Embed Size (px)
Citation preview

Psychotropics in Psychiatric Patient - Psychotic disorders:
Pharmacology and Clinical Applications of Antipsychotics
Pongsatorn MeesawatsomB. Pharm., M.Sc. (Pharmacology)
Faculty of PharmacySrinakarinwirote University

Characteristics of schizophrenia
Prevalence 0.5–1.0% of populationOnset
Positive features in late adolescence or early adulthoodAspects of cognitive deficits detectable earlier in life
ComorbidityDepression: 30–50%∼Substance abuse: 50%∼Suicide: 5–10%∼

Schizophrenia: A Disease with Various Aspects
Positive SymptomsDelusions
HallucinationsDisorganized speech
Catatonia
Negative SymptomsAffective flattening
AlogiaAvolition
AnhedoniaSocial withdrawal
Cognitive DeficitsAttentionMemory
Executive functions(e.g., abstraction)
Mood SymptomsDepression
AnxietyAggression
HostilityHopelessness
Suicidality
Social/OccupationalDysfunction
WorkInterpersonal relationship
sSelf-care

Inter-relationship between disease factors and drug-induced adverse factors in the burden of schizophrenia
Int Clin Psychopharmacol 2005, 20:183–198.
Adverse effect of antipsychotic drugs
Risk of hyperglycemia/ diabetes
Other effects•Anticholinergic•Prolactin elevation•QTc prolongation
SedationExtrapyramidal
symptoms
Tardive dyskinesia
Weight gain
Suicidality
Dysphoria
Diverse symptoms of schizophrenia
Positive symptoms
Cognitive symptoms
Negative symptoms Depression/Anxiety
Disease factors
Drug-induced factors

Treatment Goal of Schizophrenia
Rapid symptom control
Acute Phase TreatmentAcute Phase Treatment Stabilization Phase Stabilization Phase TreatmentTreatment
Maintenance Phase Maintenance Phase TreatmentTreatment
Patient relationship Insight on medication
Relapse/recurrence prevention
Adherence Functional recovery
Initiation of therapeutically effective dose
No need for initial dose titration for tolerability
Minimal drug-drug interaction
Proven efficacy and safety
Increased tolerance to occasional missed doses
Proven relapse prevention effect
Improved PSP

Factors affecting antipsychotic response
Receptor pharmacology(binding capacity)
Pharmacokinetics Pharmacogenetics(CYP450)
Patient variables Comorbid condition/polypharmacy

The Dopamine hypothesis of psychosis
Overactivity of dopamine neurons in the mesolimbic dopamine pathway may mediate the positive symptoms
Dopamine hypocactivity in mesocortical dopamine pathway may mediate the negative and cognitive symptomsDorsolateral prefrontal cortex – negative, cognitive
symptomsVentromedial prefrontal cortex – negative, affective
symptoms

Brain dopaminergic tracts
11
22
33
44
6 Lateral hypothalamus6 Lateral hypothalamus5 CTZ5 CTZ

Simplify Neurocircuitry of Dopamine in Schizophrenia
DA
Mesolimbic pathwayHyperdopaminergia
D2
Positive symptoms
DA
Mesocortical pathwayHypodopaminergia
D1
Negative symptomsCognitive symptomsAffective symptoms
Limbic PFCx

Antipsychotic Drugs: Development Timeline
Minimal efficacy with regard to positive
symptoms in 20-30% of patients
Much weaker effect on negative
symptoms than positive symptoms
Significant parkinsonian symptoms and
anticholinergic effects (poor
compliance and potentially disabling)
Tardive dyskinesia in a minimum of
20% of patients who receive chronic
neuroleptic treatment.
At least as effective as typical
neuroleptics with regard to positive
symptoms
More effective than typical agents with
regard to negative symptoms
Much lower incidence of parkinsonian
symptoms and anticholinergic effects
than typical agents
TD does occur but at much lower
incidence
Elevated risk of metabolic side effects

Therapeutic effects from D2 receptor blockade
Amelioration of the positive signs, symptoms of psychosis, manic symptoms, aggressive behaviors
Antiemetic effect
Modified J Clin Psychiatry 1999;60(suppl 10):5–14.

Adverse effects from D2 receptor blockade
Extrapyramidal symptom (EPS)Acute; akathisia, acute dystonia, parkinsonism
Late; tardive dyskinesia
Endocrine effects: prolactin elevation
Weight gain due to increase feeding
Modified J Clin Psychiatry 1999;60(suppl 10):5–14.

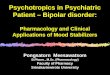
Binding affinities of chlorpromazine and haloperidol for various receptor
J Psychiatr Pract 2005;11:258–61.

Higher potency
Higher EPS
Lower anticholinergic effect
Lower potency
Low EPS
Higher anticholinergic effect
HaloperidolFluphenazine
Trifluoperazine
Thioxanthine
Perphenazine
Pimozide
Chlorpromazine
Thioridazine
Mesoridazine

Rational explanations for SDA therapeutic effects
Therapeutic effects D2-receptor blockade in the mesolimbic pathway to reduce
positive symptomsEnhanced dopamine release and 5-HT2A receptor blockade
in the mesocortical pathway to reduce negative symptoms
Side-effect profile5-HT2A antagonism in the nigrostriatal pathway reduces EP
S and tardive dyskinesia5-HT2A antagonism in the tuberoinfundibular pathway reduc
es hyperprolactinemia

DA
D1D2
Caudate/putamen
Normal function
Sunstantia nigra pars
compacta
5-HT2A
-
5-HT
Raphe
5-HTT
Role of 5-HT in Nigrostriatal Dopaminergic Synapse
Nigrostriatal tract

DA
D1D2
Caudate/putamen
EPS
5-HT2A
-
5-HT
Raphe
5-HTT
Role of 5-HT in Nigrostriatal Dopaminergic Synapse
Nigrostriatal tract
Haloperidol
Sunstantia nigra pars
compacta

DA
D1D2
Caudate/putamen
Less EPS
5-HT2A
-
5-HT
Raphe
5-HTT
Role of 5-HT in Nigrostriatal Dopaminergic Synapse
Nigrostriatal tract
SDA
Sunstantia nigra pars
compacta

Modified from Clin Ther 2004;26:649-66
All values are reported as Ki (nM).
Receptor affinities of selected atypical antipsychotic
s
Receptor HAL CLOZ OLAN RIS QUET ZIP ARI
D2 0.7 126 11 4 160 5 0.45 (partial)
5-HT1A 2600 875 >7100 210 >830 3 4.4 (partial)
5-HT2A 45 16 4 0.5 295 0.4 3.4
5-HT2C 1500 16 23 25 1500 1 15
1 6 7 19 0.7 7 10 57
2 360 8 230 3 87 – –
H1 440 6 7 20 11 47 61
M1>1500 1.9 1.9 >10,000 120 >1,000 >10,000

Effects of blockade of neuroreceptors
Receptors Effects of blockade
D2 Anipsychotic, antimanic, antiaggressive, EPS/akathisia, tardive dyskinesia, increase prolactin, weight gain
5-HT1A Anxiolytic, antidepressant, anti-EPS/akathisia
5-HT2A Anti-EPS/akathisia, possible antipsychotics, improve REM sleep
5-HT2C Possible increased appetite/weight
Modified from J Clin Psychiatry 2008;69[suppl4]:26-36.

Effects of blockade of neuroreceptors
Receptors Effects of blockade
1 Postural hypotension, dizziness, syncope, nasal
congestion
2 Antidepressive effect, increase alertness,
increase blood pressure
H1 Anxiolytic, sedation, weight gain, potentiate CNS
depressant drug
Modified from J Clin Psychiatry 2008;69[suppl4]:26-36.

Effects of blockade of neuroreceptors
Receptors Effects of blockade
M1
(central)
Memory dysfunction, delirium, confusion, sedation,
REM sleep disturbance , anti-EPS
M2, M3
(peripheral)
Blurred vision, attack or exacerbation of narrow-angle
glaucoma, dry mouth, sinus tachycardia, constipation,
urinary retention, interfere pancreatic insulin release
Modified from J Clin Psychiatry 2008;69[suppl4]:26-36.

Impact of receptor binding affinity on clinical
responses of antipsychotics

Modified from Clin Ther 2004;26:649-66
All values are reported as Ki (nM).
Receptor affinities of selected atypical antipsychotics: Potential risk
Receptor HAL CLOZ OLAN RIS QUET ZIP ARI
D2 0.7 126 11 4 160 5 0.45 (partial)
5-HT1A 2600 875 >7100 210 >830 3 4.4 (partial)
5-HT2A 45 16 4 0.5 295 0.4 3.4
5-HT2C 1500 16 23 25 1500 1 15
1 6 7 19 0.7 7 10 57
2 360 8 230 3 87 – –
H1 440 6 7 20 11 47 61
M1 >1500 1.9 1.9 >10,000 120 >1,000 >10,000 Orthostatic
hypotension
Anticholinergics
Sedation, weight gainEPS risk and
hyperprolactinemia

Modified from Clin Ther 2004;26:649-66
Receptor affinities of selected atypical antipsychotics: Potential Benefit
Receptor HAL CLOZ OLAN RIS QUET ZIP ARI
D2 0.7 126 11 4 160 5 0.45 (partial)
5-HT1A 2600 875 >7100 210 >830 3 4.4 (partial)
5-HT2A 45 16 4 0.5 295 0.4 3.4
5-HT2C 1500 16 23 25 1500 1 15
1 6 7 19 0.7 7 10 57
2 360 8 230 3 87 – –
H1 440 6 7 20 11 47 61
M1 >1500 1.9 1.9 >10,000 120 >1,000 >10,000 PD psychosis BPSD, autism Sedative action
All values are reported as Ki (nM).
Sleep quality improvement
Alleviate EPS risk

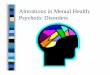
*Receptor activity measured as inhibition of forskolin-induced cAMP accumulation in CHO cells transfected with human D2L DNA.
Adapted from Burris et al. J Pharmacol Exp Ther. 2002;302:381.
0
50
100
Drug Concentration
Max
imu
m D
A R
esp
on
se (
%)*
Dopamine
100 nM Dopamine+ Haloperidol
100 nM Dopamine+ Aripiprazole
Aripiprazole
10-10 10-9 10-8 10-7 10-6 10-5
Aripiprazole Activity at Cloned Human D2 Receptors
Haloperidol
Full Receptor Activity
PartialReceptor Activity
(Modulated)
No Receptor Activity
(Blocked)

Paliperidone vs Risperidone
Paliperidone is active metabolite of risperidone via metabolism by CYP2D6.
High affinity for D2, 5-HT2A, 1 and 22 receptors receptors
Very low affinity for M1 as same as as risperidone
Expert Opin Drug Saf. 2007 ;6(6):651-62.

Pharmacokinetics differences of risperidone and paliperidone
Risperidone Paliperidone
Tmax 1-2 hr (risperidone)
3 hr (paliperidone in CYP2D6 EM)
17 hr (paliperidone in CYP2D6 PM)
1-2 Hr (IR form)
24 hr (ER form)
T1/2 3 hr 23 hr (IR and ER
form)
Elimination
pathway
CYP2D6 to paliperidone (major)
CYP3A4 (minor) CYP3A4 to (minor)
inactive metabolite
and >80% found in
urine and
60%unchanged

Adverse Effect Profile of Antipsychotics

Past Areas of Concern
Current Medical Realities
Shift in Risk Perception of Antipsychotics
SedationWeight Gain
Insulin Resistance
CHD
Hyper-lipidemia
Weight Gain
Diabetes
Prolactin
Insulin Resistance
Sedation
Hyperlipidemia
Coronary HeartDisease
Tardive Dyskinesia
TD
Prolactin

D2 Blocking-related Side Effects

Spectrum of EPSL
ate
on
set
Acu
te
on
set

Acute dystonia

Relationship between clinical effectiveness, EPS and D2 receptor occupancy
Threshold for EPS
Threshold for antipsychotic
efficacy
80%


Medication used to treat EPS
Am J Health-Sys Pharm 1997;54:2461-77.

Association of medication, target dose, and likelihood of treatment-emergent EPS
J Psychiatric Pract 2007;13:13–24.

Tardive dyskinesia (TD)
TD is a latent extrapyramidal effect generally not occurring for months or years, occur in 20% patient treated with antipsychotic.
It is characterized by abnormal movements that can occur in any part of the body, including faces, tongue, shoulders, hips, extremities, fingers, and toes

Prominent Feature of TD
Lingual-facial hyperkinesias Chewing movements
Smacking and licking of the lips
Sucking movements
Tongue movements within the oral cavity
Tongue protrusion
Tongue tremor with mouth open
Myokemic movements (worm-like movement on the surface of the tongue)
Blinking
Grotesque grimaces and spastic facial distortions
Neck and trunk movements Spasmodic torticollis
Retrocollis
Torsion movements of the trunk
Axial hyperkinesia (hip-rocking)
Choreoathetoid movements of the extremities

Neuroleptic malignant syndrome
NMS is an uncommon but serious and potentially fatal complication of therapy
It is a syndrome of EPS, hyperthermia, altered consciousness, and autonomic changes (tachycardia, unstable BP, incontinence)
Management Discontinuation of the antipsychotic agents Supportive therapy Bromocriptine may be benificial
The onset is sudden and recovery may take 5-10 days after discontinuation of the agent

Simplified Pathophysiology of Neuroleptic Malignant Syndrome (NMS)
Am J Psychiatry 2007;164:870-876.

Spectrum-based concept of NMS
J Am Acad Child Adolesc Psychiatry 1992;31:1161–4.

Proposed Treatment Algorithm for NMS Spectrum-Related Symptoms
Am J Psychiatry 2007;164:870-876.

Hyperprolactinemia: possible signs and symptoms
J Clin Psychopharmacol 2007;27:639–661.
Osteoporosis

Mean Plasma Prolactin Level Changes Over 24 Hours in 18 Patients After Taking Clozapine, Olanzapine, or Risperidone and in Five of the Same Patients After Not
Taking the Drugs
Am J Psychiatry 2002; 159:133–135

Effects of Antipsychotics on Prolactin Levels
J Clin Psychopharmacol 2007;27:639–661.

Sedation

Receptor blocking properties that affect arousal and sleep stages
Blocking of H1 sedation
Blocking of M1 sedation, REM sleep
interference
Blocking of 1, 2, 5-HT2A promote cholinergic
pedunculopontine (PPT) and laterodorsal
tegmental nuclei (LDT) firing REM sleep
improvement

Clin Ther 2004;26:649-66All values are reported as Ki (nM).
Receptor affinities of selected atypical antipsychotic
s
Receptor HAL CLOZ RIS OLAN QUET ZIP ARI
D1 210 85 460 31 455 525 265
D2 0.7 126 4 11 160 5 0.45 (partial)
D3 2 473 10 49 340 7 0.8
D4 3 35 9 27 1600 32 44
5-HT1A 2600 875 210 >7100 >830 3 4.4 (partial)
5-HT2A 45 16 0.5 4 295 0.4 3.4
5-HT2C 1500 16 25 23 1500 1 15
1 6 7 0.7 19 7 10 57
2 360 8 3 230 87 – –
H1 440 6 20 7 11 47 61
M1>1500 1.9 >10,000 1.9 120 >1,000 >10,000

SGAs and sedation
J Clin Psychiatry 2008;69 Suppl 1:18-31.

Obesity and metabolic
syndromes

Clinical issues of weight gain and antipsychotics
Not everyone gains weight
Difficult to predict who will have weight
gain
Multifactorial etiology
Not dose related ADR.
Start in first few weeks
Reach plateau between 3 months to 1 year

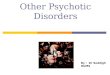
Mean weight gain during treatment withantipsychotic drugs.
CNS Drugs 2005; 19 (Suppl. 1): 1–93.

Mechanisms of antipsychotic-induced weight gain and metabolic abnormalities
Interfere feeding behavior by blocking many
neuroreceptorFeeding center
Lateral hypothalamus (DA D2)
Ventromedial hypothalamus (5-HT 5-HT2A, 5-HT2C)
Satiety center
Paraventricular nuclei (NE 1, , Histamine H1)
Interfere pancreatic insulin release
Pancreas (ACh M3 )

AtropineAtropine OlanzapineOlanzapine ClozapineClozapine
ZiprasidoneZiprasidone RisperidoneRisperidone HaloperidolHaloperidol
Diabetes 2005; 54:1552–1558.

Clin Ther 2004;26:649-66All values are reported as Ki (nM).
Receptor affinities of selected atypical antipsychotic
s
Receptor HAL CLOZ RIS OLAN QUET ZIP ARI
D1 210 85 460 31 455 525 265
D2 0.7 126 4 11 160 5 0.45 (partial)
D3 2 473 10 49 340 7 0.8
D4 3 35 9 27 1600 32 44
5-HT1A 2600 875 210 >7100 >830 3 4.4 (partial)
5-HT2A 45 16 0.5 4 295 0.4 3.4
5-HT2C 1500 16 25 23 1500 1 15
1 6 7 0.7 19 7 10 57
2 360 8 3 230 87 – –
H1 440 6 20 7 11 47 61
M1>1500 1.9 >10,000 1.9 120 >1,000 >10,000

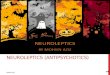
Olanzapine-Associated Weight Gain Plateaus After First 39 Weeks of Treatment
Kinon BJ, et al. J Clin Psychiatry 2001;62:92-100
Week
Mea
n W
eigh
t Cha
nge
(kg)
up
to 3
yea
rs
OLZ (N=573)
HAL (N=103)
-8 -6 -4 -2 0 2 4 6 8
0 20 40 60 80 100 120 140 160Patients Observed for 39 Weeks or More;Double-blind and open-label olanzapine.
LOCF; Median = 2.5 Years
Weight gain by olanzapine is
not dose dependent (5-20 mg dose range).

Why Less weight gain in quetiapine, ziprasidone and aripiprazole?
QuetiapineNorquetiapine inhibit
norepinephrine reuptake transporter
AripiprazoleLow affinity H1, 5-HT2C
Partial D2 agonist
ZiprasidoneModerate affinity for 1
Low affinity H1
Full 5-HT1A agonist
Inhibit 5-HT/NA reuptake transporter

SGAs and metabolic abnormalities
Clin Psy 2007;68(Suppl 7):27-33.

Monitoring protocol for patients on SDAs
Baseline 4 weeks 8 weeks 12 weeks Quarterly Annually Every 5 years
Personal/family history ()Weight (BMI) () ()Waist circumference () () () () ()Blood pressure () () () ()Fasting
plasma glucose
() () () ()Fasting lipid profile () () ()
Diabetes Care 2004; 27(2): 596-601.

Other Adverse effects
QTC interval prolongationThioridazine, ziprasidone
AgranulocytosisClozapine
EpileptogenicClozapine
Retinitis pigmentosaThioridazine > 800 mg/day

Incidence of categorical increases in QTc (Bazett correction)
There is a consensus that a QTc interval of >500ms, or an absolute in-crease of 60ms compared with drug-free baseline, puts a patient at significant risk of torsade depointes, ventricular fibrillation and sudden death

Clozapine safety issues
Clozapine is one of the atypical agents that is EPS/TD free, as same as quetiapine
However, clozapine is still reserved as last-line therapy because of its increased incidence of agranulocytosis, myocarditis/cardiomyopathy, and convulsion and the need for frequent monitoring

Clozapine safety issues
Seizure risk1-2% and increase to 3-5% if dose is greater than 600
mg/day.
Agranulocytosis1% in general95% cases in first 6 m,
peak in 4-18 week CBC weekly

Management of clozapine-induced agranulocytosis
US
New patients: weekly blood
counts
Twice weekly monitoring: WBC
3000-3500 and ANC >1500
Temporary discontinuation: WBC
2000-3000 and/or ANC 1000-
1500
Permanent discontinuation: WBC
<2000 and/or ANC <1000
> 6 months: monitor once every
two weeks
UK
New patients: weekly blood
counts
Weekly monitoring: WBC 3000-
3500 and/or ANC1500-2000
Discontinue: WBC <3000 and/or
ANC ≤1500
Weeks 19-52: at least every 2
weeks
> 52 weeks: monitor at least
monthly thereafter

Contribution of CYP450 in atypical antipsychotic drug metabolism
DrugCYP450
1A2 2C9/2C19 2D6 3A4
Aripiprazole Clozapine Olanzapine /-
Paliperidone
/-
Quetiapine Risperidone Ziprasidone
(1/3 with
aldehyde oxidase)

Enzyme Substrate Inhibitor Inducer
CYP1A2 Clozapine, olanzapine Fluvoxamine, ciprofloxacin
Carbamazepine, smoking
CYP2C19 Fluoxetine, fluvoxamine Carbamazepine, phenytoin
CYP2D6 Aripiprazole, clozapine, olanzapine, risperidone, conventional antipsychotics
Bupropion, fluoxetine, paroxetine, duloxetine
CYP3A4 Aripiprazole, clozapine,, quetiapine, ziprasidone
Azole antifungalMost of macrolide except
azitromycinARVs; indinavir,
nelfinavir, ritonavir
Carbamazepine,phenytoin, rifampin, phenobarbital

Dose-response curve for seizure risk with clozapine
Dose-response curve for extrapyramidal adverse effects with risperidone
J Psychiatric Pract 2005;11:116-122.

Acute treatment of psychoticpatients
Injectable, conventional agents are typically used such as haloperidol 5-10 mg IM or zuclopenthixol acetate 50150mg
It may be given every hour untilAcute symptoms are controlled
Side effects occur
Patient falls asleep
Once control has been obtained, the patient can be converted to oral therapy

Selection of antipsychotic agents
Based on the patient’s history and safety profile of the available agents
Newly diagnosed patients, the APA suggest initiating therapy with atypical agent (SGAs) because of these agents’improve safety profile

Monitoring of first episode
Less disturbed sleep patterns and decreased anger and anxiety should be observed within the first day or two of treatment, with gradual improvement in other symptoms in the first week and near-maximal effects in six to eight weeks
Lack of improvement in the first one to four weeks should prompt an increase in the dose, followed by a change to another drug, usually clozapine or another second-generation drug after an additional four to six weeks, if the response remains inadequate
N Eng J Med 2003;349:1738-49.

Monitoring of early adverse effects
It appears within days to weeks of starting the antipsychotic dose
It maybe transient and time limited (it will be disappear after the first month of treatment)
J Clin Psy 2007;68(Suppl 7):34-43.

Initial dose and titrationschedule for a firstepisode
J Clin Psy 2007;68(Suppl 7):3443.

Strategies for managing side effects in stable patients
J Clin Psy 2007;68(Suppl 7):34-43.

Medical Issues in Schizophrenia
Factor Prevalence in Schizophrenia
Prevalence in
General Population
Smoking 75% 25%
Obesity 50% 33%
Diabetes Mellitus 13-14% 7%
HIV 3% 0.3%
Hepatitis C 20% 1.8%
Other:
-inactivity, poor nutrition
-substance use
Meyer JM and Nasrallah H eds. Medical Illness and Schizophrenia. APPI 2003Regenold WT, et al. Increased prevalence of type 2 diabetes mellitus among psychiatric inpatients with bipolar I affective and schizoaffective disorders independent of psychotropic drug use. Journal of Affective Disorders. 2002 Jun;70(1):19-26

Medical conditions that may influence antipsychotic treatment dicisions

Antipsychotics switching
Avoid if possibleConsider in
Not responing patient with adequate trialNot able to tolerateNon-compliance (switch to depot preparation)Significant long term risk with current medication
Obesity, TD, persistent cognitive deficit, CVS problems, DDI
Patient/family member request

Switching techniques for antipsychotics
CNS Drugs 2005; 19 (1): 27-42

Dopaminergic considerations
Cross switching of 2 high potency D2
antagonist may increase EPS risk.
J Clin Psy 2007;68(Suppl 7):109.

Dopaminergic considerations
Prolong exposure of high potency D2 antagonist
results in D2 supersensitivity
Switching D2 antagonist from higher potency to
lower potency or D2 partial agonist
May lead to switch-emergent dopamine psychosis.
Improvement in prolactin-related side effects such as galactorrhea, amenorrhea and sexual dysfunction and EPS

Muscarinic considerations
There is a potential that patient who have been maintained on anticholinergic antipsychotics to develop cholinergic supersensitivity.
Nausea, vomiting and insomnia may occur when anticholinergic drugs is withdrawn or switched to less potent anticholinergic drugs.

Muscarinic considerations
If patient is being changed because of EPS in which an anticholinergic agents was initiated, the patient can remain on the anticholinergic agent until the cross taper and titrated is completed
Exception in the case of clozapine being added as the new therapy, the anticholinergic drugs should be discontinued when the cross taper and titration begins

Estimated side effects after switching
J Clin Psy 2008;69(Suppl 1):4-17.

Conclusions
Antipsychotics are not uniform drug class which different in their pharmacological profile, efficacy and ADRs.
Adherence of treatment should be enhanced by various strategies e.g.Counseling Awareness of DDIADR monitoring and management