Embed Size (px)
Citation preview

Information technologyin health care
C H A P T E R 7


nformation technology (IT) has the potential to improve the
quality, safety, and efficiency of health care. Diffusion of IT in
health care is generally low (varying, however, with the appli-
cation and setting) but surveys indicate that providers plan to
increase their investments. Drivers of investment in IT include the
promise of quality and efficiency gains. Barriers include the cost and
complexity of IT implementation, which often necessitates significant
work process and cultural changes. Certain characteristics of the health
care market—including payment policies that reward volume rather than quality, and a fragmented delivery sys-
tem—can also pose barriers to IT adoption. Given IT’s potential, both the private and public sectors have engaged
in numerous efforts to promote its use within and across health care settings. Additional steps could include
financial incentives (e.g., payment policy or loans) and expanded efforts to standardize records formats, nomen-
clature, and communication protocols to enhance interoperability. However, any policy to stimulate further
investment must be carefully considered because of the possibility of unintended consequences.
7In this chapter
• What is health informationtechnology?
• Quality and healthinformation technology
• Current status of healthinformation technology
• Efforts to encourage fasterdiffusion
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 157
C H A P T E R
IInformation technology in health care

158 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
By providing new ways for providers and their patients toreadily access and use health information, informationtechnology (IT) has the potential to improve the quality,safety, and efficiency of health care. However, relativelyfew health care providers have fully adopted IT. Lowdiffusion is due partly to the complexity of IT investment,which goes beyond acquiring technology to changingwork processes and cultures, and ensuring that physicians,nurses, and other staff use it. In addition, certain aspects ofthe market—such as payment policies that reward volumerather than quality and the fragmentation of caredelivery—do not promote IT investment, and may hinderit. Because of its potential, policymakers need to betterunderstand how information technology is diffusing acrossproviders, whether action to spur further adoption isneeded, and if so, what steps might be taken. Any policyto stimulate further investment must be carefullyconsidered because of possible unintendedconsequences—such as implementation failures due toorganizations’ inability to make the necessary culturalchanges. This chapter is a first step in increasing ourunderstanding of the current state of IT in the health careindustry. The Commission will continue to work on thisissue.
Despite considerable attention to the topic, much remainsunknown about the role of IT in the health care setting.What types of IT are being used? What is the link betweenuse of IT and quality improvements? How muchinvestment have hospitals and physicians already made ininformation technology, and in what kinds? What factorsdrive IT investments (e.g., financial returns, qualityimprovement goals, other factors)? What factors hinder ITinvestments and implementation (e.g., work flow changes,lack of compatibility with other IT, costs)? What currentsteps are being taken by public and private entities toencourage further diffusion of IT? What additional actionsmight make sense?
Delivering quality health care requires providers andpatients to integrate complex information from manydifferent sources. Thus, increasing the ability ofphysicians, nurses, clinical technicians, and others toreadily access and use the right information about theirpatients should improve care. The ability for patients toobtain information to better manage their condition and tocommunicate with the health system could also improvethe efficiency and quality of care. This potential toimprove care makes broader diffusion of IT desirable.
However, further research is needed to better understandwhat types of IT applications are most useful forimproving care in different settings and whatcircumstances are necessary to ensure successfulimplementation. Current studies show that sometechnologies lead to better care. However, the evidencebase is narrow, coming primarily from select institutionsthat developed their own systems, and may not representthe average facility.
The health care system generally uses less IT than otherindustries, but surveys indicate that providers areincreasing their investments. The extent of IT and thetypes of IT deployed vary by setting and institution. Theprevalence of IT in any setting largely reflects the strengthof the drivers and barriers to investment. For manyorganizations, quality and process improvements areprimary drivers. For others, gains in efficiency motivateinvestment. Yet, the cost and the complexity of ITimplementation, including necessary organizational andworkflow redesign, pose considerable barriers, as doesuncertainty regarding the stability of the IT industry.
The larger health care market poses additional barriers toinvestment in IT. Payment systems that tie reimbursementto the volume of services delivered, for example, maypenalize providers who improve quality in ways that resultin fewer units of service. To the extent that IT investmentslead to reduced volume, many who make the investmentwill not reap all of the benefits. Systems that integrate careacross settings tend to be more advanced users of ITbecause they are able to capture some of these efficiencies.In addition to barriers posed by payment systems, afragmented delivery system leads to redundantinvestments by multiple providers who lose the benefit ofeconomies of scale. Although this aspect of our deliverysystem is a barrier to adoption, widespread use of IT couldhelp providers coordinate care across settings, overcomingsome of the problems of fragmentation.
Both the private and public sectors have engaged innumerous efforts to promote use of IT within health careinstitutions and across care delivery settings. Activitiesinclude developing and promoting industry-widestandards; funding research to investigate the impact of ITon quality; providing incentives that encourage investmentin IT; giving grants to those investing in IT; anddeveloping strategies to improve the flow of informationacross providers. Additional activities to promote diffusion

could include changes to payment policy, institution ofloan or grant funds, and requirements to adopt specifictechnologies.
What is health information technology?
In general, IT allows health care providers to collect, store,retrieve, and transfer information electronically. However,more specific discussion of IT in health care is challengingdue to the lack of precise definitions, the volume ofapplications, and a rapid pace of change in technology.
Similar terms can be used to define different products, andthe exact functions of a system will depend on thespecifics of its implementation in a given setting. Both theterms and the functions also change over time. Forexample, computerized provider order entry (CPOE),which can minimize handwriting or other communicationerrors by having physicians or other providers enter ordersinto a computer system, can apply only to prescriptiondrugs, or may also include additional physician orders,such as x-rays or other images, consultations, andtransfers. For electronic health records (EHRs, also knownas electronic medical records, automated medical records,and computer-based patient records, among other names),multiple definitions exist, depending on the constellationof functions that are included (Brailler and Tarasawa2003).1 They can be used simply as a passive tool to storepatient information or can include multiple decisionsupport functions, such as individualized patient remindersand prescribing alerts.
When purchasing IT, providers must consider multiplefunctions and literally hundreds of applications offered bynumerous vendors. In general, the various IT applicationsfall into three categories:
• administrative and financial systems that facilitatebilling, accounting, and other administrative tasks;
• clinical systems that facilitate or provide input into thecare process; and
• infrastructure that supports both the administrative andclinical applications.
Table 7-1 provides examples of IT applications inhospitals and physicians’ offices; the accompanying textbox (p. 160) provides definitions for various clinicalsystems and other terms used in IT discussions.
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 159
Examples of health informationtechnology for hospitals
and physicians
HospitalsAdministrative Billing
and financial General ledger Cost accounting systemsPatient registrationPersonnel and payrollElectronic materials management
Clinical Computerized provider order entry for drugs, labtests, procedures
Electronic health recordPicture archiving and communication systems for
filmless imagingResults reporting of laboratory and other testsClinical decision support systemsPrescription drug fulfillment, error-alert,
transcriptionsElectronic monitoring of patients in intensive care
unitsInfrastructure Desktop, laptop, cart-based, and tablet computers
Servers and networksWireless networksVoice recognition systems for transcription,
physician orders, and medical recordsBar-coding technology for drugs, medical devices,
and inventory controlInformation security systems
PhysiciansAdministrative Billing
and financial AccountingSchedulingPersonnel and payroll
Clinical Online references (drug compendia and clinical guidelines)
Receiving lab results and other clinical information online
Electronic prescribingComputerized provider order entryClinical decision support systemsElectronic health recordE-mail communication with patients
Infrastructure Desktop and laptop computersHandheld technologyServers and network
Note: Applications listed are examples and not exhaustive.
T A B L E7-1
Type ofinformationtechnology Applications

160 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
Quality and health informationtechnology
One of the primary motivators for adopting many clinicalhealth IT applications is the belief that they improve thequality of patient care. Yet, further research is needed tobetter document and understand the link between IT and
quality, including the types of quality problemsinformation technology can be used to solve andimplementation strategies to ensure that quality objectivesare met.
Quality health care relies on physicians, nurses, patientsand their families, and others having the right informationat the right time and using it to make the right decisions.
What is health information technology?
The following technologies and terms are oftenincluded in discussions of informationtechnology in health care:
• Electronic health record (EHR): EHRs wereoriginally envisioned as an electronic file cabinet forpatient data from various sources (eventuallyintegrating text, voice, images, handwritten notes,etc.). Now they are generally viewed as part of anautomated order-entry and patient-tracking systemproviding real-time access to patient data, as well asa continuous longitudinal record of their care.
• Computerized provider order entry (CPOE):CPOE in its basic form is typically a medicationordering and fulfillment system. More advancedCPOE will also include lab orders, radiology studies,procedures, discharges, transfers, and referrals.
• Clinical decision support system (CDSS): CDSSprovides physicians and nurses with real-timediagnostic and treatment recommendations. Theterm covers a variety of technologies ranging fromsimple alerts and prescription drug interactionwarnings to full clinical pathways and protocols.CDSS may be used as part of CPOE and EHR.
• Picture archiving and communications system(PACS): This technology captures and integratesdiagnostic and radiological images from variousdevices (e.g., x-ray, MRI, computed tomographyscan), stores them, and disseminates them to amedical record, a clinical data repository, or otherpoints of care.
• Bar coding: Bar coding in a health careenvironment is similar to bar-code scanning in otherenvironments: An optical scanner is used toelectronically capture information encoded on aproduct. Initially, it will be used for medication (forexample, matching drugs to patients by using barcodes on both the medications and patients’ armbracelets), but other applications may be pursued,such as medical devices, lab, and radiology.
• Radio frequency identification (RFID): Thistechnology tracks patients throughout the hospital,and links lab and medication tracking through awireless communications system. It is neithermature nor widely available, but may be analternative to bar coding.
• Automated dispensing machines (ADMs): Thistechnology distributes medication doses.
• Electronic materials management (EMM): Healthcare organizations use EMM to track and manageinventory of medical supplies, pharmaceuticals, andother materials. This technology is similar toenterprise resource planning systems used outside ofhealth care.
• Interoperability: This concept refers to electroniccommunication among organizations so that the datain one IT system can be incorporated into another.Discussions of interoperability focus ondevelopment of standards for content andmessaging, among other areas, and development ofadequate security and privacy safeguards. �
Source: Adapted from deliverable submitted to MedPAC by Abt Associates.

Yet the health information needed to make these decisionschanges frequently; the guidelines and clinical evidencecontinually evolve, as does knowledge about the conditionof the patient. IT may provide a tool to store, integrate,and update this information base.
Beyond improving care in individual settings, health ITalso has the potential to address the problems presented bya fragmented delivery system. Most patients receive carefrom many disparate providers. The primary means ofcoordination is often through discussion with the patientsabout what other services they have received and what theother providers thought about their conditions. Informationtechnology used across settings could create a “virtual”integrated delivery system without requiring formalmergers or affiliations.
The Commission stated in its June 2003 report to theCongress that health IT was one of the more importantsystem changes necessary to improve quality (MedPAC2003). While the potential is clear, the evidence linkingquality with various IT applications is less so.
In 2000, the Institute of Medicine (IOM) released a reportfocusing on patient safety estimating that 44,000 to 98,000people die in U.S. hospitals annually as a result of medicalerrors. Many of these errors involve medications. In asubsequent report, the IOM identified IT as one of the fourcritical forces that could significantly improve health carequality and safety (IOM 2001). Partly in response to thesereports, the Leapfrog Group, a group of large employerscommitted to patient safety improvements, made hospitaladoption of CPOE a major goal for large employers andhealth plans. These influential external forces linking IT toimproved quality and patient safety have contributed to awidespread belief that adoption of IT in health care willimprove quality and safety.
In this section we present findings from a literature reviewdone for MedPAC by Abt Associates on the relationshipbetween health IT applications and quality. We findevidence that various forms of health IT improve or havethe potential to improve quality. However, because manyof these findings were based on the experiences of a feworganizations without subsequent evaluation of the uniquecircumstances that may have led to their success, theresults may not be generalizable to other organizations.Two large academic medical centers with a strongcommitment to the use of health IT conducted many of thestudies of CPOE. Each developed its own system. Studies
have not critically analyzed how these systems wereimplemented. Implementation issues such as work flowdisruption, physician involvement, and ease of use havetremendous impact on whether health IT is effective.
Some studies have shown that use of CPOE can reduce thefrequency of medication errors. However, 9 out of the 11formal analyses took place at one of two advancedinstitutions. CPOE significantly reduced (by 55 percent)serious medication errors (Bates et al. 1998). Of the 11most rigorous studies, at least 1 study showed that CPOEimproved quality and safety through one of the followingactions:
• reducing medication errors, including adverse drugevents;
• decreasing dosage errors;
• prescribing certain medicines more precisely; or
• prescribing with improved accuracy by faculty andresidents (Oren et al. 2003).
Although more limited in the types of errors it can prevent,bar coding is probably the most proven technology ofthose we discuss. Bar coding prevents errors at thepatient’s bedside by averting the administration of thewrong drug when other levels of review have failed.Studies document that bar coding reduced ambulatory andinpatient medication error and the number of adverse drugevents (Oren et al. 2003, Bates and Gawande 2003, GAO2003). One study at a Department of Veterans Affairshospital showed that bar coding of medications reducedthe kind of medical errors bar coding could prevent by 85percent (McVicar and Valdes 2003).
The types of computer-based clinical decision supportsystems (CDSS) vary widely—from preventive carereminders to notification of potential drug interactions.Therefore, the types of technology studied vary widely. A1998 review of the literature on the impact of 68computer-based clinical decision support systems showeda beneficial impact on processes of care in 43 out of 65studies and a positive impact on patient outcomes in 6 outof 14 studies (Hunt et al. 1998).
Two studies of clinical decision support systems focusedon aspects of the medication system. One found thatcomputerized reminders improve by 100 percent the useof “corollary orders,” that is, orders for other
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 161

162 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
pharmaceuticals or tests that would ensure appropriatedosage (Overhage et al. 1997). Another studied a broadrange of CDSS and found improvements in types anddoses of drugs (Teich et al. 2000). In a review of theevidence on CPOE and CDSS, researchers found that oneimportant issue in ensuring successful implementation ofeither is that the threshold for alerts must be set so thatphysicians do not receive so many “false alarms” that theinformation is ignored (Kaushal and Bates 2001).
Electronic health records are often implemented withCPOE and decision support efforts; therefore, it is difficultto evaluate separately their impact on quality. However, anelectronic health record has the potential to make healthinformation more available to providers and patients whenthey need it. The availability of lab and radiology reports,patient-specific histories, and clinical reminders, alongwith other functions such as CPOE and bar coding, havethe potential to improve quality.
The quality benefits of investment in IT are often achievedafter tremendous efforts and some initiatives have failed.A recent study of the effect of computerized guidelines formanaging heart disease in primary care found thatsophisticated reminders from an EHR failed to improveadherence to accepted practice guidelines or outcomes forpatients with heart disease (Tierney et al. 2003). ADepartment of Veterans Affairs hospital that is the test sitefor a new computer software program recently reportedsurgery delays and other problems with its new computersystem (De La Garza 2004). Even when implemented,CDSS might not be used because of physician workload orlimited training for rotating staff (Patterson et al. 2004).Other research has shown that automated systems are alsosubject to errors: U.S. Pharmacopeia reported that 10percent of medication errors it studied resulted fromcomputer-entry errors (Armstrong 2003).
IT can be a tool for improving quality and safety, but isnot the only one and is often used by providers as part of abroader effort. In 2001, the Agency for HealthcareResearch and Quality (AHRQ) determined that 14 safetypractices had greater strength of evidence regarding theirimpact and effectiveness than any practice which relied onIT. They include such low-cost items as appropriateprovision of nutrition, with a particular emphasis on earlyenteral nutrition in critically ill and surgical patients, anduse of maximum sterile barriers while placing centralintravenous catheters to prevent infections (AHRQ 2001).This is not to say that these practices are superior to IT;ideally, organizations would pursue them all.
Current status of health informationtechnology
The degree of IT use varies by health care setting:Pharmacies are generally advanced users, while othersettings such as physician offices or nursing homes arefurther behind. The kind of technology used also varies bysetting. For example, in home health, the use oftechnology that allows patients to monitor their own vitalsigns from their home and communicate results to theagency could increase the ability to address a problembefore a patient requires acute care. In both home healthand nursing home settings, use of handheld computers tocomplete documentation and capture patient assessmentinformation can increase efficiency and provide moreinformation to care givers. IT and the Internet have alsohad a significant impact on consumers. Numerouswebsites have made health information more available topatients, thereby strengthening their role in care decisions.The Internet also helps consumers choose providers byallowing insurers and others (including Medicare) to postinformation on providers including, in some instances,comparative quality information.
This section provides detailed information on twosettings—hospitals and physicians’ offices—that havereceived considerable policy attention. Further MedPACwork may focus on other settings, such as post-acute care,as well as on the impact of IT and the Internet onconsumers. This section also looks at linking health careproviders through an information infrastructure, or“interoperable” systems that allow communication amongthe IT applications used by different providers.
Information technology in hospitals Relatively little is known about the level of diffusion of ITin hospitals and strategies hospitals take when making ITinvestment decisions. Much of the existing informationabout IT diffusion comes from voluntary surveys, some ofwhich are conducted on the Internet. Therefore, the resultsmay not be representative and may be biased toward moreadvanced users of IT. Given the evolving state of thetechnology and limited availability of nationallyrepresentative surveys, varying estimates of IT diffusionexist. The following discussion draws on a literaturereview on hospital IT investments conducted for MedPACby Abt Associates. It also draws on interviews AbtAssociates conducted with hospitals that have madesignificant investments in IT, and some that have not, to

better understand IT investment decisions (Abt Associates2004a and 2004b).
Diffusion of information technology in hospitals varieswith the type of technology. Of the three major categoriesshown in Table 7-1 (p. 159), diffusion is greatest inadministrative and financial applications such as patientregistration, billing, and payroll. Clinical applications,such as computerized provider order entry for drugs orother items (e.g., lab work) and electronic health records,are less diffused. Infrastructure technologies build the basethat other technologies work from, and include bothwidely diffused technologies, such as e-mail andtelecommunications, and those that are less common, suchas wireless connections and voice recognition.Infrastructure investments also include maintaining secureinformation systems that comply with federal securityrules.
Estimates of the use of CPOE vary, but several studiesreport that 5 to 6 percent of hospitals currently have asystem (Leapfrog Group 2004, Devers and Liu 2004).Others argue that these studies may have stringentdefinitions that lead to low estimates of CPOE use(iHealthBeat 2003). Estimates of the use of EHRs inhospitals are similarly low (Glaser 2002). Other types ofclinical IT—such as picture archiving andcommunications systems (PACS) that allow digitalstorage and retrieval of x-rays, MRIs, and other images—have diffused more widely. About 15 percent of allhospitals were estimated to have PACS in 2002, with mostacademic and large hospitals having this technology. In amore recent survey of hospital executives, 49 percentindicated that they had PACS or were implementing it(Morrissey 2004).
For each type of clinical IT, academic medical centers andlarge hospitals are more likely to be advanced users.Providers who are part of integrated systems deliveringinpatient and outpatient services are also more likely tohave the necessary financial support and a clearer need toensure smooth flow of information across their systems.Those who are part of multiple hospital systems (abouthalf of all hospitals according to the American HospitalAssociation Guide 2003–2004) probably benefit from ITsupport offered by the larger organization. They may alsobe motivated to adopt IT to facilitate information flowacross system members.
Clinical applications, particularly CPOE and EHR, maynot diffuse rapidly for a number of reasons. They are
relatively new. They are costly, complex, and difficult toimplement in stages. They require significant changes inwork processes and culture for nurses, pharmacists, otherallied health professionals, and physicians to besuccessfully implemented. Finally, achieving the benefitsof these technologies for improvements in quality of careappears to hinge on the same factors that pose a risk tosuccessful implementation. As discussed below, thefinancial return to investment for these technologies isuncertain.
Though not widely diffused now, many organizations areplanning to implement clinical systems in the near future.The Healthcare Information and Management SystemsSociety (HIMSS) has conducted a survey in each of thepast three years. The most recent web-based survey(conducted November 2003 through January 2004)included 307 respondents out of nearly 2,000 chiefinformation officers or directors of information systems athealth care facilities who were asked to participate. Mostof the respondents work for health care systems andhospitals; some 86 percent came from an organization ledby a hospital (HIMSS 2004a).
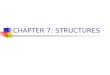
The HIMSS survey respondents reported that in the nextyear, upgrading security protocols and reducing medicalerrors and promoting patient safety will be priority issuesfor their IT departments (Figure 7-1, p. 164). Specificapplications they think most important for the next twoyears include bar coding, EHR, and clinical informationsystems (Figure 7-1, p. 164).
A recent survey of hospital investment priorities by theHealth Care Financial Management Association indicatedthat IT is as high a priority as capital construction. AmongIT applications, this survey suggested a different orderingof priorities than other surveys. The survey of 460 hospitaland system chief financial officers showed that 72 percentanticipate investing in PACS, 64 percent in CPOE, and 61percent in other major information technology. The samesurvey found that overall capital spending is expected torise 14 percent annually for the next five years, comparedwith 1 percent annual increases from 1997 to 2001(HFMA 2004).
Many systems and hospitals have recently announced ITplans. For example, Kaiser Permanente, an integratedsystem, is investing $1.8 billion to put in place a fullyoperational EHR. Catholic Health West recentlyannounced its intention to implement various forms ofhealth IT for all of its 41 hospitals.
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 163

164 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
Information technology priorities for hospitalsFIGURE7-1
Note: CPOE (computerized provider order entry), PACS (picture archiving and communications system).
Source: Healthcare CIO Results: Final Report, Leadership Survey, Healthcare Information and Management Systems Society, February 23, 2004.
Percent identifying activity as a priority
Hospital and health care executives name security and safety as top priorities for 2004
0
Upgrading security protocols
Implementing wireless systems
Implementing electronic health records
Upgrading network infrastructure
Designing process, workflow
Improving the IT department
Replacing, upgrading inpatient clinical systems
Reducing medical errors, promoting patient safety
30
30
402010 50 60
Hospital and health care executives name bar coding and other clinical applications as most important for 2004–2005
0
Bar-coded medication management
CPOE
PACS
Enterprise-wide clinical information sharing
Point-of-care decision support
Clinical information systems
Electronic health records
402010 50 60
Percent identifying application as important

Drivers of adoptionHospitals consider both financial return on investment andnonfinancial benefits when making IT investmentdecisions. Return on investment varies by the type of IT.Technologies that pay for themselves tend to diffuse morewidely. Studies dating back to the 1980s have shown thatelectronic billing and claims submission rapidly pay forthemselves and generate additional savings by decreasingthe costs of creating bills and speeding reimbursement.These technologies are practically universal. Hospitalshave also been quick to adopt other kinds of technologythat produce revenues, such as imaging equipment.
Little economic literature addresses the question of theimpact of IT on hospital financial performance. One studyoffers preliminary results indicating that investment in ITleads to increased volume in nonprofit hospitals andreduced length of stay in for-profit hospitals. The samestudy found that the longer the health IT investment, thegreater the effect (Parente and Van Horn 2002). Somereports suggest returns on investment or anticipatedsavings for several specific clinical applications. Voicerecognition software can pay for itself by loweringtranscription costs. PACS can lower costs for acquiringand storing films by storing digitized radiology images,and may reduce the workload among radiology staff(Wiley 2003). One study suggests an 18-month paybackperiod (Baldwin 2002).
Most of the hospitals with advanced IT systemsinterviewed by Abt used PACS: Of the 12 total, 10 had itin place, 1 was implementing it, and the last had put out arequest for proposals. Most of the hospitals had performedreturn on investment calculations and predicted positivereturns, which most realized. Recent diffusion estimatessuggest that PACS, at least, is becoming more common,perhaps in part because the financial return is evident.However, one of the smaller hospitals interviewed thatwas less advanced in its use of IT purchased PACS despitepredicting a negative return on investment. The projectedlack of return was due primarily to a low volume ofimaging in the facility.
The literature provides scant evidence of return oninvestment calculations for CPOE and EHR and we seelower diffusion of these technologies. Regarding CPOE,six of the interviewed hospitals have the system or areimplementing it, five plan to have it within one to threeyears, and only one had no plans to pursue it. In general,hospitals reported that patient safety and quality of care,
rather than financial returns, motivate their investments inCPOE and EHR. None of these hospitals had conducted orplanned to study return on investment for CPOE.
Calculating return on investment for clinical IT can bechallenging. The costs of CPOE and EHR can be difficultto measure because they require investment not only in thetechnologies themselves, but also in changing workprocesses, significant staff training, and ongoing systemsupport (Darves 2004). Quantifying some of the benefitsfor these applications, such as improved care processesand workflow, can be difficult. Reductions in costsstemming from reduced medical errors, shorter stays, orefficiencies in care delivery can also be hard to measure.
Furthermore, the financial returns from some qualityimprovements may accrue not to the hospital investing inthe technology, but to other parties. For example, ahospital might invest in CPOE and, through successfulimplementation, prevent an adverse drug event that wouldhave resulted in another hospital admission. The hospitalloses revenue from the avoided admission, and thepurchaser of care gains. In this example, the hospitalimproves care and the patient is clearly better off.
Closed systems of care, in which a single entity serves asboth the insurer and the provider of care, will reap all ofthe financial benefits from health IT. This may explainwhy closed systems, such as the Veterans HealthAdministration or staff model HMOs, are generally moreadvanced users of IT systems. One national health system,the National Health Service (NHS) in England, hasrecently committed to a large-scale implementation of IT(see text box, p. 166). The head of that effort recentlynoted that the NHS is able to do some things, such asnegotiate big discounts from IT vendors, that could not beeasily duplicated in the United States (AHA News Now2004).
The nonfinancial benefits hospitals consider when makingIT investment decisions include clinical efficiencies andimproved quality, patient and provider satisfaction, imageand public relations, and employee morale. A focus onimproved quality of care by the Institute of Medicine, theLeapfrog Group, and others has fueled interest in CPOE,in particular, as well as EHRs, other pharmacy systems,and lab systems. Those hospitals interviewed by Abt thathad more advanced IT systems indicated that patient careand safety were major drivers for adopting clinical IT.Consumer expectations and possible discounts on
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 165

166 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
malpractice insurance premiums for reduced medical errorrates have been cited as drivers of adoption (Scalet 2003).In addition, declining prices for IT technologies shouldfacilitate IT use.
Standards and regulations set by state and federalgovernments or accrediting agencies can also spurinvestment in IT. Electronic transaction standards put in
place through the Health Insurance Portability andAccountability Act of 1996 (HIPAA) should facilitateadoption of IT by removing some innovation barriers andproviding guidance for future investments, steeringhospitals away from applications that will not meet thestandards. Currently, hospitals are working to comply withHIPAA requirements to ensure the security of theirinformation systems (HIMSS 2004a). The recent
England plans for national information technology system
England’s government has begun contracting withinformation technology (IT) firms to implementa National Programme for IT (NPfIT) within the
National Health Service (NHS), the public agency thatprovides health care. The program consists of fourparts:
• electronic patient records, which will include acentral data repository of patient informationavailable to all health care providers;
• electronic scheduling of appointments forconsultations and hospitalizations that will beavailable to referring general practitioners and,eventually, patients;
• e-prescribing, which will allow electronicprescriptions filled by physicians to flow to both thepharmacy and the Prescription Pricing Authority thatmanages payments; and
• improved broadband communications networks tofacilitate communication across the National HealthService.
The NPfIT has an ambitious agenda that seeks toimplement the world’s largest health care IT system bythe year 2010. Because the health system in England isclosed, with the government employing staff, it canimplement a system that covers all patients andproviders. However, implementation will requirecoordination among the national health authority,regional health authorities, and local health care
providers, some of whom have already invested in theirown IT systems.
The NHS plans for the first element, electronicscheduling, to be available in some locations by thesummer of 2004, with full implementation by the endof 2005. The NHS will phase in the national databaseof electronic patient records by 2010. The NHS targetshaving 50 percent of prescriptions handledelectronically by 2005 and 100 percent by 2007.
Funding for the NPfIT includes $17 billion from thenational government, with additional funds comingfrom local health authorities. The central fundingcurrently covers only the cost of the technology, andnot the training and work process changes that will beneeded to implement health IT at the local level.
Supporters of the system predict significantimprovements in efficiency and quality of care, aspatient information will be accessible to all providers atany time. The system will also include decision-supportfunctions, such as clinical guidelines or prompts fordrug allergies. Supporters also claim that significantdiscounts can be obtained from IT contractors becauseof the size of the endeavor and the centralizedprocurement process. Others have noted the need forgreater attention to the availability of local funds forimplementation and training. Additional concernsinclude the need to involve stakeholders during design,ensure data quality, and implement adequate securityand privacy safeguards. �
Sources: Parliamentary Office of Science and Technology 2004, NHS 2004, Naik 2003, Dodge 2004.

requirement by the Food and Drug Administration (FDA)for pharmaceutical companies to include bar codes ontheir products within two years is likely to stimulateinvestment in bar coding in the near future (FDA 2004).2
However, the adoption of bar coding in hospitals maydepend on the extent to which manufacturers put bar codeson single doses of their medications, rather than puttingthem on a package containing multiple doses (Hawryluk2004).
Barriers to adoptionWhile many factors push hospitals to invest in IT, otherspose barriers. Investment in IT is costly and must competewith other priorities, including investment in bricks andmortar, as well as in technologies with more directapplication to clinical care and greater certainty forincreased revenues, such as new imaging equipment(Morrissey 2004). The availability of capital forinvestment in IT depends, of course, on hospitals’ abilityto access capital in general, which may be easier for somehospitals (e.g., those with good financial performance, for-profits, members of chains) than others. Recent estimatesof the percentage of hospital operating budgets spent onoperating IT systems indicate that 2 to 3 percent is theindustry average (Morrisey 2004, HIMSS 2004a). Capitalexpenditures on IT generally consume a larger share ofcapital budgets, although the percentage varies with eachhospital’s investment cycle.
Cost poses another barrier to adoption. The costs ofimplementation and ongoing maintenance vary by the sizeof the hospital, as well as by the functions to be installed.A full clinical IT system that includes CPOE and an EHRwill cost tens of millions of dollars; CPOE on its own wasestimated to cost about $8 million for a 500-bed hospital(First Consulting Group 2003). Installing bar coding isexpected to cost around $1 million for the average hospital(Hawryluk 2004). In addition to the costs of IT, hospitalsmay perceive lack of reimbursement for specific ITinvestments as a barrier.
The costs of implementing IT go beyond purchasing thetechnology to providing training and systems support,which case studies indicate are crucial for success.Deriving benefit from IT generally requires changingwork processes, which can be more challenging than thepurchase and installation of the technology itself (Darves2004, First Consulting Group 2003). New applicationsmust also integrate with existing systems, which makesimplementation more complex and can further increasecosts. For example, applications providing considerable
depth of support for a given department, such as PACS forradiology, may not communicate easily with an existingpatient registration system.
Nearly every study of clinical IT implementation andadoption cites physician reluctance as a major hurdle tobroader investment and overcoming it as a key to projectsuccess. A number of large-scale investments, includingthe one at Cedars-Sinai Medical Center in Los Angeles,have failed due to a lack of physician acceptance. With theexception of pharmacy settings, there is little consistentevidence that IT systems save time for providers. In someinstances, the literature suggests the reverse: Systems suchas CPOE add to clinicians’ workloads because informationmust now be entered into a computer. EHRs require evengreater levels of physician acceptance than CPOE (Darves2004, GAO 2003). The need for changes in work processand culture suggest that hospitals may not be able to movequickly when making IT investments because they canmanage only a limited amount of change at a time. Theneed to maintain full operations while undertakingsystems changes provides an additional challenge. Giventhe importance of culture and physician acceptance forimplementation of clinical IT, hospitals that employ alarge share of their physicians may find it easier toimplement because they have more control over how theirphysicians work.
Earlier we noted that federal and state regulations likeHIPAA can drive investment in IT. They may also slowadoption of some types of IT, however, if IT funds and theattention of hospital executives must be directed tospecific technologies over others. The HIPAA transactionrules require investments in IT supporting transactions,potentially at the expense of other investments. TheHIPAA privacy and security requirements may alsoincrease the complexity of the design of IT systems thatshare patient information.
In the latest HIMSS survey, respondents were asked toidentify the most significant barrier to implementing IT.Lack of financial support was cited most often; however, itwas chosen by fewer than one in four respondents (23percent). Respondents also considered the following to besignificant barriers:
• vendors’ inability to deliver products effectively (14percent);
• difficulty in providing quantifiable benefits or returnon investment from IT (13 percent); and
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 167

168 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
• difficulty achieving end-user acceptance (11 percent),among others.
Very few respondents (3 percent) considered lack ofcommon data standards to be a significant barrier (HIMSS2004a). The hospitals interviewed by Abt highlighted thefollowing as possible barriers to successfulimplementation of IT: cost, physician culture orreluctance, the need for concomitant changes in workflowand processes, retraining, poor quality of vendor offerings,and integration with existing systems.
Information technology in physicians’ practicesLike hospitals, physicians are more likely to use IT foradministrative functions (such as billing, claimssubmission, and scheduling) than for clinical functions(such as electronic health records, clinical decisionsupport, access to formularies or other references, orcomputerized provider order entry). Physicians must alsoinvest in infrastructure to support their IT applications.
Data on the use of IT by physicians and their staffs arelimited. This section reports the results of three surveys ofthe current and planned use of IT in physicians’ offices.For clinical IT, estimates of physicians’ use of EHRs intheir offices vary across surveys. Brailer and Terasawa(2003) suggest that 20 to 25 percent is a reasonableestimate of current diffusion. This estimate is higher thanthose generally quoted for hospitals, perhaps because theEHR is only one of many technologies hospitals arepursuing. A longitudinal record of patients’ care may bemore relevant in an outpatient clinic or office setting,where physicians coordinate care across settings.
The Center for Studying Health System Change (HSC)included questions on use of IT in its latest physiciansurvey. Although the information is somewhat dated—itwas conducted in 2000 and 2001—it is nationallyrepresentative of all physicians. HSC asked about use ofIT in the practice, not by the physician himself or herself.In addition, HSC did not gather information on thefrequency or intensity of IT use. The survey found thatadoption of IT varied by the application:
• 77 percent of physicians accessed the Internet,
• 53 percent obtained information on treatmentalternatives and clinical guidelines,
• 32 percent obtained information on formularies, and
• 11 percent used IT to write prescriptions (Reed 2004).
This survey compares IT use by practice and personalcharacteristics of the physician. Physicians in group andstaff model HMOs, practices with 50 or more physicians,and medical schools were most likely to use IT. Those insolo or small group practice were less likely to do so. Byspecialty, surgeons were less likely to be in practices thatuse IT than primary care physicians or those in medicalspecialties (Reed 2004). Some very large physician grouppractices, such as Harvard Vanguard Medical Associatesin Boston, the Marshfield Clinic in Wisconsin, andGeisinger Healthcare in Pennsylvania, have developed andoperated EHRs for 10 years or more.
The Healthcare Information Management Systems Societysurveyed physician and practice managers and executivesin 2003 on the use of IT in ambulatory settings. Only 16percent of the respondents (compared with about 35percent of physicians nationwide) were in a practice with1 or 2 physicians. Given that physicians in larger groupsare more likely to use IT, respondents likely representphysicians that use IT more than the national average(HIMSS 2004b).
The survey found widespread use of handheld technology,but significantly lower use of EHRs and e-mail forcommunicating with patients. The majority of surveyrespondents indicated that physicians have personal digitalassistants or some other form of handheld technology (71percent), used most commonly as a portable drugreference. Less common uses include scheduling, e-prescribing, better documenting care to facilitate billing(“charge capture”), dictating, and accessing information inan EHR. Sixty-two percent reported that they did not havean EHR, while small shares indicated that one was presentin all departments within their organization (24 percent),or in some departments (15 percent). Only 17 percentindicated that they or physicians in their organizationcommunicate with patients about clinical issues via e-mail.Reasons for not doing so included legal concerns, HIPAAprivacy concerns, and, to a much lesser extent, lack ofreimbursement.
A recent survey by Modern Physician/PricewaterhouseCoopers (436 respondents) suggests increases in the use ofIT by physicians. The survey was conducted online,however, which may bias the results toward users of IT.Forty-one percent of respondents indicated that theirorganizations have invested in an EHR, with investment

more likely in hospital-affiliated practices (61 percent)than in independent group practices (37 percent) (Versel2003). This echoes the findings by HSC, where practicetype was a predictor of IT use.
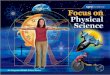
Physicians also reported using computers more foradministrative functions than for clinical functions
(Figure 7-2). The most common uses included billing orclaims submission and scheduling or patient appointmentreminders. Placing lab orders or getting results bycomputer was also common. Small shares of respondentsreported that physicians used computer-based systems toaccess clinical protocols or pathways, write prescriptions,or conduct telemedicine.
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 169
Physicians use computers more for administrative than clinical functionsFIGURE7-2
Note: The survey asked, “What do your physicians use computer-based systems for?” Charge capture means better documenting care to facilitate billing.
Source: Modern Physician/PricewaterhouseCoopers survey of executive opinions on key information systems issues, Modern Physician, November 2003.
Percent using computers for function
0
Billing and claims submission
Communication with hospital
Claims status
Patient records
Patient eligibility
Diagnostic imaging and radiology
Lab orders and results
Scheduling and patient appointment reminders
30 402010 50 60 70 80 90
Charge capture
Clinical protocols and pathways
Prescribing
Telemedicine
None of the above
Procurement of supplies
Referrals

170 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
Drivers of adoption As is the case with hospitals, a variety of motivesinfluence physicians’ use of IT. Financial returns arecertainly one consideration. We found few studies,however, on the return on investment for physician use ofIT. One might conclude that the widespread use of IT foradministrative and financial functions (e.g., billing andaccounting) indicates that these systems do bear afinancial return, or are at least useful for practicemanagement.
The evidence of a link between larger practice size andgreater use of clinical IT suggests that having a largerrevenue base or more complex practice with greatermanagement capabilities allows larger groups to bettersupport the sizeable investments needed to implementinformation systems. In addition, economies of scalereduce the per physician cost of investing for largergroups. Finally, larger groups may also have more needfor IT to communicate within the practice.
Although clinical systems require up-front financialinvestment, some argue that physicians can benefitfinancially from the increased documentation of care,leading to fewer rejected claims and enhanced revenues(CITL 2003, Versel 2003). For EHRs, savings also accruefrom reduced transcription and medical recordsmanagement costs, as physicians enter informationdirectly into the EHR and can retrieve information moreefficiently (Miller and Sim 2004).
A qualitative study of 30 physician organizations that hadEHRs found that the financial returns were uncertain, anddepended on the extent to which physicians used the EHR(Miller and Sim 2004). The study found that “the path toquality improvement and financial benefits lies in gettingthe greatest number of physicians to use the [EHR] (andnot paper) for as many of their daily tasks as possible.”Some of the practices realized no financial gains, but a fewrealized gains of more than $20,000 per physician peryear. Physicians rarely used all the capabilities of theEHR, and most combined paper processes with the EHR.
A recent study looked at the value of CPOE in ambulatorysettings and estimated that nationwide adoption couldimprove patient outcomes and save money for the healthcare system as a whole by avoiding adverse drug eventsand related hospitalizations, and by suggesting cost-effective use of medications, lab tests, and radiology(CITL 2003). These savings will not all accrue to the
providers implementing the system. However, the studyprojected that physicians could increase revenues throughthe use of IT by reducing the cost of rejected claims by atleast $10 per outpatient visit.
Both financial and nonfinancial incentives encouragephysician use of IT. In a recent survey, physiciansindicated that improving business performance, improvingthe clinical quality of care, and managing growth in thesize of the physician practice motivated the adoption of IT(Versel 2003). Moving to an EHR can decrease storagecosts for medical records; increase access, security, andefficiency of medical records; and improvedocumentation. Rooms previously used for storing paperrecords may be converted to patient exam rooms. Inaddition, some insurers are providing discounts onmalpractice when physicians have IT systems becausethey provide better documentation of the care provided(Scalet 2003).
Advances in technology or financing arrangements mayfurther spur use. Open source software that has nolicensing requirements can lower the cost of technology.In addition, some specialty organizations have negotiateddiscounts from vendors for their members. Alternatively,application service providers have begun to promotearrangements in which they own and maintain thesoftware and store data for physicians, who pay a monthlyaccess fee (Chin 2004).
Barriers to adoptionMany barriers slow physician adoption of IT. The costs ofinvesting in IT can be significant, the financial return isnot certain, and any financial benefits will not necessarilyall accrue to the physician practice bearing the costs. Mostcurrent payment policies do not include incentives for useof IT. The small size of many practices makes the start-upand maintenance costs of IT systems difficult to manage.Costs vary tremendously with the characteristics of thepractice and the applications involved. In one study, theaverage cost of an EHR varied from $16,000 to $36,000per physician (Miller and Sim 2004). Even if cost is not anissue, the complexity of the technology, limitations in theproducts currently on the market, and the time it takes tocomplete implementation pose barriers. Implementing andsupporting IT applications requires skills that have nottraditionally been part of a medical practice. In addition,physicians must make significant changes to both officeand physician workflow and take time away from seeing

patients to learn how to use IT (Brailer and Terasawa2003, Miller and Sim 2004).
Beyond the financial and technological concerns, the useof electronic systems for clinical reminders may not agreewith some physicians’ clinical practice styles, which mayrely primarily on their knowledge and experience. Inaddition, use of computers may be seen as interrupting thephysician-patient relationship by drawing away from thepersonal interaction. These systems may add to aphysician’s workload, rather than alleviating it,particularly in the initial implementation (Brailer andTerasawa 2003, Miller and Sim 2004).
Linking health care providers through information technology For information technology to become widespread,individual providers must adopt it. Once that happens,connecting them electronically could bring additionalbenefits. Health care today involves considerable sharingof information among providers such as physicians’offices, hospitals, imaging centers, and clinicallaboratories, as well as among providers and payers. Ahealth care information infrastructure would provide thenetworks and standards to allow providers within acommunity to share information electronically. Inaddition, patients could use it to access their medicalrecords or other health care information from all providers.A primary focus of those advocating a health careinformation infrastructure is development of standards formessaging so that one IT system can communicate withanother.
Few systems allow communication among providerstoday, although some cities are sharing information acrossemergency departments. Two communities have moved tohave a more comprehensive ability to share information.In Indianapolis, an intranet connecting some hospitals tofacilitate sharing of clinical information is underdevelopment. In California, Santa Barbara County has acentral system collecting radiology, pharmacy, and labreports that can be accessed by providers, payers, andlaboratories (Broder 2004).
Some see a health care information infrastructure as a keybuilding block to encourage investment by providers andincrease its value. The goal is interoperability—the abilityfor information to flow among settings of care. Theinformation infrastructure would consist of standards andnetworks that allow electronic communication among
providers, so that, for example, the electronic recordcreated during a hospital stay is accessible to the primarycare physician, or even becomes part of the electronicrecord maintained by the primary care physician.Interoperability could increase the usefulness ofimplementing IT and decrease the risk of investing in asystem that might quickly become obsolete. The healthcare information infrastructure has been a major focus ofthe Department of Health and Human Services (HHS) anda number of private initiatives, such as the eHealthInitiative and projects at the Markle Foundation.
A study to be released in 2004 suggests that standardizedhealth care information exchange could reduce nationalhealth care spending by automating how providers sharedata (CITL 2004). Currently, telephone, fax, and mail aremost often used for communication among health careproviders. Patients themselves also serve as a conduit ofinformation among providers. Electronic communicationcould reduce repeat tests and expenses for administrativetasks. However, the low diffusion and riskiness ofinvestment in IT suggest that interoperability is manyyears off. If providers do not have IT systems in place, aninformation infrastructure will have limited use. However,having an infrastructure in place may provide an incentivefor further adoption.
Efforts to encourage faster diffusion
In the previous sections, we find that current levels ofclinical IT diffusion are relatively low but increasing, andthat rates of adoption vary by type of provider andtechnology. Barriers to adoption are multifaceted andcomplex, making investment in health IT a riskyproposition for many providers. A primary driver ofadoption of IT, the need to improve quality is compelling.We find potential for IT to improve quality and patientsafety, but further evidence is needed. The question is notwhether to push for further adoption, but how, and howfast. The implementation experience of those providerswho have adopted various forms of IT suggest that cautionis warranted to ensure effective, broad implementation.
Market forces that inhibit faster diffusionof health information technologyResearch comparing diffusion of IT in different industrieshas identified two key criteria for broad diffusion: 1) theexternal market must reward the product of IT, and 2) the
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 171

172 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
organization must be capable of sustaining its commitmentto IT and continually respond to changing needs of theusers of the IT (Givens 2003). Certain attributes of thehealth care market may impede faster diffusion:
• Quality, a main reason for investing in IT, is notrewarded. While awareness of the problem is growing,payments for health care do not distinguish betweenproviders who furnish a higher quality product andthose who produce a lower quality product. Ratherthan rewarding higher quality, most fee-for-servicepayment systems emphasize volume of services. Thecurrent system rewards volume by paying every timea procedure or service is provided, regardless of itsquality. This approach encourages adoption oftechnology that supports provision of a billableservice, such as an MRI, over technology that mightimprove the quality of many services. This approachalso leads providers to try to see as many patients aspossible rather than ensuring that every patientreceives the best care possible. Clinical ITapplications sometimes add time to patientinteractions with physicians, thus causing physicianresistance to using IT, even though giving orders orhaving information available electronically could leadto higher quality care.
• The financial rewards may bypass the purchaser of IT.If a physician group invests in an IT system to bettermanage the care of their patients with chronicconditions, lower levels of hospitalization can result.But unless the change results in additional officevisits, only the payer benefits financially; thephysician group does not. If a hospital invests inCPOE to reduce adverse drug events, it could lead tofewer complications and readmissions—leading tocost savings for the payer, but lower payment for thehospital. Integrated delivery systems that combineinsurance and service delivery functions are capableof capturing savings from the use of IT and tend to bemore sophisticated users.
• The fragmented nature of health delivery also impedesfurther adoption. Without organized delivery systems,it is difficult for individual providers to adopt healthIT applications capable of communicating acrosssystems of care.
These broader market factors operate on top of the barriersto adoption noted previously, including the complexity of
implementation. The IOM recognized these complexitiesin its Crossing the Quality Chasm report.
“The challenge of applying information technologyto health care should not be underestimated. Healthcare is undoubtedly one of the most, if not the most,complex sectors of the economy. The number ofdifferent types of transactions (i.e. patient needs,interactions, and services) is very large. Sizablecapital investments and multi-year commitments tobuilding systems will be required. Widespreadadoption of many information technologyapplications will require behavioral adaptations onthe part of large numbers of patients, clinicians, andorganizations.”
The complexity and implementation costs are furtherexacerbated by the impression that vendors’ products donot necessarily perform as anticipated. On the recentHIMSS survey, the second most important reason givenfor not investing in IT was “vendors’ inability toeffectively deliver products.”
Over time, the market may naturally ease some of thesebarriers. Development of improved products could reducethe hesitation to invest. Physician acceptance mayaccelerate with more user-friendly versions andexperience. In the long term, adoption of uniformstandards also should help providers share informationacross settings of care and make investment decisions lessrisky.
However, market barriers such as fragmentation andmisaligned payment systems are fundamental problems.Current public and private efforts are attempting to correctfor many of these, but more changes may be needed tocreate conditions necessary for health IT to becomebroadly available to providers and the patients they treat.
Public and private effortsThe initiatives described in this section, in one form oranother, attempt to either strengthen the drivers of healthIT or lower the barriers. Numerous public and privateinitiatives have generally focused on one or more of thefollowing (Table 7-2):
• developing or adopting standards,
• providing incentives for providers to use health IT, or
• giving grants for research and implementation.

Several organizations, both public and private, are alsoattempting to coordinate the various stakeholders to ensureas focused an effort as possible. HHS is leading theNational Health Information Infrastructure (NHII)initiative to coordinate public and private efforts to createa national infrastructure.
Private sector organizations, such as the eHealth Initiativeand its affiliate, Connecting for Health (a group made upof a broad set of public and private sector stakeholders),and the National Alliance for Health InformationTechnology (a group made up of leaders from all healthcare sectors) are also funding strategic collaboration.
Standards development and adoptionDeveloping and adopting standards can help ensure asmooth flow of health information across providers.3 TheCongress and HHS have focused on this need in the pastfew years.
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 173
Through HIPAA, the Congress required HHS to developstandards for transactions, such as billing and claimsattachments, and required a standard policy related to theprivacy and security of health information. These effortscreated a base for standardizing health data more broadly.The privacy and security rules, for example, madediscussions of broad sharing of patient informationpossible. However, while HIPAA required thedevelopment of standard ways to move administrativedata, it did not address standardization of clinical data.4
Current HHS efforts are focused on adopting standardizedclinical messaging mechanisms and terminology. In thisarena, the public sector has been a catalyst to stimulatedevelopment and adoption, and the private sector has, forthe most part, developed the standards.
The Department of Health and Human Services has takena lead role to ensure that standards are adopted within thefederal agencies and more broadly. Working withnumerous private sector organizations and with other
Public and private health information technology initiatives
Standards Incentives Grants
Publicmmm
Note: HIPAA (Health Insurance Portability and Accountability Act of 1996), HHS (Department of Health and Human Services), EHR (electronic health record), IOM(Institute of Medicine), IT (information technology), MMA (Medicare Prescription Drug, Improvement, and Modernization Act of 2003), FDA (Food and DrugAdministration), AHRQ (Agency for Healthcare Research and Quality), CPOE (computerized provider order entry), AAFP (American Academy of Family Physicians).
T A B L E7-2
• Transactions, privacy, security, andprovider, plan, and employer identifiers(HIPAA)
• HHS adoption of standards for federalagencies and EHR functionality initiative
• E-prescribing standards (MMA)• IOM work to encourage use of IT in health
care• Commission on Systemic Interoperability
(MMA)
Private• Health Level 7 efforts to create functional
model of EHR• Numerous private sector standards
development efforts for administrativefunctions, prescriptions, labs, and clinicalterminology
• Physicians’ and standard-setting groups’development of standard definitions andterminology for a continuity of care record.
• Physician incentives through Medicaredemonstration and Medicare Advantageplans (MMA)
• FDA requirement for manufacturers tobarcode pharmaceuticals
• Leapfrog efforts to encourage CPOE• Plan and purchaser inclusion of physician
use of IT as a quality measure• AAFP effort to create affordable open-
source architecture for small practices
• Matching grants for e-prescribing (MMA)• AHRQ research on value of IT and
implementation strategies
• Markle Foundation grants to eHealthInitiative
• Regenstrief and Santa Barbara communitygrants

174 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
federal agencies such as CMS, the Department of VeteransAffairs (VA), AHRQ, and the Department of Defense, ithas broadly defined its goal as developing the NHII. Theinitiative is defined as “the technologies, standards,systems, values, and laws that enable health information tobe appropriately and safely shared among all relevanthealth decision-makers to promote improvements in healthand healthcare.” HHS’s goals include faster adoption ofclinical IT in provider settings, and across providers andgovernment agencies.
These goals require standard terms and messagingformats. HHS initiatives include:
• Giving providers the rights to use the SystemizedNomenclature of Medicine (SNOMED). HHS hasobtained the rights to the comprehensive standardmedical vocabulary of SNOMED and will make itavailable at no charge. Prior to this policy, providershad to pay for the rights to use this system forclassifying clinical information.
• Working with the Health Level 7 ( HL7) group, aprivate sector standards development organization, todefine the functions of an electronic health record. Asa first step, HHS asked the IOM to define the keycapabilities of an EHR. The IOM defined five primaryand five secondary uses of an electronic health recordsystem upon which HL7 is basing its work.
• Adopting standards for use in electronic interactionswithin the federal government. Through theConsolidated Health Informatics (CHI) initiative,HHS is working with other federal agencies to adoptcertain private sector standards for governmentagencies, such as CMS, the VA, DoD, and the Centersfor Disease Control and Prevention (CDC). Throughthis effort, the federal government is hoping to promptthe private sector to standardize clinical andmessaging terminology and logic. The CHI initiativeset out to identify all aspects of health care deliverythat may need to have standards and seek privatesector organizations that already developed standards.CHI initiative staff analyze the standards’ utility withadvice from private sector experts. The CHI initiativeis focused on 24 clinical domains. Five standards wereadopted by the federal government in March of 2003(Table 7-3). On May 6, 2004, the Secretary announcedthat HHS had adopted 15 more standards for theelectronic exchange of information across agencies.
The MMA calls for further adoption of standards. Toencourage use of e-prescribing in the new Medicareprescription drug benefit, the MMA required the Secretaryto adopt standards for such transactions. The MMA alsoestablished a Commission on Systemic Interoperability.This commission is to study the best strategy, including a“timeline and prioritization for such adoption andimplementation,” to create a nationwide system ofinteroperability of IT. The provision requires thecommission to consider the costs and benefits ofstandards, both financial and qualitative; the currentdemand on industry resources to implement the MMA andother electronic standards, including those in HIPAA; andcost-effective and efficient ways for industry to implementthe standards.
External incentives for use of healthinformation technologyThe primary driver of adoption—the relationship betweenIT and quality improvement—may be strengthened bygrants for research on the value of health IT, but also bypurchaser and plan expectations and incentives for high
Standards adopted by theConsolidated Health Informatics initiative
Note: ACR (American College of Radiology), NEMA (National ElectricalManufacturers Association), DICOM (Digital Imaging and Communicationsin Medicine), LOINC (Logical Observation Identifiers Names and Codes).
T A B L E7-3
Source of standard
Health Level 7
Joint Committee of the ACR andNEMA
National Council on PrescriptionDrug Programs
Institute of Electrical andElectronics Engineers
Regenstrief Institute
Type of information
Order entry, scheduling, admitting,discharge, and transfer
Imaging information (DICOM)
Drug ordering between retailpharmacies and health careproviders
Information exchange betweenmedical devices and the computersystems that receive theinformation (IEEE 1073)
Lab test result names (LOINC)

quality care. The concept the Commission adopted in itsJune 2003 and March 2004 reports to include incentivesfor quality improvement in the Medicare payment systemis one approach to encouraging use of IT. By rewarding aquality product, Medicare, in its purchaser role, couldprovide incentives for providers to adopt the technologynecessary to improve quality. Other strategies includeincreased payment for use of certain forms of health ITand increased reporting on quality measures. Manyorganizations find that reporting on quality measuresrequires an information system to track and report data.
Our research found a variety of private sector models inwhich incentives for quality either directly or indirectlyencouraged further diffusion of health IT. CMS has begunto explore some of these models through demonstrations.The MMA also included incentives for e-prescribing.These types of incentives are aimed at strengthening thedrivers of health IT adoption by creating an externalincentive for investment.
One way in which purchasers and plans are encouraginghealth IT use is by including measures of provider ITadoption in the quality indicators they use to rewardproviders. For example, the Leapfrog Group, anorganization made up of large purchasers, has included theadoption of CPOE as one of its key patient safety goals.As a result, hospital adoption of CPOE has become apriority for some health plans. One health plan—EmpireBlue Cross Blue Shield—in concert with several largeemployers gave direct bonuses to hospitals forimplementing the Leapfrog goals, including CPOE. InSeattle, Boeing is charging employees no copay for usinghospitals that meet Leapfrog Group standards, includinguse of CPOE. In other hospitals, patients will have to pay5 percent of their bill (Freudenheim 2004). The Bridges toExcellence initiative by several large employers hasphysician use of certain IT tools as one measure ofphysician quality. CMS is also considering such anapproach in its Doctors Office Quality project.
A less direct approach to encouraging diffusion is toreward the outcome of implementing health IT, forexample, higher quality. The relationship betweenrewarding providers for higher quality and implementationof IT is not proven. However, collecting and analyzing thedata necessary to measure quality performance, andimplementing process improvement, is easier with IT.Further, because an IT system can track patients and sendphysicians automatic reminders, physicians with IT can
identify patients who need certain diagnostic or preventiveservices.
Some private sector organizations are giving IT toproviders. Anthem Blue Cross Blue Shield and Wellpointare purchasing computers and certain software for many ofthe physicians in their networks. These plans expect tobenefit from the purchase. While this practice does notappear widespread, a recent regulatory clarification maymake it easier in the future. CMS recently issued a finalrule implementing certain provisions of the Stark II Lawwhich allows doctors to receive “technology items orservices” to encourage them to participate in community-wide health information systems.
Mandating use of a specific technology is yet anotherapproach. This has not been done directly. However, theFDA’s recent regulation requiring pharmaceuticalmanufacturers to place bar codes on their products pointsin this direction. While the rule does not require hospitalsto purchase and use the technology necessary to read thecodes on the pharmaceutical products, the FDA hopes theavailability of the coding will encourage hospitals to doso. In addition, the Joint Commission on Accreditation ofHealthcare Organizations recently proposed adding arequirement for bar coding in future hospital accreditationstandards.
Grants for research and implementationPublic and private sector grants are funding research onthe value of IT and implementation models forcommunity-wide or provider-setting adoption. TheAgency for Healthcare Research and Quality is allotting$10 million in fiscal year 2004 to create a better researchbase on the value of implementing IT. The request forapplications seeks information to allow stakeholders tomake more informed decisions regarding adopting andusing IT. AHRQ also has $7 million available for assistinghealth care systems in planning successful health ITimplementation and $24 million for organizational andcommunity-wide implementation.
The President’s budget request for 2005 calls for $50million more for hospital information technology grantsthrough AHRQ. In addition, the MMA authorized $50million in 2007 and such sums as necessary in 2008 and2009 for matching grants for physicians to purchase thesoftware and hardware necessary to e-prescribe.5
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 175

176 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
The private sector has also used grants to fund efforts toencourage further diffusion. Some of these efforts arenational collaborations around diffusion and community-level initiatives. The Markle Foundation has identifieddiffusion of health IT as a priority and funded a variety ofefforts to identify strategies to encourage diffusion. In2002, the Foundation convened and funded Connectingfor Health, a group of more than 100 public and privatestakeholders to work on data standards, privacy, andsecurity issues, and to spur national efforts to create anational health information infrastructure. In 2004, theRobert Wood Johnson Foundation is acting as a partnerwith the Markle Foundation to fund Phase II, which willlook at community-wide exchange of information,information sharing with patients, and adoption of dataexchange standards.
The Healthcare Collaborative Network (HCN) issupported by Connecting for Health, the eHealth Initiative,and IBM. The HCN is a national demonstration projectdesigned to show the feasibility of an electronicinfrastructure. It involves the electronic exchange of labresults, prescriptions, and clinical procedures amongseveral major delivery systems, including New YorkPresbyterian, Vanderbilt University Medical Center, andWishard Memorial Hospital. Several governmentagencies—CDC, FDA, and CMS—are also involved.
To support community-level projects to exchangeinformation electronically, the Foundation for the e-HealthInitiative, with $3.86 million in funding from the HealthResources and Services Administration’s office forAdvancement of Telehealth, will be giving grants toseveral communities for seed funding and other supportfor individual communities who are using IT to drivequality improvements.
In addition to these national efforts, local private sectorgroups have provided funding for two of the most well-known community-level initiatives. The RegenstriefInstitute worked with hospitals in Indianapolis to create asecure platform to share patient information and iscurrently expanding its efforts to a broader group ofproviders. In Santa Barbara, the California HealthcareFoundation provided seed money to create a system forsharing patient information among a variety of providersand public health organizations.
Potential additional actionOver time, these efforts may speed adoption of health IT.Providers who have already implemented IT successfullydid so over a lengthy time period and used a step-by-stepapproach. But significant barriers remain for manyproviders, and the market forces encouraging adoption areweak. Current efforts may need to be expanded or newstrategies developed to stimulate broader diffusion ofhealth IT.
Several legislative proposals, information technologyexperts, and research groups, such as the IOM, havesuggested other ways to encourage faster adoption of IT.6
Options include:
• Payment policy. Purchasers and plans can encouragethe adoption of IT by: 1) paying more to providerswho adopt certain forms of information technology or2) paying more for the quality product that may resultwhen information technology is used. The privatesector is using some of these payment options.However, as yet, the government has not chosen toadopt them.
• Loan funds. To provide the necessary investmentfunds, some have suggested establishing a healthtechnology loan fund or regional funds. The concept,outlined in a paper written by The Health TechnologyCenter, and widely discussed, described a revolvingfund that would be administered at the state level withmatching state and federal dollars (The HealthTechnology Center 2003). These types of funds couldalso be funded by private foundations. The state-levelaffiliates would decide how the loans would bedistributed, including the types of informationtechnology appropriate for support and the amountsand terms of the loans. These loans could also be usedto leverage investment from capital markets.
While loans would address the cost barrier, it wouldbe important to ensure that those who qualified for theloans had the capacity to implement and continue tosupport the health IT. We found through our analysisthat organizations often took a step-by-step approachto implementation, beginning with limitedapplications, and broadening the functions used over aperiod of several years. To do so required strongleadership, clear strategies for retraining all levels ofpersonnel, and a commitment to redesigning the care

process without disrupting clinical care. Loanrecipients will need this level of commitment andinfrastructure for implementing health IT. Withoutsuch an infrastructure, the IT projects funded may fail,thus leading to further concern that implementinghealth IT is too risky. Because of the need to learnmore about successful implementation strategies,loans might need to be tied to some evaluationstrategy.
Loans would also need to be well targeted toorganizations that cannot afford health IT on theirown. As our analysis shows, health organizations ofall types are beginning to adopt a wide variety of ITapplications. In addition, some applications may beencouraged over others to ensure a step-by-stepapproach.
• Grants. The federal government and privatefoundations are already using grants to spur furtherdiffusion, but these efforts could be expanded. Federalgrants could encourage further private sectorinvestment. The proposal discussed above forestablishing loan funds also envisions some grants. Indesigning grant programs, strong criteria forevaluation would allow learning from the grantees’lessons that could be applied more broadly. Inaddition, the projects should be designed so that oncethe grant funding ends, the project can be self-
sustaining. In the long term, health IT must besustained through market forces. It would also beimportant to target funds to those who are unable toinvest on their own.
• Requirements to adopt specific technology. TheMedicare program or private payers could also requireproviders to adopt certain types of technology, such asCPOE for hospitals. Alternatively, the government orother payers could require organizations to performthe types of functions for which IT is often used. Forexample, CMS could require physicians to keep trackof preventive services given to diabetic patientsthrough electronic patient registries or paper records.Over time, the provider may find adoption of IT totrack patients more efficient.
Our review shows that IT use in health care is growing,but providers do experience barriers. Implementation isdifficult, making the risk of investment high. Many publicand private organizations support increased use of healthIT, but more may be necessary. MedPAC will continue tomonitor diffusion efforts, including assessing diffusion insettings other than hospitals and physician offices andlooking at the impact of IT on consumers. We will alsoanalyze in more depth potential public actions toencourage diffusion, including efforts within the Medicareprogram. �
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 177

178 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
1 The Institute of Medicine identified the following core caredelivery-related capabilities as necessary for an EHR thatpromotes patient safety: patient health information and data,results management, order entry, decision support, electroniccommunication and connectivity, patient support,administrative processes, and reporting and population healthmanagement. Few, if any, EHRs currently in use have all ofthese capabilities (IOM 2003).
2 The two-year implementation period allows for someexceptions.
3 While standards adoption is critical in the long run, in theshort term, standards adoption could create switchover costsfor some providers and slow purchasing decisions that aredependent on standards yet to be introduced.
4 HIPAA did require the National Committee on Vital andHealth Statistics (NCVHS) to make recommendations onsome forms of clinical coding. NCVHS has discussed whetherto move from ICD–9–CM coding to ICD–10–CM. HIPAAalso required and the Secretary adopted standards forpharmacy information.
5 For these funds to be used, the Congress will need toappropriate them in this year’s budget.
6 The IOM has published a variety of reports on encouragingdiffusion of health IT and the importance of health IT toquality delivery of health care. One specific proposal includedin a report on graduate medical education was to base some ofthe distribution of indirect medical education funds onhospital adoption of IT.
Endnotes

Abt Associates, Inc. 2004a. Summary of findings from the secondround of MedPAC hospital IT investment interviews. Deliverablesubmitted to MedPAC. Cambridge, MA: Abt Associates.
Abt Associates, Inc. 2004b. Summary of findings from the firstround of MedPAC hospital IT investment interviews. Deliverablesubmitted to MedPAC. Cambridge, MA: Abt Associates.
Agency for Healthcare Research and Quality. 2001. Makinghealth care safer: A critical analysis of patient safety practices.Evidence Report/Technology Assessment no. 43 (July): 624–631.
AHA News Now. 2004. UK health service IT chief predictsshakeout among health care IT providers AHA News Now(February 25). http://www.hospitalconnect.com.
Armstrong, D. 2003. Study finds increase in medication errors atU.S. hospitals. Wall Street Journal. November 18.
Bates, D. W., and A. A. Gawande. 2003. Improving safety withinformation technology. New England Journal of Medicine 348,no. 25 (June 19): 2526–2534.
Bates, D. W., L. L. Leape, D. J. Cullen, et al. 1998. Effect ofcomputerized physician order entry and a team intervention onprevention of serious medication errors. Journal of the AmericanMedical Association 280 no.15 (October 21): 1311–1316.
Baldwin, F. D. 2002. Healthcare PACS for the future. HealthcareInformatics (November): 38–43. http://www.healthcare-informatics.com.
Brailer, D. J. 2004. Policy options for improving health careefficiency and quality through adoption of interoperableelectronic health records. Working paper. Health TechnologyCenter. San Francisco, CA. April 16.
Brailer, D. J., and E. L. Terasawa. 2003. Use and adoption ofcomputer-based patient records in the United States: A reviewand update. Manuscript. California Healthcare Foundation. March28. Oakland, CA.
Brailer, D. J., N. Augustinos, L. Evans, et al. 2003. Movingtoward electronic health information exchange: Interim report onthe Santa Barbara County data exchange. Oakland, CA:California Healthcare Foundation. July.
Broder, C. 2004. Health information exchange projectsunderscore challenges, successes. iHealthBeat. January 6.http://www.ihealthbeat.org.
Center for Information Technology Leadership. 2004. Newfindings show that investment in standardized healthcareinformation exchange would deliver $87 billion in annualhealthcare savings. Press release, CITL, Boston, MA.February 23.
Center for Information Technology Leadership. 2003. The valueof computerized provider order entry in ambulatory settings.Boston, MA: CITL.
Chin, T. 2004. Financing high-tech: You can afford it after all.American Medical News (March 8). http://www.ama-assn.org/amednews.
Darves, B. 2004. CPOE: The promise and the pitfalls.HealthLeaders (February 5). http://www.healthleaders.com.
De La Garza, P. 2004. VA vows to retrain Bay Pines staffers. St.Petersburg Times. March 23.
Devers, K. J., and G. Liu. 2004. Leapfrog patient-safetystandards are a stretch for most hospitals. Issue brief no. 77.Washington, DC: Center for Studying Health System Change.February.
Dodge, J. 2004. Exclusive: A conversation at HIMSS withRichard Granger. Health-IT World (March 29). http://www.bio-itworld.com/archive/retort/.
First Consulting Group. 2003. Computerized physician orderentry: Costs, benefits and challenges, a case study approach.Prepared for American Hospital Association and Federation ofAmerican Hospitals. January.
Food and Drug Administration. 2004. Bar code labelrequirements for human drug products and biological products.Final rule. Federal Register 69, no. 38 (February 26): 9119–9171.
Freudenheim, M., 2004. Many hospitals resist computerizedpatient care. New York Times. April 6.
General Accounting Office. 2003. Information technology:Benefits realized for selected health care functions. no.GAO–04–224. Washington, DC: GAO. October.
Givens, R. 2003. Clinical transformation: Cross-industry lessonsfor health care. New York: Deloitte Research.
Glaser, J. P. 2002. The strategic application of informationtechnology in health care organizations. Hoboken, NJ: Jossey-Bass.
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 179
References

180 I n f o rma t i o n t e c hno l ogy i n h ea l t h c a r e
Hawryluk, M. 2004. FDA targets medication errors by requiringbar codes on drugs. American Medical News (March 15).http://www.ama-assn.org/amednews.
Health Technology Center. 2003. Spending our money wisely:Improving America’s health care system by investing in healthcare information technology. San Francisco: HTC.
Healthcare Financial Management Association. 2004. Financingthe future report 2: How are hospitals financing the future? Thefuture of capital spending. Westchester, IL: HFMA. March.
Healthcare Information and Management Systems Society.2004a. 15th Annual HIMSS Leadership Survey. Final Report:Healthcare CIO. Chicago, IL: HIMSS. February 23.http://www.himss.org.
Healthcare Information and Management Systems Society.2004b. Ambulatory technology survey. Chicago, IL: HIMSS.February 9. http://www.himss.org.
Hunt, D. L., R. B. Haynes, S. E. Hanna, et al. 1998. Effects ofcomputer-based clinical decision support systems on physicianperformance and patient outcomes: A systemic review. Journal ofthe American Medical Association 280, no.15 (October21):1339–1346.
iHealthBeat. 2003. Report: Health care IT spending growthcontinues. iHealthBeat. November 20.http://www.ihealthbeat.org.
Institute of Medicine. 2003. Key capabilities of an electronichealth record system. Washington, DC. July 31.
Institute of Medicine. 2002. Leadership by example:Coordinating government roles in improving health care quality,ed. J. Corrigan, J. Eden, and B. Smith. Washington, DC: NationalAcademy Press.
Institute of Medicine. 2001. Crossing the quality chasm: A newhealth system for the 21st century. Washington, DC: NationalAcademy Press.
Institute of Medicine. 2000. To err is human: Building a saferhealth system. ed. L. Kohn, J. Corrigan, and M. Donaldson.Washington, DC: National Academy Press.
Kaushal, K., and D. W. Bates. 2001. Making health care safer: Acritical analysis of patient safety practices. Agency forHealthcare Research and Quality Evidence Report/TechnologyAssessment no. 43. Chapter 6. pg. 59-69. July.
Medicare Payment Advisory Commission. 2004. Report to theCongress: Medicare payment policy. Washington, DC: MedPAC.
Medicare Payment Advisory Commission. 2003. Report to theCongress: Variation and innovation in Medicare. Washington,DC: MedPAC.
Leapfrog Group. 2004. Leapfrog Group survey: Summary.http://www.leapfroggroup.org.
McVicar, N., and A. M. Valdes. 2003. Hospitals seek RX fordrug mistakes bar-coding, computers help cut errors. SouthFlorida Sun-Sentinel. Ft. Lauderdale, Fla. pg.1.A. July 7.
Miller, R. H., and I. Sim. 2004. Physicians’ use of electronicmedical records: Barriers and solutions. Health Affairs 23, no. 2(March/April): 116–126.
Morrissey, J. 2004. Capital crunch eats away at IT. ModernHealthcare 34, no.8 (February 23):32–62.http://www.modernhealthcare.com.
Naik, G. 2003. England plans major revamp of health care. WallStreet Journal. December 3.
National Health Service. 2004. Making IT happen: Informationabout the National Programme for IT. London, UK: NHS.
Oren, E., E. R. Shaffer, and B. J. Guglielmo. 2003. Impact ofemerging technologies on medication errors and adverse drugevents. American Journal of Health System Pharmacists 60, no.14: 1447–1458.
Overhage, J. M., W. M. Tierney, X. H. Zhou, et al. 1997. Arandomized trial of “corollary orders” to prevent errors ofomission. Journal of the American Medical InformaticsAssociation 4, no. 5 (September/October):364–375.
Parente, S., and R. Van Horn. 2002. Hospital investment ininformation technology: Does governance make a difference?Paper presented at the American Economic Association annualmeeting, January. Washington, DC.
Parliamentary Office of Science and Technology. 2004. NewNHS IT. Postnote Number 214 (February). London, UK: POST.
Patterson, E. S., A. D. Nguyen, J. P. Halloran, et al. 2004. Humanfactor barriers to the effective use of ten HIV clinical reminders.Journal of the American Medical Informatics Association 11, no.1 (Jan/Feb).
Reed, M., Center for Studying Health System Change. 2004.Memorandum to Chantal Worzala, February 3.
Rosenfeld, S., and D. Mendelson. 2004. Health informationtechnology policy: Legislative and regulatory progress in 2003and prospects for the future. Washington, DC: Health StrategiesConsultancy.

Rosenfeld, S., E. Zeitler, and D. Mendelson. 2004. Financialincentives: Innovative payment for health information technology.Washington, DC: Health Strategies Consultancy.
Scalet, S. 2003. Saving money, saving lives. CIO Magazine(August 1). http://www.cio.com.
Teich, J. M., P. R. Merchia, J. L. Schmiz, et al. 2000. Effects ofcomputerized physician order entry on prescribing practices.Archives of Internal Medicine160: 2741–2747.
Tierney, W. M., J. M. Overhage, M. D. Murray, et al. 2003.Effects of computerized guidelines for managing heart disease inprimary care. Journal of General Internal Medicine. vol.18 no.12(December): pg. 967-976.
Versel, N. 2003. Faith-based spending and other articles. ModernPhysician (November): 14–25.
Wiley, G. 2003. The PACS payoff. Imaging Economics: TheJournal of Imaging Technology Management (September).
Repo r t t o t h e Cong r e s s : New App roache s i n Med i ca r e | J u ne 2004 181


![INSTALL GUIDE OEM CH RS CH7 ADS CH7 EN - …cdncontent2.idatalink.com/.../RS-CH7/...CH7-[ADS-CH7]-EN_20160811.pdfU.S. Patent No. 8,856,780 BOX CONTENTS](https://img.dokumen.tips/doc/110x75/5af03fd77f8b9ad0618dd202/install-guide-oem-ch-rs-ch7-ads-ch7-en-ads-ch7-en20160811pdfus-patent.jpg)