Embed Size (px)
Citation preview
Science at the heart of medicine
Pulseless Oximetry
Thomas K Aldrich, MD Professor of Medicine, Pulmonary Division, Albert Einstein College of Medicine and Montefiore Medical Center [email protected] | 914.262.8855 Co-investigators: Sean Stoy, MD; Pragya Gupta, MD; Evan Lipsitz, MD; Anthony Carlese, MD; Daniel Goldstein, MD
US provisional patent application no. 61/992,292 (May 13, 2014)
Health & Bio Technology Summit | November 6, 2014

| 2
Science at the heart of medicine
PULSE OXIMETRY
Science at the heart of medicine
An indispensable tool in almost all Health Care Venues
$600-‐700m global market as of 2014. Will double by the end of the decade
n Noninvasive measurement of arterial blood oxygenaGon. • Quick • Cheap • Accurate without needing
calibraGon • Detects potenGally life-‐
threatening condiGon • Saves paGents from painful
procedures (ABGs) n But, does not work when pulse is weak or absent
North American Pulse Oximeter Market (Data and projec.ons from Micromarket Monitor 7/2014)
$0
$200
$400
$600
$800
2005 2010 2015 2020
Mill
ions
Inclusion of Global markets would drive these esGmates up at least 50% (Data from Daedal Research 11/2013)

| 3
Science at the heart of medicine
Unfortunately, current pulse oximeters DO NOT work for those who have
weak or absent pulses
Science at the heart of medicine
Two common causes of pulselessness:
Peripheral Vascular Disease: very common in older age groups, so likely to increase among paGents needing monitoring in the future. (NIH 2012)
Con.nuous-‐flow leF ventricular assist devices (LVADs): Increasing in prevalence in US (PlugMed 2012)
Pulse Oximetry Failure is not uncommon
§ Fails in 2.5%, not a trivial problem, considering the 1 billion office visits, 130 million ER visits, and 100 million surgical procedures per year (CDC esGmates)
§ The sickest paGents-‐-‐-‐those most in need of monitoring-‐-‐-‐had 7% failure rate.
Low High

| 4
Science at the heart of medicine
To solve this problem, we created and tested a new “Pulseless” Oximetry technique
Science at the heart of medicine
§ 5 to 10 second occlusion of radial and ulnar arteries § Abrupt release § Analysis of photoplethysmograms during the ~1 second after release. § The details of our proof of concept study are shown in a poster available
for view during the break.
§ To date, we have used manual occlusion of the arteries, but occlusion could be automated.
0
20000
40000
60000
80000
0 5 10 15 20 25
Ligh
t lev
el (a
rbitr
ary
units
)
Time (sec)
Raw photoplethysmograms
Red (660nm)
Infrared (905nm)

| 5
Science at the heart of medicine
Conceptual diagram of “Pulseless” Oximeter
Science at the heart of medicine
§ The device could funcGon as a standard pulse oximeter, w/ or w/o the bracelet applied to the wrist. § When pulselessness is detected, pulseless oximetry measurements would be carried out. § The screen would display photoplethysmograms, allowing verificaGon of venous oualow during occlusion and arterial inflow upon release.
Conceptual picture of device
Cross-‐sec.onal detail of occluder
bracelet
Occluder bracelet Occluder controller and
oximeter screen
Pulse oximeter probe Adjustable-
size bracket
Pneumatic or solenoid arterial occluder
Pneumatic or solenoid arterial occluder
wrist Ventral
Dorsal

| 6
Science at the heart of medicine
§ 14 studies in 5 normal subjects breathing various oxygen levels.
§ Good correlation of Red/IR ratios with measured SpO2.
Preliminary results
Calibration Curve LVAD Patients
§ 4 LVAD patients, one studied twice § Good correlation of Red/IR ratios
with measured SaO2.
Science at the heart of medicine
y = -26.726x + 111.45 R² = 0.97472
85
90
95
100
0.4 0.6 0.8 1
SpO
2 (%
)
Red/Infrared changing attenuance ratio by pulseless technique
NS #1 NS #2 NS #3 NS #4 NS #5
| 7
Science at the heart of medicine
Conclusions
• Pulseless oximetry can measure arterial oxygenation noninvasively. • Additional wavelengths could allow carboxy- & methemoglobins to
be measured. • The device could function as a standard pulse oximeter until
pulselessness is detected. > Opportunity to claim a large share of the soon-to-be $1 billion world-
wide pulse oximeter market. • The next step is to partner with a biotechnology company to:
> Build and test a fully-functional prototype > Apply for Regulatory approval > Manufacture and market the device
Science at the heart of medicine

| 8
Science at the heart of medicine
Contact Details
• Commercial/licensing interest:
Ece Auffarth, Ph.D. Contract and Licensing Manager Office of Biotechnology Albert Einstein College of Medicine Phone (718) 430-8558 Fax: (718) 430-8938 Email: [email protected] [email protected]
Science at the heart of medicine
Science at the heart of medicine
Appendix
Health & Bio Technology Summit | November 6, 2014
Pulseless Oximetry

| 10
Science at the heart of medicine
Basis of standard pulse oximetry
Science at the heart of medicine
• Transilluminate a fingertip with at least 2 wavelengths, e.g., 660nm (red) and 905nm (infrared).
• Determine absorbance of each wavelength by pulsing arterial blood (and not other components of the fingertip) by measuring changing transmission during pulses
• Convert to absorbance (really attenuance).
• Calculate ratio of attenuance of red to attenuance of infrared
660nm (red)
905nm (infrared)
Without a discernable pulse, standard pulse oximetry fails
From Weiben 1997
From Weiben 1997
| 11
Science at the heart of medicine
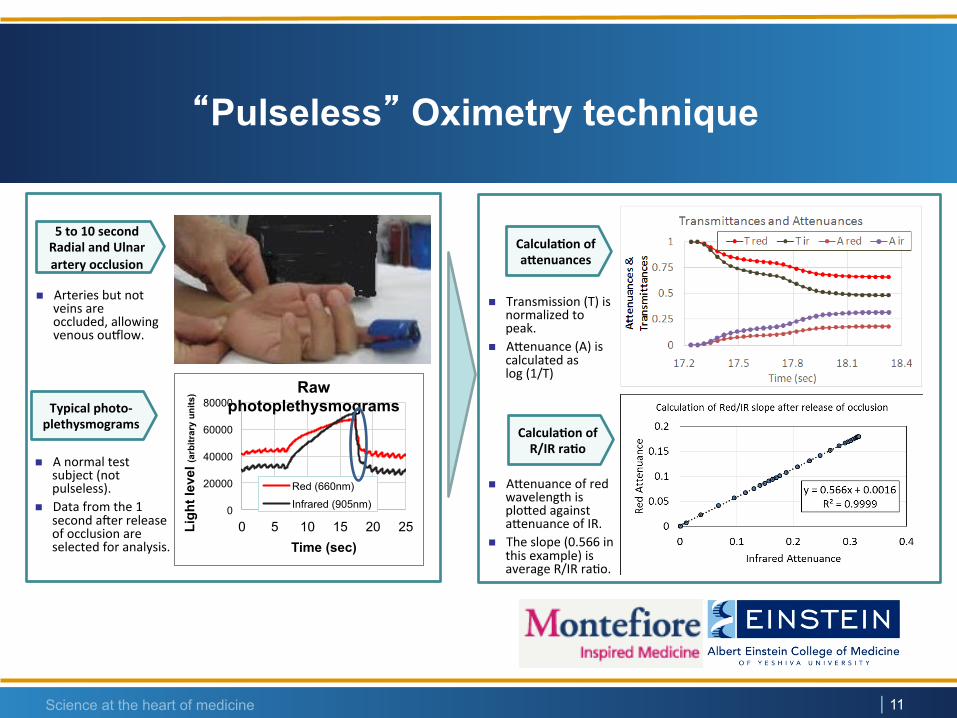
5 to 10 second Radial and Ulnar artery occlusion
Typical photo-‐plethysmograms
n A normal test subject (not pulseless).
n Data from the 1 second aeer release of occlusion are selected for analysis.
Calcula.on of aQenuances
Calcula.on of R/IR ra.o
n Transmission (T) is normalized to peak.
n Agenuance (A) is calculated as log (1/T)
n Agenuance of red wavelength is ploged against agenuance of IR.
n The slope (0.566 in this example) is average R/IR raGo.
n Arteries but not veins are occluded, allowing venous oualow.
0
20000
40000
60000
80000
0 5 10 15 20 25 Ligh
t lev
el (a
rbitr
ary
units
)
Time (sec)
Raw photoplethysmograms
Red (660nm)
Infrared (905nm)
“Pulseless” Oximetry technique
Science at the heart of medicine

| 12
Science at the heart of medicine
An example of the technique in an LVAD patient
§ Five sequential radial and
ulnar occlusions and releases in one LVAD patient.
§ Measured SaO2 was 99.5% by COoximetry.
§ Estimated SaO2 using our technique was 97.5%.
§ So far, we have studied four LVAD patients.
0
10000
20000
30000
0 20 40 60 80 100 120 140 Ligh
t lev
el (a
rbitr
ary
units
)
Time (seconds)
LVAD
Red IR
Science at the heart of medicine