Embed Size (px)
Citation preview

QIPP and the Merseyside ApproachCompetence Based Workforce Planning
Alison Johnson
Assistant Director of Organisational Development
NHS Merseyside

Some Context:•Workforce consumes about two thirds of all spending
•Affordability is the biggest challenge facing the NHS
•Compiling an affordable workforce plan is therefore a ‘must do’
•Tinkering at the edges will not be enough to meet the challenge
•A more fundamental review is required
•Competence Based Workforce Planning is new – but does provide a methodology for such a review

What Are We Trying To Achieve:
•An affordable workforce in each of the years to 2014 / 2015
•The right ‘shape and size’ of workforce to deliver the quantities and quality required by patients and Commissioners
•A workforce whose members possess the ‘right’ competences
•A modernised workforce that is ‘fit for purpose’

Process Summary
•“Competence Based Workforce Planning” is a bottom up activity which can be undertaken at the level of individual services, pathways or departments within NHS organisations. After selecting an appropriate section of the workforce, there are three main phases of work:
•Competence mapping.•Competence sampling.•Modelling possible workforce options for the future and then decision making.

The Methodology
•Establishing baseline workforce information -Mapping the workforce to the pathways and obtaining information about the roles.
•Mapping Skills for Health competences to existing job descriptions and the future pathways.
•Clustering the competences - developing a framework.•Competence sampling exercise –
To determine how much time is spent in each of the competence areas, with further analysis by role and pay band.
•Stakeholder Engagement – Workshops held with Commissioners, managers, employees, Unions, Private Voluntary and Independent sector representatives re future service and workforce changes.

An Integrated Approach:
• Planning for an affordable workforce is important
BUT: it is not the only planning element of a well thought-out and holistic approach to a review
• Other elements include:Service designProcess designFinancial planning assumptionsQuality
• The workforce plan must reflect work in these areas• - - - and vice versa!

The Knowsley Experience
Background and Context
•Knowsley Health and Wellbeing (NHS Knowsley and Knowsley Borough Council Directorate of Wellbeing Services)•Project driven by an ambition to meet future service needs, improve quality and realise efficiencies in line with QIPP•Project required major investment of time and resource to develop and implement competence based workforce planning.

What was Done?•Mapping of future competence requirements against End of Life and Long Term Conditions pathways, drawing on End of Life common core principles and broader skills for health database•Information used to develop a competence framework which was compared against current roles•Competence sampling undertaken by existing workforce to see which competences were currently being deployed, for how much time, and at what level•Workshops held at the outset, and following the sampling, to discuss workforce structures, competences and service issues

Challenges
•Identification of a manageable number of competences at the outset given the huge range of competences from which to choose. Therefore, use of high level competences through Skills for Health was key.•Good understanding of the Skills for Health tools was invaluable•Sampling competences was a difficult concept to convey to staff as we tend to think in terms of activities. Time invested in 1:1 support, a guidance document, and trial exercise•Completing of diary sheets by staff is time consuming, and time taken to support staff in this was under-estimated.

An Example Of A ‘Competence’:
• Heading ‘M&L D12 – Participate in Meetings’• It is six pages long• Details include:
Overview9 performance criteriaKnowledge of values, legislation, organisational policy & procedures and theory & practiceList of behaviours and skills
• The competence is ‘non-denominational’• - - - and may need ‘contextualising’
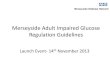
Competence Mapping:Job R
ole A
Job Role B
Job Role C
Job Role D
KSF
№Competence
Competence or Cluster title Dimension Level
Undertake Care Assessment
1 CM A1 Obtain information to inform the assessment of an individual HWB6 Level 3 X X X X
2 CM A2Establish an individual's functional capabilities in the terms of LTC clinical management
HWB6 Level 3 X X X X
3 CM A3Investigate and diagnose an unwell individual as part of LTC clinical management
HWB6 Level 4 X X X X
4 CM A4Plan, implement, monitor and review therapeutic interventions with individuals who have a LTC and their carers
HWB5 Level 3 X X X X
5 CM A5 Assess individual needs and preferences HWB2 Level 3 X X X X
6 CM A6 Enable individuals with LTC to manage their medicines HWB4 Level 3 X X X
7 CM A7 Prescribe medication for individuals with a LTC HWB7 Level 4 X X
8 CM B3Develop risk management plans to support individuals' independence and daily living within their own homes
HWB2 Level 3 X X
9 PE6Identify the learning needs of patients and carers to enable management of a defined condition
G1 Level 2 X

• The reduction in workforce size is only 5%• - - - but the financial saving is 25%, even after some
reinvestment
BEFORE AFTER
FTE FTE
Band 2 0.81 0.59
Band 3 12.01 8.77
Band 3 A&C 0.00 2.70
Band 4 3.04 14.45
Band 5 20.79 6.04
Band 6 9.44 6.41
Band 7 8.55 4.89
Band 7 Patient/Volunteer Support Officer
0.00 1.00
Band 8A 4.71 1.56
Voluntary Sector 0.00 10.00
TOTAL 59.35 56.40

Key Outcomes
•The workforce planning models have enabled development planning in alignment with service user needs•Staff are involved in designing more effective structures and roles that will provide both quality and efficient service delivery•The models project workforce and service changes with increased service user contact time and £1.2m potential recurrent savings. Savings are through change to skill mix rather than from a large reduction in staff numbers

Shaping the Workforce for the MCSS
•An affordable workforce•The right shape and size of workforce to deliver the quantities and quality of service required by commissioners•A workforce whose members possess the right competencies•Sufficient intelligence to inform the commissioning of future education and training

• “As Is” position understood through diary collection with a sample of 25% of the workforce whose destination is the MCSS
• This will provide a costed workforce model based on three approaches- minimal change- halfway house- radical change
• Workforce planning aligned to identification of new values and behaviours for the MCSS. Having the right talents requires the behaviours to be used in selection an development
• Role Profiles will be ready for late Spring for MCSS
Shaping the Workforce - Modelling Issues:
• Percentage of time in meetings
• The scope for using new technology
• Other process design issues
• CCG priorities
• The degree to which the current grade mix is consistent with the competence mix
• What would a ‘radical change’ option look like?

Key LearningKey learning
•Competence based workforce planning is not a quick win solution, it is time consuming and requires investment•Essential to secure buy-in of Executive Team, service managers, and Trade Union Representatives•If the required resource and investment is in place, its an effective way to plan for the future workforce