Embed Size (px)
Citation preview

F
P
GWa
b
c
d
e
a
AA
KSROT
1
m(rac
oKf
1d
Respiratory Physiology & Neurobiology 166 (2009) 129–141
Contents lists available at ScienceDirect
Respiratory Physiology & Neurobiology
journa l homepage: www.e lsev ier .com/ locate / resphys io l
rontiers review
ulmonary function and spinal cord injury
regory J. Schileroa,b,d,∗, Ann M. Spungena,b,c,d,e,illiam A. Baumana,b,c,d,e, Miroslav Radulovica,b,d, Marvin Lessera
Rehabilitation Research and Development Center of Excellence for the Medical Consequences of Spinal Cord Injury, The James J. Peters VA Medical Center, Bronx, NY, United StatesMedical Service, The James J. Peters VA Medical Center, Bronx, NY, United StatesSpinal Cord Injury Service, The James J. Peters VA Medical Center, Bronx, NY, United StatesDepartment of Medicine, The Mount Sinai School of Medicine, New York, NY, United StatesDepartment of Rehabilitation Medicine, The Mount Sinai School of Medicine, New York, NY, United States
r t i c l e i n f o
rticle history:ccepted 1 April 2009
eywords:pinal cord injuryespiratory Function Testsbstructive sleep apneaetraplegia
a b s t r a c t
Injury to the cervical and upper thoracic spinal cord disrupts function of inspiratory and expiratory mus-cles, as reflected by reduction in spirometric and lung volume parameters and static mouth pressures. Inassociation, subjects with tetraplegia have decreased chest wall and lung compliance, increased abdomi-nal wall compliance, and rib cage stiffness with paradoxical chest wall movements, all of which contributeto an increase in the work of breathing. Expiratory muscle function is more compromised than inspira-tory muscle function among subjects with tetraplegia and high paraplegia, which can result in ineffectivecough and propensity to mucus retention and atelectasis. Subjects with tetraplegia also demonstrateheightened vagal activity with reduction in baseline airway caliber, findings attributed to loss of sympa-thetic innervation to the lungs. Significant increase in airway caliber following inhalation of ipratropiumbromide, an anticholinergic agent, suggests that reduction in airway caliber is not due to acquired air-way fibrosis stemming from repeated infections or to abnormal hysteresis secondary to chronic inabilityof subjects to inhale to predicted total lung capacity. Reduced baseline airway caliber possibly explainswhy subjects with tetraplegia exhibit airway hyperresponsiveness to methacholine and ultrasonicallynebulized distilled water. While it has been well demonstrated that bilateral phrenic nerve pacing orstimulation through intramuscular diaphragmatic electrodes improves inspiratory muscle function, itremains unclear if inspiratory muscle training improves pulmonary function. Recent findings suggest
that expiratory muscle training, electrical stimulation of expiratory muscles and administration of a long-acting �2-agonist (salmeterol) improve physiological parameters and cough. It is unknown if baselinebronchoconstriction in tetraplegia contributes to respiratory symptoms, of if the chronic administrationof a bronchodilator reduces the work of breathing and/or improves respiratory symptoms. Less is knownregarding the benefits of treatment of obstructive sleep apnea, despite evidence indicating that the preva-pers
lence of this condition inindividuals.. Introduction
The purpose of this review is to detail the mechanisms of pul-onary physiologic impairment in persons with spinal cord injury
SCI), and to discuss methods currently available to improve respi-atory muscle strength and cough in this population. Possessingn understanding of these topics assumes great importance forlinicians involved in the care and rehabilitation of patients with
∗ Corresponding author at: Center of Excellence for the Medical Consequencesf Spinal Cord Injury, The James J. Peters VA Medical Center: Rm. 1E-02, 130 Westingsbridge Rd., Bronx, NY 10468, United States. Tel.: +1 718 584 9000x6701;
ax: +1 718 741 4675.E-mail address: [email protected] (G.J. Schilero).
569-9048/$ – see front matter. Published by Elsevier B.V.oi:10.1016/j.resp.2009.04.002
ons with tetraplegia is far greater than that encountered in able-bodied
Published by Elsevier B.V.
SCI, as well as for researchers in the field, especially when armedwith knowledge that pulmonary complications remain a majorcause of morbidity and mortality in this population. Further, givenrecent findings that persons with tetraplegia have an unusually highprevalence of obstructive sleep apnea (OSA), and mounting evi-dence linking untreated OSA to increased cardiovascular diseaserisk in the general population, this review includes a discussion ofwhat is currently known regarding OSA and its treatment in personswith SCI.
Injury to the cervical and upper thoracic cord disrupts function
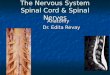
of the diaphragm, intercostal muscles, accessory respiratory mus-cles, and abdominal muscles (Fig. 1), thereby causing reduction inspirometric and lung volume parameters and static mouth pres-sures. As a result, subjects may have ineffective cough and difficultyclearing secretions which in turn predispose to mucus retention,
130 G.J. Schilero et al. / Respiratory Physiology &
Fm
amCrsbllni
2c
2
efSssesah2aAvbAvvep(
2
wri
pulmonary disease (Stepp et al., 2008). Pulmonary function vari-ables are also influenced by previous chest injury or operation, age,time since injury, obesity, and the presence of wheeze (Jain et al.,2006).
ig. 1. Diagram showing levels of innervation of the inspiratory and expiratoryuscles.
telectasis and pulmonary infections, and ultimately to significantorbidity and mortality (Fishburn et al., 1990; DeVivo et al., 1993;
otton et al., 2005). Although numerous studies have demonstratedestrictive ventilatory impairment, recent studies have also demon-trated the presence of baseline bronchoconstriction, which haseen attributed to interruption of sympathetic innervation to the
ungs. Recent studies have also focused upon factors that affectong-term pulmonary function in addition to level and complete-ess of injury, and upon methods for improving respiratory function
n SCI.
. Pulmonary function testing among subjects with spinalord injury
.1. Testing considerations
More than 80% of subjects with SCI are able to perform spirom-try and provide acceptable results using standards developedor able-bodied individuals (Ashba et al., 1993; Standardization ofpirometry, 1995; Kelley et al., 2003; Miller et al., 2005). Someubjects, however, do not fulfill American Thoracic Society (ATS)tandards because of excessive back-extrapolated volume and/orxpiratory efforts lasting fewer than 6 s. Those failing to fulfill ATStandards generally have lower baseline forced vital capacity (FVC)nd forced expiratory volume in one second (FEV1), and frequentlyave neurologically complete cervical cord injury (Kelley et al.,003). Overall, approximately 90% of subjects with chronic SCI areble to provide acceptable and reproducible spirometric results ifTS standards are modified to allow excessive back-extrapolatedolume and expiratory efforts of less than 6 s duration if there haseen a plateau of at least 0.5 s at residual volume (Kelley et al., 2003).mong those who fulfill ATS test criteria, however, there is greaterariability in baseline FEV1 values compared to able-bodied indi-iduals (Radulovic et al., 2008), which may be of significance invaluating effects of bronchodilators. Maintenance of stable headosition during FVC maneuvers reduces measurement variabilityAmodie-Storey et al., 1996).
.2. Spirometric and lung volume parameters
Historically, spirometric and lung volume studies in personsith tetraplegia and high levels of paraplegia have demonstrated
estrictive dysfunction due to neuromuscular weakness character-zed by significant reduction of vital capacity (VC), FEV1, maximal
Neurobiology 166 (2009) 129–141
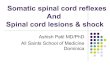
mid-expiratory flow (MMEF), peak expiratory flow (PEF), total lungcapacity (TLC), maximum voluntary ventilation (MVV), expiratoryreserve volume (ERV) and inspiratory capacity (IC), along with a sig-nificant increase in residual volume (RV), and little or no change infunctional residual capacity (FRC) (Hemingway et al., 1958; Fugl-Meyer, 1971; Fugl-Meyer and Grimby, 1971a; Ohry et al., 1975;Kokkola et al., 1975; Forner, 1980; Bluechardt et al., 1992; Roth et al.,1995; Almenoff et al., 1995a; Linn et al., 2000, 2001). One major dif-ference in tetraplegia compared to those with other neuromusculardiseases is greater preservation of inspiratory muscle function,principally of the diaphragm, relative to the compromise in expi-ratory muscle function resulting from paralysis of intercostal andabdominal musculature. This results in a disproportionate reduc-tion in percent predicted values for FVC, an expiratory maneuver,compared to TLC. Significant reduction in ERV is also reflective of themagnitude of expiratory muscle weakness. Following acute injury,vital capacity has been found to correlate well with FEV1, IC, ERV,FRC, RV, TLC and the RV/TLC ratio, indicating that during this periodVC can be used as a general measure of overall ventilatory statusin SCI (Roth et al., 1995). Incomplete lesions appear to mitigate FVCloss in tetraplegia (Linn et al., 2000, 2001). The higher the levelof injury, the more significantly pulmonary function parametersare reduced (Fig. 2). In addition to level of injury and severity ofinjury, other determinants of TLC, FRC, RV and ERV include bodymass index (BMI), total pack-years of smoking, maximal inspira-tory pressure (MIP), and physician-diagnosed chronic obstructive
Fig. 2. Correlation of forced vital capacity (FVC) and forced expiratory volume inone second (FEV1) with level of spinal cord injury (adapted from Linn et al., 2001).

ology &
2
redwi(iwd1
2
(bpsniscstoceda
2
pic(Bfiiti1eo(2rgMm
2S
wlriam
G.J. Schilero et al. / Respiratory Physi
.3. Gas exchange
Single breath nitrogen washout curves in tetraplegia have beeneported to be slightly abnormal or normal, suggesting relativelyven gas distribution (Forner, 1980). However, a xenon-133 studyemonstrated decreased ventilation of basal regions in tetraplegia,hich was attributed to “small airway disease” due to repeated
nfections, or possibly to increased basal small airway resistanceBake et al., 1972). A subsequent radioisotope study demonstratednhomogeneous ventilation in the upper and middle lung regions,
hich was attributed to changes in regional intrapleural pressureue to paradoxical movement of the thoracic cage (Hiraizumi et al.,986).
.4. Effects of smoking
Among subjects with low tetraplegia (C5–C8), high paraplegiaT1–T7), and low paraplegia (T8–L3), FEV1 and PEF were found toe significantly higher among ex-smokers and non-smokers com-ared to active smokers (Almenoff et al., 1995a). The absence of amoking effect among subjects with high tetraplegia (C4 and aboveot requiring mechanical ventilation) was attributed to overriding
njury-related functional loss. A cross-sectional evaluation of 440ubjects with SCI suggested that current smokers showed a signifi-ant excess decline in FEV1/FVC with increasing age, whereas nevermokers showed no age-related decline beyond that expected inhe general population (Linn et al., 2003). Whereas in one studyf 57 subjects with tetraplegia followed for 20 years, no signifi-ant difference was found in mean VC between non-smokers andx/current smokers (Tow et al., 2001), a recent longitudinal studyemonstrated that cigarette smoking in SCI was associated with anccelerated rate of decline of FVC and FEV1 (Stolzmann et al., 2008).
.5. Effects of body position
Pulmonary function parameters differ based upon the bodyosition at which they are measured. Among subjects with SCI,
n contrast to able-bodied individuals, FVC and FEV1 are signifi-antly higher in the supine position compared to the sitting positionEstenne and De Troyer, 1987; Chen et al., 1990; Ali and Oi, 1995;aydur et al., 2001). Expiratory reserve volume is almost uni-
ormly less throughout all injury levels compared to able-bodiedndividuals (Baydur et al., 2001). The increase in VC in SCI dur-ng recumbency has been attributed to a reduction in RV due tohe effect of gravity on abdominal contents rather than due to anncrease in intrathoracic blood volume (Estenne and De Troyer,987); elevation of the diaphragm results in greater downwardxcursion of the contracting diaphragm because muscle fibers areperating at a more favorable portion of their length-tension curveFugl-Meyer, 1971; Estenne and De Troyer, 1987; Baydur et al.,001). In support of a more favorable diaphragmatic length–tensionelationship, VC, IC, and TLC improve among subjects with tetraple-ia with abdominal binders (Maloney, 1979; Goldman et al., 1986;cCool et al., 1986; Hart et al., 2005) and those immersed in isother-al water to shoulder level (Thomaz et al., 2005).
.6. Temporal changes in pulmonary function following traumaticCI
Vital capacity and expiratory flow rates are low in the firsteek following cervical cord injury; individuals with an FVC of
ess than 25% of predicted are likely to develop respiratory failureequiring ventilator support. During the first 12 months followingnjury, VC, IC, TLC and inspiratory and expiratory flow rates increasend FRC decreases, after which time changes in VC and FRC areore gradual while TLC and ventilatory indices remain unchanged
Neurobiology 166 (2009) 129–141 131
(Ledsome and Sharp, 1981; Haas et al., 1985; Anke et al., 1993;Mueller et al., 2008). Initial improvement has been attributed toreturn of functional respiratory muscles coincident with resolu-tion of inflammation and edema above the injury level (Haas etal., 1985). Later increases have been attributed to improvement indiaphragm function (McMichan et al., 1980; Axen et al., 1985; Ooet al., 1999; Brown et al., 2006), increased performance of acces-sory respiratory muscles (Frisbie and Brown, 1994) and chest wallchanges including increased rib cage stability (McMichan et al.,1980; Haas et al., 1985). The improvement in VC has been attributedto an increase in IC resulting from a decrease in FRC (Haas et al.,1985). In general, the time course of recovery of pulmonary functionis variable following SCI and can only be weakly predicted by knowl-edge of the initial pulmonary function test values and the level oflesion (Bluechardt et al., 1992). Significant determinants of longitu-dinal decline in FVC and FEV1 include age, current smoking, increasein BMI, wheeze, and respiratory muscle strength (Stolzmann et al.,2008).
2.7. Breathing pattern and sighs
With regard to the ability of persons with SCI to take maxi-mally deep breaths or sighs, which may be of help in preventingairway collapse, assessment of breathing pattern parameters andsigh frequency has yielded variable findings (Table 1), presumablydue to methodology. Loveridge and Dubo (1990) used rubber straingauges that were attached around the rib cage and the abdomen,Spungen et al. (unpublished data) used a portable magnetometerwith electromagnetic coils secured to the rib cage and abdomen,and Bodin et al. (2003) used a body plethysmograph while sub-jects were breathing though a mouthpiece. Despite the differentmethodologies employed, findings from the 3 studies demonstratethat tidal volume (Vt), minute ventilation (Ve) and mean inspi-ratory flow (tidal volume/inspiratory time: Vt/Ti) were reducedin subjects with tetraplegia. Assessment of mean inspiratory flow(Vt/Ti), however, a widely employed measure of respiratory drive(Tobin, 1992), may not be applicable to subjects with tetraplegiabecause of underestimation of respiratory drive in the presenceof marked abnormalities in respiratory system mechanics (Tobin,1992). Loveridge and Dubo (1990) found sighs (defined as 2× meanVt) to be normal in tetraplegia, although 8 of 14 subjects withtetraplegia had no breaths greater than 2× mean Vt. Using differ-ent criteria, Spungen et al. (unpublished data) found sighs (definedas mean Vt +500 mL) to be significantly reduced among those withtetraplegia compared to gender-, age-, and height-matched con-trols.
2.8. Maximal inspiratory and expiratory pressures
Maximal mouth static respiratory pressures, which are con-sidered surrogate measures of global inspiratory and expiratorymuscle strength, are reduced among those with tetraplegia, and incontrast to normal subjects, MIP is higher than maximal expiratorypressure (MEP) due to greater compromise of expiratory musclefunction (Fugl-Meyer and Grimby, 1971a,b; Gounden, 1997). Among30 subjects with complete lesions between C5 and C8 of greaterthan 6 months duration, mean MEP in the sitting position was48 cm H2O and mean MIP was −64 cm H2O (Gounden, 1997). Staticmouth pressures have been found to correlate with level of injuryamong subjects with complete motor lesions, but not among thosewith incomplete lesions (Mateus et al., 2007). Static pressure values
are dependent upon lung volumes at which they are measured andthe type of mouthpiece used in the assessment; therefore, inter-pretation is problematic in this population. Although a flange-typemouthpiece is generally used, a study of 50 subjects with tetraple-gia demonstrated that MEP values obtained by use of a tube-style
132 G.J. Schilero et al. / Respiratory Physiology & Neurobiology 166 (2009) 129–141
Table 1Breathing pattern parameters among subjects with tetraplegia.
Loveridge and Dubo (1990) Bodin et al. (2003) Spungen et al. (unpublished data)
Tetra Control Tetra Control Tetra Control
Number of subjects 14 6 20 20 10 8Respiratory rate (RR) 20* 16 16 16 18 20Tidal volume (Vt, mL) 305* 419 600* 900 306 414Minute ventilation (Ve, L/min) 5.8 6.6 6.4* 11.3 5.2* 7.2Inspiratory time (Ti, s) 1.3 1.3 NR NR 1.6 1.5Expiratory time (Te, s) 1.9* 2.6 NR NR 2.2 2.1Mean inspiratory flow (Vt/Ti) 0.24* 0.33 0.40* 0.6 0.21* 0.28Ti/Ttot 0.44* 0.34 0.40 0.40 0.43 0.45Sighs (h) NR NR NR NR 11* 42
N
mowabupefdtei
aaspwc(Saliw9wUip
3
aoaTutwssctct(
R = not reported; tetra = tetraplegia.* p < 0.05 compared with control.
outhpiece were significantly greater than those obtained by usef an intra-oral flange-style mouthpiece due to perioral air leaksith the flange-style device (Tully et al., 1997). Similarly, among
ble-bodied individuals and subjects with muscle weakness, it haseen determined that measurements of MEP were best performedsing a large-bore circular mouthpiece or a scuba-diving mouth-iece with the cheeks supported (Koulouris et al., 1988; Rubinsteint al., 1988). When compared with cough gastric pressure, MEP wasound to be falsely low in 42% of 171 subjects with neuromuscularisease (4 with SCI) (Man et al., 2003). However, it is doubtful thathe measurement of cough gastric pressure is of value in assessingxpiratory muscle strength in SCI, because cough gastric pressures low due to abdominal muscle weakness (Siebens et al., 1964).
Sniff nasal inspiratory pressure (SNIP) has also been used tossess inspiratory muscle strength. Sniff nasal inspiratory pressuresre obtained using a tight-fitting intranasal device during a short,harp maximal inspiratory effort, with the contralateral nostrillugged or unplugged. Among able-bodied individuals and thoseith neuromuscular or skeletal disorders (none with SCI), SNIP
orrelated significantly with sniff maximum esophageal pressuresniff Pes) and with MIP (Koulouris et al., 1989; Heritier et al., 1994;tefanutti et al., 2000). However, among 61 patients undergoingssessment of global inspiratory muscle strength, 11 subjects withow MIP had normal sniff Pes and transdiaphragmatic pressure,ndicating that MIP was falsely low, possibly because of difficulties
ith the measurement technique (Laroche et al., 1988). A study ofsubjects with tetraplegia revealed significant correlation of MIPith SNIP (r = 0.8; p ≤ 0.003) (Radulovic et al., unpublished data).ltimately the usefulness of SNIP and MIP as measurements of
nspiratory muscle strength in SCI will require comparison of thesearameters with those of sniff Pes in a research protocol.
. Cough
Cough effectiveness is reduced among subjects with tetraplegiand high paraplegia due to loss of function of the major musclesf expiration including the muscles of the anterolateral wall of thebdomen, the expiratory intercostals, and the triangularis sterni (Deroyer and Estenne, 1991; Fujiwara et al., 1999). Apparent resid-al expiratory function, as reflected by ERV, has been attributedo activity of the clavicular portion of the pectoralis major muscle,hich is innervated by nerve fibers originating in the fifth, sixth, and
eventh cervical segments (De Troyer et al., 1986a), and the latis-imus dorsi muscles (Fujiwara et al., 1999). Cough modulated by the
lavicular portion of the pectoralis major muscle is an active, ratherhan passive process (Estenne and De Troyer, 1990), and muscleontraction causes dynamic airway compression during expira-ory efforts in a substantial proportion of subjects with tetraplegiaEstenne et al., 1994). Cough-induced paradoxical expansion of theabdomen is due to contraction of the pectoralis major and not dueto diaphragmatic activity (Estenne and Gorini, 1992).
Reduced expiratory pressures with ineffective cough are fre-quently associated with mucus plugging and atelectasis, two majorcauses of morbidity and mortality in SCI (Slonimski and Aguilera,2001). Problems may be amplified in the immediate post-injuryperiod, during which time excessive and tenacious mucus is pro-duced, possibly due to amplified or uninhibited parasympatheticactivity (Bhaskar et al., 1991).
Using a capsaicin challenge technique, it was determined thatcough reflex sensitivity was normal in tetraplegia, but may be sup-pressed among those receiving baclofen (Dicpinigaitis et al., 1999,2000). In another study, cough thresholds following administrationof citric acid aerosol were found to be lower among subjects withSCI compared with able-bodied individuals (Lin et al., 1999).
4. Rib cage, compliance, work of breathing and response toresistive loading
Among subjects with high tetraplegia, synchronous contrac-tion of neck muscles including the sternocleidomastoids, trapezii,platysma, mylohyoid and sternohyoid, acts to pull the sternumcranially and to expand the upper rib cage, but results in paradox-ical inward displacement of the lateral walls of the lower rib cage(Danon et al., 1979; De Troyer et al., 1986b). Conversely, isolateddiaphragmatic contraction is generally associated with expansionof the lower rib cage and collapse of the upper rib cage (Moultonand Silver, 1970; Fugl-Meyer and Grimby, 1971b; Mead et al., 1984;Estenne and De Troyer, 1985; McCool et al., 1986; Urmey et al.,1986; Scanlon et al., 1989). Collectively, these findings demonstratethat diaphragm/upper rib cage coupling is abnormal in tetraple-gia, presumably because of loss of intercostal muscle activity andincreased compliance of the abdominal wall (Moulton and Silver,1970; Goldman and Mead, 1973; De Troyer and Heilporn, 1980;Estenne and De Troyer, 1985). Rib cage paradox decreases with timeafter injury (Scanlon et al., 1989), possibly due to the developmentof bony rib cage stiffness, increased strength of cervical accessorymuscles, and improved coupling of the various rib cage elements(Estenne and De Troyer, 1986). Increase in rib cage stiffness hasbeen attributed to ankylosis of joints due to chronic inability ofsubjects to inhale deeply and to an increase in intercostal spas-ticity (Estenne and De Troyer, 1986), as has been observed amongpatients with chronic respiratory muscle weakness due to processesother than spinal cord injury (Estenne et al., 1983). In association,
chest wall, lung, and rib cage compliance are reduced in tetraple-gia, and diaphragm–abdomen compliance is increased (Stone andKeltz, 1963; Fugl-Meyer and Grimby, 1971a; Forner, 1980; Scanlonet al., 1989; Estenne and De Troyer, 1986). The decrease in lungcompliance occurs within 1 month after injury, and has been
ology &
at1par1tiSaepa11
trMittbsdatlhae1ermmma
5
hwFetbff
TR
FFEFs
Fsa
G.J. Schilero et al. / Respiratory Physi
ttributed more to lung volume loss than to intrinsic changes inhe mechanical properties of the lungs (De Troyer and Heilporn,980; Scanlon et al., 1989). The increase in abdominal wall com-liance causes abnormal distribution of ventilation by reducingppositional forces during inspiration that act to expand the lowerib cage (Estenne and De Troyer, 1985, 1987; Goldman et al., 1986,988). Alterations in chest wall, lung and abdominal compliance inetraplegia are associated with an increase in the work of breath-ng, although overall resting oxygen uptake is lower (Silver, 1963;tone and Keltz, 1963; Bergofsky, 1964a; Bergofsky, 1964b; Haas etl., 1965), and may contribute to respiratory muscle fatigue (Brownt al., 2006). Less rib cage distortion and higher pulmonary functionarameters occur among subjects with residual electromyographicctivity of intercostal and scalene muscles (Guttmann and Silver,965; De Troyer and Heilporn, 1980; Estenne and De Troyer,985).
Several studies have demonstrated that subjects with chronicetraplegia have a blunted ventilatory and occlusion pressureesponse to hypercapnia (Kelling et al., 1985; McCool et al., 1988;anning et al., 1992a; Lin et al., 1998). Findings of a normal response
n tetraplegia by Pokorski et al. (1990) may have been due tohe study of subjects with better preserved lung function thanhose evaluated in other studies (Manning et al., 1992a). It haseen suggested that the blunted response cannot be attributedolely to respiratory muscle weakness or functioning length of theiaphragm, but may be due to reduced ventilatory drive (McCool etl., 1988; Manning et al., 1992a). Among subjects with paraplegiahe response to hypercapnia is preserved through rapid and shal-ow breathing (Gorini et al., 2000). In contrast to the response toypercapnia, breath holding times and the response to inspiratorynd expiratory resistive loading is preserved in tetraplegia (Frankelt al., 1971; Kelling et al., 1985; Im Hof et al., 1986; O’Donnell et al.,993), although the sensation of loading may be blunted (Gottfriedt al., 1984). However, the oxygen cost of breathing with inspiratoryesistive loading is greater among subjects with tetraplegia, whichay be related to the elastic work of chest wall distortion, shorterean operational diaphragm length and possible differences in theechanical advantage of available inspiratory muscles (Manning et
l., 1992b).
. Airway obstruction
Historically, spirometric studies of subjects with tetraplegiaave consistently demonstrated ventilatory restrictive impairmentithout apparent air-flow obstruction (Hemingway et al., 1958;
orner, 1980). Of note, in 1965 Haas et al., suggested that differ-
nces in time constants among subjects with acute and post-acuteetraplegia compared to those with chronic injury was possi-ly due to an increase in pulmonary resistance. In 1993, it wasound that administration of the �2 agonist metaproterenol sul-ate to 34 subjects with chronic tetraplegia resulted in a significantable 2esponse to ipratropium bromide in spinal cord injury.
Tetraplegia (n = 6)
Mean ± S.D. % ch
EV1 (L) 2.11 ± 0.57 (1EV1/FVC ratio 75 ± 4 (RV (L) 0.63 ± 0.56 (5RC (L) 2.67 ± 1.02 (Gaw (cm H2O−1 s−1) 0.13 ± 0.05 (13
EV1 = forced expired volume in one second; FEV1/FVC = the ratio of the FEV1 to the forcedGaw = specific airway conductance. Values in parentheses represent percentage changel. (2005).
* p < 0.05 represents significant change following ipratropium bromide.
Neurobiology 166 (2009) 129–141 133
increase in FEV1 (≥12% and 200 mL) in 14 of the subjects (41%)(Spungen et al., 1993). The findings demonstrated that subjectswith tetraplegia have unsuspected airway obstruction not pre-viously appreciated because of normal FEV1/FVC ratios. It waspostulated that heightened responsiveness was due to interrup-tion of sympathetic innervation to the lung, thereby resultingin parasympathetic (bronchoconstrictive) predominance. Supportcame from a study which demonstrated that 12 of 25 (46%)of subjects with tetraplegia had a significant increase in FEV1following inhalation of the anticholinergic agent ipratropiumbromide (IB) (Almenoff et al., 1995b). Significant insight wasobtained from a body plethysmographic study, which revealedthat baseline specific airway conductance (sGaw) was significantlylower in tetraplegia (0.16 ± 05 cm H2O−1 s−1) compared to subjectswith paraplegia (0.26 ± 0.05 cm H2O−1 s−1) and control subjects(0.27 ± 0.05 cm H2O−1 s−1) (Schilero et al., 2005), and that subjectswith tetraplegia had a significantly greater increase in sGaw follow-ing inhalation of IB (Table 2).
To the extent that sGaw represents the number, length andpatency of the conducting airways (Butler et al., 1960), bodyplethysmography findings demonstrate that baseline airway cal-iber is reduced among subjects with tetraplegia (Schilero et al.,2005). The significant increase in sGaw in tetraplegia following IBmeets the established criteria for significant bronchodilator respon-siveness (Van Noord et al., 1994), and demonstrates that reducedbaseline caliber in tetraplegia is due to heightened vagal tone. Otherinvestigators have also found low baseline sGaw among subjectswith tetraplegia that increased significantly following inhalationof IB (Mateus et al., 2006). Of note, sGaw has been measured insubjects with chronic muscle weakness due to processes otherthan cervical cord injury (Inkley et al., 1974; Gibson et al., 1977;Demedts et al., 1982). Although many of the subjects had reducedstatic lung compliance, comparable to that found among subjectswith tetraplegia (De Troyer and Heilporn, 1980; Forner, 1980), sGawranged from normal to high. Therefore, findings of reduced baselinesGaw in tetraplegia suggest a major difference in factors govern-ing airway caliber compared with those who have general muscleweakness.
6. Autonomic nervous system and airway tone
Activity carried within parasympathetic nerves represents themajor bronchoconstrictive system in all animal species (Barnes,1986). Centrally generated efferent vagal output remains intactwith cervical cord injury. Efferent coded action potentials are car-ried in the vagus nerve to autonomic ganglia located in airway walls,
and then widely distributed throughout the lungs through post-ganglionic fibers. Synaptic transmission in autonomic ganglia andat the level of airway smooth muscle is influenced by autocoids,tachykinins, bradykinin, nitric oxide, and catecholamines (Rackeand Matthiesen, 2004). Release of norepinephrine from adrenergicParaplegia (n = 6)
Mean ± S.D. % ch
2 ± 6)* 3.24 ± 0.64 (2 ± 3)5 ± 7) 82 ± 7 (0 ± 2)7 ± 63)* 1.09 ± 0.45 (−7 ± 30)0 ± 10) 3.16 ± 0.58 (−5 ± 4)*
5 ± 47)* 0.26 ± 0.02 (19 ± 7)*
vital capacity; ERV = expiratory reserve volume; FRC = functional residual capacity;from baseline following ipratropium bromide. The data is adapted from Schilero et

1 ology &
nibK
vsnigaaaasbbecbc
ulv1elpre2ptlptc(
suTTs26Ttnbtplc
TS
THL
Dm
34 G.J. Schilero et al. / Respiratory Physi
erves may influence bronchomotor tone indirectly by modulat-ng cholinergic neurotransmission at the level of autonomic gangliay inhibiting activity of acetylcholine (Barnes, 1986; Davis andannan, 1987).
In contrast to parasympathetic innervation, sympathetic inner-ation of the lungs arising in the upper 6 thoracic segments of thepinal cord is interrupted with cervical cord injury. Postganglionicerve fibers synapse in the middle and inferior cervical ganglia and
n the upper four thoracic ganglia to enter the hilum to intermin-le with cholinergic nerves to form a dense plexus round airwaysnd vessels (Barnes, 1986). Although early studies indicated thatdrenergic (sympathetic) nerves were not present at the level ofirway smooth muscle (Richardson and Ferguson, 1979; Doidgend Satchell, 1982), additional studies, however, demonstrated thatympathetic fibers innervate the smooth muscle layer of the humanronchial tree, with a few fibers reaching the level of secondaryronchi and terminal bronchioles (Partanen et al., 1982; Laitinent al., 1985). Even sparse innervation may have physiologic signifi-ance in the regulation of bronchial smooth muscle tone in humansecause muscle cells are electrically coupled, indicating that everyell need not be innervated to contract (Partanen et al., 1982).
However, associated pharmacological manipulation studiessing electrical field stimulation of excised human tracheal and
ung tissue failed to demonstrate functional sympathetic inner-ation of human airways (Doidge and Satchell, 1982; Davis et al.,982), but demonstrated the presence of nonadrenergic, noncholin-rgic bronchodilator innervation (Lammers et al., 1988), therebyeading to the current belief that there is no functional sym-athetic innervation of human airway smooth muscle, and thatelaxation of airway smooth muscle is due to inhibitory nonadren-rgic, noncholinergic nerves (Barnes, 1986; Canning and Fischer,001). However, recent findings among subjects with high para-legia (T3 to T6) that baseline airway caliber was comparable tohat found in low paraplegia, whereas epinephrine levels wereow in high paraplegia and tetraplegia in comparison with lowaraplegia (Schmid et al., 1998), provides circumstantial evidencehat sympathetic innervation to the lung is of functional signifi-ance in the maintenance of airway tone (Radulovic et al., 2008)Table 3).
Support for the suggestion that human lung contains functionalympathetic innervation comes from studies of patients who havendergone bilateral video-assisted sympathectomy at levels T2 and3 for cure of essential hyperhidrosis (Noppen and Vincken, 1996;seng and Tseng, 2001; Vigil et al., 2005). These studies demon-trated that FEV1, FEV1/FVC and forced expiratory flow between5% and 75% of vital capacity (FEF25–75) were significantly lowermonths following surgery as compared to values before surgery.
he changes were attributed to mild impairment of bronchomo-or tone rather than to the surgical procedure, because FVC wasot decreased postoperatively. These findings, and the study ofaseline airway caliber in SCI (Radulovic et al., 2008), suggest
hat even partial pulmonary sympathetic innervation, which wouldresumably occur with lesions at T4–T6, participates in the regu-ation of airway tone and contributes to reduced baseline airwayaliber.
able 3pecific airway conductance in subjects with spinal cord injury.
sGaw (cm H2O−1 s−1) Epinephrine level (�mol/L)
etraplegia (n = 12) 0.14 ± 0.03* 0.06igh paraplegia (n = 11) 0.19 ± 0.05 0.08ow paraplegia (n = 11) 0.19 ± 0.04 0.16
ata adapted from Radulovic et al. (2008), and Schmid et al. (1998). sGaw values areean ± S.D.* p < 0.001 compared to high paraplegia and low paraplegia.
Neurobiology 166 (2009) 129–141
7. Airway hyperreactivity and baseline airway caliber
Subjects with tetraplegia, but not those with low paraplegia,demonstrate airway hyperreactivity in response to metha-choline, histamine and ultrasonically nebulized distilled water(Dicpinigaitis et al., 1994a; Singas et al., 1996; Fein et al., 1998;Grimm et al., 1999). Responders to histamine demonstrated reduc-tions in surrogate spirometric indices of airway size and airwaysize relative to lung size (FEF25–75; FEF25–75 percent predicted;FEV1 percent predicted; FEF25–75/FVC ratio) (Grimm et al., 2000).One explanation for these findings is that with preexisting air-way narrowing a small further reduction in caliber induced by abronchoconstrictive agent produces a large increase in resistance,because airway resistance is inversely proportional to the fourthpower of the radius (Cockroft and Davis, 2006). Support for thepostulation that subjects with tetraplegia have reduced baselineairway caliber comes from additional observations that IB pre-treatment blocked ultrasonically nebulized distilled water-inducedbronchoconstriction (Grimm et al., 1999), that the �-aminobutyricacid (GABA)-agonist (baclofen), and oxybutynin chloride, both withanticholinergic activity, inhibited hyperresponsiveness to metha-choline (Dicpinigaitis et al., 1994b; Singas et al., 1999) and thatpretreatment with aerosolized metaproterenol sulfate markedlyattenuated methacholine- and histamine-induced hyperrespon-siveness (DeLuca et al., 1999). Attenuation with metaproterenoldoes not specifically demonstrate abnormal sympathetic respon-siveness because beta-2 agonists cause functional airway relaxationregardless of the underlying cause of bronchoconstriction (Barnes,1986).
Further observations, however, suggest that factors in additionto reduced baseline airway caliber may contribute to histamine-induced airway hyperresponsiveness among those with tetraplegia.These include findings that pretreatment with aerosolized IB didnot attenuate histamine-induced hyperreactivity (Fein et al., 1998),and that subjects receiving baclofen or oxybutynin chloride did notdemonstrate reduced responsiveness to histamine (Singas et al.,1999; Grimm et al., 1997).
Several additional mechanisms may cause or contribute toreduced airway caliber in tetraplegia. Airway narrowing in asthmahas also been attributed to airway remodeling caused by chronicinflammation (Cockroft and Davis, 2006). The contribution ofinflammation, if any, to airway hyperreactivity in SCI has not beeninvestigated. Exaggerated bronchoconstriction and reduced base-line airway caliber may also be explained by the inability of subjectswith tetraplegia to breathe to their predicted total lung capacity(Fugl-Meyer, 1971; Kokkola et al., 1975; Ohry et al., 1975). Deepinspiration dilates the airways by exerting an increase in the air-way transmural pressure (Moore et al., 1997). Normal subjectsdevelop exaggerated airway narrowing if deep breathing is vol-untarily suppressed prior to methacholine challenge (Skloot etal., 1995), therein suggesting that bronchoconstriction in diseasessuch as asthma and chronic obstructive pulmonary disease maybe due to a failure of deep inspiration to reverse airway narrow-ing rather than an exaggerated capacity of the airways to narrow(Fish et al., 1981; Pellegrino et al., 1998). However, observationsthat subjects with tetraplegia demonstrate a dramatic increasein sGaw following inhalation of IB suggest that their inability toinhale to predicted TLC does not explain reduced baseline air-way caliber (Schilero et al., 2005). Likewise, because of rapidincrease in sGaw following IB, it is unlikely that reduced base-line airway caliber in tetraplegia is due to processes decreasing
the load on airway smooth muscle including airway cartilage soft-ening, decreased tethering of lung parenchyma, increased airwaysmooth muscle in proportion to circumference, increased wallthickness, or increased secretions in airway lumens (Moreno et al.,1986).
ology &
8
udrBliiTtafhtoadcosdoiva1tnveacp
9
htadefisfB1tchva
i1igm1mtb
G.J. Schilero et al. / Respiratory Physi
. Pulmonary symptoms
A survey of respiratory symptoms among 180 subjects with SCIsing a modified questionnaire developed for use in general epi-emiological studies (Ferris, 1978) revealed that 68% of individualseported one or more respiratory symptom (Spungen et al., 1997).reathlessness, the most prevalent complaint, was associated with
evel of injury: 73% in high tetraplegia (C5 and above not requir-ng mechanical ventilation), 58% in low tetraplegia (C6–C8), 43%n high paraplegia (T1–T7), and 29% in low paraplegia (T8–L3).he prevalence of chronic cough (18%), chronic phlegm produc-ion (30%), cough combined with chronic phlegm production (20%),nd chronic wheeze (24%) did not differ significantly among theour groups. Of note and of potential importance, subjects withigh tetraplegia reported increased breathlessness when exposedo hot air or second-hand cigarette smoke. Independent predictorsf breathlessness were level of injury, cough combined with phlegmnd/or wheeze, TLC (<60% predicted) and ERV (<0.6 L), but not age,uration of injury, completeness of injury, a history of asthma, orurrent smoking (Spungen et al., 2002). Independent predictorsf cough combined with phlegm and/or wheeze included currentmoking, breathlessness, and FEV1 (<60% predicted), but not age,uration of injury, completeness of injury, level of injury, or a historyf asthma. Other investigators have reported that breathlessnesss more prevalent among those with neurologically complete cer-ical injury, those who need a motorized wheelchair for dailyctivities, and those with SCI considered non-athletes (Ayas et al.,999; Wien et al., 1999; Grandas et al., 2005). It was determinedhat the use of a custom girdle significantly lowered breathless-ess in patients with SCI, presumably by optimizing operating lungolumes and by decreasing abdominal compliance secondary tonhanced diaphragm performance (Hart et al., 2005). The qualitynd intensity of breathlessness during methacholine-induced bron-hoconstriction and dynamic hyperinflation is comparable amongatients with tetraplegia or asthma (Lougheed et al., 2002).
. Methods to improve pulmonary function
As detailed in several recent review papers, a number of studiesave been performed to determine if resistive inspiratory muscleraining improves pulmonary function parameters in SCI (Brooksnd O’Brien, 2005; Van Houtte et al., 2006). Two studies were ran-omized with a comparison group (Loveridge et al., 1989; Liawt al., 2000). Meta-analysis could not be performed due to dif-erences in study design and outcomes. Therefore, the benefit ofnspiratory muscle training in tetraplegia remains unclear, andpontaneous recovery cannot be excluded as being responsibleor some of the observed improvements (Stiller and Huff, 1999;rooks and O’Brien, 2005). Recently it was reported that among4 subjects with acute SCI (time between lesion and inclusion inhe study at least 6 weeks) randomized to receive either normo-apnic hyperpnea or sham training for 8 weeks, that normocapnicyperpnea training was associated with an increase in maximumoluntary ventilation, and improved MIP and MEP (Van Houtte etl., 2008).
Two studies have evaluated the role of expiratory muscle train-ng among individuals with SCI (Estenne et al., 1989; Gounden,990). Training of the pectoralis major by repetitive, strenuous,sometric contractions for 6 weeks among subjects with tetraple-ia was associated with marked increases in maximal isometric
uscle strength and ERV, and a decrease in RV (Estenne et al.,989). A recent review assessing the effectiveness of expiratoryuscle training (excluding electrical stimulation) concluded that
raining tended to improve expiratory muscle strength, VC and RV,ut insufficient data was available to make conclusions concern-
Neurobiology 166 (2009) 129–141 135
ing the effects on inspiratory muscle strength, respiratory muscleendurance, quality of life, exercise performance and respiratorycomplications (Van Houtte et al., 2006).
Methods available to remove patients from ventilatory supportand/or increase inspired volumes include conventional phrenicnerve pacing, intramuscular diaphragmatic pacing, and intercostalnerve pacing (Glenn et al., 1984; DiMarco, 2005; DiMarco et al.,2005a). Combined intercostal and unilateral diaphragmatic pacingmay be a therapeutic option in selected individuals (DiMarco etal., 2005b). Of potential importance, subjects with tetraplegia haveincreased diaphragmatic fatigability with sustained pacing or dur-ing ventilatory threshold loading (Nava et al., 1996; Hopman et al.,1997), which has been attributed to a combination of loss of ribcageinspiratory muscles and alterations in chest-wall properties ratherthan to changes in diaphragmatic function (Fugl-Meyer and Grimby,1984).
Electrical stimulation methods to improve expiratory musclefunction and cough include magnetic stimulation of the expira-tory muscles by placement of a stimulation coil over the lowerback, stimulation of abdominal muscles directly by placement ofelectrodes over the surface of the abdominal wall, and electricalstimulation applied in the region of the lower thoracic spinal cord(DiMarco, 2005). Magnetic stimulation of abdominal muscles byplacement of a stimulation coil over the lower back caused increasesin esophageal pressure and expiratory flow rates, increases deemedgreater than those required to initiate dynamic airway compression(Estenne et al., 2000). Magnetic stimulation of the lower thoracicspine among 8 subjects with tetraplegia for 4 weeks was asso-ciated with an increase in MEP, ERV, and forced expiratory flowrate (Lin et al., 2001). The benefits, however, disappeared within2 weeks after discontinuation of stimulation. Increases in tidalvolume, MEP, FVC, FEV1 and PEF occur with direct stimulation ofabdominal muscles, with coughs produced by electrical stimula-tion being approximately as effective as those obtained by manualassistance (Jaeger et al., 1993; Linder, 1993; Stanic et al., 2000;Langbein et al., 2001). In a randomized 4-week controlled trial,whereby neuromuscular electrical stimulation was applied to theclavicular portion of the pectoralis major and abdominal musclesthere was a significant increase in PEF, FEV1, VC, MEP and MIP com-pared to controls (Cheng et al., 2006) that persisted for at least 3months after cessation of therapy. Abdominal binding alone hassmall effects on forced expiration as assessed by expiratory flowrate and esophageal pressure and is unlikely to improve the effi-ciency of cough (Estenne et al., 1998). A systematic review andmeta-analysis found a lack of sufficient evidence to either supportor discourage the use of an abdominal binder to improve respiratoryfunction in SCI (Wadsworth et al., 2008).
�2 adrenergic agonists have been evaluated in SCI. Signorileet al. determined in a double-blind, placebo controlled, crossoverstudy among subjects with tetraplegia given an oral short-acting �2adrenergic agent (metaproterenol) that forearm muscle strengthand size increased significantly during the time of active drugadministration (Signorile et al., 1995). Also, a placebo-controlledstudy of 3 individuals with SCI (two with tetraplegia and one withparaplegia) demonstrated that total work output during functionalelectrical stimulation cycling increased 64% during salbutamoltreatment as compared to a 27% increase with placebo treat-ment (27%) (Murphy et al., 1999). A randomized, prospective,double-blind, placebo-controlled crossover study was performedto determine if long-term administration of a long-acting �2-adrenergic agonist improved pulmonary function parameters and
static mouth pressures among subjects with tetraplegia (Grimmet al., 2006) (Table 4). During the 4-week period of salmeteroladministration, FVC, FEV1, PEF, MIP and MEP increased significantly.Although the increase in MIP and MEP suggest improvement inrespiratory muscle strength, this cannot be stated with certainty
136 G.J. Schilero et al. / Respiratory Physiology &
Table 4Effect of salmeterol on respiratory parameters among subjects with tetraplegia(n = 11).
Baseline Placebo Salmeterol
FVC (L) 3.11 ± 0.38 3.22 ± 0.41 3.36 ± 0.41*,†
FEV1 (L) 2.40 ± 0.51 2.52 ± 0.49 2.74 ± 0.52*,†
PEF (L/s) 4.63 ± 1.13 5.01 ± 1.06 5.78 ± 1.20*,†
MIP (cm H2O) −72.5 ± 18.6 −73.9 ± 21.5 −81.6 ± 20.8*,†
MEP (cm H2O) 40.9 ± 16.1 45.9 ± 19.2 51.3 ± 20.0*,†
T
balsaet
cf2
1
oamsSt2enuFumc(acwilstaAiwtiidjf
ost(L
he data are mean ± S.D. Data adapted from Grimm et al. (2006).* p < 0.001 compared to baseline.† p < 0.05 compared to placebo.
ecause MIP and MEP values are dependent on volume parameterst which they are measured, some of which also increased. Regard-ess of the mechanism, improvement in pulmonary parameters andtatic mouth pressures with salmeterol indicate that long-termdministration of a �2 adrenergic agonist should improve coughffectiveness in tetraplegia, and possibly improve respiratory symp-oms.
With regard to alternative agents, a randomized study withrossover demonstrated that administration of oral theophyllineor 6 weeks did not improve pulmonary function (Tzelepis et al.,006).
0. Sleep apnea in SCI
In middle-aged adults, the estimated prevalence of sleep dis-rdered breathing without regard to symptoms, defined as anpnea-hypopnea index (AHI) of ≥15 events/h of sleep, is 9.1% inen and 4% in women (Young et al., 1993). In four cross-sectional
creening studies that included between 22 and 50 subjects withCI, results from polysomnographic data employing the same AHIhreshold to define sleep apnea yielded a prevalence ranging from2% to 62% (Short et al., 1992; McEvoy et al., 1995; Stockhammert al., 2002; Leduc et al., 2007). In another investigation, a diag-osis of sleep apnea was made in 9 of 20 participants (45%) basedpon an apnea index of ≥5 events/h of sleep (Burns et al., 2000).indings from screening evaluations in persons with SCI that reliedpon overnight pulse oximetry with or without monitoring of bodyovement indentified a pattern of episodic oxygen desaturation
haracteristic of sleep apnea in a significant number of subjectsBraun et al., 1982; Flavell et al., 1992; Cahan et al., 1993; Bachnd Wang, 1994). Notwithstanding differences in methodologi-al design and patient selection, including little representation byomen and subjects with paraplegia, findings from the above stud-
es suggest a prevalence of sleep apnea in association with SCI ateast twice that reported in the general population. Obstructiveleep apnea (OSA) rather than central sleep apnea predominates;o which individuals with tetraplegia appear particularly prone. Inretrospective analysis of 584 male patients served by a Veteransffairs SCI Service, previously diagnosed sleep apnea was identified
n significantly more patients with tetraplegia (14.9%) than thoseith paraplegia (3.7%) (Burns et al., 2001). An association between
etraplegia and sleep apnea was also strongly suggested by find-ngs from a longitudinal assessment of sleep disordered breathingn 25 men following acute cervical SCI, among whom sleep apneaefined as an AHI ≥10 events/h of sleep developed in 62% of sub-
ects within 1 month of injury, and varied little during 1 year ofollow-up (Berlowitz et al., 2005).
Excessive daytime sleepiness coupled with OSA is indicative
f the obstructive sleep apnea syndrome (OSAS). In larger scaletudies of persons with SCI that incorporated assessment of day-ime sleepiness, the prevalence of OSAS ranged from 9% to 53%Klefbeck et al., 1998; Burns et al., 2000; Stockhammer et al., 2002;educ et al., 2007). These values exceed prevalence estimates ofNeurobiology 166 (2009) 129–141
4% in men and 2% in women reported in the general adult pop-ulation based upon minimal diagnostic criteria (AHI ≥5 events/hplus symptoms) (Young et al., 1993). The 53% prevalence of OSASrecently reported by Leduc and colleagues from a relatively largesample of 41 subjects with tetraplegia (Leduc et al., 2007) applieddiagnostic criteria recommended by the American Academy ofSleep Medicine (American Academy of Sleep Medicine Task Force,1999); the symptom of excessive daytime sleepiness, though lack-ing specificity, was reported in a significantly greater proportion ofsubjects with (19 of 22) than without OSA (10 of 19). In other studies,symptom assessment was either non-discriminatory (Klefbeck etal., 1998; Burns et al., 2000) or helped to identify only those patientswith severe OSA (AHI >40 events/h of sleep) (Stockhammer et al.,2002). Given that sleep disruption is relatively common in personswith SCI, as is the use of sedative-hypnotic medication, screeningfor OSAS based upon a complaint of excessive daytime sleepinesshas limitations (Bonekat et al., 1990; Biering-Sorensen and Biering-Sorensen, 2001). In one survey, neurogenic pain, spasticity, andvoiding difficulties were cited by respondents, approximately onehalf of whom had cervical injury, as the greatest contributors tosleep disruption (Biering-Sorensen and Biering-Sorensen, 2001).The ability to correctly identify symptomatic OSA in persons withSCI could have important therapeutic implications if treatment wasassociated with improvement in sleep quality and potentially inhealth related quality of life as has been reported in able-bodiedsubjects (Jenkinson et al., 1999; Sin et al., 2002).
Recognized risk factors for OSA in the general adult populationincluding male gender, obesity, and advancing age have been vari-ably linked to the high prevalence of OSA among subjects withtetraplegia, although findings are not uniform due to limited sam-ple sizes and differences in study design, patient recruitment, anddiagnostic methods. Body mass index, a strong predictor of OSAseverity in the general population, directly correlated with apneaseverity in four (Flavell et al., 1992; Burns et al., 2001; Stockhammeret al., 2002; Leduc et al., 2007) of the seven (Short et al., 1992;Klefbeck et al., 1998; Burns et al., 2000) studies involving patientswith SCI in which it was evaluated. Further inspection reveals thatthe association between BMI and OSA appears to be stronger if anal-ysis is limited to studies that enlisted only subjects with tetraplegiascreened by polysomnography (Stockhammer et al., 2002; Leduc etal., 2007). Similarly, neck circumference, which has been applied ina prediction rule to estimate a patient’s probability of having OSA inable-bodied subjects (Flemons et al., 1994), directly correlates withapnea severity in the three studies that included only subjects withtetraplegia (McEvoy et al., 1995; Stockhammer et al., 2002; Leducet al., 2007), and not in the two reports that included subjects withparaplegia (Short et al., 1992; Burns et al., 2000). Possible reasonsfor why exclusion of subjects with paraplegia appears to strengthenassociations between either BMI or neck circumference and OSA inpersons with tetraplegia include the greater prevalence of obesityin persons with paraplegia despite an apparently lower risk of OSA(Burns et al., 2001) and increases in neck mass that occur followingcervical spinal cord injury (Frisbie and Brown, 1994). Habitual snor-ing, another important marker of OSA in the general population, andan independent predictor of cardiovascular disease risk (Koskenvuoet al., 1987), appears to be more prevalent, of greater intensity, andpresent for more years in subjects with SCI compared to a con-trol population (Biering-Sorensen and Biering-Sorensen, 2001). Inanother survey, habitual snoring was reported in 42.6% of respon-dents, and appeared to be more common in obese subjects andthose taking antispasticity medication (baclofen, diazepam) (Ayas
et al., 2001). Snoring was equally represented, however, across alllevels of spinal cord injury, and there is no evidence to suggest thatpersons with tetraplegia snore to any greater or lesser degree thanpersons with lower level SCI. With regard to other factors, there isinsufficient evidence to link OSA prevalence in persons with SCI
ology &
tlo
tuc(aap(piimhstti
wStswaoftipCs(iwoOd5wiajhupnfitbncwmcslrttdt
G.J. Schilero et al. / Respiratory Physi
o age, smoking status, alcohol consumption, duration of injury,evel of injury, completeness of injury, pulmonary function, or usef antispasticity medications.
In addition to respiratory muscle weakness, several poten-ial factors have been proposed to explain the pathophysiologynderlying OSA in persons with tetraplegia. These include pooroordination between respiratory and pharyngeal dilator musclesCahan et al., 1993), decreased pharyngeal cross-sectional area inssociation with reduced lung volumes (Hoffstein et al., 1984),nd possibly thickening of the oropharyngeal wall through unop-osed parasympathetic stimulation of mucosal and vessel wallsWasicko et al., 1990). Preferential adoption of a supine sleepingosition common among persons with tetraplegia could impose
ncreased gravitational stress upon the upper airway. A decreasen upper airway patency could also result from loss of lean tissue
ass and fat redistribution given evidence that persons with SCIave greater adiposity for any given BMI compared to able-bodiedubjects (Spungen et al., 2003). Alternatively, the possibility existshat the increased neck circumference observed in persons withetraplegia is the result of neck muscle hypertrophy in response toncreased respiratory loads (Burns et al., 2001).
Few studies have addressed treatment of OSA in personsith SCI (Biering-Sorensen et al., 1995; Burns et al., 2001, 2005;
tockhammer et al., 2002). Short term follow-up with nasal con-inuous positive airway pressure (CPAP) was addressed in 16 of 31ubjects with tetraplegia diagnosed with OSA in a screening studyho subsequently accepted a trial of treatment (Stockhammer et
l., 2002). Five discontinued therapy within 2 weeks, four becausef mask discomfort, and one because of anxiety. Subjective benefitrom CPAP treatment was reported in ten of 11 subjects who con-inued therapy, all of whom were symptomatic before treatmentnitiation. In a retrospective analysis of persons with tetraplegia andaraplegia, 47% of 49 subjects were receiving treatment (primarilyPAP or bi-level positive airway pressure; Bi-PAP), the remainingubjects were either intolerant of CPAP/Bi-PAP or refused treatmentBurns et al., 2001). The only study to address long-term treatmentnvolved subjective responses to a mail-in survey sent to 72 patients
ith tetraplegia and paraplegia identified through a Departmentf Veterans Affairs SCI database, most previously diagnosed withSA on clinical grounds rather than through participation in a ran-om screening study (Burns et al., 2005). The response rate was4%, amounting to 40 subjects (37 with tetraplegia) diagnosedith OSA a mean of 4.2 ± 3.0 years prior to the study. The survey
ndicated that the primary reasons for originally undergoing sleeppnea testing included witnessed apneas, severe snoring, and sub-ective sleepiness, and that of the 90% of patients (36 of 40) whoad been offered CPAP/Bi-PAP therapy, 20 (54%) reported contin-ed use for an average of 6.5 nights per week (range 3–7), 6.9 ± 1.9 her night. The side effects of CPAP/Bi-PAP reported, which includedasal congestion, mask discomfort, throat and nasal dryness, and
requent awakenings were similar to those that have been reportedn able-bodied subjects (Kakkar and Berry, 2007). Of the 17 par-icipants who were not currently receiving any treatment, 13 hadeen offered CPAP and 12 had tried it, the principal reasons foron-adherence being inability to fall asleep with the mask, dis-omfort, and claustrophobia. Despite the realization that personsith tetraplegia often lack adequate hand function to readjust theask, the acceptance and compliance rates for CPAP/Bi-PAP therapy
ompared favorably with what has been reported in able-bodiedubjects (McArdle et al., 1999). The acceptance rate, however, wasikely an overestimation, as it was determined through medical
ecord review that a significantly greater percentage of respondentso the survey were receiving CPAP/Bi-PAP treatment as comparedo non-respondents (Burns et al., 2005). Of interest, the degree ofaytime sleepiness as assessed by responses to a validated ques-ionnaire developed in able-bodied subjects (Epworth SleepinessNeurobiology 166 (2009) 129–141 137
Scale), revealed no differences between respondents on therapyand those receiving no treatment. A paucity of information existsregarding other forms of therapy for OSA in persons with SCI,including conservative treatments (i.e. weight loss regimens, bodypositioning), surgical approaches, and mandibular repositioningdevices.
Obstructive sleep apnea has been associated with neurocogni-tive dysfunction both in the able-bodied population (Adams et al.,2001) and in persons with tetraplegia (Sajkov et al., 1998). Moreimportantly, in the general population there is now strong evidencelinking OSA to hypertension, stroke, and myocardial infarction(Nieto et al., 2000; Shahar et al., 2001). It is not yet known whetherthe same association exists in persons with SCI, although prematurecardiovascular disease is prevalent and a major cause for mortalityin this population (Myers et al., 2007).
11. Conclusions and future directions
Research performed over the past 25 years has greatly enhancedour understanding of respiratory system mechanics, the extent ofcompromise in pulmonary function, and the determinants of pul-monary functional decline among persons with SCI. More recentstudies have fostered a greater appreciation of airway dynamics,particularly in reference to investigations of resting airway caliber,bronchial provocation, and bronchodilator responsiveness. Personswith tetraplegia, as compared to those with paraplegia or other neu-romuscular diseases, appear to have a unique pattern of respiratoryimpairment characterized by lung volume restriction, greater com-promise of expiratory compared to inspiratory muscle function, andbaseline airway narrowing, all of which to varying degrees maycontribute to weakened cough, ineffective pulmonary clearance,increased work of breathing, and possibly to respiratory symp-tomatology and bronchial hyperresponsiveness. In addition, theseindividuals appear to be highly susceptible to the developmentof OSA, although the underlying pathophysiology as it relates torespiratory muscle paralysis and/or neurogenic mechanisms, theacute hemodynamic response to obstructed apneas, the effects oftreatment, and the long-term consequences of this condition arelargely unknown. Despite a more global level of understanding ofpulmonary physiology in other areas, however, we are still compro-mised in our ability to identify individuals with SCI who are at riskfor development of recurrent atelectasis, pneumonia, and respira-tory failure based upon known physiologic parameters, even whentaking into account level and completeness of injury. This trans-lates to a limited ability to identify at risk subgroups and to targetspecific therapies.
Further investigation is therefore warranted to identify themost accurate method for non-invasive measurement of respira-tory muscle strength in persons with SCI, and on a larger scale toassess the subacute to long-term impact upon pulmonary function,respiratory symptoms, quality of life, and incidence of pulmonarycomplications associated with inspiratory/expiratory muscle train-ing and use of anabolic agents (i.e. �2 adrenergic agonists).Ongoing research involving electrical stimulation of spinal cordsegments and inspiratory/expiratory muscle groups holds promisefor reducing respiratory complications and ventilatory dependencein persons with SCI, although at the present time the applicabil-ity of these techniques appears to be limited to highly selectedindividuals. The importance of airway obstruction and bronchialhyperreactivity in persons with tetraplegia also deserves further
study, especially with regard to the potential roles of overridingcholinergic airway tone and airway inflammation in pathogenesis,and whether use of inhaled anticholinergic agents to reduce air-way resistance leads to a reduction in respiratory symptoms, OSAseverity, pulmonary complications, and improved quality of life.
1 ology &
TanS
R
A
A
A
A
A
A
A
A
A
A
A
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
38 G.J. Schilero et al. / Respiratory Physi
o broadly facilitate answering these and other questions, there isfurther need to develop a disease-specific respiratory question-aire and quality of life instrument validated for use in persons withCI.
eferences
dams, N., Strauss, M., Schluchter, M., Redline, S., 2001. Relation of measures of sleep-disordered breathing to neuropsychological functioning. Am. J. Respir. Crit. CareMed. 163, 1626–1631.
li, J., Oi, W., 1995. Pulmonary function and posture in traumatic quadriplegia. J.Trauma 39, 334–337.
lmenoff, P.L., Spungen, A.M., Lesser, M., Bauman, W.A., 1995a. Pulmonary functionsurvey in spinal cord injury: influences of smoking and level and completenessof injury. Lung 173, 297–306.
lmenoff, P.L., Alexander, L.R., Spungen, A.M., Lesser, M., Bauman, W.A., 1995b.Bronchodilatory effects of ipratropium bromide in patients with tetraplegia.Paraplegia 33, 274–277.
merican Academy of Sleep Medicine Task Force, 1999. Sleep-related breathing dis-orders in adults: recommendations for syndrome for syndrome, definition, andmeasurement techniques in clinical research. Sleep 22, 667–689.
modie-Storey, C., Nash, M.S., Roussell, P.M., Knox, A.W., Crane, L.D., 1996. Headposition and its effect on pulmonary function in tetraplegic patients. Spinal Cord34, 602–607.
nke, A., Aksnes, A.K., Stanghelle, J.K., Hjeltnes, N., 1993. Lung volumes in tetraplegicpatients according to cervical spinal cord injury level. Scand. J. Rehabil. Med. 25,73–77.
shba, J., Garshick, E., Tun, C.G., Lieberman, S.L., Polakoff, D.F., Blanchard, J.D., Brown,R., 1993. Spirometry—acceptability and reproducibility in spinal cord injuredsubjects. J. Am. Paraplegia Soc. 16, 197–203.
xen, K., Pineda, H., Shunfenthal, I., Haas, F., 1985. Diaphragmatic function followingcervical cord injury: neurally mediated improvement. Arch. Phys. Med. Rehabil.66, 219–222.
yas, N.T., Garshick, E., Lieberman, S.L., Wien, M.F., Tun, C., Brown, R., 1999. Breath-lessness in spinal cord injury depends on injury level. J. Spinal Cord Med. 22,97–101.
yas, N.T., Epstein, L.J., Lieberman, S.L., Tun, C.G., Larkin, E.K., Brown, R., Garshick, E.,2001. Predictors of loud snoring in persons with spinal cord injury. J. Spinal CordMed. 24, 30–34.
ach, J.R., Wang, T.G., 1994. Pulmonary function and sleep disordered breathingin patients with traumatic tetraplegia: a longitudinal study. Arch. Phys. Med.Rehabil. 75, 279–284.
ake, B., Fugl-Meyer, A.R., Grimby, G., 1972. Breathing patterns and regional venti-lation distribution in tetraplegic patients and in normal subjects. Clin. Sci. 42,117–128.
arnes, P.J., 1986. Neural control of human airways in health and disease. Am. Rev.Respir. Dis. 134, 1289–1314.
aydur, A., Adkins, R.H., Milic-Emili, J., 2001. Lung mechanics in individuals withspinal cord injury: effects of injury level and posture. J. Appl. Physiol. 90, 405–411.
ergofsky, E.H., 1964a. Mechanism for respiratory insufficiency after cervical cordinjury; a source of alveolar hypoventilation. Ann. Intern. Med. 61, 435–447.
ergofsky, E.H., 1964b. Quantiation of the function of respiratory muscles in normalindividuals and quadriplegic patients. Arch. Phys. Med. Rehabil. 45, 575–580.
erlowitz, D.J., Brown, D.J., Campbell, D.A., Pierce, R.J., 2005. A longitudinal evalua-tion of sleep and breathing in the first year after cervical spinal cord injury. Arch.Phys. Med. Rehabil. 86, 1193–1199.
haskar, K.R., Brown, R., O’Sullivan, D.D., Melia, S., Duggan, M., Reid, L., 1991. Bronchialmucus hypersecretion in acute quadriplegia. Macromolecular yields and glyco-conjugate composition. Am. Rev. Respir. Dis. 143, 640–648.
iering-Sorensen, F., Biering-Sorensen, M., 2001. Sleep disturbances in the spinalcord injured: an epidemiological questionnaire investigation, including a normalpopulation. Spinal Cord 39, 505–513.
iering-Sorensen, M., Norup, P.W., Jacobsen, E., Biering-Sorensen, F., 1995. Treatmentof sleep apnoea in spinal cord injured patients. Paraplegia 33, 271–273.
luechardt, M.H., Wiens, M., Thomas, S.G., Plyley, M.J., 1992. Repeated measurementsof pulmonary function following spinal cord injury. Paraplegia 30, 768–774.
odin, P., Kreuter, M., Bake, B., Olsen, M.F., 2003. Breathing patterns during breathingexercises in persons with tetraplegia. Spinal Cord 41, 290–295.
onekat, H.W., Andersen, G., Squires, J., 1990. Obstructive disordered breathing dur-ing sleep in patients with spinal cord injury. Paraplegia 28, 392–398.
raun, S.R., Giovannoni, R., Levin, A.B., Harvey, R.F., 1982. Oxygen saturation duringsleep in patients with spinal cord injury. Am. J. Phys. Med. 61, 302–309.
rooks, D., O’Brien, K., 2005. Is inspiratory muscle training effective for individualswith cervical spinal cord injury? A qualitative systematic review. Clin. Rehabil.19, 237–246.
rown, R., DiMarco, A.F., Hoit, J.D., Garshick, E., 2006. Respiratory dysfunction andmanagement in spinal cord injury. Respir. Care 51, 853–867.
urns, S.P., Little, J.W., Hussey, J.D., Lyman, P., Lakshminarayanan, S., 2000. Sleepapnea syndrome in chronic spinal cord injury: associated factors and treatment.Arch. Phys. Med. Rehabil. 81, 1334–1339.
urns, S.P., Kapur, V., Yin, K.S., Buhrer, R., 2001. Factors associated with sleep apneain men with spinal cord injury: a population-based case-control study. SpinalCord 39, 15–22.
Neurobiology 166 (2009) 129–141
Burns, S.P., Rad, M.Y., Bryant, S., Kapur, V., 2005. Long-term treatment of sleep apneain persons with spinal cord injury. Am. J. Phys. Med. Rehabil. 84, 620–626.
Butler, J., Caro, C.G., Alcala, R., DuBois, A.B., 1960. Physiological factors affecting air-way resistance in normal subjects and in patients with obstructive respiratorydisease. J. Clin. Invest. 39, 584–591.
Cahan, C., Gothe, B., Decker, M.J., Arnold, J.L., Strohl, K.P., 1993. Arterial oxygen satura-tion over time and sleep studies in quadriplegic patients. Paraplegia 31, 172–179.
Canning, B.J., Fischer, A., 2001. Neural regulation of airway smooth muscle tone.Respir. Physiol. 125, 113–127.
Chen, C.F., Lien, I.N., Wu, M.C., 1990. Respiratory function in patients with spinal cordinjuries: effects of posture. Paraplegia 28, 81–86.
Cheng, P.T., Chen, C.-L., Wang, C.-M., Chung, C.-Y., 2006. Effect of neuromuscularelectrical stimulation on cough capacity and pulmonary function in patientswith acute cervical cord injury. J. Rehabil. Med. 38, 32–36.
Cockroft, D.W., Davis, B.E., 2006. Mechanism of airway hyperresponsiveness. J.Allergy Clin. Immunol. 118, 551–559.
Cotton, B.A., Pryor, J.P., Chinwalla, I., Wiebe, D.J., Reilly, P.M., Schwab, C.W., 2005. Res-piratory complications and mortality risk associated with thoracic spine injury.J. Trauma 59, 1400–1409.
Danon, J., Druz, W.S., Goldberg, N.B., Sharp, J.T., 1979. Function of the isolated paceddiaphragm and the cervical accessory muscles in C1 quadriplegics. Am. Rev.Respir. Dis. 119, 909–919.
Davis, C., Kannan, M.S., 1987. Sympathetic innervation of human tracheal andbronchial smooth muscle. Respir. Physiol. 68, 53–61.
Davis, C., Kannan, M.S., Jones, T.R., Daniel, E.E., 1982. Control of human airway smoothmuscle: in vitro studies. J. Appl. Physiol. 53, 1080–1087.
DeLuca, R.V., Grimm, D.R., Lesser, M., Bauman, W.A., Almenoff, P.L., 1999. Effects ofa beta2-agonist on airway hyperreactivity in subjects with cervical spinal cordinjury. Chest 115, 1533–1538.
Demedts, M., Beckers, J., Rochette, F., Bulche, J., 1982. Pulmonary function in mod-erate neuromuscular disease without respiratory complaints. Eur. J. Respir. Dis.63, 62–67.
De Troyer, A., Heilporn, A., 1980. Respiratory mechanics in quadriplegia. The respi-ratory function of the intercostal muscles. Am. Rev. Respir. Dis. 122, 591–600.
De Troyer, A., Estenne, M., Heilporn, A., 1986a. Mechanism of active expiration intetraplegic subjects. N. Engl. J. Med. 314, 740–744.
De Troyer, A., Estenne, M., Vincken, W., 1986b. Rib cage motion and muscle use inhigh tetraplegics. Am. Rev. Respir. Dis. 133, 1115–1119.
De Troyer, A., Estenne, M., 1991. The expiratory muscles in tetraplegia. Paraplegia 29,359–363.
DeVivo, M.J., Black, K.J., Stover, S.I., 1993. Causes of death during the first 12 yearsafter spinal cord injury. Arch. Phys. Med. Rehabil. 74, 248–254.
Dicpinigaitis, P.V., Spungen, A.M., Bauman, W.A., Absgarten, A., Almenoff, P.L., 1994a.Bronchial hyperresponsiveness after cervical spinal cord injury. Chest 105,1073–1076.
Dicpinigaitis, P.V., Spungen, A.M., Bauman, W.A., Absgarten, A., Almenoff, P.L., 1994b.Inhibition of bronchial hyperresponsiveness by the GABA-agonist baclofen.Chest 106, 758–761.
Dicpinigaitis, P.V., Grimm, D.R., Lesser, M., 1999. Cough reflex sensitivity in sub-jects with cervical spinal cord injury. Am. J. Respir. Crit. Care Med. 159,1660–1662.
Dicpinigaitis, P.V., Grimm, D.R., Lesser, M., 2000. Baclofen-induced cough suppres-sion in cervical spinal cord injury. Arch. Phys. Med. Rehabil. 81, 921–923.
DiMarco, A.F., 2005. Restoration of respiratory muscle function following spinal cordinjury. Review of electrical and magnetic stimulation techniques. Respir. Physiol.Neurobiol. 147, 273–287.
DiMarco, A.F., Onders, R.P., Ignagni, A., Kowalski, K.E., Mortimer, J.T., 2005a. Phrenicnerve pacing via intramuscular diaphragm electrodes in tetraplegic subjects.Chest 127, 671–678.
DiMarco, A.F., Takaoka, Y., Kowalski, K.E., 2005b. Combined intercostal anddiaphragm pacing to provide artificial ventilation in patients with tetraplegia.Arch. Phys. Med. Rehabil. 86, 1200–1207.
Doidge, J.M., Satchell, D.G., 1982. Adrenergic and non-adrenergic inhibitory nervesin mammalian airways. J. Auton. Nerv. Syst. 5, 83–99.
Estenne, M., Heilporn, A., Delhez, L., Yernault, J.-C., De Troyer, A., 1983. Chest wallstiffness in patients with chronic respiratory muscle weakness. Am. Rev. Respir.Dis. 128, 1002–1007.
Estenne, M., De Troyer, A., 1985. Relationship between respiratory muscle elec-tromyogram and rib cage motion in tetraplegia. Am. Rev. Respir. Dis. 132, 53–59.
Estenne, M., De Troyer, A., 1986. The effects of tetraplegia on chest wall statics. Am.Rev. Respir. Dis. 134, 121–124.
Estenne, M., De Troyer, A., 1987. Mechanism of the postural dependence of vitalcapacity in tetraplegic subjects. Am. Rev. Respir. Dis. 135, 367–371.
Estenne, M., Knoop, C., Vanvaerenbergh, J., Heilporn, A., De Troyer, A., 1989. Theeffect of pectoralis muscle training in tetraplegic subjects. Am. Rev. Respir. Dis.139, 1218–1222.
Estenne, M., De Troyer, A., 1990. Cough in tetraplegic subjects: an active process.Ann. Intern. Med. 112, 22–28.
Estenne, M., Gorini, M., 1992. Action of the diaphragm during cough in tetraplegicsubjects. J. Appl. Physiol. 72, 1074–1080.
Estenne, M., Van Muylem, A., Gorini, M., Kinnear, W., Heilporn, A., De Troyer, A., 1994.Evidence of dynamic airway compression during cough in tetraplegic patients.Am. J. Respir. Crit. Care Med. 150, 1081–1085.
Estenne, M., Van Muylem, A., Gorini, M., Kinnear, W., Heilporn, A., De Troyer, A., 1998.Effects of abdominal strapping on forced expiration in tetraplegic patients. Am.J. Respir. Crit. Care Med. 157, 95–98.

ology &
E
F
F
F
F
F
F
F
F
F
F
F
F
F
F
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
H
H
H
H
H
G.J. Schilero et al. / Respiratory Physi
stenne, M., Pinet, C., De Troyer, A., 2000. Abdominal muscle strength in patientswith tetraplegia. Am. J. Respir. Crit. Care Med. 161, 707–712.
ein, E.D., Grimm, D.R., Lesser, M., Bauman, W.A., Almenoff, P.L., 1998. The effectsof ipratropium bromide on histamine-induced bronchoconstriction in subjectswith cervical spinal cord injury. J. Asthma 35, 49–55.
erris, B.G., 1978. Epidemiology standardization project. Am. Rev. Respir. Dis. 118,1–120.
ish, J.E., Ankin, M.G., Kelly, J.F., Peterman, V.I., 1981. Regulation of bronchomotortone by lung inflation in asthmatic and nonasthmatic subjects. J. Appl. Physiol.50, 1079–1086.
ishburn, M.J., Marino, R.J., Ditunno Jr., J.F., 1990. Atelectasis and pneumonia in acutespinal cord injury. Arch. Phys. Med. Rehabil. 71, 197–200.
lavell, H., Marshall, R., Thornton, A.T., Clements, P.L., Antic, R., McEvoy, R.D., 1992.Hypoxia episodes during sleep in high tetraplegia. Arch. Phys. Med. Rehabil. 73,623–627.
lemons, W.W., Whitelaw, W.A., Brant, R., Remmers, J.E., 1994. Likelihood ratios for asleep apnea clinical prediction rule. Am. J. Respir. Crit. Care Med. 150, 1279–1285.
orner, J.V., 1980. Lung volumes and mechanics of breathing in tetraplegics. Paraple-gia 18, 258–266.
rankel, H.L., Guz, A., Noble, M., 1971. Respiratory sensations in patients with cervicalcord transection. Paraplegia 9, 132–136.
risbie, J.H., Brown, R., 1994. Waist and neck enlargement after quadriplegia. J. Am.Paraplegia Soc. 17, 177–178.
ugl-Meyer, A.R., 1971. Effects of respiratory muscle paralysis in tetraplegic andparaplegic patients. Scand. J. Rehabil. Med. 3, 141–150.
ugl-Meyer, A.R., Grimby, G., 1971a. Ventilatory function in tetraplegic patients.Scand. J. Rehabil. Med. 3, 151–160.
ugl-Meyer, A.R., Grimby, G., 1971b. Rib-cage and abdominal volume ventilationpartitioning in tetraplegic patients. Scand. J. Rehabil. Med. 3, 161–167.
ugl-Meyer, A.R., Grimby, G., 1984. Respiratory in tetraplegia and in hemiplegia: areview. Int. Rehabil. Med. 6, 186–190.
ujiwara, T., Hara, Y., Chino, N., 1999. Expiratory function in complete tetraplegics:study of spirometry, maximal expiratory pressure, and muscle activity of pec-toralis major and latissimus dorsi muscles. Am. J. Phys. Med. Rehabil. 78,464–469.
ibson, G.J., Pride, N.B., Davis, J.N., Loh, L.C., 1977. Pulmonary mechanics in patientswith respiratory muscle weakness. Am. Rev. Respir. Dis. 115, 389–395.
lenn, W.W., Hogan, J.F., Loke, J.S., Ciesielski, T.E., Phelps, M.L., Rowedder, R., 1984.Ventilatory support by pacing of the conditioned diaphragm in quadriplegia. N.Engl. J. Med. 310, 1150–1155.
oldman, J.M., Rose, L.S., Williams, S.J., Silver, J.R., Denison, D.M., 1986. Effect ofabdominal binders on breathing in tetraplegic patients. Thorax 41, 940–945.
oldman, J.M., Williams, S.J., Denison, D.M., 1988. The rib cage and abdominal com-ponents of respiratory system compliance in tetraplegic patients. Eur. Respir. J.1, 242–247.
oldman, M.D., Mead, J., 1973. Mechanical interaction between the diaphragm andrib cage. J. Appl. Physiol. 35, 197–204.
orini, M., Corrado, A., Aito, S., Ginanni, R., Villella, G., Lucchesi, G., De Paola, E.,2000. Ventilatory and respiratory muscle responses to hypercapnia in patientswith paraplegia. Am. J. Respir. Crit. Care Med. 162, 203–208.
ottfried, S.B., Leech, I., DiMarco, A.F., Zaccardelli, W., Altose, M.D., 1984. Sensation ofrespiratory force following low cervical spinal cord transection. J. Appl. Physiol.57, 989–994.
ounden, P., 1990. Progressive resistive loading on accessory expiratory muscle intetraplegia. S. Afr. J. Physiother. 46, 4–15.
ounden, P., 1997. Static respiratory pressures in patients with post-traumatictetraplegia. Spinal Cord 35, 43–47.
randas, N.F., Jain, N.B., Denckla, J.B., Brown, R., Tun, C.G., Gallagher, M.E., Garshick,E., 2005. Dyspnea during daily activities in chronic spinal cord injury. Arch. Phys.Med. Rehabil. 86, 1631–1635.
rimm, D.R., DeLuca, R.V., Lesser, M., Bauman, W.A., Almenoff, P.L., 1997. Effects ofGABA-B agonist baclofen on bronchial hyperreactivity to inhaled histamine insubjects with cervical spinal cord injury. Lung 175, 333–341.
rimm, D.R., Arias, E., Lesser, M., Bauman, W.A., Almenoff, P.L., 1999. Airway hyper-responsiveness to ultrasonically nebulized distilled water in subjects withtetraplegia. J. Appl. Physiol. 86, 1165–1169.
rimm, D.R., Chandy, D., Almenoff, P.L., Schilero, G., Lesser, M., 2000. Airway hyper-reactivity in subjects with tetraplegia is associated with reduced baseline airwaycaliber. Chest 118, 1397–1404.
rimm, D.R., Schilero, G.J., Spungen, A.M., Bauman, W.A., Lesser, M., 2006. Salmeterolimproves pulmonary function in persons with tetraplegia. Lung 184, 335–339.
uttmann, L., Silver, J.R., 1965. Electromyographic studies on reflex activity ofthe intercostal and abdominal muscles in cervical cord lesions. Paraplegia 3,1–22.
art, N., Laffont, I., de La Sota, A.P., Lejaille, M., Macadou, G., Polkey, M.I., Denys, P.,Lafaso, F., 2005. Respiratory effects of combined truncal and abdominal supportin patients with spinal cord injury. Arch. Phys. Med. Rehabil. 86, 1447–1451.
aas, A., Lowman, D.W., Bergofsky, E.H., 1965. Impairment of respiration after spinalcord injury. Arch. Phys. Med. Rehabil. 46, 399–405.
aas, F., Axen, K., Pineda, H., Gandino, D., Haas, A., 1985. Temporal pulmonary func-
tion changes in cervical cord injury. Arch. Phys. Med. Rehabil. 66, 139–144.emingway, A., Bors, E., Hobby, R.P., 1958. An investigation of the pulmonary functionof paraplegics. J. Clin. Invest. 37, 773–782.
eritier, F., Rahm, F., Pasche, P., Fitting, J.-W., 1994. Sniff nasal inspiratory pressure. Anoninvasive assessment of inspiratory muscle strength. Am. J. Respir. Crit. CareMed. 150, 1678–1683.
Neurobiology 166 (2009) 129–141 139
Hiraizumi, Y., Fujimaki, E., Hishida, T., Maruyama, T., Takeuchi, M., 1986. Regional lungperfusion and ventilation with radioisotopes in cervical cord-injured patients.Clin. Nucl. Med. 11, 352–357.
Hoffstein, V., Zamel, N., Phillipson, E.A., 1984. Lung volume dependence of pha-ryngeal cross-sectional area in patients with obstructive sleep apnea. Am. Rev.Respir. Dis. 130, 175–178.
Hopman, M.T., van der Woude, Dallmeijer, A.J., Snoek, G., Folgering, H.T.M., 1997. Res-piratory muscle strength and endurance in individuals with tetraplegia. SpinalCord 35, 104–108.
Im Hof, V., Dubo, H., Daniels, V., Younes, M., 1986. Steady-state responseof quadriplegic subjects to inspiratory resistive load. J. Appl. Physiol. 60,1482–1492.
Inkley, S.R., Oldenburg, F.C., Vignos, P.J., 1974. Pulmonary function in Duchenne mus-cular dystrophy related to stage of disease. Am. J. Med. 56, 297–306.
Jaeger, R.J., Turba, R.M., Yarkony, G.M., Roth, E.J., 1993. Cough in spinal cord injuredpatients: comparison of three methods to produce cough. Arch. Phys. Med. Reha-bil. 74, 1358–1361.
Jain, N.B., Brown, R., Tun, C.G., Gagnon, D., Garshick, E., 2006. Determinants of forcedexpiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVCin chronic spinal cord injury. Arch. Phys. Med. Rehabil. 87, 1327–1333.
Jenkinson, C., Davies, R.J., Mullins, R., Stradling, J.R., 1999. Comparison of ther-apeutic and subtherapeutic nasal continuous positive airway pressure forobstructive sleep apnoea: a randomised prospective parallel trial. Lancet 353,2100–2105.
Kakkar, R.K., Berry, R.B., 2007. Positive airway pressure treatment for obstructivesleep apnea. Chest 132, 1057–1072.
Klefbeck, B., Sternhag, M., Weinberg, J., Levi, R., Hultling, C., Borg, J., 1998. Obstructivesleep apneas in relation to severity of cervical spinal cord injury. Spinal Cord 36,621–628.
Kelley, A., Garshick, E., Gross, E.R., Lieberman, S.L., Tun, C.G., Brown, R., 2003. Spirom-etry testing standards in spinal cord injury. Chest 123, 725–730.
Kelling, J.S., DiMarco, A.F., Gottfried, S.B., Altose, M.D., 1985. Respiratory responsesto ventilatory loading following low cervical spinal cord injury. J. Appl. Physiol.59, 1752–1756.
Kokkola, K., Moller, K., Lehtonen, T., 1975. Pulmonary function in tetraplegic andparaplegic patients. Ann. Clin. Res. 7, 76–79.
Koskenvuo, M., Kaprio, J., Telakivi, T., Partinen, M., Heikkila, K., Sarna, S., 1987. Snoringas a risk factor for ischaemic heart disease and stroke in men. Br. Med. J. (Clin.Res. Ed.) 294, 16–19.
Koulouris, N., Mulvey, D.A., Laroche, C.M., Green, M., Moxham, J., 1988. Comparison oftwo different mouthpieces for the measurement of Pimax and Pemax in normaland weak subjects. Eur. Respir. J. 1, 863–867.
Koulouris, N., Mulvey, D.A., Laroche, C.M., Sawicka, E.H., Green, M., Moxham, J., 1989.The measurement of inspiratory muscle strength by sniff esophageal, nasopha-ryngeal, and mouth pressures. Am. Rev. Respir. Dis. 139, 641–646.
Laitinen, A., Partanen, M., Hervonen, A., Laitinen, L.A., 1985. Electron microscopicstudy on the innervation of the human lower respiratory tract: evidence ofadrenergic nerves. Eur. J. Respir. Dis. 67, 209–215.
Lammers, J-W.J., Minette, P., McCusker, M.T., Chung, K.F., Barnes, P.J., 1988. Nona-drenergic bronchodilator mechanisms in normal human subjects in vivo. J. Appl.Physiol. 64, 1817–1822.
Langbein, W.E., Maloney, C., Kandare, F., Stanic, U., Nemchausky, B., Jaeger, R.J., 2001.Pulmonary function testing in spinal cord injury: effects of abdominal musclestimulation. J. Rehabil. Res. Dev. 38, 591–597.
Laroche, C.M., Mier, A.K., Moxham, J., Green, M., 1988. The value of sniff esophagealpressures in the assessment of global inspiratory muscle strength. Am. Rev.Respir. Dis. 138, 598–603.
Ledsome, J.R., Sharp, J.M., 1981. Pulmonary function in acute cervical cord injury.Am. Rev. Respir. Dis. 124, 41–44.
Leduc, B.E., Dagher, J.H., Mayer, P., Bellemare, F., Lepage, Y., 2007. Estimated preva-lence of obstructive sleep apnea-hypopnea syndrome after cervical cord injury.Arch. Phys. Med. Rehabil. 88, 333–337.
Liaw, M.-Y., Lin, M.-C., Cheng, P.-T., Wong, M-K.A., Tang, F.-T., 2000. Resistive inspira-tory muscle training: its effectiveness in patients with acute complete cervicalcord injury. Arch. Phys. Med. Rehabil. 81, 752–756.
Lin, K.H., Wu, H.D., Chang, C.W., Wang, T.G., Wang, Y.H., 1998. Ventilatory and mouthocclusion pressure responses to hypercapnia in chronic tetraplegia. Arch. Phys.Med. Rehabil. 79, 795–799.
Lin, K.H., Lai, Y.L., Wu, H.D., Wang, T.O., Wang, Y.H., 1999. Cough threshold in peoplewith spinal cord injuries. Phys. Ther. 79, 1026–1031.
Lin, V.W., Hsiao, I.N., Zhu, E., Perkash, I., 2001. Functional magnetic stimulation forconditioning of expiratory muscles in patients with spinal cord injury. Arch. Phys.Med. Rehabil. 82, 162–166.
Linder, S.H., 1993. Functional electrical stimulation to enhance cough in quadriplegia.Chest 103, 166–169.
Linn, W.S., Adkins, R.H., Gong, H., Waters, R.L., 2000. Pulmonary function in chronicspinal cord injury: a cross-sectional survey of 222 southern California adultoutpatients. Arch. Phys. Med. Rehabil. 81, 757–763.
Linn, W.S., Spungen, A.M., Gong, H., Adkins, R.H., Bauman, W.A., Waters, R.L., 2001.Forced vital capacity in two large outpatient populations with chronic spinal
cord injury. Spinal Cord 39, 263–268.Linn, W.S., Spungen, A.M., Gong, H., Bauman, W.A., Adkins, R.H., Waters, R.L., 2003.Smoking and obstructive lung dysfunction in persons with chronic spinal cordinjury. J. Spinal Cord Med. 26, 28–35.
Lougheed, M.D., Flannery, J., Webb, K.A., O’Donnell, D.E., 2002. Respiratory sensationand ventilatory mechanics during induced bronchoconstriction in sponta-

1 ology &
L
L
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
N
N
N
O
O
O
P
P
P
40 G.J. Schilero et al. / Respiratory Physi
neously breathing low cervical quadriplegia. Am. J. Respir. Crit. Care Med. 166,370–376.
overidge, B., Badour, M., Dubo, H., 1989. Ventilatory muscle endurance training inquadriplegia: effects on breathing pattern. Paraplegia 27, 329–339.
overidge, B.M., Dubo, H.I., 1990. Breathing pattern in chronic quadriplegia. Arch.Phys. Med. Rehabil. 71, 495–499.
aloney, F.P., 1979. Pulmonary function in quadriplegia: effects of a corset. Arch.Phys. Med. Rehabil. 60, 261–265.
an, W.D., Dyroussis, D., Fleming, T.A., Chetta, A., Harraf, F., Mustfa, N., Rafferty,G.F., Polkey, M.I., Moxham, J., 2003. Cough gastric pressure and maximumexpiratory mouth pressure in humans. Am. J. Respir. Crit. Care Med. 168,714–717.
anning, H.L., Brown, R., Scharf, S.M., Leith, D.E., Weiss, J.W., Weinberger, S.E.,Schwartzstein, R.M., 1992a. Ventilatory and P0.1 response to hypercapnia inquadriplegia. Respir. Physiol. 89, 97–112.
anning, H.L., McCool, F.D., Scharf, S.M., Garshick, E., Brown, R., 1992b. Oxygen costof resistive-loaded breathing in quadriplegia. J. Appl. Physiol. 73, 825–831.
ateus, S.R., Beraldo, P.S.S., Horan, T.A., 2006. Cholinergic bronchomotor tone andairway caliber in tetraplegic patients. Spinal Cord 44, 269–274.
ateus, S.R., Beraldo, P.S., Horan, T.A., 2007. Maximal static mouth respiratory pres-sure in spinal cord injured patients: correlation with motor level. Spinal Cord45, 569–575.
cArdle, N., Devereux, G., Heidarnejad, H., Engleman, H.M., Mackay, T.W., Douglas,N.J., 1999. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome.Am. J. Respir. Crit. Care Med. 159, 1108–1114.
cCool, F.D., Pichurko, B.M., Slutsky, A.S., Sarkarati, M., Rossier, A., Brown, R., 1986.Changes in lung volume and rib cage configuration with abdominal binding inquadriplegia. J. Appl. Physiol. 60, 1198–1202.
cCool, F.D., Brown, R., Mayewski, R.J., Hyde, R.W., 1988. Effects of posture on stim-ulated ventilation in quadriplegia. Am. Rev. Respir. Dis. 138, 101–105.
cEvoy, R.D., Mykytyn, I., Sajkov, D., Flavell, H., Marshall, R., Antic, R., Thornton, A.T.,1995. Sleep apnoea in patients with quadriplegia. Thorax 50, 613–619.
cMichan, J.C., Michel, L., Westbrook, P.R., 1980. Pulmonary dysfunction follow-ing traumatic quadriplegia. Recognition, prevention, and treatment. JAMA 243,528–531.
ead, J., Banzett, R.B., Lehr, J., Loring, S.H., O’Cain, C.F., 1984. Effect of posture onupper and lower rib cage motion and tidal volume during diaphragm pacing.Am. Rev. Respir. Dis. 130, 320–321.
iller, M.R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A., Crapo, R.,Enright, P., van der Grinten, C.P., Gustafsson, P., Jensen, R., Johnson, D.C., MacIn-tyre, N., McKay, R., Navajas, D., Pedersen, O.F., Pellegrino, R., Viegi, G., Wanger,J., ATS/ERS Task Force, 2005. Standardisation of spirometry. Eur. Respir. J. 26,319–338.
oore, B.J., Verburgt, L.M., King, G.G., Pare, P.D., 1997. The effect of deep inspirationon methacholine dose-response curves in normal subjects. Am. J. Respir. Crit.Care Med. 156, 1278–1281.
oreno, R.H., Hogg, J.C., Pare, P.D., 1986. Mechanics of airway narrowing. Am. Rev.Respir. Dis. 133, 1171–1180.
oulton, A., Silver, J.R., 1970. Chest movements in patients with traumatic injuriesof the cervical cord. Clin. Sci. 39, 407–422.
ueller, G., de Groot, S., van der Woude, L., Hopman, M.T.E., 2008. Time-courses oflung function and respiratory muscle pressure generating capacity after spinalcord injury; a prospective cohort study. J. Rehabil. Med. 40, 269–276.
urphy, R.J., Hartkopp, A., Gardiner, P.F., Kjaer, M., Beliveau, L., 1999. Salbutamoleffect in spinal cord injured individuals undergoing functional electrical stimu-lation training. Arch. Phys. Med. Rehabil. 80, 1264–1267.
yers, J., Lee, M., Kiratli, J., 2007. Cardiovascular disease in spinal cord injury: anoverview of prevalence, risk, evaluation, and management. Am. J. Phys. Med.Rehabil. 86, 142–152.
ava, S., Rubini, F., Zanotti, E., Caldiroli, D., 1996. The tension-time index of thediaphragm revisited in quadriplegic patients with diaphragm pacing. Am. J.Respir. Crit. Care Med. 153, 1322–1327.
ieto, F.J., Young, T.B., Lind, B.K., Shahar, E., Samet, J.M., Redline, S., D’Agostino,R.B., Newman, A.B., Lebowitz, M.D., Pickering, T.G., 2000. Associationof sleep-disordered breathing, sleep apnea, and hypertension in a largecommunity-based study. Sleep Heart Health Study. JAMA 283, 1829–1836.
oppen, M., Vincken, W., 1996. Thoracoscopic sympathicolysis for essential hyper-hidrosis: effects on pulmonary function. Eur. Respir. J. 9, 1660–1664.
’Donnell, D.E., Sanii, R., Dubo, H., Loveridge, B., Younes, M., 1993. Steady-state venti-latory responses to expiratory resistive loading in quadriplegics. Am. Rev. Respir.Dis. 147, 54–59.
hry, A., Molho, M., Rozin, R., 1975. Alterations of pulmonary function in spinal cordinjured patients. Paraplegia 13, 101–108.
o, T., Watt, J.W., Soni, B.M., Sett, P.K., 1999. Delayed diaphragm recovery in 12patients after high cervical spinal cord injury. A retrospective review of thediaphragm status of 107 patients ventilated after acute spinal cord injury. SpinalCord 37, 117–122.
artanen, M., Laitinen, A., Hervonen, A., Toivanen, M., Laitinen, L.A., 1982.Catecholamine- and acetylcholinesterase-containing nerves in human lowerrespiratory tract. Histochemistry 76, 175–188.
ellegrino, R., Sterk, P.J., Sont, J.K., Brusasco, V., 1998. Assessing the effect of deepinhalation on airway calibre: a novel approach to lung function in bronchialasthma and COPD. Eur. Respir. J. 12, 1219–1227.
okorski, M., Morikawa, T., Takaishi, S., Masuda, A., Ahn, B., Honda, Y., 1990. Ventila-tory responses to chemosensory stimuli in quadriplegic subjects. Eur. Respir. J.3, 891–900.
Neurobiology 166 (2009) 129–141
Racke, K., Matthiesen, S., 2004. The airway cholinergic system: physiology and phar-macology. Pulm. Pharmacol. Ther. 17, 181–198.
Radulovic, M., Schilero, G.J., Wecht, J.M., Weir, J.P., Spungen, A.M., Bauman, W.A.,Lesser, M., 2008. Airflow obstruction reversibility in spinal cord injury: evidencefor functional sympathetic innervation. Arch. Phys. Med. Rehabil. 89, 2349–2353.
Richardson, J.B., Ferguson, C.C., 1979. Neuromuscular structure and function in theairways. Fed. Proc. 38, 202–208.
Roth, E.J., Nussbaum, S.B., Berkowitz, M., Primack, S., Oken, J., Powley, S., Lu, A., 1995.Pulmonary function testing in spinal cord injury: correlation with vital capacity.Paraplegia 33, 454–457.
Rubinstein, I., Slutsky, A.S., Rebuck, A.S., McClean, P.A., Boucher, R., Szeinberg, A.,Zamel, N., 1988. Assessment of maximal expiratory pressure in healthy adults.J. Appl. Physiol. 64, 2215–2219.
Sajkov, D., Marshall, R., Walker, P., Mykytyn, I., McEvoy, R.D., Wale, J., Flavell, H.,Thornton, A.T., Antic, R., 1998. Sleep apnoea related hypoxia is associated withcognitive disturbances in patients with tetraplegia. Spinal Cord 36, 231–239.
Scanlon, P.D., Loring, S.H., Pichurko, B.M., McCool, F.D., Slutsky, A.S., Sarkarati, M.,Brown, R., 1989. Respiratory mechanics in acute quadriplegia. Lung and chestwall compliance and dimensional changes during respiratory maneuvers. Am.Rev. Respir. Dis. 139, 615–620.
Schilero, G.J., Grimm, D.R., Bauman, W.A., Lenner, R., Lesser, M., 2005. Assessment ofairway caliber and bronchodilator responsiveness in subjects with spinal cordinjury. Chest 127, 149–155.
Schmid, A., Huonker, M., Stahl, F., Barturen, J.-M., Konig, D., Heim, M., Lehmann, M.,Keul, J., 1998. Free plasma catecholamines in spinal cord injured persons withdifferent injury levels at rest and during exercise. J. Auton. Nerv. Syst. 68, 96–100.
Shahar, E., Whitney, C.W., Redline, S., Lee, E.T., Newman, A.B., Javier Nieto, F.,O’Connor, G.T., Boland, L.L., Schwartz, J.E., Samet, J.M., 2001. Sleep-disorderedbreathing and cardiovascular disease: cross-sectional results of the Sleep HeartHealth Study. Am. J. Respir. Crit. Care Med. 163 (1), 19–25.
Short, D.J., Stradling, J.R., Williams, S.J., 1992. Prevalence of sleep apnoea in patientsover 40 years of age with spinal cord lesions. J. Neurol. Neurosurg. Psychiatry 55,1032–1036.
Siebens, A.A., Kirby, N.A., Poulos, D.A., 1964. Cough following transection of spinalcord at C-6. Arch. Phys. Med. Rehabil. 45, 1–8.
Signorile, J.F., Banovac, K., Gomez, M., Flipse, D., Caruso, J.F., Lowensteyn, I., 1995.Increased muscle strength in paralyzed patients after spinal cord injury: effectof beta-2 adrenergic agonist. Arch. Phys. Med. Rehabil. 76, 55–58.
Silver, J.R., 1963. The oxygen cost of breathing in tetraplegic patients. Paraplegia 1,204–214.
Sin, D.D., Mayers, I., Man, G.C., Ghahary, A., Pawluk, L., 2002. Can continuous posi-tive airway pressure therapy improve the general health status of patients withobstructive sleep apnea? A clinical effectiveness study. Chest 122, 1679–1685.
Singas, E., Lesser, M., Spungen, A.M., Bauman, W.A., Almenoff, P.L., 1996. Airwayhyperresponsiveness to methacholine in subjects with spinal cord injury. Chest110, 911–915.
Singas, E., Grimm, D.R., Almenoff, P.L., Lesser, M., 1999. Inhibition of airway hyper-reactivity by oxybutynin chloride in subjects with cervical spinal cord injury.Spinal Cord 37, 279–283.
Skloot, G., Permutt, S., Togias, A., 1995. Airway hyperresponsiveness in asthma: aproblem of limited smooth muscle relaxation with inspiration. J. Clin. Invest. 96,2393–2403.
Slonimski, M., Aguilera, E.J., 2001. Atelectasis and mucus plugging in spinal cordinjury: case report and therapeutic approaches. J. Spinal Cord Med. 24, 284–288.
Spungen, A.M., Dicpinigaitis, P.V., Almenoff, P.L., Bauman, W.A., 1993. Pulmonaryobstruction in individuals with cervical spinal cord lesions unmasked by bron-chodilator administration. Paraplegia 31, 404–407.
Spungen, A.M., Grimm, D.R., Lesser, M., Bauman, W.A., Almenoff, P.L., 1997. Self-reported prevalence of pulmonary symptoms in subjects with spinal cord injury.Spinal Cord 35, 652–657.
Spungen, A.M., Grimm, D.R., Schilero, G.J., Lenner, R., Oei, E., Bauman, W., Almenoff,P.L., Lesser, M., 2002. Relationship of respiratory symptoms with smoking statusand pulmonary function in chronic spinal cord injury. J. Spinal Cord Med. 25,23–27.
Spungen, A.M., Adkins, R.H., Stewart, C.A., Wang, J., Pierson, R.N., Waters, R.L., Bau-man, W.A., 2003. Factors influencing body composition in persons with spinalcord injury: a cross-sectional study. J. Appl. Physiol. 95, 2398–2407.
Standardization of Spirometry, 1995. 1994 Update. American Thoracic Society. Am.J. Respir. Crit. Care Med. 152, 1107–1136.
Stanic, U., Kandare, F., Jaeger, R., Sorli, J., 2000. Functional electrical stimulation ofabdominal muscles to augment tidal volume in spinal cord injury. IEEE Trans.Rehabil. Eng. 8, 30–34.
Stefanutti, D., Benoist, M.-R., Scheinmann, P., Chaussain, M., Fitting, J.-W., 2000.Usefulness of sniff nasal pressure in patients with neuromuscular or skeletaldisorders. Am. J. Respir. Crit. Care Med. 162, 1507–1511.
Stepp, E.L., Brown, R., Tun, C.G., Gagnon, D.R., Jain, N.B., Garshick, E., 2008. Determi-nants of lung volumes in chronic spinal cord injury. Arch. Phys. Med. Rehabil. 89,1499–1506.
Stiller, K., Huff, N., 1999. Respiratory muscle training for tetraplegic patients: a liter-ature review. Aust. J. Physiother. 45, 291–299.
Stockhammer, E., Tobon, A., Michel, F., Eser, P., Scheuler, W., Bauer, W., Baumberger,M., Muller, W., Kakebeeke, T.H., Knecht, H., Zach, G.A., 2002. Characteristics ofsleep apnea syndrome in tetraplegic patients. Spinal Cord 40, 286–294.
Stolzmann, K.L., Gagnon, D.R., Brown, R., Tun, C.G., Garshick, E., 2008. Longitudinalchange in FEV1 and FVC in chronic spinal cord injury. Am. J. Respir. Crit. CareMed. 177, 781–786.

ology &
S
T
TT
T
T
T
U
V
Wien, M.F., Garshick, E., Tun, C.G., Lieberman, S.L., Kelley, A., Brown, R., 1999.Breathlessness and exercise in spinal cord injury. J. Spinal Cord Med. 22,
G.J. Schilero et al. / Respiratory Physi
tone, D.J., Keltz, H., 1963. The effect of respiratory muscle dysfunction on pulmonaryfunction. Studies in patients with spinal cord injuries. Am. Rev. Respir. Dis. 88,621–629.
homaz, S., Beraldo, P., Mateus, S., Horan, T., Leal, J.C., 2005. Effects of partial isother-mic immersion on the spirometry parameters of tetraplegic patients. Chest 128,184–189.
obin, M.J., 1992. Breathing pattern analysis. Intensive Care Med. 18, 193–201.ow, A.M.P-E., Graves, D.E., Carter, R.E., 2001. Vital capacity in tetraplegics twenty
years and beyond. Spinal Cord 39, 139–144.seng, M.-Y., Tseng, J.-H., 2001. Thoracoscopic sympathectomy for palmar hyper-
hidrosis: effects on pulmonary function. J. Clin. Neurosci. 8, 539–541.ully, K., Koke, K., Garshick, E., Lieberman, S.L., Tun, C.G., Brown, R., 1997. Maximal
expiratory pressures in spinal cord injury using two mouthpieces. Chest 112,113–116.
zelepis, G.E., Bascom, A.T., Badr, M.S., Goshgarian, H.G., 2006. Effects of theophyllineon pulmonary function in patients with traumatic tetraplegia. J. Spinal Cord Med.29, 227–233.
rmey, W., Loring, S., Mead, J., Slutsky, A.S., Sarkarati, M., Rossier, A., Brown, R., 1986.Upper and lower rib cage deformation during breathing in quadriplegics. J. Appl.Physiol. 60, 618–622.
an Houtte, S., Vanlandewijck, Y., Gosselink, R., 2006. Respiratory muscle train-ing in persons with spinal cord injury: a systematic review. Respir. Med. 100,1886–1895.
Neurobiology 166 (2009) 129–141 141
Van Houtte, S., Vanlandewijck, Y., Kiekens, C., Spengler, C.M., Gosselink, R., 2008.Patients with acute spinal cord injury benefit from normocapnic hyperpnoeatraining. J. Rehabil. Med. 40, 119–125.
Van Noord, J.A., Smeets, J., Clement, J., Van de Woestijne, K.P., Demedts, M., 1994.Assessment of reversibility of airflow obstruction. Am. J. Respir. Crit. Care Med.150, 551–554.
Vigil, L., Calaf, N., Codina, E., Fibla, J.J., Gomez, G., Casan, P., 2005. Video-assisted sym-pathectomy for essential hyperhidrosis: effects on cardiopulmonary function.Chest 128, 2702–2705.
Wadsworth, B.M., Haines, T.P., Cornwell, P.L., Paratz, J.D., 2008. Abdominal binderuse in people with spinal cord injuries: a systematic review and meta-analysis.Spinal Cord.
Wasicko, M.J., Hutt, D.A., Parisi, R.A., Neubauer, J.A., Mezrich, R., Edelman, N.H., 1990.The role of vascular tone in the control of upper airway collapsibility. Am. Rev.Respir. Dis. 141, 1569–1577.
297–302.Young, T., Palta, M., Dempsey, J., Skatrud, J., Weber, S., Badr, S., 1993. The occurrence
of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 328,1230–1235.