Embed Size (px)
Citation preview
Pulmonary embolism:Risks,Diagnosis,
Prevention & Treatment

Pulmonary Embolism
• Blockade of pulmonary artery/branches by a substance travelling from elsewhere through the bloodstream

• Thrombotic• Non-thrombotic
– Fat– Amniotic fluid– Air– Tumor tissue– Foreign body

Variable presentation:
– Massive (5%)
– Sub massive (25%)
– Non-massive (70%)

Epidemiology
• 1 in 1000 cases per year ! (US)
• PE present 60-80% with DVT !>half asymptomatic thou
• 79% of patients with PE have DVT

Pathophysiology
• DVT and PE occur as a continuum
• Virchow’s Triad: (1856)
– Blood flow changes (stasis,turbulence)
– Vessel injury
– Hpercoagulability

(Serotonin,thromboxane)

Predisposing factors
– Age (>60 yrs)
– history of previous VTE
– active cancer
– Prolonged bed rest, such as heart or acute respiratory failure, obesity, neurological disease
– congenital or acquired thrombophilia
– hormone replacement therapy
– oral contraceptive therapy
– Pregnancy
– Surgery ( knee surgery, major general surgery)
– Trauma ( hip fracture, spinal cord injury)
– Central venous line
– Chemotherapy

Inherited Risk Factors
• Protein C resistance (Factor V Leiden)
• -Antithrombin III deficiency
• -Protein C deficiency
• -Protein S deficiency
• -Hyperhomocystinemia (? Acquired due to vit.B1/B6 deficiency)
• Antiphospholipid antibody
The investigation of states in theacute phase of thromboembolic disease must necessarily include checks for: a) Factor V Leiden, becauseit is the most common anomaly responsibleusing polymerase chain reaction; b) Hyperhomocysteinaemiamay usually be treated completely and quickly by the administration of vitaminsB1and B6; c) Lupus anticoagulant, because if it is present it requires intensive and immediate therapy. Inthe acute phase it is not necessary to check proteinC, protein S, or because theyare rarely deficient, and secondly because their levels

Diagnosis

Symptoms
– Dyspnoea– Chest pain (pleuritic, substernal) – Cough – Hemoptysis – Syncope

Physical Signs
• Tachypnea (>16/min) 96%• Rales 58%• Accentuated S2: 53%• Tachycardia : 44 %• Fever (>37.80C): 43%• S3 or S4 gallop: 34 %• Signs/symptoms suggesting thrombophlebitis 32%• Leg edema : 24 %• Murmur : 23 %• Cyanosis: 19 %

PE Wells scoreClinical feature Points
Clinical signs and symptoms of DVT (minimum of leg swelling and pain
with palpation of the deep veins)3
An alternative diagnosis less likely than PE 3
Heart rate > 100 beats per minute 1.5
Immobilisation more than 3 days/surgery in previous 4 weeks 1.5
Previous DVT/PE 1.5
Haemoptysis 1
Malignancy (on treatment/treated in the past 6 months/palliative) 1
Clinical probability simplified scores
PE likely More than 4
PE unlikely 4 or less
a Adapted with permission from Wells PS et al. (2000) Derivation of a simple clinical model to categorize patients’
probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thrombosis and
Haemostasis 83: 416–20

Revised Geneva Scoring system
• RISK FACTORS• Age >65 1• Previous DVT/PE 3• Surgery/ # of lower limg < 1 mnth 2• Malignancy 2• SYMPTOMS• Unilateral lower limb pain 3• Hemoptysis 2• SIGNS• HR (75-94) 3• HR (>95) 5• Pain/unilateral leg edema 4
0-3 low,4-10 intermediate,>11 high. 25 max

Investigations
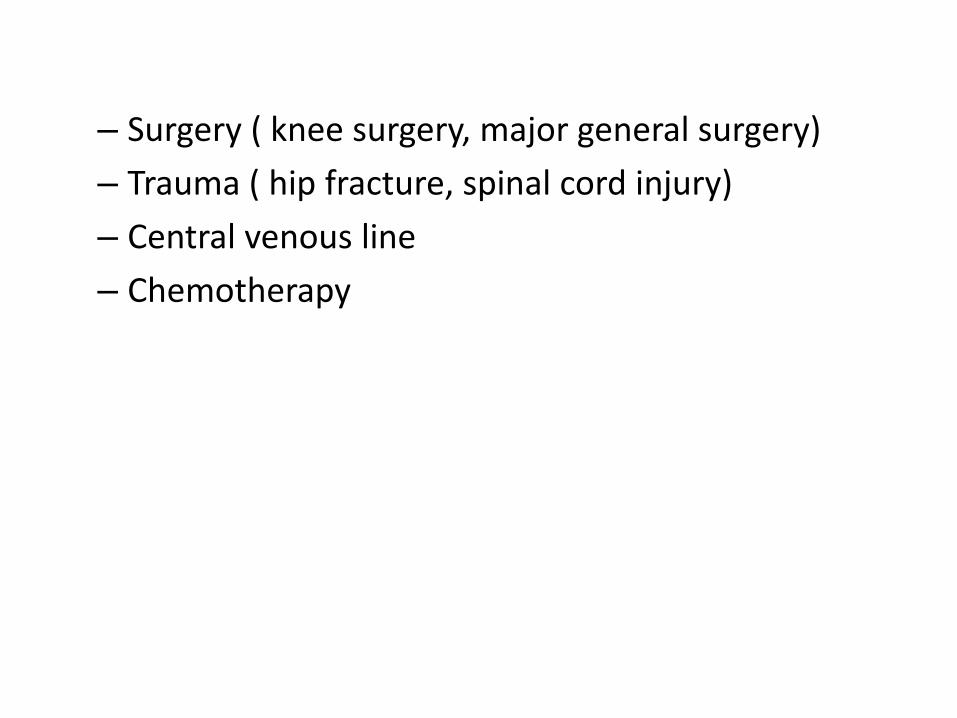
• CXResp. helpful in ruling out other causes (pneumonia/thorax)
• ECG– S1Q3T3 (insensitive without clinical symptom)– inversion of T waves in leads V1–V4– RAD, right bundle-branch block– AF

• ABGs
• Nonspecific
• hypoxemia,hypocapnia & resp. Alkalosis ↑A-a gradient
• However,Low PO2 has strong PPV for pts without respi. diseases

• D-dimer – Fibrin degradation product– elevated in the presence of thrombus.- has a negative predictive value. - a sensitivity for venous thromboembolism of 95-97% and a specificity of 45%. - D-dimer < 500 ng/mL using ELISA provides strong evidence against venous thromboembolism.

• Ischemia modified Albumin (IMA)
• Albumin produced during ischemia
• 93 % sensitive, 75% Specific for PE combined with scoring systems
• ↑ in MI, ACS

• CT - large, central PE
• PUL. ANGIOGRAPHY– emboli as small as 1 to 2 mm
• Lung V/Q Scanning • The perfusion scan defect indicates absent or decreased
blood flow due to PE. -Ventilation scans improve the specificity of the perfusion scan. - A high probability scan is defined as two or more segmental
perfusion defects in presence of normal ventilation scan.

Safe exclusion of pulmonary embolism using the Wells rule and qualitative D-dimer testing
in primary care: prospective cohort studyBMJ 2012; 345 doi
• Abstract Geert-Jan Geersing,• Design Prospective cohort study.• Setting Primary care across three different regions of the Netherlands (Amsterdam, Maastricht, and
Utrecht).• Participants 598 adults with suspected pulmonary embolism in primary care.• Interventions Doctors scored patients according to the seven variables of the Wells rule and carried
out a qualitative point of care D-dimer test. All patients were referred to secondary care and diagnosed according to local protocols. Pulmonary embolism was confirmed or refuted on the basis of a composite reference standard, including spiral computed tomography and three months’ follow-up.
• Main outcome measures Diagnostic accuracy (sensitivity and specificity), proportion of patients at low risk (efficiency), number of missed patients with pulmonary embolism in low risk category (false negative rate), and the presence of symptomatic venous thromboembolism, based on the composite reference standard, including events during the follow-up period of three months.
• Results Pulmonary embolism was present in 73 patients (prevalence 12.2%). On the basis of a threshold Wells score of ≤4 and a negative qualitative D-dimer test result, 272 of 598 patients were classified as low risk (efficiency 45.5%). Four cases of pulmonary embolism were observed in these 272 patients (false negative rate 1.5%, 95% confidence interval 0.4% to 3.7%). The sensitivity and specificity of this combined diagnostic approach was 94.5% (86.6% to 98.5%) and 51.0% (46.7% to 55.4%), respectively.
• Conclusion A Wells score of ≤4 combined with a negative qualitative D-dimer test result can safely and efficiently exclude pulmonary embolism in primary care.

Treatment


• Hemodynamic and respiratory support– Rest & Oxygen– Inotropic support +/-– Mechanical ventilation

Anticoagulation
Unfractionated Heparin– catalyzes the inactivation of thrombin and factor Xa by
antithrombin– an initial bolus of 80 IU/kg IV, followed by a continuous
infusion of 18 IU/kg/hr IV. – Rate of the heparin infusion adjusted so that the aPTT is
1.5-2.5 times the control value.

• LMWH
– inactivates factor Xa , minimally prolongs aPTT
– does not require monitoring of its anticoagulant effect (predictable dose-response relationship)
– lower risk of bleeding complications and thrombocytopenia.
– less protein C and S inhibition, less complement activation, and a lower risk of osteoporosis
– Enoxaparin- 1 mg/kg SC BD or 1.5 mg/kg OD
• Warfarin
started after therapeutic heparinization.
o Oral anticoagulant inhibits reduction of vit K to its active form depletion of vit K dependent clotting factors (2,7,9,10)
o difficult dosing, frequent monitoring, notorious interaction with other drugs/food

• Direct factor Xa inhibitors• predictable anticoagulation• no need for dose adjustments and routine coagulation monitoring
• Rivaroxaban, Apixaban

• Thrombolysisstreptokinase, Urokinase, rTPA
o Massive PE
o Hemod. Unstability, Circulatory shock

• Venous filter (IVC filter)– contraindications for anticoagulant (active haemorrhage, endangered
haemorrhage following severe brain injury or craniotomy)
– repeated episodes of PE occur despite anticoagulant therapy
• Pulmonary embolectomyfailed/contraindicated thrombolysis

Anesthetic concerns
• Maintain organ perfusion and avoid myocardial depression
• Avoid
– arterial hypoxemia,
– systemic hypotension
– pulmonary hypertension
– Histamine releasing NMBD

Amniotic fluid embolism
• amniotic fluid, fetal cells, hair, or other debris enters the mother's blood stream via the placental bed of the uterus and trigger an allergic reaction
• three prerequisites:
• Ruptured membranes (a term used to define the rupture of the amniotic sac
• Ruptured uterine or cervical veins
• A pressure gradient from uterus to vein











