Embed Size (px)
Citation preview

Pulmonary Embolism inOrthopaedic Patients: Diagnosisand Management
Abstract
Orthopaedic patients are at particularly high risk for pulmonaryembolism. There has been a trend recently toward overdiagnosisof pulmonary embolism; thus, evaluation of the nature of a clinicallyrelevant pulmonary embolism is needed, as is assessment of thetiming, risks, and outcomes of therapeutic anticoagulation insurgical patients. Recent literature shows the incidence ofpulmonary embolism to be increasing without a correspondingincrease in mortality, suggesting that not all emboli may beclinically relevant and that increasingly sensitive tests may bepicking up small emboli. The size and location of a clot or clotsmay matter when deciding on management. A risk-benefitevaluation can assist in deciding treatment.
Orthopaedic patients are at highrisk for both pulmonary embo-
lism (PE) and deep vein thrombosis(DVT). These disorders have beenwell studied in the arthroplasty pop-ulation; an American Academy ofOrthopaedic Surgeons guideline isavailable for public access.1 How-ever, this guideline does not applyto the nonarthroplasty orthopaedicpopulation and addresses prophy-laxis rather than management. Here,we discuss the diagnosis and man-agement of PE in general orthopae-dics, particularly trauma.
Symptomatic PE occurs in 2% to10% of pelvic trauma patients, andfatal PE, in 0.5% to 2%.2 Deep veinthrombi appear to occur with greaterincidence in proximal rather thandistal lower extremity fractures, al-though the clinical significance ofthis finding is unclear.3 The mostcommon signs of PE are tachycardia,low oxygen saturation, and short-ness of breath; however, the clinicalpresentation of PE is notoriously un-
reliable, and many embolisms are si-lent. In a review of 695 patients, Kimet al4 found a 27.8% rate of positiveCT results for PE in postoperativeorthopaedic patients. In that study, aprior history of thromboembolic dis-ease was the only significant predic-tor of a positive scan; a high bodymass index was a marginal predictor.Thus, a combination of patient char-acteristics and symptoms may pre-dict PE.
The magnitude of PE is a spectrumranging from central large clots totiny subsegmental clots. The clinicalrelevance of this spectrum of condi-tion is also quite varied. It is wellknown that untreated emboli canlead to death; however, many haveno clinical sequelae. How, then,should management such as aggres-sive anticoagulation, which has itsown risks and costs, be chosen? Asmethods of embolus detection be-come more sensitive for smaller oc-clusions, the clinical significance ofthese small emboli is called into
Paul Tornetta, MD
Yelena Bogdan, MD
From Boston University MedicalCenter, Boston, MA.
Dr. Tornetta or an immediate familymember serves as a paid consultantto or is an employee of, and hasreceived royalties from, Smith &Nephew, and serves as a boardmember, owner, officer, orcommittee member of the AmericanOrthopaedic Association and theOrthopaedic Trauma Association.Neither Dr. Bogdan nor anyimmediate family member hasreceived anything of value from orhas stock or stock options held in acommercial company or institutionrelated directly or indirectly to thesubject of this article.
J Am Acad Orthop Surg 2012;20:586-595
http://dx.doi.org/10.5435/JAAOS-20-09-586
Copyright 2012 by the AmericanAcademy of Orthopaedic Surgeons.
Review Article
586 Journal of the American Academy of Orthopaedic Surgeons

question. Is the management we areinstituting rational, or are we over-treating some percentage of patients?
Diagnostic Methods andTime Trends
PE is diagnosed in several ways.Clinically, many patients do notpresent with the classic symptoms ofpleuritic chest pain and shortness ofbreath. Often, unexplained tachycar-dia in a postoperative patient, com-bined with low oxygen saturation, isall that is needed to prompt a searchfor PE. D-dimer, a blood test thatmeasures fibrin degradation, may beelevated in patients with PE, but it isalso elevated in postoperative pa-tients generally and is thus unreliableas a standalone diagnostic test. TheWells score has undergone numerousiterations and remains one of themost popular clinical predictionmodels for PE diagnosis.5 The Wellsscore assigns points based on patientcharacteristics and, when combinedwith the D-dimer level, can be a veryuseful predictive tool (Tables 1 and2). However, this score has been de-veloped primarily from a nonsurgicalpatient population and thus may notapply to orthopaedic injury patients.
With regard to imaging studies forthe diagnosis of PE, pulmonary an-giography is the benchmark, but it isexpensive and invasive. The two ma-
jor and most common imaging diag-nostic modalities are CT pulmonaryangiogram (CTPA) and ventilationperfusion (VQ) scanning. The advan-tages of CTPA are direct visualiza-tion of the clot, high sensitivity, iden-tification of alternative pathology,and rapid testing time. The advan-tages of VQ scanning are low radia-tion exposure and low cost. A ran-domized trial comparing the twomethods in 1,417 patients showedthat CTPA had a higher positive pre-dictive value than did VQ scanningbut that the two methods were simi-lar in ruling out PEs.6 The negativepredictive value of CTPA appears tobe adequate; a meta-analysis of 23studies showed that the 3-month rateof recurrent, symptomatic PE in4,657 patients with high clinical sus-picion for PE and a negative CTPAwas 1.4%.7 One study in patientswith moderate to high probabilityfor PE and/or elevated D-dimer levelsgave the negative predictive value ofCTPA as 99.5%.8 CTPA is now themost common diagnostic method forPE, but it is used as part of an over-all approach that includes clinicalprediction, ultrasonography, andother modalities.
General time trends from the pastdecade show that the incidence of PEis increasing. In a sample of morethan 1 million patients from the Na-tionwide Inpatient Sample database,
the number of PE diagnoses in-creased from 126,546 cases in 1998to 229,637 in 2005, but fatal PErates dropped from 12.3% to 8.2%.9
The decreases in mortality rate maysuggest that management of PE be-
Table 2
Pulmonary Embolism Rates in a Validation Group of Patients Using the Wells Score Model and D-dimer
Pulmonary Embolism Rate (%)
Wells ScoreNormal D-dimer
(95% CI)Elevated D-dimer
(95% CI)Overall
(95% CI)
<2 2.7 (0.3–9) 0 (0–13.2) 2 (0.2–7.1)2–6 2.9 (0.4–10) 37.3 (25–50.9) 18.8 (12.4–26.6)>6 20 (5.1–71.6) 60 (32.3–83.7) 50 (27.2–72.8)
CI = confidence intervalAdapted with permission from Wells PS, Anderson DR, Rodger M, et al: Derivation of a simple clinical model to categorize patients probabilityof pulmonary embolism: Increasing the model’s utility with the SimpliRED D-dimer. J Thromb Haemost 2000;83(3):416-420.
Table 1
Wells Score for PredictingPulmonary Embolisma
Variable
No. ofPoints
Assigned
Clinical signs and symp-toms of DVT (ie, mini-mum leg swelling, painon palpation of deepveins)
3
An alternative diagnosisis less likely than PE
3
Heart rate >100 BPM 1.5Immobilization or surgery
in previous 4 weeks1.5
Previous DVT/PE 1.5Hemoptysis 1Malignancy (on treat-
ment, treated in last 6months, or palliative)
1
DVT = deep vein thrombosis,PE = pulmonary embolisma The number of points is added. Thehigher the score, the greater the likelihoodof clinical probability. (See Table 2 for per-centages.) >6 = high, 2 to 6 = moderate,<2 = low probabilityAdapted with permission from Wells PS,Anderson DR, Rodger M, et al: Derivationof a simple clinical model to categorizepatients probability of pulmonary embo-lism: Increasing the model’s utility with theSimpliRED D-dimer. J Thromb Haemost2000;83(3):416-420.
Paul Tornetta, MD, and Yelena Bogdan, MD
September 2012, Vol 20, No 9 587

came more effective over time; how-ever, better treatment modalities can-not also explain the increased PEincidence. The other explanation isthat our PE tests are overly sensitive.This would result in increased diag-nosis of small emboli, which mayhave fewer clinical sequelae. In otherwords, the diagnosis exists but maynot be clinically significant. Thistrend has been termed overdiagnosisby Wiener et al.10
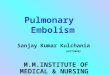
Several studies have focused onoverdiagnosis of PE. An analysis of27 million patients over a 10-yearperiod (1994 to 2004) showed adoubling of PE diagnoses without achange in mortality rate,11 whichsuggested a strong association of theincreased use of CT to explain thesechanges (Figure 1). This trend leadsto the issue of appropriate selectionof patients for these imaging studies,which are not without adverse effects(eg, radiation exposure equivalent of
100 to 400 chest radiographs). Wie-ner et al10 looked at trends beforeand after the advent of CTPA and re-ported an 81% increased incidenceof PE after CTPA with little changein mortality, as well as a 71% in-crease in complications from antico-agulation. This suggests that over-diagnosis occurs and is prevalent; inaddition, the lack of change in mor-tality implies that previously missedsmall emboli picked up by CTPAmay not be clinically important. Fur-thermore, overdiagnosis is poten-tially harmful to patients when theyare anticoagulated for clinically in-significant emboli. In one study, acomparison of clinical indicators ofPE compared with results of CTPAshowed that 25% of positive CTPAfindings were not associated withhigh clinical probability of PE;awareness of this fact could assist inpatients’ not receiving unnecessaryanticoagulation.12
Clinically RelevantPulmonary Embolism
Symptomatic PE can present in dif-ferent ways. One study describes PEaccording to three syndromes thatincrease in severity, from pulmonaryinfarction syndrome (least severe) toisolated dyspnea to circulatory col-lapse (most severe). Patients with lesssevere syndromes are more likely tohave a normal electrocardiogramand PaO2 >80 mm Hg but are lesslikely to have tachypnea, dyspnea, ora high-probability VQ scan.13 Thissuggests that PE can be stratified interms of clinical severity. It followsthat some PEs are completely asymp-tomatic and found incidentally. Theprevalence of incidental PE is ap-proximately 2.6% according to onemeta-analysis of patients undergoingCT for reasons other than PE diag-nosis (eg, evaluation of metastaticdisease).14 Incidental PE also is morecommon in hospitalized patients andthose with cancer. Incidental PE ismore likely to occur in lobar andsegmental arteries. The clinical his-tory of asymptomatic PE has beenevaluated by several studies; how-ever, the studies had small patientsample sizes, limited clinical historyof the patient populations, or limitedfollow-up time. It is clear that moreevidence is needed to assess the po-tential clinical relevance of asymp-tomatic PE.
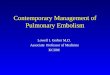
Several studies have investigatedthe size and location of the embolism(central versus segmental or subseg-mental) (Figure 2) in relation to clini-cal significance. Although some au-thors have found no correlationbetween signs and symptoms andclot size or location,15 others agreethat clot characteristics make a dif-ference. In a 5-year study of postop-erative cancer patients, Auer et al16
found a 7.8% average annual in-creased incidence in segmental and
Line graph illustrating deaths from pulmonary embolism (PE), 1992 to 2006.PEDeaths = number of deaths resulting from PE, TotPE = total number ofcases of PE. (Reproduced with permission from Burge AJ, Freeman KD,Klapper PJ, Haramati LB: Increased diagnosis of pulmonary embolismwithout a corresponding decline in mortality during the CT era. Clin Radiol2008;63[4]:381-386.)
Figure 1
Pulmonary Embolism in Orthopaedic Patients: Diagnosis and Management
588 Journal of the American Academy of Orthopaedic Surgeons

subsegmental PE, no change in over-all incidence of central PE, and nochange in overall incidence of fatalPE. Central PE was more severe thanperipheral and was associated withhypoxia, tachycardia, a higher Wellsscore, a greater number of symp-toms, higher 30-day mortality(33.3%, central PE, versus 5%, pe-
ripheral PE), and a higher rate of ad-mission to the intensive care unit. LeGal et al17 also reported that subseg-mental PE presented with less dysp-nea and less chance of being charac-terized as having a high clinicalprobability of PE.
Small emboli are being detectedwith increased frequency, but this
does not appear to influence PEoutcome. Carrier et al18 found anincreased detection rate of sub-segmental PE in multidetectorCTPA compared with single-detectorCTPA. However, the 3-month risk ofvenous thromboembolism (VTE) inuntreated patients with suspected PEand negative CTPA was similar be-
Axial CT pulmonary angiograms of the thorax demonstrating types of pulmonary embolism (PE). A, Right main centralPE (arrow). B, Segmental PE in right lower lobe (arrow). C, Subsegmental PE (arrow). D, Very small “dot” PE (arrow).Note the progressive decrease in size from main to subsegmental and dot PEs, which may not be clinically relevant.(Images courtesy of Akira Murakami, MD, Boston University Medical Center Radiology Department, Boston, MA.)
Figure 2
Paul Tornetta, MD, and Yelena Bogdan, MD
September 2012, Vol 20, No 9 589

tween single and multidetectorCTPA. Thus, the authors suggestedthat subsegmental emboli, even un-treated, may not be clinically signifi-cant. In addition, subsegmental em-boli tend to be less associated withDVT,17,19,20 which suggests a differ-ence from the more dangerous em-bolic events. Subsegmental embolialso have a rounded dot-like appear-ance, suggesting that they are part ofa normal physiologic process bywhich lung fibrinolytic activity dis-solves emboli to protect the greatersystemic circulation.19 Further, un-treated subsegmental emboli havegood outcomes with respect to recur-rent VTE and cardiopulmonary com-plications. According to the Prospec-tive Investigation of PulmonaryEmbolism Diagnosis, subsegmentalemboli are more likely to be classi-fied as low probability on a VQscan.21 Perrier et al22 showed that alow-probability VQ scan combinedwith low clinical probability resultsin only a 1% to 2% risk of subse-quent thromboembolic events (DVTor PE) for up to 6 months; in addi-tion, not instituting anticoagulationappears to be safe for a low-probability scan. In a study of 334patients (median follow-up, 8months), subsegmental emboli
showed no hemodynamic instabilityon echocardiogram, and there wasno PE recurrence or PE-related deathdespite 30% of patients not receivinganticoagulation therapy.20 Patientswith segmental emboli also had noPE recurrence, although 80% wereanticoagulated; however, they didhave a 4.5% rate of PE-relateddeaths. Thus, subsegmental emboliseem to have a better prognosis thando the larger segmental emboli (Ta-ble 3).
Currently, the American College ofChest Physicians guidelines do notmention clot size as a variable. Physi-cians often do not take size or loca-tion of the clot into account beforeinstituting anticoagulant therapy,and radiologists frequently do notdiscuss their findings with treatingphysicians. As one author notes, “Itis not always clear whether small PE,in the absence of demonstrable DVT,justify the expense, mortality, and se-rious morbidity associated with anti-coagulation.”23 He suggests thatgroups of people exist in which risksof anticoagulation for PE may out-weigh the benefits and that there are,as well, certain scenarios in whichsmall emboli should be treated (Ta-ble 4). These studies suggest thatsuch patient stratification may be
necessary, that not all emboli areequal, and that management strate-gies should be altered, particularly insurgical patients.
Anticoagulation forPulmonary Embolism
It is clear that anticoagulation is ofparamount importance in treatingclinically relevant PE to preventdeath. In a landmark study, Barrittand Jordan24 conducted a random-ized controlled trial of patients withPE. The group that received unfrac-tionated heparin with vitamin K an-tagonist (n = 16) experienced no PErecurrences or fatalities, whereas thecontrol group (n = 19) had 10 recur-rences and 5 fatalities. Since then,multiple studies have shown benefitsfor anticoagulation and, based ontheir results, societies have releasedguidelines for anticoagulation ther-apy for PE.25,26 The American Col-lege of Chest Physicians provides thefollowing grade 1 (strong) recom-mendations: a confirmed PE istreated with low-molecular-weightheparin (LMWH), monitored intra-venous or subcutaneous unfraction-ated heparin, weight-based subcuta-neous unfractionated heparin, or
Table 3
Characteristics of Patients With Pulmonary Embolus of Different Sizesa
Factor Subsegmental (n = 22) Segmental (n = 67) Central (n = 245)
Incidentally found 14 (63.6%)b 36 (53.7%) 45 (18.4%)Dyspnea 4 (18.2%) 16 (23.9%) 117 (47.8%)Surgery or trauma 14 (63.6%) 28 (41.8%) 44 (18.0%)Coexisting DVT 9 (40.9%) 41 (61.2%) 177 (72.2%)Received anticoagulation 15 (68.2%) 54 (80.6%) 229 (93.5%)PE recurrence None None 6 (2.4%)PE-related death None 3 (4.5%) 7 (2.9%)
DVT = deep vein thrombosis, PE = pulmonary embolisma Note the higher incidence of recurrence and death in larger clot sizes, despite receiving anticoagulation at a higher rate than that of thesmaller clots. (Where applicable, all P values are <0.05.)b Parentheses denote percentages of total patients in group.Adapted with permission from Cha SI, Shin KM, Lee JW, et al: Clinical characteristics of patients with peripheral pulmonary embolism. Respi-ration 2010;80(6):500-508.
Pulmonary Embolism in Orthopaedic Patients: Diagnosis and Management
590 Journal of the American Academy of Orthopaedic Surgeons

subcutaneous fondaparinux for 5days, with concurrent initiation ofvitamin K antagonists (eg, warfarin)until the international normalized ra-tio is ≥2. For PE in a patient withtransient risk factors, 3 months oftreatment is recommended; for PE ina patient without risk factors, 3months plus evaluation for lifetimeanticoagulation is recommended,
with a target international normal-ized ratio of 2.525 (Table 5). The Brit-ish Thoracic Society has similarguidelines, adding that thrombolytictherapy should be used only in mas-sive PE and that oral anticoagulationshould not be started unless PE isconfirmed with imaging. Theseguidelines emphasize the risk of anti-coagulation in certain patient sub-
groups, such as pregnant patientsand those with cancer, but postoper-ative patients are not mentioned.26
At least one response to the currentanticoagulation guidelines questionswhether they are appropriate for or-thopaedic patients.31 Each of thesemedications has drawbacks. Warfa-rin requires close monitoring and isnot predictable in its pharmacokinet-
Table 4
Suggestions for Anticoagulation Therapy for Small Pulmonary Emboli23
Cardiopulmonary Reserve Coexisting DVT Other Factor(s) Anticoagulate
Adequate No Symptomatic NoAdequate No Asymptomatic/Incidental finding NoAdequate No Anticoagulation contraindicated NoAdequate Yes — YesAdequate — Recurrent PE YesInadequate — — Yes
DVT = deep vein thrombosis, PE = pulmonary embolism
Table 5
American College of Chest Physicians Recommendations for Treatment of Pulmonary Embolism25
Type ofPulmonaryEmbolism Management
Goals of Management/Rationale
Grade ofRecommendationa
Acute LMWH, UFH, or fondaparinux × 5 d LMWH: prevent formation of newthrombi27
UFH better for increased bleedingrisk because rapidly reversed28
1C
Initiation of VKA on day 1, discontinu-ation of heparin with INR ≥2 × 24 h
Prevent extension of thrombus anddisease recurrence28
Depends on clotting factors IIand X depletion27
1A
With transient risk factors VKA × 3 mo — 1AUnprovoked/No risk fac-
torsVKA × 3 mo — 1A
Evaluation for lifetime VKA Incidence of recurrence higher at 2 yrthan provoked PE29
1C
First unprovoked PE, nobleeding risk, patientpreference
Lifetime VKA, target INR = 2.5 — 1A
PE in patients with can-cer
LMWH × 3 mo LMWH more effective in preventingrecurrence than VKA30
1A
LMWH or VKA as long as cancer re-mains active
LMWH more effective in preventingrecurrence than VKA30
1C
INR = international normalized ratio, LMWH = low-molecular-weight heparin, PE = pulmonary embolism, UFH = unfractionated heparin,VKA = vitamin K antagonista A = high-quality evidence, C = low-quality evidence
Paul Tornetta, MD, and Yelena Bogdan, MD
September 2012, Vol 20, No 9 591

ics. LMWH and fondaparinux re-quire nonoral administration. Thenewly introduced direct thrombin in-hibitor ximelagatran is an oral agentand requires no monitoring; how-ever, it causes elevation of transami-nase levels and an increased rate ofcoronary events of unclear signifi-cance.32
The timing of therapeutic anticoag-ulation for PE in postsurgical pa-tients has not been thoroughly re-searched. In a study of spine surgerypatients with PE, three patients weretreated with inferior vena cava (IVC)filters because the PE presentedwithin the first week of surgery, andthree were treated with anticoagula-tion because the PE presented 1 weekafter surgery. Neither group of pa-tients had severe complications fromthe treatment.33 The authors recom-mended a waiting period of at least 8postoperative days before institutinga full dose of anticoagulation. An-other study of neurosurgical patientscited a high mortality rate (15%) as-sociated with anticoagulation thera-py; the authors could not commenton safe timing.34
Several studies focus on the out-comes of anticoagulation therapy forPE (Table 6). In a study of 673 pa-tients with PE (of whom only 10were surgical) who were treated withanticoagulants for 3 months withcomplete follow-up, Nijkeuter et al35
found a 3% recurrence rate ofthromboembolic events (20 patients)
and a 2% recurrence rate of PE (14patients), of which 79% were fatal,mostly in the first week. Immobiliza-tion for >3 days posed significantrisk for both recurrent VTE and fatalrecurrent PE (odds ratio, 2.79). Theoverall 3-month mortality risk fac-tors in the entire PE cohort were age,immobilization, cancer, and inpatientstatus. Douketis et al36 researched alonger treatment period; in 2,052 pa-tients (310 with PE, 292 with bothDVT and PE) who were anticoagu-lated for 6 months, with an average54-month follow-up, the risk of fatalPE after stopping therapy was 0.2 to0.5 events per 100 person-years (casefatality rate, 4% to 9%). For an evenlonger treatment period, Palla et al37
looked at 497 patients with PE (33%surgical) anticoagulated for 1 year.Forty-eight patients (9.6%) had re-current PE, which was fatal in 36 of48 cases. Thirty-nine of 48 recur-rences (81.2%) occurred within 10days of diagnosis, and 2 patients hadrecurrent nonfatal PE between 6 and12 months. Finally, Stein et al27 re-viewed several studies of timing ofheparin versus vitamin K antagonistin DVT patients. Most VTE (DVT orPE) recurrences took place after 5days, even in those who were nottreated with heparin; a therapeuticlevel of heparin in 24 hours resultedin fewer recurrent events. Thesestudies suggest that the greatest riskof PE arises within the first 2 weeksand that these early recurrences have
a high fatality rate. It follows thatanticoagulation therapy is most im-portant in the first days of diagnosis,precisely when it is most dangerousto a surgical patient. However, thesestudies did not delineate the natureof the embolus, such as size and lo-cation; this must be taken into ac-count, given the earlier stated re-search on the effect of embolus size.It is also important to remember thatthe studies mentioned above focusmostly on medical rather than surgi-cal or orthopaedic patients, and sotheir results may not be applicable.In particular, the risks of anticoagu-lation on postoperative surgical sitebleeding are not addressed.
Other studies focus on the mortal-ity of untreated PE, although thereare, to our knowledge, no random-ized controlled trials of treated ver-sus untreated PE. One study re-viewed data from the ProspectiveInvestigation of Pulmonary Embo-lism Diagnosis of 20 patients whohad PE but had not received antico-agulation therapy. These patientswere more likely to have segmentalperfusion defects than were thetreated patients. One patient died,and one had recurrent PE. The au-thors concluded that “mild” PE hasa low mortality risk.38 Nielsen et al39
presented a trial of 87 patients withDVT, 43 of whom had a silent,asymptomatic PE on lung scan. All87 patients were randomized to re-ceive or not receive anticoagulation.
Table 6
Summary of Outcomes of Anticoagulation Therapy for Pulmonary Embolism
Study PatientsTreatment Duration
(mo) Follow-up (mo) Recurrence Rate
Nijkeuter et al35 673 (PE) 3 3 2%Douketis et al36 2,052 (310 PE,
292 DVT + PE)6 54 0.2–0.5/100 person-yearsa
Palla et al37 497 (PE) 12 ≥12 9.6%
DVT = deep vein thrombosis, PE = pulmonary embolisma Risk of fatal pulmonary embolism
Pulmonary Embolism in Orthopaedic Patients: Diagnosis and Management
592 Journal of the American Academy of Orthopaedic Surgeons

Anticoagulation therapy did not in-fluence PE resolution on lung scan at3-month follow-up.
The type of anticoagulation mayhave an effect on outcomes, as well.In a randomized trial, Hull et al40
looked at patients with both DVTand nonmassive PE who received ei-ther LMWH (97 patients) or unfrac-tionated heparin (103 patients).Rates of recurrent VTE events werezero versus 7%, respectively, suggest-ing that LMWH is at least as good atherapy, if not better, than standardintravenous heparin.
Therapeutic anticoagulation in-volves several risks: bleeding, throm-bocytopenia, and osteoporosis, aswell as skin necrosis and, in the caseof warfarin, teratogenicity. Of these,bleeding is most important and rele-vant for orthopaedic patients. Bleed-ing can lead to pain, prolonged reha-bilitation, compartment syndrome,return to the operating room, anemiaand transfusion, and wound infec-tion. Bleeding is a strong predictor ofmortality in hospitalized patients.41
Even prophylactic anticoagulationcarries a bleeding risk at the surgicalsite: a 6.38 relative risk for LMWHcompared with aspirin and a 4.88relative risk for warfarin comparedwith aspirin in one study.42
Much of the data on bleeding com-plications come from total joint liter-ature. The rates quoted for bleedingrange from minimal to as high as50%.43-46 None of these studies israndomized; however, they provideuseful data on risk. In a review of112 arthroplasty patients who weretreated for DVT or PE with intrave-nous heparin, Patterson et al43 foundan overall bleeding rate of 30%,with decreasing risk over time (50%if anticoagulated within 5 days ofsurgery, 40% if within 7 days, and15% if >1 week). In 41 patients(35%), heparin was discontinued be-cause of complications; 38 of thosepatients received warfarin instead
and did well. Twenty-three patientstreated for mild PE with warfarinalone had no bleeding or PE-relatedcomplications. The authors reachedseveral important conclusions: that abolus heparin dose may be too ag-gressive; that a PE should be con-firmed before instituting treatment;and, most importantly, that antico-agulation in the first postoperativeweek carries a very high risk andshould be avoided. These findingsare echoed in other studies, whichshow an increased bleeding rate inthe first month of anticoagulation.44
Supratherapeutic levels of interna-tional normalized ratio or partialthromboplastin time are also associ-ated with bleeding complications, aswell as higher transfusion require-ments and longer hospitaliza-tions.44,45
Anticoagulation therapy for evensmall pulmonary emboli carriesrisks. In one study of 43 false-negative CT scans that eventuallywere read as positive for PE, 21 pa-tients did not receive therapeutic an-ticoagulation. Patients who receivedno anticoagulation had a signifi-cantly lower rate of hemorrhage, re-nal failure, and early death than didthose who received anticoagulationtherapy.47 Another study of 71 pa-tients who received anticoagulationfor subsegmental PE and 22 who didnot showed 8 instances of hemor-rhage, including 5 major events, allin the anticoagulated patients. Inter-estingly, no patient in either groupdied of PE, and there was one PE re-currence in the anticoagulatedgroup.48 These findings emphasizethe potential harm of anticoagulanttherapy and warn against a “one sizefits all” approach to PE treatment.
IVC filters are an alternative forpatients with PE who have a highrisk of bleeding (ie, recent surgery)or who cannot tolerate anticoagu-lants. They are also indicated for pa-tients who experience a recurrent PE
despite therapeutic anticoagulation.When placed, these filters block thepassage of emboli from the lower ex-tremities to the pulmonary circula-tion. They can be permanent or re-trievable (for up to 1 year); removalcarries a risk of iatrogenic IVC in-jury, which increases with the timesince filter placement. Anticoagula-tion therapy is begun, either concur-rently with the filter or just beforeremoval, when the patient’s bleedingrisk is acceptable. Additionally, inmultiple-trauma patients, particu-larly those with long bone injury,spinal cord injury, or pelvic frac-tures, IVC filters are often placed inan attempt to prevent massive PE.One review of 9,348 orthopaedic pa-tients found a 1% total rate of filterplacement (90 patients), with 61%of 90 filters placed prophylactically.49
The ratio of prophylactic-based totreatment-based filters was 3.25 infractures and 2.1 in joint arthroplas-ties. In that study, 10% of the re-trievable filters were not able to beremoved, and a further 11% hadcomplications during removal. De-spite these risks, filters are com-monly used in orthopaedics and pro-vide another weapon in the arsenalof PE prevention and treatment.
Summary
Orthopaedic patients present a di-lemma for treating clinicians: theyare at high risk for both PE andbleeding events. The orthopaediccommunity has extensively debatedanticoagulation therapy for prophy-laxis of PE, and the American Acad-emy of Orthopaedic Surgeons haspresented clinical practice guidelinesto help guide care. However, datasuggest that we may be overdiagnos-ing PE, that not all pulmonary em-boli are the same, that small emboliare of questionable clinical rele-vance, and that the risks of anticoag-
Paul Tornetta, MD, and Yelena Bogdan, MD
September 2012, Vol 20, No 9 593

ulation therapy are not minor.
We believe that the risks and bene-fits of mangement of the diagnosis ofPE should be reviewed with the pa-tient and that a spectrum of treat-ment should be based on the size andclinical presentation of the PE, asshould the magnitude and timing ofany orthopaedic surgical procedures.At this juncture, we are unable tomake recommendations for treat-ment of small emboli. We feel thatthe subject merits additional clinicalstudy and call for development ofguidelines for anticoagulation in or-thopaedic patients with PE, specifi-cally including the size and locationof the embolus and the potential riskof bleeding.
References
Evidence-based Medicine: Levels ofevidence are described in the table ofcontents. In this article, references 6,21, 24, 36, 37, and 39 are level Istudies. References 3, 7, 12, 14, 17-20, 22, 27, 32, 33, 35, 44, 45, and47-49 are level II studies. References4, 15, 16, and 34 are level III studies.Reference 13 is a level IV study.
References printed in bold type indi-cate those published within the past5 years.
1. American Academy of OrthopaedicSurgeons: Preventing VenousThromboembolic Disease in PatientsUndergoing Elective Hip and KneeArthroplasty: Evidence-Based Guidelineand Evidence Report. Available at:http://www.aaos.org/Research/guidelines/VTE/VTE_full_guideline.pdf. AccessedJuly 26, 2012.
2. Montgomery KD, Geerts WH, PotterHG, Helfet DL: Thromboemboliccomplications in patients with pelvictrauma. Clin Orthop Relat Res 1996;329:68-87.
3. Abelseth G, Buckley RE, Pineo GE, HullR, Rose MS: Incidence of deep-veinthrombosis in patients with fractures ofthe lower extremity distal to the hip.J Orthop Trauma 1996;10(4):230-235.
4. Kim HJ, Walcott-Sapp S, Leggett K, et al:Detection of pulmonary embolism in the
postoperative orthopedic patient usingspiral CT scans. HSS J 2010;6(1):95-98.
5. Wells PS, Anderson DR, Rodger M, et al:Derivation of a simple clinical model tocategorize patients probability ofpulmonary embolism: Increasing themodel’s utility with the SimpliREDD-dimer. Thromb Haemost 2000;83(3):416-420.
6. Anderson DR, Kahn SR, Rodger MA,et al: Computed tomographic pulmonaryangiography vs ventilation-perfusionlung scanning in patients with suspectedpulmonary embolism: A randomizedcontrolled trial. JAMA 2007;298(23):2743-2753.
7. Moores LK, Jackson WL Jr, Shorr AF,Jackson JL: Meta-analysis: Outcomes inpatients with suspected pulmonaryembolism managed with computedtomographic pulmonary angiography.Ann Intern Med 2004;141(11):866-874.
8. Subramaniam RM, Blair D, Gilbert K,Coltman G, Sleigh J, Karalus N:Withholding anticoagulation after anegative computed tomographypulmonary angiogram as a stand-aloneimaging investigation: A prospectivemanagement study. Intern Med J 2007;37(9):624-630.
9. Park B, Messina L, Dargon P, Huang W,Ciocca R, Anderson FA: Recent trends inclinical outcomes and resourceutilization for pulmonary embolism inthe United States: Findings from thenationwide inpatient sample. Chest2009;136(4):983-990.
10. Wiener RS, Schwartz LM, Woloshin S:Time trends in pulmonary embolism inthe United States: Evidence ofoverdiagnosis. Arch Intern Med 2011;171(9):831-837.
11. Burge AJ, Freeman KD, Klapper PJ,Haramati LB: Increased diagnosis ofpulmonary embolism without acorresponding decline in mortalityduring the CT era. Clin Radiol 2008;63(4):381-386.
12. Ranji SR, Shojania KG, Trowbridge RL,Auerbach AD: Impact of reliance on CTpulmonary angiography on diagnosis ofpulmonary embolism: A Bayesiananalysis. J Hosp Med 2006;1(2):81-87.
13. Stein PD, Henry JW: Clinicalcharacteristics of patients with acutepulmonary embolism stratified accordingto their presenting syndromes. Chest1997;112(4):974-979.
14. Dentali F, Ageno W, Becattini C, et al:Prevalence and clinical history ofincidental, asymptomatic pulmonaryembolism: A meta-analysis. Thromb Res2010;125(6):518-522.
15. Pulido L, Grossman S, Smith EB, et al:Clinical presentation of pulmonary
embolus after total joint arthroplasty:Do size and location of embolus matter?Am J Orthop (Belle Mead NJ) 2010;39(4):185-189.
16. Auer RC, Schulman AR, Tuorto S, et al:Use of helical CT is associated with anincreased incidence of postoperativepulmonary emboli in cancer patientswith no change in the number of fatalpulmonary emboli. J Am Coll Surg 2009;208(5):871-880.
17. Le Gal G, Righini M, Parent F, vanStrijen M, Couturaud F: Diagnosis andmanagement of subsegmental pulmonaryembolism. J Thromb Haemost 2006;4(4):724-731.
18. Carrier M, Righini M, Wells PS, et al:Subsegmental pulmonary embolismdiagnosed by computed tomography:Incidence and clinical implications. Asystematic review and meta-analysis ofthe management outcome studies.J Thromb Haemost 2010;8(8):1716-1722.
19. Suh JM, Cronan JJ, Healey TT: Dots arenot clots: The over-diagnosis and over-treatment of PE. Emerg Radiol 2010;17(5):347-352.
20. Cha SI, Shin KM, Lee JW, et al: Clinicalcharacteristics of patients with peripheralpulmonary embolism. Respiration 2010;80(6):500-508.
21. The PIOPED Investigators: Value of theventilation/perfusion scan in acutepulmonary embolism: Results of theprospective investigation of pulmonaryembolism diagnosis (PIOPED).JAMA 1990;263(20):2753-2759.
22. Perrier A, Miron MJ, Desmarais S, et al:Using clinical evaluation and lung scanto rule out suspected pulmonaryembolism: Is it a valid option in patientswith normal results of lower-limb venouscompression ultrasonography? ArchIntern Med 2000;160(4):512-516.
23. Goodman LR: Editorial: Smallpulmonary emboli: What do we know?Radiology 2005;234(3):654-658.
24. Barritt DW, Jordan SC: Anticoagulantdrugs in the treatment of pulmonaryembolism: A controlled trial. Lancet1960;1(7138):1309-1312.
25. Kearon C, Kahn SR, Agnelli G, et al:Antithrombotic therapy for venousthromboembolic disease: AmericanCollege of Chest Physicians Evidence-Based Clinical Practice Guidelines (8thEdition). Chest 2008;133(6 suppl):454S-545S.
26. British Thoracic Society Standards ofCare Committee Pulmonary EmbolismGuideline Development Group: BritishThoracic Society guidelines for themanagement of suspected acutepulmonary embolism. Thorax 2003;
Pulmonary Embolism in Orthopaedic Patients: Diagnosis and Management
594 Journal of the American Academy of Orthopaedic Surgeons

58(6):470-483.
27. Stein PD, Hull RD, Matta F, YaekoubAY: Anticoagulant therapy for acutevenous thromboembolism: What wethink we know and what the data showfor the timing of recurrent events. ClinAppl Thromb Hemost 2009;15(6):609-612.
28. van Es J, Douma RA, Gerdes VE,Kamphuisen PW, Büller HR: Acutepulmonary embolism: Part 2. Treatment.Nat Rev Cardiol 2010;7(11):613-622.
29. Baglin T, Luddington R, Brown K,Baglin C: Incidence of recurrent venousthromboembolism in relation to clinicaland thrombophilic risk factors:Prospective cohort study. Lancet 2003;362(9383):523-526.
30. Lee AY, Levine MN, Baker RI, et al:Low-molecular-weight heparin versus acoumarin for the prevention of recurrentvenous thromboembolism in patientswith cancer. N Engl J Med 2003;349(2):146-153.
31. Callaghan JJ, Dorr LD, Engh GA, et al:Prophylaxis for thromboembolic disease:Recommendations from the AmericanCollege of Chest Physicians. Are theyappropriate for orthopaedic surgery?J Arthroplasty 2005;20(3):273-274.
32. Huisman MV, Bounameaux H: Treatingpatients with venous thromboembolism:Initial strategies and long-term secondaryprevention. Semin Vasc Med 2005;5(3):276-284.
33. Schizas C, Neumayer F, Kosmopoulos V:Incidence and management ofpulmonary embolism following spinalsurgery occurring while under chemicalthromboprophylaxis. Eur Spine J 2008;17(7):970-974.
34. Swann KW, Black PM, Baker MF:Management of symptomatic deep
venous thrombosis and pulmonaryembolism on a neurosurgical service.J Neurosurg 1986;64(4):563-567.
35. Nijkeuter M, Söhne M, Tick LW, et al:The natural course of hemodynamicallystable pulmonary embolism: Clinicaloutcome and risk factors in a largeprospective cohort study. Chest 2007;131(2):517-523.
36. Douketis JD, Gu CS, Schulman S,Ghirarduzzi A, Pengo V, Prandoni P:The risk for fatal pulmonary embolismafter discontinuing anticoagulant therapyfor venous thromboembolism. AnnIntern Med 2007;147(11):766-774.
37. Palla A, Ribas C, Rossi G, Pepe P,Marconi L, Prandoni P: The clinicalcourse of pulmonary embolism patientsanticoagulated for 1 year: Results of aprospective, observational, cohort study.J Thromb Haemost 2010;8(1):68-74.
38. Stein PD, Henry JW, Relyea B: Untreatedpatients with pulmonary embolism:Outcome, clinical, and laboratoryassessment. Chest 1995;107(4):931-935.
39. Nielsen HK, Husted SE, Krusell LR,Fasting H, Charles P, Hansen HH: Silentpulmonary embolism in patients withdeep venous thrombosis: Incidence andfate in a randomized, controlled trial ofanticoagulation versus no anticoagula-tion. J Intern Med 1994;235(5):457-461.
40. Hull RD, Raskob GE, Brant RF, et al:Low-molecular-weight heparin vsheparin in the treatment of patients withpulmonary embolism. Arch Intern Med2000;160(2):229-236.
41. Eikelboom JW, Quinlan DJ, O’DonnellM: Major bleeding, mortality, andefficacy of fondaparinux in venousthromboembolism prevention trials.Circulation 2009;120(20):2006-2011.
42. Brown GA: Venous thromboembolism
prophylaxis after major orthopaedicsurgery: A pooled analysis ofrandomized controlled trials.J Arthroplasty 2009;24(6 suppl):77-83.
43. Patterson BM, Marchand R, Ranawat C:Complications of heparin therapy aftertotal joint arthroplasty. J Bone Joint SurgAm 1989;71(8):1130-1134.
44. Zidane M, Schram MT, Planken EW,et al: Frequency of major hemorrhage inpatients treated with unfractionatedintravenous heparin for deep venousthrombosis or pulmonary embolism: Astudy in routine clinical practice. ArchIntern Med 2000;160(15):2369-2373.
45. Neviaser AS, Chang C, Lyman S, DellaValle AG, Haas SB: High incidence ofcomplications from enoxaparintreatment after arthroplasty. ClinOrthop Relat Res 2010;468(1):115-119.
46. Spencer FA, Emery C, Joffe SW, et al:Incidence rates, clinical profile, andoutcomes of patients with venousthromboembolism: The Worcester VTEstudy. J Thromb Thrombolysis 2009;28(4):401-409.
47. Engelke C, Rummeny EJ, Marten K:Pulmonary embolism at multi-detectorrow CT of chest: One-year survival oftreated and untreated patients.Radiology 2006;239(2):563-575.
48. Donato AA, Khoche S, Santora J,Wagner B: Clinical outcomes in patientswith isolated subsegmental pulmonaryemboli diagnosed by multidetector CTpulmonary angiography. Thromb Res2010;126(4):e266-e270.
49. Bass AR, Mattern CJ, Voos JE, PetersonMG, Trost DW: Inferior vena cava filterplacement in orthopedic surgery. Am JOrthop (Belle Mead NJ) 2010;39(9):435-439.
Paul Tornetta, MD, and Yelena Bogdan, MD
September 2012, Vol 20, No 9 595