Embed Size (px)
Citation preview

Quality Assured Spirometry
Laura Leeks
Specialist Respiratory Physiotherapist
Camden COPD and Home Oxygen Service

A Guide To Performing Quality Assured Diagnostic Spirometry
(Association for Respiratory Technology and Physiology (ARTP 2013)

Quality Assurance
“Refers to planned and systematic activities implemented to provide
adequate confidence that the results will fulfil requirements for
quality.”
Grant EL and Leavenworth RS (1988) Statistical Quality Control

Quality Assurance
“Refers to planned and systematic activities implemented to provide
adequate confidence that the results will fulfil requirements for
quality.”
Grant EL and Leavenworth RS (1988) Statistical Quality Control
Consistent processes in
place

Quality Assurance
“Refers to planned and systematic activities implemented to provide
adequate confidence that the results will fulfil requirements for
quality.”
Grant EL and Leavenworth RS (1988) Statistical Quality Control
Consistent processes in
placeResults are
valid and reliable

Spirometry is the recommended objective test performed to identify abnormalities in lung volumes and air flow
What is Spirometry?

Spirometry is the recommended objective test performed to identify abnormalities in lung volumes and air flow
What is Spirometry?
It is NOTPulmonary Lung Function
Testing
Includes transfer factor and other measures of
pulmonary function

Equipment
Person
Procedure
Interpretation
What do we need?

Equipment

3 litre syringe
Prior to every clinic / session or after every 10th patient
Calibration log maintained
Biological control
Calibration

Before the test STOP: Short acting bronchodilators for 4 hours
Long acting beta 2 agonist bronchodilators for 8 hours
Long acting muscarinic antagonist bronchodilators for 36 hours
Before the test AVOID: Smoking for at least 24 hours
Eating a large meal
Vigorous exercise
Wearing tight clothing
Pre-test advice

Contraindications
Absolute Active Infection Conditions that might cause
serious consequences if aggravated by forced expiration: Dissecting / unstable aortic
aneurysm Current pneumothorax Recent surgery – opthalmic,
abdominal, thoracic, neurosurgery
Relative Suspected respiratory infection
in last 4-6 weeks Undiagnosed symptoms e.g.
Haemoptysis Conditions that might be
aggravated by forced expiration: Prior pneumothorax Unstable vascular system
(e.g. MI in last month, uncontrolled hypertension, PE or haemorrhagic event)
Previous relevant surgery Patient too unwell Communication problems

Vital signs
Height (arm span if unable to stand)
Weight (BMI)
Age
Gender
Ethnicity
Pre-test measurements

Global Lung Function Initiative (GLI) reference values not the European Community of Coal and Steel (ECSS)
Hong Kong Chinese 100% (as per Caucasian)
Japanese American 11% Reduction
Polynesians 10% Reduction
North Indians and Pakistanis 10% Reduction
South Indians and African Descent 13% Reduction
Ethnicity and predicted values
Quanjer et al (2012) Multi-ethnic reference values for spirometry for the 3-85 year age range: The Global Lung Function 2012 Equations. Report of the Global Lung Function Initiative (GLI), ERS Task Force to establish improved Lung Function Reference Values. European Respiratory Journal 40(6) 1324 - 1343
Global Lung Function Initiative (GLI) reference values not the European Community of Coal and Steel (ECSS)
Hong Kong Chinese 100% (as per Caucasian)
Japanese American 11% Reduction
Polynesians 10% Reduction
North Indians and Pakistanis 10% Reduction
South Indians and African Descent 13% Reduction
Ethnicity and predicted values
Quanjer et al (2012) Multi-ethnic reference values for spirometry for the 3-85 year age range: The Global Lung Function 2012 Equations. Report of the Global Lung Function Initiative (GLI), ERS Task Force to establish improved Lung Function Reference Values. European Respiratory Journal 40(6) 1324 - 1343
Less accurate in ‘young’ (under
estimates) and ‘old’ (over estimate)

Global Lung Function Initiative (GLI) reference values not the European Community of Coal and Steel (ECSS)
Hong Kong Chinese 100% (as per Caucasian)
Japanese American 11% Reduction
Polynesians 10% Reduction
North Indians and Pakistanis 10% Reduction
South Indians and African Descent 13% Reduction
Ethnicity and predicted values
Quanjer et al (2012) Multi-ethnic reference values for spirometry for the 3-85 year age range: The Global Lung Function 2012 Equations. Report of the Global Lung Function Initiative (GLI), ERS Task Force to establish improved Lung Function Reference Values. European Respiratory Journal 40(6) 1324 - 1343
Less accurate in ‘young’ (under
estimates) and ‘old’ (over estimate)
Download software onto the desktop
spirometer so automatically calculates the
reduction when put in ethnicity
Vital Capacity (VC)
Forced Vital Capacity (FVC)
Forced Expiratory Volume in 1 second (FEV1)
FEV1/FVC
FEV1/VC
(Maximal inspiration for maximal exhalation)
Procedure
If baseline spirometry obstructive picture
Salbutamol
2.5mg via nebuliser
4 x 100mcg (as single puffs) via spacer
Perform spirometry 15 minutes after bronchodilation
Post-bronchodilator testing

If baseline spirometry obstructive picture
Salbutamol
2.5mg via nebuliser
4 x 100mcg (as single puffs) via spacer
Perform spirometry 15 minutes after bronchodilation
Post-bronchodilator testing
This is not reversibility testing
for asthma(although it is the same process)

“Operator trained and assessed to ARTP or equivalent standards” (expert clinician program – portfolio)
No more than 100ml variation
Within 5%
Observe technique
No more than 8 forced manoeuvres in one session
Appropriate rest time between manoeuvres
Repeatability

Recording results
Actual values
Largest FEV1
Largest VC or FVC
Percentage predicted values
FEV1
FVC
Lower limit of normal
FEV1/VC or FEV1/FVC
Levy et al (2009) Diagnostic Spirometry in Primary Care; proposed standards for general practice compliant with ATS and ERS. Primary Care Respiratory Journal 18(3) 130-147

Graphs

Interpretation
Flow Volume graph

Volume Time graph
Interpretation

Tongue or teeth obstructing mouthpiece
Leak around mouthpiece
Cough
Slow start
Early stop
Poor effort
Common technical errors

2nd Breath

2nd Breath
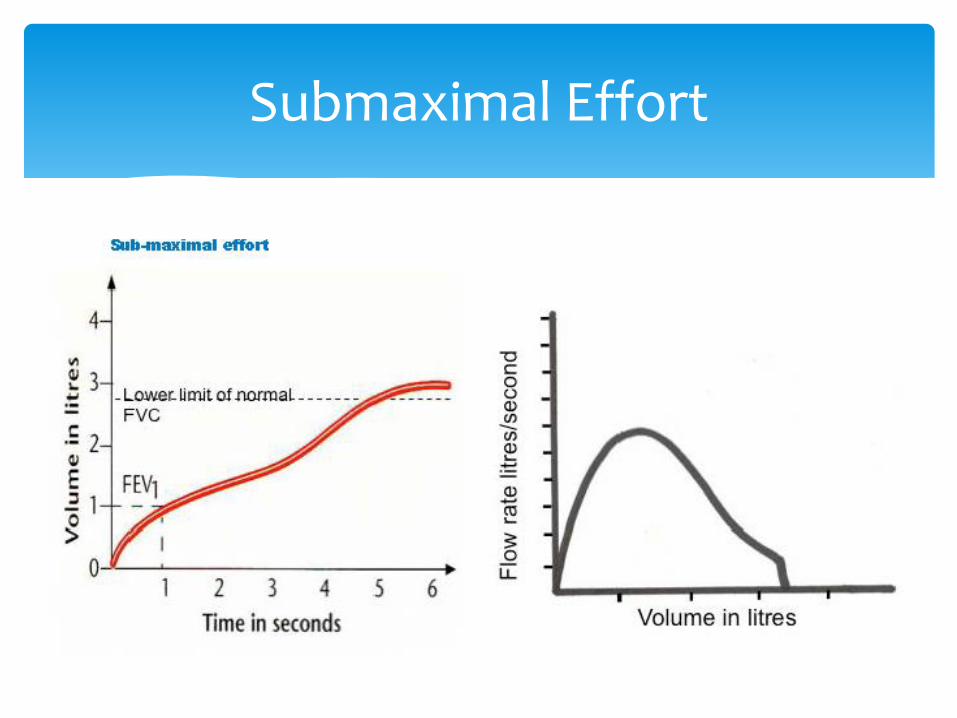
Submaximal Effort

Submaximal Effort
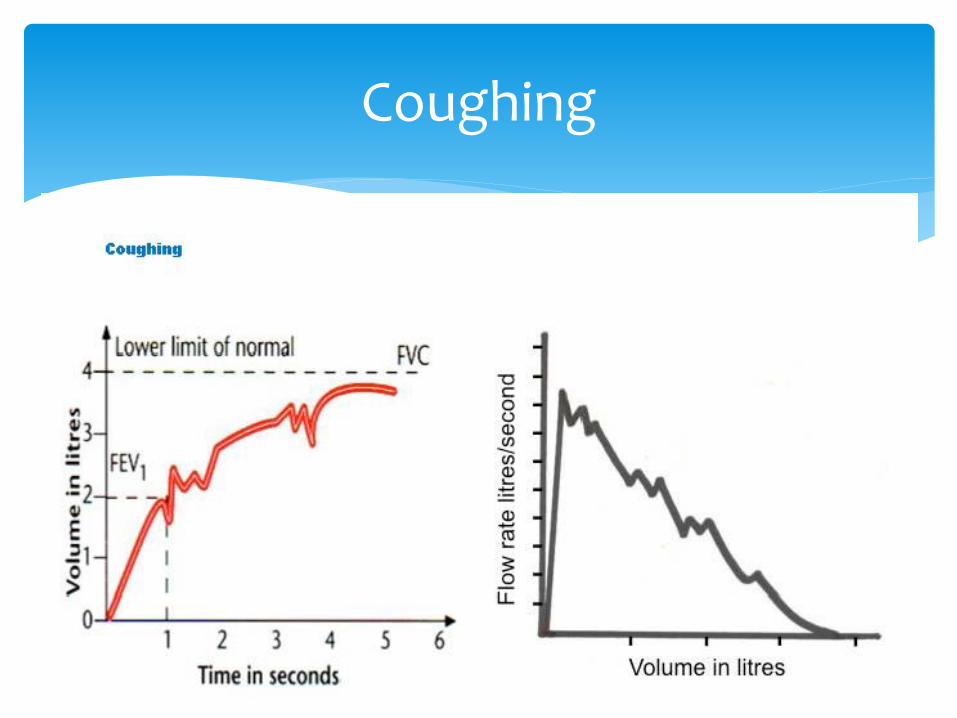
Coughing

Coughing

Slow start

Early Stop

Early Stop

FEV1/FVC < 0.7
Lower limits of normal
Obstructive picture
© Global Initiative for Chronic Obstructive Lung Disease, Inc. (2017)www.goldcopd.org

1. Patient Demographics
2. Technical acceptance of blows
3. Number of blows
4. Quality of blows
5. Reproducibility
6. Airflow obstruction (FEV1/FVC)
7. Severity (FEV1 % predicted)
8. Limitations
9. Reversibility
10. Check the Clinical Picture
Top 10 tips for reporting results