Embed Size (px)
Citation preview
This article was downloaded by: [University of Cambridge]On: 08 October 2014, At: 09:15Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
QuestPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uqst20
Putting Physical Activity on the PolicyAgendaCatherine B. Woods a & Nanette Mutrie ba School of Health and Human Performance , Dublin City University ,Dublin , Irelandb School of Psychological Sciences and Health , University ofStrathclyde , Glasgow , UKPublished online: 09 May 2012.
To cite this article: Catherine B. Woods & Nanette Mutrie (2012) Putting Physical Activity on thePolicy Agenda, Quest, 64:2, 92-104, DOI: 10.1080/00336297.2012.669318
To link to this article: http://dx.doi.org/10.1080/00336297.2012.669318
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Quest, 64:92–104, 2012Copyright © National Association for Kinesiology in Higher Education (NAKHE)ISSN: 0033-6297 print / 1543-2750 onlineDOI: 10.1080/00336297.2012.669318
Putting Physical Activity on the Policy Agenda
CATHERINE B. WOODS
School of Health and Human Performance, Dublin City University, Dublin, Ireland
NANETTE MUTRIE
School of Psychological Sciences and Health, University of Strathclyde, Glasgow, UK
The purpose of this paper is to outline why physical activity policy is important in terms of promotingpopulation based increases in physical activity. The promotion of physical activity through public pol-icy happens globally and nationally, however to be successful it should also happen at state and locallevels. We outline the rationale for the promotion of physical activity and the decrease of inactivityfrom a public health perspective. The World Health Organization guidelines for physical activity arethen presented, followed by current physical activity prevalence rates in Europe and the US. We offera description of what physical activity policy is and the key criteria for inclusion in order to increasethe likelihood of its success. Finally, we present two case studies in relation to physical activity pol-icy from Scotland and Ireland. Throughout we discuss how education and physical education couldbenefit from such policies, or be hindered by lack of relevant policy.
Keywords physical activity, policy, public health, physical education
Physical inactivity involves little or no movement and has recently been identified as thefourth leading risk factor for mortality in the world (http://www.globalpa.or.uk). Physicalactivity involves any bodily movement that is produced by the contraction of the skele-tal muscles and that substantially increases energy expenditure (Caspersen, Powell, &Christenson, 1985). Regular participation in health enhancing physical activity (activitythat is sufficiently above baseline activity to produce health gain) has numerous healthbenefits including a reduction in coronary heart disease and stroke, diabetes, hypertension,colon cancer, breast cancer, and depression (World Health Organization, 2003; Mathers,Stevens, & Mascarenhas, 2009). The majority of most populations do not engage in suf-ficient physical activity to gain these health benefits. The high risk and high prevalenceof inactivity in most countries around the world make the promotion of physical activitya major public health concern. In addition, physical inactivity contributes substantially todirect and indirect healthcare costs. Such an important health behavior should be central toeducation programs and activities.
Yet physical activity has more to offer than purely individual or societal health ben-efits. Physical education, the systematic introduction to, and education in, sport, exercise,and physical activity as part of the school curriculum, provides children with opportunitiesto not only learn about movement skills, but also to learn through these activities aboutother aspects of knowledge (Hardman, 2008). Physical activity can also help promote sus-tainable development; urban design principles or transport policies that promote pedestrian
Address correspondence to Catherine B. Woods, School of Health and Human Performance,Dublin City University, Dublin 9, Ireland. E-mail: [email protected]
92
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 93
and bicycle travel give people the chance to opt to walk or cycle as a form of transport, thuspotentially reducing greenhouse gas emissions, congestion and air pollution (Heath et al.,2006).
The global recommendations on physical activity for health published by the WorldHealth Organization (WHO) in 2010 aim to provide scientifically-informed guidanceon how much physical activity (in terms of frequency, intensity, time and type) differ-ent population subgroups should do in order to accrue health benefits (World HealthOrganization, 2010a). According to these recommendations, all children and young people(aged 5–17 years) should accumulate at least 60 minutes of moderate to vigorous-intensityphysical activity daily. While most of this activity will be aerobic in nature, the impor-tance of incorporating activities that strengthen muscle and bone at least three times perweek was also suggested. For this age group opportunities to be active should be facili-tated through the family, the school and the community where the child lives, and includeactivities like play, games, sports, transportation, recreation, physical education, or plannedexercise. Clearly education has a major role to play both in educating children about thelevel of activity they should be doing to gain health benefits, but also in giving children theskills and attitudes which will help them lead a physically activity life. A main contributorto this education will be the physical education opportunities available to children.
For adults (aged 18–64 years), the WHO recommends participation in at least150 minutes of moderate-intensity aerobic activity per week, or at least 75 minutes ofvigorous-intensity aerobic activity weekly, or an equivalent combination of moderate- andvigorous-intensity activity (with activity performed in bouts of at least 10 minute dura-tion). Additional benefits can be accrued relative to increasing the duration of the activityat each intensity level. Similar aerobic physical activity recommendations exist for olderadults (65 years plus), with the addition of advice for those with poor mobility, or otherhealth conditions that might limit their ability to engage in physical activity. Additionally,engaging in muscle strengthening activities which involve the major muscle groups on atleast two days per week is encouraged for all adults.
These guidelines have been adopted by numerous countries worldwide (Department ofHealth and Children, 2009; OECD, 2010; U.S. Department of Health and Human Services,2008; UK Department of Health, 2004; Chief Medical Officers, 2011). Physical activityguidelines are important because they clarify for individuals, physical activity profession-als, physical education teachers, and other key stakeholders in physical activity promotionhow much physical activity is required to benefit current and future health. This is impor-tant advocacy information as it can be used to inform physical activity policy formation,by for example, providing starting points from which to set targets for physical activitypromotion at population level or to justify the need for curriculum time for physical educa-tion and extra-curricular activities. Guidelines also inform surveillance of population levelsof physical activity, allowing for monitoring over time and inter-country comparisons tobe determined and can also be used by those in charge of quality control in educationto determine if schools are achieving goals in relation to physical education and relatedactivity.
However, levels of physical activity in most populations are low, with levels of physicalinactivity rising in many countries. In Europe, approximately one in five children meet thephysical activity guidelines for developing their current and future health (Currie et al.,2008; OECD, 2010). In 2001, 45.4% of U.S. adults self-reported achieving the US physicalactivity recommendations (Centers for Disease Control and Prevention, 2003). More thanhalf of the total adult population across the European Union (EU) and across the US arenow overweight or obese, and the rate of obesity has more than doubled over the past
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

94 C. B. Woods and N. Mutrie
20 years in most EU countries (OECD, 2010; Flegal, Carrol, Ogden, & Curtin, 2010).Physical inactivity is a public health issue.
From this background it is clear that intervention is needed to promote population lev-els of physical activity. Traditional physical activity programs that focus on the individualhave had limited success in promoting long-term adherence to physical activity (Mutrie &Woods, 2003). Obstacles can prevent even the most motivated individual from being active.These obstacles include car as opposed to pedestrian orientated transportation systems,sedentary jobs, poor physical education provision leading to a lack of skill, competence orunderstanding, lack of, or poorly maintained parks and other green spaces, and communitydesigns that require driving (King & Sallis, 2009). An ecological approach to the promo-tion of physical activity is recognized as having potential to meet this grand challenge.Ecological models recognize the importance of individual influences (intra-individual) onhealth behavior, but they also identify the contribution of social and environmental factors(extra-individual) (Sallis, Owen, & Fisher, 2008). They also adhere to the Ottawa Charterfor Health Promotion (World Health Organization, 1986). Figure 1 gives an example ofhow an ecological model works; it posits that behavior is influenced by intra-individual(e.g. attitudes, knowledge, skill), and extra-individual (at (1) interpersonal, for example,teacher-child relationship; (2) organizational, for example, provision of physical educationwithin a school setting; (3) community, for example, relationships between schools in howthey address the needs of children and youth in after-school sport, and (4) public policy,for example, educational policy on frequency and duration of physical education classeswithin the school timetable) factors.
At the public policy level, the initiation, co-ordination and implementation of poli-cies that promote physical activity, enhance opportunities for whole populations to beactive, and develop environments that promote active choices are necessary (Bull, Bellew,Schoppe, & Bauman, 2004). This, policy based approach, is endorsed by the World HealthAssembly (in 2004, and again in 2008) in Resolution WHA57.17: Global Strategy on
Individual
SocialEnvironment
PhysicalEnvironment
Policy
Figure 1. Graphic representation of the social-ecological model (color figure available online).
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 95
diet, Physical Activity and Health, and Resolution WHA61.14: Prevention and Controlof Non-communicable Diseases (NCD), and most recently in the High-level Meeting of theUnited Nations General Assembly on the prevention and control of NCD (World HealthOrganization, 2004; World Health Organization, 2008; United Nations General Assembly,2011). The resolutions urged Member States and Governments to develop national physi-cal activity action plans and policies, with the ultimate aim of increasing physical activitylevels in their populations. Prior to these resolutions, the Center for Disease Prevention andHealth Promotion (CDC) and the World Health Organization (WHO) set up the CDC WHOCollaborating Center for Physical Activity and Health Promotion. This center is locatedwithin the Division of Nutrition and Physical Activity at the CDC, and over the past decadeit has helped focus global health policy on physical activity promotion by (1) building anevidence-base for interventions, (2) developing tools for surveillance of population levelsof physical activity, (3) evaluation, and (4) building capacity of those working in physicalactivity and health promotion (Pratt, Epping, & Dietz, 2009). Pratt and colleagues indicatedthat today physical activity is central to good public health practice globally and nationally;however, they identified a future challenge as the development of this practice at state andlocal level. The development of physical activity policy is central to this change in practice,as a co-ordinated approach where global, national, regional, state, and local level policiesthat promote, enhance, and develop opportunities for individuals, groups, and whole popu-lations to be physically active are supported (irrespective of their origin—health, education,sport and recreation, transport, and so on). The remainder of this manuscript will discusswhat a physical activity policy is, guidelines on how to write one and examples of goodpractice that include practice in physical education. Although reference is drawn through-out to a “national” physical activity policy, this information equally applies to physicalactivity policy written for state, regional, or local areas.
What is Physical Activity Policy?
A policy is a statement of intent. Policy may be conceptualized as . . . “formal writtencodes, regulations or decisions bearing legal authority . . . as written standards that guidechoices or . . . as unwritten social norms that influence or guide behavior” (Schmid, Pratt, &Witmer, 2006, p. S22). Health-related public policy is when public policy impacts directlyor indirectly on health, by for example, at a national level through legislation creating sup-portive environments for individuals to engage in health promoting behavior. This can occurat a national level (for example, a law preventing individuals from smoking in workplaces)or at a local level (for example, a school or a school district adopting a physical activitypolicy that facilitates active school transport). A physical activity policy is an example ofa public health policy. It is a document that defines physical activity as a priority area;that identifies specific population goals and targets, and that provides a framework foraction, or an action plan to achieve these goals (Bellew, Schoppe, Bull, & Bauman, 2008).Ideally, a physical activity policy should also define of roles and responsibilities of involvedpartners, allocation of resources, and clearly identify accountability for implementation ofspecific components of the policy aligned to a realistic and achievable timeframe (Bullet al., 2004).
Why is PA Policy Important?
A successful national physical activity policy has the potential to influence the health andwell-being of an entire population. Successful state or local policies have the potential
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

96 C. B. Woods and N. Mutrie
to influence all of the individuals within their geographical area, or specific setting, forexample, a school or workplace. Policy can give support, coherence, and visibility at thepolitical level, while also making it possible for the organizations involved at national,regional, and local levels—for example, national government sectors, regional or localauthorities, stakeholders, and the private sector—to be logical and consistent in theiractions to achieve a shared goal (World Health Organization, 2010b). It can give all rel-evant organizations a mandate to adopt shared strategies based on identified roles andresponsibilities.
This policy approach to the promotion of physical activity requires collaboration andinteraction among policy makers from several different sectors, each tackling the physicalactivity goal for different reasons but with the same agenda to get the population or popu-lation subgroup more active. A number of different government sectors can play a role inachieving national physical activity goals. Although the main policy focus of these differ-ent sectors is probably not “to increase levels of population physical activity,” if the policymakers within each sector can be convinced that physical inactivity is a problem that needsto be addressed, then they can change their public policy or allocate their public fundsin ways designed to address this problem (Leyden, Reger-Nash, Bauman, & Bias, 2008).Additionally, advocacy in partnership for adequate resources and accountability for use ofthese resources as well as acknowledgment of contribution could potentially lead to a betterpolicy. However, this leveraging of existing sector assets requires active engagement andcooperation across a number of sectors (Mowen & Baker, 2009). WHO recently outlinedthe potential role of different government sectors, identifying the specific roles that can beplayed by public health, transport, environment, sport, and education sectors in the promo-tion of physical activity. For example, in Ireland, the Smarter Travel Policy (Departmentof Transport, 2009) states that there is a need to “minimize the negative impacts of trans-port on the local and global environment through reducing localized air pollutants andgreenhouse gas emissions” (p. 27), and one strategy it proposes to do this is “of all travelmodes, cycling and walking have the lowest environmental impact. If we are to success-fully promote cycling and walking as realistic alternatives to the private car we need toensure that they are, as far as possible, a safe and pleasant experience” (2008, p. 42). Thefocus here is not on health, but on sustainability and environmental impact, yet with closecollaboration both the health and the sustainability goals can be achieved. Similarly, thepromotion of mixed land-use or urban planning strategies that facilitate physical activitywould come under the remit of the environment sector, creating school environments (notjust curricula) that promote and encourage active lifestyles would be the remit of educationand so on.
The Toronto Charter for Physical Activity was launched in May 2010 by the GlobalAdvocacy Council for Physical Activity (see www.globalpa.org.uk). This document is a callfor action and an advocacy tool; its aim is to create sustainable opportunities for physicallyactive lifestyles for everyone. Within the Toronto Charter there are nine guiding principleslisted for a population based approach to physical activity. These guiding principles iden-tify the importance of evidence based approaches, of embracing equity by reducing socialand health inequalities or removing disparities in access to physical activity. Importantly,the principles acknowledge the need to move beyond the individual to include environmen-tal and social determinants of physical inactivity. Other principles identify sustainability,a life-course approach to promoting activity and the need to garner political support andresource commitment at the highest level. Four key action areas are identified; each areamakes a unique contribution but also builds and is shaped by the other areas. Each area
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 97
requires action in partnership and the actors are listed as government, civil society, aca-demic institutions, professional associations, the private sector, and other organizations aswell as the communities themselves.
Area one: Implement a national policy and action plan. The Toronto Charter outlineshow the presence of such a policy or plan will unify the many different sectors in work-ing together to achieve a common goal. It also states how it would help clarify politicaland financial commitment to the promotion of physical activity. Key components of such apolicy or plan include: engaging relevant stakeholders, identifying clear leadership, know-ing roles and actions of all stakeholders, having an implementation plan that identifiestimelines, funding, and accountability. Ensuring that evidence based guidelines on physi-cal activity and health are adopted and having a repertoire of different strategies that areevidence-informed and inclusive of different social, cultural, and economic backgrounds isalso recommended. Even though the Toronto Charter stresses the importance of this areaas a key population based approach it suggests that the absence of such a policy or planshould not prevent, nor delay regional, state, or local efforts to increase physical activity orto develop relevant policy at their levels (Globalpa.org.uk).
Area two: Introduce policies that support physical activity. This area highlights sup-portive policy and the regulatory environment in which this is placed. It cites examples suchas urban planning and design to support sustainable transport options, fiscal policies to sub-sidise physical activity participation or educational policies to ensure quality opportunitiesare provided to all children both within and outside the curriculum timetable at the schoolsetting.
Area three: Reorient services and funding to prioritise physical activity. This areaexplains how different government sectors can still deliver their core business, but changetheir priorities to focus on health enhancing physical activity goals. This would allow formultiple benefits to be achieved, but these would need to be recognized as important andgiven adequate priority. For example in Sport, Parks, and Recreation, changing the focusaway from elite or competitive sport participation to include a mass participation, an inac-tive or a disabilities focus and consequently provide staff training to build capacity in theseareas. In Health this would involve giving greater priority to primary prevention and healthpromotion, as opposed to secondary or tertiary prevention.
Area four: Develop partnerships for Action. Programs that focus on changing healthbehavior of individuals within one sector can be labor, time, and money intensive. Ratherpartnership that links programs across sectors, for example, education, transport, sports,parks, and recreation and other sectors could create efficiencies, enhance use of community-based physical activity programmes and increase physical activity (Mowen & Baker, 2009).Examples of different partnerships and collaborations across national, regional, and locallevels are given within the Toronto Charter see www.globalpa.org.uk.
Characteristics of Successful Physical Activity Policy
Based on a review of literature and on consensus meetings representing experiences ofwriting physical activity policies from around the world a set of characteristics for generat-ing successful physical activity policy were published (Bellew et al., 2008). These criteriadescribed by the acronym HARDWIRED, are explained in Table 1 and reflect the “charac-teristics absolutely essential for national physical activity policy development” (p. 2). Theauthors go on to suggest that these need to be embedded for the long-term in order to deliversuccessful outcomes.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014
98 C. B. Woods and N. Mutrie
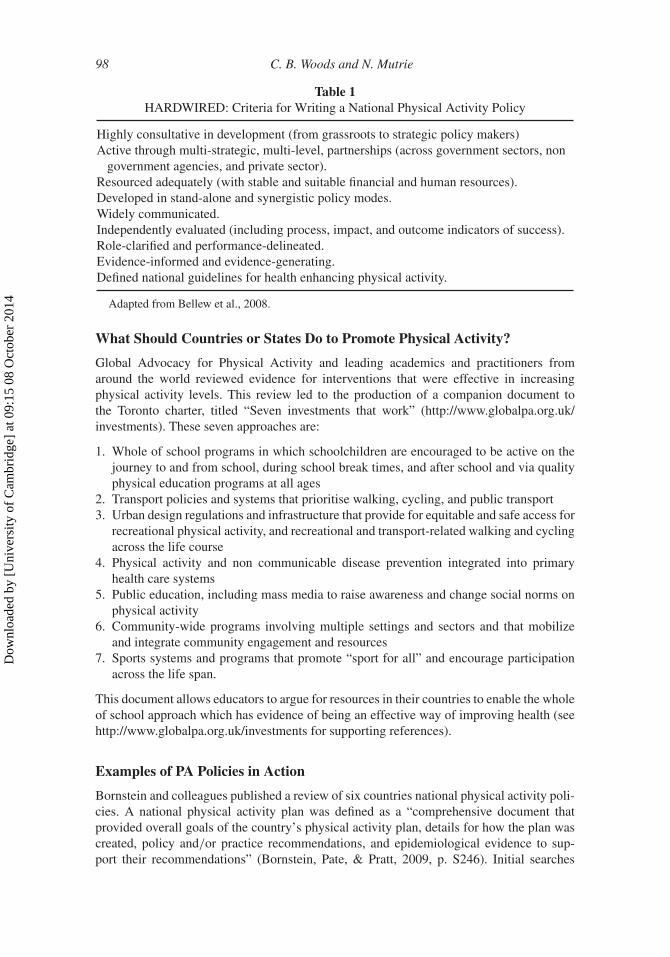
Table 1HARDWIRED: Criteria for Writing a National Physical Activity Policy
Highly consultative in development (from grassroots to strategic policy makers)Active through multi-strategic, multi-level, partnerships (across government sectors, non
government agencies, and private sector).Resourced adequately (with stable and suitable financial and human resources).Developed in stand-alone and synergistic policy modes.Widely communicated.Independently evaluated (including process, impact, and outcome indicators of success).Role-clarified and performance-delineated.Evidence-informed and evidence-generating.Defined national guidelines for health enhancing physical activity.
Adapted from Bellew et al., 2008.
What Should Countries or States Do to Promote Physical Activity?
Global Advocacy for Physical Activity and leading academics and practitioners fromaround the world reviewed evidence for interventions that were effective in increasingphysical activity levels. This review led to the production of a companion document tothe Toronto charter, titled “Seven investments that work” (http://www.globalpa.org.uk/investments). These seven approaches are:
1. Whole of school programs in which schoolchildren are encouraged to be active on thejourney to and from school, during school break times, and after school and via qualityphysical education programs at all ages
2. Transport policies and systems that prioritise walking, cycling, and public transport3. Urban design regulations and infrastructure that provide for equitable and safe access for
recreational physical activity, and recreational and transport-related walking and cyclingacross the life course
4. Physical activity and non communicable disease prevention integrated into primaryhealth care systems
5. Public education, including mass media to raise awareness and change social norms onphysical activity
6. Community-wide programs involving multiple settings and sectors and that mobilizeand integrate community engagement and resources
7. Sports systems and programs that promote “sport for all” and encourage participationacross the life span.
This document allows educators to argue for resources in their countries to enable the wholeof school approach which has evidence of being an effective way of improving health (seehttp://www.globalpa.org.uk/investments for supporting references).
Examples of PA Policies in Action
Bornstein and colleagues published a review of six countries national physical activity poli-cies. A national physical activity plan was defined as a “comprehensive document thatprovided overall goals of the country’s physical activity plan, details for how the plan wascreated, policy and/or practice recommendations, and epidemiological evidence to sup-port their recommendations” (Bornstein, Pate, & Pratt, 2009, p. S246). Initial searches
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 99
yielded 252 documents from 52 countries or regions, but following an inclusion criteria,for example, excluding documents that did not represent one country a total of 6 docu-ments from 6 countries emerged and were included in the review. The countries representedwere Australia, United Kingdom, Scotland, Sweden, Northern Ireland, and Norway (HealthPromotion Agency for Northern Ireland, 1997; The Strategic Inter-Governmental Forumon Physical Activity and Health, 2005; National Food Administration & National Instituteof Public Health, 2005; Scottish National Physical Activity Task Force, 2003; Ministryof Health and Care Services, 2005; UK Department of Health, 2009). In common, allplans included key elements like consultation with key stakeholders; development ofcoalitions across government, nongovernment and private sectors; use of individual andenvironmental strategies for intervention. Most plans were found to be remiss in includingdetails on funding for implementation or evaluation of the plan, two of the key compul-sory elements highlighted by Bellew and colleagues (Bellew et al., 2008). Evaluation andreview of the plan were conducted by only two countries, Northern Ireland and Scotlandrespectively.
Bornstein and colleagues (Bornstein et al., 2009) provide an overview of the processthat different countries’ went through in order to develop their physical activity plans.This process gives details on the consultation methodology and/or the relevant nationaldocuments that were published prior to the publication of the physical activity plan, butwere important in paving the way for the national plan to be adopted. Their paper out-lines the subpopulations targeted, for example, people aged 50+ (N. Ireland), children(Australia), and adults (Scotland, Norway), and it provides details on the overall visionand the strategic objectives of each country’s plan. The vision statements for each countryare different, but include reference to increasing levels of health related physical activity,to decreasing sedentary or inactive behavior, to increasing population health and wellbe-ing through physical activity and to populations enjoying the benefits of physical activityas part of their everyday life. From the vision statements numerous strategic objectivesare highlighted. These objectives are presented under different sector headings includingbusiness/industry, education, healthcare, mass media, parks/recreation/ fitness/sport, pub-lic health, transportation/urban design/ community planning, volunteer and non-profit, andan “other” category. This supports the importance of following the HARDWIRED criteriain order to ensure that all potential partners are engaged in a strategic manner in order totackle the challenge of inactivity.
Similar findings are reported by the World Health Organization in their recentpolicy content analysis, “Promoting sport and enhancing health in European Union (EU)countries” (World Health Organization, 2011). Twenty-five national documents from15 EU member states were identified from a total of 130 documents (27 EU memberstates) as meeting the inclusion criteria. These were analyzed, and it was found that theywere issued mainly by government ministries (for example, education, culture and sport,health, welfare, or local government), had a specified timeframe (this varied from 2 to20 years) and gave some information on the policy development process (although thequality of this information was mixed, ranging from alluding to a consultation processthrough to a detailed account of all stakeholders and the approach taken to engage thesekey groups). They also had defined participation targets that covered the continuum fromelite sport to sport for all and to health enhancing physical activity. Target groups, settings,and implementation strategies were presented, for example, children were targeted inall strategies, mainly in the school setting and through physical education (p. 32). WHOhighlighted the Dutch strategy “Time for Sport” as an example of good practice for budgetallocation. Under its focus “Participation through Sport” it allocated a specific budget
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

100 C. B. Woods and N. Mutrie
for each target set, for example, “Education through sport and school,” one of six areasunder this focus was allocated a budget of C1.5 million per year for a total of five yearsto achieve its objectives (World Health Organization, 2011, p. 36). One critique by WHOwas that although most of the documents analyzed mentioned evaluation, the specificevaluation information provided along with measurable outcome indicators was varied andquite often absent. Adhering to a “HARDWIRED”criteria would stress the importance ofevaluation, and ideally the independent quality of this evaluation.
Will These Policies Help Educators?
We have already pointed out that the existence of global or national policies can help edu-cators argue for resources, provide evidence for approaches that are effective, and provide aframework for monitoring progress. However, the efficacy of such an intervention strategyis yet to be determined (Hoehner et al., 2008; Mowen & Baker, 2009). Evaluating whetheror not policy has been effective in this regard is not straightforward and change can beattributed to many causes. We will use examples from our own countries—Scotland andIreland—to show how different approaches, one based on policy, the other lack of policy,have potential impact for provision of physical education within the school setting.
In Scotland, a national policy was agreed by all political parties in 2003. The policywas entitled “let’s make Scotland more active.” The policy had a broad aim of increas-ing the proportion of people in Scotland leading physically active lives. In particular, thepolicy set a target for 2022 of 50% adults and 80% of children meeting the minimum lev-els of physical activity for health gain. Several priorities emerged including children andyoung people. One part of the policy suggested that all schools (from nursery to senior)should provide a minimum of two hours of quality physical education in curriculum timeeach week and adopt a “whole of school” approach to helping children achieve a minimumof 60 minutes of activity each day. In 2005, it was reported that less than 5% of schoolsachieved the minimum of two hours of physical education. However, in 2010 the percent-age of schools providing the two hours of physical education had risen to 50% (http://www.scotland.gov.uk/Topics/Education/Schools /HLivi /PEactivity). While it is difficult to saythat the policy caused this change in time spent in physical education, it is also difficultto see alternative explanations for the observed increase. The national policy for physi-cal activity in Scotland preceded a review of the whole school curriculum (including allsubjects, not just physical education or health education) and in forming our new approach“the curriculum for excellence” a health and well-being strand was informed by the need forphysical activity in general and also for quality physical education in primary and secondaryschools. Education Scotland has in turn supplied in-service courses and on line resourcesto help head teachers, class room teachers, and physical education teachers deliverthis health and well-being strand of the new curriculum (http://www.ltscotland.org.uk/learningteachingandassessment/curriculumareas/healthandwellbeing/index.asp). In thisway, education policy was influenced by global and national policy and appears tohave had a positive effect on the percentage of schools providing the minimum require-ment of two hours of physical education. To achieve this, more specialist physicaleducation teachers have been trained and more curriculum resources have been pro-vided. The policy was reviewed in 2009 by a panel of independent experts. The fullreport can be found at: http://www.healthscotland.com/uploads/ documents/9159-1150-HS%20PA%205yr%20Review%20Final.pdf. The conclusions from the review were thatthe policy was still relevant and the 2022 targets could be met if efforts were sustainedand refined. Refinements included more attention to segments of the population seen from
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 101
National Health Survey data to be making slow progress towards the 2022 targets. Twoparticular target groups were noted: older adults and adolescent girls. This re-statement ofthe policy and refinement of target groups may help deliver the increased physical activitygoals for Scotland and may also influence how schools tackle the low levels of activity foradolescent girls in particular. As a result of the review a summit was organized involvingeducators, local service providers, practitioners and academics to make suggestions on howto improve activity levels for adolescent girls within and beyond school (http://www.paha.org.uk/Resource/ teenage-girls-physical-activity-summit). This is another example of howeducators can benefit from physical activity policy.
In Ireland, no national physical activity policy exists. Consequently, a national visionfor physical activity with clear goals, a strategic plan of action, an identification ofresources, partners nor evaluation mechanisms exist. There are many policy documentswithin different government sectors that identify physical activity promotion as part oftheir agenda. The Ready, Steady, Play! A national play policy (National Children’s Office,2004) outlines the need “to plan for an increase in public play facilities and thereby improvequality of life of children living in Ireland, providing them with more quality play oppor-tunities” (p. 8). The Department of Transport’s policy for Ireland 2009–2020 encouragesschools to adopt “active travel plans,” advocates for “a strong cycling culture in the cities,towns, villages, and rural areas of Ireland” (Department of Transport, 2009, p. 42) andTeenspace: A national recreation policy—12–18 year olds has, as its second objective, the“need to develop increased opportunities for dance and physical activity, and tackle genderissues around provision in sport” (Office for the Minister of Children and Youth Affairs,2007). However, without a “clear stand along/single issue physical activity policy state-ment” (Bellew et al., 2008, p. 2) these related strands of physical activity policy embeddedwithin other agendas may be less effective. Without the backing of a national physicalactivity policy, within which there is a defined role for education (particularly physicaleducation) then it is more difficult to convince decision makers of its contribution, needand importance. In 2010, a working group was set up by the Health Services Executive(HSE) and its purpose was to provide the Department of Health and Children with an ini-tial draft national physical activity plan. Membership of this group included representativesfrom the sectors of Health, Transport, Education, Environment, Sport, local authorities, NonGovernmental Organizations and academics. It was chaired by the HSE. The academics onthe working group were invited from three different third level institutions in the Republicof Ireland and one from the North of Ireland to provide a whole island approach to thepromotion of physical activity. The academics represented the areas of sport and exercisescience, physical activity, and public health and physical education teacher education. Theirrole was to provide scientific information and to lead on the writing of the draft plan. Thisimportant advocacy opportunity, although outside the academic remit of research or teach-ing, provided a unique chance to ensure that current scientific information was availableto a key group of policy decision makers from a number of different government sectorsin Ireland. Information provided included the evidence base for why physical activity isan important public health issue, statistics on the prevalence of physical activity and inac-tivity in Ireland (and compared to other countries), advice on the recommended minimumamounts of physical activity necessary for health benefit and perspective on current capac-ity in physical education, sport, and physical activity and on the need for evidence-basedintervention in different areas was highlighted. The role of quality physical education wasclearly documented and is included in the draft plan, along with the need to provide chil-dren and young people with a broad range of opportunities to engage in physical activityoutside of school, recommendations relevant to other sectors are also present. The first draft
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

102 C. B. Woods and N. Mutrie
of the national physical activity plan is with the HSE, and it is hoped that it will influencethe writing of the current national public health policy by strengthening the inclusion ofphysical activity as a determinant of health. The challenge will be to ensure that it is cir-culated widely to all key stakeholders, for example physical education teachers, coaches,parents, architects, engineers, planners, urban designers, and so on, for consideration andfeedback prior to finalization, consistent with the HARDWIRED criteria. Upon completionof the consultation, an implementation plan will then need to be drawn up.
Conclusion
In conclusion, this paper has provided an overview of what a physical activity policyis, why it is important and key criteria that can influence the success of such a doc-ument. Recent physical activity policy documents have been referenced, and two casestudies discussed. The policy space that any country devotes to the physical activity needsof its citizens is varied; good policy does not guarantee better resources, but it has thepotential to influence practice through formal written codes, regulations or standards toguide choices. Consequently, policy has the potential to increase the likelihood that qual-ity physical education is offered to all children and young people, that opportunities tobe active are enhanced through urban design, planning, and transport policies that facili-tate active modes of travel, that national targets are set, monitored and evaluated ensuringaccountability is determined. Ultimately, a national or state physical activity policy hasthe potential to increase the likelihood that the physical, social and mental well beingthat can be achieved through regular health enhancing physical activity for all the pop-ulation is achieved. The role of the academic in this development is clear; they need tobe able to produce good scientific evidence—found in physical education, physiology,psychology, public health, planning and transport, etc.—into meaningful advice and rec-ommendations for the key policy makers in the various government sectors in order toensure that the potential of physical activity in the promotion of health (in its broadestsense) is realized.
Acknowledgments
This paper was presented at the Association Internationale des Ecoles Superieuresd’Education Physique [International Association for Physical Education in HigherEducation] International Conference hosted by the University of Limerick in June 2011.The main theme of the conference was “Moving People, People Moving” and this paperwas presented under the sub-theme of physical activity and health policies: implementationand implications within and beyond school. Professor Mutrie presented the keynote paper“Putting policy firmly on the physical activity agenda” and Dr. Woods provided a response,placing the issues raised in an Irish context. The session was chaired by Mr. Peter Smythfrom the Irish Sports Council.
References
Bellew, B., Schoppe, S., Bull, F. C., & Bauman, A. (2008). The rise and fall of Australian physicalactivity policy 1996–2006: A national review framed in an international context. Australia andNew Zealand Health Policy, 5(18), 1–10.
Bornstein, D. B., Pate, R. R., & Pratt, M. (2009). A review of the national physical activity plans ofsix countries. Journal of Physical Activity and Health, 6(S2), S245–S264.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

Physical Activity Policy 103
Bull, F., Bellew, B., Schoppe, S., & Bauman, A. (2004). Developments in national physical activitypolicy: An international review and recommendations towards better practice. Journal of Scienceand Medicine in Sport, 7(1), S93–S104.
Caspersen, C., Powell, K. E., & Christenson, G. (1985). Physical activity, exercise and physi-cal fitness: Definitions and distinctions for health-related research. Public Health Reports, 100,126–131.
Centers for Disease Control and Prevention (2003). Prevalence of physical activity, including lifestyleactivities among adults—United States, 2000–2001. MMWR, 5(32), 764–769.
Chief Medical Officers (2011). Start Active, Stay Active: A report on the physical activity for healthfrom the four home countries. London: UK Department of Health.
Currie, C. E., NiGabhainn, S., Godeau, E., Roberts, C., Smith, R., & Currie, D. (2008). Inequalitiesin young people’s health: HBSC international report from 2005–2006 survey.
Department of Health and Children (2009). The national physical activity guidelines for Ireland.Dublin: The Stationary Office.
Department of Transport (2009). Smarter Travel: A sustainable transport future. A new transportpolicy for Ireland 2009–2020. Dublin: Department of Transport.
Flegal, K., Carrol, M., Ogden, C., & Curtin, L. (2010). Prevalence and trends in obesity among USadults, 1999–2008. Journal of the American Medical Association, 303(3), 235–241.
Hardman, K. (2008). Physical education in schools: A global perspective. Kinesiology, 40, 5–28.Health Promotion Agency for Northern Ireland (1997). Physical activity: An investment in public
health. The Northern Ireland Physical Activity Strategy Action Plan 1998–2002 Belfast: HPANI.Heath, G. W., Brownson, R. C., Kruger, J., Miles, R., Powell, K. E., Ramsey, L. T., et al. (2006). The
effectiveness of urban design and land use and transport policies and practices to increase physicalactivity: A systematic review. Journal of Physical Activity and Health, 3, S55–S76.
Hoehner, C. M., Soares, S., Perez, D., Riberio, I. C., Joshu, C. E., & Pratt, M. (2008). Physical activityinterventions in Latin America: A systematic review. American Journal of Preventive Medicine,34, 224–233.
King, A. C., & Sallis, J. F. (2009). Why and how to improve physical activity promotion: Lessonsfrom behavioral science and related fields. Preventive Medicine, 49, 286–288.
Leyden, K. M., Reger-Nash, B., Bauman, A., & Bias, T. (2008). Changing the hearts and minds ofpolicy makers: An exploratory study associated with the West Virginia Walks Campaign. AmericanJournal of Health Promotion, 22(3), 204–207.
Mathers, C., Stevens, G., & Mascarenhas, M. (2009). Mortality and burden of disease attributable toselected major risks. Geneva: World Health Organization.
Ministry of Health and Care Services (2005). The Action Plan on Physical Activity 2005–2009.Working together for Physical Activity. Norway: Ministry of Health and Care Services.
Mowen, A. J., & Baker, B. L. (2009). Park, Recreation, Fitness and Sport Sector Recommendationsfor a more physically active America: A white paper for the United States National PhysicalActivity Plan. Journal of Physical Activity and Health, 6(S2), S236–S244.
Mutrie, N., & Woods, C. B. (2003). How can we get people to become more active? A problemwaiting to be solved. In J. McKenna & C. Riddoch (Eds.), Perspectives on Health and Exercise(1st ed., pp. 129–152). Basingstoke, Uk: Palgrave Macmillan.
National Children’s Office (2004). Read, Steady, Play! A national play policy Dublin: NationalChildren’s Office.
National Food Administration & National Institute of Public Health (2005). Background Materialto the Action Plan for Healthy Dietary Habits and Increased Physical Activity. Uppsala, Sweden:National Food Administration.
OECD (2010). Health at a Glance: Europe 2010. OECD Publishing. Retrieved from http://www.oecd.org/
Office for the Minister of Children and Youth Affairs (2007). Teenspace: A national recreation policyfor young people. Dublin: Minister for Children and Youth Affairs.
Pratt, M., Epping, J. N., & Dietz, W. H. (2009). Putting physical activity into public health: Ahistorical perspective from the CDC. Preventive Medicine, 49, 301–302.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014

104 C. B. Woods and N. Mutrie
Sallis, J., Owen, N., & Fisher, E. B. (2008). Ecological models of health behavior. In K. Glanz,B. K. Rimer, & K. Viswanath (Eds.), Health Behavior and Health Education. Theory, Researchand Practice (4th ed.), San Francisco, CA: Jossey-Bass.
Schmid, T., Pratt, M., & Witmer, L. (2006). A framework for physical activity policy research.Journal of Physical Activity and Health, 3, S20–S29.
Scottish National Physical Activity Task Force (2003). Let’s Make Scotland More Active: A Strategyfor Physical Activity. Edinburgh: Scottish Executive.
The Strategic Inter-Governmental Forum on Physical Activity and Health (2005). National PublicHealth Partnership, Be Active Australia: A Framework for Health Sector Action for PhysicalActivity 2005–2010. Melbourne, Australia: National Public Health Partnership.
U.S. Department of Health and Human Services (2008). Physical activity guidelines for Americans.Retrieved from http://www.health.gov/paguidelines/
UK Department of Health (2004). At least five a week: Evidence on the impact of physical activityand its relationship to health. A report from the Chief Medical Officer. London: Department ofHealth.
UK Department of Health (2009). Be Active. Be Healthy: A plan for getting the nation moving.London: Department of Health.
United Nations General Assembly. (2011). Political declaration of the High-level Meeting of theGeneral Assembly on the Prevention and Control of Non-communicable Diseases, p. 1–12.Retrieved from http://www.globalpa.org.uk/
World Health Organization (1986). The Ottawa Charter for Health Promotion. Retrieved fromwww.euro.who.int/pubrequest/
World Health Organization (2003). Health and development through physical activity and sport.Geneva, Switzerland: World Health Organization. Retrieved from www.euro.who.int/pubrequest/
World Health Organization (2004). Resolution WHA57.17. Global Strategy on Diet, Physical Activity,and Health. In: Fifty-seventy World Health Assembly, Geneva, 17–22 May 2004. Resolutionsand decisions, annexes. Geneva: World Health Organization. Retrieved from www.euro.who.int/pubrequest/
World Health Organization (2008). 2008–2013 Action Plan for the Global Strategy for the Preventionand Control of Noncommunicable Diseases. Geneva: World Health Organization. Retrieved fromwww.euro.who.int/pubrequest/
World Health Organization (2010a). Global Recommendations on Physical Activity for Health.Geneva: WHO. Retrieved from www.euro.who.int/pubrequest/
World Health Organization (2010b). Review of physical activity promotion policy developmentand legislation in European Union Member States (Rep. No. 10). Copenhagen: World HealthOrganization. Retrieved from www.euro.who.int/pubrequest/
World Health Organization (2011). Promoting sport and enhancing health in European Unioncountries: A policy content analysis to support action. Copenhagen: World Health OrganizationRegional Office for Europe. Retrieved from www.euro.who.int/pubrequest/
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
09:
15 0
8 O
ctob
er 2
014