31]. It is speculated that because
respiratory muscles are left intact and pain is less after
this approach, the chest wall mechanics are better
preserved. Because of these favorable effects, median
sternotomy became the incision of choice for some
surgeons [53,54]. Hazelrigg et al [43] showed no
significant difference between median sternotomy
and staged VATS in terms of 6-minute walk and
dyspnea scores after lung volume reduction surgery
for pulmonary emphysema. The authors’ preliminary

I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323320
observation with a similar ongoing study on bilateral
VATS and median sternotomy for lung reduction
patients supports these findings. Cooper et al [55]
showed that the recovery of spirometric function is
significantly faster after median sternotomy than after
lateral thoracotomy.
Degree of lung resection and lung function
changes
For thoracic surgeons, there are two questions
to answer preoperatively in deciding the extent of
the resection:
1. What is the optimal resection for the pathology?
2. What resection can be tolerated by the patient?
The second question is the focus of this review.
In practice, the correlation between lung tissue
resected and the change in lung function is not linear.
Ali et al [56] showed good correlation in lung
function changes and resected lung when three or
more segments are removed. In smaller resections
(wedge resection or segmentectomy), pulmonary
function tests were better preserved than predicted.
Wedge resection, on patients with marginal FEV1
levels, often can be done in patients with less than
3 cm peripheral malignancies with low risk. Careful
evaluation of x-ray studies and cardiopulmonary
function is mandatory [57]. In high-risk patients,
the minimally invasive approach may be the choice
to minimize early postoperative respiratory insuffi-
ciency [23,29].
Postoperative management
Inadequate pain control not only creates discom-
fort for the patient, but also it may cause an additional
reduction in lung function by impairment of respira-
tory effort and atelectasis. This impairment is promi-
nent in patients with obesity, a significant history of
smoking, old age, and preexisting cardiovascular
disease [32]. The VATS approach often is tolerated
well in terms of postoperative pain–related pulmo-
nary morbidity [41,42,52].
Pain control strategies are an important determi-
nant of postoperative pulmonary function [32,57–59].
Of pain regimens, thoracic epidural analgesia seems to
be the most practical and favorable method in terms of
preservation of lung function [32,57]. The lung func-
tion is preserved in the 40% to 60% range with
thoracic epidural analgesia after thoracotomy. Tho-
racic epidural analgesia also has been shown to im-
prove outcomes significantly with regard to length of
hospital stay and postoperative pulmonary complica-
tions [58,60,61].
Systemic opioid analgesia has some depressive
effects on lung function even though in some studies
pain control is as good as the epidural analgesia [32].
The authors’ approach for patients with marginal lung
function is to use thoracic epidural analgesia with
ketorolac to avoid or minimize the depressive effects
of opioids.
Long-term changes in pulmonary function
After lung resections, the remaining lung expands,
the mediastinum shifts, and the diaphragm rises to
lessen the size of the thorax. Vital capacity and total
lung capacity typically decrease. In marginal patients,
this decrease may lead to an increase in oxygen
requirement in the short-term [31].
In the perioperative period, postoperative physical
reconditioning and anemia can augment the magni-
tude of functional loss. After the acute phase, this
reconditioning of lung function reaches a steady state.
This steady state is related to the extent of lung
resection and other concomitant disability. Although
a change in lung volume occurs, the exercise capac-
ity may not correlate [62]. The overall exercise tole-
rance depends on the matched blood flow, diffusion
through the capillaries, affinity of hemoglobin to
oxygen, and mitochondrial activity. The VO2max,
which is a reflection of the patient’s physical and
cardiopulmonary function, depends more on the car-
diac output and peripheral oxygen extraction and
uptake than maximal ventilation and diffusing ca-
pacity [63]. Enhancing the cardiac output and oxy-
gen extraction with regular exercise improves the
patient’s overall functional status and oxygenation
without changing the chronic restrictive changes after
lung resection. This is the concept behind pulmonary
rehabilitation in marginal patients in the preoperative
and postoperative periods [62]. For all of the previ-
ously mentioned reasons, cardiopulmonary disability
after lung surgery depends on the preoperative exer-
cise tolerance, postoperative physical recovery, and
regular exercise more than the preoperative spiromet-
ric volumes. A less invasive procedure may provide
faster recovery and better postoperative cardiopulmo-
nary function in the acute phase of the postoperative
period [41,49]. Conversely, large resections, such as
a pneumonectomy, have profound effects on cardio-
pulmonary function in the long-term. Nezu et al

I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323 321
[64] showed that lobectomy patients recover more
quickly than pneumonectomy patients during the first
6 months after surgery. The VO2max continues to
decrease for 6 months after surgery, after which time
it stabilizes.
Summary
Pulmonary function is affected by several varia-
bles. The more marginal the patient, the more impor-
tant the preoperative and perioperative assessment
becomes. VATS might be tolerated well with regard
to pulmonary function in the early postoperative
period. It has allowed thoracic surgeons to expand
surgical indications to patients that previously would
not have been considered.
References
[1] Ploeg AJ, Kappetein AP, vanTongeren RB, Pahlplatz
PV, Kastelein GW, Breslau PJ. Factors associated with
perioperative complications and long-term results after
pulmonary resection for primary carcinoma of the
lung. Eur J Cardiothorac Surg 2003;23:26–9.
[2] Jordan S, Mitchell JA, Quinlan GJ, Goldstraw P, Evans
TW. The pathogenesis of lung injury following pulmo-
nary resection. Eur Respir J 2000;15:790–9.
[3] Deslauriers J, Ginsberg RJ, Dubois P, Beaulieu M,
Goldberg M, Piraux M. Current operative morbidity
associated with elective surgical resection for lung can-
cer. Can J Surg 1989;32:335–9.
[4] Motta G, Ratto GB. Complications of surgery in the
treatment of lung cancer: their relationship with the
extent of resection and preoperative respiratory func-
tion tests. Acta Chir Belg 1989;89:161–5.
[5] Morice RC, Peters EJ, Ryan MB, Putnam JB, Ali MK,
Roth JA. Exercise testing in the evaluation of patients
at high risk for complications from lung resection.
Chest 1992;101:356–61.
[6] Nagasaki F, Flehinger BJ, Martini N. Complications of
surgery in the treatment of carcinoma of the lung.
Chest 1982;82:25–9.
[7] Harpole Jr DH, DeCamp Jr MM, Daley J, et al. Prog-
nostic models of thirty-day mortality and morbidity
after major pulmonary resection. J Thorac Cardiovasc
Surg 1999;117:969–79.
[8] American College of Physicians. Preoperative pulmo-
nary function testing. Ann Intern Med 1990;112:
793–4.
[9] Reilly JJ. Preparing for pulmonary resection: preopera-
tive evaluation of patients. Chest 1997;112: 206S–8S.
[10] Culver BH. Preoperative assessment of the thoracic
surgery patient: pulmonary function testing. Semin
Thorac Cardiovasc Surg 2001;13:92–104.
[11] Brunelli A, Al Refai M, Monteverde M, Sabbatini A,
Xiume F, Fianchini A. Predictors of early morbidity
after major lung resection in patients with and with-
out airflow limitation. Ann Thorac Surg 2002;74:
999–1003.
[12] Cottrell JJ, Ferson PF. Preoperative assessment of
the thoracic surgical patient. Clin Chest Med 1992;
13:47–53.
[13] Reilly Jr JJ, Mentzer SJ, Sugarbaker DJ. Preoperative
assessment of patients undergoing pulmonary resec-
tion. Chest 1993;103:342S–5S.
[14] Schuurmans MM, Diacon AH, Bolliger CT. Functional
evaluation before lung resection. Clin Chest Med
2002;23:159–72.
[15] Slinger PD, Johnston MR. Preoperative assessment for
pulmonary resection. Anesthesiol Clin North Am
2001;19:411–33.
[16] McCrae KM, Slinger PD, Sandler AN. Anesthesia. In:
Pearson FG, Cooper JD, Deslauriers J, et al, editors.
Thoracic surgery. 2nd edition. New York: Churchill
Livingstone; 2002. p. 51–82.
[17] Cerfolio RJ, Allen MS, Trastak VF, et al. Lung resec-
tion in patients with compromised pulmonary function.
Ann Thorac Surg 1996;62:348–51.
[18] Nakahara K, Ohno K, Hashimoto J, et al. Prediction of
postoperative respiratory failure in patients undergoing
lung resection for cancer. Ann Thorac Surg 1988;46:
549–52.
[19] Gass GD, Olsen GN. Preoperative pulmonary func-
tion testing to predict postoperative morbidity and
mortality. Chest 1986;89:127–35.
[20] Ferguson MK, Little L, Rizzo L, et al. Diffusing capac-
ity predicts morbidity and mortality after pulmonary
resection. J Thorac Cardiovasc Surg 1988;96: 894–900.
[21] Markos J, Mullan BP, Hillman DR, et al. Preoperative
assessment as a predictor of mortality and morbidity
after lung resection. Am Rev Respir Dis 1989;139:
902–10.
[22] Ferguson MK, Reeder LB, Mick R. Optimizing selec-
tion of patients for major lung resection. J Thorac Car-
diovasc Surg 1995;109:275–83.
[23] McKenna RJ, Fischel RJ, Brenner M, Gelb AF. Com-
bined operations for lung volume reduction surgery
and lung cancer. Chest 1996;110:885–8.
[24] Olsen GN, Bolton JWR, Weiman DS, Hornung CA.
Stair climbing as an exercise test to predict the post-
operative complications of lung resection: two years’
experience. Chest 1991;99:587–90.
[25] Rao V, Todd TRJ, Kuus A, Buth KJ, Pearson FG.
Exercise oximetry versus spirometry in the assessment
of risk prior to lung resection. Ann Thorac Surg 1995;
60:603–9.
[26] Walsh GL, Morice RC, Putnam Jr JB, et al. Resection
of lung cancer is justified in high-risk patients selected
by exercise oxygen consumption. Ann Thorac Surg
1994;58:704–11.
[27] Slinger PD, Johnston MR. Preoperative evaluation of
the thoracic surgery patient. In: Kaplan JA, Slinger PD,
editors. Thoracic anesthesia. 3rd edition. Philadelphia:
Churchill Livingstone; 2003. p. 1–23.
I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323322
[28] Cordiner A, DeCarlo F, DeGennaro R, Pau F, Flore F.
Prediction of postoperative pulmonary function follow-
ing thoracic surgery for bronchial carcinoma. Angiol-
ogy 1991;42:985–9.
[29] DeMeester SR, Patterson GA, Sundaresan RS, Cooper
JD. Lobectomy combined with volume reduction for
patients with lung cancer and advanced emphysema.
J Thorac Cardiovasc Surg 1998;115:681–8.
[30] Tschernko EM. Anesthesia considerations for lung vol-
ume reduction surgery. Anesthesiol Clin North Am
2001;19:591–609.
[31] Bolton JW, Weiman DS. Physiology of lung resection.
Clin Chest Med 1993;14:293–303.
[32] Hazelrigg SR, Cetindag IB, Fullerton J. Acute and
chronic pain syndromes after thoracic surgery. Surg
Clin North Am 2002;82:849–65.
[33] Fry WA, Kehoe TJ, McGee JP. Axillary thoracotomy.
Am Surg 1990;56:460–2.
[34] Horowitz MD, Ancalmo N, Oschner JL. Thoracotomy
through the auscultory triangle. Ann Thorac Surg
1989;47:782–3.
[35] Bethencourt DM, Holmes EC. Muscle-sparing postero-
lateral thoracotomy. Ann Thorac Surg 1988;45:337–9.
[36] Mitchell RL. The lateral limited thoracotomy incision:
standard for pulmonary operations. J Thorac Cardio-
vasc Surg 1990;99:590–6.
[37] Pecora DV. A functionally and cosmetically superior
thoracotomy incision. Surg Gynecol Obstet 1957;104:
626–8.
[38] Baeza OR, Foster ED. Vertical axillary thoracotomy:
a functional and cosmetically appealing incision. Ann
Thorac Surg 1976;22:287–8.
[39] Lemmer Jr JH, Gomez MN, Symrent T, et al. Limited
lateral thoracotomy: improved postoperative pulmo-
nary function. Arch Surg 1990;125:873–7.
[40] Hazelrigg SR, Boley TB, Landreneau RJ, et al. The
effect of muscle-sparing versus standard posterolateral
thoracotomy on pulmonary function, muscle strength,
and postoperative pain. J Thorac Cardiovasc Surg
1991;101:394–401.
[41] Nomori H, Ohtsuka T, Horio H, Naruke T, Seumasu K.
Difference in the impairment of vital capacity and
6-minute walking after a lobectomy performed by tho-
racoscopic surgery, an anterior limited thoracotomy, an
anteroaxillary thoracotomy, and a posterolateral thora-
cotomy. Surg Today 2003;33:7–12.
[42] Ferson PF, Landreneau RJ, Dowling RD, et al. Com-
parison of open versus thoracoscopic lung biopsy for
diffuse infiltrative pulmonary disease. J Thorac Cardi-
ovasc Surg 1993;106:194–9.
[43] Hazelrigg SR, Boley TM, Magee MJ, Lawyer CH,
Henkle JQ. Comparison of staged thoracoscopy and
median sternotomy for lung volume reduction. Ann
Thorac Surg 1998;66:1134–9.
[44] McKenna Jr RJ, Wolf RK, Brenner M, Fischel RJ,
Wurnig P. Is lobectomy by video-assisted thoracic sur-
gery an adequate cancer operation? Ann Thorac Surg
1998;66:1903–8.
[45] Demmy TL, Curtis JJ. Minimally invasive lobectomy
directed toward frail and high-risk patients: a case-con-
trolled study. Ann Thorac Surg 1999;68:194–200.
[46] Furrer M, Rechsteiner R, Eigenmann V, Signer C,
Althaus U, Ris HB. Thoracotomy and thoracoscopy:
postoperative pulmonary function, pain and chest wall
complains. Eur J Cardiothorac Surg 1997;12:82–7.
[47] Nakata M, Saeki H, Yokoyama N, Kurita A, Takiyama
W, Takashima S. Pulmonary function after lobectomy:
video-assisted thoracic surgery versus thoracotomy.
Ann Thorac Surg 2000;70:938–41.
[48] Landreneau RJ, Hazelrigg SR, Mack MJ, et al. Post-
operative pain-related morbidity: video-assisted thorac-
ic surgery versus thoracotomy. Ann Thorac Surg 1993;
56:1285–9.
[49] Nomori H, Horio H, Naruke T, Suemasu K. What is
the advantage of a thoracoscopic lobectomy over a
limited thoracotomy procedure for lung cancer sur-
gery? Ann Thorac Surg 2001;72:879–84.
[50] Nagahiro I, Andou A, Aoe M, Sano Y, Date H, Shi-
mizu N. Pulmonary function, postoperative pain, and
serum cytokine level after lobectomy: a comparison of
VATS and conventional procedure. Ann Thorac Surg
2001;72:362–5.
[51] DeCamp MM, Jaklitsch MT, Mentzer SJ, Harpole Jr
DH, Sugarbaker DJ. The safety and versatility of vid-
eo-thoracoscopy: a prospective analysis of 895 consec-
utive cases. J Am Coll Surg 1995;181:113–20.
[52] Landreneau RJ, Wiechmann RJ, Hazelrigg SR, Mack
MJ, Keenan RJ, Ferson PF. Effect of minimally inva-
sive thoracic surgical approaches on acute and chronic
postoperative pain. Chest Surg Clin N Am 1998;8:
891–906.
[53] Asaph JW, Keppel JF. Midline sternotomy for the treat-
ment of primary pulmonary neoplasms. Am J Surg
1984;147:589–92.
[54] Urschel Jr HC, Razzuk MA. Median sternotomy as a
standard approach for pulmonary resection. Ann
Thorac Surg 1986;41:130–4.
[55] Cooper JD, Nelems JM, Pearson FG. Extended indica-
tions for median sternotomy in patients requiring pul-
monary resection. Ann Thorac Surg 1978;26:413–20.
[56] Ali MK, Mountain CF, Ewer MS, Johnston D, Haynie
TP. Predicting loss of pulmonary function after pulmo-
nary resection for bronchogenic carcinoma. Chest
1980;77:337–42.
[57] Miller JI, Grossman GD, Hatcher DR. Pulmonary
function test criteria for operability and pulmonary
resection. Surg Gynecol Obstet 1981;153:893–5.
[58] Peeters-Asdourian C, Gupta S. Choices in pain man-
agement following thoracotomy. Chest 1999;115:
122S–4S.
[59] Eng J, Sabanathan S. Continuous extrapleural intercos-
tal nerve block and post-thoracotomy pulmonary com-
plications. Scand J Thorac Cardiovasc Surg 1992;26:
219–23.
[60] Miguel R, Hubbell D. Pain management and spirome-
try following thoracotomy: a prospective, randomized
study of four techniques. J Cardiothorac Vasc Anesth
1993;7:529–34.

I.B. Cetindag et al / Thorac Surg Clin 14 (2004) 317–323 323
[61] Kavanagh BP, Katz J, Sandler AN. Pain control after
thoracic surgery: a review of current techniques. An-
esthesiology 1994;81:737–59.
[62] Heerdt PM. Cardiovascular adaptation to lung resec-
tion. In: Kaplan JA, Slinger PD, editors. Thoracic
anesthesia. 3rd edition. Philadelphia: Churchill Living-
stone; 2003. p. 423–35.
[63] Hsia CC. Coordinated adaption of oxygen transport
in cardiopulmonary disease. Circulation 2001;104:
963–9.
[64] Nezu K, Kushibe K, Tojo T, et al. Recovery and limi-
tation of exercise capacity after lung resection for lung
cancer. Chest 1998;113:1511–6.

Thorac Surg Clin 14 (2004) 325–330
Acute postoperative compromise in cardiovascular function
after chest surgery
Joseph LoCicero III, MD
Department of Surgery, Center for Clinical Oncology, and Center for Interventional Technology, University of South Alabama,
2451 Fillingim Street, Mastin 719, Mobile, AL 36617, USA
Major chest operations place a significant strain recommend that pericardial defects, regardless of the
on all physiologic systems in the body. Strain on the
cardiovascular system can lead to the most serious
problems or even death. The problems are not limited
to ischemia, arrhythmias, or heart failure, but also
include cardiac herniation and hypertensive crisis.
Cardiac herniation
Unless promptly diagnosed and treated, cardiac
herniation can be a fatal complication of any lung
procedure. Although herniation most often occurs
after right pneumonectomy [1], it can occur after left
pneumonectomy [2] or even after lobectomy on either
side [3]. Small defects are the most dangerous.
Because of the rhythmic rocking of the heart, it
literally can jump through the defect. On the right
side, the superior and inferior vena cavae become
twisted, and blood return is severely compromised.
On the left side, the cavae are stretched and cause
diminished blood return. The patient immediately
becomes hypotensive, hypoxemic, tachypneic, and
tachycardic. Diagnostic tests should not be necessary,
but the characteristic chest radiograph confirms sus-
picions (Fig. 1) [4]. The patient should be turned with
the operative side up. The heart may return to the
normal position. Immediate return to the operating
room and repair of the pericardial defect is necessary.
If the patient is unstable, emergency thoracotomy in
the postanesthesia care unit may be necessary. To
prevent this devastating complication, most authors
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00020-9
E-mail address: [email protected]
defect size, should be closed with a prosthetic patch.
Arrhythmias
Postoperative cardiac arrhythmias and ischemia
are common problems after thoracotomy. Groves et al
[5] monitored the heart rates of 82 patients having a
major thoracotomy. They discovered that the number
of patients with silent myocardial ischemia doubled
after thoracotomy. Patients who had ischemia had an
average postoperative resting heart rate of 93 beats/
min as opposed to patients without ischemia who
had an average postoperative resting heart rate of
82 beats/min. The investigators noted 12% of patients
developed atrial arrhythmias, none of which were
associated with myocardial ischemia.
The treatment of postoperative arrhythmias is
controversial. A brief review of the most commonly
used medications is presented in Table 1 [6]. Ventricu-
lar arrhythmias are rare after thoracotomy, and the
treatment relies primarily on resuscitation of the
hemodynamically unstable patient. The principles of
correcting electrolyte abnormalities and oxygenation
deficits and ruling out myocardial ischemia should
be paramount for patients showing ventricular ectopy
or tachycardia.
For atrial tachyarrhythmia, when the diagnosis has
been established, the first priority is to assess hemo-
dynamic stability. If the patient experiences syncope
or if the blood pressure is less than 80 mmHg systolic,
synchronous electrical cardioversion should be per-
formed. The first shock typically is delivered at 200 J,
with subsequent shocks at 300 J and 360 J. Conscious
s reserved.
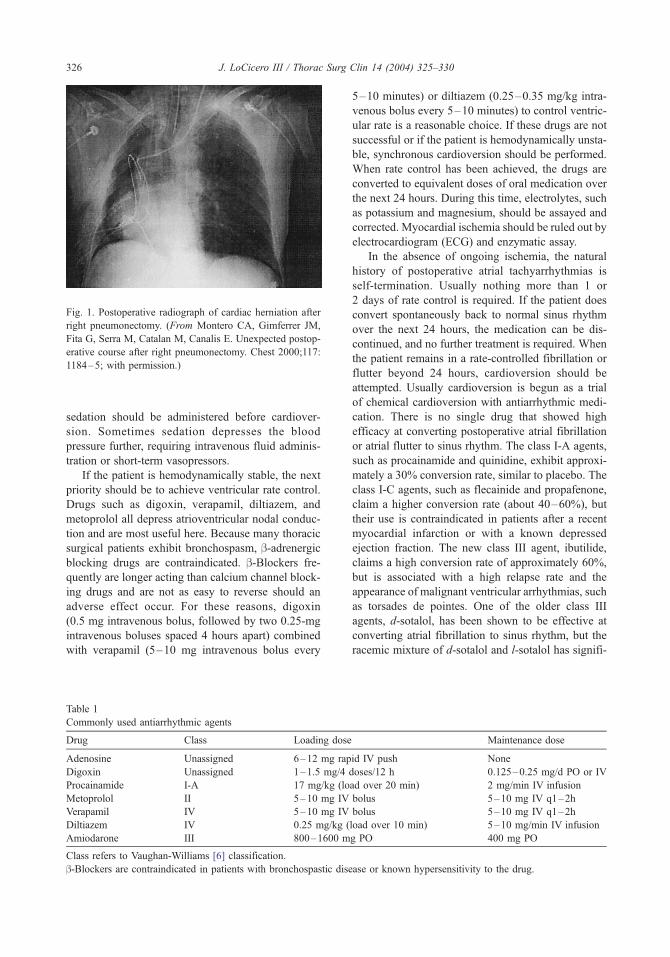
Fig. 1. Postoperative radiograph of cardiac herniation after
right pneumonectomy. (From Montero CA, Gimferrer JM,
Fita G, Serra M, Catalan M, Canalis E. Unexpected postop-
erative course after right pneumonectomy. Chest 2000;117:
1184–5; with permission.)
J. LoCicero III / Thorac Surg Clin 14 (2004) 325–330326
sedation should be administered before cardiover-
sion. Sometimes sedation depresses the blood
pressure further, requiring intravenous fluid adminis-
tration or short-term vasopressors.
If the patient is hemodynamically stable, the next
priority should be to achieve ventricular rate control.
Drugs such as digoxin, verapamil, diltiazem, and
metoprolol all depress atrioventricular nodal conduc-
tion and are most useful here. Because many thoracic
surgical patients exhibit bronchospasm, b-adrenergicblocking drugs are contraindicated. b-Blockers fre-
quently are longer acting than calcium channel block-
ing drugs and are not as easy to reverse should an
adverse effect occur. For these reasons, digoxin
(0.5 mg intravenous bolus, followed by two 0.25-mg
intravenous boluses spaced 4 hours apart) combined
with verapamil (5–10 mg intravenous bolus every
Table 1
Commonly used antiarrhythmic agents
Drug Class Loading dose
Adenosine Unassigned 6–12 mg rap
Digoxin Unassigned 1–1.5 mg/4
Procainamide I-A 17 mg/kg (lo
Metoprolol II 5–10 mg IV
Verapamil IV 5–10 mg IV
Diltiazem IV 0.25 mg/kg (
Amiodarone III 800–1600 m
Class refers to Vaughan-Williams [6] classification.
b-Blockers are contraindicated in patients with bronchospastic dise
5–10 minutes) or diltiazem (0.25–0.35 mg/kg intra-
venous bolus every 5–10 minutes) to control ventric-
ular rate is a reasonable choice. If these drugs are not
successful or if the patient is hemodynamically unsta-
ble, synchronous cardioversion should be performed.
When rate control has been achieved, the drugs are
converted to equivalent doses of oral medication over
the next 24 hours. During this time, electrolytes, such
as potassium and magnesium, should be assayed and
corrected. Myocardial ischemia should be ruled out by
electrocardiogram (ECG) and enzymatic assay.
In the absence of ongoing ischemia, the natural
history of postoperative atrial tachyarrhythmias is
self-termination. Usually nothing more than 1 or
2 days of rate control is required. If the patient does
convert spontaneously back to normal sinus rhythm
over the next 24 hours, the medication can be dis-
continued, and no further treatment is required. When
the patient remains in a rate-controlled fibrillation or
flutter beyond 24 hours, cardioversion should be
attempted. Usually cardioversion is begun as a trial
of chemical cardioversion with antiarrhythmic medi-
cation. There is no single drug that showed high
efficacy at converting postoperative atrial fibrillation
or atrial flutter to sinus rhythm. The class I-A agents,
such as procainamide and quinidine, exhibit approxi-
mately a 30% conversion rate, similar to placebo. The
class I-C agents, such as flecainide and propafenone,
claim a higher conversion rate (about 40–60%), but
their use is contraindicated in patients after a recent
myocardial infarction or with a known depressed
ejection fraction. The new class III agent, ibutilide,
claims a high conversion rate of approximately 60%,
but is associated with a high relapse rate and the
appearance of malignant ventricular arrhythmias, such
as torsades de pointes. One of the older class III
agents, d-sotalol, has been shown to be effective at
converting atrial fibrillation to sinus rhythm, but the
racemic mixture of d-sotalol and l-sotalol has signifi-
Maintenance dose
id IV push None
doses/12 h 0.125–0.25 mg/d PO or IV
ad over 20 min) 2 mg/min IV infusion
bolus 5–10 mg IV q1–2h
bolus 5–10 mg IV q1–2h
load over 10 min) 5–10 mg/min IV infusion
g PO 400 mg PO
ase or known hypersensitivity to the drug.

J. LoCicero III / Thorac Surg Clin 14 (2004) 325–330 327
cant b-blocking activity and is relatively contraindi-
cated in thoracic surgical patients.
Despite its relative lack of efficacy, the most often
used and recommended drug for chemical cardiover-
sion is procainamide. It is easy to give a loading dose
(17 mg/kg intravenously over 20 minutes), has rela-
tively few acute limiting side effects (hypotension,
nausea), and is quickly metabolized. In contrast to
quinidine, which has anticholinergic side effects, pro-
cainamide has some antiadrenergic effects and can
‘‘double’’ as an atrioventricular nodal blocking drug.
When the patient has been given a loading dose of
procainamide, he or she is started on a continuous
infusion of 2 to 4 mg/min. If the patient is taking oral
medications, Procanbid (Monarch Pharmaceuticals,
Bristol, Tennessee) can be started by mouth when
the loading dose is completed. The infusion is
stopped after the second oral dose.
Although used mainly for ventricular arrhythmias,
amiodarone is increasingly popular for rate control in
atrial tachyarrhythmias. After acute intravenous dos-
ing in humans, amiodarone may have a mild negative
inotropic effect. After oral dosing, however, amiodar-
one produces no significant change in left ventricular
ejection fraction, even in patients with depressed left
ventricular ejection fraction. Amiodarone increases
the cardiac refractory period without influencing rest-
ing membrane potential except in automatic cells, in
which the slope of the prepotential is reduced, gen-
erally reducing automaticity. These electrophysiologic
effects are reflected in a decreased sinus rate of 15%
to 20%, increased P-R and QT intervals of about 10%,
development of U waves, and changes in T-wave
contour. Rarely, QT prolongation has been associated
with worsening of arrhythmia. Amiodarone has
many potential side effects, including pulmonary
toxicity, worsening arrhythmias, liver failure, and loss
of vision.
Myocardial infarction
Perhaps the most feared postoperative complica-
tion is a myocardial infarction. The World Health
Organization definition of myocardial infarction re-
quires two of the following three conditions be met:
(1) symptoms, (2) myocardial enzyme release, and
(3) compatible ECG changes. This definition poses a
dilemma, however, to categorize the many postopera-
tive patients who exhibit myocardial enzyme release
but are devoid of symptoms or ECG changes. Most
clinicians consider a significant enzyme release as a
myocardial infarction despite the failure to meet strict
criteria. Several conditions may result in the release
of troponin, including blunt myocardial trauma, aortic
dissection, pulmonary embolism, esophageal rupture,
peptic ulcer disease, pancreatitis, and cholecystitis.
Unstable angina, non–ST segment elevation myo-
cardial infarctions, and ST segment elevation myocar-
dial infarctions represent a continuum of degree of
coronary artery occlusion and amount of myocardial
necrosis, with ST segment elevation infarctions rep-
resenting 100% occlusions and significant necro-
sis. ST segment elevation myocardial infarctions
usually are treated aggressively with aspirin, oxygen,
b-blockers, morphine, intravenous nitroglycerin, and
early cardiac catheterization with percutaneous inter-
vention. These myocardial infarctions are exceedingly
rare in the postoperative patient. For acute non–ST
segment elevation myocardial infarctions and unstable
angina, the treatment is largely medical, only rarely
requiring urgent percutaneous intervention. The risks
of hemorrhage in the surgical patient must be weighed
against the potential benefits of each therapy to make
an informed decision as to which treatments to use.
Several randomized trials have shown the benefits
of aspirin in unstable coronary syndromes with a
relative risk reduction of death or myocardial infarc-
tion of more than 50% by the Research on Instability
in Coronary Artery Disease (RISC) study group in
1990 [7]. A meta-analysis of six randomized trials by
Oler et al in 1996 [8] showed that patients treated
with a combination of aspirin and heparin had a
33% reduction in death or myocardial infarction com-
pared with patients treated with aspirin alone. A meta-
analysis by Yusuf et al [9] showed a 13% reduction in
the progression to acute myocardial infarction with
the use of these agents in unstable angina.
Low-molecular-weight heparins have several ad-
vantages over conventional unfractionated heparin,
including ease of subcutaneous administration, reli-
able bioavailability and anticoagulant effect, lower
rates of heparin-induced thrombocytopenia, and de-
creased sensitivity to platelet factor 4 inhibition.
These agents inhibit thrombin and possess potent
anti–factor Xa activity. The largest studies to date in
patients with unstable angina/non–ST segment eleva-
tion myocardial infarctions, ESSENCE (Efficacy and
Safety of Subcutaneous Enoxaparin in Non-Q Wave
Coronary Events) with 3171 patients [10] and throm-
bolysis in myocardial infarction (TIMI) IIB with
4020 patients [11], found that the primary end points
of death, myocardial infarction, or recurrent ischemia
are reduced significantly with enoxaparin compared
with unfractionated heparin. In the ESSENCE trial,
the 30-day end point was reached in 19.8% in the
enoxaparin group compared with 23.3% in the unfrac-

J. LoCicero III / Thorac Surg Clin 14 (2004) 325–330328
tionated heparin group (P = .016). In TIMI IIB, there
was a 15% relative risk reduction in the primary end
point at 14 days (P = .03).
Glycoprotein IIb/IIIa inhibitors have been shown
to be useful in acute coronary syndromes. These
agents inhibit platelet aggregation, reducing distal
embolization and preventing subsequent myocardial
infarctions. They also display late benefit (3 years),
which may be due to anti-inflammatory properties
caused by inhibition of MAC-1 on white blood cells
and by plaque stabilization, which reduce long-term
target vessel revascularization. These agents reduce
adverse cardiac events by 22% to 56% at 30 days in
high-risk and low-risk patients undergoing percuta-
neous coronary interventions. In patients with acute
coronary syndromes not undergoing percutaneous
interventions, there is more modest evidence of bene-
fit with these agents.
b-Blockers also have been shown to improve
mortality in acute coronary syndrome patients. In
the ISIS-1 (First International Study of Infarct Sur-
vival) trial, 16,027 patients were randomized to
receive intravenous atenolol, 5 to 10 mg, followed
by oral atenolol, 100 mg daily [12]. The atenolol
patients had a 7-day reduction in mortality from 4.3%
to 3.7%. Another study showing the benefits of
b-blockers in acute myocardial infarction was the
MIAMI (Metoprolol in Acute Myocardial Infarction)
trial, in which more than 5700 patients were random-
ized to receive intravenous metoprolol, 15 mg or less,
followed by oral metoprolol or placebo [13]. The
b-blocker patients had a 13% reduction in mortality
at 15 days. Compared with aspirin, heparin, and
b-blockers, there is no clear mortality benefit associ-
ated with use of nitroglycerin.
The goals of managing patients who have had
demand myocardial infarctions either before or after
operation are simple: decrease myocardial oxygen
demand, and increase myocardial oxygen supply.
The simplest and most effective way to decrease
demand is to decrease heart rate and blood pressure
using b-blockers. The mortality benefits of this agent
were discussed previously. It also is important to pay
attention to the intravascular volume status of the
postoperative patient because increased filling pres-
sures can cause increased oxygen demand and lead
to increased catecholamine levels, creating a vicious
cycle. Another factor that significantly increases myo-
cardial oxygen demand is fever. Elevation of the body
temperature by 2�C can result in an increase of energy
consumption of greater than 20% as reported by
Kluger et al [14]. Standing doses of antipyretics should
be considered in a patient with a recent myocardial
infarction (or stroke) in whom fever is present.
Hypertension
Perioperative hypertension is especially important
because of the potential for producing myocardial
ischemia. Weitz [15] noted that perioperative hyper-
tension or hypotension occurs in 25% of hyper-
tensive patients who undergo surgery. Hypertensive
events occur most frequently in patients with a resting
diastolic blood pressure greater than 110 mm Hg
undergoing carotid, abdominal aortic, peripheral
vascular, intraperitoneal, or intrathoracic surgeries.
A multivariate analysis performed by Browner et al
[16] in male veterans after thoracic surgery found
a 3.8 odds ratio for postoperative death in hyperten-
sive patients compared with normotensive patients.
Other data are conflicting, however. A prospective
randomized multicenter study by Forrest et al [17]
of more than 17,000 patients found that preopera-
tive hypertension was associated with bradycardia,
tachycardia, and hypertension but had no impact
on mortality.
Weitz [15] noted that perioperative hypertension
tends to occur at four different times: (1) during
intubation and induction of anesthesia (owing to
sympathetic stimulation with adrenergic mediated
vasoconstriction); (2) intraoperatively secondary to
pain; (3) early postoperatively secondary to pain,
hypothermia, hypoxia, and volume overload or hypo-
volemia; and (4) 24 to 48 hours postoperatively as
fluid is immobilized. Hypertension often occurs with-
in 48 hours of stopping preoperative antihypertensive
agents and sedatives. b-Blocker withdrawal some-
times occurs 4 days postoperatively, however.
The treatment of perioperative hypertension
depends on the cause. If hypertension occurs during
intubation, surgical incision, or emergence from
anesthesia, it often is due to increased sympathetic
tone, and the treatment is generally short-acting
b-blockers or narcotics. If the hypertension occurs 24
to 96 hours postoperatively, the preoperative anti-
hypertensives should be restarted as a first line of
therapy. Prevention is paramount. Often long-acting
preparations can be given before surgery, or if an
extended period of bowel rest is expected postopera-
tively, standing intravenous antihypertensive therapy
should be considered. It generally is indicated to
continue the outpatient antihypertensive regimen
throughout the perioperative period, especially with
regard to b-blockers and clonidine because these
medications tend to cause the most severe with-
drawal reactions. Lastly, congestive heart failure is
a frequent cause of postoperative hypertension. A
combination of nitrates and diuretics is effective first-
line therapy.

J. LoCicero III / Thorac Surg Clin 14 (2004) 325–330 329
Heart failure
Chronic heart failure
Chronic heart failure usually is known preopera-
tively, and the patient can be prepared well in advance
of the surgery to be in optimal condition. The usual
maneuvers of judicial fluid administration, afterload
reduction, rate control, and use of inotropic agents
help most patients through the postoperative period.
According to data on perioperative congestive
heart failure in the 1950s and 1960s, most exacerba-
tion of heart failure developed within 1 hour of
cessation of anesthesia; this was due to a combination
of hypertension/hypotension, ischemia, intraoperative
fluid administration, sympathetic stimulation, ces-
sation of positive-pressure ventilation, and hypoxia.
According to Weitz [15], a second peak occurred
between 24 and 48 hours and may be related to
the reabsorption of interstitial fluid, myocardial is-
chemia, and possibly withdrawal of long-term oral
medications. Insertion of a pulmonary artery cathe-
ter perioperatively is controversial. In January 2003,
Sandham et al reported a randomized trial in 1994
high-risk elderly patients undergoing major surgery
[18]. In-hospital mortality at 6 months and at
12 months did not differ appreciably between the
two groups. The only significant difference obtained
was the development of pulmonary embolism in eight
patients with a pulmonary artery catheter versus none
in the standard care group (P = .004). Another
interesting finding was a trend toward improved
survival in New York Heart Association class III or
class IV patients, although the number of patients in
this category was small.
The appropriate course of action depends on the
cause, with a crucial distinction made between acute
management and long-term therapy. To understand
this distinction better, one needs to understand the
neurohumoral paradigm for treating chronic heart
failure patients. When the heart is failing, many
neurohormones circulate at high levels, which help
the body maintain perfusion of the brain and organs.
In the short-term, this circulation of neurohormones
conveys a survival benefit by maintaining an ade-
quate cardiac output and blood pressure. These neu-
rohormones are toxic to the heart over the long run,
resulting in fibrosis, apoptosis, and remodeling, while
increasing the myocardial propensity to fibrillate.
Examples of these potentially toxic substances in-
clude angiotensin 2, aldosterone, epinephrine, and
possibly endothelin. The majority of the medications
used in chronic heart failure are antagonists of the
above-mentioned toxins. Angiotensin-converting en-
zyme inhibitors are used not only for their benefits in
afterload reduction; but rather as general inhibitors of
the generation of angiotensin II. Hydralazine is a
much more potent afterload reducer, but it lacks the
antitoxin effects of the aforementioned agents and has
little, if any, mortality benefits.
The neurohumoral paradigm is in contradistinction
to acute heart failure management theory. Here the
paradigm is a simple pump theory. The pump theory
treats the heart as a pump, which is affected by preload,
inotropy and afterload. The first step in managing
heart failure in the perioperative period is to identify
destabilizing factors, such as fluid overload, anemia,
or fever, and remedy these if possible. The next step
is simple pump theory with various medical and
mechanical tools at the clinician’s disposal.
Nitroglycerin is a potent preload reducer that
works by venodilation. Other agents that reduce pre-
load include diuretics (including hemodialysis) and
positive-pressure ventilation, including biphasic posi-
tive airway pressure.
Digoxin is too weak to be considered an inotrope
in the acute management phase. Dobutamine, a non-
selective b-agonist, is a potent inotrope and an
afterload reducer. Dopamine also is a nonselective
b-agonist in doses of 5 to 10 mg/kg/min. Dopamine
tends to increase afterload, however, due to its
a1-agonist activity, making it a less desirable agent
in acute heart failure. Milrinone, a phosphodiesterase
inhibitor, is a potent inotrope and an afterload reducer.
Diuretics also decrease afterload.
Nitroprusside is the most potent afterload reducer.
This agent must be used with caution and usually
with an arterial line because of its ability to cause
severe hypotension. Additionally, thiocyanate levels
should be checked in all patients taking this drug for
more than 24 hours, especially in patients with renal
failure. Hydralazine is another suitable pure afterload-
reducing agent, which can be given intravenously or
orally. Nesiritide is a recombinant human brain type
of natriuretic peptide, which acts as a venodilator and
arterial dilator and a diuretic. Additionally, this agent
antagonizes the renin-angiotensin-aldosterone system
and the sympathetic nervous system.
Acute right heart failure
Large pulmonary resections may produce acute
right heart failure even in patients who are thought to
have normal ventricular function before operation.
The small pulmonary bed may limit the flow of blood
out of the right heart producing pulmonary hyperten-
sion and increased right ventricular afterload. In some
cases, patients develop significant pulmonary edema,

J. LoCicero III / Thorac Surg Clin 14 (2004) 325–330330
which increases the pulmonary resistance. Positive-
pressure ventilation may limit the pulmonary edema,
but also may increase right heart strain. Inhaled nitric
oxide has not shown long-term success in adults.
Drugs that reduce pulmonary artery pressure may
be beneficial, however, such as nitroprusside, nitro-
glycerin, prostacyclin, and iloprost. Galie et al [19]
reviewed three trials showing efficacy of the prosta-
cyclin analogues. Specifically, inhaled iloprost im-
proved symptoms, exercise capacity, and clinical
events in patients with pulmonary hypertension and
inoperable chronic thromboembolic pulmonary hy-
pertension. Although none of the studies involved
critically ill patients, the favorable effects of prosta-
noids observed in all studies coupled with different
profiles of adverse events and tolerability for each
prostacyclin analogue allow the unique opportunity
to select the most appropriate compound for the
individual patient with pulmonary hypertension.
Summary
Attention to preoperative cardiovascular risk fac-
tors, appropriate preparation, early recognition, and
treatment are essential to prevent potential cata-
strophic cardiac events from leading to life-threaten-
ing situations in the postoperative period.
References
[1] Shimizu J, Ishida Y, Hirano Y, et al. Cardiac herniation
following intrapericardial pneumonectomy with partial
pericardiectomy for advanced lung cancer. Ann Thorac
Cardiovasc Surg 2003;9:68–72.
[2] Hidvegi RS, Abdulnour EM, Wilson JA. Herniation
of the heart following left pneumonectomy. J Can
Assoc Radiol 1981;32:185–7.
[3] Ohri SK, Siddiqui AA, Townsend ER. Cardiac tor-
sion after lobectomy with partial pericardectomy. Ann
Thorac Surg 1992;53:703–5.
[4] Montero CA, Gimferrer JM, Fita G, Serra M, Catalan
M, Canalis E. Unexpected postoperative course after
right pneumonectomy. Chest 2000;117:1184–5.
[5] Groves J, Edwards ND, Carr B, Sherry KM. Periopera-
tive myocardial ischemia, heart rate and arrhythmia
in patients undergoing thoracotomy, an observational
study. Br J Anaesth 1999;83:850–4.
[6] Vaughan Williams EM. A classification of antiarrhyth-
mic actions reassessed after a decade of new drugs.
J Clin Pharmacol 1984;24:129–47.
[7] RISC Group. Risk of myocardial infarction and death
during treatment with low dose aspirin and intravenous
heparin in men with unstable coronary artery disease.
Lancet 1990;336:827–30.
[8] Oler A, Whooley MA, Oler J, Grady D. Adding hepa-
rin to aspirin reduces the incidence of myocardial
infarction and death in patients with unstable angina:
a meta-analysis. JAMA 1996;276:811–5.
[9] Yusuf S, Wittes J, Friedman L. Overview of results
of randomized clinical trials in heart disease: 2. un-
stable angina, heart failure, primary prevention with
aspirin, and risk factor modification. JAMA 1988;260:
2088–93.
[10] Goodman SG, Cohen M, Bigonzi F, et al. Randomized
trial of low molecular weight heparin (enoxaparin) ver-
sus unfractionated heparin for unstable coronary artery
disease: one-year results of the ESSENCE Study. Effi-
cacy and Safety of Subcutaneous Enoxaparin in Non-Q
Wave Coronary Events. J Am Coll Cardiol 2000;36:
693–8.
[11] Cohen M, Theroux P, Weber S, et al. Combination
therapy with tirofiban and enoxaparin in acute coro-
nary syndromes. Int J Cardiol 1999;71:273–81.
[12] Randomised trial of intravenous atenolol among 16
027 cases of suspected acute myocardial infarction:
ISIS-1. First International Study of Infarct Survival
Collaborative Group. Lancet 1986;2:57–66.
[13] Metoprolol in Acute Myocardial Infarction. Patients
and methods. The MIAMI Trial Research Group. Am
J Cardiol 1985;56:3G–9G.
[14] Kluger MJ, Kozak W, Conn CA, Leon LR, Soszynski
D. The adaptive value of fever. Infect Dis Clin N Am
1996;10:1–20.
[15] Weitz HH. Perioperative cardiac complications. Med
Clin North Am 2001;85:1151–69.
[16] Browner WS, Li J, Mangano D. In-hospital and long-
term mortality in male veterans following noncardiac
surgery. The Study of Peioperative Ischemia Research
Group. JAMA 1992;268:228–32.
[17] Forrest JB, Rehder K, Cahalan MK, et al. Multicenter
study of general anesthesia: III. predictors of severe
perioperative adverse outcomes [erratum in Anesthe-
siology 1992 Jul;77(1):222]. Anesthesiology 1992;76:
3–15.
[18] Sandham JD, Hull RD, Brant RF, Knox L, Pineo GF,
Doig CJ, et al. Canadian Critical Care Clinical Trials
Group: A randomized, controlled trial of the use of
pulmonary-artery catheters in high-risk surgical pa-
tients. N Engl J Med 2003 Jan 2;348(1):5–14.
[19] Galie N, Manes A, Branzi A. Prostanoids for pulmo-
nary arterial hypertension. Am J Respir Med 2003;2:
123–37.

Thorac Surg Clin 14 (2004) 331–343
Shoulder function after thoracic surgery
Wilson W.L. Li, MSc, T.W. Lee, FRCS,Anthony P.C. Yim, MD, FRCS, FACS, FCCP, FHKAM*
Division of Cardiothoracic Surgery, Department of Surgery, The Chinese University of Hong Kong, Prince of Wales Hospital,
Shatin, NT, Hong Kong SAR, China
For most thoracic procedures, posterolateral tho- ability to use the upper extremity depends on the
racotomy (PLT) has long been the standard surgical
approach. This incision provides excellent access into
the chest cavity, but it may require the division of
several major chest wall muscles and spreading of the
ribs. Experience has shown that this incision may lead
to serious postoperative morbidity, including chronic
pain, compromised pulmonary function, and restric-
tion of shoulder function [1,2]. The disabling effect of
thoracic surgery on shoulder function is a commonly
overlooked and rarely accurately investigated compli-
cation. Proper shoulder function is a prerequisite,
however, for effective arm and hand function and
for performing multiple tasks involving mobility,
ambulation, and activities of daily living [3]. Postop-
erative shoulder dysfunction is an important factor in
determining return to normal preoperative functioning
and could become a serious long-term disability if
neglected. This article describes the common causes
of shoulder dysfunction after thoracic surgery, the
available data on postoperative shoulder dysfunction
comparing different access modalities, and the poten-
tial contribution of upper extremity revalidation for
the postoperative recovery course.
Causes of postoperative shoulder dysfunction
The shoulder is composed of the glenohumeral
joint and scapulothoracic articulation and is served by
various muscles, together providing the complex
movements of the human upper limb [4]. A person’s
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00021-0
* Corresponding author.
E-mail address: [email protected] (A.P.C. Yim).
strength and range of motion (ROM) of the shoulder,
both of which could be affected by pain [3]. Shoulder
dysfunction after thoracotomy is a frequently encoun-
tered complication in the early postoperative period
[1,2,5–8]. Although the exact prevalence has not
been defined, it has been reported that disability in
shoulder function occurs in 10% to 26% of the pa-
tients in the first year after surgery [9]. More than
1 year after thoracotomy, 15% to 33% of patients still
experience subjective restriction of ipsilateral shoul-
der function [9,10].
It has never been investigated whether shoulder
dysfunction occurs disproportionately more often
after thoracic surgery compared with other surgical
specialties. Nevertheless, postoperative shoulder dys-
function after other nonthoracic surgical procedures
directly affecting the chest wall and shoulder area
seems to be common. In breast cancer surgery, radi-
cal mastectomy removes the breast along with the
underlying pectoralis major and pectoralis minor
muscles. It is well established that this procedure is
associated with considerable early and late postoper-
ative impairment of shoulder ROM and shoulder
strength. Axillary dissection, potentially complicated
with lymphedema, further worsens postoperative
shoulder function [11–13]. Even with muscle-spar-
ing techniques, 2% to 51% of patients after surgical
treatment of early-stage breast cancer have long-
term impairment of shoulder ROM [14], and 17%
to 33% of patients have prolonged decreased shoul-
der strength [14]. Significant correlation has been
found in this group of patients between upper limb
morbidity and poorer quality of life [14]. In cardiac
surgery, it has been reported that 1.5% to 24% of
patients undergoing median sternotomy experience
s reserved.

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343332
brachial plexus injury, significantly affecting postop-
erative shoulder function [15–20]. It is believed that
this injury is caused by compression of the brachial
plexus secondary to sternal retraction [15–20], es-
pecially when internal mammary artery harvesting
occurs [19,20]. Additionally, median sternotomy can
cause first rib fractures, which also could be associ-
ated with brachial plexus injury [15,16,20]. In con-
trast, shoulder dysfunction after surgical procedures
not affecting the chest wall or shoulder area is rare.
Reported cases are sporadic and are related mainly
to peripheral nerve injury [21–23]. Retrospective
studies have reported that the incidence of upper
extremity nerve palsies after total hip arthroplasty
was only 0.15% to 0.22% [22,23].
It seems that shoulder dysfunction after surgical
procedures directly affecting the chest wall or shoul-
der area and shoulder dysfunction after surgical
procedures not affecting the chest wall or shoulder
area are two separate entities. Shoulder dysfunction
after the latter is rare. It is caused almost solely by
peripheral nerve injuries, frequently as a result of im-
proper patient positioning [21–23], and has an ex-
cellent chance of full functional recovery [22–24].
Shoulder dysfunction after thoracotomy or breast
cancer surgery is far more common and often be-
comes a long-term complication [9,10,14]. Various
aspects of thoracic procedures can contribute to
postoperative shoulder dysfunction, including posi-
tioning of the patient, muscle division, injury to the
long thoracic nerve, and postoperative pain.
Positioning of the patient
Most patients undergoing thoracic surgery need to
be placed in a full lateral decubitus position. This
includes all PLTs, lateral thoracotomies, and video-
assisted thoracic surgery (VATS) procedures. The
operating table should be flexed at the level of the
nipples, to widen the intercostal spaces on the oper-
ated side. Especially with VATS procedures, this sim-
ple procedure could render excessive rib retraction
unnecessary, potentially reducing postoperative pain
[25,26]. Anterolateral and axillary thoracotomies
usually require the patient to be in a supine position,
with the side to be operated tilted at 30� to 45�.Whether in full lateral decubitus position or su-
pine position, shoulder abduction greater than 90�should be avoided at all times to prevent brachial
plexus neuropathy [27–30]. In addition, in the full
lateral decubitus position, chest rolls should be placed
under the ‘‘down-side’’ lateral thorax, potentially
decreasing the risk of brachial plexus neuropathy
in the down arm [28]. Regardless of the position,
attention should be given to potential pressure areas.
After placing the arms in a comfortable position, care
should be taken to ensure that both ulnar nerves are
protected from pressure damage to prevent periopera-
tive ulnar nerve injury.
Improper positioning of the upper extremity of the
patient can lead to peripheral nerve injuries and
frozen shoulder syndrome, limiting postoperative
shoulder function [21,28–31]. The exact contribution
of patient malpositioning to shoulder dysfunction
after thoracic procedures has not been investigated.
Nevertheless, proper positioning of the patient is im-
perative in all surgical procedures to reduce the oc-
currence of perioperative neuropathies [28,29]. Ulnar
neuropathy is the most common perioperative nerve
injury, followed by lesions of the brachial plexus
[21,30,31]. Particularly brachial plexus neuropathy
could affect postoperative shoulder function severely,
causing decreased muscle strength of shoulder and
arm, shoulder pain, and numbness and abnormal
sensations of the shoulder area [27]. It has been
suggested that lesions at the brachial plexus are likely
to be stretch induced [27–30]. Several positions of
the upper extremity have been associated with an
increased risk for brachial plexus neuropathy, includ-
ing shoulder depression, shoulder abduction greater
than 90�, lateral rotation of the arm, full elbow ex-
tension, forearm supination, and lateral flexion of
the patient’s head to the opposite site [27–30]. The
American Society of Anesthesiologists has formulated
empirically based recommendations on patient posi-
tioning to prevent some of these positions [28]. These
position strategies are proposed mainly for the supine
or prone position, however, and essentially are estab-
lished based on expert opinion rather than evidence-
based data. Whether these protective measures are
truly effective in preventing perioperative peripheral
neuropathies needs to be evaluated. The relevance of
these position strategies for patients in the full lateral
decubitus position needs to be investigated further.
Muscle division
The shoulder girdle is served by various muscles,
together providing stability and the complex move-
ments of the human upper limb [4]. Depending on the
chosen approach of chest entry, several of the shoul-
der girdle muscles have to be divided (Table 1).
PLT is the standard thoracic incision for most
major procedures on lung, esophagus, and other
posterior mediastinal structures. It requires the divi-
sion of the lateral edges of the lower part of the
trapezius at the back of the incision and a large section
of the lattisimus dorsi in the front. The latissimus dorsi

Table 1
Standard thoracic incisions and shoulder girdle muscle division
Thoracic incision Muscles divided
Approximate length
of incision (cm) Rib spreading
Posterolateral thoracotomy Trapezius (lateral edge
of lower portion)
15–30 Yes
Lattisimus dorsi
Serratus anterior
Muscle-sparing thoracotomy None 8–20 Yes
Anterolateral thoracotomy Pectoralis major 8–20 Yes
Pectoralis minor
Serratus anterior
Axillary thoracotomy None 6–15 Yes
Median sternotomy None 15–25 Sternum spreading
VATS (utility thoracotomy) Lattisimus dorsi 6–10 No
Serratus anterior
Table 2
Direct actions of shoulder girdle muscles affected by
thoracic surgery
Muscle divided Supported shoulder girdle action
Lattisimus dorsi Upper arm
Adduction
Extension
Internal rotation
Accessory breathing muscle
Serratus anterior Scapula
Protraction
Upward rotation
Fixation of scapula against
thoracic wall
Trapezius (lower portion) Scapula
Static support
Retraction
Pectoralis major Upper arm
Adduction
Flexion
Internal rotation
Accessory breathing muscle
Pectoralis minor Scapula
Protraction
Downward rotation
From Halder AM, Itoi E, An KN. Anatomy and biome-
chanics of the shoulder. Orthop Clin North Am 2000;31:
159–76; with permission.
W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343 333
muscle is divided at the level of the skin incision, and
the vascular pedicles are cauterized carefully. The
inferior portion of the muscle is denervated. The
serratus anterior muscle is divided in a slightly inferior
level to preserve the innervation of its main bulk. The
serratus anterior occasionally can be spared (as in a
lateral thoracotomy), although transection is impor-
tant for a wider exposure of the chest cavity. Most of
these muscles have no unique line of action (Table 2)
[4]. The latissimus dorsi is the main adductor of
the shoulder, but also functions as an extensor and
internal rotator. Its innervation is supplied by the tho-
racodorsal nerve. When the arm is fixed, the latis-
simus dorsi also can raise the lower ribs, acting as
an accessory breath muscle. The serratus anterior,
innervated by the long thoracic nerve, protracts and
upwardly rotates the scapula. It keeps the scapula
applied to the thoracic wall and maintains the stabil-
ity of the scapula during arm elevation and pushing
[32–34]. Of the trapezius muscle, usually only the
lateral edges of the ascending part is divided, respon-
sible for depression and static support of the scapula.
It is reasonable to assume that dividing one or more
of these muscles could affect significantly postopera-
tive shoulder strength and ROM in various directions.
Preservation of major chest wall muscles repeatedly
has been suggested to preserve postoperative shoulder
ROM and shoulder strength in various types of mus-
cle-sparing thoracotomies [1,2,7,35–39]. Alternative,
less invasive access modalities include anterolateral
thoracotomy, axillary thoracotomy [39–42], ausculta-
tory triangle thoracotomy [36,37], and muscle-sparing
PLT [1,7,35].
The lateral (muscle-sparing) thoracotomy is the
only real substitute for PLT. The consistent difference
between PLT and muscle-sparing thoracotomy is the
preservation of the latissimus dorsi and serratus ante-
rior muscles. Location, length of incision, and amount
of rib spreading are similar [1,2,7,35]. Various modi-
fications exist with different skin incisions. One
common incision is a transverse one, which starts
from the anterior axillary line to below the scapular
tip. Soft tissue is dissected to facilitate posterior
mobilization of the latissimus dorsi and preservation

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343334
of the long thoracic neurovascular bundle. The serra-
tus anterior is split along its fibers over the selected
intercostal space. The intercostal muscles are divided
well beyond the incision to allow maximal rib spread-
ing. This incision is as versatile as PLT in experienced
hands, but not for most surgeons on most common
procedures because the operative field can be reduced
greatly [1,7,35,38]. Although studies have reported
significant benefits regarding postoperative shoulder
dysfunction with muscle-sparing techniques [1,2,7,
37,38], the exact contribution and importance of
division of each shoulder girdle muscles have not
been elucidated properly [39].
With VATS procedures, only a minithoracotomy
is necessary for retrieval of the specimen. The inci-
sion is placed over the fourth intercostal space in
the anterolateral chest and generally is 6 to 8 cm in
length. In this location, only a small portion, if any, of
the latissimus dorsi muscle needs to be divided,
whereas the serratus anterior muscle is split along
the direction of its fibers [26]. Differences between
VATS and the more traditional thoracotomy include
the length of the incision and amount of muscle
division and, more importantly, the avoidance of rib
spreading. It has been reported that VATS patients
experience significantly less early postoperative
shoulder dysfunction compared with PLT patients
[5,6,8,9]. Whether VATS is associated with less
shoulder dysfunction compared with muscle-sparing
thoracotomy needs to be investigated.
In addition to muscle division, it has been reported
that PLT causes postoperative atrophy of the latissi-
mus dorsi and serratus anterior, objectified by CT
[43]. This phenomenon most likely is caused by
denervation of these muscles [44]. It is unclear,
however, whether these radiologic findings correlate
with significant postoperative shoulder dysfunction.
Injury of the long thoracic nerve
Perioperative injury to the long thoracic nerve is
an uncommon, but important and easily avoidable
cause of shoulder dysfunction after thoracic surgery
[32–34]. Perioperative injury to the long thoracic
nerve can result in serious postoperative shoulder
dysfunction through weakness or paralysis of the
serratus anterior muscle. Subsequent scapular wing-
ing and loss of scapular rotation cause inability to flex
or abduct the shoulder fully [32–34,45,46] and
potentially disabling limitation of activities of daily
living [33].
The long thoracic nerve is a pure motor nerve,
innervating the serratus anterior muscle. It originates
from the anterior branches of the fifth, sixth, and sev-
enth cervical roots. The fifth and sixth roots, along
with the dorsal nerve of the scapula, pass across the
fibers of the scalenus medius muscle, whereas the
seventh cervical root passes anteriorly. The nerve runs
from behind the clavicle to reach the first rib, and from
there it descends along the lateral wall of the thorax
down to the eighth and ninth ribs to supply the serratus
anterior muscle with nerves.
The nerve’s long and superficial course makes it
susceptible to damage at various levels [33,34,46].
Given the location of the long thoracic nerve, it may
be especially prone to injury with axillary thoraco-
tomy incisions, VATS port insertion, first rib resec-
tions, and chest tube placement [46]. The risk of long
thoracic nerve injury should be minimal, however, if
the anatomy is considered when operating in the an-
terior scapular region.
In addition to perioperative damage, long thoracic
nerve injury by extreme abduction during general
anesthesia has been reported [32–34]. It is recom-
mended to avoid extreme abduction during patient
positioning at all times.
Postoperative pain and shoulder dysfunction
It is well established that thoracic procedures are
considered to be among the most painful surgical
incisions [1,2,47–50]. Acute postoperative wound
pain is anticipated as with all surgical procedures
and is caused by local tissue trauma, muscle division,
and peripheral and intercostal nerve injury [47–50].
Postoperative pain has significant overlap with post-
operative shoulder dysfunction [1,3,5,9,47,51,52].
It is reasonable to assume that pain can cause func-
tional limitations of the ipsilateral shoulder. Corre-
spondingly, movements of the shoulder girdle can
provoke or aggravate postoperative wound pain [1,5,
9,47,51–53]. Postoperative frozen shoulder, with or
without preexistent shoulder disease, also might be an
aggravating or causative factor to chronic post-thora-
cotomy pain [47,51–53]. The exact relationship
between postoperative shoulder function and pain is
complex. The precise impact of postoperative pain on
shoulder dysfunction, but also conversely of shoulder
dysfunction on postoperative pain, is elusive.
Less invasive access modalities, such as muscle-
sparing techniques, have been suggested to reduce
access trauma and consequently decrease postopera-
tive pain. Although muscle-sparing techniques have
significant benefits regarding postoperative shoulder
dysfunction [1,2,7,37,38], it has not reduced signifi-
cantly the incidence of acute and chronic postopera-
tive pain. Muscle division is unlikely to be the sole
contributing factor determining postoperative pain.

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343 335
In addition to muscle division, all traditional tho-
racotomy incisions require a certain amount of rib
spreading, causing direct intercostal nerve damage
and rib injury. Excessive spreading could lead to pain-
ful rib fractures and costochondral separations. There
now is increasing evidence that the excessive morbid-
ity of a thoracotomy is mainly the result of intercostal
nerve damage after rib spreading [1,54–57]; this is
illustrated by the fact that pain-related morbidity after
VATS procedures, in which rib spreading is unneces-
sary or minimized, is significantly less compared with
PLT and muscle-sparing alternatives [5,9,26,47,58].
The exact contribution to postoperative shoulder
function needs to be investigated.
In addition to postoperative wound pain, ipsilateral
shoulder pain is a contributing factor to postoperative
shoulder dysfunction [59,60]. It is a well-recognized
and separate entity from incisional wound pain, with a
reported incidence of 75% to 78% [59–61]. It has
been hypothesized that this phenomenon is caused by
referred pain through the phrenic nerve due to irrita-
tion of the pericardium, mediastinum, and dia-
phragmatic pleural surfaces [60,61]. It also has been
suggested that the suprascapular nerve plays an im-
portant role, transmitting pain signals caused by
excessive strain of the shoulder joint capsule as a re-
sult of positioning the patient in the lateral decubitus
position [62,63]. It has been shown, however,
that suprascapular nerve block has no effect on ipsi-
lateral shoulder pain, making this theory highly de-
batable [61].
Postoperative outcome
The available data on shoulder dysfunction after
thoracic surgery are limited. Shoulder dysfunction
has long been an overlooked entity, and substantiat-
ing assessments were scarce. With the emergence of
alternative, less invasive thoracic incisions, however,
clinical comparison between different access modali-
ties has become more proficient and comprehensive.
Studies increasingly include proper evaluation of
shoulder function as an important postoperative out-
come for comparison, either between standard PLT
and muscle-sparing techniques (Table 3) or more
recently between VATS and the traditional access
modalities (Table 4).
Posterolateral thoracotomy versus muscle-sparing
thoractomy
In a prospective, randomized, blinded study, Ha-
zelrigg et al [1] assessed early postoperative shoulder
strength and shoulder ROM in 50 patients who had to
undergo thoracotomy for various thoracic procedures,
comparing standard PLT with a latissimus dorsi–
sparing and serratus anterior–sparing thoracotomy.
Location and length of the incision were similar for
both procedures [35]. They found that both groups
had significant decrease in shoulder ROM at 1 week
postoperatively, without significant differences be-
tween the two groups. Strength of the latissimus
dorsi and serratus anterior was better preserved in
the muscle-sparing group at 1 week postoperatively.
ROM and shoulder strength seemed to return to
preoperative levels at 1 month after surgery in both
groups. In another prospective, randomized study
with 30 patients using similar surgical techniques,
Sugi et al [7] found significantly better ROM for
patients from the muscle-sparing group 2 weeks after
surgery. Shoulder ROM returned to baseline values at
1 month after surgery in both groups. These findings
are supported by a more recent prospective, random-
ized, blinded study assessing 60 patients [2]. The
authors found that shoulder ROM returned to preop-
erative values 2 weeks after muscle-sparing thoracot-
omy, whereas this was the case in the PLT group only
1 month after surgery. Although shoulder strength
was significantly impaired in the PLT group 1 week
postoperatively, shoulder strength was preserved in
the muscle-sparing group. As suggested by previous
studies [1,7], shoulder ROM and shoulder strength
returned to preoperative values 1 month after surgery
in both groups. Conversely, Kutlu et al [38] reported
that shoulder strength did not return to preoperative
levels 3 months after surgery. They suggested that the
benefits of a muscle-sparing thoracotomy on shoulder
strength persist at least 3 months postoperatively.
Significant shoulder function benefits have not been
found when only the serratus anterior was spared [64].
The available data show that latissimus dorsi–
sparing and serratus anterior– sparing procedures
benefit early postoperative shoulder strength and
ROM compared with standard PLT [1,2,7,38], espe-
cially in the first month after surgery. It is unclear,
however, until when these benefits persist. Data on
long-term postoperative shoulder function are scarce.
In a large prospective, nonrandomized study with
335 patients, Landreneau et al [65] found that patients
after a muscle-sparing thoracotomy had similar per-
ceived level of shoulder strength 1 year after surgery
compared with patients from the PLT group (97%
versus 92% of preoperative level; P = .07). In a cross-
sectional study, Khan et al [37] compared 10 patients
undergoing PLT with 10 matched patients who un-
derwent an auscultatory triangle thoracotomy. They
assessed postoperative shoulder strength using a

Table 3
Comparative studies on shoulder function after thoracotomy (non–muscle sparing versus muscle-sparing techniques)
Author Year Study design Access modalities N
Shoulder function
evaluation
A essments
ti e frame Results
Early postoperative results
Hazelrigg et al [1] 1991 Prospective
randomized
blinded
PLT vs MS
(LD + SA)
24 vs 26 Physician assessment
(physiotherapist)
P op
P top
wk
mo
Shoulder strength
Significant decrease at 1 wk
postop in PLT group
Returns to preop levels at
1 month postop in PLT group
Preservation of shoulder strength
at 1 wk and 1 mo postop in
MS group
ROM
Significant decrease at 1 wk
postop in both groups
Returns to preop levels at
1 mo postop in both groups
No significant differences
between groups
Sugi et al [7] 1996 Prospective
randomized
PLT vs MS
(LD + SA)
15 vs 15 Physician assessment
(physiotherapist)
P op
P top
ay 1,3,5,7,14
mo
ROM
Significantly better shoulder
ROM for MS patients up
to 14 days after surgery
Returns to preop levels at
1 mo postop in both groups
Mouton et al [64] 1999 Prospective
blinded
PLT vs MS (SA) 14 vs 14 Physician assessment
(physiotherapist)
P op
P top
wk
mo
y
Shoulder function
No significant differences
between groups at 2 wk, 3 mo
and 3 y after surgery
Kutlu et al [38] 2001 Prospective
randomized
blinded
PLT vs MS
(LD + SA)
10 vs 10 Physician assessment
(+ dynamometer)
P op
P top
mo
Shoulder strength
Significant decrease at 3 mo
postop in PLT group
No significant decrease at 3 mo
postop in MS group
Significantly better shoulder
strength for MS patients at
3 mo postop
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)331–343
336
ss
m
re
os
1
1
re
os
d
1
re
os
2
3
3
re
os
3

Akcali et al [2] 2003 Prospective
randomized
blinded
PLT vs MS
(LD + SA)
30 vs 30 Physician assessment
(physiotherapist)
Preop
Postop
1 wk
2 wk
1 mo
Shoulder strength
Significant decrease at 1 wk
postop in PLT group
Returns to preop levels at 1 mo
postop in PLT group
Preservation of shoulder strength
at 1 wk and 1 mo postop in
MS group
ROM
Significant decrease at 1 wk
postop in both groups
Returns to preop levels at 1 mo
postop in PLT group
Returns to preop levels at 2 wk
postop in MS group
Significantly better in MS group
at 1 wk and 2 wk postop
Late postoperative results
Landreneau et al [65] 1996 Prospective LT vs MS
(LD + SA)
187 vs 148 Questionnaire Postop
1 y
Shoulder strength
No significant differences between
groups (92% vs 97% of preop
level, P = .07)
Khan et al [37] 2000 Cross
sectional
case-matched
PLT vs ATT 10 vs 10 Physician assessment
(+ muscle strength
testing machine)
> 1 y postop
(mean 37 mo, range
12–60 mo)
Shoulder strength
Significantly better shoulder strength
for ATT patients >1 y postop
(78% vs 102% of preop level,
P = .04)
Abbreviations: ATT, auscultatory triangle thoracotomy; LT, lateral thoracotomy; MS (SA), serratus anterior-sparing thoracotomy; MS (LD + SA), latissimus dorsi and serratus anterior-
sparing thoracotomy; PLT, poterolateral thoracotomy; ROM, shoulder range of motion.
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)331–343
337

Table 4
Comparative studies on shoulder function after thoracic surgery (thoracotomy versus VATS)
Author Year Study design Access modalities N
Shoulder function
evaluation
Assessm nts
time fra e Results
Early postoperative results
Radberg et al [6] 1995 Retrospective PLT vs VATS 25 vs 24 Questionnaire
(visual analogue scale)
Postop
1 wk
ROM
Significantly less ROM complaints
at 1 wk after surgery for VATS
patients (75 vs 35, P < .05)
Reduced ROM lasted median 3 wk
in VATS patients and 10 wk in
PLT patients
Furrer et al [66] 1997 Prospective PLT vs VATS 15 vs 15 Physician assessment Postop Shoulder function
4 mo Shoulder function was normal in
all but one patient after PLT
No significant differences
between groups
Li et al [8] 2003 Prospective PLT vs VATS 11 vs 18 Physician assessment
(physiotherapist)
Questionnaire
Preop
Postop
1 wk
1 mo
3 mo
ROM
Significantly better ROM for
VATS patients at 1 wk and
1 mo postop
Shoulder strength
Significantly better shoulder
strength for VATS patients at
1 wk postop
Shoulder function-related QOL
No significant differences
between groups
Landreneau et al [5] 1993 Prospective (MS) LLT vs
VATS
57 vs 81 Physician assessment
(dynamometer)
Preop
Postop
day 3
day 2
Shoulder strength
Significant decrease at postop day 3
in both groups (56% vs 59%
of preop level, P = NS)
Significantly better shoulder
strength for VATS patients at
postop day 21 (59% vs 85%
of preop level, P = .01)
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)331–343
338
e
m
1
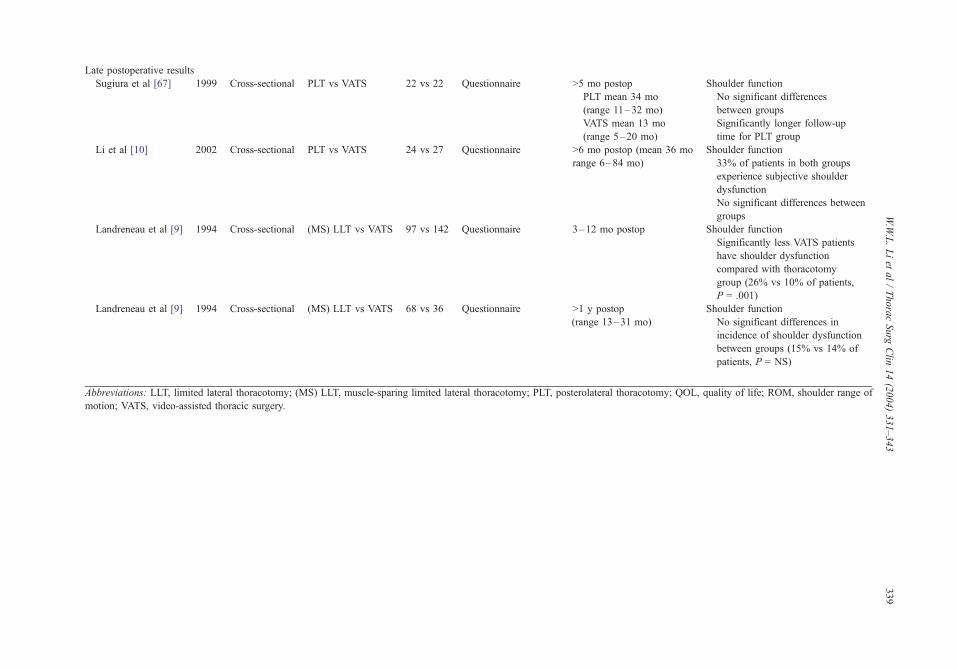
Late postoperative results
Sugiura et al [67] 1999 Cross-sectional PLT vs VATS 22 vs 22 Questionnaire >5 mo postop Shoulder function
PLT mean 34 mo
(range 11–32 mo)
No significant differences
between groups
VATS mean 13 mo
(range 5–20 mo)
Significantly longer follow-up
time for PLT group
Li et al [10] 2002 Cross-sectional PLT vs VATS 24 vs 27 Questionnaire >6 mo postop (mean 36 mo
range 6–84 mo)
Shoulder function
33% of patients in both groups
experience subjective shoulder
dysfunction
No significant differences between
groups
Landreneau et al [9] 1994 Cross-sectional (MS) LLT vs VATS 97 vs 142 Questionnaire 3–12 mo postop Shoulder function
Significantly less VATS patients
have shoulder dysfunction
compared with thoracotomy
group (26% vs 10% of patients,
P = .001)
Landreneau et al [9] 1994 Cross-sectional (MS) LLT vs VATS 68 vs 36 Questionnaire >1 y postop
(range 13–31 mo)
Shoulder function
No significant differences in
incidence of shoulder dysfunction
between groups (15% vs 14% of
patients, P = NS)
Abbreviations: LLT, limited lateral thoracotomy; (MS) LLT, muscle-sparing limited lateral thoracotomy; PLT, posterolateral thoracotomy; QOL, quality of life; ROM, shoulder range of
motion; VATS, video-assisted thoracic surgery.
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)331–343
339

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343340
muscle strength testing machine measuring maximal
strength throughout the ROM of that muscle and
found that even after more than 1 year after surgery,
the auscultatory triangle thoracotomy group still had
24% greater shoulder adduction strength than the
PLT group.
Video-assisted thoracic surgery
The fact that access trauma is reduced with VATS
has been well documented. There is general consen-
sus on the benefits of this approach with respect to
less postoperative pain, better preservation of pulmo-
nary function, and earlier return to normal activities
[26,58]. The available data on shoulder function after
VATS are inconclusive, however, originating mainly
from cross-sectional and retrospective studies. In one
of the few prospective studies available, Li et al [8]
assessed early postoperative shoulder strength, ROM,
and shoulder function–related quality of life compar-
ing PLT with VATS. They found that VATS patients
had significantly better shoulder strength 1 week
postoperatively and significantly better ROM 1 week
and 1 month after surgery. These differences did not
lead to significant differences in shoulder function–
related quality of life between the two groups, how-
ever. In another small prospective study comparing
PLT with VATS, Furrer et al [66] reported no signif-
icant differences between the two groups 4 months
after surgery.
Radberg et al [6] analyzed 25 patients who had
undergone thoracoscopy and compared the outcome
with 24 patients who had undergone conventional
surgery for spontaneous pneumothorax. Using a ques-
tionnaire and visual analogue scales to grade postop-
erative shoulder ROM complaints, patients in the
thoracoscopy group reported significantly less impair-
ment of shoulder movement 1 week after surgery
(35 versus 75 on visual analogue scale; P < .05) and
were able to return to work and daily activities earlier
(3 weeks versus 8 weeks after surgery; P < .001).
Regarding late postoperative shoulder function,
two small, cross-sectional, questionnaire-based stud-
ies [10,67] found no significant differences between
VATS and PLT patients more than 6 months after
surgery. The available data seem to indicate that
VATS has significant benefits for early postoperative
shoulder function compared with thoracotomy poten-
tially 1 month after surgery [5,6,8]. The level of
evidence is poor, however, and the number of patients
studied is limited. Prospective randomized compar-
isons with large groups of patients and proper long-
term follow-up are necessary to evaluate the potential
benefits of VATS for postoperative shoulder function.
There has been no published report so far on a
study comparing VATS with muscle-sparing tho-
racotomy with respect to shoulder function. Ne-
vertheless, studies comparing VATS with lateral
thoracotomy (with or without muscle sparing)
showed that the former is associated with less short-
term shoulder dysfunction [5,9]. In a prospective,
nonrandomized study with 138 patients, Landreneau
et al [5] measured the strength of the latissimus dorsi
and serratus anterior muscle groups with a standard
dynamometer. They found that VATS was associated
with significantly better short-term shoulder strength
3 weeks after surgery (59% versus 85% of baseline
value; P = .01). In a follow-up study in an expanded
group of patients [9] using self-developed question-
naires to assess shoulder restriction, the same inves-
tigators reported that these benefits persist 1 year after
surgery. No significant differences were found be-
tween the two groups more than 1 year after surgery.
Postoperative shoulder rehabilitation
Various factors contribute to an improved out-
come after thoracic surgery, including early mobili-
zation [68,69], chest physiotherapy [70], breathing
exercises [71], and incentive spirometry [71,72], all
of which would be more effective given good anal-
gesia with minimal side effects [47–50]. Chest drains
should be removed as soon as clinically acceptable.
Physiotherapy exercises also are advised to im-
prove mobility of the shoulder, prevent frozen shoul-
der syndrome, and reduce postoperative shoulder
dysfunction. Specifically with upper extremity exer-
cise modalities, improvement in shoulder strength
and function can be expected [73,74]. It is suggested
that exercise training can lead to improvement in the
ability to perform activities of daily living, exercise
endurance, pulmonary function, and quality of life
[73,74]. The exact contribution of upper extremity
training to the above-mentioned variables is unclear,
however, and should be explored further.
Summary
Thoracic procedures are considered to be among
the most painful surgical incisions and are associated
with considerable postoperative pain and shoulder
dysfunction, severely affecting mobility and activities
of daily living. Improper patient positioning, muscle
division, perioperative nerve injury, rib spreading,
and consequent postoperative pain influence the
patient’s postoperative shoulder function and quality

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343 341
of life. To reduce access trauma and postoperative
morbidity, various alternative modalities have been
proposed to replace the standard PLT, including
muscle-sparing techniques and VATS. Initial evalua-
tions suggest that these alternatives are associated
with significantly better postoperative shoulder func-
tion. Proper comparative studies using standardized
questionnaires, objective evaluations, or quality-
of-life assessments are scarce, however. Proper post-
operative care, including early mobilization and
effective physiotherapy, is a cornerstone in successful
patient rehabilitation and rapid return to normal daily
activities. Whether upper extremity exercises can
contribute to improvement in postoperative shoulder
function and the ability to perform activities of daily
living needs to be studied further.
Acknowledgments
The authors are indebted to Shirley Lam, Division
of Cardiothoracic Surgery, Department of Surgery,
Prince of Wales Hospital, Hong Kong SAR, for her
help and dedication in data collection and preparation
of the manuscript.
References
[1] Hazelrigg SR, Landreneau RJ, Boley TM, et al. The
effect of muscle-sparing versus standard posterolateral
thoracotomy on pulmonary function, muscle strength,
and postoperative pain. J Thorac Cardiovasc Surg
1991;101:394–401.
[2] Akcali Y, Demir H, Tezcan B. The effect of standard
posterolateral versus muscle-sparing thoracotomy on
multiple parameters. Ann Thorac Surg 2003;76:
1050–4.
[3] Triffitt PD. The relationship between motion of the
shoulder and the stated ability to perform activities of
daily living. J Bone Joint Surg Am 1998;80:41–6.
[4] Halder AM, Itoi E, An KN. Anatomy and biomechan-
ics of the shoulder. Orthop Clin North Am 2000;31:
159–76.
[5] Landreneau RJ, Hazelrigg SR, Mack MJ, et al. Post-
operative pain-related morbidity: video-assisted tho-
racic surgery versus thoracotomy. Ann Thorac Surg
1993;56:1285–9.
[6] Radberg G, Dernevik L, Svanvik J, Thune A. A com-
parative retrospective study of thoracoscopy versus
thoracotomy for the treatment of spontaneous pneumo-
thorax. Surg Laparosc Endosc 1995;5:90–3.
[7] Sugi K, Nawata S, Kaneda Y, Nawata K, Ueda K,
Esato K. Disadvantages of muscle-sparing thoracoto-
my in patients with lung cancer. World J Surg 1996;20:
551–5.
[8] Li WW, Lee RL, Lee TW, et al. The impact of thoracic
surgical access on early shoulder function: video-
assisted thoracic surgery versus posterolateral thora-
cotomy. Eur J Cardiothorac Surg 2003;23:390–6.
[9] Landreneau RJ, Mack MJ, Hazelrigg SR, et al. Pre-
valence of chronic pain after pulmonary resection
by thoracotomy or video-assisted thoracic surgery.
J Thorac Cardiovasc Surg 1994;107:1079–86.
[10] Li WW, Lee TW, Lam SS, et al. Quality of life follow-
ing lung cancer resection: video-assisted thoracic sur-
gery vs thoracotomy. Chest 2002;122:584–9.
[11] Yap KP, McCready DR, Narod S, Manchul LA, Tru-
deau M, Fyles A. Factors influencing arm and axillary
symptoms after treatment for node negative breast car-
cinoma. Cancer 2003;97:1369–75.
[12] Gosselink R, Rouffaer L, Vanhelden P, Piot W, Troos-
ters T, Christiaens MR. Recovery of upper limb func-
tion after axillary dissection. J Surg Oncol 2003;83:
204–11.
[13] Rietman JS, Dijkstra PU, Geertzen JH, et al. Short-
term morbidity of the upper limb after sentinel lymph
node biopsy or axillary lymph node dissection for
stage I or II breast carcinoma. Cancer 2003;98:690–6.
[14] Rietman JS, Dijkstra PU, Hoekstra HJ, et al. Late mor-
bidity after treatment of breast cancer in relation to
daily activities and quality of life: a systematic review.
Eur J Surg Oncol 2003;29:229–38.
[15] Vander Salm TJ, Cereda JM, Cutler BS. Brachial plex-
us injury following median sternotomy. J Thorac Car-
diovasc Surg 1980;80:447–52.
[16] Vander Salm TJ, Cutler BS, Okike ON. Brachial
plexus injury following median sternotomy: part II.
J Thorac Cardiovasc Surg 1982;8:914–7.
[17] Morin JE, Long R, Elleker MG, Eisen AA, Wynands
E, Ralphs-Thibodeau S. Upper extremity neuropathies
following median sternotomy. Ann Thorac Surg 1982;
34:181–5.
[18] Stangl R, Altendorf-Hofmann A, von der Emde J. Bra-
chial plexus lesions following median sternotomy in
cardiac surgery. Thorac Cardiovasc Surg 1991;39:
360–4.
[19] Vahl CF, Carl I, Muller-Vahl H, Struck E. Brachial
plexus injury after cardiac surgery: the role of internal
mammary artery preparation: a prospective study on
1000 consecutive patients. J Thorac Cardiovasc Surg
1991;102:724–9.
[20] Sharma AD, Parmley CL, Sreeram G, Grocott HP.
Peripheral nerve injuries during cardiac surgery: risk
factors, diagnosis, prognosis, and prevention. Anesth
Analg 2000;91:1358–69.
[21] Kroll DA, Caplan RA, Posner K, Ward RJ, Cheney
FW. Nerve injury associated with anesthesia. Anesthe-
siology 1990;73:202–7.
[22] Nercessian OA, Macaulay W, Stinchfield FE. Periph-
eral neuropathies following total hip arthroplasty.
J Arthroplasty 1994;9:645–51.
[23] Posta Jr AG, Allen AA, Nercessian OA. Neurologic
injury in the upper extremity after total hip arthro-
plasty. Clin Orthop 1997;345:181–6.
W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343342
[24] Ben-David B, Stahl S. Prognosis of intraoperative bra-
chial plexus injury: a review of 22 cases. Br J Anaesth
1997;79:440–5.
[25] Yim AP. Minimizing chest wall trauma in video-assis-
ted thoracic surgery. J Thorac Cardiovasc Surg 1995;
109:1255–6.
[26] Yim AP. VATS major pulmonary resection revisited—
controversies, techniques, and results. Ann Thorac Surg
2002;74:615–23.
[27] Cooper DE, Jenkins RS, Bready L, Rockwood Jr CA.
The prevention of injuries of the brachial plexus sec-
ondary to malposition of the patient during surgery.
Clin Orthop 1988;228:33–41.
[28] ASATask Force on Prevention of Perioperative Periph-
eral Neuropathies. Practice advisory for the prevention
of perioperative peripheral neuropathies: a report by
the American Society of Anesthesiologists Task Force
on Prevention of Perioperative Peripheral Neuropa-
thies. Anesthesiology 2000;92:1168–82.
[29] Coppieters MW, Van de Velde M, Stappaerts KH. Po-
sitioning in anesthesiology: toward a better understand-
ing of stretch-induced perioperative neuropathies.
Anesthesiology 2002;97:75–81.
[30] Warner MA. Perioperative neuropathies. Mayo Clin
Proc 1998;73:567–74.
[31] Cheney FW, Domino KB, Caplan RA, Posner KL.
Nerve injury associated with anesthesia: a closed
claims analysis. Anesthesiology 1999;90:1062–9.
[32] Vastamaki M, Kauppila LI. Etiologic factors in isolated
paralysis of the serratus anterior: a report of 197 cases.
J Shoulder Elbow Surg 1993;2:240–3.
[33] Kauppila LI, Vastamaki M. Iatrogenic serratus anterior
paralysis: long-term outcome in 26 patients. Chest
1996;109:31–4.
[34] Wiater JM, Flatow EL. Long thoracic nerve injury.
Clin Orthop 1999;368:17–27.
[35] Bethencourt DM, Holmes EC. Muscle-sparing pos-
terolateral thoracotomy. Ann Thorac Surg 1988;45:
337–9.
[36] Horowitz MD, Ancalmo N, Ochsner JL. Thoracotomy
through the auscultatory triangle. Ann Thorac Surg
1989;47:782–3.
[37] Khan IH, McManus KG, McCraith A, McGuigan JA.
Muscle sparing thoracotomy: a biomechanical analysis
confirms preservation of muscle strength but no im-
provement in wound discomfort. Eur J Cardiothorac
Surg 2000;18:656–61.
[38] Kutlu CA, Akin H, Olcmen A, Biliciler U, Kayserilio-
glu A, Olcmen M. Shoulder-girdle strength after stan-
dard and lateral muscle-sparing thoracotomy. Thorac
Cardiovasc Surg 2001;49:112–4.
[39] Ginsberg RJ. Alternative (muscle-sparing) incisions in
thoracic surgery. Ann Thorac Surg 1993;56:752–4.
[40] Baeza OR, Foster ED. Vertical axillary thoracotomy:
a functional and cosmetically appealing incision. Ann
Thorac Surg 1976;22:287–8.
[41] Massimiano P, Ponn RB, Toole AL. Transaxillary
thoracotomy revisited. Ann Thorac Surg 1988;45:
559–60.
[42] Fry WA, Kehoe TJ, McGee JP. Axillary thoracotomy.
Am Surg 1990;56:460–2.
[43] Frola C, Serrano J, Cantoni S, Casiglia M, Turtulici I,
Loria F. CT findings of atrophy of chest wall muscle
after thoracotomy: relationship between muscles in-
volved and type of surgery. AJR Am J Roentgenol
1995;164:599–601.
[44] Duchateau J, Declety A, Lejour M. Innervation of the
rectus abdominis muscle: implications for rectus flaps.
Plast Reconstr Surg 1988;82:223–8.
[45] Warner JJ, Navarro RA. Serratus anterior dysfunction:
recognition and treatment. Clin Orthop 1998;349:
139–48.
[46] Salazar JD, Doty JR, Tseng EE, et al. Relationship of
the long thoracic nerve to the scapular tip: an aid to
prevention of proximal nerve injury. J Thorac Cardio-
vasc Surg 1998;116:960–4.
[47] Hazelrigg SR, Cetindag IB, Fullerton J. Acute and
chronic pain syndromes after thoracic surgery. Surg
Clin North Am 2002;82:849–65.
[48] Kavanagh BP, Katz J, Sandler AN. Pain control after
thoracic surgery: a review of current techniques. An-
esthesiology 1994;81:737–59.
[49] Savage C, McQuitty C, Wang D, Zwischenberger JB.
Postthoracotomy pain management. Chest Surg Clin N
Am 2002;12:251–63.
[50] Soto RG, Fu ES. Acute pain management for patients
undergoing thoracotomy. Ann Thorac Surg 2003;75:
1349–57.
[51] Landreneau RJ, Wiechmann RJ, Hazelrigg SR, Mack
MJ, Keenan RJ, Ferson PF. Effect of minimally inva-
sive thoracic surgical approaches on acute and chronic
postoperative pain. Chest Surg Clin N Am 1998;8:
891–906.
[52] d’Amours RH, Riegler FX, Little AG. Pathogenesis
and management of persistent postthoracotomy pain.
Chest Surg Clin N Am 1998;8:703–22.
[53] Dajczman E, Gordon A, Kreisman H, Wolkove N.
Long-term postthoracotomy pain. Chest 1991;99:
270–4.
[54] Benedetti F, Amanzio M, Casadio C, et al. Postopera-
tive pain and superficial abdominal reflexes after pos-
terolateral thoracotomy. Ann Thorac Surg 1997;64:
207–10.
[55] Benedetti F, Vighetti S, Ricco C, et al. Postoperative
pain and superficial abdominal reflexes after postero-
lateral thoracotomy. J Thorac Cardiovasc Surg 1998;
115:841–7.
[56] Rogers ML, Henderson L, Mahajan RP, Duffy JP. Pre-
liminary findings in the neurophysiological assessment
of intercostal nerve injury during thoracotomy. Eur J
Cardiothorac Surg 2002;21:298–301.
[57] Nara T, Saito S, Obata H, Goto F. A rat model of
postthoracotomy pain: behavioural and spinal cord
NK-1 receptor assessment. Can J Anaesth 2001;48:
665–76.
[58] Swanson SJ, Batirel HF. Video-assisted thoracic sur-
gery (VATS) resection for lung cancer. Surg Clin North
Am 2002;82:541–59.

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 331–343 343
[59] Burgess FW, Anderson DM, Colonna D, Sborov MJ,
Cavanaugh DG. Ipsilateral shoulder pain following
thoracic surgery. Anesthesiology 1993;78:365–8.
[60] Scawn ND, Pennefather SH, Soorae A, Wang JY, Rus-
sell GN. Ipsilateral shoulder pain after thoracotomy
with epidural analgesia: the influence of phrenic nerve
infiltration with lidocaine. Anesth Analg 2001;93:
260–4.
[61] Tan N, Agnew NM, Scawn ND, Pennefather SH,
Chester M, Russell GN. Suprascapular nerve block
for ipsilateral shoulder pain after thoracotomy with
thoracic epidural analgesia: a double-blind comparison
of 0.5% bupivacaine and 0.9% saline. Anesth Analg
2002;94:199–202.
[62] Holt M. Ipsilateral shoulder pain following thoracic
operations. Anesthesiology 1993;79:192.
[63] Mark JB, Brodsky JB. Ipsilateral shoulder pain follow-
ing thoracic operations. Anesthesiology 1993;79:192.
[64] Mouton W, Fischer G, Striffeler H, et al. Is the function
of the serratus anterior muscle disturbed following di-
vision during a standard thoracotomy? Thorac Cardio-
vasc Surg 1999;47:188–9.
[65] Landreneau RJ, Pigula F, Luketich JD, et al. Acute and
chronic morbidity differences between muscle-sparing
and standard lateral thoracotomies. J Thorac Cardio-
vasc Surg 1996;112:1346–51.
[66] Furrer M, Rechsteiner R, Eigenmann V, Signer C,
Althaus U, Ris HB. Thoracotomy and thoracoscopy:
postoperative pulmonary function, pain and chest wall
complaints. Eur J Cardiothorac Surg 1997;12:82–7.
[67] Sugiura H, Morikawa T, Kaji M, Sasamura Y, Kondo
S, Katoh H. Long-term benefits for the quality of life
after video-assisted thoracoscopic lobectomy in pa-
tients with lung cancer. Surg Laparosc Endosc Per-
cutan Tech 1999;9:403–8.
[68] Zehr KJ, Dawson PB, Yang SC, Heitmiller RF. Stan-
dardized clinical care pathways for major thoracic
cases reduce hospital costs. Ann Thorac Surg 1998;
66:914–9.
[69] Cerfolio RJ, Pickens A, Bass C, Katholi C. Fast-track-
ing pulmonary resections. J Thorac Cardiovasc Surg
2001;122:318–24.
[70] Stiller KR, Munday RM. Chest physiotherapy for the
surgical patient. Br J Surg 1992;79:745–9.
[71] Hall JC, Tarala RA, Tapper J, Hall JL. Prevention of
respiratory complications after abdominal surgery:
a randomised clinical trial. BMJ 1996;312:148–53.
[72] Hall JC, Tarala R, Harris J, Tapper J, Christiansen K.
Incentive spirometry versus routine chest physiother-
apy for prevention of pulmonary complications after
abdominal surgery. Lancet 1991;337:953–6.
[73] ACCP/AACVPR Pulmonary Rehabilitation Guidelines
Panel. American College of Chest Physicians and
American Association of Cardiovascular and Pulmo-
nary Rehabilitation. Pulmonary rehabilitation: joint
ACCP/AACVPR evidence-based guidelines. Chest
1997;112:1363–96.
[74] British Thoracic Society. Pulmonary rehabilitation.
Thorax 2001;56:827–34.

Thorac Surg Clin 14 (2004) 345–352
Postthoracotomy pain syndrome
Manoj K. Karmakar, MD, FRCA, FHKCA, FHKAM*,Anthony M.H. Ho, MS, MD, FRCPC, FCCP, FHKCA, FHKAM
Department of Anaesthesia and Intensive Care, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin,
Hong Kong, China
Thoracotomy not only causes severe pain in the Incidence
immediate postoperative period but in a significant
number of patients it also produces long term post-
thoracotomy pain [1–3] that often lasts for months or
even years after surgery. The International Associa-
tion for the Study of Pain defines postthoracotomy
pain syndrome (PTPS) as pain that recurs or persists
along a thoracotomy incision for at least 2 months
following the surgical procedure [4]. Pain in this
condition is unrelated to infection or persistent or
recurrent tumor. Postthoracotomy pain syndrome has
also been referred to as chronic postthoracotomy pain
[5–7], postthoracotomy intercostal neuralgia [8], or
postthoracotomy neuralgia [3,5,9] in the literature.
Although recognized as a sequela of thoracotomy
since 1944 [10], when the first reference to this con-
dition was made by two United States army surgeons,
Blades and Dugan [10], a lack of data in the literature
until the 1990s suggests that it had been overlooked
or neglected as a clinical entity. In 1991 Dajczman
et al [11] published the first report on the preva-
lence, severity, and functional significance of PTPS.
Since then there has been growing interest on
this subject and postthoracotomy pain syndrome is
now a well-recognized long-term morbidity of tho-
racic surgery. Nevertheless, there is still a paucity of
objective data in the literature on PTPS. This article
presents the current understanding of postthoracot-
omy pain syndrome.
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00022-2
Financial support was entirely from departmental/ins-
titutional resources.
* Corresponding author.
E-mail address: [email protected]
(M.K. Karmakar)
It is difficult to quote the true incidence of post-
thoracotomy pain syndrome. Widely varying inci-
dence rates have been reported (Table 1), ranging
from 5% to 80% [2,3,9,11–19]. Different definitions
used to describe and assess pain, lack of large,
prospective studies, small sample size, varying sur-
gical techniques, nonstandard perioperative manage-
ment, varying periods of follow-up care, and so forth
have made the estimation of the incidence of PTPS
difficult. Nonetheless, published data suggest that
PTPS is a fairly common condition and can affect
more than 50% of patients who undergo thoracotomy.
It is a chronic condition, and as many as 30% of
patients might still experience pain 4 to 5 years after
surgery [11]. There is a decrease in the severity of
pain with time [2,13], although in the unfortunate few
there might be worsening of pain [13].
Characteristics of pain in postthoracotomy pain
syndrome
Most patients experience pain along the general
area of the thoracotomy scar [6,14], but pain can also
occur elsewhere in the chest [6,14], in the back [6,14],
or in more than one location [6,14]. Pain can occur
spontaneously or can be evoked by a particular
stimulus or activity. Allodynia, the sensation of pain
in response to a normally nonpainful stimulus, is a
frequent feature of PTPS [1]. The majority of patients
report their pain as an aching sensation [3,6,14–16, 9]
or tenderness [6,14], but it can also be described as
a continuous dysesthetic burning and aching [3,6,
14–16,19], lancinating pain [6], or a combination of
s reserved.

Table 1
Incidence of postthoracotomy pain syndrome
Reference Study design No. of patients studied
Time elapsed since
thoracotomy Incidence of PTPS
Dajczman et al, 1991 [11] Retrospective 56 Median 19.5 mo 54%
Cohort
Questionnaire
Kalso et al, 1992 [14] Retrospective
Cohort
134 Mean 30.3
(range 15–48) mo
44%
Questionnaire
Follow up
Conacher, 1992 [9] Retrospective 3109 �3 mo 5%
Records survey
Richardson et al, 1994 [3] Retrospective 883 �2 mo 22.3% at 2 mo
Cohort 14% at 1 y
Questionnaire
Landreneau et al, 1994 [16] Retrospective
Cohort
68 3–31 mo 44% at < 1 y
and 29% at > 1 y
Questionnaire
Keller et al, 1994 [12] Retrospective 238 �3 mo 11%
Cohort
Katz et al, 1996 [15] Retrospective 30 1.5 y 52%
Cohort
Telephone interview
Perttunen et al, 1999 [2] Prospective 84 �3 mo 80% at 3 mo
Standardized
Letter interview
75% at 6 mo and
61% at 1 y
Hu et al, 2000 [19] Retrospective, 372 28F12 mo 41% at 21F12 mo
Cohort
Telephone interview
Gotoda et al, 2001 [13] Retrospective 85 1 y 41%
Cohort
Questionnaire
Senturk et al, 2002 [17] Prospective 69 6 mo 62% at 6 mo
Randomized
Ochroch et al, 2002 [18] Prospective 157 12 mo 21.2% at 12 mo
Randomized
Double-blind
M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352346
sensations [14]. The involved site can have altered
sensation [14,19] and might be sensitive to touch or
change in temperature [1]. Pain is constant in 33%
to 80% of cases [3], but it can also be intermittent
in nature or come on ‘‘a few times a week’’ or ‘‘few
times a month’’ [11].
The severity of pain varies, but in the majority of
patients (80%) it is usually mild [11], often described
only as discomfort by patients and scoring 4 or less on
a 10-point visual analogue pain scale [11]. The
majority of patients do not seek medical advice and
declare it only on direct questioning [5,16]. Only a
small number of patients consider their pain to be
bothersome enough to seek medical advice [1,11].
Most declare it only on direct questioning [5]. Severe,
persistent, and debilitating pain only affects 4% to 5%
of patients suffering from PTPS [1,2,5,14]. Shoulder
movement worsens pain in a significant number of
patients (23.7%) [3]. In some cases movement of the
ipsilateral shoulder is so painful that frozen shoulder
can result from disuse [1]. Other factors that have been
cited to aggravate or induce pain in PTPS include
emotional stress [1,2], change in the weather [2], and
such activities as carrying heavy objects [2], lying on
the operated side [2], sitting [2], and working with the
hands on the operated side [2].
Etiology/pathogenesis
The exact mechanism for the pathogenesis of
PTPS is still not clear, but cumulative evidence sug-
gests that it is a combination of neuropathic and
nonneuropathic (myofascial) pain. The burning, dys-

M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352 347
esthesia, and allodynia sensation that is commonly
reported by sufferers of PTPS is typical of neuropathic
pain (ie, pain that is initiated or caused by a primary
lesion or dysfunction in the nervous system) [20].
Trauma to the intercostal nerve during thoracotomy is
the most likely cause and might occur because of
direct surgical trauma, stretching of the nerve during
rib retraction, suture entrapment of the nerve, or local
inflammation, edema, and fibrosis. Based on experi-
mental peripheral nerve injury data, a combination of
peripheral and central nervous system pain-related
phenomena contribute to neuropathic pain [20]. Pe-
ripheral nervous system changes include ectopic and
spontaneous neuronal discharge, ephaptic conduction
or crossexcitation, alteration in ion channel expres-
sion, collateral sprouting of primary afferent neurons,
and sprouting of sympathetic nerves into the dorsal
root ganglion and nociceptor sensitization [20]. Cen-
tral nervous system changes include central sensitiza-
tion, spinal reorganization, decrease in inhibitory
activity within the spinal cord, and cortical reorgani-
zation [20].
PTPS can also originate from the muscle and fas-
cia, producing myofascial pain syndrome [1,21,22],
which is characterized by steady aching muscle pain,
stiffness, limited range of movement, and trigger
points [1]. Two types of trigger points are seen: one
adjacent to the wound (44%) and the other in the
scapular region in a taut muscular band (67%) [21]. It
is difficult to differentiate the neuropathic from the
nonneuropathic component of pain when they coexist
[21]. Trigger point injection with local anesthetic is
considered to be the most effective treatment of
myofascial pain; the presence of a trigger point in the
scapular region in patients who have PTPS increased
the chance of success of treatment significantly [21].
Several local factors can also cause PTPS and
must be considered when evaluating these patients,
such as healing rib fracture, frozen shoulder, local
infection/pleurisy, costochondritis/costochondral dis-
location, and local tumor recurrence [16]. Local
tumor recurrence can cause pain in the area of the
incision by direct invasion of the chest wall, ribs, or
pleura and by compression of the intercostal nerves,
nerve roots, or spinal cord [1]. Vertebral collapse as a
result of tumor invasion can also be involved. Tumor
recurrence must therefore be excluded as a cause of
persistent pain when managing these patients.
Predictors for postthoracotomy pain syndrome
Several factors have been identified as predictors
for developing PTPS. Pain intensity 24 hours after
surgery [14,15] and analgesic consumption during the
first postoperative day [2] and week [2] are signifi-
cantly higher in patients who develop PTPS. A strong
association has been found with the female gender
[18], preoperative narcotic usage [12], chest wall
resection [12], pleurectomy [12] and postoperative
radiotherapy [23]. d’Amours et al, in their review on
the pathogenesis and management of persistent post-
thoracotomy pain, reported that the healing pattern of
the postthoracotomy scar has no influence on the
occurrence of PTPS [1]. Patients who have well-
healed scars might have as much pain as patients
who have keloid scars [1]. Sabanathan et al, in their
retrospective review, also found that cryoprobe neu-
rolysis of the intercostal nerve and benign esophageal
disease increased the likelihood of developing PTPS,
whereas rib resection and continuous extrapleural
intercostal nerve block with bupivacaine decreased
the likelihood of developing PTPS [23]. Adding a
nonsteroidal anti-inflammatory drug (NSAID) to the
above regimen brought about a further reduction in
the incidence of PTPS [3]. Others have also reported
that the nature of disease (benign or malignant) does
not influence the incidence or severity of PTPS [2].
Influence of acute pain management on the
development of postthoracotomy pain syndrome
Since reports of a predictive relationship between
a more intense acute pain experience [15] and greater
analgesic usage [2] in the postoperative period after
thoracotomy and PTPS, it has been suggested that
adopting an aggressive and effective postoperative
analgesic regimen and protecting the central ner-
vous system from sensitization after thoracotomy
[3] might reduce the incidence of PTPS. To date
only a few studies have evaluated the effects of anal-
gesic regimens or techniques on the incidence of
PTPS objectively.
Richardson et al., in a retrospective review of
1000 postthoracotomy patients over a 10-year period,
assessed the influence of acute postoperative pain
management on the incidence of PTPS at 2 months
after surgery [3]. The use of systemic opiates alone
was associated with a 23.4% incidence of PTPS [3].
Cryoprobe neurolysis of the intercostal nerve in-
creased the likelihood of developing PTPS (31.6%)
[3]. In contrast, using a continuous extrapleural para-
vertebral infusion of bupivacaine in conjunction with
systemic opiates reduced the incidence of PTPS
(14.8%) [3]. Adding an NSAID to this regimen
further reduced the incidence of PTPS (9.9%) [3].

M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352348
Hu et al [19] retrospectively reviewed 372 patients
who had undergone posterolateral thoracotomy. Of
these, 159 were finally analyzed. One hundred nine-
teen patients received thoracic epidural anesthesia
(TEA) in combination with general anesthesia (GA)
and 40 patients received only GA. TEA was initiated
before the skin incision and continued intraoperatively
using bupivacaine 0.5%. Epidural morphine, injected
intermittently every 12 hours, was used for analgesia
for 3 days after surgery [19]. The overall incidence of
PTPS was 41%, lasting for approximately 21 F12 months. The incidences of PTPS in patients who
received GA or GA plus TEAwere comparable (39%
versus 42%) [19]. More recently, Obata et al [24], in a
prospective, randomized, double-blind study, com-
pared the effects of a continuous thoracic epidural
infusion, initiated 20 minutes before (pre group) or on
completion of thoracotomy (post group) and contin-
ued for 72 hours, on early and long-term postthor-
acotomy pain [24]. The pre group not only
experienced less acute pain but the incidence of
long-term pain was also significantly lower 6 months
after surgery [24]. There were also a greater number of
pain-free patients in the pre group than in the post
group at 3 and 6 months after surgery [24]. Senturk
et al [17], in a prospective, randomized, single-blind
study of 69 patients, compared the effects of three
analgesic regimes: (1) thoracic epidural analgesia
initiated before (pre-TEA) or (2) after surgical incision
(post-TEA) and (3) intravenous patient-controlled
analgesia (IVPCA) on acute postoperative pain and
on the incidence of PTPS 6 months after thoracotomy
[17]. Patients in the pre-TEA group experienced
significantly less pain compared with the IVPCA or
post-TEA group during the first 48 hours after surgery
[17]. The overall incidence of PTPS 6 months after the
thoracotomy was 62% [17]. The incidence and inten-
sity of PTPS was also significantly lower in the pre-
TEA (45%) group than in the post-TEA (63%) and
IVPCA (78%) groups [17]. Although Obata et al [24]
and Senturk et al [17] demonstrated a preemptive
analgesic effect and a reduction in the incidence of
PTPS in the groups in which TEA was commenced
before the surgical incision [17], Ochroch et al [18]
were unable to demonstrate comparable results. In a
prospective, randomized, double-blind study they
compared PTPS in 157 patients who were randomly
assigned to receive TEA initiated prior to incision or
at the time of rib approximation [18]. The overall
incidence of PTPS was 21.2% [18] and there was no
difference in the incidence between the two study
groups 1 year after surgery [18].
The method of acute pain management therefore
has a variable effect on the incidence of PTPS. This
variable result is not surprising considering what is
involved in afferent nociception after a thoracotomy.
Pain after thoracotomy is conveyed to the central
nervous system not only by way of the intercostal
(somatic) nerves but also by way of the sympathetic
chain, phrenic nerve, vagus nerve, and (in the case of
ipsilateral shoulder pain) by way of the brachial
plexus. Moreover, TEA is unable to abolish somato-
sensory-evoked potentials to thoracic dermatomal
stimulation, suggesting that the blockade produced
by a TEA is incomplete [25,26]. Thus, no single
analgesic technique can provide total pain relief or
prevent central sensitization of the nervous system
after thoracotomy. A multimodal analgesic regimen,
or balanced analgesia [3], comprising of a regional
anesthetic technique initiated before thoracotomy
incision and continued into the postoperative period
in conjunction with a systemic opiate and a NSAID
might be more effective for postthoracotomy analgesia
and preventing central sensitization, thereby reducing
the incidence of PTPS. Richardson et al [3] certainly
believed that this balanced analgesic approach,
together with gentler surgical handling of the chest
wall aided by rib resection, was what contributed to the
low incidence of PTPS (9.9%) in their retrospective
series [3]. Future research should evaluate the effects
of a balanced analgesic regimen on the incidence of
PTPS in a prospective, randomized setting.
Influence of surgical technique on the
development of postthoracotomy pain syndrome
To reduce the impact of a standard posterolateral
thoracotomy on tissue injury and thereby acute and
long-term postthoracotomy pain, several investigators
have modified their surgical approach while per-
forming thoracic surgery. These modifications include
muscle-sparing thoracotomy [27,28], rib resection [3],
different types of suturing techniques to close the
chest [29], and video-assisted thoracoscopic surgery
(VATS) [30– 34]. Objective data on how these
technical modifications affect PTPS are still sparse,
however, and the results of these studies must be
interpreted with caution.
During a standard posterolateral thoracotomy, the
lattisimus dorsi and the serratus anterior muscles are
cut, whereas in a muscle-sparing thoracotomy these
two muscles are retracted. A muscle-sparing thora-
cotomy, when compared to a standard posterolateral
thoracotomy, has been shown to reduce acute post-
operative pain [27], but it does not influence the
frequency of long-term pain when assessed 1 year
after the operation [28].

M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352 349
Rib resection is often performed during thoracot-
omy to allow rib spreading with a reduced likelihood
of rib fracture and disruption of the posterior costo-
vertebral elements. A small segment of rib is excised
between the angle of the rib and its articulation with
the transverse process of the vertebra. The only study
that had evaluated the effect of rib resection on the
incidence of PTPS is a retrospective review Richard-
son et al of 1000 patients after thoracotomy by [3].
Rib resection was identified as one of the interven-
tions that reduced the likelihood of developing PTPS
[3]. With no further objective data or data from ran-
domized studies it is not possible to draw any firm
conclusion regarding whether or not rib resection in-
fluences the incidence of PTPS.
At the level of thoracotomy or at the adjacent in-
tercostal spaces, the intercostal nerve can often be
entrapped in the sutures that are used to close the
thoracotomy wound, resulting in PTPS [8]. A recent
nonrandomized study [29] found that patients who had
pericostal sutures (stitches placed on top of the fifth
rib and on top of the seventh rib), as opposed to intra-
costal sutures (stitches placed on top of the fifth rib and
through small holes drilled in the bed of the sixth rib) to
close their thoracotomy wound experienced more pain
at 2 weeks, 1 month, 2 months, and 3 months after
surgery [29]. The pericostal group of patients also
more commonly reported their pain as hot/burning,
shooting, or stabbing in nature [29], suggesting a
higher incidence of intercostal nerve damage.
VATS is a minimally invasive approach of per-
forming thoracic surgery and has been touted as a
way of reducing postoperative pain-related morbidity
associated with standard thoracotomy. Most surgical
procedures for benign or malignant diseases of
the chest, which in the past would have required a
thoracotomy, can now be performed safely using a
VATS approach. Patients who undergo thoracic sur-
gery by way of a VATS approach experience signifi-
cantly less acute postoperative pain [33] and require
fewer doses of narcotics postoperatively [33] when
compared with patients who undergo standard thora-
cotomy. Despite these early benefits, a significant
number (20–36%) of patients undergoing VATS still
suffer from PTPS [16,30,31,34]. Few studies have
compared the incidence of PTPS after VATS and
standard thoracotomy objectively. Landreneau et al
[16], in their retrospective review of patients under-
going VATS (n = 178) or lateral thoracotomy (n =
165) for pulmonary resection, found that patients who
underwent VATS experienced significantly less pain
throughout the first year after surgery [16]; however,
after the first year the incidence of pain was compa-
rable between the two groups [16]. Others have also
reported that the incidence of PTPS is comparable
between VATS and thoracotomy patients [30,32].
Current evidence therefore suggests that VATS re-
duces early postoperative pain but does not influence
the incidence of PTPS. Long-term pain after VATS is
neuropathic in nature and commonly reported in the
area of the trocar insertion site [34] or along the
thoracoabdominal dermatomal distribution of the in-
tercostal nerve involved at the intercostal space where
the camera port was inserted [35], which indicates that
inadvertent injury to the intercostal nerve during blind
trocar insertion, blunt dissection of the intercostal
space, or excessive torquing of the instruments (trocar)
in the intercostal space are involved. To reduce the
likelihood of intercostal nerve injury, Richardson and
Sabanathan [36] resected an ellipse of the superior
aspect of the rib with a device called the sari punch
prior to inserting the ports and aligned all of their
instruments along one intercostal space [36]. None of
the 40 patients who had this modification in their series
reported pain 2 months after surgery [36]. Yim et al
[35] reported several other maneuvers to minimize
intercostal nerve trauma during VATS: [1] flexing the
operating table 30� between the level of the nipples
and the level of the umbilicus (with less flexion in
elderly patients) to open up the intercostal spaces [2],
absolutely avoiding torquing of the thoracoscope
and switching to a 30� lens when visualization of the
lateral chest wall is required [3], not using rigid ports
(except staple cutters), introducing the instruments
directly through the wound [4], using smaller tele-
scopes (5 mm) for simpler procedures, and [5] deliv-
ering surgical specimens through the anterior port as
the anterior intercostal spaces are wider. By adopting
these maneuvers Yim et al observed an overall im-
provement in the incidence of PTPS in their VATS
patients [35] and only 15% of their patients were
reporting some discomfort in the clinic [35].
Postthoracotomy pain syndrome and quality of
life
In 1944 Blades and Dugan identified that soldiers
who sustained war wounds of the thorax suffered from
intercostal pain that interfered with rehabilitation and
return to duty [10]. Nearly six decades later there are
still limited objective data on how PTPS affects
patient’s quality of life. Published data suggest that
PTPS can adversely affect patient’s quality of life.
Fortunately, pain only ‘‘slightly or moderately’’
[11] interferes with normal daily living in 23% to
50% of patients [2]. The most frequently reported
complaint is sleep disturbance, which is seen in 20%

M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352350
to 63% of PTPS sufferers [2,3,6,19]. Pain can also
affect patients’ ability to exercise [3], go shopping [3]
or even work in some cases [3]. In a small subset of
patients pain can be severe and can be described as a
true disability to the extent that these patients are
incapacitated [5]. In these cases even the gentlest of
tactile stimulation on the affected side (eg, wearing
clothes or a gust of wind) can provoke paroxysms of
intense pain in the area of the thoracotomy wound
[1]. Although pain variably affects activities of nor-
mal daily living in patients who have PTPS, Perttu-
nen et al observed that the severity of limitation
diminished with time [2].
Ochroch et al [18] objectively evaluated physical
activity 4, 8, 12, 24, 36, and 48 weeks after thoracot-
omy in patients who were managed using TEA during
the postoperative period [18]. Physical activity was
assessed with the 10-question subset of the Quality-
of-Life Short Form Health Survey (SF-36), which
rates each activity on a three-point scale such that
the possible physical activity range is 10 to 30 [18].
The physical activity score was significantly lower
than preoperative values throughout the study period
and it was significantly lower in patients who reported
pain than in patients who reported no pain [18].
Although women were found to experience greater
postoperative and long-term pain than men, there was
no gender difference in physical activity [18].
Based on the functional status, Dajczman et al [11]
grouped patients after thoracotomy into three groups:
Group 1—individuals who are asymptomatic beyond
a brief period but might admit on questioning to numb-
ness at the incision site;Group 2—(the bulk of patients)
are those who experience mild, frequent chest pain that
can persist for years. Pain, being mild in intensity,
does not interfere with daily living or require medical
intervention; Group 3—a small subset of patients who
have debilitating pain that requires regular analgesics
and ongoing medical intervention [11].
Apart from the physical limitation that PTPS can
cause, as in most chronic pain syndromes, psycho-
logical morbidity can occur and can affect patient’s
quality of living. This is particularly true for PTPS
because patients might interpret the resurgence of
pain after a pain-free period after thoracotomy as
recurrence of malignancy. Chronic depression [19]
and anxiety are common presentations and might
manifest as suicidal tendencies.
Management
When patients present at follow-up clinics after
thoracotomy with symptoms suggestive of PTPS,
one must first exclude any recurrence of their primary
disease or malignancy as a cause for the persistent
pain. If there is a recurrence then it should be treated
appropriately. Otherwise, management should be
based on how much disability the PTPS is causing.
If pain is not causing any disability, then patients
should be managed conservatively. The majority of
patients who have PTPS can be managed conserva-
tively. If pain is causing disability, it is an indication
for referral to a pain management specialist.
At the pain clinic, management is multidiscipli-
nary and involves the pain specialist, social worker,
psychologist or psychiatrist, and the physical thera-
pist. It is important to inform the patient at the out-
set of treatment that there is no singular treatment
modality that is curative for PTPS and the focus
must be on reducing disability and improving qual-
ity of life. A through psychological evaluation must
be performed on initial evaluation by a psycholo-
gist or psychiatrist. As with most forms of neuro-
pathic pain, treatment of PTPS is also difficult and
often unsatisfactory. First-line management includes
physical therapy, NSAIDs, transcutaneous electrical
nerve stimulation, tricyclic antidepressants, antiepi-
leptics, sodium channel blockers, and opioids. Tri-
cyclic antidepressants are effective in managing
neuropathic pain and are used in doses and at
plasma levels that are much lower than that required
to treat depression. Amitriptyline, the drug most
commonly used, is started at relatively low doses
and increased slowly until an improvement is seen or
when excessive side effects ensue. Anticonvulsants
(eg, carbamazepine, phenytoin, valproic acid) are the
other group of drugs that are useful in managing
neuropathic pain because they suppress ectopic im-
pulse generation [1]. Gabapentin, a new anticonvul-
sant, has recently been used to treat neuropathic pain,
but data on its efficacy in patients who have PTPS
are still not available. Sodium channel blockers (eg,
lidocaine and mexilitine) also suppress abnormal
impulse generation in the nervous system and bring
about an improvement in symptoms in patients who
have neuropathic pain. The use of opioids to manage
noncancer pain is somewhat controversial because of
the potential for abuse. It is best used as part of a
multimodal treatment plan. Patients might often re-
quire more than one form of treatment for controlling
their pain.
If these measures are ineffective in controlling
pain, then more invasive measures such as nerve
blocks (intercostal nerve block, paravertebral block,
sympathetic nerve block), trigger point injection,
and long-term neuromodulation using epidural anal-
gesia or spinal cord stimulation can be tried.

M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352 351
Throughout the course of management there must be
continued surveillance for the recurrence of disease
or malignancy.
Summary
Postthoracotomy pain syndrome is relatively
common and is seen in approximately 50% of
patients after thoracotomy. It is a chronic condition,
and about 30% of patients might still experience pain
4 to 5 years after surgery. In the majority of patients
pain is usually mild and only slightly or moderately
interferes with normal daily living. In a small subset
of patients pain can be severe and can be described
as a true disability to the extent that these patients
are incapacitated. The exact mechanism for the
pathogenesis of PTPS is still not clear, but cumula-
tive evidence suggests that it is a combination of
neuropathic and nonneuropathic (myofascial) pain.
Trauma to the intercostal nerve during thoracotomy
is the most likely cause. Because pain does not cause
disability in the majority of patients, management is
usually conservative. If pain is causing disability
then multidisciplinary pain management involving
the pain specialist, social worker, physical therapist,
and a psychologist is required. It is mandatory to
exclude recurrence of disease or malignancy as a
cause for the pain prior to initiating treatment. As
with most forms of neuropathic pain, treatment of
PTPS is also difficult and patients might require
more than one form of therapy to control pain and
reduce disability. Based on current evidence, it is
not possible to draw any firm conclusion regarding
whether any form of analgesic or surgical technique
can influence the generation of PTPS. Preemptive
analgesia initiated prior to surgery shows promise
and might help reduce the incidence of PTPS.
Scientific evidence is steadily growing but there is
still a need for large, prospective, randomized trials
evaluating PTPS. Until more is known about this
condition and how to prevent the central and
peripheral nervous system changes that produce
long-term pain after thoracotomy, patients must
be warned preoperatively about the possibility of
developing PTPS and how it might affect their
quality of life after surgery. In addition, measures
such as selecting the least traumatic and painful
surgical approach, avoiding intercostal nerve trauma,
and adopting an aggressive multimodal perioperative
pain management regimen commenced before the
surgical incision should be performed to prevent
postthoracotomy pain syndrome.
References
[1] d’Amours RH, Riegler FX, Little AG. Pathogenesis
and management of persistent postthoracotomy pain.
Chest Surg Clin N Am 1998;8(3):703–22.
[2] Perttunen K, Tasmuth T, Kalso E. Chronic pain after
thoracic surgery: a follow-up study. Acta Anaesthesiol
Scand 1999;43(5):563–7.
[3] Richardson J, Sabanathan S, Mearns AJ, Sides C, Goul-
den CP. Post-thoracotomy neuralgia. Pain Clin 1994;
7(2):87–97.
[4] Merskey H. Classification of chronic pain: description
of chronic pain syndromes and definitions of pain
terms. Pain 1986;3:S138–9.
[5] Rogers ML, Duffy JP. Surgical aspects of chronic post-
thoracotomy pain. Eur J Cardiothorac Surg 2000;18(6):
711–6.
[6] Tiippana E, Nilsson E, Kalso E. Post-thoracotomy
pain after thoracic epidural analgesia: a prospective
follow-up study. Acta Anaesthesiol Scand 2003;47(4):
433–8.
[7] Landreneau RJ, Wiechmann RJ, Hazelrigg SR, Mack
MJ, Keenan RJ, Ferson PF. Effect of minimally inva-
sive thoracic surgical approaches on acute and chronic
postoperative pain. Chest Surg Clin N Am 1998;8(4):
891–906.
[8] Hardy PA. Post-thoracotomy intercostal neuralgia.
Lancet 1986;1(8481):626–7.
[9] Conacher ID. Therapists and therapies for post-
thoracotomy neuralgia. Pain 1992;48(3):409–12.
[10] Blades B, Dugan DJ. War wounds of the chest.
J Thorac Surg 1944;13:294–306.
[11] Dajczman E, Gordon A, Kreisman H, Wolkove N.
Long-term postthoracotomy pain. Chest 1991;99(2):
270–4.
[12] Keller SM, Carp NZ, Levy MN, Rosen SM. Chronic
post thoracotomy pain. J Cardiovasc Surg [Torino]
1994;35(6 Suppl 1):161–4.
[13] Gotoda Y, Kambara N, Sakai T, Kishi Y, Kodama K,
Koyama T. The morbidity, time course and predictive
factors for persistent post-thoracotomy pain. Eur J Pain
2001;5(1):89–96.
[14] Kalso E, Perttunen K, Kaasinen S. Pain after thoracic
surgery. Acta Anaesthesiol Scand 1992;36(1):96–100.
[15] Katz J, Jackson M, Kavanagh BP, Sandler AN. Acute
pain after thoracic surgery predicts long-term post-
thoracotomy pain. Clin J Pain 1996;12(1):50–5.
[16] Landreneau RJ, Mack MJ, Hazelrigg SR, Naunheim K,
Dowling RD, Ritter P, et al. Prevalence of chronic pain
after pulmonary resection by thoracotomy or video-
assisted thoracic surgery. J Thorac Cardiovasc Surg
1994;107(4):1079–85.
[17] Senturk M, Ozcan PE, Talu GK, Kiyan E, Camci E,
Ozyalcin S, et al. The effects of three different analge-
sia techniques on long-term postthoracotomy pain.
Anesth Analg 2002;94(1):11–5.
[18] Ochroch EA, Gottschalk A, Augostides J, Carson KA,
Kent L, Malayaman N, et al. Long-term pain and activ-
ity during recovery from major thoracotomy using tho-
M.K. Karmakar, A.M.H. Ho / Thorac Surg Clin 14 (2004) 345–352352
racic epidural analgesia. Anesthesiology 2002;97(5):
1234–44.
[19] Hu JS, Lui PW, Wang H, Chan KH, Luk HN, Tsou MY,
et al. Thoracic epidural analgesia with morphine does
not prevent postthoracotomy pain syndrome: a survey
of 159 patients. Acta Anaesthesiol Sin 2000;38(4):
195–200.
[20] Bridges D, Thompson SW, Rice AS. Mechanisms of
neuropathic pain. Br J Anaesth 2001;87(1):12–26.
[21] Hamada H, Moriwaki K, Shiroyama K, Tanaka H,
Kawamoto M, Yuge O. Myofascial pain in patients
with postthoracotomy pain syndrome. Reg Anesth Pain
Med 2000;25(3):302–5.
[22] Hazelrigg SR, Cetindag IB, Fullerton J. Acute and
chronic pain syndromes after thoracic surgery. Surg
Clin N Am 2002;82(4):849–65.
[23] Sabanathan S. Has postoperative pain been eradicated?
Ann R Coll Surg Engl 1995;77(3):202–9.
[24] Obata H, Saito S, Fujita N, Fuse Y, Ishizaki K, Goto
F. Epidural block with mepivacaine before surgery
reduces long-term post-thoracotomy pain. Can J
Anaesth 1999;46(12):1127–32.
[25] Lund C, Hansen OB, Mogensen T, Kehlet H. Effect
of thoracic epidural bupivacaine on somatosensory
evoked potentials after dermatomal stimulation. Anesth
Analg 1987;66(8):731–4.
[26] Dahl JB, Rosenberg J, Lund C, Kehlet H. Effect of
thoracic epidural bupivacaine 0.75% on somatosensory
evoked potentials after dermatomal stimulation. Reg
Anesth 1990;15(2):73–5.
[27] Hazelrigg SR, Landreneau RJ, Boley TM, Priesmeyer
M, Schmaltz RA, Nawarawong W, et al. The effect of
muscle-sparing versus standard posterolateral thoracot-
omy on pulmonary function, muscle strength, and post-
operative pain. J Thorac Cardiovasc Surg 1991;101(3):
394–400.
[28] Landreneau RJ, Pigula F, Luketich JD, Keenan RJ,
Bartley S, Fetterman LS, et al. Acute and chronic mor-
bidity differences between muscle-sparing and stan-
dard lateral thoracotomies. J Thorac Cardiovasc Surg
1996;112(5):1346–50.
[29] Cerfolio RJ, Price TN, Bryant AS, Sale BC, Bartolucci
AA. Intracostal sutures decrease the pain of thoracot-
omy. Ann Thorac Surg 2003;76(2):407–11.
[30] Furrer M, Rechsteiner R, Eigenmann V, Signer C,
Althaus U, Ris HB. Thoracotomy and thoracoscopy:
postoperative pulmonary function, pain and chest
wall complaints. Eur J Cardiothorac Surg 1997; 12(1):
82–7.
[31] Hutter J, Miller K, Moritz E. Chronic sequels after
thoracoscopic procedures for benign diseases. Eur J
Cardiothorac Surg 2000;17(6):687–90.
[32] Kirby TJ, Mack MJ, Landreneau RJ, Rice TW. Lobec-
tomy—video-assisted thoracic surgery versus muscle-
sparing thoracotomy. A randomized trial. J Thorac
Cardiovasc Surg 1995;109(5):997–1001.
[33] Landreneau RJ, Hazelrigg SR, Mack MJ, Dowling RD,
Burke D, Gavlick J, et al. Postoperative pain-related
morbidity: video-assisted thoracic surgery versus tho-
racotomy. Ann Thorac Surg 1993;56(6):1285–9.
[34] Passlick B, Born C, Sienel W, Thetter O. Incidence of
chronic pain after minimal-invasive surgery for spon-
taneous pneumothorax. Eur J Cardiothorac Surg 2001;
19(3):355–8.
[35] Yim AP. Minimizing chest wall trauma in video-
assisted thoracic surgery. J Thorac Cardiovasc Surg
1995;109(6):1255–6.
[36] Richardson J, Sabanathan S. Pain management in
video assisted thoracic surgery: evaluation of localised
partial rib resection. A new technique. J Cardiovasc
Surg [Torino] 1995;36(5):505–9.

Thorac Surg Clin 14 (2004) 353–365
Quality of life after lung cancer resection
Wilson W.L. Li, MSc, T.W. Lee, FRCS,Anthony P.C. Yim, MD, FRCS, FACS, FCCP, FHKAM*
Division of Cardiothoracic Surgery, Department of Surgery, The Chinese University of Hong Kong, Prince of Wales Hospital,
Hong Kong SAR, China
Lung cancer continues to be the most common on preoperative and postoperative QOL in NSCLC
cancer in the world, with the highest cancer mortality
rate by far [1,2]. For early-stage, stage I and II non–
small-cell lung cancer (NSCLC), surgical resection
remains the treatment of choice and offers the best
chance of cure [3–7]; however, only a minority of pa-
tients have resectable disease [8]. Furthermore, prog-
nosis remains grim even after surgical treatment.
Only 46% to 79% of stage I and 33% to 58% of
stage II lung cancer patients survive at 5 years after
lung cancer resection [8–11].
In a patient population that has such a high
mortality rate, evaluation and preservation of quality
of life (QOL) after treatment is imperative. Tradition-
ally, the main interest of the oncologic surgeon is the
long-term survival rate after tumor resection; how-
ever, from the patient’s point of view, survival statis-
tics inadequately deal with important issues regarding
daily life that arise before and after surgical treatment.
Patients are often more interested how surgery will
affect their physical functioning and performance of
activities of daily living [12]. Therefore, postopera-
tive QOL and factors influencing postoperative QOL
should be identified to facilitate preoperative guid-
ance and improvement of care. Furthermore, with
the advent of minimal access techniques in thoracic
surgery [13,14], QOL measurement could play an
important role in selecting the optimal access modal-
ity to perform lung cancer resection.
This review presents the basic concepts of QOL
research, several commonly used QOL measurement
instruments, and a summary of the available data
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00023-4
* Corresponding author.
E-mail address: [email protected] (A.P.C. Yim).
patients. This article also discusses the potential
role of minimal access surgery in the management
of NSCLC.
Quality of life and health-related quality of life
QOL is a subjective, dynamic, multidimensional
concept incorporating all aspects that have impact on
a person’s life [15–19]. Although there is no con-
sensus on the definition of QOL, there is general
agreement that it should include health status and
social and psychological well-being [15–20]. In a
study in which 108 newly diagnosed lung cancer
patients were asked to define good QOL, family life
(55%) was considered to be as important as health
(56%), followed by social life and leisure activities
(42%) [21]. In addition, some argue that spirituality
and environment health, as expressed by safety of the
environment and accessibility of health care and
social services, are also important factors to consider
[18–20].
Health, which is defined by the World Health
Organization as ‘‘a state of complete physical, mental
and social well-being, and not merely the absence of
disease and infirmity’’ [22], has a significant impact
on QOL. While QOL covers all imaginable aspects
of a person’s well-being, health-related QOL more
specifically focuses on aspects of life that are affected
by disease and medical intervention [23,24]. Never-
theless, QOL and health-related QOL are often used
interchangeably in medical literature. Therefore, the
term QOL is used in this article to indicate health-
related QOL for consistency with the majority of
available literature.
s reserved.

Surg Clin 14 (2004) 353–365
Measuring quality of life
QOL is a subjective measurement of a person’s
well-being and should therefore be assessed based
upon the patient’s point of view [25]. Proxy or sur-
rogate evaluations should be avoided whenever pos-
sible; it has been shown that family members or
professional caregivers systematically underestimate
QOL and underreport the amount of symptoms of the
subject [25–29].
QOL assessments can be performed through sev-
eral modes of administration, all with advantages and
disadvantages in terms of costs, response rate, patient
burden, interviewer bias, and amount of missing
items [30–35]. Traditional methods to collect QOL
data are face-to-face interviews, self-administration
by mail, and telephone interviews. While face-to-face
interviews ensure compliance, decrease errors, and
decrease the amount of missing items [30,31], it is
much more expensive when compared with other
modes of QOL assessment. Phone interviews appear
to be an appropriate alternative, being cost-effective
and providing low rate of missing items and high
consent rates [31–33]. It has been suggested that
these different methods of collecting QOL data pro-
vide similar and directly comparable results [35];
however, one should be cautious when interpreting
QOL data from clinical studies collected with mixed
methods [33,34]. More recently, various electronic
modes of administration have become a subject of
interest in the collection of QOL data. Initial reports
have suggested that computer administration [36,37]
and QOL assessment through the Internet [38] can
avoid the occurrence of missing data and are cost
effective. Furthermore, results can be automatically
entered into an electronic database, saving time on
entering and verifying data from paper question-
naires [36–39]; however, it remains be to confirmed
whether or not electronic versions of existing QOL
instruments produce data comparable with traditional
paper questionnaires.
QOL is a dynamic concept [40], varying over time
and depending on changes over time, changes be-
cause of treatment effects, or alterations in the disease
situation. These changes are also modified by psy-
chological phenomena such as adaptation, coping,
expectancy, and optimism [40], which can vary with
time and experience. Although cross-sectional studies
yield valuable information, the dynamic characteristic
of QOL is best assessed in a longitudinal setting.
Before treatment, baseline assessments should be
undertaken followed by regular evaluations at proper
time intervals depending on the type of QOL instru-
ment and purpose of the study [17].
W.W.L. Li et al / Thorac354
QOL is measured with QOL instruments that
must conform to certain attributes and review criteria
[41,42]. Because QOL is a multidimensional con-
struct that involves physical functioning and psycho-
logical and social aspects of well-being [15–20], an
important facet of QOL measurement instruments
is that they measure all of these domains [20,25,
41–43]. Unidimensional instruments evaluating a sin-
gle domain are simply not comprehensive enough to
measure QOL adequately [25,43]. Proper QOL in-
struments must also comply with certain psycho-
metric properties, including reliability, validity, and
sensitivity [41,42]. Reliability estimates the extent
to which an instrument is free of measurement error
and involves test– retest reliability and internal con-
sistency. Test– retest reliability indicates that the same
scores should be obtained from the same patient in
repeated measurements, assuming the subject has
remained unchanged in the meantime. Furthermore,
in a questionnaire in which multiple items are com-
bined into separate scales, items within a single scale
should show an adequate degree of internal consist-
ency—this is assessed using the Cronbach’s coeffi-
cient alpha and should be above the range of 0.7
[23,42,44]; however, a reliability coefficient ap-
proximating 1.0 indicates that there is too little dis-
crimination among the separate items, suggesting that
the items are measuring the same (or nearly the
same) thing.
Validity refers to the extent to which an instrument
measures what it is supposed to measure, and
involves content, construct, and criterion validity.
Content validity is the appropriateness of the items
to the purpose of the instrument. Construct validity is
the ability of the instrument to be sensitive to differ-
ent levels of QOL in a variety of patient groups.
Criterion validity refers to the extent the scores of the
instrument correlate to other, already validated or
‘‘gold standard’’ instruments.
Finally, QOL instruments should be responsive
to change [41,42,45]. Especially when evaluating
the effects of medical interventions in a longitudinal
setting, it is essential that the questionnaire can
detect any changes in QOL resulting from disease
or treatment.
Quality of life instruments
QOL measurement instruments can be divided
into two main categories: generic instruments and
specific instruments (Table 1). Generic instruments
are designed to measure QOL in a broad range of
populations, conditions, and interventions. While ge-
neric instruments allow comparison between popu-

Table 1
Commonly used instruments for assessing quality of life in lung cancer patients
Instrument Items Scales/domains Reference
General
Medical Outcome Study 36-Item
Short-Form Health Survey (SF-36)
36 Eight health concepts: physical functioning (PF), role
limitations because of physical problems (RP), bodily
pain (BP), general health (GH), vitality (VT), social
functioning (SF), role limitations because of emotional
problems (RE), mental health (MH)
[46,47]
One additional item on health transition
Items can be combined into one physical component
summary and one mental component summary
Ferrans and Powers Quality of Life
Index (QLI)
66 Four subscales: health and functioning, social and
economic, psychological/spiritual, family
[48]
Items can be combined into one Total Quality of Life Score
Sickness Impact Profile (SIP) 136 Two overall domains (physical, psychosocial) with 12
categories (sleep and rest, eating, work, home management,
recreation and pastimes, ambulation, mobility, body care
and movement, social interaction, alertness behavior,
emotional behavior, communication)
[49–51]
Nottingham Health Profile (NHP) 45 Six domains: physical abilities, pain, social isolation,
emotional reactions, energy level, sleep
[52]
World Health Organization Quality
of Life Instrument (WHOQOL-100)
100 Six domains: physical, psychological, independence, social,
environment, spiritual
[18,19]
One general health/QOL facet
Cancer-specific
European Organization for Research
and Treatment of Cancer Quality
of Life Questionnaire ‘‘Core’’ 30
items (EORTC QLQ-C30)
30 Five functioning scales (physical, role, cognitive,
emotional, social)
Eight symptom scales (fatigue, nausea/vomiting,
pain, dyspnea, sleep disturbance, appetite loss,
constipation, diarrhea)
[54]
Financial impact of disease and treatment
One Global health + 1 global QOL scale
Functional Assessment Of Cancer
Therapy (FACT-G, version 3)
34 Five domains: physical well-being, social/family well-being,
relationship with doctor, emotional well-being, functional
well-being
[56]
Items can be combined into a FACT-G Total Score
Functional Living Index-Cancer (FLIC) 22 Five domains: physical well-being and ability, emotional
state, sociability, family situation, nausea
[57]
Rotterdam Symptom Checklist (RSC) 39 Three domains: physical symptom distress, psychological
distress, activities of daily living level
[58]
One item on overall quality of life
Lung cancer-specific
EORTC Lung Cancer-Specific
Questionnaire module (EORTC
CLC-LC13) used in combination
with EORTC QLQ-C30
13 Lung cancer-associated symptoms (coughing, haemoptysis,
dyspnea, pain)
Side effects from chemo- and radiotherapy (sore mouth,
trouble swallowing, neuropathy, hair loss)
[55]
Functional Assessment Of Cancer
Therapy — Lung (FACT-L,
version 3)
44 Five domains: physical well-being, social/family well-being,
relationship with doctor, emotional well-being, functional
well-being
[59]
Lung cancer subscale (lung cancer symptoms, cognitive
function, regret of smoking)
Items can be combined into a FACT-G Total Score, a Lung
Cancer Subscale Score, and a Trial Outcome Index
Lung Cancer Symptom Scale (LCSS) 15 Four patient scales: symptoms, total symptomatic
distress, activity status, overall quality of life
[60]
One observer scales: symptoms
W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365 355

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365356
lations and disease states, they might not be sensitive
enough to detect changes caused by specific treat-
ments or conditions in a particular clinical setting.
Examples of generic instruments are the Medical
Outcomes Study 36-Item Short-Form Health Survey
(SF-36) [46,47], Ferrans and Powers Quality of Life
Index (QLI) [48], Sickness Impact Profile (SIP)
[49–51], Nottingham Health Profile (NHP) [52],
and the World Health Organization Quality of Life
Instrument (WHOQOL-100) [18,19]. The Ferrans and
Powers QLI should not be confused with the Spitzer
QL-Index [53], which is essentially a proxy evalua-
tion of QOL as QOL is objectified through an inter-
view with the physician including topics such as
activity, living, health, support, and outlook on life.
Specific instruments are focused on the impact of
a particular disease, condition, or symptom on QOL.
Because disease-specific instruments are designed to
assess specific effects of the disease or its treatment,
they are more likely to be responsive to change. In
oncology, one of the most widely used instruments is
the European Organization for Research and Treat-
ment of Cancer Quality of Life Core Questionnaire
(EORTC QLQ-C30) [54], which can be supplemented
with the site-specific lung cancer module (EORTC
QLQ-LC13) [55]. Other commonly used cancer-spe-
cific instruments are the Functional Assessment of
Cancer Therapy scale (FACT-G) [56], Functional
Living Index–Cancer (FLIC) [57], and the Rotterdam
Symptom Checklist (RSC) [58]. Lung cancer-specific
instruments include the Functional Assessment of
Cancer Therapy–Lung questionnaire (FACT-L) [59]
and the Lung Cancer Symptom Scale (LCSS) [60].
The choice of QOL instrument depends on the
purpose of the study [23]. When evaluating the effect
of a particular treatment of a specific disease, a
disease-specific instrument should be adequate.
When comparing results between different popula-
tions or between different diseases, generic instru-
ments might be more suitable. For the assessment of
QOL in lung cancer patients, the EORTC QLQ-C30
is the best-developed and most frequently reported
instrument, often supplemented with the EORTC
QLQ-LC13 [61,62]. More specifically for lung can-
cer patients receiving surgical treatment, the SF-36
is the most commonly used instrument (Table 2)
[63–67], acknowledged for its well-established reli-
ability, validity, and responsiveness in various surgi-
cal populations [63]; however, general instruments or
even lung cancer-specific instruments might not be
sensitive enough to identify areas that are likely to be
affected by lung cancer surgery, including postopera-
tive shoulder dysfunction [68,69] and postthora-
cotomy pain [68–72]. These problems could be
resolved by designing new lung cancer surgery-spe-
cific questionnaires, by developing specific modules
to supplement existing instruments (eg, FACT-G and
EORTC QLQ-C30), or by the addition of a small
number of items to existing questionnaires. Li et al
attempted to develop nine additional surgery-related
items to supplement the EORTC CLC-QLQ30 and
EORTC CLC-LC13 [73]; however, these items re-
main to be properly validated in a larger population.
Until lung cancer surgery-specific QOL instruments
or other solutions are available, a reasonable option is
the selection of a lung cancer-specific questionnaire
(eg, EORTC QLQ-C30 supplemented with EORTC
QLQ-LC13) or a well-validated general instrument
(eg, SF-36) supplemented with additional items on
postoperative shoulder dysfunction, postthoracotomy
pain, and other thoracic surgery-related complaints.
Previous studies
QOL data concerning lung cancer patients after
surgical treatment are reported infrequently. In an ex-
tensive review on QOL in lung cancer patients
covering literature from 1970 to 1995, 42 studies
were identified on QOL in NSCLC patients [61];
however, only one study focused on QOL after
surgical treatment [74]. Fortunately, QOL has been
noted as an increasingly important outcome measure-
ment after surgical treatment of NSCLC [75], and a
growing number of studies has been published on this
matter in recent years (Table 2).
Dales et al [74] were one of the first groups to use
standardized questionnaires to assess QOL in lung
cancer patients after surgical treatment in a prospec-
tive manner. In patients who have possible lung
cancer undergoing thoracotomy, QOL was measured
using the SIP and Spitzer QL-Index complemented
with the Clinical Dyspnea Index and Pneumoconiosis
Research Unit Index to measure perceived dyspnea.
The questionnaires were administered preoperatively
and 1, 3, 6, and 9 months after surgery. One hundred
seventeen patients were entered into the study, 26
(22%) of whom did not have a postoperative diag-
nosis of lung cancer. Dales et al found that dyspnea
and QOL significantly worsened at 1 and 3 months
postoperatively. In the first 3 months after surgery,
40% to 50% of the patients had dyspnea at rest or
with light activities and required major assistance in
managing household. Furthermore, 20% of patients
required assistance in basic activities of daily living
such as washing, toileting, and eating; however, QOL
and the degree of dyspnea returned to preoperative
levels at 6 to 9 months after surgery. Old age,

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365 357
magnitude of surgery, and the presence of cancer
were found to be independently associated with lower
levels of postoperative QOL. Unfortunately, no data
on postoperative pain or its effect on QOL were re-
ported in this study.
Similar findings were reported by Zieren et al [76],
who also used the Spitzer QL-Index with the EORTC
QLQ-CLC36 (an older version of the EORTC QLQ-
CLC30 questionnaire) to assess QOL in lung cancer
patients after surgical resection through an antero-
lateral thoracotomy. Fifty-two patients were assessed
on one occasion 12 months after surgery and 20 pa-
tients were followed prospectively. In the prospective
part of the study QOL assessments were performed
preoperatively, at discharge (median 11 days post-
operatively), and at 3 months, 6 months, 9 months,
and 12 months after surgery. Preoperatively, disease
symptoms and limitations relating to job and house-
hold tasks were the most frequent dysfunctions. These
restrictions in role functioning and limitations in
physical functioning increased in the first 3 months
postoperatively but improved again within 6 to
9 months after surgery. QOL scores in all domains
returned to baseline values at 12 months postopera-
tively despite the high prevalence of distressing
symptoms. At 1 year after surgery 73% of patients
still experienced dyspnea on running and 21% had
dyspnea at rest. In addition, 69% of patients com-
plained of coughing, 62% of fatigue, and 60% of pain.
Fatigue and pain were the symptoms most highly
correlated with a lower global QOL score. Restriction
in role functioning was common, with 54% reporting
a partial and 21% a complete incapacity to perform
household tasks. Eighty-five percent of patients could
not perform strenuous activities and 27% of patients
had trouble walking even a short distance. On the
other hand, 15% of the patients reported no physical
limitations at all and 25% of patients had no difficulty
in performing household tasks. The majority of
patients (81%) had no social or financial problems.
Pneumonectomy was significantly associated with
lower physical functioning and higher frequency of
symptoms in the first 3 months after surgery.
Mangione et al [63] prospectively assessed QOL
in three different surgical groups, including patients
undergoing lung cancer resection (n = 123), hip ar-
throplasty, and abdominal aortic aneurysm repair.
QOL was assessed using the SF-36 and evaluations
were performed before and 1, 6, and 12 months after
surgery. These researchers found that lung cancer pa-
tients before surgery have significantly lower scores
on the mental QOL scales (including social function-
ing, role limitations caused by mental problems,
mental health, health perception, and vitality) when
compared with the healthy population; however,
physical functioning between the two groups was
similar. The authors suggested that this is because
only patients who have localized disease were con-
sidered as candidates for surgical treatment. In the
first year after surgery QOL deteriorated in all sub-
scales, contributing to the physical construct of the
SF-36. Physical functioning worsened and bodily
pain and role limitations because of physical health
problems increased significantly. Furthermore, post-
operative vitality and health perception also declined
significantly. These changes persisted at least up to
12 months after surgery. On the other hand, subscales
contributing to the mental construct improved at
1 year after surgery. No further data were reported
on which symptoms or aspects of the postoperative
course could be responsible for the decline in QOL.
Handy et al [66] also used the SF-36 in combina-
tion with the Ferrans and Powers QLI to prospec-
tively assess QOL in 139 patients before and 6 months
after lung cancer resection through various access
modalities. They also found that lung cancer patients
before surgical treatment had poorer QOL when com-
pared with a healthy control group, and they reported
significantly lower scores in role limitations because
of emotional problems, mental health, and energy
subscales. Furthermore, in contrast to the previously
mentioned findings by Mangione et al [63], signifi-
cantly lower levels of preoperative physical function-
ing were also reported. After lung cancer resection,
QOL deteriorates even further at 6 months after
surgery. A significant persistent decline was found
in physical functioning, role limitations because of
physical problems, social functioning, mental health,
and bodily pain when compared with preoperative
levels. Although not worsened after surgery, post-
operative emotional role functioning remained signifi-
cantly lower when compared with a healthy control
population. On the other hand, levels of energy and
general health status at 6 months after surgery were
similar with the healthy control group. Postoperative
subjective dyspnea scores and visual analog pain
scores were also significantly worse when compared
with the preoperative baseline values; however, it
remains unclear whether or not a significant rela-
tionship was present between higher dyspnea and
pain scores and lower QOL scales. DLCO less than
45% predicted was the sole predictive clinical pa-
rameter and was associated with worse preoperative
physical functioning and QOL and worse postopera-
tive QOL, health and functioning, and psychological/
spiritual status.
In a recent study on cost and QOL after lung
cancer surgery, Welcker et al [67] measured QOL

Table 2
Available data on quality of life studies in patients who have non–small-cell lung cancer after surgical treatment
Article Year Design N Access modalities QOL instrument(s)
Assessment
time frame QOL outcome
Dales et al [74] 1994 Prospective
Descriptive
117 Thoracotomy SIP
Spitzer QL-Index
Preoperative
Postoperative
QOL significantly worsened at 1 and 3 mo after surgery and
returned to preoperative levels at 6 and 9 mo postoperatively
1 mo
3 mo
6 mo
9 mo
Older age, larger extent of surgery, and the presence of
cancer were independently associated with lower levels of
postoperative QOL
Zieren et al [76] 1996 Descriptive 52 Anterolateral
thoracotomy
EORTC QLQ-CLC36
Spitzer QL-Index
Postoperative
12 mo
Most limitations of QOL were related to physical and
role functions
High prevalence of distressing symptoms (73% exertional
dyspnea, 69% coughing, 62% fatigue, 60% pain)
Fatigue and pain were the symptoms most highly correlated
with a lower global QOL score
Majority of patients (81%) had no social or financial problems
Prospective
Descriptive
20 Anterolateral
thoracotomy
EORTC QLQ-CLC36
Spitzer QL-Index
Preoperative
Postoperative
11 d
QOL (especially role and physical functioning) deteriorated
in the first 3 mo after surgery and returned to preoperative
levels at 6–9 mo postoperatively
3 mo
6 mo
9 mo
Pneumonectomy was significantly associated with more
disease symptoms and greater limitations in physical
functioning when compared with lobectomy
Mangione et al [63] 1997 Prospective
Descriptive
123 PLT SF-36 Preoperative
Postoperative
1 mo
6 mo
12 mo
Lung cancer patients before surgical treatment have significantly
lower scores on the mental QOL scales when compared with the
healthy population (including social functioning, role limitations
because of mental problems, mental health, health perception and
vitality) but similar scores on physical functioning
QOL deteriorated in the first year after surgery in all
subscales contributing to the physical construct of the
SF-36 (physical functioning, role limitations because of
physical health problems, bodily pain, vitality, and health
perception)
Subscales contributing to the mental construct improved
at 1 y after surgery
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)353–365
358

Handy et al [66] 2002 Prospective
Descriptive
139 PLT (57.6%)
Sternotomy
(36.7%)
MS (5.0%)
VATS (0.7%)
SF-36
QLI
Preoperative
Postoperative
6 mo
Lung cancer patients before surgical treatment have
sig ificantly lower QOL when compared with a healthy
co rol group (regarding the physical functioning,
em tional role functioning, mental health, and energy
su cales)
QO deteriorates even further at 6 mo after surgery
(si ificant persistent decline in physical functioning,
ph ical role functioning, social functioning, mental
he th, and bodily pain)
DL O <45% predicted was the sole predictive clinical
pa meter (associated with worse preoperative physical
fu tioning and QOL and worse postoperative QOL,
he th and functioning, and psychological/spiritual status)
Welcker et al [67] 2003 Descriptive 22 Anterolateral
thoracotomy
SF-36 Postoperative
12 mo
Lu cancer patients at 12 months after surgery have
lo r scores on almost all SF-36 subscales (except bodily
pa ) when compared with normal healthy population and
pa nts who have other forms of cancer or chronic diseases
Myrdal et al [64] 2003 Cross-sectional
Descriptive
112 MS SF-36 + three
self-developed lung
specific questions
Median follow-up time:
23 mo postoperatively
(range 4–48)
Pa nts after lung cancer resection have significantly
wo e scores in most QOL domains (except bodily pain)
wh n compared with a healthy control group
Pa nts after lung cancer resection have significantly
wo e physical function when compared with matched
pa nts who had undergone CABG
Pn monectomy and FEV1 <60% before surgery had a
sig ificant correlation with lower scores for the physical
su mary component
Co tinued smoking after surgery was associated with
lo r scores for mental health and vitality
Sarna et al [65] 2002 Cross-sectional
Descriptive
142 Not reported SF-36
QOL-Survivor
Mean follow-up time:
10.4 y postoperatively
(range 5–22)
Lo -term survivors of lung cancer after surgical resection
ha worse physical function but better mental health when
co pared with patients who have other forms of cancer
an chronic lung disease
Lo -term survivors of lung cancer after surgical resection
be ve they have good QOL (50% viewed the cancer
ex rience as contributing to positive life changes and
71 described themselves as hopeful about the future)
Di essed mood was the strongest predictor of poor
lo -term QOL
(continued on next page)
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)353–365
359
n
nt
o
bs
L
gn
ys
al
C
ra
nc
al
ng
we
in
tie
tie
rs
e
tie
rs
tie
eu
n
m
n
we
ng
ve
m
d
ng
lie
pe
%
str
ng

Table 2 (continued)
Article Year Design N Access modalities QOL instrument(s)
Assessment
time frame QOL outcome
Sugiura et al [77] 1999 Cross-sectional
Comparative
44 PLT vs VATS Self-developed
questionnaire
(six items)
Mean follow-up time:
PLT 34 mo
(range 11–32)
VATS 13 mo
(range 5–20)
VATS patients had an earlier return to preoperative activity
(2.5 versus 7.8 mo, P = 0.03)
Significantly fewer VATS patients had acute and chronic
chest pain requiring medication (0 versus 4 patients, P= 0.01)
VATS patients were more satisfied with the size of the
scar and the operation as a whole
Li et al [73] 2002 Cross-sectional
Comparative
51 PLT vs VATS EORTC CLC-30
EORTC CLC-LC13
+ nine self-developed
lung cancer surgery-
specific questions
Mean follow-up time:
PLT 39.4 mo
(range 7–75)
VATS 33.5 mo
(range 6–84)
Both groups of patients enjoyed good QOL and high
levels of functioning without significant differences between
the groups
Most common symptoms were fatigue (74–92%), dyspnea
(75–85%), coughing (75–82%), and pain (67–71%)
All three self-developed multi-item QOL scales demonstrated
good reliability
Abbreviations: MS, muscle-sparing thoracotomy; PLT, posterolateral thoracotomy.
W.W.L.Liet
al/ThoracSurg
Clin
14(2004)353–365
360

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365 361
using the SF-36 in 49 subjects. One year postopera-
tively, lung cancer patients had lower scores on all
QOL subscales when compared with healthy volun-
teers, chronic obstructive pulmonary disease patients,
and patients who had other forms of cancer. Lesser
extent of resection and lower tumor stage correlated
significantly with higher quality-adjusted life years.
Lung cancer and lung cancer resection cause
significant deterioration of early postoperative QOL
[63,66,74,76]; however, the long-term effect of lung
cancer resection on QOL remains unclear given that
the available data originate mainly from a few retro-
spective analyses. Myrdal et al [64] compared long-
term QOL in 112 lung cancer patients after surgical
resection with patients undergoing coronary artery
bypass grafting (CABG) and a healthy control group.
The SF-36 was used to assess QOL, supplemented
with three additional lung-specific questions on the
presence of pain in the chest, breathlessness, and
cough. In addition, the Hospital Anxiety and Depres-
sion Scale (HAD) was used to measure anxiety and
depression. At a median follow-up of 23 months
after surgery (range 4–48 months), patients after lung
cancer resection had significantly worse physical
function when compared with the CABG group.
Correspondingly, lung cancer patients also had sig-
nificantly higher levels of breathlessness on physical
effort. Furthermore, pneumonectomy and FEV1 less
than 60% before surgery had a significant correlation
with lower scores for the physical summary compo-
nent. Continued smoking after surgery was associated
with lower scores for mental health and vitality. No
differences were found between the two groups
regarding depression or anxiety. Both groups also
reported significantly worse scores in most QOL
domains when compared with the healthy control
group. Surprisingly, bodily pain was the only sub-
scale that did not differ from the healthy control
group. The authors concluded that patients after lung
cancer surgery have a QOL comparable to that of
CABG patients; however, lung cancer patients have
lower levels of physical functioning, possibly be-
cause of reduced pulmonary function. Furthermore,
despite having been operated on because of a serious
malignancy, they report no significant impairment of
social function, mental status, anxiety, or depression.
In a similar report Sarna et al [65] reported that
long-term survivors of lung cancer after surgical
treatment have good QOL. They assessed QOL in
142 patients who had been disease-free for at least
5 years (mean 10.4 years, range 5–22 years) using the
SF-36, the QOL-Survivor questionnaire, and the
Center for Epidemiologic Studies Depression Scale.
When asked about their QOL, 50% of patients viewed
the cancer experience as contributing to positive life
changes and 71% described themselves as hopeful
about the future. Then again, 27% of patients re-
ported fatigue, 24% of patients reported aches or
pains, and 30% of patients reported problems with
anxiety. Furthermore, FEV1 was only 68% of pre-
dicted value. Nevertheless, despite having decreased
pulmonary function, multiple symptoms, and comor-
bidities, this did not seem to affect their overall QOL.
Also, distressed mood was shown to be the strongest
predictor of poor long-term QOL.
In summary, lung cancer and lung cancer resec-
tion cause significant deterioration in postoperative
QOL [63,66,74,76]. The available data suggest that
early-stage lung cancer patients already have signifi-
cantly lower QOL when compared with the normal
population before surgical treatment [63,66]. Signifi-
cant impairment was not only observed in physical
functioning [66] but also in mental health and emo-
tional functioning [63,66]. After lung cancer resec-
tion QOL deteriorates even further at 3 to 6 months
after surgery [63,66,74,76]. Postoperative pain [63,66]
and dyspnea [66,74] could be important causes of
disability. While some studies suggest that QOL
returns to baseline levels 6 to 9 months postopera-
tively [74,76], others report that QOL is still signifi-
cantly impaired at 6 months [66] and at 1 year after
surgery [63].
Prospective data analyzing long-term postopera-
tive QOL are not available. Nevertheless, available
data suggest that long-term survivors after lung cancer
surgery enjoy good QOL despite impaired physical
functioning [64,65]; however, although cross-sec-
tional studies yield valuable information, QOL is a
dynamic concept that is best assessed in a longitudi-
nal, prospective setting. Without preoperative baseline
evaluations, the effect of lung cancer and its treatment
on long-term QOL cannot be properly defined.
Despite recent increasing interest in QOL assess-
ment in lung cancer patients after surgical treatment,
available data remain limited. Postoperative QOL
data (collected in a prospective manner) of only
399 patients have been published so far. Moreover,
timing of assessment, the QOL instruments, and
access modalities used have been variable, compli-
cating interpretation and generalization of the infor-
mation at hand. Future studies need to be prospective
and longitudinal, and should include larger study
populations and a longer follow-up period to portray
the course of QOL in lung cancer patients more
accurately before and after surgical treatment. Fur-
thermore, it should be clarified which symptoms are
responsible for the deterioration of QOL after surgery
to improve postoperative care.

Surg Clin 14 (2004) 353–365
Minimal access surgery and quality of life
The application of video-assisted thoracic surgery
(VATS) for lung cancer resection remains controver-
sial [13,14]. The early postoperative benefits of this
approach such as less postoperative pain, less shoul-
der dysfunction, preservation of pulmonary function,
and earlier return to preoperative activity are well
documented [13,14]; however, the success of a cancer
operation is firstly judged by the long-term survival
of patients. Although there was initial skepticism
regarding the oncologic adequacy of VATS lung can-
cer resection, an increasing number of reports now
show consistently that the intermediate to long-term
survival is at least as good as—if not superior to—
the standard approach [13,14]. Given the apparent
equivalent survival outcome between the two access
modalities, QOL assessments become increasingly
important to help guide clinical decision making re-
garding selection of treatment option.
Data on QOL after VATS lung cancer resection are
extremely limited. In the previously mentioned pro-
spective study by Handy et al [66], only 0.7% of the
139 patients studied had lung cancer resection per-
formed through VATS. The sample size was too small
to provide helpful comments or multivariate analysis.
No other studies are available that assess the early
postoperative QOL in patients after VATS lung cancer
resection. Two small cross-sectional studies have
compared long-term QOL after lung cancer resection
through VATS with lung cancer resection through
thoracotomy [73,77]. Sugiura et al [77] compared
QOL in patients after lung cancer resection through
VATS or posterolateral thoracotomy (PLT). They used
a self-designed questionnaire with six items on time to
return to preoperative activity, narcotic medication
requirement, numbness in or around the incision,
shoulder function restriction, satisfaction with the size
of the scar, and satisfaction with the operation as a
whole. Twenty-two patients were recruited in both
groups. At a mean follow-up time of 21 months (range
5–43 months) they found that VATS patients had
an earlier return to preoperative activity (2.5 versus
7.8 months, P = 0.03), and significantly fewer VATS
patients had acute and chronic chest pain requiring
medication (zero versus four patients; P = 0.01).
Furthermore, VATS patients were more satisfied with
the size of the scar and the operation as a whole.
No significant differences between the groups were
found on shoulder dysfunction. However, all these
results should be interpreted with caution; there was a
significantly shorter follow-up for VATS patients
(12.6 months versus 33.6 months; P = 0.0001),
making comparison between the two groups less
W.W.L. Li et al / Thorac362
valid. Moreover, one should argue whether or not
QOL was really measured [41–43]; global QOL or
functioning status was not assessed and psychometric
properties (eg, validity and reliability) of the ques-
tionnaire used was not evaluated.
Li et al [73] used the EORTC QLQ-C30 and the
EORTC QLQ-LC13 supplemented with nine self-
developed lung cancer surgery-specific items on
shoulder dysfunction, scar-related complaints, post-
thoracotomy pain, and satisfaction with the surgical
procedure. They found that both groups of patients,
after a mean follow-up time of 33.5 months in the
VATS group and 39.4 months in the PLT group,
enjoyed good QOL and high levels of functioning
despite a fairly high incidence of symptoms. The most
common symptoms were fatigue (74–92%), dyspnea
(75–85%), coughing (75–82%), and pain (67–71%).
Furthermore, the three self-developed multi-item
QOL scales demonstrated good reliability.
Summary
Lung cancer continues to be the most common
cancer in the world, with the highest cancer mortality
rate by far. Although resection remains the treatment
of choice in early-stage NSCLC, the prognosis
remains grim even after surgical treatment. In a
patient population with such a high mortality rate,
evaluation and preservation of QOL after treatment
is imperative.
Early-stage lung cancer patients already have sig-
nificantly lower QOL when compared with the normal
population before surgical treatment, with significant
impairment in physical and emotional functioning.
Lung cancer resection causes further deterioration of
QOL, especially in the first 3 to 6 months after sur-
gery. While some studies suggest that QOL returns to
baseline levels at 6 to 9 months postoperatively, others
report that QOL is still significantly impaired at
6 months and 1 year after surgery. Although pros-
pective studies analyzing long-term postoperative
QOL are not available, retrospective data suggest that
long-term survivors after lung cancer surgery enjoy
good QOL despite impaired physical functioning.
QOL studies on VATS lung cancer resection are
extremely limited.
More prospective, longitudinal studies with larger
study populations and longer follow-up periods are
needed to portray the course of QOL in lung cancer
patients more accurately and to improve postopera-
tive care. Furthermore, comparative studies between
VATS and the standard thoracic incisions (including
QOL assessments) must be performed to guide clini-

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365 363
cal decision making regarding selection of optimal
access modality for performing lung cancer resection.
Acknowledgments
The authors are indebted to Shirley Lam, Division
of Cardiothoracic Surgery, Department of Surgery,
Prince of Wales Hospital, Hong Kong SAR, for her
help and dedication in data collection and preparation
of the manuscript.
References
[1] Parkin DM, Pisani P, Ferlay J. Global cancer statistics.
CA Cancer J Clin 1999;49(1):33–64.
[2] Jemal A, Murray T, Samuels A, Ghafoor A, Ward E,
Thun MJ. Cancer statistics, 2003. CA Cancer J Clin
2003;53(1):5–26.
[3] Deslauriers J, Gregoire J. Surgical therapy of early non-
small cell lung cancer. Chest 2000;117(4 Suppl 1):
104S–9S.
[4] British Thoracic Society, Society of Cardiothoracic
Surgeons of Great Britain and Ireland Working Party.
BTS guidelines: guidelines on the selection of patients
with lung cancer for surgery. Thorax 2001;56(2):
89–108.
[5] Tanoue LT, Ponn RB. Therapy for stage I and stage
II non-small cell lung cancer. Clin Chest Med 2002;
23(1):173–90.
[6] Smythe WR. Treatment of stage I non-small cell lung
carcinoma. Chest 2003;123(1 Suppl):181S–7S.
[7] Scott WJ, Howington J, Movsas B, American College
of Chest Physicians. Treatment of stage II non-small
cell lung cancer. Chest 2003;123(1 Suppl):188S–201S.
[8] Mountain CF. Revisions in the International System
for Staging Lung Cancer. Chest 1997;111(6):1710–7.
[9] van Rens MT, de la Riviere AB, Elbers HR, van Den
Bosch JM. Prognostic assessment of 2,361 patients
who underwent pulmonary resection for non-small cell
lung cancer, stage I, II, and IIIA. Chest 2000;117(2):
374–9.
[10] Naruke T, Tsuchiya R, Kondo H, Asamura H. Progno-
sis and survival after resection for bronchogenic carci-
noma based on the 1997 TNM-staging classification:
the Japanese experience. Ann Thorac Surg 2001;71(6):
1759–64.
[11] Fang D, Zhang D, Huang G, Zhang R, Wang L, Zhang
D. Results of surgical resection of patients with primary
lung cancer: a retrospective analysis of 1,905 cases.
Ann Thorac Surg 2001;72(4):1155–9.
[12] Cykert S, Kissling G, Hansen CJ. Patient preferences
regarding possible outcomes of lung resection: what
outcomes should preoperative evaluations target? Chest
2000;117(6):1551–9.
[13] Swanson SJ, Batirel HF. Video-assisted thoracic sur-
gery (VATS) resection for lung cancer. Surg Clin North
Am 2002;82(3):541–59.
[14] Yim AP. VATS major pulmonary resection revisited—
controversies, techniques, and results. Ann Thorac
Surg 2002;74(2):615–23.
[15] Cella DF, Bonomi AE. Measuring quality of life: 1995
update. Oncology [Huntingt] 1995;9(11 Suppl):47–60.
[16] Sloan JA, Cella D, Frost M, Guyatt GH, Sprangers M,
Symonds T. Clinical Significance Consensus Meeting
Group. Assessing clinical significance in measuring
oncology patient quality of life: introduction to the
symposium, content overview, and definition of terms.
Mayo Clin Proc 2002;77(4):367–70.
[17] Soni MK, Cella D. Quality of life and symptom mea-
sures in oncology: an overview. Am J Manag Care
2002;8(18 Suppl):S560–73.
[18] The World Health Organization Quality of Life as-
sessment (WHOQOL). Position paper from the
World Health Organization. Soc Sci Med 1995;41(10):
1403–9.
[19] Bonomi AE, Patrick DL, Bushnell DM,Martin M. Vali-
dation of the United States’ version of the World
Health Organization Quality of Life (WHOQOL) in-
strument. J Clin Epidemiol 2000;53(1):1–12.
[20] Naughton MJ, Shumaker SA. The case for domains
of function in quality of life assessment. Qual Life
Res 2003;12(Suppl 1):73–80.
[21] Montazeri A, Milroy R, Gillis CR, McEwen J. Quality
of life: perception of lung cancer patients. Eur J Cancer
1996;32A(13):2284–9.
[22] World Health Organization. Constitution of the world
health organization: chronicle of the world health orga-
nization 1. Geneva: WHO; 1947.
[23] Whalen GF, Ferrans CE. Quality of life as an outcome
in clinical trials and cancer care: a primer for surgeons.
J Surg Oncol 2001;77(4):270–6.
[24] Bottomley A. The cancer patient and quality of life.
Oncologist 2002;7(2):120–5.
[25] Osoba D. Lessons learned from measuring health-re-
lated quality of life in oncology. J Clin Oncol 1994;
12(3):608–16.
[26] Sprangers MA, Aaronson NK. The role of health care
providers and significant others in evaluating the qual-
ity of life of patients with chronic disease: a review.
J Clin Epidemiol 1992;45(7):743–60.
[27] Stephens RJ, Hopwood P, Girling DJ, Machin D.
Randomized trials with quality of life endpoints: are
doctors’ ratings of patients’ physical symptoms inter-
changeable with patients’ self-ratings? Qual Life Res
1997;6(3):225–36.
[28] Wilson KA, Dowling AJ, Abdolell M, Tannock IF.
Perception of quality of life by patients, partners and
treating physicians. Qual Life Res 2000;9(9):1041–52.
[29] Sneeuw KC, Sprangers MA, Aaronson NK. The role of
health care providers and significant others in evaluat-
ing the quality of life of patients with chronic disease.
J Clin Epidemiol 2002;55(11):1130–43.
[30] O’Toole BI, Battistutta D, Long A, Crouch K. A com-
parison of costs and data quality of three health survey

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365364
methods: mail, telephone and personal home interview.
Am J Epidemiol 1986;124(2):317–28.
[31] Guyatt GH, Feeny DH, Patrick DL. Measuring health-
related quality of life. Ann Intern Med 1993;118(8):
622–9.
[32] Perkins JJ, Sanson-Fisher RW. An examination of
self-and telephone-administered modes of administra-
tion for the Australian SF-36. J Clin Epidemiol 1998;
51(11):969–73.
[33] McHorney CA, Kosinski M, Ware Jr JE. Comparisons
of the costs and quality of norms for the SF-36 health
survey collected by mail versus telephone interview:
results from a national survey. Med Care 1994;32(6):
551–67.
[34] Weinberger M, Oddone EZ, Samsa GP, Landsman PB.
Are health-related quality-of-life measures affected by
the mode of administration? J Clin Epidemiol 1996;
49(2):135–40.
[35] Hawthorne G. The effect of different methods of col-
lecting data: Mail, telephone and filter data collection
issues in utility measurement. Qual Life Res 2003;
12(8):1081–8.
[36] Velikova G, Wright EP, Smith AB, Cull A, Gould A,
Forman D, et al. Automated collection of quality-of-
life data: a comparison of paper and computer touch-
screen questionnaires. J Clin Oncol 1999;17(3):
998–1007.
[37] Ryan JM, Corry JR, Attewell R, Smithson MJ. A com-
parison of an electronic version of the SF-36 General
Health Questionnaire to the standard paper version.
Qual Life Res 2002;11(1):19–26.
[38] Bliven BD, Kaufman SE, Spertus JA. Electronic col-
lection of health-related quality of life data: validity,
time benefits, and patient preference. Qual Life Res
2001;10(1):15–22.
[39] Drummond HE, Ghosh S, Ferguson A, Brackenridge
D, Tiplady B. Electronic quality of life questionnaires:
a comparison of pen-based electronic questionnaires
with conventional paper in a gastrointestinal study.
Qual Life Res 1995;4(1):21–6.
[40] Allison PJ, Locker D, Feine JS. Quality of life: a dy-
namic construct. Soc Sci Med 1997;45(2):221–30.
[41] Velikova G, Stark D, Selby P. Quality of life instruments
in oncology. Eur J Cancer 1999;35(11):1571–80.
[42] Scientific Advisory Committee of the Medical Out-
comes Trust. Assessing health status and quality-of-life
instruments: attributes and review criteria. Qual Life
Res 2002;11(3):193–205.
[43] Smith KW, Avis NE, Assmann SF. Distinguishing be-
tween quality of life and health status in quality of life
research: a meta-analysis. Qual Life Res 1999;8(5):
447–59.
[44] Nunnally JC, Bernstein IH. Psychometric theory. 3rd
edition. New York: McGraw Hill; 1994.
[45] Terwee CB, Dekker FW, Wiersinga WM, Prummel
MF, Bossuyt PM. On assessing responsiveness of
health-related quality of life instruments: guidelines
for instrument evaluation. Qual Life Res 2003;12(4):
349–62.
[46] Ware Jr JE, Sherbourne CD. The MOS 36-item short-
form health survey (SF-36). I. Conceptual framework
and item selection. Med Care 1992;30(6):473–83.
[47] McHorney CA, Ware Jr JE, Raczek AE. The MOS
36-Item Short-Form Health Survey (SF-36): II. Psy-
chometric and clinical tests of validity in measuring
physical and mental health constructs. Med Care
1993;31(3):247–63.
[48] Ferrans CE, Powers MJ. Quality of life index: develop-
ment and psychometric properties. ANS Adv Nurs Sci
1985;8(1):15–24.
[49] Gilson BS, Gilson JS, Bergner M, Bobbit RA, Kressel
S, Pollard WE, et al. The sickness impact profile. De-
velopment of an outcome measure of health care. Am
J Public Health 1975;65(12):1304–10.
[50] Bergner M, Bobbitt RA, Pollard WE, Martin DP, Gil-
son BS. The sickness impact profile: validation of a
health status measure. Med Care 1976;14(1):57–67.
[51] Bergner M, Bobbitt RA, Carter WB, Gilson BS. The
Sickness Impact Profile: development and final revi-
sion of a health status measure. Med Care 1981;19(8):
787–805.
[52] Hunt SM, McEwen J, McKenna SP. Measuring health
status: a new tool for clinicians and epidemiologists.
J R Coll Gen Pract 1985;35(273):185–8.
[53] Spitzer WO, Dobson AJ, Hall J, Chesterman E, Levi J,
Shepherd R, et al. Measuring the quality of life of
cancer patients: a concise QL-index for use by physi-
cians. J Chronic Dis 1981;34(12):585–97.
[54] Aaronson NK, Ahmedzai S, Bergman B, Bullinger M,
Cull A, Duez NJ, et al. The European Organization for
Research and Treatment of Cancer QLQ-C30: a qual-
ity-of-life instrument for use in international clinical
trials in oncology. J Natl Cancer Inst 1993;85(5):
365–76.
[55] Bergman B, Aaronson NK, Ahmedzai S, Kaasa S,
Sullivan M. The EORTC QLQ-LC13: a modular sup-
plement to the EORTC Core Quality of Life Question-
naire (QLQ-C30) for use in lung cancer clinical trials.
EORTC Study Group on Quality of Life. Eur J Cancer
1994;30A(5):635–42.
[56] Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E,
Bonomi A, et al. The Functional Assessment of Cancer
Therapy scale: development and validation of the gen-
eral measure. J Clin Oncol 1993;11(3):570–9.
[57] Morrow GR, Lindke J, Black P. Measurement of quality
of life in patients: psychometric analyses of the Func-
tional Living Index-Cancer (FLIC). Qual Life Res
1992;1(5):287–96.
[58] de Haes JC, van Knippenberg FC, Neijt JP. Measuring
psychological and physical distress in cancer patients:
structure and application of the Rotterdam Symptom
Checklist. Br J Cancer 1990;62(6):1034–8.
[59] Cella DF, Bonomi AE, Lloyd SR, Tulsky DS, Kap-
lan E, Bonomi P. Reliability and validity of the Func-
tional Assessment of Cancer Therapy-Lung (FACT-L)
quality of life instrument. Lung Cancer 1995;12(3):
199–220.
[60] Hollen PJ, Gralla RJ, Kris MG, Potanovich LM. Qual-

W.W.L. Li et al / Thorac Surg Clin 14 (2004) 353–365 365
ity of life assessment in individuals with lung cancer:
testing the Lung Cancer Symptom Scale (LCSS). Eur
J Cancer 1993;29A(Suppl 1):S51–8.
[61] Montazeri A, Gillis CR, McEwen J. Quality of life in
patients with lung cancer: a review of literature from
1970 to 1995. Chest 1998;113(2):467–81.
[62] Bottomley A, Efficace F, Thomas R, Vanvoorden V,
Ahmedzai SH. Health-related quality of life in non-
small-cell lung cancer: methodologic issues in ran-
domized controlled trials. J Clin Oncol 2003;21(15):
2982–92.
[63] Mangione CM, Goldman L, Orav EJ, Marcantonio ER,
Pedan A, Ludwig LE, et al. Health-related quality of
life after elective surgery: measurement of longitudinal
changes. J Gen Intern Med 1997;12(11):686–97.
[64] Myrdal G, Valtysdottir S, Lambe M, Stahle E. Quality
of life following lung cancer surgery. Thorax 2003;
58(3):194–7.
[65] Sarna L, Padilla G, Holmes C, Tashkin D, Brecht ML,
Evangelista L. Quality of life of long-term survivors
of non-small-cell lung cancer. J Clin Oncol 2002;
20(13):2920–9.
[66] Handy Jr JR, Asaph JW, Skokan L, Reed CE, Koh S,
Brooks G, et al. What happens to patients undergoing
lung cancer surgery? Outcomes and quality of life be-
fore and after surgery. Chest 2002;122(1):21–30.
[67] Welcker K, Marian P, Thetter O, Siebeck M. Cost and
quality of life in thoracic surgery—a health economic
analysis in a German center. Thorac Cardiovasc Surg
2003;51(5):260–6.
[68] Hazelrigg SR, Landreneau RJ, Boley TM, Priesmeyer
M, Schmaltz RA, Nawarawong W, et al. The effect
of muscle-sparing versus standard posterolateral thora-
cotomy on pulmonary function, muscle strength, and
postoperative pain. J Thorac Cardiovasc Surg 1991;
101(3):394–401.
[69] Akcali Y, Demir H, Tezcan B. The effect of standard
posterolateral versus muscle-sparing thoracotomy on
multiple parameters. Ann Thorac Surg 2003;76(4):
1050–4.
[70] DajczmanE,GordonA,KreismanH,WolkoveN. Long-
term postthoracotomy pain. Chest 1991;99(2):270–4.
[71] Hazelrigg SR, Cetindag IB, Fullerton J. Acute and
chronic pain syndromes after thoracic surgery. Surg
Clin N Am 2002;82(4):849–65.
[72] Stammberger U, Steinacher C, Hillinger S, Schmid
RA, Kinsbergen T, Weder W. Early and long-term
complaints following video-assisted thoracoscopic
surgery: evaluation in 173 patients. Eur J Cardiothorac
Surg 2000;18(1):7–11.
[73] Li WW, Lee TW, Lam SS, Ng CS, Sihoe AD, Wan IY,
et al. Quality of life following lung cancer resection:
video-assisted thoracic surgery vs thoracotomy. Chest
2002;122(2):584–9.
[74] Dales RE, Belanger R, Shamji FM, Leech J, Crepeau
A, Sachs HJ. Quality-of-life following thoracotomy
for lung cancer. J Clin Epidemiol 1994;47(12):1443–9.
[75] Chen JC, Johnstone SA. Quality of life after lung can-
cer surgery: a forgotten outcome measure. Chest 2002;
122(1):4–5.
[76] Zieren HU, Muller JM, Hamberger U, Pichlmaier H.
Quality of life after surgical therapy of bronchogenic
carcinoma. Eur J Cardiothorac Surg 1996;10(4):233–7.
[77] Sugiura H, Morikawa T, Kaji M, Sasamura Y, Kondo
S, Katoh H. Long-term benefits for the quality of life
after video-assisted thoracoscopic lobectomy in pa-
tients with lung cancer. Surg Laparosc Endosc Percu-
tan Tech 1999;9(6):403–8.

Thorac Surg Clin 14 (2004) 367–374
Quality of life after esophageal surgery
Hiran C. Fernando, MD, FRCS, FACS, James D. Luketich, MD, FACS*
Division of Thoracic and Foregut Surgery, University of Pittsburgh Medical Center, 200 Lothrop Street, Suite C-800,
Pittsburgh, PA 15213, USA
Maintaining an acceptable quality of life (QOL) is One of the oldest instruments to measure QOL is
a key factor after any surgical operation; however, for
diseases of the esophagus, QOL assumes unparalleled
importance compared with other organs because
nutritional intake is so crucial to patient satisfaction.
The incidence of adenocarcinoma of the esophagus is
increasing significantly in the Western world. Most
patients will have significant impairment of QOL
because of the dysphagia associated with an obstruct-
ing tumor. Although esophagectomy can improve
QOL [1], concerns over the high morbidity and
mortality associated with this operation have led to
a reluctance by some physicians to refer patients to
surgery, and in some cases nonresectional treatments
such as photodynamic therapy are favored [2,3].
QOL is also a key issue when treating benign
esophageal diseases. In contrast to esophageal cancer,
in which palliation of dysphagia and cure are impor-
tant issues, gastroesophageal reflux disease (GERD)
is a disease that primarily affects QOL. A number of
new treatment modalities are becoming available for
GERD [4]. As these are introduced into clinical
practice, QOL measurement should be an important
part of their evaluation.
Despite the importance of QOL, this outcome
measure is rarely measured in surgical practice. Most
surgical publications typically report only standard
outcomes such as mortality and morbidity. This can,
in part, be explained by the lack of a gold standard
instrument to measure QOL and the perception that
QOL measurement is difficult to define objectively
and too time-consuming to collect.
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00024-6
* Corresponding author.
E-mail address: [email protected] (J.D. Luketich).
the Karnofsky index [5,6]. This venerable tool has
been most useful to measure performance status and
predict ability to tolerate therapy in oncology patients;
however, it is insufficient in many aspects because it
exclusively evaluates physical functioning and does
not give significant weight to other domains of QOL.
Another disadvantage of the Karnofsky index is its
reliance on an observer’s assessment of a patient’s
level of independence and activity rather than the
patient’s own assessment of their QOL.
Recently, a number of newer instruments have
been developed to measure QOL. These include the
Sickness Impact Profile [7], the Functional Living
Index in Cancer [8], and the MOS-SF36 [9]. These
newer instruments all rely on subjective assessment
by the patient rather than assessment by a potentially
biased observer. Subjective assessment of QOL by
the patient rather than objective evaluation by a
doctor or other caregiver has been demonstrated to
provide a more accurate assessment of QOL [10].
This article provides an overview of instruments
used to measure QOL and their increasing application
following esophageal surgery for cancer and GERD.
Overview of quality of life instruments
QOL is a concept that is easy to grasp intuitively
but difficult to measure reliably. In the everyday sense
of the phrase, QOL can include such aspects as
personal income, location of residence, leisure time
and activities, interpersonal relationships, meaningful
work, and spiritual fulfillment, among other nonmedi-
cal aspects of life. In medicine, however, what one
attempts to assess is health-related QOL (HRQOL),
which measures the impact of disease on physical,
s reserved.

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374368
psychological, and social health. The World Health
Organization previously defined QOL as an absence
of infirmity and a state of physical, social, and mental
well-being [11]. Although these definitions might be
obvious, their measurement might not be.
QOL instruments have internal characteristics that
should be assessed more rigorously. These qualities
include reliability, validity, responsiveness, appropri-
ateness, practicality, and interpretability. Reliability
implies that the instrument must produce the same
result on repeated assessment of the same level of
QOL. Validity implies that the instrument measures
what it is purported to measure. Responsiveness (sen-
sitivity to change) is the ability of the instrument to
detect clinically important changes in QOL as a result
of treatment or over time. The appropriateness of an
instrument depends on how well the instrument
measures the relevant aspects of QOL for a given
health problem. Practicality reflects the ease with
which the instrument can be used by health care
professionals and patients. Interpretability is how
well the result of the questionnaire can be understood
by the clinician using the results. All of these factors
should be considered when selecting a QOL instru-
ment for use in clinical practice or research.
QOL instruments can generally be categorized as
generic or disease-specific. Generic instruments mea-
sure global QOL and are broadly applicable across
several diseases, whereas disease-specific instruments
assess specific diagnostic groups to measure clinically
important changes within these diseases. This sensi-
tivity to change (responsiveness) might be one of the
most important characteristics of instruments used to
evaluate the effects of treatments. The advantages of
a generic instrument are that a single instrument can be
used in several settings, detecting differential effects
on the various aspects of health status, and that
comparisons after interventions for different diseases
are possible. Additionally, generic instruments allow
comparisons to normal populations and patients who
have other chronic diseases. The disadvantages of
generic instruments are that they might not focus ade-
quately on an area of interest (eg, severity of symp-
toms) and they might not be responsive enough (ie,
might not measure changes as a result of an interven-
tion), which might be important for a study on the
effects of a particular treatment. Disease-targeted
instruments focus on a specific condition and its re-
lated symptoms. The specificity of condition-specific
instruments can increase their responsiveness to detect
small treatment changes over time; however, many of
these instruments have not been as extensively vali-
dated by longitudinal studies, as generic instruments
have. Many practitioners are reluctant to use a variety
of instruments for multiple disease types (eg, a spe-
cific questionnaire for each digestive disease).
A third group of QOL instruments are those that
measure specific symptoms. These instruments do
not take into consideration other QOL issues such
as social interactions or psychological stresses; how-
ever, these are still of value if a primary endpoint of
treatment or a common major complication of treat-
ment is the symptom being evaluated. The authors
have previously used symptom-specific instruments
to evaluate dysphagia after esophagectomy [12] or
photodynamic therapy [3] and pain severity after
thoracotomy [13].
Generic quality of life instruments
Probably the most well known generic instrument
is the Medical Outcomes Study Short Form 36 (SF36)
[9]. This instrument was originally developed by John
Ware and the Medical Outcomes Trust and has gained
increasing popularity in several clinical settings. This
36-item questionnaire has been validated extensively
and normal values for various populations have been
well defined. When originally developed, scores were
expressed as eight domains of QOL, including physi-
cal functioning, role physical, bodily pain, general
health, vitality, social functioning, role emotional, and
mental health. Subsequently, these eight-domain
scores were combined into two scores [14], a physical
component summary (PCS) and mental component
summary (MCS) score.
The SF36 has become one of the most popular
and widely used QOL instruments in the United
States and worldwide, with several foreign trans-
lations available.
The Psychological General Well-Being Index
(PGWB) was developed to measure subjective well-
being or distress [15]. Since its introduction in 1984 it
has been used in many studies, including the evalua-
tion of QOL in upper gastrointestinal diseases [16].
It assesses six dimensions of QOL: anxiety, depressed
mood, positivewell-being, self-control, general health,
and vitality. These are then combined to give an overall
score. This instrument has been popular in several
European studies of GERD.
Disease-specific instruments used to evaluate
gastroesophageal reflux disease and esophageal
cancer
The Gastrointestinal Symptom Rating Scale
(GSRS) was constructed initially to measure severity

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374 369
of symptoms in peptic ulcer disease and irritable
bowel syndrome [16]. It is a seven-grade Likert scale
questionnaire that contains 15 items. It has been
found to be satisfactory with respect to internal con-
sistency, validity, and responsiveness. It has been
used to assess GERD and seems to be adequate for
this purpose [17].
The Gastroesophageal Reflux Disease–Health
Related Quality of Life Scale (HRQOL) was devel-
oped by Velanovich to assess GERD severity [18].
The HRQOL is a disease-specific instrument that
consists of 10 questions. Nine questions relate to
different aspects of GERD with each response scored
from 0 to 5. The best possible score is 0 (no sym-
ptoms) and the worst possible score is 5 (most severe
symptoms). The tenth question relates to an overall
assessment of satisfaction. In a study comparing the
HRQOL to the SF36 performed in 43 patients who
had GERD, 59% of patients preferred the HRQOL,
62% felt it was easier to understand, and 86% felt
it was more reflective of their symptoms [19].
The authors’ group’s preference has been to use the
HRQOL in combination with the SF36 because the
authors feel that the combination of a disease spe-
cific and generic instrument is advantageous [20].
Another instrument, the Reflux-Related Visual Ana-
logue Scale, has been developed recently. Data about
its validity and reliability have yet to be published,
although Blomqvist et al [21] showed that there is a
good correlation with specific symptoms of GERD
assessed preoperatively and after antireflux surgery.
The European Organization for Research and
Treatment of Cancer (EORTC) has developed a
disease-specific instrument for application in esopha-
geal cancer [22]. This instrument uses an esophageal
module (QLQ-OES18) with items specific to aspects
of esophageal cancer. The esophageal module is used
in combination with the EORTC core questionnaire
(the QLQ-C30). The QLQ-C30 has been used previ-
ously for lung, breast, and ovarian cancer [23].
Quality of life measurement in esophageal cancer
Comparison of esophagectomy to palliative treatment
of esophageal cancer
A few studies have compared QOL after palliative
treatment and resection of esophageal cancer. As may
be expected, one of the concerns with this approach is
that patients who receive palliative care tend to be
older and have poorer baseline QOL scores [24]. In a
study of 69 patients who underwent resection or
palliation with radiation and stent placement, QOL
was measured using a cancer-specific scale (Rotter-
dam Symptom Checklist) and a dysphagia score [24].
After treatment, QOL scores initially deteriorated in
both groups, but at 16 weeks improvements were
seen in the resection group only. Dysphagia scores
improved in both groups at 6 weeks, but at 16 weeks
further improvements were seen in the surgical
group only.
Another study involved 59 patients who under-
went esophagectomy and 26 who were palliated with
radiation with or without stent placement. This study
used the QLQ-C30 and a dysphagia score [25].
Statistically significant differences were found be-
tween the two groups with respect to the physical,
emotional, and cognitive function scores, favoring the
resection patients. Additionally, posttreatment dys-
phagia scores were worse in the patients who had
palliative treatment only. The dysphagia scores did
not correlate with any of the individual QOL scales or
items, indicating that although dysphagia is an im-
portant issue, other factors contribute to overall
QOL in esophageal cancer. Although these studies
are biased in favor of the functionally better surgical
groups, the superior results with esophagectomy sup-
port the role of esophagectomy in providing palliation
and relief of dysphagia when feasible.
Outcome after open esophagectomy
A study by Wong et al [1] compared 49 patients
who underwent curative open esophagectomy (OE)
to 39 patients who underwent palliative OE. There
were no significant differences between these groups
with respect to preoperative risk factors, although
Eastern Cooperative Oncology Group (ECOG) per-
formance status was worse in the palliative group
preoperatively. Although pain and overall QOL scores
were worse in the palliative group at 9 months, there
were no differences with regard to sleep and leisure
activity between the groups. Additionally, the type and
quantity of oral intake improved significantly in both
groups after surgery with no differences seen at 18
months of follow-up care. This study again demon-
strates the positive impact of esophagectomy on QOL
even if resection is incomplete.
Esophagectomy is a complex and challenging
operation. Total morbidity rates are usually not docu-
mented in surgical series, but when they are reported
they appear to be around 60% [26,27]. The signifi-
cant physiological challenges to the patient and the
possibility of increased morbidity after esophagec-
tomy lead clinicians to expect that QOL will initially
decrease during the immediate postoperative period

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374370
but will improve eventually. A few studies have
addressed the issue of intermediate and long-term
follow-up care after OE. Zieran et al [28] followed a
cohort of 30 patients over a 1-year period using the
EORTC QOL questionnaire and the Spitzer index
after OE. All patients had curative operations and
were disease-free during this 12-month period Dys-
phagia was the most severe symptom before surgery
and had improved by discharge from the hospital.
Global QOL, however, deteriorated significantly after
operation and did not recover until about 6 months
after operation. At 12 months, QOL scores were
slightly higher than preoperative values. A study by
Blazeby et al [27] used the QLQ-C30 and the EORTC
QLQ-OES24 in 17 patients who survived for at least
2 years after OE and compared these to 38 patients
who survived for less than 2 years after OE. At
6 weeks all patients reported decreased functional,
symptom, and global QOL scores compared with
preoperative scores. In both groups dysphagia im-
proved after surgery and was maintained until death
or the duration of the study. In the patients who
died within 2 years, former QOL levels were never
regained, whereas in patients who survived for more
than 2 years, QOL scores had recovered by 9 months
after operation.
Probably the best-reported long-term QOL data
come from the Mayo clinic experience [29]. They
reported on 107 patients who had survived for 5 or
more years after OE. The median survival time was
10.2 years. At the time of follow-up, 60% of patients
complained of reflux, 53% of dumping, and 25% of
dysphagia to solid food. Only 17% were completely
asymptomatic. A cervical anastomosis was associated
with significantly (P < 0.05) less reflux, and dumping
occurred more frequently (P < 0.05) in younger
patients and women. QOL was measured using the
SF36. Physical function scores were significantly less
than national norms; however, scores measuring abil-
ity to work, social interaction, daily activity, emotional
dysfunction, and health perception were similar to
national norms. Surprisingly, mental health scores
were better than national norms. This study illustrates
that even though a high percentage (83% in this study)
of long-term survivors after OE will complain of
gastrointestinal symptoms such as reflux or dumping,
most aspects of QOL will still be preserved.
The Mayo clinic also reviewed their long-term
follow-up care after OE with a preoperative diagnosis
of high-grade dysplasia [26]. This is a challenging
group of patients because most will be relatively
asymptomatic compared with patients who have more
advanced cancers. There were 54 patients in this
series, of whom 35% were found to have an invasive
cancer. Using the SF36 they found that the role
physical and role emotional scores in the high-grade
dysplasia patients were better than norms, whereas
the patients who had cancer had poorer health per-
ception scores. Physical function, social function,
mental health, bodily pain, and energy/fatigue were
similar. Despite the high operative morbidity (57%)
seen in this group of patients, the findings of a 35%
incidence of unsuspected cancer and the acceptable
QOL seen at follow-up support the role of resection
for patients who have high-grade dysplasia.
Outcomes after minimally invasive esophagectomy
A number of approaches to esophagectomy are
used by surgeons. The mortality from OE has been
reported to be in the range of 6% to 7% in published
series [30]. It appears that mortality is related to the
experience and volume of esophagectomy cases per-
formed at individual centers rather than the approach
used. In a report summarizing nationwide statistics,
mortality ranged from 8% in high-volume centers to
as high as 23% in low-volume centers [31]. In view
of the high chance of morbidity and mortality, it is
perhaps not surprising that some patients might be
treated nonoperatively without evaluation by a sur-
geon. The authors’ group explored the role of mini-
mally invasive esophagectomy and now favors this
approach to esophagectomy. The authors recently
published the results of their first 222 cases [12].
The authors’ standard approach includes a right
video-assisted thoracic surgery (VATS) mobilization
of the thoracic esophagus combined with a lapa-
roscopic transhiatal approach and neck anastomosis
[12]. Minimally invasive esophagectomy (MIE)
offers the potential to lower morbidity and allow
quicker return to normal function than OE. If mor-
tality and morbidity are reduced, a greater number of
patients might be referred and benefit from MIE. In
the authors’ series of 222 patients, mortality occurred
in 1.4% of patients and major morbidity occurred in
32%. The median hospital stay was 7 days, which is
lower than that reported in most series of OE. QOL
was measured using the SF36 and dysphagia was
measured using a scale from 0 (no dysphagia) to
5 (severe dysphagia). Because reflux is often reported
after esophagectomy [29], the authors also recorded
heartburn severity using the HRQOL [18]. At a mean
follow-up of 19 months the mean HRQOL score was
4.6, which represents a normal (no reflux) score.
Only 4% of patients complained of significant reflux
(HRQOL score �15), supporting the continued use of
a neck anastomosis. SF36 scores were compared with

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374 371
age-matched norms. PCS scores were not significantly
different, whereas MCS scores were slightly but
statistically (P = 0.001) lower than United States
norms (49.67 versus 52.68). Pre- and postoperative
scores were only available in 57 patients. In these
patients PCS and MCS scores were not significantly
different from preoperative values, suggesting preser-
vation of QOL. Dysphagia scores were excellent
(mean 1.4). The authors previously reviewed the
results of MIE in a cohort of 41 patients aged 75 years
or older [32]. There were no preoperative deaths,
major morbidity occurred in 19% of patients, and
median length of stay was 7 days. These data also
support the use of MIE in older patients who have
esophageal cancer.
Based on these data the authors believe that MIE
(performed in centers experienced in minimally in-
vasive surgical techniques and malignant esophageal
surgery) is a good therapeutic option that can be
performed with acceptable morbidity and mortality
and result in a preserved QOL.
Quality of life measurement in gastroesophageal
reflux disease
Quality of life measurement after surgical therapy of
gastroesophageal reflux disease
Laparoscopic fundoplication has been shown to
be a safe procedure that can be performed with ac-
ceptable results; however, the role of the operation
remains controversial and continues to be debated in
the literature. Before the routine use of laparoscopic
fundoplication, a study by Pope demonstrated the
benefits of open fundoplication on QOL [33]. Over
the last 12 years, larger and larger series of laparo-
scopic fundoplication have been reported using QOL
measures. In an earlier study, QOL measurements
using the PGWB index (generic) and the GSRS (dis-
ease-specific) were reported in 40 patients and dem-
onstrated improvement after operation [34]. More
recently, reports of 300 patients (using the SF36)
and 500 patients using another disease-specific in-
strument, the Gastrointestinal Quality of Life Index,
have been reported [35,36]. These single-center
studies demonstrated improved QOL after operation.
A study from Pittsburgh used a disease-specific GERD
score, symptom-specific heartburn and dysphagia
scores, in 297 patients before and after operation
[37]. At a mean follow-up of 31.4 months, symp-
tom-specific and disease-specific scores improved,
with only 10% of patients requiring proton pump
inhibitor (PPI) for typical GERD symptoms.
Other studies have compared open and laparo-
scopic approaches. In one nonrandomized study
Bloomqvist compared open and minimally invasive
approaches, with similar outcomes demonstrated be-
tween groups [21]. In another study Velanovich [38]
compared open and laparoscopic antireflux operation
and found superior physical function and bodily pain
scores at 6 weeks in the laparoscopic group, indicat-
ing that these patients had a quicker recovery com-
pared with patients who underwent open operation.
The group from the University of Southern California
used the SF36 to compare 72 patients who had a
laparoscopic Nissen fundoplication to 33 patients
who had more complex hiatal hernias and strictures
who underwent transthoracic Nissen fundoplication
[39]. Although the laparoscopic group recovered
more quickly with less postoperative discomfort at
long-term follow-up, QOL scores were similar and
were only significantly decreased for patients who
(not surprisingly) had recurrent reflux symptoms. The
laparoscopic group was more likely to use acid
suppression medications and tended to be less satis-
fied, arguing that an open operation is preferred, at
least for patients who have advanced gastroesopha-
geal reflux disease.
The authors’ group has previously reported their
experience with 200 giant hiatal hernia repairs per-
formed laparoscopically [40]. These complex hiatal
hernias had at least 30% of the stomach within the
mediastinum. In most cases, in the later part of the
series, a laparoscopic Collis gastroplasty was per-
formed because the authors believe that this proce-
dure helps prevent problems with recurrence of the
hernia when a shortened esophagus is present [41].
HRQOL was used to evaluate patients in follow-up
(mean scores 2.4), and scores were felt to be in the
excellent or good range in 92% of patients.
Another group of patients who have complex
GERD are patients who have previously undergone
antireflux operation. It is often argued that these
complex operations should be approached using open
techniques because results will be worse than with
primary repair and have been reported ranging from
66% to 76% [42]; however, if the same principles as
open surgery are employed (ie, full workup of the
patient preoperatively, complete takedown of the
previous repair, assessment for the presence of a
shortened esophagus with appropriate use of a Collis
gastroplasty), results will be as good as with an open
operation. The authors’ series of 80 laparoscopic
reoperations included the use of the SF36, HRQOL,
and a dysphagia score ranging from 1 (no dysphagia)
to 5 (severe dysphagia—unable to tolerate saliva) at a
mean follow-up period of 18 months [43]. SF36 PCS

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374372
and MCS scores were similar to normal values and
mean HRQOL scores were 6, which is within the
normal range. Dysphagia scores improved signifi-
cantly (from 2 to 1.3) and only 18% of patients
reported that they were dissatisfied.
Age is sometimes felt to be a contraindication to
laparoscopic antireflux surgery. GERD primarily af-
fects QOL, and the operation might have a significant
positive effect even in the elderly, higher surgical risk
patient who has severe GERD. The authors recently
compared outcomes between an older and younger
group of patients, all of whom had complete fundo-
plications [44]. Despite a longer length of stay in the
older population, follow-up HRQOL, SF36, and
dysphagia scores were excellent and similar between
the two groups of patients, supporting the role of the
operation for older patients.
Medical versus surgical therapy: how does quality
of life compare?
This question continues to be an area of intense
discussion, particularly with the introduction of
newer medications and the increasing availability of
the laparoscopic antireflux operation. In one of the
few randomized studies that have been reported, open
fundoplication was compared with medical therapy
using histamine-2 antagonist (H2A) in a multicenter
Veteran’s Administration (VA) setting [45]. Patients
in this study maintained a diary of symptoms to
construct a gastroesophageal reflux disease activity
index (GRACI). In the initial report from this study
with 2-year follow-up, the mean activity index and
grade of esophagitis were better in the surgical group.
A follow-up study on these patients was published
recently [46]. The median follow-up period was
7.3 years for the medical group and 6.3 years for the
surgical group, with follow-up available in 91 medical
and 38 surgical patients. Follow-up included use of
the SF36 and the GRACI. A large number of the
surgical patients (62%) required antireflux medica-
tions; however, this number was still significantly
lower than the proportion of medical patients requir-
ing antireflux medications (92%). GRACI scores and
SF36 bodily pain scores were significantly better in
the surgical group. Another randomized study from
Sweden compared open fundoplication to PPI with
5 years of follow-up [47]. In this study the PGWB
(generic instrument) and the GSRS (disease-specific)
were used. QOL scores were found to be similar
between the groups. There were more treatment fail-
ures in the medical group, although when higher-dose
omeprazole was used this difference did not reach
statistical significance.
The authors’ group compared patients undergoing
medical therapy to patients undergoing laparoscopic
antireflux operations [20]. The study population in-
cluded all patients presenting with a primary diagno-
sis of reflux to the gastroenterology or surgical clinic
during a 1-year period. Despite the surgical group
demonstrating more severe reflux (based on greater
usage of PPI and propulsid) before therapy, results
were better in the surgical cohort. Reflux severity
using the HRQOL was 4 in the surgical group versus
21 in the medical group. SF36 scores were signifi-
cantly better in six of the eight domains of QOL in
the surgical group.
Summary
QOL measurement is being reported with increas-
ing frequency in the surgical literature. The authors
and others have found that the use of a generic
instrument such as the SF36 used in combination
with a disease-specific instrument will provide the
most comprehensive information. GERD is a signifi-
cant health problem that primarily affects the QOL
of a large segment of the population. New therapies
for GERD continue to be developed and introduced
into clinical practice. QOL assessment should be an
important part of the evaluation of these new thera-
pies. Similarly, the management of esophageal cancer
and high-grade dysplasia is also controversial. QOL
assessment should be a crucial factor in determining
which surgical or nonoperative approach is used for
these patients
References
[1] Branicki FJ, Law SY, Fok M, Poon RT, Chu KM,
Wong J. Quality of life in patients with cancer of the
esophagus and gastric cardia. Arch Surg 1998;133:
316–22.
[2] Wang KK. Photodynamic therapy of Barrett’s esopha-
gus. Gastrintest Endosc Clin N Am 2000;10:409–19.
[3] Litle VR, Luketich JD, Christie NA, Buenaventura
PO, Alvelo-Rivera M, McCaughan JS, et al. Photo-
dynamic therapy as palliation for esophageal cancer:
experience in 215 patients. Ann Thorac Surg 2003;76:
1687–92.
[4] De Hoyas A, Fernando HC. Endoscopic therapies in
reflux disease. Prob Gen Surg; in press.
[5] Karnofsky DA, Abelmann WH, Craver LF, et al. The
use of the nitrogen mustards; in the palliative treatment

H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374 373
of carcinoma.With particular reference to bronchogenic
cancer. Cancer 1948;1:634–56.
[6] Ganz PA, Lee JJ, Siau J. Quality of life assessment. An
independent prognostic variable for survival in lung
cancer. Cancer 1991;67:3131–5.
[7] Selby PJ, Chapman JAW, Etazdi-Amoli J, et al. The
development of a method for assessing the quality of
life in cancer patients. Br J Cancer 1984;50:13–22.
[8] Shipper H, Clinch J, McMurry A, et al. Measuring the
quality of life of cancer patients: the Functional Living
Index–Cancer: development and validation. J Clin
Oncol 1984;2:472–83.
[9] Ware JE, Sherbourne CD. TheMOS 36-item short-form
health survey (SF-36). Med Care 1992;30:473–83.
[10] Blazeby JM, Williams MH, Alderson D, Farndon JR.
Observer variation in assessment of quality of life in-
patients with esophageal cancer. Br J Surg 1995;82:
1200–3.
[11] World Health Organization. The constitution of the
WHO. WHO Chron 1947;1:29.
[12] Luketich JD, Alvelo-Rivera M, Buenaventura PO,
Christie NA, McCaughan JS, Litle VR, et al. Minimally
invasive esophagectomy: outcomes in 222 patients.
Ann Surg 2003;238:486–94.
[13] Luketich JD, Sullivan EA, Alvelo-Rivera M, Ward JA,
Land S, Landreneau RJ. et al. A randomized prospec-
tive trial of thoracic epidural (EPI) versus intercostals
nerve catheter plus patient-controlled analgesia (ICN–
PCA) with morphine for pain control following thora-
cotomy [abstract]. Presented at the Society Thoracic
Surgeons 40th Annual Meeting, 2004.
[14] Ware Jr JE, Kosinski M, Keller SD. SF-36 physical
and mental health summary scales: a user’s manual.
Boston: The Health Institute, New England Medical
Center; 1994.
[15] Dupuy HJ. The Psychological General Well-Being
(PGWG) Index. In: Wenger NK, Mattson ME, Furberg
CF, Elinson J, editors. Assessments of quality of life in
clinical trials of cardiovascular therapies. New York:
Le Jacq Publishing; 1984. p. 170–83.
[16] Svedlund J, Sjodin I, Dotevall G. GSRS-a clinical rat-
ing scale for gastrointestinal symptoms in patients with
irritable bowel syndrome and peptic ulcer disease. Dig
Dis Sci 1988;33:129–34.
[17] Dimenas E, Glise H, Hallerback B, Hernqvist H, Sved-
lund J, Wiklund I. Quality of life in patients with upper
gastrointestinal symptoms. An improved evaluation of
treatment regoimens? Scan J Gastroenterol 1993;28:
681–7.
[18] Velanovich V, Vallance SR, Gusz JR, Tapia FV, Har-
kabus MA. Quality of life scale for gastroesophageal
reflux disease. J Am Coll Surg 1996;183:217–24.
[19] Velanovich V. Comparison of generic (SF36) vs dis-
ease-specific (GERD-HRQOL) quality of life scales
for gastroesophageal reflux disease. J Gastrointest Surg
1998;2:141–5.
[20] Fernando HC, Schauer PR, Rosenblatt M, Wald A,
Buenaventura P, Ikramuddin S, et al. Quality of life
after antireflux surgery compared with non-operative
management for severe gastroesophageal reflux dis-
ease. J Am Coll Surg 2002;194:23–7.
[21] Blomqvist A, Lonroth H, Dalenback J, Ruth M,
Wiklund I, Lundell L. Quality of life assessment after
laparoscopic and open fundoplications: result of a pro-
spective, clinical study. Scan J Gastroenterol 1996;31:
1052–8.
[22] Blazeby JM, Conroy T, Hammerlid E, Fayers P, Sezer
O, Koller M, et al. Clinical and psychometric validation
of an EORTC questionnaire module, the EORTCQLQ-
OES18, to assess quality of life in patients with oeso-
phageal cancer. Eur J Cancer 2003;39(10):1384–94.
[23] Osoba D, Zee B, Pater J, Warr D, Kaizer L, Laitreille J.
Psychomotor properties and responsiveness of the
EORTC quality of life questionnaire (QLQ-C30) in
patients with breast, ovarian and lung cancer. Qual Life
Res 1994;3:353–64.
[24] O’Hanlon DM, Harkin M, Karat D, Sergeant T, Hayes
N, Griffin SM. Quality-of-life assessment in patients
undergoing treatment for esophageal carcinoma. Br J
Surg 1995;82:1682–5.
[25] Blazeby JM, Williams MH, Alderson D, Farndon JR.
Observer variation in assessment of quality of life in
patients with esophageal cancer. Br J Surg 1995;82:
1200–3.
[26] Headrick JR, Nichols FC, Miller DM, Allen MS, Tras-
tek VF, Deschamps C, et al. High-grade esophageal
dysplasia: long-term survival and quality of life after
esophagectomy. Ann Thorac Surg 2002;73:1697–703.
[27] Blazeby JM, Farndon JR, Donovan J, Alderson D. A
prospective longitudinal study examining the quality
of life in patients with esophageal carcinoma. Cancer
2000;88:1781–7.
[28] Zieran HU, Jacobi CA, Zieran J, Muller JM. Quality
of life following resection of esophageal carcinoma.
Br J Surg 1996;83:1772–5.
[29] McLarty A, Deschamps C, Trasek V, Allen MS, Pairo-
lero PC, Harmsen WS. Esophageal resection for can-
cer of the esophagus: long-term function and quality
of life. Ann Thorac Surg 1997;631:568–72.
[30] Kelsen DP, Ginsberg R, Pajak TF, et al. Chemotherapy
followed by surgery compared with surgery alone for
localized esophageal cancer. N Engl J Med 1998;339:
1979–84.
[31] Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hos-
pital volume and surgical mortality in the United
States. N Engl J Med 2002;346:1128–37.
[32] Perry Y, Fernando HC, Buenaventura PO, Christie NA,
Luketich JD. Minimally invasive esophagectomy in
the elderly. JSLS 2002;6:299–304.
[33] Pope II CE. The quality of life following antireflux
surgery. World J Surg 1992;6:335–58.
[34] Glise H, Hallerback B, Johannon B. Quality of life
assessments in evaluation of laparoscopic Rosetti fun-
doplication. Surg Endosc 1995;9:183–9.
[35] Hunter JG, Trus TL, Branum GD, Pasiut M, Wykypiel
Jr H, Herrmann R, et al. A physiological approach to
laparoscopic fundoplication for gastroesophageal re-
flux disease. Ann Surg 1996;223:673–87.
H.C. Fernando, J.D. Luketich / Thorac Surg Clin 14 (2004) 367–374374
[36] Kamolz T, Granderath FA, Bammer T, et al. Mid and
long-term quality of life assessments after laparoscopic
fundoplication and refundoplication: a single unit re-
view of more than 500 antireflux procedures. Dig Liver
Dis 2002;34:470–6.
[37] Papasavas PK, Keenan RJ, Yeaney WW, Caushaj PF,
Gagne DJ, Landreneau RJ. Effectiveness of laparo-
scopic fundoplication in relieving the symptoms of
gastroesophageal reflux disease (GERD) and elimi-
nating antireflux medical therapy. Surg Endosc 2003;
8:1200–5.
[38] Velanovich V. Comparison of symptomatic and quality
of life outcomes of laparoscopic versus open antireflux
surgery. Surgery 1999;126:782–9.
[39] Streets CG, DeMeester SR, DeMeester TR, Peters JH,
Hagen JA, Crookes PF, et al. Excellent quality of life
after Nissen fundoplication depends on successful
elimination of reflux symptoms and not the invasive-
ness of the surgical approach. Ann Thorac Surg 2002;
74:1019–25.
[40] Pierre AF, Luketich JD, Fernando HC, Christie NA,
Buenaventura PO, Litle VR, et al. Results of lapa-
roscopic repair of giant paraesophageal hernias:
200 consecutive patients. Ann Thorac Surg 2002;74(6):
1909–15.
[41] Luketich JD, Grondin SC, Pearson FG. Minimally in-
vasive approaches to acquired shortening of the esopha-
gus: laparoscopic Collis-Nissen gastroplasty. Semin
Thorac Cardiovasc Surg 2000;12:173–8.
[42] Siewert JR, Isolauri J, Feussner H. Reoperation fol-
lowing failed fundoplication. World J Surg 1989;13:
791–7.
[43] Luketich JD, Fernando HC, Christie NA, Buenaven-
tura PO, Ikramuddin S, Schauer PR. Outcomes after
minimally invasive reoperation for gastroesophageal
reflux disease. Ann Thorac Surg 2002;74(2):328–31.
[44] Fernando HC, Schauer PR, Buenaventura PO, Christie
NA, Close JM, Luketich JD. Outcomes of minimally
invasive antireflux operations in the elderly: a compar-
ative review. JSLS 2003;7(4):311–5.
[45] Spechlar SJ. Comparison of medical and surgical ther-
apy for complicated gastroesophageal reflux disease in
veterans. N Engl J Med 1992;326:786–92.
[46] Spechlar SJ, Lee E, Ahnen D, Goyal RK, Hirano I,
Ramirez F, et al. Long-term outcome of medical and
surgical therapies for gastroesophageal reflux disease.
Follow-up of a randomized controlled trial. JAMA
2001;285:2331–8.
[47] Lundell L, Miettinen P, Myrvold HE, Pederson SA,
Liedman B, Hatlebakk JG, et al. Continued (5-year)
follow-up of a randomized clinical study comparing
antireflux surgery and omeprazole in gastroesophageal
reflux disease. J Am Coll Surg 2001;192:172–81.

Thorac Surg Clin 14 (2004) 375–383
Quality of life after lung volume reduction surgery
Douglas E. Wood, MD
Section of General Thoracic Surgery, Lung Cancer Research, University of Washington, Box 356310, 1959 NE Pacific,
AA-115, Seattle, WA 98195-6310, USA
Chronic obstructive pulmonary disease (COPD) therapies for emphysema, the most recent of which
is a heterogeneous disease manifested by airflow
obstruction and hyperinflation. Patients with emphy-
sema compose a subset of COPD patients in which
loss of elastic retraction on the terminal bronchioles
results in abnormal permanent enlargement of the
airspaces and destruction of the alveolar walls. The
resulting airflow obstruction and hyperinflation re-
sult in increased work of breathing and inefficient
use of respiratory muscles. There is a simultaneous
loss of the alveolar capillary membrane, decreasing
the area of gas exchange. These physiologic changes
all can be quantified by various measures of pulmo-
nary function. Patients typically have a marked de-
crease in expiratory flow volumes and diffusing
capacity, combined with overinflation of the lung
volumes measured by plethysmography. These
physiologic changes are reflected in a diminishing
functional capacity of the emphysema patient, most
commonly measured by the 6-minute walk test or
exercise studies. These commonly measured variables
of pulmonary function and exercise capacity act only
as easily measurable surrogates for quality of life
(QOL), however.
In general, patients remain asymptomatic until
fairly profound decreases occur in pulmonary func-
tion. Despite medical therapy, in patients with ad-
vanced disease, function deteriorates episodically but
relentlessly. The increased work of breathing leads
to progressive dyspnea, which subsequently leads to
progressive inactivity and physical deconditioning. A
vicious cycle ensues with patients disabled by breath-
lessness, fatigue, irritability, and depression. It is this
spectrum of symptoms that are the target of palliative
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00029-5
E-mail address: [email protected]
is lung volume reduction surgery (LVRS).
The modern era of LVRS was initiated in the early
1990s by Cooper et al [1] at Washington University.
Using a median sternotomy to perform bilateral sta-
pled wedge resections on patients with heterogeneous
emphysema and hyperinflation resulted in an objec-
tive improvement in forced expiratory volume in
1 second (FEV1) of 82%. This improvement led to a
rapid dissemination of LVRS with initial publications
confirming objective improvement in FEV1 and the
6-minute walk test. These initial results have been
refined and confirmed by additional case-control
series [2–5], randomized studies [6–11], and the
multi-institutional prospective randomized National
Emphysema Treatment Trial (NETT) [12]. Cooper
et al [1] correctly identified health-related quality of
life (HRQOL) as the most important outcome af-
fected by LVRS and examined QOL measures pro-
spectively in patients undergoing LVRS at
Washington University. Other authors have variably
examined HRQOL after lung reduction surgery, more
commonly reporting the more easily measured objec-
tive variables of pulmonary function and exercise
capacity. A variety of disease-specific and generic
instruments for measurement of QOL have been used
and increasingly reported as the most important
clinical outcome after LVRS.
Because the relationship between spirometric and
exercise measures and QOL are indirect and nonlin-
ear, it is important to examine HRQOL as a primary
outcome measure after LVRS. Although patients with
more severe spirometric limitations might be expected
to have the most dyspnea, patients with similar FEV1
values may have different degrees of symptoms [13].
Similarly the relationship between exercise measure-
ments and QOL is inconsistent [13,14]. Dyspnea is
s reserved.

D.E. Wood / Thorac Surg Clin 14 (2004) 375–383376
important, but it is only a single symptom affecting
QOL, and no physiologic or functional variable can
summarize adequately the impact of emphysema on
symptoms and HRQOL. A measurement of HRQOL
provides the best estimate of treatment effect for
LVRS rather than any of the commonly measured
physiologic outcomes.
Quality-of-life instruments
A variety of disease-specific and general instru-
ments for measuring HRQOL have been used by
authors evaluating LVRS outcomes (Box 1). Disease-
specific instruments focus on specific symptoms
within the disease category, such as shortness of
Box 1. Instruments used to measurehealth-related quality of life in lung volumereduction surgery patients
Disease specific
St. George’s Respiratory Questionnaire(SGRQ)
Chronic Respiratory Questionnaire(CRQ)
Transitional Dyspnea Index (TDI)Modified Medical Research Council
Dyspnea Index (MRC)Borg ScaleUniversity of California San Diego
(UCSD) Shortness of BreathQuestionnaire
Mahler Baseline Dyspnea Index
General
Medical Outcomes Study Short-FormHealth Survey (SF-36)
Sickness Impact Profile (SIP)Nottingham Health Profile (NHP)
Preference based
Standard GambleTime Trade-offWillingness to PayQuality of Well-Being Questionnaire
(QWB)Health Utility IndexEuropean Quality of Life tools (EuroQol)
breath in a patient with emphysema. These disease-
specific measures are likely to be more sensitive
because their content is directly related to the disease
in question. Disease-specific measures are more likely
to be sensitive to small but clinically important
changes in health status compared with general in-
struments for measuring HRQOL. The commonly
used lung disease–specific measures include the
Transitional Dyspnea Index, modified Medical Re-
search Council dyspnea index (MRC dyspnea index),
St. George’s Respiratory Questionnaire (SGRQ),
Chronic Respiratory Questionnaire (CRQ), Borg
Scale, and University of California San Diego
(UCSD) Shortness of Breath Questionnaire.
General HRQOL instruments have the advantage
of a comprehensive evaluation, including the ability
to compare QOL across diseases. General HRQOL
instruments may be less sensitive in detecting subtle
differences of symptoms within the disease category
but may be more relevant to overall assessment of
HRQOL. These general instruments look at the to-
tal impact of disease on a patient’s QOL independent
from disease-specific symptoms. General HRQOL
instruments frequently used in evaluating LVRS out-
comes include the Medical Outcome Study Short-
Form Health Survey (SF-36), the Sickness Impact
Profile (SIP) and the Nottingham Health Profile.
An additional complexity in QOL studies is that
disease-specific or general instruments that assess
only functional status miss other important aspects
of HRQOL. Patients with a similar functional impair-
ment may experience a different impact on their
QOL. Decisions about an invasive procedure such
as LVRS depend not only on the expected improve-
ment in QOL, but also on the potential morbidity and
mortality of the procedure. Most HRQOL question-
naires do not account for this difference in perception
of functional status and the patient’s willingness to
accept risk. Preference-basedHRQOLmeasures evalu-
ate the degree of impairment, the impact of the
impairment on the patient, and the willingness of
the patient to undergo risk to improve QOL. These
preference-based HRQOL measures provide an im-
portant means for measuring the impact of an inter-
vention such as LVRS [15]. Instruments of preference
assessment include the Standard Gamble, Time Trade-
off, and Willingness to Pay and the standardized
instruments of the Quality of Well-Being Question-
naire (QWB), the Health Utility Index, and the
European Quality of Life tools [15].
Instruments for measuring HRQOL are well vali-
dated and reliable, although they are less familiar to
clinicians caring for emphysema patients than spiro-
metric and functional studies. Because of this lack of
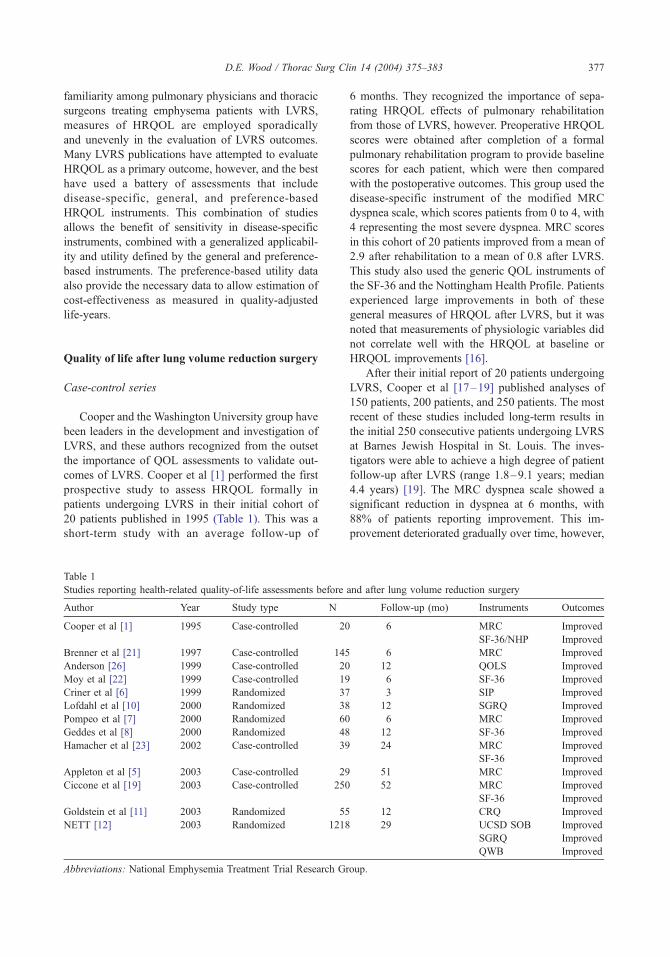
D.E. Wood / Thorac Surg Clin 14 (2004) 375–383 377
familiarity among pulmonary physicians and thoracic
surgeons treating emphysema patients with LVRS,
measures of HRQOL are employed sporadically
and unevenly in the evaluation of LVRS outcomes.
Many LVRS publications have attempted to evaluate
HRQOL as a primary outcome, however, and the best
have used a battery of assessments that include
disease-specific, general, and preference-based
HRQOL instruments. This combination of studies
allows the benefit of sensitivity in disease-specific
instruments, combined with a generalized applicabil-
ity and utility defined by the general and preference-
based instruments. The preference-based utility data
also provide the necessary data to allow estimation of
cost-effectiveness as measured in quality-adjusted
life-years.
Quality of life after lung volume reduction surgery
Case-control series
Cooper and the Washington University group have
been leaders in the development and investigation of
LVRS, and these authors recognized from the outset
the importance of QOL assessments to validate out-
comes of LVRS. Cooper et al [1] performed the first
prospective study to assess HRQOL formally in
patients undergoing LVRS in their initial cohort of
20 patients published in 1995 (Table 1). This was a
short-term study with an average follow-up of
Table 1
Studies reporting health-related quality-of-life assessments before
Author Year Study type N
Cooper et al [1] 1995 Case-controlled 20
Brenner et al [21] 1997 Case-controlled 145
Anderson [26] 1999 Case-controlled 20
Moy et al [22] 1999 Case-controlled 19
Criner et al [6] 1999 Randomized 37
Lofdahl et al [10] 2000 Randomized 38
Pompeo et al [7] 2000 Randomized 60
Geddes et al [8] 2000 Randomized 48
Hamacher et al [23] 2002 Case-controlled 39
Appleton et al [5] 2003 Case-controlled 29
Ciccone et al [19] 2003 Case-controlled 250
Goldstein et al [11] 2003 Randomized 55
NETT [12] 2003 Randomized 1218
Abbreviations: National Emphysemia Treatment Trial Research Gr
6 months. They recognized the importance of sepa-
rating HRQOL effects of pulmonary rehabilitation
from those of LVRS, however. Preoperative HRQOL
scores were obtained after completion of a formal
pulmonary rehabilitation program to provide baseline
scores for each patient, which were then compared
with the postoperative outcomes. This group used the
disease-specific instrument of the modified MRC
dyspnea scale, which scores patients from 0 to 4, with
4 representing the most severe dyspnea. MRC scores
in this cohort of 20 patients improved from a mean of
2.9 after rehabilitation to a mean of 0.8 after LVRS.
This study also used the generic QOL instruments of
the SF-36 and the Nottingham Health Profile. Patients
experienced large improvements in both of these
general measures of HRQOL after LVRS, but it was
noted that measurements of physiologic variables did
not correlate well with the HRQOL at baseline or
HRQOL improvements [16].
After their initial report of 20 patients undergoing
LVRS, Cooper et al [17–19] published analyses of
150 patients, 200 patients, and 250 patients. The most
recent of these studies included long-term results in
the initial 250 consecutive patients undergoing LVRS
at Barnes Jewish Hospital in St. Louis. The inves-
tigators were able to achieve a high degree of patient
follow-up after LVRS (range 1.8–9.1 years; median
4.4 years) [19]. The MRC dyspnea scale showed a
significant reduction in dyspnea at 6 months, with
88% of patients reporting improvement. This im-
provement deteriorated gradually over time, however,
and after lung volume reduction surgery
Follow-up (mo) Instruments Outcomes
6 MRC Improved
SF-36/NHP Improved
6 MRC Improved
12 QOLS Improved
6 SF-36 Improved
3 SIP Improved
12 SGRQ Improved
6 MRC Improved
12 SF-36 Improved
24 MRC Improved
SF-36 Improved
51 MRC Improved
52 MRC Improved
SF-36 Improved
12 CRQ Improved
29 UCSD SOB Improved
SGRQ Improved
QWB Improved
oup.

Fig. 1. Long-term improvements in modified Medical Research Council Dyspnea Scale after lung volume reduction surgery.
White represents improved, gray shows no change, and black indicates worse. (From Ciccone AM, Meyers BF, Guthrie TJ, et al.
Long-term outcome of bilateral lung volume reduction in 250 consecutive patients with emphysema. J Thorac Cardiovasc Surg
2003;125:513–25; with permission.)
D.E. Wood / Thorac Surg Clin 14 (2004) 375–383378
with a percentage of patients continuing to report an
improved dyspnea scale decreasing to 60% at 3 years
and 45% at 5 years (Fig. 1) [19]. The SF-36 also
showed marked improvement compared with base-
line after pulmonary rehabilitation. With follow-up
successful in greater than 90% of patients at 1, 3, and
5 years, 96% of patients reported a substantial im-
provement at 6 months postoperatively. Although this
improvement also slowly deteriorated over time, at
5 years after LVRS (n = 100), 79% of patients
remained improved in their general QOL score com-
pared with preoperatively (Fig. 2) [19].
These data from the Washington University group
sound compelling regarding the improvement in the
disease-specific and generic QOL in patients after
Fig. 2. SF-36 physical functioning scores from before lung volume
AM, Meyers BF, Guthrie TJ, et al. Long-term outcome of bilate
emphysema. J Thorac Cardiovasc Surg 2003;125:513–25; with pe
LVRS, even with long-term follow-up. These data
are strengthened by the prospective evaluation of pa-
tients and by a high rate of follow-up compliance.
These data also are limited, however, by the progres-
sive censoring of dying patients and patients under-
going lung transplantation, both expected to represent
poor performing patients or patients with worse out-
comes. Of the initial 250 patients, 96 (38%) had died
at the time of the report, and an additional 7% of
patients had undergone lung transplantation [19].
Combined, 45% of patients, representing the patients
with the worst outcomes, were excluded from follow-
up analysis. This survivorship bias could result in
an overly optimistic view of long-term outcomes
after LVRS. Other case-control series are often limited
reduction surgery (baseline) and after surgery. (From Ciccone
ral lung volume reduction in 250 consecutive patients with
rmission.)

D.E. Wood / Thorac Surg Clin 14 (2004) 375–383 379
by the similar effect of a follow-up bias, with poor-
performing patients failing to return for follow-up and
positively skewing postoperative analysis [20].
Brenner et al [21] used the MRC dyspnea scale to
compare dyspnea before and after LVRS in 145 pa-
tients. In this series, the MRC dyspnea scale improved
by at least 1 point in nearly 90% of patients with fol-
low-up greater than 6 months. Approximately 60% of
patients had 6-month improvement in the MRC scale
of 2 or greater. Neither baseline FEV1 nor change in
FEV1 correlated well with dyspnea, confirming the
importance of HRQOL outcomes over physiologic
outcomes for validating efficacy of LVRS.
Because LVRS has been combined most frequently
with an intensive pulmonary rehabilitation program,
each of these interventions may have a cumulative
effect on HRQOL. Some studies, such as those de-
scribed earlier from the Washington University group,
have tried to distinguish between improvements due
to rehabilitation versus improvements due to LVRS by
defining the postrehabilitation assessments as the
patient’s baseline. Other studies have not clearly
defined whether QOL assessments were performed
before or after pulmonary rehabilitation or whether a
routine pulmonary rehabilitation was used before
LVRS. Moy et al [22] specifically assessed HRQOL
by the generic instrument SF-36 before pulmonary
rehabilitation, after pulmonary rehabilitation, and
again 6 months after LVRS. Although this analysis
of 19 patients was small, it allowed the direct analysis
of the impact of pulmonary rehabilitation, the impact
of LVRS, and the cumulative impact of both inter-
ventions on HRQOL. These authors found no signifi-
cant change in any of the domains of the SF-36 after
pulmonary rehabilitation compared with baseline
measures [22]. Patients experienced significant im-
provement in only one domain, vitality, at 6 months
after LVRS compared with scores after pulmonary
rehabilitation. When comparing the combined effects
of pulmonary rehabilitation and LVRS, however,
patients experienced significant improvements from
baseline (prerehabilitation) in four of the eight do-
mains of the SF-36, including physical functioning,
role limitations due to physical problems, social func-
tioning, and vitality [22]. The combination of pulmo-
nary rehabilitation and LVRS resulted in significant
improvements in HRQOL, but each intervention con-
tributed in a distinct way. Pulmonary rehabilitation
accounted for more than 90% of the improvements
in role limitations due to physical problems, whereas
LVRS accounted for nearly all the improvements in
physical functioning and vitality [22].
Hamacher et al [23] from Zurich specifically
investigated disease-specific and general QOL out-
comes 2 years after LVRS in 39 patients prospec-
tively assessed before LVRS with the MRC dyspnea
scale and the SF-36. Marked improvements were
seen in the dyspnea scale with patients having a
mean preoperative score of 3.9 (maximum dyspnea
= 4), which decreased 3 months postoperatively to a
mean score of 1.5. This improvement was largely
sustained throughout the follow-up period, slightly
deteriorating 2 years after LVRS to a mean score of 2
[23]. In the general measure of HRQOL, the SF-36
showed significant improvement in six of eight
domains at 3, 6, 12, and 18 months after LVRS.
Improvements occurred in the domains of physical
functioning, role physical, general health, vitality,
social functioning, and mental health, with no signifi-
cant improvements in the domains of bodily pain and
role emotional. Although there was some deteriora-
tion at 24 months, improvements continued to be
statistically significant in five of the six improved
domains, only returning to baseline in the domain of
general health [23]. The strength of this European
study lies in its prospective analysis and the exami-
nation of longer term outcomes measured at 2 years
after LVRS. Because patients did not routinely un-
dergo pulmonary rehabilitation, it would seem that
the study would be less confounded by the additional
impact of pulmonary rehabilitation on LVRS and that
the benefits would be related purely to the surgical
intervention. The additional medical attention paid to
the preoperative and postoperative LVRS patient is
likely to contribute additional health benefits func-
tionally beyond that conferred by the surgery alone,
however, and paradoxically may make it harder to
separate LVRS outcomes from preoperative medical
management. A series that specifically conducts pul-
monary rehabilitation and measures HRQOL after a
course of pulmonary rehabilitation partially controls
for the increased medical attention provided to the
LVRS patient and the benefit, independent from
surgery, that may result. The Hamacher study is
limited further by the fact that more than half of the
patients undergoing LVRS surgery in this center were
censored as a result of patient mortality, loss of
follow-up, intervening lung transplantation, poor
comprehension of the German language, or short
follow-up. These patients lost for evaluation had the
potential to confound the results, most likely skewing
the reported results in a favorable direction for the
reasons of follow-up and survivorship bias as de-
scribed earlier.
A series from Australia published by Appleton
et al [5] further examined long-term outcomes in
HRQOL after LVRS. This retrospective analysis of
29 survivors of 54 patients undergoing LVRS exam-

D.E. Wood / Thorac Surg Clin 14 (2004) 375–383380
ined patients from 3 to 5.5 years after surgery (mean
51 months) and found a significant and sustained
improvement in the modified MRC dyspnea scores.
Although the Dartmouth Primary Care Cooperative
Quality of Life Questionnaire was used to assess
general HRQOL, this was assessed only postopera-
tively and so was not able to be assessed prospec-
tively related to patient function before LVRS. These
outcomes, including examination of the Care Giver
Burden Scale, simply revealed that recipients of
LVRS have similar QOL and burden to caregivers
as other individuals with chronic illnesses [5]. The
major limitation of this study is that it was conducted
retrospectively. The lack of prospective assessments
substantially limits the credibility and reliability of
the findings because they rely on patient recollection
several years after surgery.
Many additional case-control series of LVRS
have used some element of QOL assessment and have
been summarized in two reviews of LVRS [2,15].
Cordova et al [24] used the SIP before and after
LVRS and showed significant improvements in phys-
ical and psychosocial scores and overall scores 3 to
12 months after LVRS. This study confirmed the
cumulative benefits of pulmonary rehabilitation and
LVRS, showing a sustainable improvement after
8 weeks of pulmonary rehabilitation with additional
improvement occurring after LVRS. Few centers have
reported HRQOL using respiratory disease–specific
instruments. Bagley et al [25] used the Chronic Res-
piratory Questionnaire (CRQ), a disease-specific ques-
tionnaire developed for use in patients with COPD.
Short-term follow-up in this study noted improve-
ments in dyspnea, fatigue, emotional function, and
mastery. The SGRQ also has been used in LVRS
studies as a disease-specific HRQOL instrument;
this instrument is discussed later in a review of
the NETT.
Overall QOL was prospectively assessed in 20 pa-
tients before and after LVRS by the researchers at
the University of Washington. This study used the
Quality of Life Scale and showed significant improve-
ment in Quality of Life Scale at 3, 6, and 12 months
after surgery correlating with similar improvements
in FEV1 and exercise capacity [26].
Although many studies failed to identify a direct
or linear relationship between physiologic or func-
tional outcomes with the outcomes of HRQOL,
researchers at Temple University specifically exam-
ined these correlations [27]. QOL was assessed by the
SIP and correlated to changes in FEV1 and exercise
capacity before and after LVRS. Although there was
no significant correlation between changes in SIP
scores and routine measures of lung function, exer-
cise capacity, or gas exchange, changes in SIP did
correlate to the change in oxygen cost of breathing
(volume of oxygen use-to-respiratory minute volume
ratio), reduction in residual volume-to-total lung ca-
pacity ratio, and the subjective assessment of post-
operative steroid and oxygen requirements [27].
Randomized studies
Seven randomized trials of LVRS have been
published, and six of these provide an assessment
of HRQOL [6–8,10–12]. The first was performed
by Criner et al [6] at Temple University and random-
ized 37 patients to undergo pulmonary rehabilitation
versus pulmonary rehabilitation followed by LVRS.
The SIP was significantly improved after 8 weeks
of rehabilitation, and this was maintained during
3 months of additional rehabilitation. Further im-
provement in the SIP was noted 3 months after
LVRS, however, compared with the initial improve-
ment gained after rehabilitation.
Lofdahl et al [10] from Sweden randomized
38 patients to rehabilitation versus rehabilitation fol-
lowed by LVRS and followed these patients using
preoperative and postoperative QOL as measured by
the SGRQ. Although published only in abstract form,
this study showed impressive improvement in the
total SGRQ and the domains of symptoms, activity,
and impact.
Pompeo et al [7] published the largest single-
institution randomized series, evaluating 60 patients
who were randomized to pulmonary rehabilitation ver-
sus LVRS. The surgical patients in this series did not
undergo preoperative or postoperative pulmonary
rehabilitation, so these patients did not benefit from
the cumulative impact of rehabilitation plus LVRS.
This group evaluated only the MRC dyspnea index
as a disease-specific measure of HRQOL along with
several other physiologic and functional outcomes.
This group identified significant improvement in the
dyspnea index, in the medically randomized arm
6 months after pulmonary rehabilitation. There was
a further significant improvement of the dyspnea
index, however, in the surgically randomized patients
compared with medical patients [7].
Until the publication of the NETT, the British trial
published by Geddes et al [8] received the most
attention. This trial randomized 48 patients to a
6-week program of outpatient rehabilitation followed
by randomization to either continued rehabilitation or
LVRS. The QOL was assessed with SF-36 before ran-
domization and at follow-up 3, 6, 12, and 24 months
after randomization. Although scores in the SF-36
tended to decline over time in the medically random-
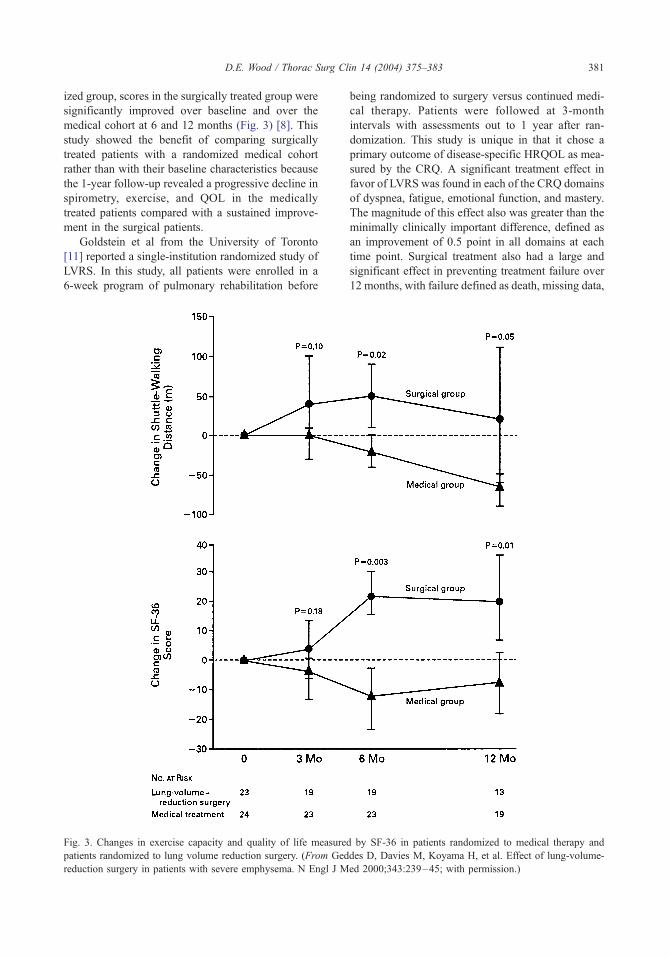
D.E. Wood / Thorac Surg Clin 14 (2004) 375–383 381
ized group, scores in the surgically treated group were
significantly improved over baseline and over the
medical cohort at 6 and 12 months (Fig. 3) [8]. This
study showed the benefit of comparing surgically
treated patients with a randomized medical cohort
rather than with their baseline characteristics because
the 1-year follow-up revealed a progressive decline in
spirometry, exercise, and QOL in the medically
treated patients compared with a sustained improve-
ment in the surgical patients.
Goldstein et al from the University of Toronto
[11] reported a single-institution randomized study of
LVRS. In this study, all patients were enrolled in a
6-week program of pulmonary rehabilitation before
Fig. 3. Changes in exercise capacity and quality of life measure
patients randomized to lung volume reduction surgery. (From Ged
reduction surgery in patients with severe emphysema. N Engl J M
being randomized to surgery versus continued medi-
cal therapy. Patients were followed at 3-month
intervals with assessments out to 1 year after ran-
domization. This study is unique in that it chose a
primary outcome of disease-specific HRQOL as mea-
sured by the CRQ. A significant treatment effect in
favor of LVRS was found in each of the CRQ domains
of dyspnea, fatigue, emotional function, and mastery.
The magnitude of this effect also was greater than the
minimally clinically important difference, defined as
an improvement of 0.5 point in all domains at each
time point. Surgical treatment also had a large and
significant effect in preventing treatment failure over
12 months, with failure defined as death, missing data,
d by SF-36 in patients randomized to medical therapy and
des D, Davies M, Koyama H, et al. Effect of lung-volume-
ed 2000;343:239–45; with permission.)

D.E. Wood / Thorac Surg Clin 14 (2004) 375–383382
treatment complications, or consistent decrease in at
least two domains of the CRQ. Although limited by a
small sample size (n = 55) and only 1-year follow-up,
this study did take into account dead and missing
patients, which are censored from data analysis in
most other studies [11].
National Emphysema Treatment Trial
The NETT is the first published multi-institutional
randomized trial on LVRS [12]. This trial has several
strengths over previously reported trials. The first is
the aspect of randomization after a period of formally
prescribed pulmonary rehabilitation, which provides
a common baseline formedically and surgically treated
patients and eliminates rehabilitation as a confound-
ing outcome variable. The second is its conduct as a
multi-institutional trial to minimize the outcomes that
may be specific or unique to a single center and less
applicable to practice across a broad spectrum of
academic or community centers. The third advantage
of the NETT was its size, with 1218 patients random-
ized, over an order of magnitude larger than any of
the other randomized studies of LVRS. Fourth, the
NETT used disease-specific and preference-based
instruments for measurement of HRQOL for a thor-
ough examination of the impact of LVRS in symp-
toms and overall QOL. Fifth, the NETT chose
outcomes at 2 years to examine durability of benefits
achieved by LVRS and did not allow crossover in the
study. Finally, similar to the Toronto study by Gold-
stein et al [11], the NETT included all patients in its
analysis, including patients who had died or were
missing data points, to avoid any skewing of out-
comes by follow-up or survivorship bias.
The NETT evaluated the symptom of dyspnea via
the UCSD Shortness of Breath Questionnaire, exam-
ined disease-specific HRQOL via the SGRQ, and
evaluated general QOL via the preference-based
QWB. Dyspnea was significantly improved in surgi-
cally randomized patients at 6, 12, and 24 months
compared with baseline and compared with progres-
sive worsening of symptoms in the medically ran-
domized patients [12]. With a threshold of 8 units of
improvement in SGRQ defined as significant, the
overall surgical cohort was much more likely to see
a significant improvement in SGRQ than medically
randomized patients (33% versus 9%). Upper lobe
emphysema versus non–upper lobe emphysema and
high exercise capacity versus low exercise capacity
were found to be important preoperative variables
predicting differential outcomes between medically
treated patients and patients undergoing LVRS. Of
the four subgroups identified in the NETT, three had
an improved opportunity for substantial benefit in the
SGRQ. These included all upper lobe–predominant
emphysema patients and patients with non–upper
lobe emphysema but low baseline exercise capacity
after a course of pulmonary rehabilitation. When
high-risk patients were excluded from the analysis
[28], the QWB was statistically improved in surgi-
cally treated patients compared with medical patients
at 6, 12, and 24 months [12].
The results from the NETT have provided rein-
forcement and validation of the data provided in
previous case-control or small randomized series
despite a conservative statistical analysis. Although
a randomized study, the NETT analysis compared
patients with their baseline, similar to the case control
series, to provide data regarding the changes to be
anticipated after LVRS. When surgically treated
patients were compared with the progressive decline
in function of medically treated patients, however,
these differences between groups seem even more
profound. A companion study about the cost-effec-
tiveness of LVRS also was performed alongside the
clinical NETT trial [29]. This study was able to take
advantage of the preference-based utility score,
QWB, to assess the cost-effectiveness ratio for LVRS
compared with medical therapy. These data are pro-
vided in another article in this issue.
Summary
The common physiologic and functional variables
that quantify limitation in emphysema patients have
been the most common outcomes measured after
LVRS. Spirometric values and exercise capacity are
merely surrogates, however, for their impact on
symptoms and QOL in patients with severe emphy-
sema. Because LVRS has been developed as a surgery
to palliate disabling symptoms of emphysema, many
studies now have included HRQOL outcomes along
with the commonly measured physiologic and func-
tional outcomes. Some studies have centered on the
QOL as the primary outcome instead of physiologic
variables. Many symptom scales and disease-specific
and general instruments of HRQOL have been used
for evaluating emphysema patients before and after
LVRS. Case-control studies and randomized studies
have shown a consistent improvement in symptoms
related to emphysema and general QOL. These studies
validate the use of LVRS as a palliative therapy for se-
lected patients with emphysema. The NETT suggests
that this benefit is applicable primarily to patients
with an upper lobe–predominant pattern of emphy-
sema or patients with low exercise capacity. Valida-
D.E. Wood / Thorac Surg Clin 14 (2004) 375–383 383
tion or refinement of these criteria depends on the
continued contributions of the many investigators
performing LVRS.
References
[1] Cooper JD, Trulock EP, Triantafillou AN, et al. Bilat-
eral pneumectomy (volume reduction) for chronic ob-
structive pulmonary disease. J Thorac Cardiovasc
Surg 1995;109:106–16.
[2] Flaherty KR, Martinez FJ. Lung volume reduction
surgery for emphysema. Clin Chest Med 2000;21:
819–48.
[3] Cooper JD, Patterson GA, Sundaresan RS, et al.
Results of 150 consecutive bilateral lung volume re-
duction procedures in patients with severe emphy-
sema. J Thorac Cardiovasc Surg 1996;112:1319–30.
[4] Gelb AF, McKenna Jr RJ, Brenner M, Epstein JD,
Zamel N. Lung function 5 yr after lung volume reduc-
tion surgery for emphysema. Am J Respir Crit Care
Med 2001;163:1562–6.
[5] Appleton S, Adams R, Porter S, Peacock M, Ruffin R.
Sustained improvements in dyspnea and pulmonary
function 3 to 5 years after lung volume reduction sur-
gery. Chest 2003;123:1838–46.
[6] Criner GJ, Cordova GC, Furukawa S, et al. Prospective
randomized trial comparing bilateral lung volume
reduction surgery to pulmonary rehabilitation in severe
chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 1999;160:2018–27.
[7] Pompeo E, Marino M, Notroni I, Matteucci G, Mineo
TC. Reduction pneumoplasty versus respiratory reha-
bilitation in severe emphysema: a randomized study.
Ann Thorac Surg 2003;70:948–54.
[8] Geddes D, Davies M, Koyama H, et al. Effect of lung-
volume reduction surgery in patients with severe
emphysema. N Engl J Med 2000;343:239–45.
[9] Goodknight-White S, Jones WJ, Baaklini J, et al. Pro-
spective randomized controlled trial comparing bilater-
al lung volume reduction surgery (LVRS) to medical
therapy alone in patients with severe emphysema.
Chest 2000;118(Suppl 4):102S.
[10] Lofdahl CG, Hillerdal G, Strom K. Randomized con-
trolled trial of volume reduction surgery—preliminary
results up to 12 months. Am J Respir Crit Care Med
2000;161:A585.
[11] Goldstein RS, Todd TRJ, Guyett G, et al. Influence
of lung volume reduction surgery (LVRS) on health
related quality of life in patients with chronic obstruc-
tive pulmonary disease. Thorax 2003;58:405–10.
[12] National Emphysema Treatment Trial Research Group.
A randomized trial comparing lung volume reduction
surgery with medical therapy for severe emphysema.
N Engl J Med 2003;348:2059–73.
[13] Redelmeier D, Goldstein R, Min S, et al. Spirometry
and dyspnea in patients with COPD: when small differ-
ences mean little. Chest 1996;109:1163–8.
[14] Ries A, Kaplan R, Limberg T, et al. Effects of pulmo-
nary rehabilitation on physiologic and psychosocial
outcomes in patients with chronic obstructive pulmo-
nary disease. Ann Intern Med 1995;122:823–32.
[15] Yusen RD, Morrow LE, Brown KL. Health-related
quality of life after lung volume reduction surgery.
Semin Thorac Cardiovasc Surg 2002;14:403–12.
[16] Yusen R. What outcomes should be measured in
patients with COPD? Chest 2001;119:327–8.
[17] Cooper JD, Patterson GA, Sundaresan RS, et al.
Results of 150 consecutive bilateral lung volume re-
duction procedures in patients with severe emphy-
sema. J Thorac Cardiovasc Surg 1996;112:1319–29.
[18] Yusen RD, Morrow LE, Brown KL. Health-related
quality of life after lung volume reduction surgery.
Semin Thorac Cardiovasc Surg 2002;14:403–12.
[19] Ciccone AM, Meyers BF, Guthrie TJ, et al. Long-term
outcome of bilateral lung volume reduction in 250
consecutive patients with emphysema. J Thorac Cardio-
vasc Surg 2003;125:513–25.
[20] Butler CW, Snyder M, Wood DE, Curtis JR, Albert
RK, Benditt JO. Underestimation of mortality follow-
ing lung volume reduction surgery resulting from in-
complete followup. Chest 2001;119:1056–60.
[21] Brenner M, McKenna RJ, Gelb AF, et al. Dyspnea
response following bilateral thoracoscopic staple lung
volume reduction surgery. Chest 1997;112:916–23.
[22] Moy ML, Ingenito EP, Mentzer SJ, Evans RB, Reilly
Jr JJ. Health-related quality of life improves following
pulmonary rehabilitation and lung volume reduction
surgery. Chest 1999;115:383–9.
[23] Hamacher J, Buchi S, Georgescu CL, et al. Improved
quality of life after lung volume reduction surgery. Eur
Respir J 2002;19:54–60.
[24] Cordova F, O’Brien G, Furukawa S, et al. Stability of
improvement in exercise performance and quality of
life following bilateral lung volume reduction surgery
in severe COPD. Chest 1997;112:907–15.
[25] Bagley PH, Davis SM, O’Shea M, et al. Lung volume
reduction surgery at a community hospital: program
development and outcomes. Chest 1997;111:1552–9.
[26] Anderson KL. Change in quality of life after lung vol-
ume reduction surgery. Am J Crit Care 1999;8:389–96.
[27] Leyenson V, Furukawa S, Kuzma AM, et al. Correla-
tion of changes in quality of life after lung volume
reduction surgery with changes in lung function, exer-
cise, and gas exchange. Chest 2000;118:728–35.
[28] National Emphysema Treatment Trial Research Group.
Patients at high risk of death after lung-volume-reduc-
tion surgery. N Engl J Med 2001;345:1075–83.
[29] National Emphysema Treatment Trial Research Group.
Cost effectiveness of lung volume-reduction surgery
for patients with severe emphysema. N Engl J Med
2003;348:2092–102.

Thorac Surg Clin 14 (2004) 385–407
Quality of life after lung transplantation
Cliff K. Choong, MBBS, FRACS, Bryan F. Meyers, MD*
Division of Cardiothoracic Surgery, Department of Surgery, Washington University School of Medicine, Suite 3108,
Queeny Tower, One Barnes–Jewish Hospital Plaza, St. Louis, MO 63110, USA
Lung transplantation is now an accepted form of lung transplantation. Survival alone is not a compre-
treatment for many end-stage lung diseases. After the
report of the first clinically successful lung transplan-
tation in 1983, the number of lung transplantations
and lung transplant centers increased substantially.
Between 1985 and 2001, 14,586 lung transplanta-
tions had been performed and registered with the
International Society of Heart and Lung Trans-
plantation. Numerous studies have reported the im-
provements in pulmonary function and exercise
performance after lung transplantation. The survival
of lung transplant recipients also has improved as a
result of improved patient selection, perioperative
care, surgical techniques, and immunosuppression
regimens. Although some studies also have shown a
survival benefit after lung transplantation for patients
with specific diagnoses, the survival benefit of trans-
plant in many diseases remains debatable [1].
Importance of quality-of-life measurements in
lung transplantation
Traditionally the outcome of lung transplantation
has been measured by graft function and patient
survival. When lung transplantation first became
feasible, the criteria for listing a patient for transplant
included the stipulation that life expectancy be less
than 1 year in the absence of the transplant. As
survival expectations and organ waiting times have
increased, so too have the life expectancies of pa-
tients referred for transplant. Quality-of-life (QOL)
measurement now is increasingly recognized as an
important tool of health care assessment and is
especially appropriate for evaluating the effects of
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00025-8
* Corresponding author.
E-mail address: [email protected] (B.F. Meyers).
hensive way to summarize the existence of survivors
of lung transplantation or that of patients with chronic
lung disease managed without transplantation. Some
transplant recipients experience dramatic relief of
symptoms and a clear prolongation of life, whereas
other recipients may experience posttransplant com-
plications, such as bronchiolitis obliterans syndrome
(BOS), and remain in a disabling state of disease. The
pretransplant existence may be of such poor quality
that many potential recipients would accept any risks
for an opportunity at improved health and function,
even if it meant shortening their life to do so. A
careful evaluation in the improvement in QOL before
and after lung transplantation is important and forms
a necessary outcome measure to be viewed alongside
statistics for overall survival and graft function.
QOL studies also allow the direct comparison of
lung transplantation with other specific treatments for
end-stage lung diseases. These therapies include
prostaglandin infusion pumps for primary pulmonary
hypertension or lung volume reduction surgery for
severe emphysema. It is difficult to compare distinctly
different therapies based on duration of survival alone
when one therapy carries a higher early mortality risk
in exchange for a chance at greatly improved func-
tional status and improved longevity among the
survivors. This information is important and useful
as a resource for potential recipients considering lung
transplantation and for physicians considering referral
of their patients for lung transplantation.
Finally, QOL assessment facilitates the measure-
ment of efficiency of medical and surgical therapies.
The surgical treatment of end-stage lung disease with
lung transplantation and subsequent postoperative
management are expensive. QOL measurement
allows for the estimation of utility and allows valua-
tion and comparison of competing therapeutic options
s reserved.

Box 2. Quality-adjusted life-years
Quality-adjusted life-years (QALY) =health utility score � survival or lifeexpectancy in years.
Examples
Medical group before transplantation
Health utility score: 0.31Life expectancy: 2.7 years
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407386
in cost-utility analyses. The combination of duration
of life and QOL after lung transplantation must be
quantified to justify the high costs of transplantation
in the current era of cost containment in medical
expenditures. Quantifying QOL after lung transplan-
tation and comparing it with the QOL after other
medical therapies allows calculation and comparison
of quality-adjusted life expectancy and makes possi-
ble the economic evaluation of these disparate treat-
ments. Sensitivity analyses of the resulting cost-utility
estimates would point practitioners to the problem
areas that act as barriers to improved efficiency.
QALY = 0.31 � 2.7 = 0.84Bilateral lung transplant recipient group
Health utility score: 0.82Life expectancy: 5 years
General strategies in assessing quality of life for
lung transplant candidates and recipients
A wide variety of instruments and indices have
been used in QOL studies performed in lung trans-
Box 1. Classification of quality-of-lifeinstruments
Global
Look at overall life satisfaction
Generic
Allow assessment of basic valuesthat are relevant for everyone’shealth status
Allow assessment to be performedacross all types of patientpopulations regardless of underlyingdiagnosis or treatment regimen
Allow for comparisons between oramong disparate diseases
Lack focus on disease-specific issues,such as a dyspnea index
Limited sensitivity to changes indisease condition
Disease specific
Limited to a specific patientpopulation with that particulardisease condition
Provide better sensitivity to diseasechanges
QALY = 0.82 � 5 = 4.1
QALY gained of bilateral lung recipientgroup over medical group= 4.1� 0.84=3.3 life-years gained.
plantation [2–33]. In general, they can be classified
as global, generic, or disease specific (Box 1). Global
instruments assess the overall well-being of the
patient, whereas generic instruments evaluate one
or more areas of QOL in such a way that is applica-
ble across a wide variety of disease diagnoses and
population groups. Unidimensional generic question-
naires focus on a single area or domain, such as
physical functioning, whereas multidimensional ques-
tionnaires evaluate several domains, such as psycho-
logical, social, and physical areas. Disease-specific
questionnaires are used for particular conditions, such
as the dyspnea index for patients with lung diseases,
to provide better sensitivity to changes caused by
therapy or passage of time. In addition to the generic
instruments, some studies have applied a utility
estimation generic tool, such as the European Quality
of Life tools (EuroQol) EQ5D, Quality of Well-Being
(QWB) scale, Standard Gamble, and Time Trade Off
to assess QOL [4,9,12,33]. These instruments allow a
utility value, usually a value in the range of 0 (worst
health) to 1 (best health), to be attached to the health-
related QOL evaluation. The utility value allows
direct measurement of QOL as an outcome and
enables adjustment of survival times to produce
quality-adjusted survival (Box 2).

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 387
Quality-of-life instruments used in lung
transplantation studies
Table 1 provides a brief description of the various
QOL instruments. Most studies have used a multi-
dimensional generic instrument, such as the Notting-
ham Health Profile (NHP), the EuroQol, the Medical
Outcome Study 36-Item Short Form (MOS-SF36),
the QWB, and the Quality of Life Index (QLI)
to evaluate the QOL in candidates and recipients
(Table 2) [2–4,6,9,10]. Most of these instruments
consist of simple, self-administered questionnaires
and are chosen for simplicity, the ease in application
and analyses, and the cost savings that result from
self-administered questionnaires. These instruments
have the advantage of being validated across a wide
variety of diseases and patient populations. Most
of the published studies in the lung transplant litera-
ture have combined a multidimensional generic in-
strument with a single-dimension instrument such,
as the State-Trait Anxiety Inventory (STAI) or the
Zung Self-Rating Depression Scale (Z-SDS) [15,17].
Studies from the United Kingdom and the Netherlands
frequently have used either the Nottingham Health
Profile or the EuroQoL (see Table 2) [34–40]. Studies
from Canada and United States typically have used
instruments that originated from North America, such
as the MOS-SF36 [5,21,24,31,41,42].
The EuroQol, Standard Gamble, and Time Trade
Off are generic instruments or techniques that provide
a utility estimation tool [4,12,33]. The EuroQol
EQ5D is a simple generic instrument that evaluates
five dimensions of QOL (see Table 1). In each
dimension, a respondent can indicate one of three
categories: no problem, moderate problem, or severe
problems. Combinations of these categories result in
243 permutations of health states. A regression equa-
tion defines a utility value for these health states. The
possible health utility value ranges from �0.59 (se-
vere problems in all five dimensions) to 1 (no
problem in all dimensions) and is translated onto a
scale of 0 representing death to 1 representing best
possible health state. An individual’s EQ5D utility
value is based on the absence or presence of moderate
or severe problems in the five dimensions. The
EuroQol has the advantage of being a simple self-
administered questionnaire requiring about 1 minute
for completion with a track record of reliable use in
many studies. The Time Trade Off and Standard
Gamble techniques allow participants to evaluate
the impact of the disease or intervention on their
QOL. The values indicated by the study subjects
provide preference-weighted measures of utility esti-
mation. A scenario reflecting the health state of
interest is developed, then utility weights are derived
from the individual subject’s evaluation responses.
Such utility estimation tools were used in several of
the reviewed studies [36,43,44].
The strategy of any study is based on the goal of
the study and the availability of patients for study.
Some authors have employed cross-sectional studies
to evaluate QOL before and after transplantation.
These studies are easier to perform compared with
longitudinal evaluation. The advantages are that the
study can be performed relatively faster and cheaper
in that they can be applied to all patients awaiting
transplant or in the posttransplant period. Cross-
sectional studies are less valuable in drawing com-
parisons across time because the variability among
subjects is inherently greater than variability over
time in a given subject. The cross-sectional studies
tend to be observational and descriptive without any
specific hypothesis testing involved. Longitudinal
studies are more useful because they account for
intersubject variability with repeated measures of
the same subjects. These studies take longer to
complete, require a larger population of patients,
and are generally more expensive to execute.
Descriptive studies
Cross-sectional studies
Busschbach et al [36] evaluated the feasibility of
applying QOL instruments on lung transplant patients
before and after transplantation. Three patients each
were studied before and after bilateral lung transplan-
tation, all of whom had cystic fibrosis. The authors
reported that the methodology was feasible, and the
preliminary results suggested that the improvement
in QOL after bilateral lung transplantation was com-
parable to that seen after heart transplantation. Cohen
et al [45] assessed the degree to which pretransplant
psychological measures were associated with physi-
cal health, QOL, and overall adjustment after trans-
plantation. The study compared 17 pretransplant
candidates with 60 recipients and found associations
between QOL and adjustment in recipients. Lanuza
et al [46] reported on the QOL, symptom experiences,
and work status of single-lung and bilateral lung
transplant recipients. There was no pretransplant
comparative group in this observational descriptive
study. The 48 respondents represented a response
rate of 87% and were 1.5 F 0.7 years posttransplant.
Approximately 90% of the respondents were very
satisfied with their QOL. No associations were found

Table 1
Quality-of-life instruments used in lung transplantation studies
Name of instrument Type No. questions Domains assessed
Nottingham Health
Profile (NHP) [2]
Generic Part I
38 yes/no items
Part II
7 yes/no items
Part I and II take only several
minutes to complete
Part I evaluates 6 specific domains:
1. Physical mobility (8 items)
2. Pain (8 items)
3. Energy (3 items)
4. Sleep (5 items)
5. Social isolation (5 items)
6. Emotional reaction (9 items)
Part II evaluates 7 areas of task performance
most affected by health
1. Occupation
2. Ability to perform jobs around the home
3. Social life
4. Sexual life
5. Home life
6. Hobbies
7. Holidays
EuroQol – EQ5D [3,4] Generic Respondent indicates 1 of
3 categories for each domain:
No problem
Moderate problem
Severe problem
5 specific domains:
1. Mobility
2. Self-care
3. Usual activities
4. Pain and discomfort
5. Anxiety or depression
EuroQol – Visual
Analogue Scale [3,4]
Global Single question: scale of 0
(worst) to 100 (best possible
health)
Subjective overall assessment of health
by respondent
Overall QOL visual
analog scale
(OQOLVAS) [5]
Global Visual analogue scale of 0
(worst possible QOL) to 100
(best possible QOL)
Subjective global assessment of QOL
Medical Outcomes Study
Short Form–20
(MOS SF-20) [6,62]
Generic 20-item questionnaire assessing
6 dimensions. Each dimension
is scored as a summated rating
scale and adjusted so that
scores range from 0 (worst) to
100 (best)
Evaluates 6 dimensions of ‘‘core health
concepts’’
1. Limitations in physical activities because of
health problems
2. Limitations in social activities because of
physical or emotional problems
3. Limitations in usual role activities because
of physical health problems
4. Bodily pain
5. General mental health
6. General health perceptions
Medical Outcome Study
Short Form–36
(MOS SF-36) [6,62]
Generic 36-item questionnaire Assesses 8 health concepts
1. Limitations in physical activities
because of health problems
2. Limitations in social activities because of
physical or emotional problems
3. Limitations in usual role activities because
of physical health problems
4. Bodily pain
5. General mental health
6. Limitations in usual role activities because
of emotional problems
7. Energy and fatigue (vitality)
8. General health perceptions
(continued on next page)
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407388

Table 1 (continued)
Name of instrument Type No. questions Domains assessed
General Health/QOL
Rating Scale
(GHQOLRS) [7]
Generic 5-item questionnaire using
6-point scale
Assesses subject’s overall satisfaction in the
following areas
1. QOL
2. Current health
3. Psychological/emotional strength
4. Physical strength
5. Satisfaction with the outcome of treatment
General health
questionnaire
(GHQ) [8]
Generic 60-item questionnaire Was developed to help primary care physicians
screen for nonpsychotic psychiatric disorders
and consists of 4 subscales
1. Somatic symptom
2. Anxiety and insomnia
3. Social dysfuction
4. Depression
Quality of Well-Being
scale (QWB) [9]
Generic
preference
weighted
Has 3 scales of function;
each step on these
scale has its own associated
preference weight
Also has 23 symptom/problem
complexes for the subject to
indicate the presence or
absence of each complex
on a given day
Measures 3 aspects of function
1. Mobility
2. Physical activity
3. Social activity
In addition, each patient is classified according
to the symptom or problems that bothered him
or her most. Observed function and symptomatic
complaints are then weighted by preference and
integrated in a manner that places the individual
on a continuum between death (0) and optimal
function (1) for any point in time. Provides
a utility-based outcome measure with a score
on a continuum ranging from 0 (dead) to 1
(optimal function)
Quality of Life
Index (QLI) [10]
Generic 32-item questionnaire and
subject respond to each item
on a 6-point Likert-type scale
ranging from ‘‘very satisfied’’
to ‘‘very dissatisfied’’
The instruments consists of 2 sections: one
measures satisfaction with various domains of
life, and the other measures the importance of
the domain to the subject. The satisfaction and
importance sections have 32 items that assess
the following areas: health care, physical
health and functioning, marriage, family,
friends, stress, standard of living, occupation,
education, leisure, future retirement, peace of
mind, personal faith, life goals, personal
appearance, self-acceptance, general
happiness, and general satisfaction
Index of Well
Being (IWB) [11]
Standard Gamble
(SG) [33]
Generic
Generic
preference
weighted
Requires an interview that
follows a structured
questionnaire. Interview
averages about 75 min
Interview is conducted and
requires 15 – 30 min.
Subject is offered 2 alternatives.
Alternative 1 is a treatment
with 2 possible outcomes:
either the patient returns to
normal health and lives for
an additional t years
(probability P), or the
patient dies immediately
Respondents are asked to describe and assess
their experience in 15 separate domains of life
and to respond to more general measures
regarding their lives as a whole
The interview is to assist patient in assigning
a utility score in the range of 0 (death) to 1
(perfect health). Patients are asked to choose
between living with the disease or having a
risky operation that could result in either
complete cure or immediate death. The main
principle is that patients are willing to accept
a higher risk of death if their health state is
worse than if their health is relatively good.
The amount of risk the patient is willing
(continued on next page)
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 389

Table 1 (continued)
Name of instrument Type No. questions Domains assessed
(probability 1-P). Alternative 2
has the certain outcome of
chronic state i for t years.
Probability P is varied
until the respondent is
indifferent between 2
alternatives, at which point
the required preference
value for state i is P
to take reveals information about the QOL of
the health states
Time Trade-Off
(TTO) [12]
Generic
preference
weighted
2 alternatives are offered.
Alternative 1 is state i for time
t followed by death; alternative
2 is full (or normal) health for
time x. Time is varied until the
respondent is indifferent
between 2 alternatives, at
which point the required
preference value for state
i is given by hi = x/t.
The technique was derived from Standard
Gamble that avoids the difficult risk factor.
Patients are asked to indicate the maximal
number of years they are willing to give up to
avoid a poor state of health: ‘‘. . ..if there was
a medicine that could change your present
health state, but it would decrease your life by
10 years, would you take that medicine. . ..?’’
Patients in extremely poor health state tend
to accept a substantial decrease in their life span.
The number of years of life that patients are
willing to give up gives an indication of the
quality of life in that particular health state
Sickness Impact
Profile (SIP) [13]
Generic 136-item questionnaire;
it can be administered by
an interviewer in
20–30 min or can be
self-administered
SIP scores are reported for the total tool, for
physical and psychological dimensions, and
for 12 functional categories
1. Sleep and rest
2. Emotion
3. Body care
4. Home management
5. Mobility
6. Social interaction
7. Ambulation
8. Alertness
9. Communication
10. Recreation
11. Eating
12. Work
Hospital Anxiety and
Depression Scale
(HADS) [14]
Generic 14-item questionnaire Assessment of depression and anxiety in
physically ill patients
State-Trait Anxiety
Inventory (STAI) [15]
Domain
specific
20-item questionnaire Anxiety
Beck Depression
Inventory (BDI) [16]
Domain
specific
21-item self-report depression
inventory
Measurement of patient depressive symptoms
Zung Self-rating
Depression Scale
(Z-SDS) [17]
Symptom Checklist-90
(SCL-90) [18]
Domain
specific
Generic
20-item questionnaire
Items are rated on a 5-point
scale
Assesses depressive symptoms
Assesses various types of symptoms including
anxiety, depression and anger-hostility
Brief Symptom
Inventory (BSI) [19]
Generic 53-item multidimensional,
psychological symptom
inventory. Each item has a
5-point scale ranging from
0 to 4
Includes 3 global indexes
1. Global Severity Index
2. Positive Symptom Total
3. Positive Symptom Distress Index
(continued on next page)
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407390

Table 1 (continued)
Name of instrument Type No. questions Domains assessed
and 9 primary symptom dimensions
1. Somatization
2. Obsessive-compulsive
3. Interpersonal sensitivity
4. Depression
5. Anxiety
6. Hostility
7. Phobic anxiety
8. Paranoid ideation
9. Psychosis
Symptom Frequency/
Symptom Distress Scale
(SFSD) [20]
Generic A list of 27 symptoms Assesses the frequency of symptoms and the
distress caused by these symptoms
Transplant Symptom
Frequency and Distress
Scale (TSFQ) [21]
Generic 29-item questionnaire Assesses 29 symptoms commonly experienced
secondary to chronic illness and
immunosuppression
Karnofsky Performance
Status (KPS) [22]
Generic A list of 11 states of health
and for each state, an index
may be assigned ranging
from 0 (death) to 100
(health state
without problems)
Measure of patient functioning in day-to-day
activity. Evaluates intensity of treatment and
ability to take care of oneself
UCLA Loneliness
Scale–Revised [23]
Generic 20-item questionnaire Assesses the quality of relationship with
others. It consists of 2 subscales — loneliness
and companionship—and has a total
loneliness score
Difficulty with Adherence
(DWA) [24]
Generic 8-item questionnaire with a
4-point rating scale
Patients are asked to rate the degree of difficulty
in following posttransplant medical regimes in
the areas of
1. Taking medications regularly
2. Coming in for clinic regularly
3. Undergoing biopsies when necessary
4. Undergoing other invasive procedures
5. Abstaining from smoking
6. Abstaining from alcohol
7. Staying in shape
8. Keeping weight down
Sleep Disturbance
(SD) [24]
Generic 7-item questionnaire Measures the amount of sleep disturbance
experienced by patients during the previous 2 wk
Illness Intrusive
Rating Scale
(IIRS) [25]
Generic 13-item questionnaire Assesses patients’ perceptions of the degree
to which their transplant and the associated
posttransplant medical regimen interferes with
13 life domains, including work, active
recreation, passive recreation, financial situation,
relationship with spouse, sex life, family relations,
other social relations, self-expression and
self-improvement, religious expression, and
community and civic involvement
Body Cathexis
Scale (BC) [26]
Generic 46-item questionnaire Assesses the degree of a person’s satisfaction
with various parts or processes of the body
Derogatis Sexual
Functioning Inventory
(DSFI) [27]
Generic Self-report test of
sexual functioning
Assesses and quantifies nature of current sexual
functioning and comprises 10 subtests, including
information, experience, drive, attitude, psychologi-
cal symptoms, affects, gender role definition,
fantasy, body image, and sexual satisfaction
(continued on next page)
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 391

Table 1 (continued)
Name of instrument Type No. questions Domains assessed
Rosenberg Self-Esteem
Scale (RSES) [28]
Generic Composed of 10 items (5 are
positive and 5 negative).
Participants indicate the extent
to which they agree with each
statement on a scale of 1,
‘‘strongly agree,’’ to 4,
‘‘strongly disagree.’’ Higher
scores indicate lower
self-esteem
Measure of general self-esteem
Basic Personality
Inventory (BPI) [29]
Generic 240-item true/false
self-report inventory
Assesses 12 domains of psychopathology
Campbell Sense of
Well-Being Scale
(CSWBS) [30]
Generic 8 7-point semantic differential
scales of polarized adjectives
Assesses overall life quality
Perceived Social Support
Related to Transplantation
(PSS) [31]
Disease
specific
10-item questionnaire on a
4-point Likert-type
response scale
Assesses the extent to which individuals feel
supported by the people in their lives (ie, family,
friends, transplant team members)
Pulmonary-specific QOL
Scale (PQLS) [32]
Disease
specific
25-item questionnaire on a
5-point Likert-type
response scale
Assesses the effects of pulmonary disease on
7 areas
1. Physical functioning
2. Psychological/emotional status
3. Functional status/activities of daily living
4. Social activities
5. Intimacy/relationship/sexuality
6. Occupational functioning
7. View of self
Abbreviation: QOL, quality of life.
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407392
between QOL and variables such as diagnosis, gen-
der, and transplant type (ie, single versus bilateral).
Stilley et al [47] examined depression, anxiety,
anger-hostility, and overall quality of life in 36 lung
and 14 heart-lung transplant recipients. The mean
anxiety symptoms were elevated over normative
levels, and nearly half of the subjects showed clini-
cally significant distress in one or more areas. The
findings suggested that anxiety symptoms, relatively
common in patients with chronic lung disease, remain
relatively common after lung transplantation. The
pretransplant psychiatric history, educational level,
posttransplant caregiver support, and health concerns
were important independent predictors of the recipi-
ent psychological outcome. The study did not find
any significant differences between lung and heart-
lung recipients, but it lacked statistical power to
exclude such differences.
Anyanwu et al [40] used the EuroQol instru-
ment to compare 87 pretransplant candidates with
225 transplant recipients in four transplant units.
Health status of the pretransplant group was evaluated
over 3 months in two hospitals. There were 28 patients
listed for single-lung transplantation, 24 for bilateral
lung transplantation, and 34 for heart-lung transplan-
tation. Of the posttransplant respondents, 106 had
received single-lung transplants, 79 had received
bilateral lung transplants and 70 had received heart-
lung transplants. The analysis of the EuroQol ques-
tionnaires was divided into four epochs: 0 to 6 months,
7 to 18 months, 19 to 36 months, and more than
36 months, with 41, 43, 61, and 110 patients in each
epoch. QOL in all five EuroQol domains was better in
the transplanted group than in the waiting list group.
Sixty-one percent Of the wait-list patients, 61% ex-
perienced extreme problems in one or more of the five
EuroQol domains. One year after transplantation, 20%
of the single-lung transplant recipients and none of the
bilateral or heart-lung transplant recipients reported
extreme problems in one or more of the five domains.
The mean utility value of the waiting list group was
0.31 versus 0.61 for single-lung transplant, 0.82 for
bilateral transplant, and 0.87 for heart-lung transplant
recipients 3 years posttransplantation.
The utility values reported in the Anyanwu study
[40] were in agreement with other earlier published
reports [34,36,37,48,49]. The study explored other
utility measures by recording self-rated health status
using the visual analogue scale, which ranged from
0 (worst health) to 100 (best health). The pretrans-

Table 2
Quality-of-life studies in lung transplantation
Author journal,
year, study country Type of study Instruments
Type of
transplant
(no. patients)
Disease diagnosis
(no. of patients)
No. candidate
patients
No. recipient
patients Overall results
O’Brien et al [35],
J Epidemiol
Community Health,
1988, UK
Prospective
longitudinal
NHP HLT Not mentioned 48 28 at 3 mo
24 at 6 mo
13 at 12 mo
Recipients reported
significant improvement
in QOL at 3 mo
after transplant
Improvements sustained
at 6 and 12 mo
after transplant
NHP was found to be
easy to use as an
interview or postal
follow-up
Caine et al [34]
Transplant Proc,
1991, UK
Prospective
longitudinal
NHP HLT CF 54 13 out of 24 at
interval of 3–6 mo
after transplant
Recipients who
responded reported
marked improvement in
QOL after transplantation
Busschbach et al
[36], Chest, 1994,
Netherlands
Manzetti et al [56],
Heart Lung
Transplant,
1994, US
Cross-sectional
pilot study
Comparative
(comparison of
education versus
education plus
exercise on the
effects of QOL)
SG
TTO
KPS
EuroQol VAS
NHP
QWB
QLI
SFSD
BLT
NA
CF
Emphysema (1);
bronchiectasis (2);
CF (2); pulmonary
fibrosis (2);
sarcoidosis (2)
3
9 total; education
group (4);
education plus exercise
group (5)
3 (12, 14, and
16 mo after
transplant)
NA
Feasible to measure QOL
with SG, TTO, and
EuroQol-VAS
Patients do not experience
high levels of stress when
interviewer chooses
appropriate interviewing
settings
Lung transplantation
results in improvement
in QOL similar to that
after heart transplantation
QWB scores and 6-min
walk distance improved
over time in both groups
Similar improvement in
QOL and symptom
experiences between
(continued on next page)
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
393

Table 2 (continued)
Author journal,
year, study country Type of study Instruments
Type of
transplant
(no. patients)
Disease diagnosis
(no. of patients)
No. candidate
patients
No. recipient
patients Overall results
2 groups
Education plus exercise
conferred no benefit
beyond those achieved by
education alone
Gross et al [41];
Chest, 1995 US
Ramsey et al [44],
J Heart Lung
Transplant,
1995, US
Cross-sectional
longitudinal study
(5 before and after
transplant and
18 after transplant
at 2 time period)
Cross-sectional
MOS 20
KPS
IWB
SIP
SG
SLT (34)
BLT (7)
HLT (13)
SLT
BLT
COPD
A1AD
PPH
Others
Emphysema
CF
A1AD
IPF
PPH
Others
44
21
54 total
(16 at 6–18 mo
17 at 19–34 mo
21 at >35 mo
after transplant)
18 at 2 time points
18 months apart
23
Dramatic improvements
in health status and QOL
occurred after successful
lung transplant and remain
stable over time
Recipients reported
significantly higher level
of happiness, satisfaction
with life and health than
candidates
Recipients reported better
function on Karnofsky
Index and in every MOS
20 dimension except pain
No significant differences
in QOL between recipients
from 3 different time
periods suggesting that
the improvement remained
stable with time BOS
adversely affected quality
of life
Overall QOL improved
significantly after
transplantation
Most functional disabilities
improve after transplant
Significant improvement
in utility scores
in recipients
QOL gains may
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
394

not be equal for all
pretransplant conditions
Squier et al [50],
Am J Respir
Crit Care Med,
1995, US
Longitudinal
(evaluation of
whether baseline
QOL values
were predictive
of survival)
QWB
BDI
Not
mentioned
CF
COPD
Restrictive PVD
74 49 Pretransplant QWB
was the most significant
predictor of survival
Depression scores
were not predictive
of survival
Littlefield et al
[24], Gen Hosp
Psychiatry,
1996, Canada
Limbos et al
[42], Chest, 1997,
Canada and US
Comparison of QOL
between lung, heart,
and liver recipients
Cross-sectional
Female
patients only
MOS SF-36
MHI
STAI
UCLALSR
DWA
SD
IIRS
MOS SF-36
RSES
HADS
DSFI
BC
2 open-ended
questions
Lung, heart,
and liver
Not
mentioned
Not mentioned
Emphysema
CF
PPH
IPF
Congenital bronchiectasis
NA
7
263 recipients
(representing
a response
rate of 83%)
59 lung
55 heart
149 liver
Median time since
transplantation
was 26 mo
34 (representing
a response rate
of 63%)
Lung transplant
recipients reported
better functioning in
the domains of
physical, psychological
and social functioning
and less difficulty
complying with
medical regimens
than did heart and
liver recipients
Lung patients’ level
of functioning was
equivalent to or better
than published norms
for SF-36
Recipients reported
a higher level of
physical and
general health
No significant
difference in anxiety
Body satisfaction and
sexual functioning
were negatively
correlated with age
and depression
Body satisfaction
remained a concern
for 42% of recipients
No significant
(continued on next page)
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
395
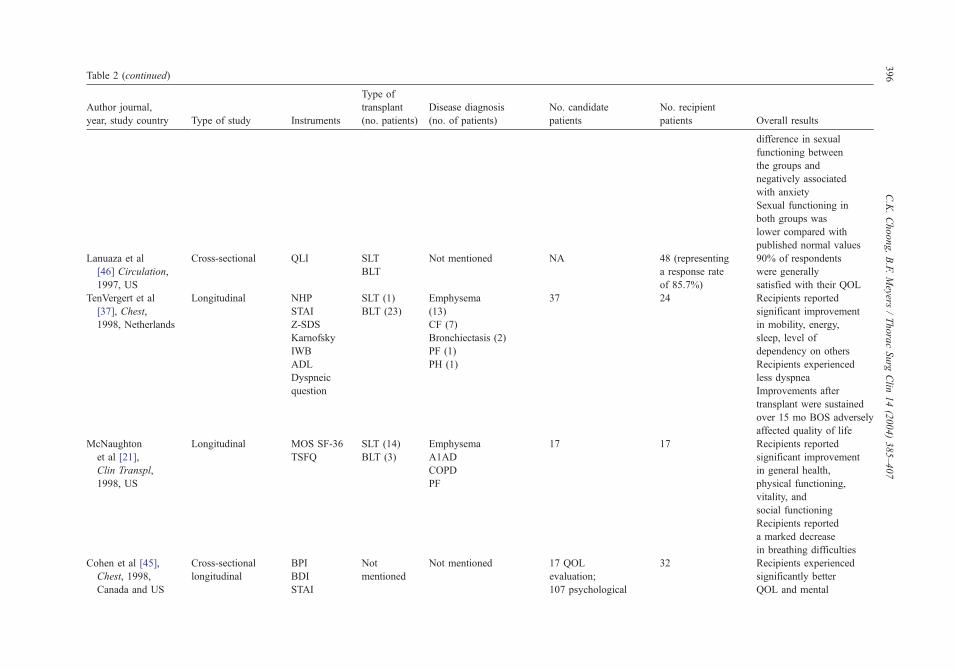
Table 2 (continued)
Author journal,
year, study country Type of study Instruments
Type of
transplant
(no. patients)
Disease diagnosis
(no. of patients)
No. candidate
patients
No. recipient
patients Overall results
difference in sexual
functioning between
the groups and
negatively associated
with anxiety
Sexual functioning in
both groups was
lower compared with
published normal values
Lanuaza et al
[46] Circulation,
1997, US
Cross-sectional QLI SLT
BLT
Not mentioned NA 48 (representing
a response rate
of 85.7%)
90% of respondents
were generally
satisfied with their QOL
TenVergert et al
[37], Chest,
1998, Netherlands
Longitudinal NHP
STAI
Z-SDS
Karnofsky
IWB
ADL
Dyspneic
SLT (1)
BLT (23)
Emphysema
(13)
CF (7)
Bronchiectasis (2)
PF (1)
PH (1)
37 24 Recipients reported
significant improvement
in mobility, energy,
sleep, level of
dependency on others
Recipients experienced
less dyspnea
question Improvements after
transplant were sustained
over 15 mo BOS adversely
affected quality of life
McNaughton
et al [21],
Clin Transpl,
1998, US
Cohen et al [45],
Chest, 1998,
Canada and US
Longitudinal
Cross-sectional
longitudinal
MOS SF-36
TSFQ
BPI
BDI
STAI
SLT (14)
BLT (3)
Not
mentioned
Emphysema
A1AD
COPD
PF
Not mentioned
17
17 QOL
evaluation;
107 psychological
17
32
Recipients reported
significant improvement
in general health,
physical functioning,
vitality, and
social functioning
Recipients reported
a marked decrease
in breathing difficulties
Recipients experienced
significantly better
QOL and mental
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
396
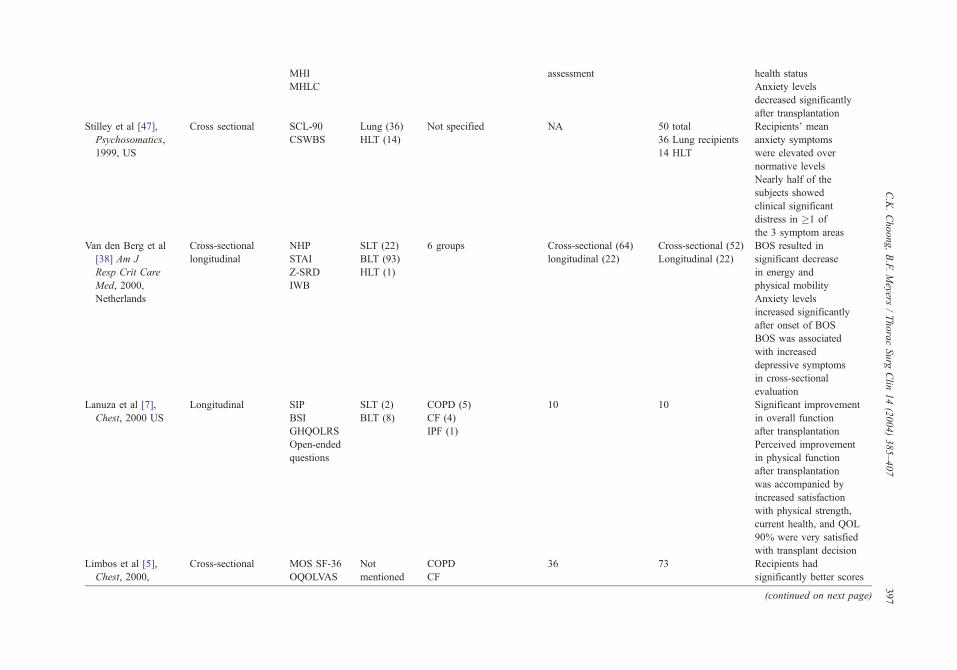
MHI
MHLC
assessment health status
Anxiety levels
decreased significantly
after transplantation
Stilley et al [47],
Psychosomatics,
1999, US
Cross sectional SCL-90
CSWBS
Lung (36)
HLT (14)
Not specified NA 50 total
36 Lung recipients
14 HLT
Recipients’ mean
anxiety symptoms
were elevated over
normative levels
Nearly half of the
subjects showed
clinical significant
distress in �1 of
the 3 symptom areas
Van den Berg et al
[38] Am J
Resp Crit Care
Med, 2000,
Netherlands
Lanuza et al [7],
Chest, 2000 US
Cross-sectional
longitudinal
Longitudinal
NHP
STAI
Z-SRD
IWB
SIP
BSI
GHQOLRS
Open-ended
questions
SLT (22)
BLT (93)
HLT (1)
SLT (2)
BLT (8)
6 groups
COPD (5)
CF (4)
IPF (1)
Cross-sectional (64)
longitudinal (22)
10
Cross-sectional (52)
Longitudinal (22)
10
BOS resulted in
significant decrease
in energy and
physical mobility
Anxiety levels
increased significantly
after onset of BOS
BOS was associated
with increased
depressive symptoms
in cross-sectional
evaluation
Significant improvement
in overall function
after transplantation
Perceived improvement
in physical function
after transplantation
was accompanied by
increased satisfaction
with physical strength,
current health, and QOL
90% were very satisfied
with transplant decision
Limbos et al [5],
Chest, 2000,
Cross-sectional MOS SF-36
OQOLVAS
Not
mentioned
COPD
CF
36 73 Recipients had
significantly better scores
(continued on next page)
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
397

Table 2 (continued)
Author journal,
year, study country Type of study Instruments
Type of
transplant
(no. patients)
Disease diagnosis
(no. of patients)
No. candidate
patients
No. recipient
patients Overall results
Canada BSI
DSFI
HADS
RSES
BC
PPH
IPF
Others
in the measures of MOS
SF-36 total, physical
health, role limitations due
to physical health, general
health, vitality, and social
functioning subscale
MOS SF-36 emotional
health and role limitations
were similar in candidate
and recipient groups
and lower than
published norms
Significant proportion of
patients in both groups
had borderline or clinical
levels of anxiety
The RSES and DSFI
mean scores were lower
than published norms in
both groups
TenVergert et al
[39], Psychol
Rep, 2001,
Netherlands
Longitudinal
comparative
(QOL in patients
with emphysema
versus other
indications)
NHP
STAI
Z-SRDS
IWB
KPS
RSQ
Not
mentioned
Emphysema (23)
Others (19)
(CF 8, PH 4, PF 2,
bronchiectasis 5)
Emphysema (23)
Other (19)
4, 7, 13, and
25 months after
transplantation
No significant
differences in
QOL between
emphysema and other
indications either before
or after transplantation
Before transplantation,
both groups reported
major restrictions on the
dimension of energy and
mobility of NHP, low
experienced well-being,
depressive symptoms, and
high dyspnea
About 4 mo after
transplantation,
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
398

most health-related
QOL measures
improved significantly
The improvements
noted after transplant
maintained in the
following 21 mo
Anyanwu et al [40],
Thorax, 2001, UK
Cross sectional
(before and after
transplant)
Comparative
(SLT versus BLT
& HLT)
EuroQol SLT
BLT
HLT
Not mentioned 87 (28 listed for
SLT, 24 for BLT,
34 for HLT)
225 (106 had
received SLT,
79 BLT
and 70 HLT)
Recipients experienced
significantly better QOL
BLT and HLT recipient
groups reported better
QOL than SLT
recipient group
Napolitano et al [31],
Chest, 2002, US
Comparative
(comparison
of telephone-based
psychosocial
intervention versus
none on the
effects of QOL
in candidates)
MOS SF-36
GHQ
PQLS
PSS
PSRT
NA COPD (25)
CF (9)
PPH (10)
Others (27)
Intervention (36)
Control (35)
NA Intervention group
reported greater
general well-being,
better general QOL,
better disease-specific
QOL, and higher level
of social support than
the control group
Abbreviations: ADL, Activities of daily living; A1AD, a1 antitrypsin deficiency; BC, Body Cathexis Scale; BDI, Beck depression inventory; BLT, bilateral lung transplant; BOS,
bronchiolitis obliterans syndrome; BPI, Basic Personality Inventory; BSI, Brief Symptom Inventory; CF, cystic fibrosis; COPD, chronic obstructive pulmonary disease; CSWBS, Campbell
Sense of Well-Being Scale; DSFI, Derogatis Sexual Functioning Inventory; DWA, difficulties with adherence; GHQ, general health questionnaire; GHQOLRS, General Health/QOL Rating
Scale; HADS, Hospital anxiety and depression scale; HLT, Heart-lung transplant; IWB, Index of Well-Being; KPS, Karnofsky performance status; MHI, Mental Health Inventory; MHLC,
Multidimensional Health Locus of Control Scales; MOS, Medical Outcome study; NA, not applicable; NHP, Nottingham Health Profile; OQOLVAS, Overall quality of life visual analogue
scale; PF, pulmonary fibrosis; PH, pulmonary hypertension; PPH, primary pulmonary hypertension; PQLS, pulmonary-specific quality-of-life scale; PSRT, perceived stress related to
transplantation; PSS, perceived social support related to transplantation; PVR, pulmonary vascular disease; QLI, Quality of Life Index; QOL, quality of life; QWB, Quality of Well-being
scale; RSES, Rosenberg Self-Esteem Scale; RSQ, respiratory-specific questions; SCL-90, Symptom Checklist-90; SD, sleep disturbance; SFSD, Symptom Frequency/Symptom Distress
scale; SG, Standard Gamble; SIP, Sickness Impact profile; SLT, single lung transplant; SRS, Satisfaction rating scale; STAI, State-Trait Anxiety Inventory; TSFQ, Transplant symptom
frequency and distress scale; TTO, Time Trade-Off; UCLALSR, UCLA Loneliness Scale-Revised; VAS, Visual Analogue Scale; Z-SDS, Zung-Self-rating Depression Scale.
C.K.Choong,B.F.Meyers
/ThoracSurg
Clin
14(2004)385–407
399

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407400
plant group had a mean score of 35 F 19 (FSD),
whereas the posttransplant groups had mean scores of
60 F 19 for single-lung transplant, 77 F 18 for
bilateral lung transplant, and 79 F 19 for heart-lung
transplant recipients at 3 years. The limitations in the
study included the assumptions that the health status
of the pretransplant group was constant and the
changes of the response variable were a reflection
of individual variations in health status rather than
factors related to the preoperative diagnosis or dura-
tion on the waiting list. The study did not take into
consideration that ill patients are more likely to be
nonparticipants and these same patients would have a
poor QOL. There was an additional selection bias in
that the sickest patients and the patients who died
either on the waiting list or early after lung trans-
plantation were excluded from the evaluation.
Longitudinal studies
Some studies evaluated QOL in a longitudinal
fashion, comparing the QOL differences with time
progression in the same group of patients. These
studies are more powerful in detecting differences
over time between groups of patients because the
use of sequential measurements in the same patients
reduces the variance and enhances statistical power.
Two early studies from the United Kingdom evaluated
QOL in the same patients before and after heart-lung
transplantation. In a prospective study, O’Brien et al
[35] used the Nottingham Health Profile in 48 candi-
dates and followed the patients after heart-lung trans-
plantation. Posttransplant evaluation was performed
in 28 recipients at 3 months, with the numbers
declining to 24 at 6 months and 13 at 12 months.
The study found a significant improvement in the
QOL at 3, 6, and 12 months posttransplantation. Caine
et al [34] evaluated the QOL of 54 candidates with
cystic fibrosis. Twenty-four patients underwent heart-
lung transplantation, and 13 of the 24 completed the
questionnaires 3 to 6 months posttransplantation. A
marked improvement in QOL was found among the
respondents after transplantation. Similar observa-
tional work has been reported by Gross et al [41].
Squier et al [50] investigated the association
between quality of well-being and survival in lung
transplant candidates. Predictors of survival were
evaluated for 74 transplant candidates. Each patient
completed the QWB, a utility-based outcome mea-
sure that gives a score on a continuum ranging from 0
(dead) to 1 (optimal function), and a measure of
depressive symptoms (Beck Depression Inventory).
During the study, 24 patients died, including 13 of 49
transplant recipients and 11 of 25 of the transplanted
patients. The most significant predictor of survival
was the QWB score. The study concluded that health-
related QOL was an important predictor of survival
for patients with serious lung diseases.
TenVergert et al [37] conducted a longitudinal
study on 24 Dutch lung transplant candidates and
followed them up at several intervals after lung
transplantation. Various generic QOL instruments
were used as outlined in Table 2. Disease-specific
questionnaires on severity of dyspnea also were
evaluated. The study enrolled 37 transplant recipi-
ents, 10 patients died during the study, and 3 other
patients were unable to complete questionnaires be-
cause of poor health. Although the study has a small
sample size of 24 responding patients, it allowed an
accurate evaluation in change in the QOL in the same
group of patients over time. Transplant candidates
reported major restrictions on mobility and energy in
the NHP. Also reported were low levels of well-
being, frequent depressive symptoms, difficulty in
performing activities of daily living, and low ability
for self-care. Improvements were recorded in mobil-
ity, energy, sleep, freedom from dependency on
others, and dyspnea 4 months posttransplantation.
These improvements were maintained in the follow-
ing 15 months.
Cohen et al [45] examined the predictors of QOL
posttransplantation by evaluating archival data for
107 transplant candidates with pretransplant psy-
chological assessments and posttransplant physical
health status data. Pretransplant anxiety, depression,
and personality inventory scores were not associated
with posttransplant physical health. Of the 107 can-
didates, 32 later completed adjustment and QOL
questionnaires after their transplantation. Signifi-
cantly improved QOL and mental health status were
found in the 32 patients posttransplantation. In
13 patients with data before and after transplantation,
anxiety levels decreased significantly after the opera-
tion. Pretransplant anxiety and psychopathology were
associated strongly with posttransplant adjustment
and QOL. Patients with posttransplant sleep distur-
bances had poorer adjustment and QOL.
Sustained improvement in QOL after lung trans-
plantation was found in several other longitudinal
studies [35,37,40,51]. These findings suggest that the
improved QOL among living and responding recipi-
ents remains. It is widely acknowledged, however,
that these findings of sustained improvement during
the follow-up period posttransplantation may be due
to selection bias because stable and healthy patients
were most likely to participate. Similarly the small
sample sizes may have had insufficient power to

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 401
detect statistical differences, or the length of time
between data collection intervals was too short.
Comparative studies
Quality-of-life differences between single-lung versus
bilateral lung recipients
Anyanwu et al [40] found that single-lung trans-
plant recipients reported more problems in all five
domains compared with bilateral lung transplant
recipients and heart-lung transplant recipients. The
health profiles and utility scores were consistently
better in bilateral lung transplant and heart-lung
transplant groups compared wth the single-lung trans-
plant group. These results also correlated with the
self-rated visual analogue scale scores. Apart from
Anyanwu’s study, few other studies specifically com-
pared the QOL of single-lung versus bilateral lung
recipients. Some studies indirectly support these
findings of better QOL in bilateral lung transplant
recipients versus single-lung transplant recipients
[52,53]. Gartner et al [52] assessed the health utility
of 16 single-lung transplant recipients and 4 bilateral
lung transplant recipients using a generic instrument
and reported a mean utility score of 0.60. A higher
utility score of 0.8 was reported by van Enckevort
et al [53] from the Dutch lung transplantation pro-
gram, in which most recipients had received bilateral
lung transplants (43 of 57). Physiologic differences
between single-lung and bilateral lung transplants
may provide additional explanations for the differ-
ences in observed posttransplant QOL [54]. Single-
lung transplant recipients have less improvement in
forced vital capacity and forced expiratory volume in
1 second (FEV1). Most recipients of two lungs
achieve their predicted total lung capacity within
1 year; however, similar improvements do not occur
with single-lung transplant recipients. In addition, the
presence of native disease in the contralateral non-
transplanted lung can cause physiologic and patho-
logic changes. Bavaria et al [55] reported results in
comparison of single-lung versus bilateral lung trans-
plantation in patients with emphysema and found
superiority in the FEV1, 6-minute walk test, and other
clinical indices in recipients of bilateral lungs com-
pared with patients who received a single lung. The
authors suggested that bilateral lung transplantation
provided better symptomatic improvement than sin-
gle-lung transplantation in patients with emphysema.
These physiologic differences may account for much
of the difference in QOL between the two operations.
Pretransplant differences between patients may play a
role as well. In the report from the United Kingdom,
single-lung transplantations were reserved primarily
for selected cases of emphysema and pulmonary
fibrosis [40]. Patients undergoing single-lung trans-
plantation are often older emphysema patients,
whereas bilateral lung transplant recipients are youn-
ger patients with cystic fibrosis. Native disease and
age of the patient may contribute further to the
differences in the posttransplant QOL observed be-
tween single-lung transplant and bilateral lung trans-
plant recipients.
Quality of life with emphysema versus other
indications
TenVergert et al [39] evaluated health-related
QOL before and after lung transplantation in patients
with emphysema and compared the results with other
end-stage lung disease diagnostic groups. Twenty-
three emphysema patients and 19 patients with other
indications completed self-administered question-
naires before lung transplantation and at intervals
after transplantation between 1992 and 1999. The
mean age in the emphysema group was 49.3 years,
and in all others it was 33.4 years (range 20 to
50 years). Male patients composed approximately
61% in the emphysema group and 42% in the other
group. The questionnaire included the NHP, the
STAI, the Z-SDS, the Index of Well-Being, the self-
report Karnofsky Index, and four respiratory-specific
questions. No significant differences were found
between the two diagnostic groups on most dimen-
sions of health-related QOL before or after transplan-
tation. Before transplantation, both groups reported
major restrictions on the dimensions of energy and
mobility of the NHP, low levels of well-being, de-
pressive symptoms, and high levels of dyspnea. Four
months after transplantation, most health-related
QOL measures improved significantly in both groups,
and these improvements were maintained in the fol-
lowing 21 months.
Influence of exercise and education on quality of
life in lung transplant candidates
Manzetti et al [56] evaluated the impact of an
exercise program on QOL in patients awaiting lung
transplantation. This pilot study served as an initial
step toward evaluating outcomes of a health mainte-
nance program on exercise tolerance and QOL. Nine
lung transplant candidates were randomized to par-
ticipate in a 6-week health maintenance program

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407402
consisting of education alone or education plus exer-
cise. The subjects completed cardiopulmonary exer-
cise testing, a 6-minute walk test, the QWB, Quality
of Life Index, and Symptom Frequency/Symptom
Distress scale before and after completion of the
program. QWB scores and 6-minute walk distance
improved over time in both groups. The study did not
find differences between the two groups. Candidates
awaiting lung transplantation perceived an improved
quality of well-being and increased walk distance
after participation in a health maintenance program,
but the addition of exercise did not confer any
additional benefits beyond the benefits achieved
by education.
Impact of bronchiolitis obliterans on quality of life
Few studies have evaluated the effect of BOS on
QOL. Gross and Raghu [48] reported on five recipi-
ents who developed BOS and found decrements in
their health-related QOL particularly in the dimen-
sions of physical functioning, social functioning, and
bodily pain. In a longitudinal study by TenVergert
et al [37], 6 of the 24 patients developed BOS within
19 months posttransplantation. Physical functioning
was significantly lower in these 6 patients compared
with the remaining 18 patients without BOS. The
study found no differences in the areas of social and
psychological functioning between the two groups. In
a cross-sectional evaluation by Van den Berg et al
[38], the QOL of 64 recipients without BOS was
compared with 52 recipients with BOS. Patients
with BOS reported more restrictions of energy and
physical mobility as captured by the NHP. The
domains of pain, sleep, social interaction, and emo-
tional reactions were not affected. Patients with
BOS also reported more depressive symptoms and
anxiety after transplantation. The study also per-
formed a longitudinal analysis on 22 recipients who
completed QOL questionnaires before and after the
development of BOS. The findings were similar to
the findings of the cross-sectional evaluation except
that no change in depressive symptoms could be
found after the onset of BOS. The authors’ explana-
tion for the decreased energy and physical mobility
in recipients with BOS was that it was due to a
decrease in lung function.
Employment
It seems logical that the ability to pursue active
employment would be associated strongly with QOL
and utility. Various studies have evaluated the QOL
and employment status in lung transplantation candi-
dates and recipients [35–37,39,44–46]. O’Brien et al
[35] reported that health-related employment prob-
lems decreased from a prevalence of 77% pretrans-
plantation to 15% posttransplantation. Other studies
have agreed that a large percentage of candidates
awaiting lung transplantation were not employed,
although improvements in QOL posttransplantation
have not reliably resulted in an improvement in
employment status. Gross et al [41] found no signifi-
cant change in the employment status between the
candidates and the transplant recipients. In their
study, 24% of the transplant candidates and 16% of
the recipients were employed part-time or full-time.
In the Dutch study, 25% of the patients were working
at a median duration of 20 hours a week before
transplantation [37]. Of the transplant candidates,
60% reported inability to work for pay as a result
of lung disease. Nineteen months after transplanta-
tion, 33% of the patients had returned to work part-
time with a median duration of 18 hours a week.
None of the patients had returned to paid employment
full-time. Cohen et al [45] also found that despite
the reported improvement in QOL, functioning, and
satisfaction after lung transplantation, there was
little change in employment patterns posttransplanta-
tion. The 1997 United Network for Organ Sharing
(UNOS) Registry Report for Heart and Lung Trans-
plantation [57] stated that although most lung trans-
plant patients have no limitations that should exclude
them from working, approximately 40%, not includ-
ing patients who are retired, are not working. It seems
that improvements in QOL do not correlate with
improvement in employment status.
Economic evaluations and cost-effectiveness
Despite the importance placed on cost analysis in
the current climate of escalating health care costs, few
studies have evaluated the cost-effectiveness of lung
transplantation. Ramsey et al [43] performed a pilot
study in the United States comparing the costs and
outcomes of the first 25 patients who received lung
transplantation at the University of Washington with
24 patients who were on the lung transplant waiting
list. The study calculated inpatient and outpatient
charges from hospital billing services and home
health agencies. Quality-adjusted life-year calcula-
tions as shown in Box 2 earlier were incorporated
into the study. The quality adjustments were derived
from utility scores obtained through Standard Gamble
interviews and survival data from the International

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 403
Lung Registry and published studies on lung trans-
plant waiting lists. Transplantation charges were
found to average $164,989 (median $152,071). The
average monthly posttransplant charges were calcu-
lated to be $11,917 in year 1 and $4525 for subse-
quent years, whereas the pretransplant monthly costs
for recipients were $3395. The QOL utility scores
were 0.80 in recipients and 0.68 in pretransplant
candidates. The calculated life expectancy was sim-
ilar between the two groups: The recipient group was
estimated at 5.89 years, and the candidate group
was estimated at 5.32 years. The incremental cost
per quality-adjusted life-year gained for lung trans-
plant patients was calculated to be $176,817. The
study concluded that lung transplantation can im-
prove quality of life substantially, but it is an expen-
sive treatment. The high costs of postrecovery care
and lower than expected life gains in life were the
principal barriers to cost-effectiveness. One might
question the representativeness of the cost data,
given the fact that the data were obtained in the
earliest period of lung transplant experience for the
reporting center.
Reports from the Netherlands suggest that lung
transplantation extends life expectancy approximately
4.5 years, whereas Dutch programs for heart and liver
transplantation showed extensions of life expectancy
by 9 to 15 years [53,58,59]. The average costs per life-
year gained for lung, heart, and liver transplantation
were 76,120 Euros, 32,840 Euros, and 26,870 Euros.
The study concluded that lung transplantation was an
expensive surgical treatment modality, and the cost-
effectiveness was unfavorable compared with other
solid-organ transplant programs due to the associated
substantial morbidity and mortality and the smaller
gain in survival [53,60]. Quality adjustment of the
survival is important because patients with emphy-
sema, the most common indication for lung trans-
plantation, may continue to live for many years on the
waiting list. This durability on the wait-list may result
in a limited calculated survival benefit for these
patients [1].
Anyanwu et al [61] performed an economic eval-
uation of lung transplantation in the United Kingdom,
analyzing and comparing the cost-effectiveness of
single-lung transplant, bilateral lung transplant, and
heart-lung transplant. The study evaluated a 4-year
cohort of patients involving 1030 patients on the
waiting list: 260 single-lung transplant, 199 bilateral
lung transplant, and 218 heart-lung transplant recipi-
ents. The 4-year national survival data were extrapo-
lated to 15 years by means of parametric techniques.
The EuroQol utility scores (scale 0 to 1) for this study
were obtained from a cross-section of patients in a
parallel study evaluating QOL in lung transplantation
[40]. The mean expected survival during the 15-year
period was 2.7 years in the medical group, 4.7 years
in the single-lung transplant group, 5 years in the
bilateral lung transplant group, and 5.2 in the heart-
lung transplant group. The EuroQol utility score was
0.31 in the medical group, whereas the recipient
groups had a better utility score of greater than
0.6 (range 0.61 to 0.87) during the each of 4 separate
postoperative QOL evaluation. The resultant quality-
adjusted life expectancies were 0.8 for the medical
group, 3.0 for the single-lung transplant group, 4.1
for the bilateral lung transplant group, and 4.4 for the
heart-lung transplant group, resulting in quality-ad-
justed life-year gains of 2.1 for single-lung transplant,
2.4 for bilateral lung transplant, and 2.5 for heart-lung
transplant groups. The mean cost of medical treat-
ment only in US dollars, was estimated at $73,564.
Costs for single-lung transplant were $176,640,
whereas cost estimates for bilateral lung transplant
and heart-lung transplant were $180,528 and
$178,387. The costs per quality-adjusted life-year
gained were $48,241 for single-lung transplant,
$32,803 for bilateral lung transplant, and $29,285
for heart-lung transplant. The sensitivity analysis
reported that the principal determinants of cost-
effectiveness were QOL and maintenance costs
after transplantation. The authors concluded that
although lung transplantation results in survival and
QOL gains, it was expensive, with cost-effectiveness
limited by substantial morbidity and mortality and
high maintenance costs.
Limitations and barriers to quality-of-life
assessment in lung transplantation clinical
practice
Although QOL now is recognized as an important
outcome measure in clinical practice, few institutions
have used it for lung transplantation. The major
barriers to routine QOL measurement seems to be
the complexity of some measurements requiring the
use of detailed questionnaires or interviews. These
techniques may require considerable time by the
patient and researcher. The lack of experience with
QOL measurements, the shortage of health care
personnel to coordinate and analyze the measure-
ments, and budget limitation further contribute to its
barriers in clinical practice.
Many limitations have been pointed out for each
of the QOL studies involving lung transplantation
and are outlined in Table 3. Most of the reports
evaluating QOL in lung transplantation have consid-

Table 3
Study limitations
Author, journal, year Limitations
O’Brien et al [35],
J Epidemiol Community Health, 1988
<50% of recipients completed questionnaires 12 mo
after transplant
No reasons stated for decrease in posttransplant response
Small no. of posttransplant respondents
The much less common practice of heart-lung transplantation
these days makes the results and generalizations of the
findings limited
Caine et al [34], Transplant Proc, 1991 Only 13 out of 25 recipients completed questionnaires
Small no. of posttransplant respondents
The much less common practice of heart-lung transplantation
these days makes the results and generalizations of the
findings limited
Busschbach et al [36], Chest, 1994 Small no. of patients in the cross-sectional study (3 candidates
and 3 recipient patients)
No indication of how comparable the cohort groups were
Some patients had problem associated with long-term
memory recall
Manzetti et al [56], Heart Lung
Transplant, 1994
Small sample size of 9 patients
Limited duration of follow-up
Gross et al [41], Chest, 1995 Small no. of patients in 3 separate recipient groups
Ramsey et al [44], J Heart Lung
Transplant, 1995
Cross-sectional study
Small sample size
Squier et al [50], Am J Respir
Crit Care Med, 1995
Small no. of subjects
Heterogeneity of sample
Limited long-term follow up
QWB scores accounted for a small but significant portion
of survival variance
Littlefield et al [24], Gen Hosp
Psychiatry, 1996
Mean age of lung transplant group was younger than that of
heart transplant group
Limbos et al [42], Chest, 1997 Exclusion of men limit ability to make generalization about
the findings
Small no. of subjects in candidate cohort
Large amount of missing data
20% of sample group did not complete the entire sexual
functioning tool, which meant that findings regarding sexual
tool may not be representative of the sample
Lanuaza et al [46], Circulation, 1997 Lack a pretransplant group for comparison
Small sample size for subgroup comparisons
TenVergert et al [37], Chest, 1998 13 patients did not complete posttransplant questionnaires
Small sample size
McNaughton et al [21], Clin
Transpl, 1998
Small sample size
Cohen et al [45], Chest, 1998 Cross-sectional study
Small no. of patients in longitudinal arm
Stilley et al [47], Psychosomatics, 1999 No pretransplant group for comparison
Small no. of patients in the 2 separate recipient groups
Van den Berg et al [38], Am J Resp
Crit Care Med, 2000
Cross-sectional study
Small no. of patients in longitudinal analysis
Less than half of patients with BOS (22 of 52) were involved
in the longitudinal analysis
Lanuza et al [7], Chest, 2000 Small sample size of 10 patients
Short posttransplant follow-up of 3 mo
(continued on next page)
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407404

Table 3 (continued)
Author, journal, year Limitations
Anyanwu et al [40], Thorax, 2001 Cross-sectional study
Preoperative diagnosis, duration on the waiting list, and type of
lung transplant proposed were not taken into consideration
No mention of no. of patients who declined participation
Abbreviations: BOS, bronchiolitis obliterans syndrome; QWB, Quality of Well-being scale.
C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 405
ered all lung transplant candidates and recipients as a
single homogeneous group. Lung transplant candi-
dates and recipients are a heterogeneous group of
patients, however. Patients on the transplant waiting
list have end-stage pulmonary disease that is the
result of one of many underlying diseases, including
emphysema, cystic fibrosis, pulmonary fibrosis, pul-
monary hypertension, and other causes. Most of the
studies on QOL in lung transplantation were not
controlled for the many important covariates that
might help explain QOL differences, such as gender,
age, comorbidities, and severity of lung disease.
While these variables are known to affect survival,
they also affect QOL and therefore must be adjusted
for [1]. Physiologic variables, such as FEV1, often
were not taken into consideration in most studies. The
influence of these variables on QOL is understudied
in lung transplantation. Despite the fact that gender
has been shown to influence risk of mortality in lung
transplantation, only a few studies have incorporated
gender as a study variable. Age may vary greatly
across lung transplant candidates due to different
diagnostic groups, such as younger age in patients
with cystic fibrosis and older age in patients with
chronic obstructive airway disease. Only a few
reports included type of transplant procedure as a
study variable, and the symptom experiences of lung
transplant patients were examined in only a few
studies [21,40,46,56]. In some studies in which
cohorts were considered similar for comparison, the
studies did not show or address the similarity in terms
of demographic data [34,36].
Various types of lung transplant procedures (sin-
gle-lung, bilateral, or heart-lung) are performed and
are determined by the patient’s underlying diagnosis,
institutional surgical practice, availability of organs,
and other factors. Earlier reports from the late 1980s
and early 1990s included many heart-lung and bilat-
eral lung transplant procedures [34,35]. The peak of
these procedures was reached around 1989, and since
then the most common procedures performed have
been single-lung and bilateral lung transplants. The
effects of these various procedures often were not
taken into consideration in the evaluation of QOL
after lung transplantation.
Most of the studies performed have been retro-
spective or cross-sectional in nature (see Table 2).
Cross-sectional studies may be useful in describing
QOL at a particular time but may not be accurate in
assessing changes over time because the cohorts of
patients before and after transplantation are different.
Only a few studies have been performed as a longi-
tudinal design evaluating prospective pretransplant-
to-posttransplant changes in the same group of
patients (Table 2). Some studies had only a few
patients in their study population, and some studies
did not describe methods in patient sampling [21,56].
Because many different QOL instruments were
used in different studies and in different countries,
interpretations in the comparisons of QOL results
across the various studies can be difficult, making
generalizations difficult. Some studies also did not
report the reliability and validity of the QOL instru-
ments used [5,7,21,24,31].
Summary
Despite the potential differences in patient char-
acteristics, study designs, and types of instruments
used, this review of the literature showed several
common findings. Important improvements in QOL
are reported after lung transplantation. These im-
provements were observed when cross-sectional
comparisons were made across the cohort of candi-
dates and recipients and during longitudinal follow-
up of patients at pretransplant and posttransplant
time points. The improvements in QOL after trans-
plantation seem to be sustained for at least 1 to
3 years after transplant. Lung transplant recipients
generally were satisfied with their decision to have
undergone transplantation.
Many issues require further clarification. Variables
that may influence QOL before and after lung trans-

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407406
plantation, such as age, sex, pretransplant diagnosis,
and type of procedure performed, should be consid-
ered carefully as study variables. Carefully designed,
prospective longitudinal studies with many patients
would result in stronger conclusions regarding the
importance of QOL assessment in lung transplanta-
tion. It would be useful for a few QOL measurement
tools to emerge as standard instruments so that many
centers and investigators could adopt them to use
independently. Standard instruments would allow
comparison of outcomes between centers and would
allow meta-analyses of multiple studies using the
same methodology. Interpretation of the studies
would be improved because there would be improved
familiarity with a few tools, rather than vague recog-
nition of a large variety of tools.
References
[1] Hosenpud JD, Bennett LE, Keck BM, et al. Effect of
diagnosis on survival benefit of lung transplantation
for end-stage lung disease. Lancet 1998;351:24–7.
[2] Hunt MS, McEwen J, McKenna SP. Measuring health
status. London: Croom Helm; 1986.
[3] EuroQol-Group. EuroQol: a new facility for the mea-
surement of health related quality of life. Health Policy
(NY) 1990;16:199–208.
[4] Brooks R. EuroQol: the current state of play. Health
Policy (NY) 1996;37:53–72.
[5] Limbos MM, Joyce DP, Chan CK, Kesten S. Psy-
chological functioning and quality of life in lung
transplant candidates and recipients. Chest 2000;118:
408–16.
[6] Ware JE, Snow KK, Kosinki M, Gandek B. SF-36
health survey: manual and interpretation guide. Bos-
ton: The Health Institute; 1993.
[7] Lanuza DM, Lefaiver C, McCabe M, et al. Prospective
study of functional status and quality of life before and
after lung transplantation. Chest 2000;118:115–22.
[8] Goldberg DP, Hillier VF. A scaled version of the
General Health Questionnaire. Psychol Med 1979;9:
139–45.
[9] Anderson JP, Kaplan RM, Berry CC, et al. Interday
reliability of function assessment for a health status
measure: the Quality of Well-being Scale. Med Care
1989;27:1076–83.
[10] Ferrans CE, Powers MJ. Quality of life index: devel-
opment and psychometric properties. Adv Nurs Sci
1985;8:15–74.
[11] Campbell A. Subjective measures of well-being. Am
Psychol 1976;31:117–24.
[12] Eisen GM, Locke 3rd GR, Provenzale D. Health-related
quality of life: a primer for gastroenterologists. Am
J Gastroenterol 1999;94:2017–21.
[13] Bergner M, Bobbitt RA, Carter WB. The Sickness
Impact Profile: development and final revision of a
health status measure. Med Care 1981;19:787–805.
[14] Zigmond AS, Snaith RP. The hospital anxiety and de-
pression scale. Acta Psychiatr Scand 1983;67:361–70.
[15] Spielberger CD, Vagg PR, Barker LR, et al. The factor
structure of the State-Trait Anxiety Inventory. In: Sara-
son IG, Speilberger CD, editors. Stress and anxiety,
vol. 7. New York: Hemisphere; 1980. p. 167–89.
[16] Beck AT, Ward CH, Mendelson M, et al. An inventory
for measuring depression. Arch Gen Psychiatry 1961;
4:561–71.
[17] Zung WWK, Durham NC. A self-rating depression
scale. Arch Gen Psychiatry 1980;35:243–9.
[18] Derogatis LR. SCL-90-R: Symptom Checklist 90 re-
vised: administration, scoring, and procedure manual.
3rd edition. Minneapolis, MN: National Computer
Systems Inc.; 1994.
[19] Derogatis LR, Spencer PM. The brief symptom inven-
tory (BSI): administration scoring and procedures man-
ual. Baltimore: Clinical Psychometric Research; 1982.
[20] Lough ME, Lindsy AM, Shinn JA, Stotts NA. Impact
of symptom frequency and symptom distress on self-
reported quality of life in heart transplant recipients.
Heart Lung 1987;16:193–200.
[21] MacNaughton KL, Rodrigue JR, Cicale M, Staples
EM. Health-related quality of life and symptom fre-
quency before and after lung transplantation. Clin
Transplant 1998;12:320–3.
[22] Grieco A, Long CJ. Investigation of the Karnofsky
performance status as a measure of quality of life.
Health Psychol 1984;3:129–42.
[23] Cutrona EE. Transition to college: loneliness and
the process of social adjustment. In: Peplau SA, Perl-
man D, editors. Loneliness: a sourcebook of current
theory, research and therapy. New York: Wiley-Inter-
science; 1982. p. 291–309.
[24] Littlefield C, Abbey S, Fiducia D, et al. Quality
of life following transplantation of the heart, liver,
and lungs. Gen Hosp Psychiatry 1996;18(6 Suppl):
36S–47S.
[25] Devins GM, Binik YM, Hutchinson TA, et al. The
emotional impact of end-stage renal disease: impor-
tance of patients’ perceptions of intrusiveness and con-
trol. Int J Psychiat Med 1986;13:327–43.
[26] Secord PF, Jourard SM. The appraisal of body cathexis:
body-cathexis and the self. J Consult Psychol 1953;17:
343–7.
[27] Derogatis LR. Derogatis Sexual Functioning Inven-
tory (DSFI). Baltimore: Clinical Psychometric Re-
search; 1975.
[28] Rosenberg M. Society and the adolescent self image.
Princeton, NJ: Princeton University Press; 1965.
[29] Kroner DG, Reddon JR, Beckett N. Basic personality
inventory clinical and validity scales: stability and in-
ternal consisteny. J Psychopathol Behav Assess 1991;
13:147–54.
[30] Campbell A, Converse PE, Rodgers WL. The quality
of American life: perceptions, evaluations, and satis-
factions. New York: Russel Sage Foundation; 1976.

C.K. Choong, B.F. Meyers / Thorac Surg Clin 14 (2004) 385–407 407
[31] Napolitano MA, Babyak MA, Palmer S, et al. Effects
of a telephone-based psychosocial intervention for pa-
tients awaiting lung transplantation. Chest 2002;122:
1176–84.
[32] Napolitano MA. Development of a pulmonary-specific
quality of life scale (PQLS) [abstract]. Ann Behav Med
1999;21:S168.
[33] Torrance GW. Measurement of health state utilities for
economic appraisal. J Health Econ 1986;5:1–30.
[34] Caine N, Sharples LD, Smyth R, et al. Survival and
quality of life of cystic fibrosis patients before and
after heart-lung transplantation. Transplant Proc 1991;
23(1 Pt 2):1203–4.
[35] O’Brien BJ, Banner NR, Gibson S, Yacoub MH. The
Nottingham Health Profile as a measure of quality of
life following combined heart and lung transplantation.
J Epidemiol Community Health 1988;42:232–4.
[36] Busschbach JJ, Horikx PE, van den Bosch JM, et al.
Measuring the quality of life before and after bilateral
lung transplantation in patients with cystic fibrosis.
Chest 1994;105:911–7.
[37] TenVergert EM, Essink-Bot ML, Geertsma A, et al. The
effect of lung transplantation on health-related quality
of life: a longitudinal study. Chest 1998;113:358–64.
[38] van Den Berg J, Geertsma A, van Der Bij W, et al.
Bronchiolitis obliterans syndrome after lung transplan-
tation and health-related quality of life. Am J Respir
Crit Care Med 2000;161:1937–41.
[39] TenVergert EM, Vermeulen KM, Geertsma A, et al.
Quality of life before and after lung transplantation
in patients with emphysema versus other indications.
Psychol Rep 2001;89:707–17.
[40] Anyanwu AC, McGuire A, Rogers CA, Murday AJ.
Assessment of quality of life in lung transplantation
using a simple generic tool. Thorax 2001;56:218–22.
[41] Gross CR, Savik K, Bolman RM, Hertz MI. Long-term
health status and quality of life outcomes of lung trans-
plant recipients. Chest 1995;108:1587–93.
[42] Limbos MM, Chan CK, Kesten S. Quality of life in
female lung transplant candidates and recipients. Chest
1997;112:1165–74.
[43] Ramsey SD, Patrick DL, Albert RK, et al. The cost-
effectiveness of lung transplantation: a pilot study.
Chest 1995;108:1594–601.
[44] Ramsey SD, Patrick DL, Lewis S, et al. Improvement
in quality of life after lung transplantation: a prelimi-
nary study. The University of Washington Medical
Center Lung Transplant Study Group. J Heart Lung
Transplant 1995;14:870–7.
[45] Cohen L, Littlefield C, Kelly P, et al. Predictors of
quality of life and adjustment after lung transplanta-
tion. Chest 1998;113:633–44.
[46] Lanuza DM, Norton N, McCabe M, Garrity JE. Lung
transplant patients’ quality of life and symptom expe-
riences. Circulation 1997;96:I2460.
[47] Stilley CS, Dew MA, Stukas AA, et al. Psychological
symptom levels and their correlates in lung and heart-
lung transplant recipients. Psychosomatics 1999;40:
503–9.
[48] Gross CR, Raghu G. The cost of lung transplantation
and the quality of life post-transplant. Clin Chest Med
1997;18:391–403.
[49] Dennis C, Caine N, Sharples L, et al. Heart-lung trans-
plantation for end-stage respiratory disease in patients
with cystic fibrosis at Papworth Hospital. J Heart Lung
Transplant 1993;12(6 Pt 1):893–902.
[50] Squier HC, Ries AL, Kaplan RM, et al. Quality of well-
being predicts survival in lung transplantation candi-
dates. Am J Respir Crit Care Med 1995;152(6 Pt 1):
2032–6.
[51] Gross CR, Savik K, Bolman 3rd RM, Hertz MI.
Long-term health status and quality of life outcomes of
lung transplant recipients. Chest 1995;108:1587–93.
[52] Gartner SH, Sevick MA, Keenan RJ, Chen GJ. Cost-
utility of lung transplantation: a pilot study. J Heart
Lung Transplant 1997;16:1129–34.
[53] van Enckevort PJ, ten Vergert EM, Bonsel GJ, et al.
Technology assessment of the Dutch lung transplanta-
tion program. Int J Technol Assess Health Care 1998;
14:344–56.
[54] Girgis RE, Fishman R, Theodore J. Physiology and
pharmacology of the transplanted lung. In: Cooper
D, Miller LW, Patterson GA, editors. The transplanta-
tion and replacement of thoracic organs. Dordrecht:
Kluwer; 1996. p. 489–504.
[55] Bavaria JE, Kotloff R, Palevsky H, et al. Bilateral
versus single lung transplantation for chronic obstruc-
tive pulmonary disease. J Thorac Cardiovasc Surg
1997;113:520–7.
[56] Manzetti JD, Hoffman LA, Sereika SM, et al. Exercise,
education, and quality of life in lung transplant candi-
dates. J Heart Lung Transplant 1994;13:297–305.
[57] Keck BM, Bennett LE, Fiol BS, Daily OP, Novick RJ,
Hosenpud JD. Worldwide thoracic organ transplanta-
tion: a report from UNOS/ISHLT International Regis-
try for Thoracic Organ Transplantation. Clin Transpl
1998;12:39–52.
[58] Bonsel GJ, Klompmaker IJ, Essink-Bot ML, et al. Cost-
effectiveness analysis of the Dutch liver transplantation
programme. Transplant Proc 1990;22:1481–4.
[59] Geertsma A, TenVergert EM, de Boer WJ, van der Bij
W. The need for lung transplantation in the Nether-
lands. Transpl Int 1997;10:457–61.
[60] Al MJ, Koopmanschap MA, van Enckevort PJ,
et al. Cost-effectiveness of lung transplantation in
The Netherlands: a scenario analysis. Chest 1998;113:
124–30.
[61] Anyanwu AC, McGuire A, Rogers CA, Murday AJ.
An economic evaluation of lung transplantation.
J Thorac Cardiovasc Surg 2002;123:411–20.
[62] Ware JE, Sherbourne CD. The MOS 36-item short-
form health survey (SF-36): I. conceptual framework
and item selection. Med Care 1992;30:473–83.

Thorac Surg Clin 14 (2004) 409–416
Return to work after thoracic surgery: an overlooked
outcome measure in quality-of-life studies
Chuong D. Hoang, MDa, Marc C. Osborne, BSa,Michael A. Maddaus, MDa,b,*
aSection of General Thoracic Surgery, Division of Cardiovascular and Thoracic Surgery,
University of Minnesota Medical School, 420 Delaware Street S.E., MMC 207, Minneapolis, MN 55455, USAbCenter for Minimally Invasive Surgery, University of Minnesota Medical School, Minneapolis, MN 55455, USA
A report from the National Center for Health Sta- Numerous studies have investigated thoroughly
tistics in 2000 (http://www.cdc.gov/nchs/fastats/
insurg.htm) showed that every year in the United
States, nearly 1 million thoracic procedures are per-
formed to treat patients with malignant and nonma-
lignant pathology—a number almost twice that for
coronary artery bypass graft surgery [1]. Tradition-
ally, open thoracotomy has been the technique of
choice. The usual patient rehabilitation period has
been prolonged, requiring 6 to 8 weeks. During this
period, the patient is not likely to resume normal
activity or be able to return to work. Increasingly,
chest physicians are beginning to recognize that
optimization of the number of thoracic surgery
patients who return to work must be considered an
important outcome measure and rehabilitation aim.
Multiple series (discussed subsequently) from the
minimally invasive thoracic surgery literature suggest
that earlier return to work can be achieved and is
likely more desirable for patients and cost-effective
for health care systems. In a public survey of patients
undergoing a chest organ transplant, 72% of respon-
dents agreed that the recipient’s return to work or
ability for other regular activity was second in im-
portance only to survival [2,3].
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00026-X
* Corresponding author. Section of General Thoracic
Surgery Division of Cardiovascular and Thoracic Surgery,
University of Minnesota Medical School, 420 Delaware
Street S.E., MMC 207, Minneapolis, MN 55455.
E-mail address: [email protected]
(M.A. Maddaus).
the return-to-work rate and factors that influence it in
patients undergoing surgical procedures such as
inguinal hernia repair [4], coronary artery bypass
graft surgery [5], and kidney transplants [6]. Similar
studies have not been published, however, to the best
of the authors’ knowledge, that directly pertain to
thoracic surgical procedures involving the lung or
esophagus. Data on this topic are currently available,
in general, only as related components of a limited
number of quality-of-life (QOL) studies dealing with
thoracic cancer resection and less so with benign
thoracic pathologies. The authors reviewed selected
studies that investigated QOL after thoracic surgery
and included at least partial return-to-work data. To
underscore the broad implications of an improved
understanding of return to work after thoracic sur-
gery, first the general concepts of worker absenteeism
are discussed. By identifying the deficiencies in the
literature, the authors hope to help inspire a logical
series of much-needed clinical studies to bring clari-
fication to this important topic.
Worker absenteeism for surgical procedures
In analyzing the costs of illness among their
employees, American businesses generally classify
the costs into two groups: direct and indirect costs
[7]. Direct costs are costs that can be measured or
calculated easily, such as payments for medical goods
and services to health maintenance organizations or
insurance companies. Indirect costs are a broad cate-
s reserved.

C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416410
gory of expenses incurred secondary to an employ-
ee’s illness, including costs of recruitment, training,
and other accommodations to temporary, long-term
absence or to permanent loss of a skilled worker.
Worker absenteeism serves as a proxy for these
indirect costs of illness; often, absenteeism is meant
to measure worker ‘‘productivity.’’ Calculating indi-
rect costs of illness by using worker absenteeism rates
is not straightforward, however.
In 1989, one review estimated that American
businesses spend about $37 billion per year because
of employees’ absence from work [8]. In addition to
the significant societal costs, employees incur sizable
personal costs that are more difficult to quantitate di-
rectly. A sense of the magnitude of these costs may be
inferred from Department of Labor statistics (2003)
indicating that although most (79%) employees in
private industry earn some paid time off, relatively
few carry either short-term (37%) or long-term (28%)
disability insurance that would cover their lost wages
in the event of an extended absence [9]. A significant
percentage of workdays lost are the result of surgical
procedures to correct common health problems. The
Department of Labor includes surgical procedures
such as aortocoronary artery bypass, cholecystecto-
my, appendectomy, abdominal hysterectomy, and
mastectomy, but makes little or no mention of tho-
racic surgical procedures. Nevertheless, it is likely
safe to infer that the costs of thoracic surgery would
be considerable.
Return to work as a valid outcome measure
The ability to resume normal work activity
(ie, return to work) is the equivalent clinical assess-
ment of health-related worker absenteeism, a con-
struct more often used by economists and public
health experts. An operational definition of return
to work is the time elapsed between undergoing a
surgical procedure and returning to normal daily
activities. Although return to work can be measured,
there are large overall variations in reported rates,
even among closely related studies [10,11]. Return to
work after a particular type of surgical procedure is
poorly understood and vaguely defined.
Jones et al [4] conducted a prospective study in
inguinal hernia repair patients to characterize better
the confounding variables that may affect return to
work after surgery. Bivariate analysis showed that
nonsurgical factors, such as age, education level,
income level, and type of occupation, significantly
influenced the actual return-to-work rate postopera-
tively. Mittag et al [5] reached similar conclusions
in a comparative analysis of return to work after cor-
onary artery bypass graft surgery, which represents
a much more complicated disease and a much more
invasive procedure (compared with inguinal her-
nia epair).
Those two studies, taken together, suggest that
(1) return to work is a complex concept, influenced
not only by the type of surgical procedure, but also by
a multitude of other variables; (2) the issue of return
to work after many types of surgical procedures
warrants further investigation; and (3) return to work
is a highly desirable outcome measure as perceived
by patients and increasingly by the health care in-
dustry. The central importance and validity of return
to work after thoracic surgical procedures are likely to
be high.
Return to work after thoracic surgery
The authors identified potentially relevant articles
in the National Library of Medicine PubMed database
(1966–2003) by computerized methods in two inde-
pendent searches (C.D.H and M.C.O). The following
key words were used (combined with the Boolean
operators ‘‘OR’’): return to work, RTW, quality of life,
QOL, thoracic, lung, esophagus, surgery, video-
assisted thoracoscopic, and VATS. These two
searches provided the initial database of articles for
review. Additional possible articles were found by
manual searches. There were no specific criteria for
inclusion of articles, but articles were excluded if
they were not in the English language. A total of
69 journal articles were reviewed.
Specific studies aimed at investigating the impact
of thoracic surgery on return-to-work or on inability-
to-work rates remain to be published. Preoperative
employment status and return to work were men-
tioned briefly in a few studies, although rarely dis-
cussed in depth (Table 1). In general, those two
variables were documented as part of a global effort
to study QOL issues resulting from thoracic surgery
for a variety of pathologic processes, such as lung
cancer, esophageal cancer, and other nonmalignant
diseases (eg, spontaneous pneumothorax).
Lung cancer
Lung cancer is among the most common of ma-
lignancies in the United States, accounting for 14%
of all malignancies [12]. Most lung cancer patients
have non– small cell lung carcinoma (NSCLC).
NSCLC accounts for more cancer-related deaths

Table 1
Selected thoracic surgery studies with return-to-work results
Study Design Surgical intervention
Instrument used
or end point RTW results
Lung cancer Dales et al [18]
(1994)
Prospective
cohort
Open thoracotomy QL Index Work-related activity impairment levels were:
24% preoperative, increased to 52% at 1 mo
postoperative, and returned to baseline at 6 mo
(27%) and 9 mo (17%). Extent of resection
correlated with worsening QOL
Zieren et al [20]
(1996)
Prospective
cohort
Open thoracotomy Self-developed
questionnaire
Preoperative, 50% of patients were employed
full-time and 25% were retired due to
disease-induced limitations. At 5 mo
postoperative, 60% returned to full-time
employment, 40% of patients retired permanently
Demmy et al [21]
(1999)
Case-control VATS versus
thoracotomy
Average time to
return of full activity
Survivors in the VATS group returned to full
activity on average at 2.2 mo postoperative
versus 3.6 mo for thoracotomy. At 3 mo
postoperative 31% of VATS patients had limited
activity versus 44% of thoracotomy patients
Sugiura et al [22]
(1999)
Prospective
cohort
VATS versus
thoracotomy
Average time to
resume normal
activity; self-developed
questionnaire
VATS patients resumed normal activity at 2.5 mo
postoperative versus 7.8 mo for thoracotomy patients
Esophageal cancer Zieren et al [31]
(1996)
Prospective
cohort
Transthoracic
or transhiatal
Self-developed
questionnaire
Postoperative, 30% of patients remained employed
full-time; no preoperative data presented.
McLarty et al [28]
(1997)
Prospective
cohort
Transthoracic Medical Outcomes
Study Short Form-36
at 5 y postoperative
No significant difference in RTW in patients
undergoing esophageal resection compared with a
cancer-free matched population
Benign thoracic
pathology
Paris et al [35]
(1998)
Prospective
cohort
Bilateral or
single-lung
transplantation
Self-developed
questionnaire
Preoperative, 50% of patients were employed and
44% were medically disabled. At median follow-up
of 25 mo postoperative, 22% were employed, 38%
were unemployed but medically fit to work, and
29% were disabled
Stammberger et al
[34] (2000)
Prospective
cohort
VATS (PTX,
SPN, pleura, or
interstitial lung)
Self-developed
questionnaire
Of 140 patients employed preoperative, 89%
returned to work within 2 wk and 99% returned
within 12 wk
Abbreviations: PTX, pneumothorax; QL or QOL, quality of life; RTW, return to work; SPN, solitary pulmonary nodule; VATS, video-assisted thoracoscopic surgery.
C.D.Hoanget
al/ThoracSurg
Clin
14(2004)409–416
411

C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416412
than the next three most common malignancies
(breast, prostate, and colon) combined [12].
For the estimated 9 million US cancer survivors,
self-reported multidimensional health-related QOL
descriptions of physical and social well-being (among
other parameters) after their diagnosis and treatment
have been increasing steadily [13,14]. Information on
lung cancer survivors in general remains sparse,
however. QOL end points have become important
benchmarks for evaluating short-term and long-term
results for lung cancer survival [15]. Detailed infor-
mation on return-to-work rates after lung cancer
thoracotomy to treat cancer remains elusive.
Open surgical series
Schag et al [16] were among the first researchers
to comment specifically on return to work after
thoracic surgery in a cross-sectional QOL study of
lung, prostate, and colon cancer survivors who were
now disease-free. In their report on a sample of
57 lung cancer patients, the specific type of surgical
procedure was not made available. Overall, the lung
cancer group had more problems at short-term, inter-
mediate-term, and long-term time points (compared
with the other cancer groups). Exact figures were
unavailable, but the lung cancer group had more
difficulty in the postoperative period with return to
work and with the ability to function at near their
preoperative capacity. The Schag study revealed
many deficiencies with regard to return to work,
which the authors likely never intended to address
directly. This theme persists in other, more recent
studies on QOL after lung cancer thoracotomy.
Handy et al [17], in their prospective study of
131 patients, documented QOL as a function of lung
cancer surgical resection but failed to report all of
their available data pertaining to return to work. Their
outcomes questionnaire included employment status;
however, only the preoperative employment figure
(32.4%) was mentioned in their results.
In contrast, Dales et al [18] prospectively enrolled
117 patients who underwent thoracotomy with a
certain or presumptive diagnosis of lung cancer. Their
study documented multiple QOL variables, including
work activity, at four separate postoperative time
points up to 9 months. They compared patients with
proven NSCLC (n = 91) with patients without ma-
lignancy (n = 26). Work-related activity was assessed
by using the QL-index [19]; scores were arbitrarily
dichotomized into ‘‘better’’ (not defined by the
authors) and ‘‘poor’’ (defined as requiring major
assistance or reduction in work, not working/study-
ing, or not managing a household) scores. Work-
related activity already was impaired in 26% (n = 24)
of NSCLC patients preoperatively, a percentage that
increased to 52% (n = 47, P < .005) at 1 month post-
operatively. The impairment in work-related activity
returned to preoperative baseline at 6 (27%, n = 25)
and 9 (19%, n = 17) months in survivors. The reason
for curtailed work (or home) activities preoperatively
and at 9 months postoperatively was due to dyspnea,
as measured by the Clinical Dyspnea Index. The
extent of surgical resection negatively correlated with
global QOL scores, but it was not possible to deter-
mine, from the data as presented, whether or not this
observation held true for return-to-work rates.
Similarly, Zieren et al [20] addressed the return-
to-work issue in two groups of patients with bron-
chogenic NSCLC who underwent open thoracotomy.
Employment status was assessed directly in 52 ‘‘post-
operative’’ patients and in another 20 ‘‘follow-up’’
patients. The postoperative group comprised patients
who had a curative resection and completed a QOL
analysis at 1 year after surgery; the follow-up group
comprised disease-free survivors who completed
QOL assessments preoperatively and postoperatively
(at a total of six time points) 1 year after surgery.
Only 50% (n = 10) of the follow-up patients were
employed full-time preoperatively; another 25%
(n = 5) of follow-up patients reported that they retired
preoperatively due to disease-induced job limitations.
After a median of 5 months postoperatively, 60%
(n = 6) of follow-up patients returned to full-time
employment; the other patients in this group retired
permanently. Some follow-up patients underwent
postoperative radiotherapy for N2 disease, but Zieren
et al [20] were not able to determine any significant
return-to-work differences in radiotherapy patients
versus patients receiving only surgery. The return-
to-work information in the postoperative group was
less complete, with no preoperative employment sta-
tus given. At 1 year postoperatively, 63% (n = 33)
of the postoperative patients had retired perma-
nently, and only 12% (n = 6) of patients were em-
ployed full-time.
Minimally invasive surgical series
Return-to-work rates have been cited more fre-
quently in minimally invasive thoracic surgery stud-
ies to support the argument that this surgical approach
is more beneficial to patients. Overall the available
literature suggests that return-to-work ability is likely
to be better preserved with minimally invasive tech-
niques (compared with traditional open thoracotomy).
This conclusion is based on only a few studies that
present partial data on postoperative ability to resume
normal activity—not on direct effects related to return
to work.

C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416 413
Demmy and Curtis [21] compared 38 patients
who required lung resection for bronchogenic malig-
nancy in a case-control study design. Nineteen
patients with a high preoperative risk underwent
video-assisted thoracoscopic surgery (VATS). Their
functional outcomes were compared with outcomes
of 19 patients who underwent thoracotomy. Survivors
in the VATS group were able to return to ‘‘full
activity’’ at an average of 2.2 months, whereas the
thoracotomy group required a significantly longer
average of 3.6 months (P < .001). The authors
presume that the term full activity encompassed, in
part, return to work ability, albeit not directly
assessed. At 3 months postoperatively, only 31%
(n = 5) of VATS patients had limited activity versus
44% (n = 8) of thoracotomy patients (P < .01).
Logistic regression analyses did not show post-
operative reduced activity levels to be an indepen-
dent risk factor for morbidity and mortality.
Similarly, Sugiura et al [22] compared long-term
QOL using a self-developed questionnaire in patients
with stage I NSCLC who underwent lobectomy by
VATS (n = 22) versus by thoracotomy (n = 22). The
VATS patients resumed ‘‘normal activity’’ within an
average of 2.5 months, which was significantly
shorter than the average of 7.8 months required by
the thoracotomy patients (P < .03). Return to work
was not directly assessed, and the term normal
activity was never defined or discussed in detail.
Lewis et al [23] also made oblique reference to return
to work rates in a study of 250 VATS patients, stating
that most resumed preoperative activity within 7 to
10 days, and some returned to work in that period;
specific figures from this large cohort were not
presented, however.
Esophageal cancer
Most patients with esophageal cancer present with
advanced disease; overall 5-year survival rates are
poor. Early detection and surgical resection provide
the best chance for cure. Survival at 5 years for
patients with resected stage I esophageal carcinoma
is estimated at 50% to 85%; with resected stage II
carcinoma, survival is 20% to 50% [24–26]. World-
wide, most patients with esophageal cancer have the
squamous type. The incidence of adenocarcinoma
of the esophagus and the gastroesophageal junction
has risen fourfold, however, since the 1970s—the
most rapid increase of any type of cancer. Esophageal
adenocarcinoma now accounts for greater than 50%
of all cases of esophageal cancer in the United
States, causing about 10,000 deaths per year [27].
Compared with lung cancer, esophageal cancer has
been the focus of even fewer QOL studies performed
to evaluate the effect of surgical resection. Conse-
quently, information on return to work after esoph-
ageal resection that includes a thoracic incision
is incomplete.
McLarty et al [28] reported on long-term QOL in
64 patients who underwent esophageal resection (an
Ivor Lewis esophagogastrectomy for most) who were
disease-free at 5 years. The return-to-work ability
postoperatively was assessed with the Medical Out-
comes Study 36-Item Short-Form Health Survey;
the esophagectomy group was compared with the
national norm (a cancer-free matched patient popula-
tion). McLarty et al [28] found no significant differ-
ence in return to work, although detailed preoperative
and postoperative data were not available.
Branicki et al [29] observed at 1 month after
esophagectomy for cancer that few patients had
returned to full-time or part-time work and that most
were retired. Additional details were not available,
including the specific type of surgical procedure
performed. It is difficult to discern whether these
return-to-work results may be a consequence of a
thoracic incision. This same concern applies to pre-
operative work status figures reported by Blazeby et al
[30]: They did not mention the specific type of
surgical resection. In their study of QOL after esoph-
ageal cancer in a large cohort, only 28% (n = 74) of
patients were able to work full-time preoperatively;
they did not present postoperative data.
The study by Zieren et al [31], which assessed
employment status as part of a QOL study in two
patient groups who underwent esophageal surgery,
had similar shortcomings. A group (postoperative)
comprised 119 patients who completed a QOL ques-
tionnaire at 12 months postoperatively, and a second
group (follow-up) comprised 30 patients who com-
pleted QOL questionnaires preoperatively and post-
operatively at six time points up to 1 year. In the
postoperative group, only 30% (n = 36) of patients
remained in full-time employment. No preoperative
work data were presented. In the follow-up group,
50% (n = 15) of patients worked full-time, but the
effect of surgery on return to work could not be
discerned because postoperative work data were not
provided. These data should be interpreted with
caution because only 15% of all patients were ap-
proached via a transthoracic route; most patients had
an abdominal incision and transhiatal approach.
Benign thoracic pathology
The published reports on nonmalignant thoracic
conditions mention only briefly return-to-work issues

C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416414
related to the surgical procedure. Bousamra et al [32]
conducted a small (n = 17) study to compare out-
comes for patients who underwent VATS versus
thoracotomy for resection of benign neurogenic me-
diastinal tumors. On average, return to work required
less time for the VATS group (4.3 weeks) versus the
thoracotomy group (7.7 weeks), although the differ-
ence was not statistically significant. Bertrand et al
[33] also cited earlier ‘‘return to occupational activ-
ity’’ (42 F 34 days) in 163 young adults who
underwent VATS for spontaneous pneumothorax.
This interval was significantly (P < 0.001) shorter
compared with a matched group of 87 patients who
underwent lateral limited thoracotomy for the same
disease in a separate study, but required 74F 60 days
before their return to work. Both groups required
relatively lengthy periods before their return to work,
which was attributed to prevailing cultural attitudes
of the French population under study.
Stammberger et al [34] presented more complete
data regarding return-to-work issues in relation to
VATS for patients with pneumothorax (n = 70),
pulmonary nodules (n = 44), interstitial lung disease
(n = 20), pleural effusion (n = 20), and empyema
(n = 19). Of the 140 patients employed preoperatively,
125 (89%) were able to return to work within 2 weeks.
The other 15 patients, for a postoperative interval
of 3 to 16 weeks, were unable to return to work
(14 because of chest pain, 1 because of shoulder
pain). At 12 weeks postoperatively, a total of 139
(99%) of the patients who were employed preopera-
tively were able to return to work; 1 patient experi-
enced disabling shoulder pain. These impressive data
should be interpreted with caution, however, because
the study was retrospectively performed with an
unvalidated, self-reported questionnaire. The lack of
a control group of patients who underwent open
thoracotomy is another serious limitation.
Lung transplantation is the only subfield of gen-
eral adult thoracic surgery in which detailed and
complete data regarding return-to-work rates are
available, but from only one study. Multiple studies
have reported on the impact that a solid organ
transplant in general likely exerts on return to work,
but, to the authors’ knowledge, only one such study
[35] focused on the lung. In that study, Paris et al [35]
evaluated data from 99 lung transplant recipients
(43 single, 56 bilateral) from two centers by a
stepwise discriminant analysis to identify factors
influencing return to work posttransplant. Preopera-
tively, 50% (n = 50) of the patients were employed,
and 44% (n = 44) were medically disabled; postop-
eratively, after a median follow-up of 25 months,
22% (n = 22) were employed, 38% (n = 38) were
unemployed but medically fit to work, and 29%
(n = 29) were disabled. The adjusted (for subjects
physically able to work) return-to-work rate of 37%
(22 of 60 patients) was similar to other types of organ
transplant recipients.
In the Paris et al [35] study, lung transplant
recipients were less likely to be employed if they
were older or had a lower educational level. The rate
of spousal employment decreased regardless of the
recipient’s employment status (P < .01) and resulted
in a decreased mean family income. Significant
factors that fostered return to work included pretrans-
plant employment, self-reported ability to work, and
objectively measured improvement in functional sta-
tus. Certain social barriers to employment posttrans-
plant included changes in lifestyle priorities, the
restrictive cost or unavailability of health insurance,
and hiring discrimination. The type of surgical trans-
plant (single or bilateral) did not affect return to work
in these patients.
Unanswered questions and the need for future
studies
From the few pertinent articles reviewed here
(see Table 1), it is evident that the large gaps of
knowledge about return to work after thoracic surgery
may not be addressed in the near future. Multiple
reasons contribute to this situation. First, chest sur-
geons generally do not recognize that return to work
is a highly important outcome variable after thoracic
procedures. Consequently, they likely are not inter-
ested in characterizing return-to-work issues related
to thoracic surgery. Compounding this problem is the
fact that the term return to work remains poorly
defined and inconsistently used. None of the studies
cited except that by Paris et al [35] explicitly defined
return to work, and none of the studies reported
return-to-work results in a standard fashion.
The available data on return to work after thoracic
surgery are conflicting, with no clear patterns. Reas-
ons include limited sample sizes, heterogeneous
patient populations, and different experimental study
designs used by the investigators. Initial clinical
investigations aimed at addressing these deficiencies
are warranted, to establish a foundation for future,
larger trials (multi-institutional, prospective, random-
ized, and appropriately controlled). Likely what will
be revealed about return to work related to thoracic
surgery is that there are a host of complex, influen-
tial factors, some of which are controllable and
others uncontrollable.

C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416 415
Summary
In the literature on thoracic surgery, return to work
has received little attention in QOL investigations. At
present, it is difficult to appreciate clinically mean-
ingful trends in return to work after thoracic surgery,
even within a specialized area, such as lung cancer
resection. It is evident, however, that return to work is
not a simple variable, easily measured; rather, it is a
complex construct that is influenced by a multitude
of personal and societal factors. Focusing only on
disease-related or treatment-related symptoms renders
QOL studies limited in scope and perhaps in useful-
ness. Return to work is not a trivial component of
global postsurgical QOL; it should be recognized as a
major factor. Patients have indicated that maintaining
return-to-work ability is as highly valued as their
overall health. Surgical societies should design, vali-
date, and implement a simple data collection instru-
ment to characterize better return to work after
thoracic surgery.
Acknowledgment
The authors are grateful to Dr. Mary Knatterud for
expert editorial assistance.
References
[1] National Center for Health Statistics. Number of inpa-
tient surgical procedures. Advance data from vital
and health statistics; No. 329. Hyattsville MD: Na-
tional Center for Health Statistics; 2002.
[2] Montazeri A, Gillis CR, McEwen J. Quality of life in
patients with lung cancer: a review of literature from
1970 to 1995. Chest 1998;113:467–81.
[3] Cykert S, Kissling G, Hansen CJ. Patient preferences
regarding possible outcomes of lung resection: what
outcomes should preoperative evaluations target?
Chest 2000;117:1551–9.
[4] Jones KR, Burney RE, Peterson M, Christy B. Return
to work after inguinal hernia repair. Surgery 2001;129:
128–35.
[5] Mittag O, Kolenda KD, Nordman KJ, Bernien J, Mau-
rischat C. Return to work after myocardial infarction/
coronary artery bypass grafting: patients’ and physi-
cians’ initial viewpoints and outcome 12 months later.
Soc Sci Med 2001;52:1441–50.
[6] Matas AJ, Lawson W, McHugh L, et al. Employment
patterns after successful kidney transplantation. Trans-
plantation 1996;61:729–33.
[7] Walsh DC. Work, health, and productivity. ed 16. New
York: Oxford University Press; 1991.
[8] Walsh DC, Connor E, Tracey LV, Goldberg GA,
Egdahl RH. Posthospital convalescence and return
to work. Health Aff (Millwood) 1989;8:76–90.
[9] US Bureau of Labor Statistics. Employee benefits in
private industry, summary 2003. Washington, DC: US
Bureau of Labor Statistics, office of Compensation and
Working Conditions; 2003.
[10] Callesen T, Kehlet H. Postherniorrhaphy pain. Anes-
thesiology 1997;87:1219–30.
[11] Callesen T, Klarskov B, Bech K, Kehlet H. Short con-
valescence after inguinal herniorrhaphy with standard-
ised recommendations: duration and reasons for delayed
return to work. Eur J Surg 1999;165:236–41.
[12] Jemal A, Murray T, Samuels A, Ghafoor A, Ward E,
Thun MJ. Cancer statistics, 2003. CA Cancer J Clin
2003;53:5–26.
[13] Gotay CC, Muraoka MY. Quality of life in long-term
survivors of adult-onset cancers. J Natl Cancer Inst
1998;90:656–67.
[14] Dow KH, Ferrell BR, Haberman MR, Eaton L. The
meaning of quality of life in cancer survivorship.
Oncol Nurs Forum 1999;26:519–28.
[15] Langenhoff BS, Krabbe PF, Wobbes T, Ruers TJ.
Quality of life as an outcome measure in surgical on-
cology. Br J Surg 2001;88:643–52.
[16] Schag CA, Ganz PA, Wing DS, Sim MS, Lee JJ. Qual-
ity of life in adult survivors of lung, colon and prostate
cancer. Qual Life Res 1994;3:127–41.
[17] Handy Jr JR, Asaph JW, Skokan L, et al. What hap-
pens to patients undergoing lung cancer surgery?
Outcomes and quality of life before and after surgery.
Chest 2002;122:21–30.
[18] Dales RE, Belanger R, Shamji FM, et al. Quality-of-
life following thoracotomy for lung cancer. J Clin Epi-
demiol 1994;47:1443–9.
[19] Spitzer WO, Dobson AJ, Hall J, et al. Measuring
the quality of life of cancer patients: a concise
QL-index for use by physicians. J Chronic Dis 1981;
34:585–97.
[20] Zieren HU, Muller JM, Hamberger U, Pichlmaier H.
Quality of life after surgical therapy of bronchogenic
carcinoma. Eur J Cardiothorac Surg 1996;10:233–7.
[21] Demmy TL, Curtis JJ. Minimally invasive lobectomy
directed toward frail and high-risk patients: a case-
control study. Ann Thorac Surg 1999;68:194–200.
[22] Sugiura H, Morikawa T, Kaji M, Sasamura Y, Kondo
S, Katoh H. Long-term benefits for the quality of life
after video-assisted thoracoscopic lobectomy in pa-
tients with lung cancer. Surg Laparosc Endosc Per-
cutan Tech 1999;9:403–8.
[23] Lewis RJ, Caccavale RJ, Bocage JP, Widmann MD.
Video-assisted thoracic surgical non-rib spreading
simultaneously stapled lobectomy: a more patient-
friendly oncologic resection. Chest 1999;116:1119–24.
[24] Vigneswaran WT, Trastek VF, Pairolero PC, Des-
champs C, Daly RC, Allen MS. Extended esopha-
gectomy in the management of carcinoma of the
upper thoracic esophagus. J Thorac Cardiovasc Surg
1994;107:901–7.
[25] Vigneswaran WT, Trastek VF, Pairolero PC, Des-
C.D. Hoang et al / Thorac Surg Clin 14 (2004) 409–416416
champs C, Daly RC, Allen MS. Transhiatal esopha-
gectomy for carcinoma of the esophagus. Ann Thorac
Surg 1993;56:838–46.
[26] O’Rourke I, Tait N, Bull C, Gebski V, Holland M,
Johnson DC. Oesophageal cancer: outcome of modern
surgical management. Aust N Z J Surg 1995;65:11–6.
[27] Chen X, Yang CS. Esophageal adenocarcinoma: a
review and perspectives on the mechanism of carcino-
genesis and chemoprevention. Carcinogenesis 2001;
22:1119–29.
[28] McLarty AJ, Deschamps C, Trastek VF, Allen MS,
Pairolero PC, Harmsen WS. Esophageal resection for
cancer of the esophagus: long-term function and
quality of life. Ann Thorac Surg 1997;63:1568–72.
[29] Branicki FJ, Law SY, Fok M, Poon RT, Chu KM,
Wong J. Quality of life in patients with cancer of the
esophagus and gastric cardia: a case for palliative
resection. Arch Surg 1998;133:316–22.
[30] Blazeby JM, Conroy T, Hammerlid E, et al. Clinical
and psychometric validation of an EORTC question-
naire module, the EORTC QLQ-OES18, to assess
quality of life in patients with oesophageal cancer.
Eur J Cancer 2003;39:1384–94.
[31] Zieren HU, Jacobi CA, Zieren J, Muller JM. Quality
of life following resection of oesophageal carcinoma.
Br J Surg 1996;83:1772–5.
[32] Bousamra 2nd M, Haasler GB, Patterson GA, Roper
CL. A comparative study of thoracoscopic vs. open re-
moval of benign neurogenic mediastinal tumors. Chest
1996;109:1461–5.
[33] Bertrand PC, Regnard JF, Spaggiari L, et al. Immediate
and long-term results after surgical treatment of primary
spontaneous pneumothorax by VATS. Ann Thorac Surg
1996;61:1641–5.
[34] Stammberger U, Steinacher C, Hillinger S, Schmid
RA, Kinsbergen T, Weder W. Early and long-term
complaints following video-assisted thoracoscopic sur-
gery: evaluation in 173 patients. Eur J Cardiothorac
Surg 2000;18:7–11.
[35] Paris W, Diercks M, Bright J, et al. Return to work
after lung transplantation. J Heart Lung Transplant
1998;17:430–6.

Thorac Surg Clin 14 (2004) 417–428
Chronic respiratory failure after lung resection: the role of
pulmonary rehabilitation
Bartolome R. Celli, MDa,b,*
aDivision of Pulmonary and Critical Care Medicine, Caritas St. Elizabeth’s Medical Center, Seton 3 Pulmonary,
736 Cambridge Street, Brighton, MA 02135, USAbDepartment of Medicine, Tufts University, Boston, MA, USA
Patients with advanced chronic respiratory dis- Definition and goals
ease frequently have distressing symptoms, limita-
tions in exercise ability, and reductions in health and
functional status that persist despite optimal pharma-
cologic management. Pulmonary rehabilitation com-
plements standard medical therapy and can provide
additional, clinically meaningful benefit in these
areas. Pulmonary rehabilitation has become the stan-
dard of care for patients who are motivated to par-
ticipate in such programs. Patients improve their
exercise and functional capacity, decrease their dysp-
nea, improve their health status, and perhaps postpone
premature morbidity and mortality. Although pulmo-
nary rehabilitation was designed and is applied pri-
marily to symptomatic patients who are limited due
to chronic obstructive pulmonary disease (COPD), the
same fundamental principles seem to be applicable to
other disease states leading to disability. Pulmonary
rehabilitation has become an essential component in
the optimization of therapy in patients considered for
lung volume reduction surgery and an absolute requi-
site for patients undergoing lung transplant. Pulmo-
nary rehabilitation has a major role in the prevention
of complications.
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S1547-4127(04)00017-9
* Caritas St. Elizabeth’s Medical Center, Seton 3
Pulmonary, 736 Cambridge Street, Brighton, MA 02135.
E-mail address: [email protected]
Rehabilitation attempts to restore the individ-
ual to the fullest medical, mental, emotional, social,
and vocational potential to which he or she is capable.
Based on this basic concept, pulmonary rehabilita-
tion has been defined as ‘‘a multidisciplinary program
of care for patients with chronic respiratory impair-
ment that is individually tailored and designed to
optimize physical and social performance and auton-
omy.’’ [1] From this definition, it follows that pul-
monary rehabilitation has three major goals:
1. To control, alleviate, and, as much as possible,
reverse the symptoms and pathophysiologic
processes leading to respiratory impairment
2. To improve functional status and participation
in daily activities
3. To enhance health-related quality of life and
attempt to prolong the patient’s life
The concept of pulmonary rehabilitation has two
other important elements: its use of a wide array of
disciplines to achieve these goals and its recognition
that the patient has unique medical problems and
needs that require an individualized approach. In the
case of surgery, pulmonary rehabilitation includes the
psychological support required during the stressful
period before and after the operation and the appro-
priate timing to optimize results.
Pulmonary rehabilitation and its components have
been recognized by clinicians as an effective inter-
vention since at least the middle of the 20th century
s reserved.

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428418
[2–4]. Since the 1980s, pulmonary rehabilitation has
risen to prominence as a state-of-the-art, scientifically
proven intervention for patients with chronic lung
disease. Its current importance as a therapeutic option
is underscored by the following three events:
1. Its incorporation as the ‘‘best therapy’’ with
which lung volume reduction surgery was
compared in the National Emphysema Treat-
ment Trial [5]
2. A Cochrane report showing the effectiveness of
pulmonary rehabilitation in meta-analyses [6]
3. Its endorsement by the Global Initiative for
Obstructive Lung Disease and its prominent
position in their treatment algorithm for
COPD [7]
Over time, what previously was considered a form
of therapy reserved only for the most severe patients
now is recommended for patients with symptoms that
limit their performance, usually with moderate sever-
ity of disease. Several studies influential in the
development of pulmonary rehabilitation are listed
in Table 1 [8–10,12–14,]. These studies show the
science behind pulmonary rehabilitation and the ef-
fectiveness of this form of treatment.
Before 1991, much of the literature supporting
pulmonary rehabilitation consisted of descriptions
of comprehensive pulmonary rehabilitation and pre-
sentations of uncontrolled, preintervention and postin-
tervention studies showing its effectiveness primarily
in reducing hospital use. In 1991, Casaburi et al [8]
reported on a study of 19 COPD patients who were
randomized to either higher or lower levels of exer-
cise training on a cycle ergometer, 5 days per week
for 8 weeks. The patients who trained at lower levels
exercised longer so that the total amount of work was
roughly equivalent in both groups. Low levels of
Table 1
Selected studies in the development of pulmonary rehabilitation
Year First author Importance i
1991 Casaburi [8] Shows a dos
1994 Goldstein [9] First of man
of pulmonar
1994 Reardon [10] First study to
1995 Ries [12] A landmark
in multiple o
1996 Maltais [13] Shows the im
COPD and t
2000 Griffiths [14] This large ra
substantial re
Abbreviation: COPD, chronic obstructive pulmonary disease.
exercise resulted in lactic acid production, indicating
a low aerobic capacity at baseline. Both levels of
training led to significant physiologic benefits, mani-
fest by a reduced lactic acidosis and ventilatory re-
quirement at the same work rate. Patients who trained
at higher intensity had more physiologic benefit,
however, than patients who trained at lower intensity.
Subsequently, Goldstein et al [9] reported a prospec-
tive, randomized, controlled trial of pulmonary reha-
bilitation in which 89 patients were randomized to
either pulmonary rehabilitation, initially given in an
inpatient setting, or conventional medical care. The
group that participated in pulmonary rehabilitation
had significantly greater increases in the 6-minute
walk distance, submaximal cycle endurance time, and
health status compared with the group that received
standard medical care. This was the first of several
randomized, controlled trials of pulmonary rehabili-
tation that unequivocally established the effectiveness
of pulmonary rehabilitation as a treatment option for
chronic lung disease.
Reardon et al [10] reported on 20 COPD patients
who were randomized to either comprehensive out-
patient pulmonary rehabilitation or a waiting period,
during which they were given conventional medical
care. Rehabilitation led to significant improvement in
exertional dyspnea, measured during incremental
treadmill exercise testing, and overall, question-
naire-rated dyspnea with daily activities. This was
the first study to show the effectiveness of pulmonary
rehabilitation on dyspnea, the most important symp-
tom in advanced lung disease. Subsequent studies
by O’Donnell et al showed that the reduction in
post–exercise training dyspnea was associated with
decreased ventilatory demand, probably owing to
improved exercise efficiency [11].
Ries et al [12] reported on 119 patients with COPD
who were randomized to either comprehensive out-
n pulmonary rehabilitation
e-dependent physiologic benefit from exercise training
y randomized controlled trials establishing the effectiveness
y rehabilitation
prove that pulmonary rehabilitation relieves dyspnea
study showing the effectiveness of pulmonary rehabilitation
utcome areas
portance of biochemical abnormalities in the muscles of
heir improvement with pulmonary rehabilitation
ndomized trial showed, among other positive outcomes, a
duction in health care use after pulmonary rehabilitation

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428 419
patient pulmonary rehabilitation or education alone.
Compared with education alone, rehabilitation led to
significant improvement in dyspnea, maximal exer-
cise capacity, exercise endurance, and self-efficacy
for walking. The last-mentioned refers to the patient’s
confidence in successfully managing respiratory
symptoms associated with walking. Positive results
declined over time, approaching those of the control
group by 18 to 24 months. The decline in gains made
over time underscored the importance of strategies to
improve long-term adherence with rehabilitation.
This concept has led to the current concept that
patients considered for lung transplantation must
continue the gains obtained from rehabilitation
through maintenance of the exercise program [15].
Maltais et al [13] reported on 11 patients with
COPD who were evaluated before and after 36 ses-
sions of high-intensity endurance training. In addition
to the expected physiologic training effect (including
reduced exercise-induced lactic acidosis), exercise
training led to increased levels of oxidative enzymes
in muscle biopsy specimens. The improvement in
biochemical markers correlated with reduced lactic
acid production during exercise. Along with other
work, this study proves that exercise training improves
skeletal muscle oxidative capacity in COPD patients,
and this improvement has clinical importance.
Griffiths et al [14] presented data on 200 patients
with chronic lung disease who were randomized to
either 6 weeks of multidisciplinary pulmonary reha-
bilitation or standard medical management. In addi-
tion to showing substantial improvements in exercise
performance and health-related quality of life, the
pulmonary rehabilitation intervention led to fewer
days in the hospital and fewer primary care home
visits in the 1-year follow-up period. A subsequent
study from this group [16] provided evidence support-
ing the cost-effectiveness of pulmonary rehabilitation.
Rationale for pulmonary rehabilitation
Pulmonary rehabilitation has a minimal, if any,
effect on the abnormal lung function of individuals
with chronic lung disease. Despite this minimal ef-
fect, rehabilitation usually results in clinically signifi-
cant improvement in multiple outcome areas of
considerable importance to the patient, including re-
duction in exertional dyspnea and dyspnea associated
with daily activities, improvement in exercise perfor-
mance and in health status, and reduction in health
care use.
The apparent paradox whereby functional capac-
ity can improve without major change in pulmonary
function is explained by the fact that a considerable
portion of the dyspnea and functional status and
health status limitations from chronic lung disease
results from extrapulmonary effects of the disease,
which do respond to treatment. Some of the associ-
ated systemic manifestations include nutritional de-
pletion [17,18], decrease in lower extremity muscle
mass and peripheral muscle weakness and fatigability
[19,20], alterations in peripheral muscle fiber type,
and reduction in peripheral muscle oxidative en-
zymes. These manifestations, in addition to the clas-
sic changes of cardiovascular deconditioning, poor
pacing techniques, maladaptive coping skills, and
fear and anxiety for dyspnea-producing activities,
result in a vicious cycle of ever further decondition-
ing and debilitation. The accumulated evidence indi-
cates that pulmonary rehabilitation is highly effective
in improving and in some instances reverting many of
these systemic abnormalities.
Indications for pulmonary rehabilitation
Pulmonary rehabilitation is indicated for patients
with chronic respiratory disease who have persistent
symptoms or disability despite standard medical
therapy. Fig. 1 depicts the course of patients with
lung function limitation over time and the role of
pulmonary rehabilitation. Although all patients with
chronic respiratory disease are eligible for considera-
tion for pulmonary rehabilitation, to date, COPD is
the most common disease for which patients are re-
ferred, often from one or more of the following
symptoms or conditions:
1. Severe dyspnea or fatigue
2. Decreased exercise ability
3. Interference with performing activities of
daily living
4. Impaired health status
5. Decreased occupational performance
6. Nutritional depletion
7. Increased medical resource consumption
Persistent symptoms and limitation in these clini-
cal areas—not just the specific physiologic impair-
ment of the lungs (eg, a low forced expiratory volume
over time or hypoxemia)—dictate the need for this
intervention. Symptoms, exercise performance, func-
tional status, and health status individually correlate
relatively poorly with pulmonary function abnormali-
ties. There are no specific threshold pulmonary func-
tion inclusion criteria for pulmonary rehabilitation.
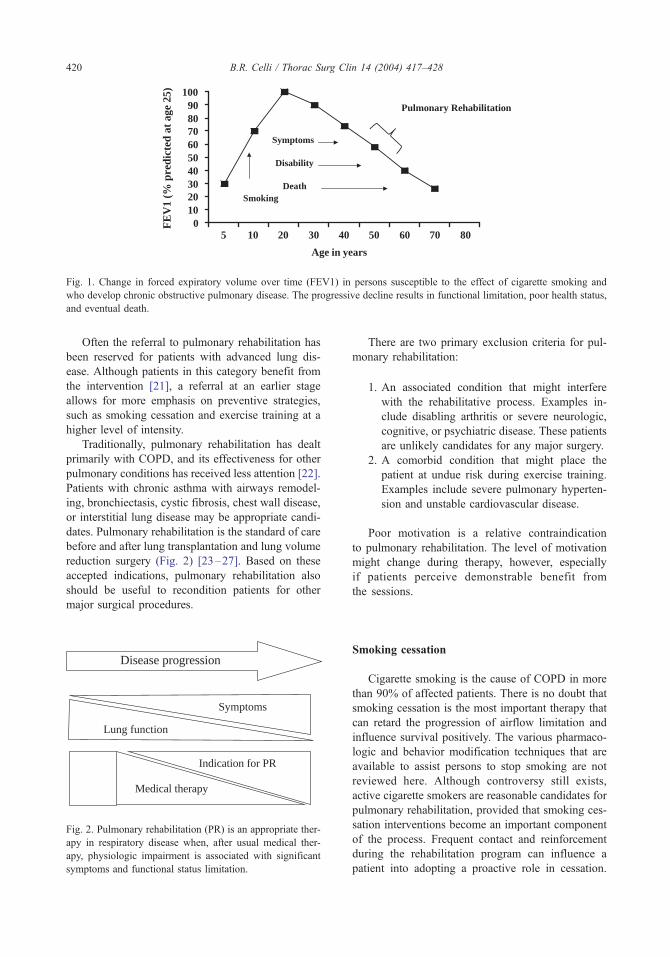
0102030405060708090
100
5 10 20 30 40 50 60 70 80
Age in years
FE
V1
(% p
redi
cted
at a
ge 2
5)
Symptoms
Disability
DeathSmoking
Pulmonary Rehabilitation
Fig. 1. Change in forced expiratory volume over time (FEV1) in persons susceptible to the effect of cigarette smoking and
who develop chronic obstructive pulmonary disease. The progressive decline results in functional limitation, poor health status,
and eventual death.
B.R. Celli / Thorac Surg Clin 14 (2004) 417–428420
Often the referral to pulmonary rehabilitation has
been reserved for patients with advanced lung dis-
ease. Although patients in this category benefit from
the intervention [21], a referral at an earlier stage
allows for more emphasis on preventive strategies,
such as smoking cessation and exercise training at a
higher level of intensity.
Traditionally, pulmonary rehabilitation has dealt
primarily with COPD, and its effectiveness for other
pulmonary conditions has received less attention [22].
Patients with chronic asthma with airways remodel-
ing, bronchiectasis, cystic fibrosis, chest wall disease,
or interstitial lung disease may be appropriate candi-
dates. Pulmonary rehabilitation is the standard of care
before and after lung transplantation and lung volume
reduction surgery (Fig. 2) [23–27]. Based on these
accepted indications, pulmonary rehabilitation also
should be useful to recondition patients for other
major surgical procedures.
Disease progression
Lung function
Symptoms
Indication for PR
Medical therapy
Fig. 2. Pulmonary rehabilitation (PR) is an appropriate ther-
apy in respiratory disease when, after usual medical ther-
apy, physiologic impairment is associated with significant
symptoms and functional status limitation.
There are two primary exclusion criteria for pul-
monary rehabilitation:
1. An associated condition that might interfere
with the rehabilitative process. Examples in-
clude disabling arthritis or severe neurologic,
cognitive, or psychiatric disease. These patients
are unlikely candidates for any major surgery.
2. A comorbid condition that might place the
patient at undue risk during exercise training.
Examples include severe pulmonary hyperten-
sion and unstable cardiovascular disease.
Poor motivation is a relative contraindication
to pulmonary rehabilitation. The level of motivation
might change during therapy, however, especially
if patients perceive demonstrable benefit from
the sessions.
Smoking cessation
Cigarette smoking is the cause of COPD in more
than 90% of affected patients. There is no doubt that
smoking cessation is the most important therapy that
can retard the progression of airflow limitation and
influence survival positively. The various pharmaco-
logic and behavior modification techniques that are
available to assist persons to stop smoking are not
reviewed here. Although controversy still exists,
active cigarette smokers are reasonable candidates for
pulmonary rehabilitation, provided that smoking ces-
sation interventions become an important component
of the process. Frequent contact and reinforcement
during the rehabilitation program can influence a
patient into adopting a proactive role in cessation.

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428 421
The inclusion of a smoking patient in a rehabilitation
program may help achieve cessation and help the
patient qualify for surgery.
Components of a comprehensive pulmonary
rehabilitation program
Exercise training
Comprehensive exercise training, including upper
and lower extremity endurance training and strength
training, is an essential component of comprehensive
pulmonary rehabilitation. Inclusion of exercise train-
ing follows the current knowledge that the peripheral
muscles in chronic lung disease not only are wasted,
but also appear to have alterations in fiber-type
distribution and decreased metabolic capacity. Exer-
cise training improves endurance, increases level of
functioning, aids in performance of activities of daily
living, helps reduce systemic blood pressure, im-
proves lipid profiles, tends to counteract depression,
reduces anxiety associated with dyspnea-producing
activities, and facilitates sleep.
Exercise training for patients with chronic lung
disease—similar to healthy individuals—is based on
general principles of intensity (higher levels of train-
ing produce more results), specificity (only muscles
that are trained show an effect), and reversibility
(cessation of regular exercise training leads to loss
of training effect) [28]. Many patients also are limited
by peripheral muscle and cardiovascular decondi-
tioning, with an early onset of anaerobic metabolism
and lactic acidosis during exercise. This decondition-
ing is responsive to exercise training. Additionally,
many respiratory disease patients often are capable of
exercising for prolonged periods at levels close to
their peak exercise capacity. Higher levels of exercise
training such as this result in greater improvement in
exercise performance [29]. The demonstrated reduc-
tion in ventilation and lactate levels at identical
submaximal work after high-intensity exercise train-
ing strongly suggests that a training effect is attain-
able in many patients with advanced lung disease. A
dose-related increase in oxidative enzymes in the
peripheral muscles accompanies these physiologic
adaptations to training [19]. A reduction in lactic
acid production has been shown to be associated with
improvement in oxidative capacity of the peripheral
muscles [30].
Most pulmonary rehabilitation programs empha-
size endurance training of the lower extremities, often
advocating sustained exercise for about 20 to 30 min-
utes, two to five times a week. This training may
include pedaling on a stationary cycle ergometer,
walking on a motorized treadmill, climbing stairs,
or walking on a flat surface such as a corridor or
auditorium. Training usually is performed at levels
equal to or greater than 50% or 60% of the maximal
work rate. For patients unable to maintain this inten-
sity for the recommended duration, interval training,
consisting of 2 to 3 minutes of high-intensity (60% to
80% maximal exercise capacity) training alternating
with equal periods of rest, has similar results with less
dyspnea [31].
The total duration of exercise training depends on
the individual pulmonary rehabilitation program but
should reflect the patient’s underlying respiratory
disease, his or her level of physical and cardiovascu-
lar conditioning, and the progress made during the
exercise training sessions. COPD guidelines (Global
Initiative for Obstructive Lung Disease) recommend
at least 8 weeks of exercise training as part of a
pulmonary rehabilitation program [7]. When patients
are considered for surgical procedures that may
require less waiting time, however, the programs
can be compressed to 3 weeks with daily sessions.
This approach should provide enough training to
obtain benefits and avoid the waiting periods that
often generate anxiety in the patient.
Although the strength of the upper extremity mus-
cles is relatively preserved compared with that of the
lower extremities in COPD [20,32], use of these
muscles is associated with considerable dyspnea.
Endurance training of the upper extremities is impor-
tant [33] because the arms are used in many activities
of daily living, and the arm muscles are accessory
muscles of respiration. Training can be accomplished
using supported arm exercises, such as arm ergometry,
or unsupported arm exercises, such as lifting free
weights or dowels or stretching elastic bands.
Because peripheral muscle weakness or depletion
contributes to exercise limitation in patients with lung
disease [34], strength training is a rational component
of exercise training during pulmonary rehabilitation.
Weight-lifting training alone involving the upper and
lower extremities increases muscle strength and en-
durance performance on a cycle ergometer [35]. The
current practice of pulmonary rehabilitation usually
adds strength training to standard aerobic training.
This combination increases muscle strength and
mass, but its additive effect on health status has not
been proved [36].
Inspiratory muscle training increases strength and
endurance of the inspiratory muscles [37,38]. Most
studies have not established a link, however, between
improvements in respiratory muscle strength or en-
B.R. Celli / Thorac Surg Clin 14 (2004) 417–428422
durance and dyspnea, exercise performance, or health
status [39]. Newer approaches emphasizing endur-
ance training of the respiratory muscles at more
precise percentages of maximal capacity are promis-
ing, although not yet proved.
Education
Education is an integral component of virtually all
comprehensive pulmonary rehabilitation programs.
Besides providing the patient and the family impor-
tant information on the disease process, its comor-
bidity, and its treatment, education encourages active
participation in health care, promoting adherence and
self-management skills [40]. Additionally, education
helps the patient and family find ways to cope better
with the illness. Important components of the educa-
tional process are encouraging a healthy lifestyle,
incorporating adaptive techniques learned in rehabili-
tation into the home setting, and promoting long-term
adherence with the rehabilitative instructions.
Education usually is provided in small group
settings and a one-to-one format. Educational needs
are determined as part of the initial evaluation, then
are reassessed during the course of the program.
Box 1. Educational elements of acomprehensive pulmonary rehabilitationprogram
Normal pulmonary anatomy andphysiology
Pathophysiology of lung diseaseDescription and interpretation of
medical testsBreathing retrainingBronchial hygieneMedicationsExercise principlesActivities of daily living and energy
conservationRespiratory modalitiesSelf-assessment and symptom
managementNutritionPsychosocial issuesEthical issuesAdvance directives
Advance directive discussions are an important com-
ponent of pulmonary rehabilitation [41]. Generally,
many standard topics are addressed in the educational
sessions (Box 1).
Education is a component of virtually all pul-
monary rehabilitation programs. Consequently, few
studies evaluate the effectiveness of this single com-
ponent as isolated therapy. A study evaluating self-
management strategies (which are prominent in
comprehensive pulmonary rehabilitation) applied to
the home setting showed this form of therapy to be
effective, however, in improving health status and
reducing use of medical resources. Although no
studies have evaluated the role of education in the
rehabilitation of patients considered for surgery, it is
believed that instruction of patients in the prevention
of pulmonary complications is crucial to better out-
comes [42–45].
Psychosocial training and support
Psychosocial problems (eg, anxiety, depression,
deficiencies with coping, and decreased self-efficacy)
contribute to the burden of advanced respiratory
disease [46]. Psychosocial and behavioral interven-
tions vary widely among comprehensive pulmonary
rehabilitation programs but often involve educational
sessions or support groups, focusing on areas such as
coping strategies or stress management techniques.
Techniques of progressive muscle relaxation, stress
reduction, and panic control may reduce not only
anxiety, but also dyspnea [47]. Educational efforts
also may improve coping skills. Participation by
family members or friends in pulmonary rehabilitation
support groups is encouraged. Informal discussions
of symptoms frequently present in chronic lung dis-
ease and common concerns may provide emotional
support to patients and their families. Individuals
with substantial psychiatric disease should be re-
ferred for appropriate professional care outside of
the program.
Few studies have evaluated the effect of pul-
monary rehabilitation on psychological outcomes. A
randomized, controlled trial of comprehensive pul-
monary rehabilitation failed to show a significant
effect on depression. In one noncontrolled study of
pulmonary rehabilitation, depression and anxiety lev-
els decreased, however, after 1 month of pulmonary
rehabilitation. This program included psychological
counseling and stress management sessions twice
weekly in addition to standard exercise training and
educational topics [48].

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428 423
Nutritional support
Nutritional depletion, including decreased weight
and abnormalities in body composition, such as de-
creased lean body mass, is present in 20% to 35% of
patients with stable COPD [49,50]. This depletion
undoubtedly contributes to the morbidity of COPD.
Nutritional depletion is associated with reductions in
respiratory muscle strength [51], handgrip strength,
exercise tolerance [52], and health status [53]. Nutri-
tional depletion and alteration in body composition
also are significant predictors of mortality of COPD,
independent of forced expiratory volume over time
[54,55]. For all the aforementioned reasons, nutri-
tional optimization is a recommended component of
comprehensive pulmonary rehabilitation.
The benefit from simple nutritional supplementa-
tion to underweight patients with chronic lung disease
has not been substantial, with one meta-analysis of
nutritional intervention for COPD reporting only a
1.65-kg increase in weight after intervention [56].
Further studies are needed to determine the optimal
approach to treatment of nutritional depletion in
chronic lung disease.
Physical modalities of ventilatory therapy
Physical modalities of ventilatory therapy have
been part of the armamentarium of pulmonary reha-
bilitation over the years, but conclusive evidence
supporting their effectiveness in pulmonary rehabili-
tation is lacking. These modalities comprise two
categories: controlled breathing techniques (diaphrag-
matic breathing exercise, pursed-lip breathing, and
bending forward) and chest physical therapy (postural
drainage and chest percussion and vibration position).
Controlled breathing techniques are aimed at decreas-
ing dyspnea, and chest physical therapy is aimed at
enhancing drainage of secretions. Reputed benefits of
these modalities include less dyspnea, a decrement in
anxiety and panic attacks, and improvement in sen-
sation of well-being. These modalities require careful
instruction by persons familiar with the techniques. It
often is necessary to involve relatives because many
of these modalities require the help of another person
(eg, chest percussion).
Breathing training is aimed at controlling the
respiratory rate and breathing pattern, possibly result-
ing in decreased air trapping. It also may decrease the
work of breathing by improving the position and
function of the respiratory muscles [57]. The easiest
of these maneuvers is pursed-lip breathing: Patients
inhale through the nose and exhale over 4 to 6 sec-
onds through lips pursed in a whistling or kissing
position. The exact mechanism by which pursed-lip
breathing decreases dyspnea is unknown. It does not
seem to change functional residual capacity or oxygen
uptake, but it does decrease respiratory frequency,
increase tidal volume, and improve blood gases.
Bending forward posture has been shown to result
in a decrease in dyspnea in some patients with severe
COPD at rest and during exercise. The best explana-
tion for this improvement is through improved dia-
phragmatic function, as the increased gastric pressure
in these positions places the diaphragm in a better
contracting position.
Diaphragmatic breathing is a technique aimed at
changing the breathing pattern from one in which the
ribcage muscles are the predominant pressure genera-
tors to a more normal one in which the pressures are
generated with the diaphragm. It usually is practiced
for at least 20 minutes two to three times daily. The
patient should start the training in the supine position
and when familiar with it perform breathing in the
upright posture. The patient is instructed to breathe in
trying to displace outwardly the hand that is placed
on the abdomen. The patient exhales with pursed lips
while encouraged to use the abdominal muscles in an
attempt to return the diaphragm to a more lengthened
resting position. Although most patients report im-
provement in dyspnea, this technique results in mini-
mal, if any, changes in oxygen uptake and resting
lung volume. Similar to pursed lip breathing, there is
usually a decrease in respiratory rate, minute venti-
lation, and increased tidal volume.
Chest physical therapy is used to attempt to
remove airways secretions. The different techniques
include postural drainage, chest percussion, vibration,
and directed cough. Postural drainage uses gravity to
help drain the individual lung segments. Chest per-
cussion should be performed with care in patients
with osteoporosis or bone problems. Cough also is an
effective technique for removing excess mucus from
the larger airways. Patients with COPD have im-
paired cough mechanisms (maximal expiratory flow
is reduced, ciliary beat is impaired), and the mucus
itself has altered viscoelastic properties.
Because cough spasms may lead to dyspnea,
fatigue, and worsened obstruction, directed cough
might be helpful by modulating the beneficial effect
and preventing the untoward effects. With controlled
coughs, patients are instructed to inhale deeply, hold
their breath for a few seconds, then cough two or three
times with the mouth open. Patients also are instructed
to compress the upper abdomen to assist in the cough.
Pulmonary functions do not improve with any of
these techniques. A combination of postural drain-

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428424
age, percussion, vibration, and cough increases the
clearance of inhaled radiotracers and increases spu-
tum volume and weight. The most important crite-
rion for chest physical therapy is the presence of
sputum production.
The use of one or more of these modalities during
the perioperative period is the routine in high-risk
surgery, including lung-volume reduction surgery
and transplantation. An adequate preparation of
the patient makes him or her more capable of man-
aging the postoperative period with more knowledge
and confidence.
Vaccination
The causes of exacerbations of COPD are poorly
understood and probably are multifactorial. Influenza
virus and Streptococcus pneumoniae may play a role,
and when either of these infections occurs, patients
with chronic lung disease have an increased incidence
of serious complications, including death [58]. One of
the national health objectives in the United States for
2000 was to increase influenza and pneumococcal
vaccination levels to greater than 60% among persons
at high risk for complications and all persons 65 years
old or older; this includes all patients with COPD and
other forms of chronic lung disease, regardless of age.
Because the influenza vaccine is type specific and
serotypes are constantly changing, vaccination must
be repeated every year, preferably at the beginning of
the season in the fall. The pneumococcal vaccine is
polyvalent, and its benefits should last a lifetime [59].
One of the responsibilities of a rehabilitation program
is to educate enrollees about the importance of
vaccination against influenza and pneumococcal
infections and to ensure that it is performed and, for
influenza, repeated annually. Although not specific
for surgery, it is recommended that attention be paid
to these details because a healthier individual is more
likely to have a better outcome.
Long-term adherence to pulmonary rehabilitation
Although the short-term effects of pulmonary
rehabilitation in multiple outcome areas are firmly
established, the long-term effectiveness of this ther-
apy often is disappointing. In controlled trials of
pulmonary rehabilitation, gains in exercise perfor-
mance and health status obtained after 6 to 8 weeks
of therapy essentially disappear by 18 to 24 months
[60,61]. It seems illogical, however, to expect that a
therapy that is applied only for 6 to 8 weeks could
modify the natural course of the disease substanti-
ally. The decline in function probably is greater than
what would be expected from progression of the
underlying disease process. In all likelihood, two
factors are mainly responsible for this drop-off in
effectiveness: (1) exacerbations of underlying lung
disease, leading to prolonged symptoms and a reas-
sumption of a more sedentary lifestyle, and (2) a
gradual decline in adherence to the postrehabilitation
exercise prescription.
The pulmonary rehabilitation program designed
for patients undergoing lung reduction surgery or
lung transplant must include strategies to promote
long-term adherence. One approach would be to
incorporate more actively the principles of pulmonary
rehabilitation (including exercise training) into the
home setting. This approach is supported by studies
of home-based programs, which suggest that gains
made in this setting may be longer lasting [62] than
the gains of hospital-based programs. Additionally,
giving a ‘‘booster shot’’ of pulmonary rehabilitation
after an exacerbation, emphasizing short periods of
supervised exercise training to return the patient to
baseline performance, would seem to be a reasonable
intervention in selected cases.
Program organization
The pulmonary rehabilitation program needs a
coordinator to organize the different components into
a functioning unit. The coordinator develops the
integrated program and monitors its progress and
function. The program should have resources avail-
able to teach and supervise respiratory therapy tech-
niques (eg, oxygen, use of inhalers, nebulizers),
physical therapy (breathing techniques, chest physical
therapy, postural drainage), exercise conditioning
(upper and lower extremity), and activities of daily
living (work simplification, energy conservation).
Also desirable are services to evaluate and advise
on nutritional needs, psychological evaluation, and
support of vocational counseling [63].
The decision whether to have an inpatient or an
outpatient program depends on the methods of reim-
bursement, patient population, available personnel,
and institutional policy. The ideal system is one that
provides an in-hospital component for patients who
may benefit from the program while recovering from
acute exacerbations and an outpatient component
(including home therapy) that could complete the
program started in the hospital. This system ensures
good continuity of care.

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428 425
Outcomes and pulmonary rehabilitation
Outcome analysis can be defined as the assess-
ment of the ‘‘consequences’’ of an intervention.
Pulmonary rehabilitation does not affect the degree
of respiratory impairment as measured by tests of
physiologic pulmonary function. Exercise training
in rehabilitation increases the content of oxidative
enzymes in the trained muscles, however, and this
is accompanied by a beneficial delay in the gen-
eration of lactate (a marker of muscle performance).
This delay results in improved exercise performance
and dyspnea and may be responsible, at least in
part, for the improved functional capacity of these
patients. Although pulmonary rehabilitation does
not change the impairment (lung function), it has a
profound impact on the disability and handicap of
the patient.
Outcome assessment for pulmonary rehabilitation
encompasses three different areas: (1) a generalized
audit of the effectiveness of the global pulmonary
rehabilitation program and its components; (2) evalua-
tion of individual patient response to the interven-
tion; and (3) assessment of the effect of pulmonary
rehabilitation on society, especially with respect to
its effect on health care use and its cost-effective-
ness. Commonly used outcome measures are listed
in Table 2.
Evaluating the effectiveness of the pulmonary
rehabilitation program is important in continuous
quality assessment. Testing can be made in several
areas, especially in the measurement of dyspnea,
exercise performance, and health status. Dyspnea
evaluation falls into two categories: measurement of
exertional dyspnea during standardized exercise test-
Table 2
Examples of outcome assessment for pulmonary rehabilitation
Exertional dyspnea Borg scale or visual anal
Dyspnea with daily activities Modified Medical Resea
Dyspnea Indexes (BDI/T
Functional exercise capacity 6-min walk test, increme
Laboratory measures of exercise
performance
Incremental cardiopulmo
work rate
Health status Chronic Respiratory Dise
Questionnaire (SGRQ), M
Functional performance Pulmonary Functional St
Dyspnea Questionnaire (
Nutritional status/body composition Body mass index, body c
x-ray absorption
Psychological variables Measurement of anxiety
(HAD) questionnaire
ing, and questionnaire-measurement of breathless-
ness. Exertional dyspnea usually is rated using a
Borg scale or visual analogue scale [63]. Question-
naire-measurement of dyspnea usually assesses dysp-
nea associated with daily activities or the effect of
exertional dyspnea in limiting activities [64].
Exercise performance can be measured in the
laboratory, using protocols involving incremental
treadmill or stationary bicycle exercise. Field tests
of exercise performance, such as the 6-minute walk
test or the shuttle walk test, are performed more com-
monly. The 6-minute walk test is easy to perform,
relates well to functional status, and is responsive to
the pulmonary rehabilitation intervention. For the
shuttle walk test [65], the patient is instructed to
walk around a 10-m course at gradually increasing
speeds. Speed is determined by an auditory beeping
signal that sets the pace. The test is terminated when
the patient cannot complete the course in time,
usually because of breathlessness. Total distance
traveled is the variable assessed. Fig. 3 shows the
increase in the 6-minute walk distance of 26 patients
who underwent lung reduction surgery at St. Eliz-
abeth’s Medical Center.
Health status often is assessed using respiratory-
specific questionnaires, such as the Chronic Respira-
tory Disease Questionnaire (CRQ) or the St. George’s
Respiratory Questionnaire (SGRQ) [66,67]. Some
pulmonary rehabilitation programs also may use a
generic instrument, such as the Medical Outcomes
Study Short Form 36 (SF-36) [25], to complement
information from the respiratory-specific question-
naires. Using these tools, it has been shown that lung
surgery does result in significant improvement in
these outcomes [5,25,68–70]. Assessment in the
ogue scale during exercise testing
rch Council (MRC) questionnaire, Baseline and Transitional
DI), San Diego Shortness of Breath Questionnaire
ntal and endurance shuttle walk tests
nary exercise testing, endurance testing at constant
ase Questionnaire (CRQ), St. George’s Respiratory
edical Outcomes Study Short Form 36 (SF-36)
atus Scale (PFSS), Pulmonary Function Status and
PFSDQ)
omposition using bioelectrical impedance or dual-energy
and depression using the Hospital Anxiety and Depression

100
150
200
250
300
350
Baseline 2 weeks 4 weeks 6 weeks 8 weeks
6 M
WD
(met
ers)
Fig. 3. The 6-minute walk distance (6MWD) of patients
completing a comprehensive pulmonary rehabilitation
program at St. Elizabeth’s Medical Center increased 22%
after 8 weeks of training.
B.R. Celli / Thorac Surg Clin 14 (2004) 417–428426
areas of nutrition and body composition, educational
goal achievement, and psychosocial variables (eg,
anxiety, depression, or coping skills) also is possible.
Despite the short time that has elapsed since the
introduction of outcome studies, there is evidence
that pulmonary rehabilitation results in significant
improvement in many outcomes, all of which are im-
portant to patients. These outcomes include reduced
exertional dyspnea, decreased dyspnea with daily
activities, increased exercise performance of the
lower and upper extremities, increased peripheral
muscle strength, increased strength and endurance of
respiratory muscles, increased self-efficacy for walk-
ing, improved health status, and reduced health care
use and increased cost-effectiveness.
Summary
Pulmonary rehabilitation gradually has become
the gold standard treatment for patients with severe
lung disease, especially COPD. By definition, reha-
bilitation services are provided to patients with symp-
toms, most of whom have moderate-to-advanced lung
disease. Because new therapeutic strategies, such as
lung volume-reduction surgery and lung transplanta-
tion, require well-conditioned patients, pulmonary
rehabilitation is becoming a crucial component of
the overall treating strategy of many patients who
heretofore were deemed untreatable. The positive
results in several randomized trials have documented
the effectiveness of pulmonary rehabilitation. Cur-
rently, pulmonary rehabilitation should be made
available to all patients with symptomatic respiratory
disease and be an integral part of any program
considering high-risk surgery.
References
[1] Pulmonary rehabilitation. Official statement of the
American Thoracic Society. Am J Respir Crit Care
Med 1999;159:1666–82.
[2] Barach AL. Breathing exercises in pulmonary emphy-
sema and allied chronic respiratory disease. Arch Phys
Med Rehabil 1995;36:379–90.
[3] Haas ACH. Rehabilitation in chronic obstructive lung
disease: a 5-year study of 252 male patients. Med
Clin North Am 1969;53:593–606.
[4] Petty TL, Nett LM, Finigan MM, Brink GA, Corsello
PR. A comprehensive care program for chronic airway
obstruction: methods and preliminary evaluations of
symptomatic and functional improvement. Ann Intern
Med 1969;70:1109–20.
[5] Fishman A, Martinez F, Naunheim K, et al. A random-
ized trial comparing lung-volume-reduction surgery
with medical therapy for severe emphysema. N Engl
J Med 2003;348:2059–73.
[6] Lacasse Y, Brosseau L, Milne S, et al. Pulmonary re-
habilitation for chronic obstructive pulmonary disease
(Cochrane Review). London, UK: John Wiley & Sons,
The Cochrane Library; 2003.
[7] Pauwels RA, Buist AS, Calverley PM, et al. Global
strategy for the diagnosis, management, and prevention
of chronic obstructive pulmonary disease. NHLBI/
WHO Global Initiative for Chronic Obstructive Lung
Disease (GOLD) Workshop summary. Am J Respir
Crit Care Med 2001;163:1256–76.
[8] Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF,
Wasserman K. Reductions in exercise lactic acidosis
and ventilation as a result of exercise training in pa-
tients with obstructive lung disease. Am Rev Respir
Dis 1991;143:9–18.
[9] Goldstein RS, Gort EH, Stubbing D, et al. Randomised
controlled trial of respiratory rehabilitation. Lancet
1994;344:1394–7.
[10] Reardon J, Awad E, Normandin E, et al. The effect of
comprehensive outpatient pulmonary rehabilitation
on dyspnea. Chest 1994;105:1046–52.
[11] O’Donnell DE, Bain DJ, Webb KA. Factors contribut-
ing to relief of exertional breathlessness during hyper-
oxia in chronic airflow limitation. Am J Respir Crit
Care Med 1997;155:530–5.
[12] Ries AL, Kaplan RM, Limberg TM, et al. Effects
of pulmonary rehabilitation on physiologic and psy-
chosocial outcomes in patients with chronic obstruc-
tive pulmonary disease. Ann Intern Med 1995;122:
823–32.
[13] Maltais F, Simard AA, Simard C, Jobin J, Desgagnes P,
Leblanc P. Oxidative capacity of the skeletal muscle
and lactic acid kinetics during exercise in normal sub-
jects and in patients with COPD. Am J Respir Crit
Care Med 1996;153:288–93.
[14] Griffiths TL, Burr ML, Campbell IA, et al. Results at
1 year of outpatient multidisciplinary pulmonary reha-
bilitation: a randomised controlled trial. Lancet 2000;
355:362–8.

B.R. Celli / Thorac Surg Clin 14 (2004) 417–428 427
[15] Palmer SM, Tapson VF. Pulmonary rehabilitation in
the surgical patient: lung transplantation and lung vol-
ume reduction surgery. Respir Care Clin N Am 1998;4:
71–83.
[16] Griffiths TL, Phillips CJ, Davies S, et al. Cost effec-
tiveness of an outpatient multidisciplinary pulmonary
rehabilitation programme. Thorax 2001;56:779–84.
[17] Schols AM, Slangen J, Volovics L, et al. Weight loss
is a reversible factor in the prognosis of chronic ob-
structive pulmonary disease. Am J Respir Crit Care
Med 1998;157:1791–7.
[18] Wouters EF, Schols AM. Prevalence and pathophysi-
ology of nutritional depletion in chronic obstructive
pulmonary disease. Respir Med 1993;87(Suppl B):
45–7.
[19] Maltais F, Leblanc P, Simard C, et al. Skeletal mus-
cle adaptation to endurance training in patients with
chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 1996;154:442–7.
[20] Whittom F, Jobin J, Simard PM, et al. Histochemical
and morphological characteristics of the vastus lateralis
muscle in COPD patients: comparison with normal
subjects and effects of exercise training. Med Sci
Sports Exerc 1998;30:1467–74.
[21] ZuWallack RL, Patel K, Reardon JZ, et al. Predictors
of improvement in the 12-minute walking distance fol-
lowing a six-week outpatient pulmonary rehabilitation
program. Chest 1991;99:805–8.
[22] Novitch RS, Thomas HM. Rehabilitation of patients
with chronic ventilatory limitation from nonobstructive
lung diseases. In: Casaburi R, Petty T, editors. Princi-
ples and practice of pulmonary rehabilitation. Philadel-
phia: Saunders; 1993. p. 416–23.
[23] Celli BR. Pulmonary rehabilitation for COPD: A prac-
tical approach for improving ventilatory conditioning.
Postgrad Med 1998;103:159–68.
[24] Cordova FC, Criner GJ. Surgery for chronic obstructive
pulmonary disease: the place for lung volume reduc-
tion and transplantation. Curr Opin Pulm Med 2001;7:
93–104.
[25] de Torres JP, Pinto-Plata V, Ingenito E, et al. Power
of outcome measurements to detect clinically signifi-
cant changes in pulmonary rehabilitation of patients
with COPD. Chest 2002;121:1092–8.
[26] Geiger-Bronsky M. Pulmonary rehabilitation and self-
care after ambulatory surgery. J Perianesth Nurs 1998;
13:382–93.
[27] Yusen RD, Lefrak SS, Gierada DS, et al. A prospec-
tive evaluation of lung volume reduction surgery in
200 consecutive patients. Chest 2003;123:1026–37.
[28] American College of Sports Medicine. Position stand:
the recommended quantity and quality of exercise for
developing and maintaining cardiorespiratory and mus-
cular fitness in healthy adults. Med Sci Sports Exerc
1990;22:265–74.
[29] Normandin EA, McCusker C, Connors M, et al. An
evaluation of two approaches to exercise conditioning
in pulmonary rehabilitation. Chest 2002;121:1085–91.
[30] Sala E, Roca J, Marrades RM, et al. Effects of endur-
ance training on skeletal muscle bioenergetics in chro-
nic obstructive pulmonary disease. Am J Respir Crit
Care Med 1999;159:1726–34.
[31] Vogiatzis I, Nanas S, Roussos C. Interval training as an
alternative modality to continuous exercise in patients
with COPD. Eur Respir J 2002;20:12–9.
[32] Bernard SP, Leblanc F, Whittom G, et al. Peripheral
muscle weakness in patients with chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 1998;
158:629–34.
[33] Celli BR. Physical reconditioning of patients with res-
piratory disease: Legs, arms, and breathing retraining.
Respir Care 1994;39:482–501.
[34] Hamilton N, Killian KJ, Summers E, Jones NL. Mus-
cle strength, symptom intensity, and exercise capacity
in patients with cardiorespiratory disorders. Am J
Respir Crit Care Med 1995;152:2021–31.
[35] Simpson K, Simpson K, Killian K, et al. Randomised
controlled trial of weightlifting exercise inpatients
with chronic airflow limitation. Thorax 1992;47:70–5.
[36] Bernard S, Withom F, LeBlanc P, et al. Aerobic and
strength training in patients with chronic obstructive
pulmonary disease. Am J Respir Crit Care Med 1999;
159:896–901.
[37] Leith D, Bradley M. Ventilatory muscle strength and
endurance training. J Appl Physiol 1976;41:508–16.
[38] Weiner P, Magadle R, Beckerman M, et al. Compari-
son of specific expiratory, inspiratory, and combined
muscle training programs in COPD. Chest 2003;124:
1357–64.
[39] Lotters F, van Tol B, Kwakkel G, et al. Effects of
controlled inspiratory muscle training in patients
with COPD: a meta-analysis. Eur Respir J 2002;20:
570–6.
[40] Hopp JW, Neisch CM. Patient and family education.
In: Hodgkin JE, Connors GL, Bell CW, editors. Pul-
monary rehabilitation guidelines to success. Philadel-
phia: Lippincott; 1993. p. 72–85.
[41] Heffner JE, Fahy B, Hilling L, Barbieri C. Outcomes
of advance directive education of pulmonary rehabili-
tation patients. Am J Respir Critic Care Med 1997;155:
1055–9.
[42] Bezanson J. Respiratory care of older adults after
cardiac surgery. J Cardiovasc Nurs 1997;12:71–83.
[43] Celli BR, Rodriguez KS, Snider GL. A controlled trial
of intermittent positive pressure breathing, incentive
spirometry, and deep breathing exercises in preventing
pulmonary complications after abdominal surgery. Am
Rev Respir Dis 1984;130:12–5.
[44] Chumillas S, Ponce JL, Delgado F, et al. Prevention
of postoperative pulmonary complications through
respiratory rehabilitation: a controlled clinical study.
Arch Phys Med Rehabil 1998;79:5–9.
[45] Szekely LA, Oelberg DA, Wright C, et al. Preoperative
predictors of operative morbidity and mortality in
COPD patients undergoing bilateral lung volume re-
duction surgery. Chest 1997;111:550–8.
[46] Kaplan RM, Ries AL, Prewitt LM, Eakin E. Self-effi-
cacy expectations predict survival for patients with
B.R. Celli / Thorac Surg Clin 14 (2004) 417–428428
chronic obstructive pulmonary disease. Health Psychol
1994;13:366–8.
[47] Renfroe KL. Effect of progressive relaxation on dysp-
nea and state anxiety in patients with chronic obstruc-
tive pulmonary disease. Heart Lung 1988;17:408–13.
[48] Emery C, Leatherman NE, Burker EJ, MacIntyre NR.
Psychological outcomes of a pulmonary rehabilitation
program. Chest 1991;100:613–7.
[49] Schols AM, Mostert R, Soeters PB, et al. Body com-
position and exercise performance in patients with chro-
nic obstructive pulmonary disease. Thorax 1991;46:
695–9.
[50] Wilson DO, Rogers RM, Wright EC, Anthonisen NR.
Body weight in chronic obstructive pulmonary disease.
Am Rev Respir Dis 1989;139:1435–8.
[51] Engelen MP, Schols AM, Baken WC, et al. Nutritional
depletion in relation to respiratory and peripheral
skeletal muscle function in out-patients with COPD.
Eur Respir J 1994;7:1793–7.
[52] Palange P, Forte S, Felli A, et al. Nutritional status
and exercise tolerance in patients with COPD. Chest
1995;107:1206–12.
[53] Shoup R, Dalsky G, Warner S, et al. Body composi-
tion and health-related quality of life in patients with
obstructive airways disease. Eur Respir J 1997;10:
1576–80.
[54] Marquis K, Debigare R, Lacasse Y, et al. Midthigh
muscle cross-sectional area is a better predictor of mor-
tality than body mass index inpatients with chronic
obstructive pulmonary disease. Am J Respir Crit Care
Med 2002;166:809–13.
[55] Schols AM, Slangen J, Volovics L, Wouters EFM.
Weight loss is a reversible factor in the prognosis of
chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 1998;157:1791–7.
[56] Ferreira IM, Brooks D, Lacasse Y, Goldstein RS. Nu-
tritional intervention in COPD: a systematic overview.
Chest 2001;119:353–63.
[57] Faling LJ. Pulmonary rehabilitation: physical modali-
ties. Clin Chest Med 1986;7:599–603.
[58] Gordon A. Vaccines and vaccinations. N Engl J Med
2001;345:1042–53.
[59] Nichol K, Margolis KL, Wuorenma J, Von Sternberg T.
The efficacy and cost effectiveness of vaccination
against influenza among elderly persons living in the
community. N Engl J Med 1994;331:778–84.
[60] Guell R, Casan P, Belda J, et al. Long-term effects of
outpatient rehabilitation of COPD: a randomized trial.
Chest 2000;117:976–83.
[61] Troosters T, Gosselink R, Decramer M. Short- and
long-term effects of outpatient rehabilitation in patients
with chronic obstructive pulmonary disease: a random-
ized trial. Am J Med 2000;109:207–12.
[62] Wijkstra PJ, Koeter GH. Outpatient pulmonary reha-
bilitation. Chest 2002;121:2082–3.
[63] Hodgkin JE, Celli B, Connors GL. Pulmonary rehabili-
tation: guidelines to success. 3rd edition. Philadelphia:
Lippincott; 2001.
[64] Mahler DA. Dyspnoea in chronic obstructive pul-
monary disease. Monaldi Arch Chest Dis 1998;53:
669–71.
[65] Singh SJ, Morgan MDL, Scott S, Walters D, Hardman
AE. Development of a shuttle walking test of disability
in patients with chronic airways obstruction. Thorax
1992;47:1019–24.
[66] Guyatt O, Berman LB, Townsend M, Pugsley SO,
Chambers LW. A measure of quality of life for clini-
cal trials in chronic lung disease. Thorax 1987;42:
773–8.
[67] Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A
self-complete measure of health status for chronic
airflow limitation: The St. George’s Respiratory Ques-
tionnaire. Am Rev Respir Dis 1992;145:1321–7.
[68] Ciccone AM, Meyers BF, Guthrie TJ, et al. Long-term
outcome of bilateral lung volume reduction in 250
consecutive patients with emphysema. J Thorac Cardio-
vasc Surg 2003;125:513–25.
[69] McKenna Jr RJ, Gelb A, Brenner M. Lung volume
reduction surgery for chronic obstructive pulmonary
disease: where do we stand? World J Surg 2001;25:
231–7.
[70] Moy ML, Ingenito EP, Mentzer SJ, et al. Health-related
quality of life improves following pulmonary rehabili-
tation and lung volume reduction surgery. Chest 1999;
115:383–9.
Index
Note: Page numbers of article titles are in boldface type.
A
Acute right heart failure, after lung surgery, 329–330
Amiodarone, for arrhythmias, after lung surgery, 327
Arrhythmias, after lung surgery, 325–327
Aspirin, for myocardial infarction, after lung
surgery, 327
Atrial tachyarrhythmias, after lung surgery, 325–327
B
b-Blockers, for myocardial infarction, after lung
surgery, 328
Breathing training, in pulmonary rehabilitation, after
lung resection, 423
Bronchiolitis obliterans, and quality of life, 402
Bronchoscopy, to predict postoperative pulmonary
function, 319
C
Cardiac herniation, after lung surgery, 325
Cardiopulmonary function, after lung surgery,
325–330
acute right heart failure and, 329–330
arrhythmias and, 325–327
cardiac herniation and, 325
chronic heart failure and, 328–329
hypertension and, 328
myocardial infarction and, 327–328
to predict postoperative pulmonary function, 318
Chemotherapy, and preoperative pulmonary
function, 299
Chest physical therapy, in pulmonary rehabilitation,
after lung resection, 423
Chronic heart failure, after lung surgery, 328–329
Chronic obstructive pulmonary disease, lung
resection for, pulmonary rehabilitation after.
See Pulmonary rehabilitation.
lung volume reduction surgery for, quality of life
after. See Quality of life.
pulmonary function in, preoperative optimization
of. See Pulmonary function.
Computed tomography, to predict postoperative
pulmonary function, 319
D
Diaphragmatic breathing, in pulmonary
rehabilitation, after lung resection, 423
Directed cough, in pulmonary rehabilitation, after
lung resection, 423
DLCO, to predict postoperative pulmonary
function, 318
E
Emphysema, lung transplantation for, quality of life
after, 401
Epidural anesthesia, thoracic, and postthoracotomy
pain syndrome, 348
Esophageal surgery, quality of life after. See Quality
of life.
return to work after, 413
Exercise tests, and preoperative pulmonary function,
297, 299
Exercise training, in pulmonary rehabilitation, after
lung resection, 421–422
F
Fundoplication, for gastroesophageal reflux disease,
quality of life after, 371
1547-4127/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/S1547-4127(04)00101-X
Thorac Surg Clin 14 (2004) 429–433
G
Gastroesophageal reflux disease, surgery for,
quality of life after. See Quality of life, after
esophageal surgery.
Glycoprotein IIb/IIIa inhibitors, for myocardial
infarction, after lung surgery, 327–328
H
Heart failure, after lung surgery, 328–330
Heparin, for myocardial infarction, after lung
surgery, 327
Hypertension, after lung surgery, 328
pulmonary, and preoperative pulmonary
function, 299
I
Inspiratory muscle training, and preoperative
pulmonary function, 300
L
Laparoscopic fundoplication, for gastroesophageal
reflux disease, quality of life after, 371
Long thoracic nerve, injury of, thoracic surgery
and, 334
Low-molecular-weight heparin, for myocardial
infarction, after lung surgery, 327
Lung surgery, cardiovascular function after.
See Cardiopulmonary function.
pulmonary function after.
See Pulmonary function.
pulmonary function optimization before.
See Pulmonary function.
quality of life after. See Quality of life.
return to work after. See Thoracic surgery, return
to work after.
risk acceptance and risk aversion in, 287–293
decision making in, 290–292
numeracy in, 287–288
patient preferences in, 288–290
Lung transplantation, quality of life after.
See Quality of life.
return to work after, 414
Lung volume reduction surgery, quality of life after.
See Quality of life.
M
Magnetic resonance imaging, to predict postoperative
pulmonary function, 319
Median sternotomy, pulmonary function after,
319–320
Minimally invasive thoracic surgery. See Video-
assisted thoracoscopic surgery.
Muscle-sparing thoracotomy, shoulder disorders
after, 333–335, 340
Myocardial infarction, after lung surgery, 327–328
Myofascial pain, in postthoracotomy pain
syndrome, 347
N
Neurogenic tumors, video-assisted thoracoscopic
surgery for, return to work after, 414
Neurohumoral paradigm, for chronic heart
failure, 329
Neuropathic pain, in postthoracotomy pain
syndrome, 347
Nutritional status, and preoperative pulmonary
function, 299, 300
Nutritional support, in pulmonary rehabilitation, after
lung resection, 423
P
Pain control, postoperative, and postthoracotomy
pain syndrome, 347–348
and reduced pulmonary function, 320
and shoulder disorders, 334–335
Postthoracotomy pain syndrome, 345–352
and quality of life, 349–350
etiology of, 346–347
incidence of, 345
management of, 350–351
myofascial pain in, 347
neuropathic pain in, 347
pain characteristics in, 345–346
pain control and, 347–348
pathogenesis of, 346–347
posterolateral thoracotomy and, 348
predictors of, 347
rib resection and, 349
surgical technique and, 348–349
thoracic epidural anesthesia and, 348
video-assisted thoracoscopic surgery and, 349
Index / Thorac Surg Clin 14 (2004) 429–433430

Procainamide, for arrhythmias, after lung
surgery, 327
Pulmonary function, postoperative, 317–323
degree of resection and, 320
long-term changes in, 320–321
pain control and, 320
preoperative assessment for, 317–319
bronchoscopy in, 319
cardiopulmonary function in, 318
computed tomography in, 319
DLCO in, 318
magnetic resonance imaging in, 319
spirometry in, 317–318
surgical approach and, 319–320
median sternotomy, 319–320
thoracotomy, 319
video-assisted thoracoscopic surgery, 319
preoperative optimization of, 295–304
age in, 299
future research on, 301
gender in, 299
in chronic obstructive pulmonary disease, 295,
297, 299
exercise tests in, 297, 299
prediction of, 295, 297
pulmonary function tests in, 297
scoring systems in, 299
inspiratory muscle training in, 300
nutritional status in, 299, 300
patient selection in, 300–301
preoperative chemotherapy and radiation
therapy in, 299
pulmonary function tests in, 300–301
pulmonary hypertension in, 299
smoking cessation in, 300
Pulmonary function tests, and preoperative
pulmonary function, 297, 300–301
Pulmonary hypertension, and preoperative
pulmonary function, 299
Pulmonary rehabilitation, after lung resection,
417–428
definitions and goals of, 417–419
education in, 422
exercise training in, 421–422
indications for, 419–420
long-term adherence to, 424
nutritional support in, 423
outcomes of, 425–426
program organization in, 424
psychosocial training and support in, 422
rationale for, 419
smoking cessation in, 420–421
vaccination in, 424
ventilatory therapy in, 423–424
Q
Quality of life, after esophageal surgery, 367–374
instruments for, 367–369
after laparoscopic fundoplication, 371
after minimally invasive esophagectomy,
370–371
after open esophagectomy, 369–370
after open fundoplication, 371
disease-specific, 368–369
EORTC questionnaires, 369, 370
Gastroesophageal Reflux Disease–Health
Related Quality of Life Scale, 369
Gastrointestinal Symptom Rating Scale,
368–369
generic, 368
in esophageal cancer, 369
in gastroesophageal reflux disease,
371–372
Psychological General Well-Being
Index, 368
SF-36, 368
Spitzer Quality of Life Index, 370
versus medical therapy, 372
after lung resection, 305–315
clinical studies on, 356–362
comparison of results in, 310–311
data analysis in, 311–314
evaluation criteria in, 309
imputation methods in, 307–308
instruments for, 354, 356
EORTC Quality of Life Questionnaires,
355, 356, 357, 358, 360, 362
Ferrans and Powers Quality of Life
Index, 355
Functional Assessment of Cancer
Therapy, 355
Functional Living Index-Cancer, 355
Lung Cancer Symptom Scale, 355
Nottingham Health Profile, 355
Rotterdam Symptom Checklist, 355
SF-36, 355, 357, 358, 359
Sickness Impact Profile, 355, 356, 358
Spitzer Quality of Life Index, 356,
357, 358
WHO Quality of Life Instrument, 355
long-term, 361
measurement of, 354
simulation study in, 308–309
symptom assessment in, 306–307
Index / Thorac Surg Clin 14 (2004) 429–433 431

versus health-related quality of life, 353–356
with video-assisted thoracoscopic surgery, 362
after lung transplantation, 385–407
bronchiolitis obliterans and, 402
comparative studies on, 401
cross-sectional studies on, 387, 392, 400
economic evaluation and cost-effectiveness in,
402–403
employment and, 402
exercise and education in, 401–402
for emphysema, 401
instruments for, 386–387
Basic Personality Inventory, 392
Beck Depression Inventory, 390
Body Cathexis Scale, 391
Brief Symptom Inventory, 390–391
Campbell Sense of Well-Being Scale, 392
Derogatis Sexual Functioning
Inventory, 391
Difficulty with Adherence, 391
EuroQol, 387, 388, 392
General Health/QOL Rating Scale, 389
general health questionnaire, 389
Hospital Anxiety and Depression
Scale, 390
Illness Intrusive Rating Scale, 391
Index of Well Being, 389
Karnofsky Performance Status, 391
Nottingham Health Profile, 388
Overall QOL visual analog scale, 388
Perceived Social Support Related to
Transplantation, 392
Pulmonary-specific QOL Scale, 392
Quality of Life Index, 389
Quality of Well-Being scale, 389
Rosenberg Self-Esteem Scale, 392
SF-20, 388
SF-36, 388
Sickness Impact Profile, 390
Sleep Disturbance, 391
Standard Gamble, 387, 389–390
State-Trait Anxiety Inventory, 390
Symptom Checklist-90, 390
Symptom Frequency/Symptom Distress
Scale, 391
Time Trade Off, 387, 390
Transplant Symptom Frequency and
Distress Scale, 391
UCLA Loneliness Scale-Revised, 391
Zung Self-rating Depression Scale, 390
limitations in, 403–405
longitudinal studies on, 400–401
significance of, 385–386
after lung volume reduction surgery, 375–383
case-control series of, 377–380
instruments for, 376–377
National Emphysema Treatment Trial on, 382
randomized studies of, 380–382
R
Radiation therapy, and preoperative pulmonary
function, 299
Respiratory failure, after lung resection, pulmonary
rehabilitation for. See Pulmonary rehabilitation.
Rib resection, and postthoracotomy pain
syndrome, 349
S
Shoulder disorders, after thoracic surgery, 331–343
etiology of, 331–335
muscle division, 332–334
patient positioning, 332
postoperative pain, 334–335
long thoracic nerve injury, 334
posterolateral versus muscle-sparing
thoracotomy, 335, 340
rehabilitation for, 340
video-assisted thoracoscopic surgery, 334, 340
Smoking cessation, and preoperative pulmonary
function, 300
in pulmonary rehabilitation, after lung resection,
420–421
Spirometry, to predict postoperative pulmonary
function, 317–318
T
Tachyarrhythmias, atrial, after lung surgery, 325–327
Thoracic epidural anesthesia, and postthoracotomy
pain syndrome, 348
Thoracic surgery, return to work after, 409–416
as outcome measure, 410
costs of absenteeism, 409–410
for benign thoracic pathology, 413–414
for esophageal cancer, 413
for lung cancer, 410, 412–413
open surgery, 412
video-assisted thoracoscopic surgery,
412–414
future research on, 414
shoulder disorders after. See Shoulder disorders.
Index / Thorac Surg Clin 14 (2004) 429–433432
Thoracotomy, pain after. See Postthoracotomy
pain syndrome.
pulmonary function after, 319
return to work after, 412, 414
shoulder disorders after. See Shoulder disorders,
after thoracic surgery.
V
Vaccination, in pulmonary rehabilitation, after lung
resection, 424
Ventilatory therapy, in pulmonary rehabilitation, after
lung resection, 423
Video-assisted thoracoscopic surgery, and
postthoracotomy pain syndrome, 349
pulmonary function after, 319
quality of life after, 362
return to work after, 412–414
shoulder disorders after, 334, 340
Index / Thorac Surg Clin 14 (2004) 429–433 433