Embed Size (px)
DESCRIPTION
PULMONARY REHABILITATION IN RESTRICTIVE PULMONARY DISEASES. Doç. Dr. Pınar Ergün Atatürk Göğüs Hastalıkları ve Göğüs Cerrahisi Eğitim Araştırma Hastanesi. Presentation plan. Rationals ? Interstitial Lung Diseases Chest Wall Disorders Neuromuscular Disorders Obesity- related Disorders. - PowerPoint PPT Presentation
Citation preview

PULMONARY REHABILITATION IN RESTRICTIVE PULMONARY DISEASES
PULMONARY REHABILITATION IN RESTRICTIVE PULMONARY DISEASES
Doç. Dr. Pınar ErgünAtatürk Göğüs Hastalıkları ve
Göğüs Cerrahisi Eğitim AraştırmaHastanesi

Rationals ?
Interstitial Lung Diseases Chest Wall Disorders Neuromuscular Disorders Obesity- related Disorders
Disease specific approaches ?
Presentation planPresentation plan

Key Considerations
Patient selection
Multidisciplinary
team
Special equipments
Individual goals
Rationals for Pulmonary Rehabilitation ?
Rationals for Pulmonary Rehabilitation ?
•Interstitial lung disease•Chest wall disoders•Neuromuscular disorders•Obesity related respiratory disorders

Restrictive Pulmonary Diseases
Restrictive Pulmonary Diseases
Muscle disfunctionNutrition Skelatel Cardiovascular Psychosocial
Exercise intoleranceSymptoms
Disability + Impaired Quality of Life
The Rationale for PR (II)
Complex treatment interventions often requiredo Immunosuppressive medicationso CPAP/BIPAP- acclimatization, training,
coaching, reassuranceo Transplantationo Mechanical ventilation/end of life decisions
Limited time for patient education and training with self-management strategies in the routine clinical setting


Pulmonary Rehabilitation is Effective
for the Non-COPD Patients !
Rationale-III

INTERSTITIAL LUNG DISEASES
IPF Sarcoidosis Ocupational lung diseases Hypersensitivity pneumonia Drug induced Collagen vascular diseases ARDS BOOP
PULMONARY REHABILITATION
PULMONARY REHABILITATION

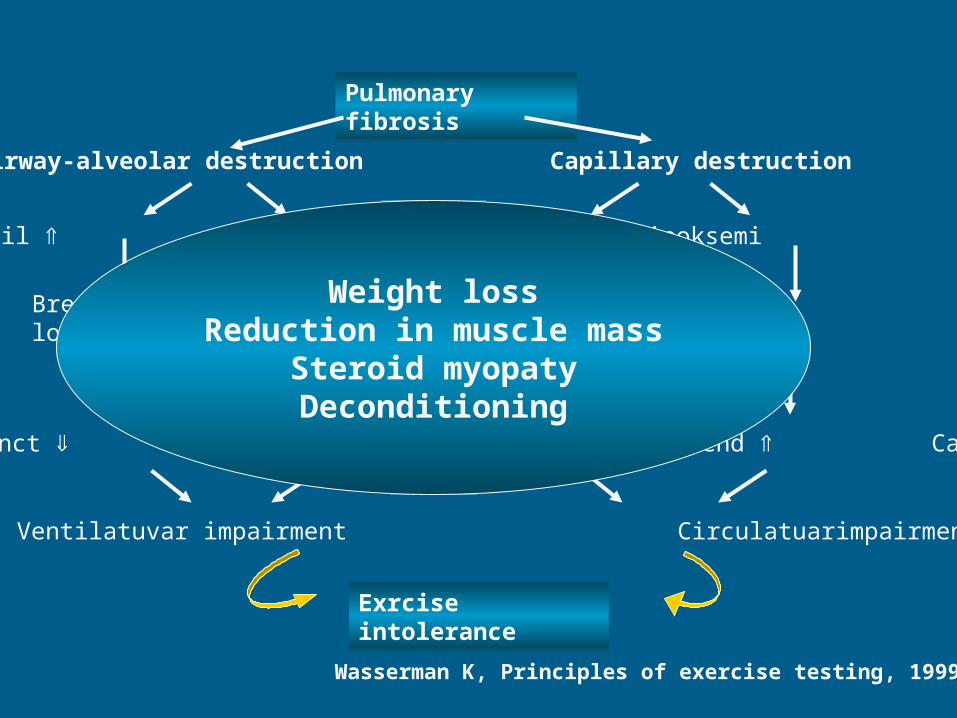
Pulmonary fibrosisPulmonary fibrosis
Airway-alveolar destruction Capillary destruction
Elastic recoil Vd/Vt Hypoxemia PVR
Breathing workload Left vent pre load
Vent. funct Vent. demand CO demand Cardiac funct
Ventilatory impairment Circulatory impairment
Exrcise intoleranceExrcise intolerance
Wasserman K, Principles of exercise testing, 1999
Pulmonary fibrosisPulmonary fibrosis
Airway-alveolar destruction Capillary destruction
Elastic recoil Vd/Vt Hipoksemi PVR
Breathing workload Left vent pre load
Vent. funct Vent. demend CO demend Cardiac funct
Ventilatuvar impairment Circulatuarimpairment
Exrcise intoleranceExrcise intolerance
Wasserman K, Principles of exercise testing, 1999
Weight lossReduction in muscle mass
Steroid myopatyDeconditioning

Chest 2005;127:2028-33
Improvement in muscle function leads to increase in
exercise tolerance

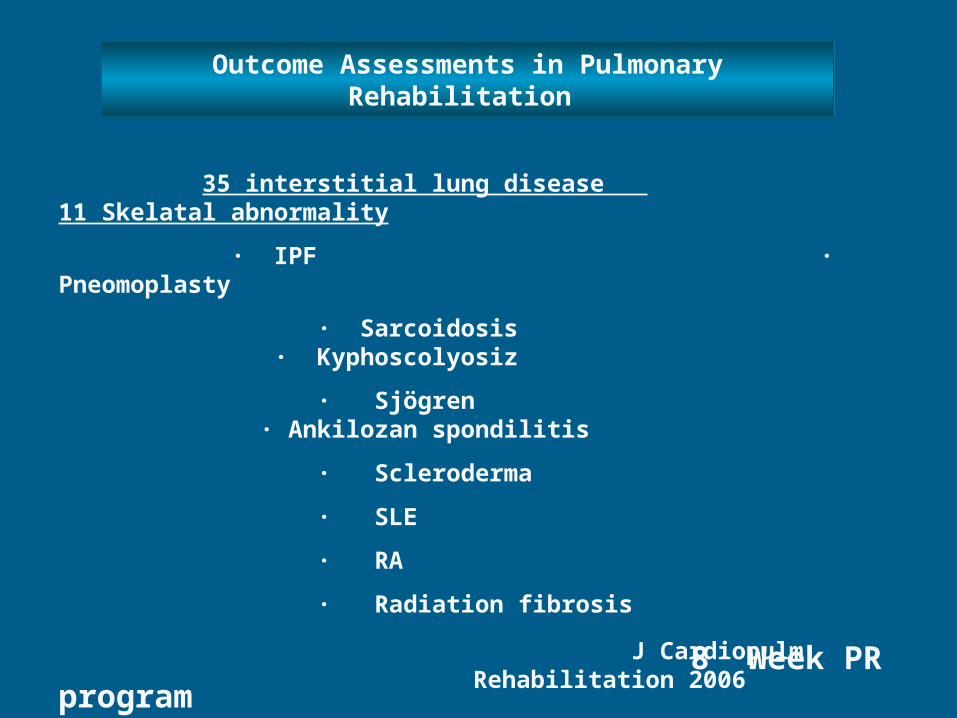
35 interstitial lung disease 11 Skelatal abnormality
∙ IPF ∙ Pneomoplasty
∙ Sarcoidosis ∙ Kyphoscolyosiz
∙ Sjögren ∙ Ankilozan spondilitis
∙ Scleroderma
∙ SLE
∙ RA
∙ Radiation fibrosis
8 Week PR program
J Cardiopulm Rehabilitation 2006
Outcome Assessments in Pulmonary Rehabilitation
Outcome Assessments in Pulmonary Rehabilitation

Outcome assessment in pulmonary rehabilitation
Exercise endurance↑
HRQL↑
Hospital addmitions ↓
J Cardiopulm Rehabilitation 2006

Disease specific programs !

PULMONARY REHABILITATION
PULMONARY REHABILITATION
CHEST WALL DISORDERS NEUROMUSCULAR DISEASE
CHEST WALL DISORDERS NEUROMUSCULAR DISEASE

RATIONALS ?RATIONALS ?
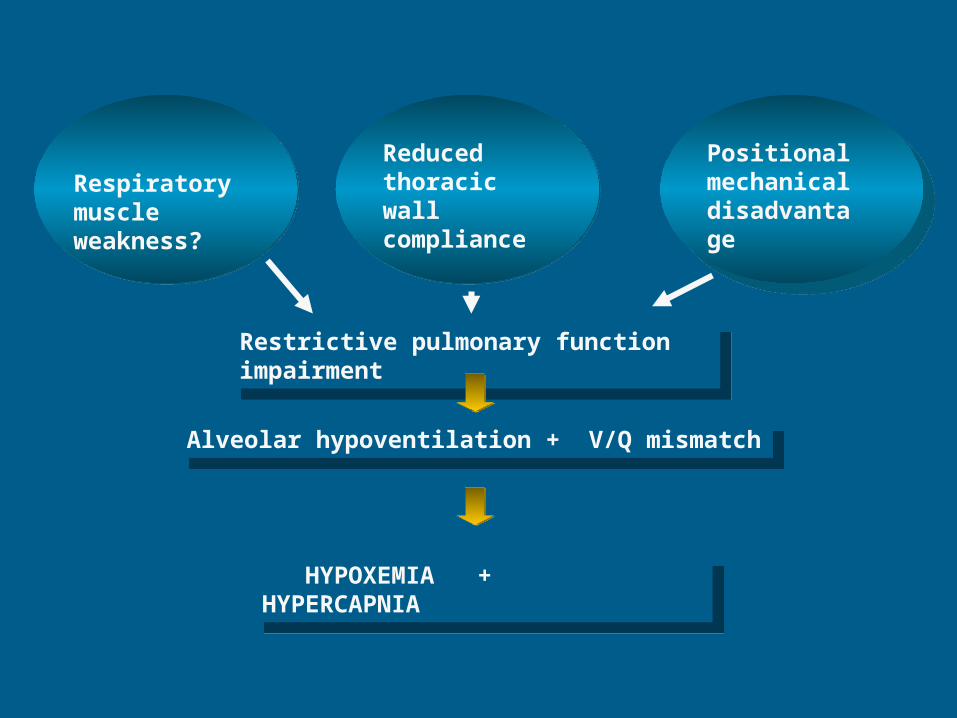
Respiratory muscle weakness?
Reduced thoracic wall compliance
Positional mechanical disadvantage
Restrictive pulmonary function impairment
Restrictive pulmonary function impairment
Alveolar hypoventilation + V/Q mismatchAlveolar hypoventilation + V/Q mismatch
HYPOXEMIA + HYPERCAPNIA
HYPOXEMIA + HYPERCAPNIA

Respiratory muscle weakness ?
Reduced thoracic wall compliance
Positional mechanical disadvantage
Restrictive pulmonary function impairment
Restrictive pulmonary function impairment
Alveolar hipoventilation + V/Q mismatchAlveolar hipoventilation + V/Q mismatch
HYPOXEMIA + HYPERCAPNIA
HYPOXEMIA + HYPERCAPNIAReduction in exercise toleranceReduction in exercise tolerance
NIPPVRMT
NIPPVRMT
SYMPTOMSRapid shallow breathingDyspnea
Peripheral muscle weakness

Internal medicine 2006
• VO2 peak ↑ (13.6±2.8, 14.8 ± 2.8)
• 6 MWD↑ (399±62, 467±65)

MRC ADL 6 DYT
6DYT
Chest 2003;123:1988-95
Pulmonary rehabilitation is effective in symptomatic
patients with Post TB
Pulmonary rehabilitation is effective in symptomatic
patients with Post TB

Problems faced
Respiratory muscle weakness
Peripheral weakness
Anatomical changes
• Reduced tidal volumes• Reduced lung
compliance• Ineffective cough• General fatigue• Decreased mobility• Positioning limitations• Possible impaired
swallowing and increased risk of aspiration
Faced Problems

• Reduce work of breathingIncrease tidal volumes and maintain lung
compliance
• Improve secretion clearance and effectiveness of cough• Maximise independence• Optimise quality of life
AIMS PR
NIMV
Breathing exercise

•
Harms et al. J Appl Physiol 1997; 1573-1583
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5
PS
PAV
CPAP
SHAM
Time Bianchi L, et al, ERJ, 1998
BORG
•Breathing work rate increase induce reductions in VO2 demand for peripheral muscles•Reduction in work load of respiratory muscles serve for peripheral muscles

Short-Term Effect of Nasal Intermittent Positive-Pressure Ventilation in Patients with Restrictive Thoracic DiseasePınar Ergün, Gülümser Aydın, Ülkü Yılmaz Turay, Yurdanur Erdoğan, Atalay Çağlar, Çiğdem Biber
Respiration 2002;69:303-308
ATS dispnea score:
2.5 ± 0.9’-1.6 ± 0.4 (p < 0.01)
6MWD 320.66 ± 93.56 to 382.41 ± 121.20 m
(p < 0.05)

Respiratory Muscle TrainingRespiratory Muscle Training
SkoliosisCyphosisCyphoskoliosis
Changes in AirwayResistance (?)
Physiopathology
Changes in muscle length
Changes in Compliance
Increased DemandsNutrients and O2
Nutrients and O2 Delivery
can be compromised
Changes in Chest Wall Changes in Chest Wall

Chest Wall Deformities & RM Training
Few studies
RM training appears to improve - Lung function, dyspnea & exercise toleranceEffects on the disease time-course: unknown
Few studies
RM training appears to improve - Lung function, dyspnea & exercise toleranceEffects on the disease time-course: unknown
RestTraining
Respiratory Muscle TrainingRespiratory Muscle Training

Amyotrophic Lateral SclerosisMultiple SclerosisSpine Cord injuryMiasthenia GravisDuchenne’s Muscular DystrophyPost-polio SyndromeGuillain-Barré SyndromeMyotonic Dystrophy (Steinert’s Disease)
Changes in AirwayResistance (?)
Physiopathology
Inefficiency of Muscles
Changes in Compliance
Increased DemandsNutrients and O2
Nutrients and O2 Delivery
can be compromised
Changes inThorax Geometry
RESPIRATORY MUSCLE RESPIRATORY MUSCLE TRAININGTRAININGRESPIRATORY MUSCLE RESPIRATORY MUSCLE TRAININGTRAINING
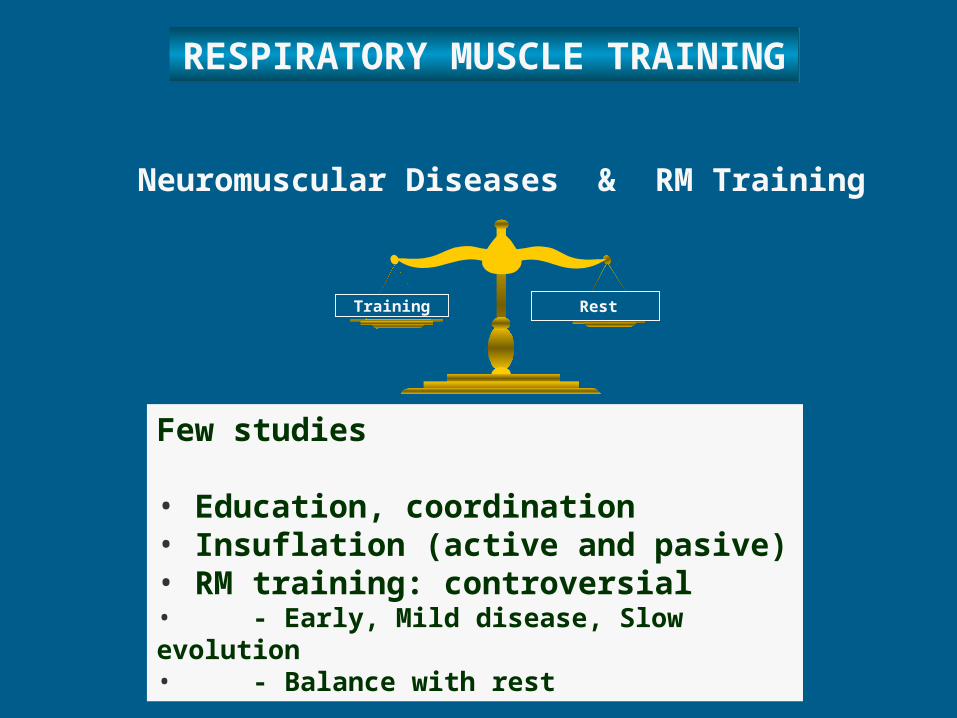
Neuromuscular Diseases & RM Training
Few studies • Education, coordination• Insuflation (active and pasive)• RM training: controversial • - Early, Mild disease, Slow evolution• - Balance with rest
RestTraining
RESPIRATORY MUSCLE TRAINING
RESPIRATORY MUSCLE TRAINING

Results: Intermittant-RMT is effective in generalized MG patients in improving respiratory muscle force and patern,endurance.
Chest 2005;128:1524-30
Chest 2001;120:765-69
PULMONARY REHABILITATION; is indicated in ALL patients with chronic respiratory diseases who is sypmtomatic and whose health related quality of life is impaired

Patient AssessmentExerciseEducationPsychosocial/Nutritional
interventionOutcomes measurement
Core Components of PR for the “Non-COPD” Patient
Core Components of PR for the “Non-COPD” Patient

CPET: -identify exercise factors contributing
to symptoms and limitation
-formulate the exercise prescription
-Identify pulmonary vascular or cardiac limitations and/or need for supplemental O2
-Incremental exercise to high intensity NOT recommended for known severe pulmonary HTN or degenerative neuromuscular disease
Asses candidacy for inpatient PR
Special Considerations in Patient Assessment

Patient AssessmentExercise trainingEducationPsychosocial/Nutritional
interventionOutcomes measurement
Core Components of PR for the “Non-COPD” Patient
Core Components of PR for the “Non-COPD” Patient

DISEASE SPECIFIC CONSEDERATOIN IN EXERCISE TRAINING (I)
Interstitial lung disease;
Pacing and energy conservation techniques
Slow and deep breathing Adequete oxygenation

Neuromuscular and Chest wall disease Maintain conditioning, avoid fatigue Consultation with neurologist/physiatrist Low intensity aerobic/water-based exercise Shorter, more frequent exercise sessions Emphasis on optimizing functional status Acclimatization to non-invasive ventilation
Disease-specific Considerations in Exercise Training (II)

Obesity related respiratory diseases
Strength and endurans exercise training/ Upper and Lower extremity Consider low-impact water-based exerciseBariatric equipment may be needed
Cardiac and musculo skeletal intervention before enrollment
Disease-specific Considerations in Exercise Training
(III)

Aerobic and Strength Training No evidence-based guidelines for exercise
prescription or training Mode, intensity and duration individualized
to patient ability and need using resources available
Age- and interest- specific modes
oxygen saturation > 90% Maintain Meet metabolic needs, avoid
anaerobic metabolism and exercise-induced increased PA pressure
o Test O2 saturation using patients’ own portable system
EXERCISE TRAINING

Patient AssessmentExerciseEducationPsychosocial/Nutritional
interventionOutcomes measurement
Core Components of PR for the “Non-COPD” Patient
Core Components of PR for the “Non-COPD” Patient

EDUCATION:EDUCATION: PR program staff: Knowledge of physiologic basis of exercise/functional
impairment, symptoms and available therapies for different disorders
PATIENT and FAMILY Nature and expected course of disease Physiologic basis of symptoms an exercise limitations Rational for and proper use of supplemental oxygen Pulmonary drainage technigues Nutrition Recognition of symptoms and sings of secondary
infection Prevention strategies Coping techniques for assistance in managing anxiety
and depression Training options for and outcomes of mechanical
ventilation

DISEASE SPECIFIC PROGRAM MANAGEMENT
DISEASE SPECIFIC PROGRAM MANAGEMENT
Ensure patient safety,individual goals Individual education sessions may be
needed Written and video educational materials
Assess outcomes acording to goalsIndividual, disease specific
approaches is necessaryIndividual, disease specific approaches is necessary
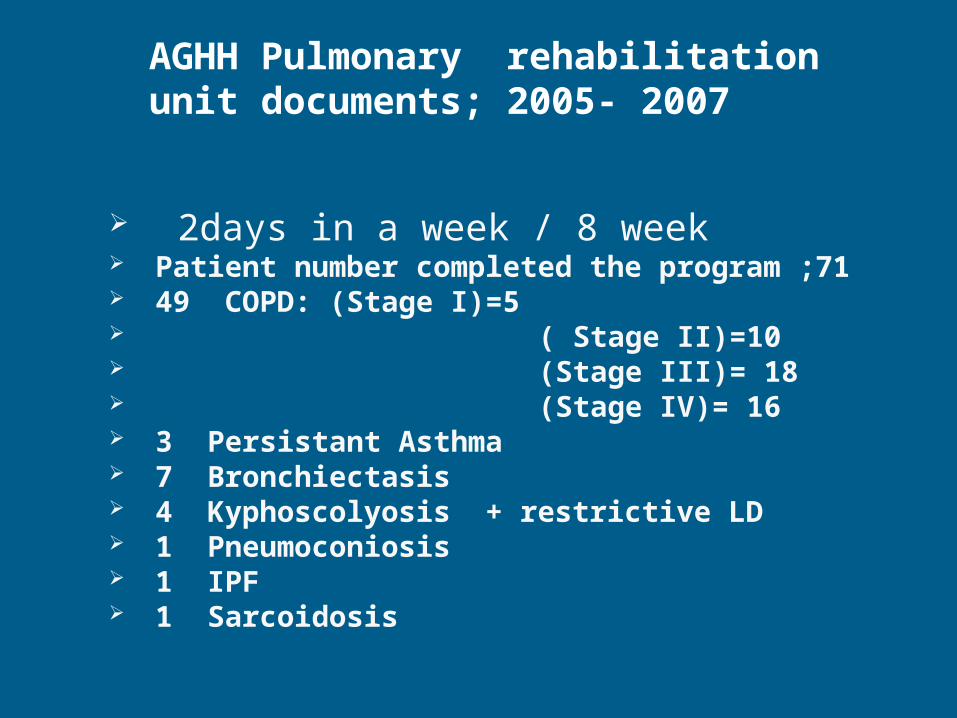
2days in a week / 8 week Patient number completed the program ;71 49 COPD: (Stage I)=5 ( Stage II)=10 (Stage III)= 18 (Stage IV)= 16 3 Persistant Asthma 7 Bronchiectasis 4 Kyphoscolyosis + restrictive LD 1 Pneumoconiosis 1 IPF 1 Sarcoidosis
AGHH Pulmonary rehabilitation unit documents; 2005- 2007

0
1
2
3
4
5
6
KO
AH
1
KO
AH
2
KO
AH
2
KO
AH
2
KO
AH
2
KO
AH
2
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
3
KO
AH
4
KO
AH
4
KO
AH
4
KO
AH
4
KO
AH
4
KO
AH
4
KO
AH
4
KO
AH
4
Bro
nşie
ktaz
i
Bro
nşie
ktaz
i
Bro
nşie
ktaz
i
Res
trik
tif
Res
trik
tif
Ast
ım
Ast
ım
MRCönce
MRCsonra
PR Outcomes/DISPNEA

0
5
10
15
20
25
30
35
40
45
KOAH1 KOAH2 KOAH3 KOAH3 KOAH4 KOAH4 KOAH4 Restriktif Astım
Endurans sonra
Enduransönce
PR Outcomes/ EXERCISE TOLERANCEEn
du
ran
s/D
akik
a

0
20
40
60
80
100
120
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
CRDQönce
CRDQ sonra
PR Outcomes/ HRQL

0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
SGRQönce
SGRQsonra
PR Outcomes/ HRQL






























